Journal of Lymphoedema - Wounds · PDF fileexperience of lymphoedema treatment and care Case...
28
Editorial Lymphoedema and the impact of social and societal factors – can we do better? Research and audit Head and neck lymphoedema management practices Detecting subclinical secondary lymphoedema using bioimpedance: A preliminary study Practice development Evidence and tradition in conflict: The Swedish experience of lymphoedema treatment and care Case report Use of a two-layer compression system in severe bilateral leg lymphoedema with ulceration: A case report THE BIANNUAL ONLINE JOURNAL FOR IMPROVING PCTICE, ISING AWARENESS AND SEING STANDARDS FOR CARE December 2013 Vol 8 Issue 2 Lymphoedema JOURNAL OF ISSN 1750-7235
Transcript of Journal of Lymphoedema - Wounds · PDF fileexperience of lymphoedema treatment and care Case...

EditorialLymphoedema and the impact of social and societal factors – can we do better?
Research and auditHead and neck lymphoedema management practices
Detecting subclinical secondary lymphoedema using bioimpedance: A preliminary study
Practice developmentEvidence and tradition in conflict: The Swedish experience of lymphoedema treatment and care
Case reportUse of a two-layer compression system in severe bilateral leg lymphoedema with ulceration: A case report
THE BIANNUAL ONLINE JOURNAL FOR IMPROVING PRACTICE, RAISING AWARENESS AND SETTING STANDARDS FOR CARE
December 2013 Vol 8 Issue 2
LymphoedemaJournal of
ISSN 1750-7235

Listen to June’s story at kerramaxcare.co.uk
Dedicated to Exudate Management
Crawford Healthcare Ltd | King Edward Court | King Edward Road | Knutsford
Cheshire | WA16 0BE | UK | Tel +44 (0)1565 654920 | Email [email protected]
KerraMax & KerraMax Care are trade marks of Crawford Woundcare Ltd | © Copyright Crawford Healthcare Ltd, 2013.
She was too embarassed to eatlunch with the other residents.
I vowed to change all that.JUNE – INDEPENDENT NURSE CONSULTANT
NEW IMPROVED
DRESSING
12343 KerraMax Lunch 280x210 Ad JTV.indd 1 01/02/2013 16:00

Journal of Lymphoedema, 2013, Vol 8, No 2 3
LymphoedemaJournal of
Editorial
Lymphoedema and the impact of social and societal factors – can we do better? 5
Neil Piller
Research and audit
Head and neck lymphoedema management practices 8
Amanda Purcell
Detecting subclinical secondary lymphoedema using bioimpedance: A preliminary study 16
Maho Takeuchi, Toyoko Yoshizawa, Yuko Kusaka, Yoshihito Furusawa,
Yasuka Nakamura, Fumi Atogami, Hitoshi Niikura
Practice development
Evidence and tradition in conflict: The Swedish experience of lymphoedema treatment and care 21
Polymnia Nikolaidis, Katarina Karlsson
Case report
Use of a two-layer compression system in severe bilateral leg lymphoedema with ulceration: 24
A case report
Malou van Zanten, Beth Kean
Instructions for authors 27
December 2013 Vol 8 Issue 2

David Addiss Senior Program Officer, Fetzer Institute, Kalamazoo, Michigan, USA
Jane Armer Professor, Sinclair School of Nursing , Director, Nursing Research, Ellis Fischel Cancer Center, University of Missouri-Columbia, Columbia, Missouri , USA
Jane Bostock Lymphoedema Specialist, Senior Occupational Therapist, Royal Cornwall Hospital, Truro, Cornwall, UK
Rebecca Billingham Macmillan Lymphoedema Nurse Specialist, University Hospital of North Staffordshire, Stoke-on-Trent, Staffordshire, UK
Håkan Brorson Consultant Plastic Surgeon, The Lymphedema Unit, Department of Plastic and Reconstructive Surgery, Malmö University Hospital, Malmö, Sweden
Anne Clements Lymphoedema Specialist, Bristol North Primary Care Team, Bristol, UK
Isabel Forner Cordero Specialist in Physical Medicine and Rehabilitatio, Lymphedema Unit, Hospital Universitario La Fe, Valencia, Spain
Robert Damstra Dermatologist, Nij Smellinghe Hospital, Department of Dermatology, Phlebology and Lymphology, Drachten, The Netherlands
Sandy Ellis Nurse Consultant, Lymphoedema, St George’s Hospital, London, UK
Ethel Földi Physician-in-Chief of the Földi Clinic, Special Clinic for Lymphology in Hinterzarten, Germany
Mei Fu Assistant Professor, College of Nursing , New York University, New York, USA
Alan Irvine Consultant Paediatric Dermatologist, Our Lady’s Children’s Hospital, Dublin, Ireland
Karin Johansson Registered Physiotherapist, Lymphoedema Unit, RTA, Lund University Hospital, Lund, Sweden
Vaughan Keeley Consultant in Palliative Medicine, Derby Hospitals NHS Foundation Trust, Nightingale Macmillan Unit, Derby, UK
Eilish Lund Lead Lymphoedema Nurse, Nightingale House Hospice, Wrexham, Wales
John MacDonald FACS President, Association for the Advancement of Wound Care, Fort Lauderdale, Florida, USA
Peter Mortimer Professor of Dermatological Medicine, Cardiac and Vascular Sciences (Dermatology Unit), St George’s Hospital, University of London, London, UK
Saravu Narahari Director, Institute of Applied Dermatology, Kasaragod, Kerala, India
Editorial boardLindsey Mathews Managing Editor
Adam Bushby Sub-Editor
Business staffRob YatesPublishing Director [email protected]
Paul JonesBusiness Manager [email protected]
Editorial staff
All rights reserved. No part of this publication may be reproduced, stored, or transmitted in any form or by any means without the prior written permission of the Journal of Lymphoedema. Opinions expressed in articles are those of the authors and do not necessarily reflect those of the Journal of Lymphoedema or the editorial/advisory board. Advertisements have no influence on editorial content or presentation.
Journal detailsJournal of Lymphoedema is a copyright of Wounds UK, A Schofield Healthcare Media company, 1.03 Enterprise House, 1–2 Hatfields, London, SE1 9PGTel: 020 7627 1510 [email protected]
SubscriptionsTel: 020 7627 1510 or www.lymphormation.orgPersonal annual in the UK £40.00 International annual £60.00 Institutional subscription £80.00
For change of address, mail or email your old and new address to Journal of Lymphoedema Tel: 020 7627 1510 or [email protected]
Printed in Great Britain by Pensord, Pontllanfraith, Blackwood, NP12 2YA
ISSN 1750-7235
LymphoedemaJournal of
Moriya Ohkuma Department of Dermatology, Sakai Hospital, Kinki University, School of Medicine, Sakai shi, Osaka, Japan
Hugo Partsch Professor of Dermatology, Emeritus, Medical University of Vienna, AustriaRebecca Penzer Community Dermatology Specialist Nurse and Clinical Lead for Community Dermatology, Norfolk Community Health and Care, UKCheryl Pike Clinical Lymphoedema Physiotherapist Specialist, South-west WalesPatricia Price Professor of Health Sciences, Wound Healing Research Unit, Cardiff University, Cardiff, WalesStanley Rockson Director, Stanford Center for Lymphatic and Venous Disorders, Stanford University School of Medicine, Stanford, CaliforniaTerence Ryan Emeritus Professor of Dermatology, Green College, Oxford; Adviser on Morbidity Control to Global Alliance for the Elimination of Lymphatic Filariasis, Oxford, UKSaskiat Thiadens Founder and Executive Director, National Lymphedema Network Inc,, Oakland, California, USAJacquelyne Todd Physiotherapist Consultant in Lymphoedema, Leeds Lymphoedema Service, Cookridge Hospital, Leeds, UKAnna Towers Associate Professor, Department of Oncology, McGill University, Montreal, CanadaWinifred Schneider Head Doctor, Baumrainklinik Haus am Schlosspark, Bad Berleburg , GermanyMargaret Sneddon Macmillan Senior University Teacher, Director for Chronic Oedema Education, University of Glasgow, Glasgow, ScotlandAnita Wallace Chair, Lymphoedema Support Network, London, UKJustine Whitaker Director and Nurse Consultant, Northern Lymphology Ltd and Senior Lecturer, University of Central Lancashire, UKRichard White Professor of Tissue Viability, Institute of Health, Social Care and Psychology, University of Worcester, UKJane Wigg Clinical Nurse Manager, Wolverhampton Lymphoedema Service, Wolverhampton, UKMary Woods Head of Lymphoedema, Department of Rehabilitation, Royal Marsden NHS Trust Hospital, London, UKFran Worboys Clinical Nurse Specialist in Tissue Viability, Tower Hamlets Primary Care Trust, East London, UK
4� Journal�of�Lymphoedema,�2013,�Vol�8,�No�2
Christine Moffatt, EditorHonorary Professor, Nursing and Healthcare, University of Glasgow, Glasgow, UK; Director, International Lymphoedema Framework
Neil Piller, Clinical EditorProfessor and Director, Lymphoedema Assessment Clinic, Flinders Medical Centre, South Australia, Australia

Editorial
Journal of Lymphoedema, 2013, Vol 8, No 2 5
Neil Piller
Lymphoedema and the impact of social and societal factors – can we do better?
Both secondary and primary lymphoedema continue to be a problem worldwide. Surprisingly, it’s
not only developing countries where remains an issue. But have we really performed much better over the past 20 years in managing this condition?
In developed countries, improvements have been made in the detection of cancers. Earlier detection means conservative interventions, less interference with the lymphatic vessels, and fewer nodes removed. 3D radiotherapy means a specific area can be targeted and surrounding tissues protected, not because they are shielded, but because the dose can be focused in three dimensions at a point even in the deep subfascial tissues.
Many surgical groups now combine cancer treatment surgery with reconstructive surgery – minimising tissue trauma and reducing the risk of unnecessary lymphatic damage and soft-tissue scarring, which is a major impediment to lymphatic vessel regrowth. Lymphatic imaging techniques have also improved with the introduction of indo-cyanine green to accurately show where the lymphatic collectors are and how they are working, so treatment can be better focussed on these patterns. We also have tools such as bioimpedance spectroscopy and tissue dielectric constants, which can detect small differences in tissue fluids in local and general areas (at a range of depths in the case of the latter). Unfortunately, for both of these treatment methods – despite what many believe is good science and strong evidence – these early detection techniques are used by only a few clinicians and therapists, and even then only in major centres. Surely is easier to manage fluids, rather than wait until there is the accumulation of fat in the superficial facial
health inequalities, arise because of the circumstances in which people grow, live, work and age, and the systems put in place to deal with illness. The conditions in which people live and die are in turn shaped by political, social and economic forces”.
In Australia, for instance, we have one of the better healthcare systems in the world, but for most people (with the exception of some in top-level private health) Medicare-paid access to adequate support for the basics of lymphoedema care – massage, garments, and bandaging – cannot be obtained; individuals pay for these themselves generally. Despite perceptions of best care up front, unless a patient has got the funds to support their own follow-up care, they won’t get it.
The key principles for all of us to recognise and fight for are those linking to our social determinants of health; risk factors in our living or working conditions. At a basic level, these include access to adequate nutrition, education, safe water, healthcare; and wellbeing associated in policy areas covering housing, employment, transport, education, and the environment. For instance, in terms of the latter, living in a hot climate, compliance can be an issue. For example, it’s not easy wearing a thick compression garment when its 35 degrees centigrade with 95% humidity.
Wherever in the world we are, there are strong social factors revolving around our level of employment, our financial status, and the level and type of health insurance. Just because one lives in a developed country does not necessarily mean better access to healthcare – even though the quality of healthcare may be orders of magnitude better than some developing countries. The society in which we live, our friends, family and colleagues also make a difference, our healthcare providers, our healthcare advice, and of course our compliance! Then we all have those practical issues: distance from healthcare providers, time taken to
Neil Piller is Director Lymphoedema Research Unit, Department of Surgery, School of Medicine, Flinders University, Adelaide, South Australia, Australia.
area and increasing induration of the fascia and above, and associated further lymphatic compromise?
For primary lymphoedema, we have the opportunity of genetic screening in developed nations, but costs are often beyond most of those at risk. This is unfortunate since we are more aware that many of the current secondary lymphoedemas may have an underlying genetic aberration. This leads to issues with the lymphatic system, ranging from an inability to pump hard, effectively, and with reasonable pressure, to less lymphatic capillaries and collectors, to disorganised collector paths and nodal hypoplasia.
Regardless of the country, it’s often economic and social conditions that influence individual and group differences in health status.
We all have a range of risk factors in our lives, including our living and working environments. These coincide with individual factors (such as behavioural risk factors – like not taking care of our skin or not heeding advice about weight and diet management or genetics), which influence the risk of contracting a disease or disorder, or vulnerability to that disease or disorder. Broadly, these are classified as the social determinants of health.
There is strong evidence that these risk factors in the environment are influenced by public policies that reflect the influence of prevailing political ideologies and policies of those in governance. The World Health Organization (WHO) states: “This unequal distribution of health-damaging experiences is not in any sense a natural phenomenon, but is the result of a toxic combination of poor social policies, unfair economic arrangements (where the already well-off and healthy become even richer and the poor who are already more likely to be ill become even poorer), and bad politics.”
The organisation goes on to state, “[...] these inequities in health, avoidable

Editorial
6 Journal of Lymphoedema, 2013, Vol 8, No 2
to change political, social, and economic determinants of health, and thus of a chronic condition, such as lymphoedema.
Five per cent of women who undergo conservative sentinel lymph node removal and almost 20% who undergo axillary clearance develop lymphoedema in the USA (www.lymphnet.org). There is wide-ranging incidence of leg and genital lymphoedema (10%–60%) following groin clearances associated with bowel or reproductive system cancer treatment. It is also becoming clear that lymphoedema is more prevalent than the commonly quoted figure of 1.3 per 100 (indicated by the prevalence of the Stemmer sign; Pannier et al, 2007) and this is tied to the fact there are many more primary forms of lymphoedema than perhaps we would like to acknowledge (Brice and Connell, 2008). Add in the fact that many more are at risk of lymphoedema across the developing world and it begs the question – where is our voice?
ReferencesBrice G, Connell F (2008) Lymphoedema: primary or
secondary, how does one tell? Journal of Lymphoedema 3(2): 8–9
Pannier F, Hoffman B, Stang A et al (2007) Prevalence of Stemmer’s sign in the general population. Phlebologie 36: 289–92
Maybe we need to realise that “lymphoedema”, while a word describing lymphatic insufficiency, is not the right word to describe this chronic condition. Perhaps we have to link lymphoedema more with the term “chronic oedema”. Very few die of lymphoedema, but those with the condition suffer immeasurably, with an enlarged limb, often deplorable quality of life, and sometimes with no one to turn to.
There are few other diseases/disorders in the developing and developed world that are so poorly acknowledged, managed, and supported by governments and health systems, despite (in the case of lymphoedema) a significant long-term loss of that person’s productivity, as well as poor social acceptance.
We have an obligation to pool resources – both domestically and internationally – to: address the cost of lymphoedema care and support; improve access to, and funding of, garments; facilitate the education of clinicians and the public (particularly those at risk); and determine the best pathway to diagnosis, treatment and services.
It all starts with the pressure we can all put on governments and health systems
undertake treatment, time needed off work, and treatment fatigue to name but a few.
No matter where we live there can be poor health outcomes; not just those living in developing countries, but those at the lower end of the socioeconomic scale. Poor outcomes can occur for marginalised groups anywhere, and these can be linked to social exclusion, stress, limited education, and limited or no access to support.
So what do we need to do? We have good templates for practice, best practice statements and consensus documents, but these can be ineffective, if our social and societal factors don’t allow access to their recommendations.
Groups like the International Lymphoedema Framework, the International Society for Lymphology, the European Society of Lymphology, and others need to work in concert with larger, politically strong groups, such as the WHO and the United Nations Development Programme, and the World Union of Wound Healing Societies, and think about how groups associated with wound care around the world have made significant improvements in patient outcomes for acute and chronic wounds, and how we might do the same for lymphoedema.

SAVE THE DATE!INTERNATIONAL LYMPHOEDEMA FRAMEWORK 2014 CONFERENCE
Day Conference, University of Glasgow, 5-7th JuneOnline Conference, 29th May - 4th June
The full conference experience opens with a week-long online programme (29th May - 4th June) and follows with the main three-day event set in the beautiful historic buildings of the University of Glasgow, Scotland (5th - 7th June). The online conference is free to attend and both events are packed with presentations showcasing the latest research and ideas on lymphoedema.
2014 will be a notable year for Glasgow, Scotland – not only hosting sportsmen and women from around the world for the Commonwealth Games, but also having the honour and excitement of hosting the International Lymphoedema Framework (ILF) conference.
This conference will present exciting new developments in determining the prevalence of lymphoedema. It will focus on how the latest research offers the potential to reduce the incidence, prevalence and impact of lymphoedema on peoples’ lives. It will bring together international speakers from the fields of clinical practice, research and policy including Prof. Neil Piller from Australia, Prof. Christine Moffatt from the United Kingdom and Prof. Sugama from Japan. With over 100 presentations, seminars and workshops, the programme will be of interest to a wide range of delegates. There is special encouragement and support to those from developing economy countries, and for researchers new to the field of lymphoedema, to come and share their work, with awards being presented for best abstract and best poster. In addition, this year there are new awards for achievements in the course of your work and for those who inspire you; see the following website for details: www.ilfconference.org
One of the special tracks will be on eHealth – exploring how digital technology and social media can provide new opportunities in the field of lymphoedema. Presentations and workshops will examine approaches to improving care, sharing research and building learning communities, investigating new ways of delivering care, of learning and of working with patients for maximum impact. Another is dealing with complex lymphoedema. In addition, on 6th June, there will be an integrated Patients Day where some of the latest strategies for enabling self-management will be demonstrated and discussed.
Complementing the educational elements of the programme, there will be opportunities to build up your network of friends and colleagues. On the evening of 5thJune, the Lord Provost will host a Civic Reception in the stunning Glasgow City Chambers (City Hall). On 6th June, a Conference Dinner will be held at the Thistle Hotel, Glasgow where you can experience the fun of an informal Ceilidh (Scottish music and dance), some mini Scottish Highland Games and the presentation of the awards.
What next? The full programme will be available on the website when all the submitted abstracts have been reviewed and speakers confirmed. In the meantime, if you wish to submit an abstract for an oral or poster presentation or receive all the latest news of the conference programme and social events, please register your interest online at www.ilfconference.org. We look forward to seeing you in Glasgow giving you a great Scottish welcome!
Margaret Sneddon, Chair of Organising Committee

Research and audit
8� Journal�of�Lymphoedema,�2013,�Vol�8,�No�2
Amanda Purcell
Head and neck lymphoedema management practices
Head� and� neck� lymphoedema�(HNL)� can� be� classified� as�primary� or� secondary.� Primary�
HNL�is�caused�by�congenital�impairment�of�the�lymphatic�system�and�is�rare.�Secondary�HNL� commonly� develops� as� a� result� of�acquired� damage� to� the� lymphatic� system�during�treatment�for�head�and�neck�cancer�or� blockage� by� the� cancer� itself� (Thoma,�2012).�
Surgery� and� radiotherapy� are� the� two�primary� modalities� used� to� treat� head�and� neck� cancer� and� both� can� precipitate�the� development� of� HNL.� HNL� is� most�common� following� head� and� neck� cancer�surgery,� but� is� most� severe� after� treatment�with� combined� surgery� and� radiotherapy�(Micke�et�al,�2003;�Lewin�et�al,�2010).��
The� prevalence� of� HNL� is� difficult� to�quantify,�but�in�comparison�to�other�types�of�lymphoedema,�it�is�less�common�(Smith�and� Lewin,� 2010).� Reported� HNL� rates�range�from�12.1%�(Chen�et�al,�2010)�to�48%�(Büntzel�et�al,�2007),�to�75.3%�(Deng�et�al,�2012)�of�samples�of�head�and�neck�cancer�patients.�Such�variation�arises�from�the�use�
AssessmentThere� is� no� gold� standard� test� available� to�diagnose�HNL�(Deng�et�al,�2011),�but�a�wide�range�of�assessment�tools�are�used�to�measure�and�monitor�the�condition.�The�complexities�of�the�head�and�neck�region�make�assessment�challenging.� Depending� on� the� assessment�used� and� the� area� examined,� evaluation� of�lymphoedema�can�vary�substantially.
Assessment of internal lymphoedemaInternal�oedema�cannot�be�physically�palpated�and� is� invisible� without� instrumentation�(Deng�et�al,�2012),�such�as�videofluoroscopy�or�endoscopy.�Internal�HNL�can��be�described�in�terms�of�the�degree�of�oedema�present�using�the�Patterson�Scale�(Patterson�et�al,�2007).
Internal� HNL� can� affect� swallowing� with�reports� of� up� to� 30%� of� people� with� HNL�having� associated� swallowing� dysfunction�(Lewin� et� al,� 2010).� Internal� HNL� can�occur� in� combination� or� in� isolation�from� external� HNL,� as� reported� by� Deng��et� al� (2012)� in� a� sample� of� head� and� neck�cancer� patients� (n=81)� where� 39.4%� had�internal� lymphoedema� alone;� 9.8%� had�
Abstract
Lymphoedema management of the head and neck is a valuable, yet under-recognised, area of practice. The author has embarked on a recent study trip to examine head and neck lymphoedema practices in the UK and USA, in comparison to those in Australia. Visits were conducted to established, hospital-based lymphoedema clinics in six major UK centres and two major US centres. A high degree of variability was observed in head and neck lymphoedema management practices. This article aims to document various assessment and treatment approaches for head and neck lymphoedema to improve awareness of the condition, to highlight the need for routine assessment, and outline the treatment modalities available.
Key words
Assessment, head and neck, lymphoedema, treatment
Amanda Purcell, Team Leader Consultant, Occupational Therapy, Princess Alexandra Hospital, Brisbane, Queensland, Australia
Declaration of interest: The author received financial support from the Churchill Trust to fund clinic visits and travel.
of� different� definitions� of� lymphoedema,�variations�in�the�assessments�used,�and�also�due� to� the� changing� presentation� of� head�and�neck�cancer.�
Historically,� head� and� neck� cancer� was:�mediated�by�prolonged�exposure�to�alcohol�and� tobacco;� presented� at� an� older� age�(60–80);� and,� had� a� relatively� low� cure�rate� (National� Cancer� Institute,� 2013).�There�is�an�increasing�trend�towards�virally�mediated�head�and�neck�cancer�associated�with� the� human� papilloma� virus� (HPV;�Chaturvedi� et� al,� 2011).� HPV-positive�cancer� commonly� presents� at� a� younger�age� (40–60� years)� and� is� associated� with�relatively�higher�cure�rates,�compared�with�HPV-negative� types� (National� Cancer�Institute,�2013).�
With� the� increase� in� HPV-positive�head� and� neck� cancer,� patients� may�present� with� HNL� at� a� younger� age� and�survive� longer� than� they�would�have�done�previously.� Individuals� who� develop� HNL�may� experience� a� greater� impact� from� the�morbidity� of� the� condition� and� may� be�more�active�in�seeking�treatment.

JOBST® Bella™ Lite Comfortable and effective
Regular length armsleeve
Available NOW on FP10 / GP10
n Two compression classes
n Three sizes and two lengths
n Soft, fine-knit construction
Ready-to-wear, circular-knit, upper limb compression garments
To place an order or for further information, please contact Customer Services on 0845 122 3600
or email [email protected].
BSN medical Limited. • PO Box 258 • Willerby • Hull • HU10 6WT Tel: 01482 670100 • Fax: 01482 670111 • www.bsnmedical.co.uk® Registered trade mark © BSN medical Limited, October 2013 0115/1013

Research and audit
10� Journal�of�Lymphoedema,�2013,�Vol�8,�No�2
external� lymphoedema� alone;� and� 50.8%�had� combined� internal� and� external�lymphoedema.� The� use� of� informal�swallowing� assessment/screening� can� be�employed� to� determine� an� association�with�HNL.�Questions�asked�include:�•� Is�the�swelling�worse�in�the�morning?•� Does�it�change�throughout�the�day?•� Is� your� swallowing� worse/better�
when�your�swelling�is�worse/better?
Observations of current practiceInternal� lymphoedema� assessment� is�not� routine� in� most� practices.� Due� to�the� additional� equipment� and� expertise�required,� internal� assessment� is� more�common�as�a�research�tool.
Assessment of external HNLExternal� HNL� describes� visible� swelling�in� the� soft� tissues� of� the� head� or� neck�(Deng� et� al,� 2012).� The� most� common�locations� for� external� HNL� are� the� neck�or� submental� region� (Lewin� et� al,� 2010;�Deng� et� al,� 2012).� External� HNL� can� be�measured� using� objective� or� subjective�assessments.�
•� Surface� tape� measurements� between�facial�landmarks�can�be�used�to�evaluate�HNL.� Although� tape� measurements�do� not� represent� a� volumetric�measurement,� they� can� be� used� to�monitor� progress� over� time.� Some�measurement�systems�only�evaluate�the�face�(Schultze-Mosgau�et�al,�1995;�Piso�et�al,�2001),�however,�a�combined�facial�and�neck�assessment�may�be�preferable�for�HNL�(Smith�and�Lewin,�2010).�
•� Digital�photography�is�a�simple�way�to�record� changes� in� HNL.� � Consistent�distance,� focus,� and� location� should�be� used� to� allow� photographs� to� be�compared� accurately� over� time� (e.g.�via�use�of�wall�markings�or�a�string�line�between�subject�and�camera).�
Other� more� sophisticated� assessments� of�HNL� have� been� reported� in� the� literature,�such� as� handheld� scanning� laser� (Harrison�et� al,� 2004),� 3D� optical� scanning� (Rana��et�al,�2011),�ultrasound�measurement�(Piso�et� al,� 2001).� However,� these� methods� were�not� observed� in� most� clinical� practices.�This� may� reflect� the� additional� challenges�
Objective assessmentThe�objective�assessment�of�HNL�has�proved�challenging� for� a� number� of� reasons:� the�head�and�neck�region�is�not�a�uniform�shape;�it� surrounds� many� different� anatomical�structures;�and�it�has�no�contralateral�area�for�comparison.�Assessments�include:•� Palpation� is� used� to� feel� pitting/
thickening/fibrosis�of�the�epidermis�and�dermis� externally� and� in� the� intraoral�compartment.� This� is� an� essential�assessment�in�HNL�(Thoma,�2012).
•� Visual� inspection� is� used� to� describe�changes� in� the� architecture� of� the� skin�and� tissues;� location� of� oedema;� skin�condition;�oral�mucosa�and�airways.
•� Rating�scales�are�used�to�systematise�the�descriptions� obtained� from� palpation�and�visual�inspection.�Rating�scales�may�combine� qualitative� and� quantitative�observations.� Examples� include:�International� Society� of� Lymphology�rating� scale� (International� Society� of�Lymphology,� 2013;� Table 1);� MD�Anderson�HNL�rating�scale�(Smith�and�Lewin,�2010;�Table 2);�Common�toxicity�criteria�(Cheville�et�al,�2003;�Table 3).
Grade Description
0 Swelling�is�not�yet�evident�despite�impaired�lymph�transport.�Subjective�symptoms�and�subtle�tissue/fluid�changes�may�be�present.1 Early�swelling�reduces�with�limb�elevation;�pitting�may�be�present.2 Hard�swelling�that�does�not�respond�to�elevation;�pitting�is�present�until�late�stages�when�excess�fat�and�fibrosis�may�be�present.3 Lymphostatic�elephantiasis;�pitting�may�be�absent;�trophic�skin�changes�present.
Table�1.�International�Society�of�Lymphology�(2013)�rating�scale.
Grade Description
0 No�visible�oedema,�but�patient�reports�“heaviness”.1a Soft�visible�oedema;�no�pitting,�reversible.1b Soft�pitting�oedema;�reversible.2 Firm�pitting�oedema�(longer-lasting�pitting);�not�reversible;�no�tissue�changes.
3 Irreversible;�tissue�changes�(not�commonly�seen�in�head�and�neck�lymphoedema).
Table�2.�MD�Anderson�head�and�neck�lymphoedema�rating�scale�(Smith�and�Lewin,�2010).
Grade Description
1 Localised�to�dependent�areas�and�no�disability�or�functional�impairment.2 Localised�facial�or�neck�oedema�with�functional�impairment.3 Generalised�facial�or�neck�oedema�with�functional�impairment�(e.g.,�difficulty�in�turning�neck�or�opening�mouth�compared�to�baseline).4 Severe�with�ulceration�or�cerebral�oedema;�tracheotomy�or�feeding�tube�indicated.
Table�3.�Common�toxicity�criteria�v3.0�(Cheville�et�al,�2003).

Available on
Prescription
A simple and effective alternative to bandaging and stockings*
[email protected] 01844 208842 www.hadhealth.com* Lawrence S. "Use of a Velcro® wrap system in the management of lower limb lymphoedema/chronic oedema." J Lymphoedema 2008:3(2). P 65-70.

Research and audit
12� Journal�of�Lymphoedema,�2013,�Vol�8,�No�2
associated�with� these�assessments,� in� terms�of� the� expense� involved� in� accessing� the�relevant�equipment.�
Observations of current practicePalpation� and� visual� inspection� were� the�most� consistently� observed� assessments�followed� by� the� use� of� HNL� rating� scales.�Objective� assessment� commonly� occurs� at�initial�assessment�and�discharge;�evaluation�at� other� treatment� points� is� less� consistent.�Clinics� without� a� specific� focus� on� HNL�use� more� generalised� assessments� –� such�as� observation� –� whereas� clinics� focusing�on� HNL� use� tape� measurements� or�standardised�photography.
Subjective assessmentDiscrepancies� between� objective� and�subjective� evaluation� of� HNL� may� occur.�A� bidirectional� relationship� is� possible�where�a�condition�rated�as�moderate�using�objective� measures� may� be� subjectively�perceived� as� either� severe� or� mild.� For�example,� Deng� et� al� (2012)� conducted� a�study� with� 30� participants,� all� of� whom�were� objectively� assessed� as� having�HNL.� When� self� rating� their� symptoms,�only� 13.3%� of� participants� reported� the�presence� of� swelling� in� the� head� and� only�16.7%� reported� the� presence� of� swelling�in�the�face.�This�discrepancy�highlights�the�importance�of�recording�both�objective�and�subjective� data.� Subjective� assessment� of�HNL� and� its� associated� symptoms� can� be�made�using�the�following�tools:•� The� Distress� Thermometer� (0–100;�
National� Comprehensive� Cancer�Network,� 2013)� or� Visual� Analogue�Scale�(0–10;�Torrance�et�al,�2001)�can�be� adapted� for� use� in� measuring� the�level�of�distress�caused�by�HNL.
•� Symptom� burden� indexes� record�the� presence� of� a� range� of� symptoms�common� after� head� and� neck� cancer�treatment� (e.g.� change� in� swallowing,�talking,� taste,� and� the� presence� of�swelling).� High� levels� of� symptom�burden� have� been� reported� in� HNL�patients�in�terms�of�frequency,�severity,�and� distress� (Deng� et� al,� 2012).�Symptom� indexes� are� designed� to�record� the� number� and/or� intensity�of� symptoms� present� and� can� be�used� to� monitor� progress.� Examples�include:�the�MD�Anderson�Symptom�Inventory� (Rosenthal� et� al,� 2007;�2008);� the� Lymphedema� Symptom�
reportedly�difficult�to�achieve�(Mihara,�et�al,�2011)�and�should�only�be�applied�with� low� pressure� (International�Lymphoedema� Framework,� 2012)�to� avoid� constriction� and� potential�increase� in� facial� oedema� (Smith�and� Lewin,� 2010).� Compression�bandaging�with�short�stretch�bandages�can� be� applied� under� the� chin� and�around� the� head,� secured� with� a�Velcro®� (Velcro� Limited)� attachment�(Klose� and� Strößbenreuther,� 2006)�or� cohesive� bandages� can� be� used� to�avoid� the� need� for� fixation� (Gilbert��et�al,�2011).�Bandages�are�generally�low�in�cost,�use�materials�available�to�most�lymphoedema� clinics,� are� relatively�easily�assembled,�and�can�be�adjustable�to� respond� to� changes� in� oedema.�However,� they� can� be� cumbersome�to�apply�and�do�not�provide�coverage�of� all� areas� of� the� head� and� neck.�Compression� garments� are� an�alternative� to� compression� bandages.Custom� face� masks� are� required� to�cover� extensive� areas� of� swelling� –� to�support�irregular�anatomy�–�or�for�use�with� extensive� oedema� (particularly�anterior�cheek�swelling).�Off-the-shelf�compression� can� be� better� suited� to�oedema� confined� to� the� neck� region.�A� variety� of� inserts� can� be� used�underneath� or� within� bandaging� and�garments:�open�cell�foam�in�a�flat�sheet�can�be�used�to�create�bulk�and�increase�the� stiffness� of� the� compression� on�tissues;�closed�cell�foam�in�small�pieces�between� tape� can� be� used� to� “break�up”�areas�of�thickening.�
•� Exercise/movement� aims� to� increase�the� individual's� range� of� motion� and�reduce�the�effects�of�fibrosis� � through�the�use�of�pure�range�of�motion�exercises�for� the� face,� neck� and� shoulders,� and�composite� range� of� motion� exercises�(e.g.� neck� extension� and� lateral�flexion;� Forster,� 2006;� Stubblefield,�2011).� Exercise/movement� can�compensate�for�a�reduction�in�natural�muscle� movements� occurring� as� a�result� of� eating� softer� foods,� altered�speech� patterns,� and� reduced� activity.�If�natural�movement�has�not�returned,�prescribed�exercises�may�assist� lymph�drainage,� particularly� if� performed� in�conjunction�with�compression.�
•� MLD� has� been� reported� as� the�primary� treatment�modality� for�HNL�
Intensity� and� Distress� Survey� –� Head�and�Neck�(Deng�et�al,�2012).
•� Quality� of� life� assessments� have� been�developed� for� use� following� head�and� neck� cancer� treatment,� rather�than� specifically� for� HNL.� They�commonly� include� measurement� of�communication,� speech,� appearance,�swallowing,� eating,� and� oral�symptoms.� No� quality� of� life� scales�currently� available� contain� specific�reference� to� lymphoedema,� however,�related� scales� include:� Quality� of� Life�Instrument�for�Head�and�Neck�Cancer�(Morton� and� Witterick,� 1995);�Functional� Assessment� of� Cancer�Therapy�(Cella�et�al,�1993);�University�of� Michigan� Head� and� Neck� Quality�of� Life� Questionnaire� (Terrell��et� al,� 1997);� Head� and� Neck� Cancer�Inventory� (Funk� et� al,� 2003);� the�European� Organization� for� Research�and� Treatment� of� Cancer� Quality� of�Life� Questionnaire� –� Head� and� Neck�35�(Bjordal�et�al,�1994);�University�of�Washington� Quality� of� Life� Revised�(Rogers�et�al,�2002).
Observations of current practiceSubjective� assessment� was� less� common�than� objective� assessment� in� the� clinical�practices� observed.� The� Distress�Thermometer� and� Visual� Analogue� Scale�were�the�only�tools�observed�in�clinical�use.�Quality�of�life�tools�were�not�used�clinically�and�may�be�more�relevant�as�research�tools.
TreatmentHNL�is�a�complex�condition�with�a�variable�presentation� and� thus� a� multimodal�treatment� approach� may� be� required� to�achieve� successful� outcomes.� The� use� of� a�wide� variety� of� treatment� modalities� was�observed�in�the�clinics�visited.�Intensity�and�duration� of� modality� application� was� also�highly�variable�with�some�advocating�only�therapist-directed� treatment� and� others�recommending�primarily�patient-�or�carer-delivered�treatment.
Treatment modalitiesManual� lymphatic� drainage� (MLD)� and�light�compression�are�reported�as�being�the�core� HNL� treatment� modalities� (Mihara�et� al,� 2011;� International� Lymphoedema�Framework,�2012).�However,�a�wide�variety�of�techniques�are�employed�in�practice:•� Compression�of� the�head�and�neck� is�

Do you need to demonstrate that a wound care intervention offers value for money?
A new international consensus can help
Understand what is meant by ‘cost-effective wound management’Appreciate the different
types of economic analysis used in healthcareInterpret information
on cost and cost-effective-ness of wound care modalities and protocols Set up systems to collect
the data for analysisMake an appropriate case
for cost-effective wound management
Free to download from www.woundsinternational.comSoon to be available in French, German, Italian and Spanish
Untitled-2 1 16/12/2013 13:03

Research and audit
14� Journal�of�Lymphoedema,�2013,�Vol�8,�No�2
management� (Lee� et� al,� 2013)� with�positive� clinical� benefits� reported�(Piso� et� al,� 2001;� Smith� and� Lewin,�2010),� however,� strong� evidence�is� lacking.� Contraindications� for�head� and� neck� MLD� may� include�hyperthyroidism,� hypersensitive�carotid� sinus,� cardiac� arrhythmia,�and� arteriosclerosis� in� the� carotid�artery� (Strößbenreuther,� 2012).�MLD� pathways� follow� the� expected�anatomical� pathway� of� the� lymph�vessels� (Thoma,� 2012).� However,�recent� anatomical� findings� have�shown� that� the� superficial� lymphatic�drainage� of� the� head� and� neck� is�“virtually� unpredictable”� (Pan� et� al,�2008).� Different� lymphatic� network�patterns�have�been�observed�between�subjects� and� even� between� different�facial� sides� of� the� same� subject� (Pan�et�al,�2008)�with�vessels�from�one�area�of� tissue� draining� to� different� lymph�node�groups�(Pan�et�al,�2011)�crossing�the�midline�and�crossing�scars�(Maus��et� al,� 2012).� These� findings� may�indicate�a�need�for�more�individualised�MLD�pathways�in�future.�
•� The� implementation� of� a� skin� care�regimen�is�recommended�to�maintain�skin� integrity� and� prevent� infection�(Lee�et�al,�2013).�Cellulitis�is�a�known�complication� of� lymphoedema� and,�while�rates�in�the�head�and�neck�region�appear�lower�than�in�the�limbs,�limited�data� are� available.� In� one� of� the� few�HNL� treatment� studies� published�(n=18),� Piso� et� al� (2001)� reported� a�17%�infection�rate.�
•� Elastic� taping� (e.g.� Kinesio®� tape)� can�be� used� to� assist� removal� of� oedema�from� congested� areas� by� opening�initial�lymphatics�and�lifting�superficial�skin� to� decrease� pressure� (Kase� and�Stockheimer,�2006).�In�the�absence�of�coronary�artery�disease�or�bruits�in�the�carotid�arteries,�taping�of�the�neck�can�be�employed�(Kase�and�Stockheimer,�2006;� Coopee,� 2011).� However,� if�symptoms� are� present,� taping� in� the�neck� should� be� avoided� (Coopee,�2011).
•� Scar/fibrosis� management:�techniques� such� as� elastomer� putty�used� under� compression� (Klose� and�Strößbenreuther,�2006),�or�myofascial�release,� are� used� to� reduce� scarring�and�fibrosis�of� the�neck,�and� improve�
lymphoedema� to� balance� clinical�outcomes� with� health� insurance�limitations,� staffing� restrictions,� and�patient� travel� distances.� Training,�provision� of� pictorial� guides� and�instructions,� and� follow-up� therapist�review� are� all� required� to� support�this� approach� (Rockson� and� Vaillant-Newman,� 2011).� Advantages� include�reduced� therapy� resource� use� and�patient� convenience,� however,� self-management� techniques� may� not�be� as� effective� as� therapist-directed�treatment� (Rockson� and� Vaillant-Newman,�2011).�
•� An� alternative� approach� is� to�commence� a� self� management�programme� for� a� quarantined� period,�followed� by� therapist-directed�treatment� if� self� management�outcomes�have�been�unsatisfactory.�
DiscussionThe� author� observed� the� delivery� of� a�wide�range�of� treatments� for�HNL.�There�are� several� possible� explanations� for� this�variability.�Different�stages�of�HNL�may�be�best� suited� to� different� treatments.� Deng��et�al�(2012)�found�that�of�those�with�HNL,�some�“had�pure�lymphoedema,�some�had�a� mixture� of� lymphoedema� and� fibrosis,�and� others� had� only� fibrosis”.� Due� to� the�frequent� occurrence� of� fibrotic� tissue�following� treatment� for� head� and� neck�cancer,� a� combination� of� fibrotic� tissue�reduction� techniques� and� lymphoedema�techniques� are� required� for� clinical�effectiveness�(Klose�and�Strößbenreuther,�2006).
Further� variability� in� treatment�modalities� may� be� reflective� of� the�clinicians’� professional� background� and�prior� experience.� HNL� treatment� is�primarily�provided�by�nurses,�occupational�therapists,� physiotherapists,� and� speech�pathologists.� Each� profession� has� its� own�inherent� skill� set� that� may� predispose� a�clinician�to�a�preference�for�certain�types�of�treatment.� For� example,� physiotherapists�were� observed� commonly� performing�myofacial� release,� whereas� speech�pathologists� focused� on� the� interaction�between�lymphoedema�and�swallowing.
Perhaps�the�most�likely�explanation�for�treatment�variation�is�the�limited�research�currently� available� into� HNL� treatment.�There�is� little�evidence�to�guide�clinicians�in� choosing� the� most� effective� treatment�
associated� movement,� as� well� as�lymphatic�drainage.�
•� Gentle� inclination� of� the� head� and�upper� body� when� sleeping� can�assist� drainage.� The� neck� is� held� in� a�neutral�position�with�caution�to�avoid�excessive� neck� flexion.� This� position�can� be� achieved� by� using� a� foam�wedge,�elevation�of�the�head�of�the�bed�or�the�use�of�pillows.��
•� Deep� breathing� is� used� for� the�management� of� other� types� of�lymphoedema� and� is� inconsistently�employed�with�HNL.�Further�research�into� the� mechanism� of� action� is�required�to�facilitate�evaluation�of�this�technique.
Other�treatments�have�been�reported�in�the�literature,�but�were�not�observed�in�clinical�practice� at� the� sites� visited� (i.e.� cooling�therapy� [Rana� et� al,� 2011],� low-level� light�therapy�[Lee�et�al,�2013],�and�surgery�with�lymphaticovenous� anastomosis� [Mihara��et�al,�2011]).
Observations of current practiceMultiple� treatment� modalities� are�available�for�HNL,�however,�each�therapist�demonstrated�a�preferential�use�of�only�one�or� two� key� modalities.� The� key� modalities�chosen� varied� between� clinics� however�MLD�and�compression�(with�inserts)�were�the� most� commonly� utilised.� While� the�effectiveness� of� each� technique� appeared�to� differ� between� patients,� the� most�consistently� positive� results� observed� by�the� author� occured� with� the� use� of� gentle�compression�and�inserts.
Treatment intensityPerhaps� the� greatest� variation� in� practice�occurred� in� the� design� of� HNL� treatment�programme�intensity.�The�models�observed�fell�into�three�broad�categories.�These�were:•� Therapist-directed�treatment�followed�
by�self�care:�using�a�therapist-directed�approach� (Piso� et� al,� 2001),� the�therapist� delivers� treatments� directly�to�the�patient,�requiring�multiple�clinic�visits�with�the�patient�performing�self�management�on�the� intervening�days.�This�approach�is�commonly�preferred�for�moderate–severe�HNL�due�to�the�improved�outcomes�observed.
•� Self� care� only� (Smith� and� Lewin,�2010;� Jeffs� et� al,� 2011)� is� used� for�patients� with� mild� to� moderate�

Research and audit
Journal�of�Lymphoedema,�2013,�Vol�8,�No�2� 15
for� HNL,� therefore� a� multifaceted�approach� is� regularly� employed.� With� no�gold� standard� assessment� available,� those�currently�being�used�are�inconsistent�and,�as�a�consequence,�treatment�outcomes�are�difficult� to� compare.� Many� assessments�are� not� suitable� for� use� in� the� clinical�environment,� which� limits� individual�assessment�of�the�outcomes�of�therapy.�The�future�development�of�clinically�accessible�assessments�for�HNL�is�essential.�
ReferencesBjordal� K,� Ahlner-Elmqvist� M,� Tollesson� E� et� al� (1994)�
Development� of� a� European� Organization� for� Research�and� Treatment� of� Cancer� (EORTC)� questionnaire�module�to�be�used�in�quality�of�life�assessments�in�head�and�neck�cancer�patients.�EORTC�Quality�of�Life�Study�Group.�Acta Oncol�33(8):�879–85
Büntzel� J,� Glatzel� M,� Mücke� R� et� al� (2007)� Influence� of�amifostine� on� late� radiation-toxicity� in� head� and� neck�cancer� –� a� follow-up� study.� Anticancer Res� 27(4A):�1953–6
Cella� DF,� Wiklund� I,� Shumaker� SA,� Aaronson� NK� (1993)�Integrating� health-related� quality� of� life� into� cross-national�clinical�trials.�Qual Life Res�2(6):�433–40
Chaturvedi� AK,� Engels� EA,� Pfeiffer� RM� et� al� (2011)Human�papillomavirus�and�rising�oropharyngeal�cancer�incidence� in� the� United� States.� J Clin Oncol� 29(32):�4294–301
Chen�M-H,�Chang�P,�Chen�P-M�et�al�(2010)�Prolonged�facial�edema�is�an�indicator�of�poor�prognosis�in�patients�with�head� and� neck� squamous� cell� carcinoma.� Support Care Cancer 18(10):�1313–9
Cheville� AL,� McGarvey� CL,� Petrek� JA� et� al� (2003)� The�grading�of�lymphedema�in�oncology�clinical�trials.�Semin Radiat Oncol 13(3):�214–25
Coopee�R�(2011)�Elastic�Taping�(Kinesio�Taping�Method).�In:�Skirven�TM,�Osterman�AL,�Fedorczyk�J,�Amadio�PC�(eds)� Rehabilitation of the Hand and Upper Extremity.�Elsevier�Mosby,�Philadelphia,�PA:�1529–38
Deng�J,�Ridner�SH,�Dietrich�MS�et�al�(2012)�Prevalence�of�secondary� lymphedema� in� patients� with� head� and� neck�cancer.�J Pain Symptom Manage�43(2):�244–52
Deng� J,� Ridner� SH,� Murphy� BA� (2011)� Lymphedema� in�patients� with� head� and� neck� cancer.� Oncol Nurs Forum 38(1):�E1–E10
Deng� J,� Ridner� SH,� Murphy� BA,� Dietrich� MS� (2012)�Preliminary� development� of� a� lymphedema� symptom�assessment�scale�for�patients�with�head�and�neck�cancer.�Support Care Cancer�20(8):�1911–8
Forster�R�(2006)�Considerations�for�functional�rehabilitation�in� head� and� neck� lymphedema.� In:� FÖldi� M,� FÖldi� E,�Strößbenreuther�RHK,�Kubik�S�(eds)�FÖldi’s Textbook of Lymphology.�Mosby�Elsevier,�Munich:�680–1
Funk� GF,� Karnell� LH,� Christensen� AJ� et� al� (2003)Comprehensive� head� and� neck� oncology� health� status�assessment.�Head Neck�25(7):�561–75
Gilbert� J,� Zanichelli� C,� Eaton� K� (2011)� Compression�appliances�in�head�and�neck�lymphoedema�management�–� An� innovation.� Paper� presented� at� the� British�Lymphology� Society� Conference,� Nottingham:��2�October
Harrison� JA,� Nixon� MA,� Fright� WR,� Snape� L� (2004)� Use�of� hand-held� laser� scanning� in� the� assessment� of� facial�swelling:� a� preliminary� study.� Br J Oral and Maxillofac Surg�42:�8-17
International� Lymphoedema� Framework� (2012)� Best�Practice� for� the� Management� of� Lymphoedema� (2nd�edn)� Compression� Therapy:� A� Position� Document�on� Compression� Bandaging.� Available� at:� http://bit.ly/19X7Rkc�(accessed�20.12.2013)�
International�Society�of�Lymphology�(2013)�The�diagnosis�
Strößbenreuther� RHK� (2012)� Treatment� of� the� cervical�lymph� nodes� and� their� tributary� regions.� In:� FÖldi� M,�FÖldi� E,� Strößbenreuther� RHK,� Kubik� S� (eds)� FÖldi’s Textbook of Lymphology.�Mosby�Elsevier,�Munich:�470–3
Stubblefield� MD� (2011)� Radiation� fibrosis� syndrome:�neuromuscular� and� musculoskeletal� complications� in�cancer�survivors.�PMR�3(11):�1041–54
Terrell� JE,� Nanavati� KA,� Esclamado� RM� et� al� (1997)�Head�and� neck� cancer-specific� quality� of� life:� instrument�validation.� Arch Otolaryngol Head Neck Surg� 123(10):�1125–32
Thoma�H�(2012)�Treatment�of�lymphedema�of�the�head.�In:��FÖldi�M,�FÖldi�E,�Strößbenreuther�RHK,�Kubik�S�(eds)�FÖldi’s Textbook of Lymphology.�Mosby�Elsevier,�Munich:�604–8
Torrance� GW,� Feeny� D,� Furlong� W� (2001)� Visual� analog�scales:�do�they�have�a�role�in�measurement�of�preference�for�health�states?�Med Decis Making�21(4):�329–34
VanSwearingen� JM,� Brach� JS� (1996)� The� Facial� Disability�Index:� reliability� and� validity� of� a� disability� assessment�instrument� for� disorders� of� the� facial� neuromuscular�system.�Phys Ther�76(12):�1288–98
and� treatment� of� peripheral� lymphedema.� 2013�consensus� document� of� the� International� Society� of�Lymphology.�Lymphology�46(1):�1–11
Jeffs�E,�Huit�M,�Thompson�S�(2011)�Management�of�Head�and�Neck�Lymphoedema:�Care�Pathway.�Paper�presented�at� the� British� Lymphology� Society� Conference,�Nottingham:�2�October
Kase� K,� Stockheimer� KR� (2006)� Kinesio Taping for Lymphoedema and Chronic Swelling.� Kinesio� Taping�Association,�Albuquerque,�NM
Klose� G,� Strößbenreuther� RHK� (2006)� Complete�Decongestive�Therapy�for�Secondary�Lymphedema�of�the�Head� and� Neck.� In:� FÖldi� M,� FÖldi� E,� Strößbenreuther�RHK,� Kubik� S� (eds)� FÖldi’s Textbook of Lymphology.�Mosby�Elsevier,�Munich:�667–79
Lee� N,� Wigg� J,� Caroll� J� (2013)� The� use� of� low� level� light�therapy�in�the�treatment�of�head�and�neck�lymphoedema.�Journal of Lymphoedema 8(1):�35–42
Lewin�JS,�Hutcheson�KA,�Barringer�DA,�Smith�BG�(2010)�Preliminary�experience�with�head�and�neck�lymphedema�and�swallowing�function�in�patients�treated�for�head�and�neck� cancer.� Perspectives on Swallowing and Swallowing Disorders (Dysphagia)�19(2):�45–52
List� MA,� Ritter-Sterr� C,� Lansky� SB� (1990)� A� performance�status� scale� for� head� and� neck� cancer� patients.� Cancer 66(3):�564–9
Maus�EA,�Tan�IC,�Rasmussen�JC�et�al�(2012)�Near-infrared�fluorescence� imaging� of� lymphatics� in� head� and� neck�lymphedema.�Head Neck 34(3):�448–53
Micke� O,� Bruns� F,� Mucke� R� et� al� (2003)� Selenium� in�the� treatment� of� radiation-associated� secondary�lymphedema.�Int J Radiat Oncol Biol Phys�56(1):�40–9
Mihara� M,� Uchida� G,� Hara� H� (2011)� Lymphaticovenous�anastomosis� for� facial� lymphoedema� after� multiple�courses� of� therapy� for� head-and-neck� cancer.� J Plast Reconstr Aesthet Surg�64(9):�1221–5
Morton�RP,�Witterick�IJ�(1995)�Rationale�and�development�of�a�quality-of-life� instrument� for�head-and-neck�cancer�patients.�Am J Otolaryngol 16(5):�284–93
National� Cancer� Institute� (2013)� Head and Neck Cancers.�Available� at:� http://1.usa.gov/1e7FJSU� (accessed�12.12.2013)
National� Comprehensive� Cancer� Network� (2013)� NCCN: Distress Thermometer for Patients.�Available�at:�http://bit.ly/1i3JedY�(accessed�19.12.2013)
Pan�WR,�Le�Roux�CM,�Briggs�CA�(2011)�Variations�in�the�lymphatic�drainage�pattern�of�the�head�and�neck:�further�anatomic�studies�and�clinical�implications.�Plast Reconstr Surg�127(2):�611–20
Pan�WR,�Suami�H,�Taylor�GI�(2008)�Lymphatic�drainage�of�the�superficial� tissues�of� the�head�and�neck:�anatomical�study� and� clinical� implications.� Plast Reconstr Surg�121(5):�1614–24
Patterson� JM,� Hildreth� A,� Wilson� JA� (2007)� Measuring�edema�in� irradiated�head�and�neck�cancer�patients.�Ann Otol Rhinol Laryngol�116(8):�559–64
Piso� DU,� Eckardt� A,� Liebermann� A� (2001)� Early�rehabilitation�of�head-neck�edema�after�curative�surgery�for� orofacial� tumors.� Am J Phys Med Rehabil� 80(4):�261–9
Rana� M,� Gellrich� NC,� Joos� U� et� al� (2011)� 3D� evaluation�of� postoperative� swelling� using� two� different� cooling�methods� following� orthognathic� surgery:� a� randomised�observer� blind� prospective� pilot� study.� Int J Oral Maxillofac Surg�40(7):�690–6
Rockson�SG,�Vaillant-Newman�A-M�(2011)�Head�and�neck�lymphedema.�In:�Lee�B-B,�Bergan�JJ,�Rockson�SG�(eds)Lymphedema: A Concise Compendium of Theory and Practice.�Springer,�London:�295–306
Rogers�SN,�Gwanne�S,�Lowe�D�(2002)�The�addition�of�mood�and� anxiety� domains� to� the� University� of� Washington�quality�of�life�scale.�Head Neck�24(6):�521–9
Schultze-Mosgau,� S,� Schmelzeisen,� R,� Frolich,� JC,� Schmele�H� (1995)� Use� of� ibuprofen� and� methylprednisolone�for� the�prevention�of�pain�and�swelling�after�removal�of�impacted�third�molars.�J Oral Maxillofac Surg�53(1):�2–7
Smith� BG,� Lewin� JS� (2010)� Lymphedema� management� in�head�and�neck�cancer.�Curr Opin Otolaryngol Head Neck Surg�18(3):�153–8

Research and audit
16 Journal of Lymphoedema, 2013, Vol 8, No 2
Maho Takeuchi, Toyoko Yoshizawa, Yuko Kusaka, Yoshihito Furusawa, Yasuka Nakamura, Fumi Atogami, Hitoshi Niikura
Detecting subclinical secondary lymphoedema using bioimpedance: A preliminary study
Secondary lymphoedema reduces both a patient’s physical and psychological quality of life (QOL; Franks et al, 2006;
Chase and Wenzel, 2011; Fu et al, 2013) and is frequently seen in cancer patients after treatment that includes lymph node dissection (LND) or radiation therapy (Moffatt et al, 2003). The major symptoms of lymphoedema include discomfort, heaviness, problems with physical mobility, and pain. The condition can be debilitating and require intensive, costly treatment (Ryan et al, 2003; Tiwari, 2003). As the condition is irreversible, patients with, or at risk of developing, lymphoedema require care throughout their life.
Prevention and early intervention are two of the main issues in lymphoedema care (Paskett et al, 2012). Precise assessment of the condition is important for timely intervention and to prevent worsening of the patient’s condition. In many cases, lymph transport impairment is only suspected after the reporting of discomfort, by which time a severe
At low frequencies, most of the current will flow preferentially through the extracellular fluid (ECF). In contrast, reactance of the cell membranes decreases at higher frequencies, and the current passes through both the ECF and intracellular fluid (ICF; Dittmar and Reber, 2002). The ratio of the body water component ECF/ICF or ECF/total body fluid (TBF) is widely used to assess fluid changes in oedematous patients, including those with lymphoedema.
Sakuda et al (2010) showed the characteristics of body fluid by ICF/ECF in breast cancer patients after surgery (Sakuda et al, 2010). Some studies have shown the success of using MF-BIA as a tool to predict the early onset of lymphoedema (Cornish et al, 2001; Halaska et al, 2010). However, there is currently no reliable index to predict the occurrence of lymphoedema.
The aim of the present prospective study was to detect the potential occurrence of secondary lymphoedema due to LND by examining
Abstract
Background: Early intervention is an important facet of the prevention of secondary lymphoedema. However, it is difficult to predict symptoms before swelling becomes clinically significant. Aims: To detect the potential occurrence of secondary lymphoedema due to lymph node dissection (LND) by examining variance in body water composition from pre- to early post-operative phases. Methods: This prospective observational study was carried out on two groups of patients who had undergone gynaecologic surgery, with or without LND (LND and control [CONT] groups, respectively). Weight, lower-limb circumference, and the ratio of extracellular fluid to total body fluid (E/T) were measured preoperatively and on postoperative day 7 (POD 7). Results: Eighteen patients completed the study (LND group, 12; CONT group, 6). Two patients in the LND group had genital swelling on POD7. In the LND group, a significant increase in E/T in the right leg and body trunk was observed. Conclusion: Early changes in LND group E/T were observed. Further studies are required to develop a reliable index for predicting the occurrence of lymphoedema.
Key words
Bioimpedance analysis, early assessment, secondary lymphoedema
Maho Takeuchi, PhD student, Department of Palliative Nursing ; Toyoko Yoshizawa, Professor, Women’s Health Nursing ; Yuko Kusaka, Master’s student, Women’s Health Nursing ; Yoshihito Furusawa, Attending Staff, Department of Physical Medicine and Rehabilitation; Yasuka Nakamura, Assistant Professor, Women’s Health Nursing ; Fumi Atogami, Associate Professor, Women’s Health Nursing ; Hitoshi Niikura, Professor, Department of Gynecology; all at Tohoku University Graduate School of Medicine, Sendai, Japan
Declaration of interest: None.
condition has often developed (Weissleder and Schuchhardt, 2008).
Preventing lymphoedema following cancer treatment is an important issue with long-term health costs. Preventive education for postoperative patients with gynaecological, prostate, or breast cancer with LND in Japan is provided twice by national health insurance; perioperatively on admission for surgery, and within one month of discharge.
A reliable predictive index for the onset of lymphoedema that enables early intervention and preventative care is required.
Multiple frequency bioimpedance analysis (MF-BIA) is a noninvasive method used in various clinical settings to estimate body fluid (Bellizzi et al, 2006; Mager et al, 2008). In recent years, MF-BIA has been applied to the quantification of lymphoedema (Hayes et al, 2009; Loudon et al, 2012). The technique is based on different conductive and resistive properties when a small electric current is applied to tissues in vivo (Ackland et al, 2004).

MADE TO MEASURE2 FABRICSPertex & Goldpunkt
Availab
le on
GLOVES * PANTYHOSE * THIGH WITH WAIST ATTACHMENT
NO CHARGE OR CODE FOR:CLOSED TOE * NON-STANDARD COLOURFLY FOR MEN * SLANT CUT
email [email protected] or check www.hadhealth.com
REPEAT NUMBER SYSTEMFOR SIMPLE RE-ORDERING
Y-HEEL™ DESIGNFOR ADDED COMFORT (as standard)
* Regular Training Courses* Bespoke training for clinics
HaddenhamTraining Academy
DRU
G
TARIFF
CCL 1, 2 & 3 CCL 2, 3 & 4
ONE CODEFOR ORDERING

Research and audit
variance in the body water composition of patients’ lower limbs before, and during the early stages after, LND.
MethodsA prospective, single-centre, observational, preliminary study of two groups of patients who had undergone gynaecological surgery, with are without LND, was conducted between February and September 2011.
SettingsThis study was conducted in the outpatient department of the gynaecology unit and the outpatient department of the lymphoedema care ward at a university hospital in the Tohoku region, Japan.
SamplePatients scheduled to undergo gynaecological surgery were potential candidates for the study, except those who were diagnosed with primary lymphedema or had other oedema-related episodes (e.g. kidney, liver, or circulation disorders). Patients were divided into two groups according to whether or not they had undergone LND: a LND group, and a control (CONT) group, respectively.
ProcedurePatients were recruited on the date of admission. The first examination (pre-OPE) was conducted after informed consent was obtained, and the second examination was conducted on the seventh day postoperatively (POD7), after the patient’s general condition was stable and after all drainage, intravenous drips, and staples had been removed. Due to the circadian variation in body water, measurements were conducted between 2pm and 4pm local time.
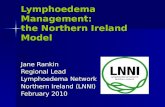
Assessment of lower-limb conditionsThe circumference of each lower limb was measured at the following seven locations with a plastic measuring tape: acrotarsium
Statistical analysisDemographic characteristics were summarised. Wilcoxon’s test was used to evaluate the statistical significance of differences between the two groups, and between pre-OPE and POD7 measurements.
A P-value of <0.05 was considered significant. All tests were two tailed. The authors acknowledge that the comparisons in this analysis may inflate the type 2 error rate in this pilot study. Data were managed in Microsoft Excel and analysed in SPSS predictive analytics software, while the study was assessed and approved by the Ethics Committee of Tohoku University Graduate School of Medicine.
ResultsTwenty-one patients (LND n=14; CONT n=7) participated in the study. The key demographic, diagnostic, and treatment characteristics are detailed in Table 1. They were: cancer of the cervix (LND, n=3; CONT, n=1), cancer of the uterus (LND, n=10; CONT, n=2), cancer of the ovary (LND, n=1; CONT, n=1), and three other diseases (myoma, ovarian tumour, and choriocarcinoma) in the CONT group.
The extension of LND in the LND group comprised one case of pelvic lymphadenectomy and 13 cases of paraaortic lymphadenectomy. In the CONT group, all patients underwent abdominal total hysterectomy (ATH, n=1) or ATH and bilateral salpingo-oophorectomy (BSO, n=6). Two patients in the LND group were unable to participate in the study on POD7 due to their still receiving an intravenous drip, and one patient in the CONT group was discharged early and therefore missed
(mid-foot); immediately above the ankle joint; 10 cm distal to the patella; directly above the patella; 12 cm and 20 cm proximal to the patella; and at the uppermost part of the lower limb (Figure 1).
MF-BIAFor taking body water measurements a bioimpedance spectrometer was used. Before the examination, patients urinated and removed jewellery. Patients wore hospital gowns or clothes without any metallic accessories. The measurement took place with the patient in the supine position after a minimum of 5 minutes rest. Both upper limbs were positioned away from the body trunk, and the thighs were opened to about 30°. The ratio of ECF to TBF (E/T) was then calculated. The “eight electrodes method” (Bosy-Westphal et al, 2013) was employed to measure the fluid content of the whole body and also specific body parts (i.e. right/left upper limb, body trunk, and right/left lower limb).
For healthy individuals, E/T values of 0.36 to 0.40 are expected; higher E/T values indicate an increase in TBF (Van Loan and Mayclin, 1992; Kyle et al, 2004).
Figure 1. Location of the circumference measurement.
18 Journal of Lymphoedema, 2013, Vol 8, No 2
Lymph node dissection (n=14)Mean±SD Median
Control (n=7)Mean±SD Median
Z-value P-value
Age (years) 55.1±9.5 57.0 43.5±12.8 42.0 2.01 0.044
Height (cm) 158.0±7.3 158.0 156.1±7.1 155.7 0.10 0.920
Weight (kg) 58.5±9.3 57.6 67.7±23.4 57.0 0.50 0.615
BMI (kg/m2) 23.5±3.5 22.9 27.9±10.5 26.5 0.01 0.315
Cancer type Cervical Uterine Ovarian Other / unknown
N %3 21.410 71.41 7.1- -
N %1 14.32 28.61 14.33 42.9
- - - -
- - - -
Surgery type (LND)Pelvic lymphadenectomy
Paraaortic lymphadenectomy
N %1 7.113 92.9
N - -
% - -
- -
- -
Table 1. Patient characteristics.

Research and audit
Journal of Lymphoedema, 2013, Vol 8, No 2 19
the POD7 measurement. Twelve patients in the LND group and six patients in the CONT group completed the study, and their data were subsequently analysed.
No significant differences in age, height, weight, or body mass index were identified between the LND and CONT groups by Wilcoxon’s test. Two patients from the LND group reported an oedematous condition around their vulva on POD7, which was confirmed by their physician. No other swelling was reported by these two patients or by any other patients in the study.
Weight and circumferential changesNo significant differences were observed between the LND and CONT groups at either examination. An unexpected, but significant, decrease in circumference 12 cm distal to the patella on both legs (P=0.013) in the LND group was seen between pre-OPE and POD7 (Table 2). No significant differences in circumferential measurements were observed in the CONT group.
Bioimpedance analysis The LND group showed a significantly higher E/T than the CONT group in the body trunk on POD7 (P=0.04). No significant differences in other regions of the body were observed.
and lower limbs. Our results are compatible with these observations. The changes were only observed in the right lower limb. This might be due to the short follow-up period (7 days) and small sample size, which are limitations of this study. The short-term and unexpected trend in decreasing circumference 12 cm and 20 cm proximal to the patella in the LND group (Table 3) could also be due to the limitations of the study.
A previous retrospective study showed that 75% of postsurgical lymphoedema cases occur within one year (Beesley et al, 2007). In another retrospective study, Tada et al (2009) reported that secondary lymphoedema of the lower limbs can be observed at a mean of 4.2 months after the surgery but can occur as early as 0.1 month. Prospectively, monitoring parameters related to lymphoedema presurgery would allow detection of subtle changes before patients are aware of their symptoms, allowing early intervention.
The MF-BIA was used to monitor one of these parameters in the present study. Halaska et al (2006) also used this method to prospectively assess patients for lymphoedema 3 months before and 6 months after surgery for uterine cervical cancer. They reported a 47.6% prevalence of lymphoedema 6 months after surgery. Since lymphoedema has been reported in some studies as early as 0.1 month after surgery, it is reasonable to assume that some changes would have occurred 3 months after surgery. This would be consistent with the subtle changes the authors observed in the lower limbs after only a week (POD7).
This short-term study does not include any of the effects of adjuvant therapy, such as radiotherapy, which is reported to increase the risk of lymphoedema (Tada et al, 2009). Therefore, the authors propose follow-up of parameters related to lymphoedema (particularly changes in body fluid) before and as early as possible after surgery to avoid missing the opportunity for timely treatment.
Early detection and management of lymphoedema have another benefit; reducing the potential risk of infection and hospitalisation in the longer term. Chronic oedema is a known risk factor for cellulitis, which can become recurrent after a single soft tissue infection (Swartz, 2004). Cox (2006) also found that there is a strong association between oedema and cellulitis, each of which is both a risk factor for, and
Table 3 provides a summary of the E/T of the body fluid in each region at each examination. In the LND group, POD7 E/T was significantly higher than that of pre-OPE in the body trunk (P=0.003) and right lower limb (P=0.005).
No significant differences between the two groups were seen throughout the measurement term (pre-OPE to POD7). Measurements in the upper limb indicated significant changes in E/T.
DiscussionThis study revealed changes in the lower limb during the early phase after gynaecological surgery with LND. Patients who had LND showed a change in E/T in the right lower limb and trunk, although subjective symptoms were reported in only few cases (Table 3). This finding indicates that body fluid changes could be detected before the symptomatic awareness. Cornish et al (2001) have previously made this point by using the MF-BIA technique in breast cancer patients, however, there are limited studies relevant to gynaecologic cancer-related lymphoedema.
After gynaecological cancer surgery with LND, swelling is often clinically observed in the genital and inguinal region and can extend to other regions, such as the upper
Pre-OPE (cm)Mean±SD Median
POD7 (cm)Mean±SD Median
Z-value P-value
Weight (kg) 59.3±9.8 57.6 58.4±9.3 57.0 0.84 0.401
Right leg
1. Acrotarsium 21.1±1.1 21 21.0±1.1 20.7 0.41 0.681
2. Ankle 20.3±1.7 20 19.9±1.5 19.5 1.20 0.229
3. 10cm lower patella 34.2±2.5 34.4 33.4±2.1 33.5 1.65 0.100
4. Patella 33.5±2.9 32.8 33.0±2.9 32.6 0.40 0.688
5. 12cm upper patella 41.5±3.7 40.4 40.4±3.4 39.7 2.49 0.013
6. 20cm upper patella 47.9±4.2 48.2 47.2±4.2 47.6 1.91 0.056
7. Upper most 51.9±5.2 52.45 51.9±5.3 51.7 1.07 0.283
Left leg
1. Acrotarsium 21.01±1.1 20.8 20.8±1.1 20.4 1.43 0.514
2. Ankle 20.2±1.8 19.8 20.6±2.3 19.5 1.23 0.218
3. 10cm lower patella 33.8±2.4 34.4 35.7±5.2 32.5 1.79 0.074
4. Patella 33.4±2.9 32.9 32.7±2.7 32.7 1.21 0.228
5. 12cm upper patella 41.3±3.6 41.7 40.1±3.7 40.4 2.49 0.013
6. 20cm upper patella 47.5±4.4 47.8 46.5±4.0 47.6 2.27 0.023
7. Upper most 51.9±5.3 52.3 51.6±4.7 52.3 2.81 0.412
Table 2. Circumference measurement of the lower limb preoperatively (pre-OPE) and seventh day postoperatively (POD7) in the lymph node dissection group (n=12).

Research and audit
References Ackland GL, Singh-Ranger D, Fox S et al (2004) Assessment of
preoperative fluid depletion using bioimpedance analysis. Br J Anaesth 92(1): 134–6
Beesley V, Janda M, Eakin E et al (2007) Lymphedema after gynecological cancer treatment : prevalence, correlates, and supportive care needs. Cancer 109(12): 2607–14
Bellizzi V, Scalfi L, Terracciano V et al (2006) Early changes in bioelectrical estimates of body composition in chronic kidney disease. J Am Soc Nephrol 17(5): 1481–7
Bosy-Westphal A, Schautz B, Later W et al (2013) What makes a BIA equation unique? Validity of eight-electrode multifrequency BIA to estimate body composition in a healthy adult population. Eur J Clin Nutr 67 (Suppl 1): S14–21
Chase DM, Wenzel L (2011) Health-related quality of life in ovarian cancer patients and its impact on clinical management. Expert Rev Pharmacoecon Outcomes Res 11(4): 421–31
Cornish BH, Chapman M, Hirst C et al (2001) Early diagnosis of lymphedema using multiple frequency bioimpedance. Lymphology 34(1): 2–11
Cox NH (2006) Oedema as a risk factor for multiple episodes of cellulitis/erysipelas of the lower leg: a series with community follow-up. Br J Dermatol 155(5): 947–50
Dittmar M, Reber H (2002) Evaluation of different methods for assessing intracellular fluid in healthy older people: a cross-validation study. J Am Geriatr Soc 50(1): 104–10
Franks PJ, Moffatt CJ, Doherty DC et al (2006) Assessment of health-related quality of life in patients with lymphedema of the lower limb. Wound Repair Regen 14(2): 110–8
Fu MR, Ridner SH, Hu SH et al (2013) Psychosocial impact of lymphedema: a systematic review of literature from 2004 to 2011. Psychooncology 22(7): 1466–84
Halaska MJ, Komarek V, Mala I et al (2006) A method for the detection of post-operative lymphoedema after operation for breast cancer: multifrequency bioelectrical impedance analysis. J Appl Biomed 4(4): 179–85
Halaska MJ, Novackova M, Mala I et al (2010) A prospective study of postoperative lymphedema after surgery for cervical cancer. Int J Gynecol Cancer 20(5): 900–4
Hayes SC, Reul-Hirche H, Turner J (2009) Exercise and secondary lymphedema: safety, potential benefits, and research issues. Med Sci Sports Exerc 41(3): 483–9
Kyle UG, Bosaeus I, De Lorenzo AD et al (2004) Bioelectrical impedance analysis--part I: review of principles and methods. Clin Nutr 23(5): 1226–43
Loudon A, Barnett T, Piller N et al (2012) The effect of yoga on women with secondary arm lymphoedema from breast cancer treatment. BMC Complement Altern Med 12: 66
Mager JR, Sibley SD, Beckman TR (2008) Multifrequency bioelectrical impedance analysis and bioimpedance spectroscopy for monitoring fluid and body cell mass changes after gastric bypass surgery. Clin Nutr 27(6): 832–41
Moffatt CJ, Franks PJ, Doherty DC et al (2003)Lymphoedema: an underestimated health problem. QJM 96(10): 731–8
Paskett ED, Dean JA, Oliveri JM, Harrop JP (2012) Cancer-related lymphedema risk factors, diagnosis, treatment, and impact: a review. J Clin Oncol 30(30): 3726–33
Ryan M, Stainton MC, Jaconelli C et al (2003) The experience of lower limb lymphedema for women after treatment for gynecologic cancer. Oncol Nurs Forum 30(3): 417–23
Sakuda H, Satoh M, Sakaguchi M et al (2010) Physiological characteristics of the body fluid in lymphedematous patients postbreast cancer surgery, focusing on the intracellular/extracellular fluid ratio of the upper limb. Jpn J Nurs Sci 7(1): 108–18
Swartz MN (2004) Clinical practice. Cellulitis. N Engl J Med 350(9): 904–12
Tada H, Teramukai S, Fukushima M, Sasaki H (2009)Risk factors for lower limb lymphedema after lymph node dissection in patients with ovarian and uterine carcinoma. BMC Cancer 9: 47
Tiwari A, Cheng KS, Button M et al (2003) Differential Diagnosis, Investigation, and Current Treatment of Lower Limb Lymphedema. Arch Surg 138(2): 152–61
Van Loan MD, Mayclin PL (1992) Use of multi-frequency bioelectrical impedance analysis for the estimation of extracellular fluid. Eur J Clin Nutr 46(2): 117–24
Weissleder H, Schuchhardt C (2008) Lymphedema Diagnosis and Therapy (4th edn). Viavital Verlag, Essen
AcknowledgementsThis work was supported by the Japan Society for the Promotion of Science KAKENHI (Grant Number 23390506). The authors would like to thank all participants for taking part in this study. We are also grateful to Rhian Davies, University of Glasgow, for her advice on the writing of this article.
consequence of, the other. Reducing oedema is effective in reducing cellulitic episodes, however, prevention of lymphoedema through early intervention may be the most effective prevention of cellulitis.
The authors are mindful that the swelling of limbs in the early phase following surgery is a temporary symptom (Moore, 1958; Wilmore, 2002) and secondary lymphoedema is often a late manifestation; a longer follow-up period is needed to predict the occurrence of lymphoedema. However, assessment and understanding of swelling or oedematous symptoms following surgery is important and may better inform our understanding of the clinical course of lymphoedema.
In the future, the authors intend to extend the observation period to prospectively monitor the spread of lymphoedema to other regions of the body and to elucidate the clinical course of lymphoedema in this patient population.
ConclusionBody water changes were observed in the early postoperative phase in LND patients. MF-BIA is one of the tools for detecting potential early changes, even before the appearance of subjective symptoms. The methodological feasibility of this study has opened up the possibility of further studies on lymphoedema.
Pre-OPE POD7 Z-value P-value
Mean±SD Median Mean±SD Median
LND group
1. Right upper limb 0.3771±0.005 0.379 0.3771±0.045 0.376 0.717 0.474
2. Left upper limb 0.3799±0.003 0.381 0.3779±0.003 0.379 0.760 0.447
3. Body trunk 0.3937±0.005 0.384 0.3927±0.005 0.391 2.936 0.003
4. Right lower limb 0.3919±0.008 0.387 0.3919±0.008 0.391 2.807 0.005
5. Left lower limb 0.3904±0.007 0.387 0.3904±0.007 0.389 1.423 0.311
6. Total body 0.3905±0.005 0.385 0.3905±0.005 0.388 2.807 0.005
Control group
1. Right upper limb 0.3773±0.003 0.379 0.3770±0.006 0.3775 0.365 0.715
2. Left upper limb 0.3785±0.003 0.379 0.3784±0.005 0.3790 0.406 0.684
3. Body trunk 0.3782±0.007 0.381 0.3830±0.009 0.3865 1.753 0.080
4. Right lower limb 0.3777±0.009 0.380 0.3798±0.016 0.3850 0.813 0.416
5. Left lower limb 0.3820±0.009 0.387 0.3870±0.100 0.3870 1.483 0.138
6. Total body 0.3788±0.007 0.382 0.3826±0.103 0.3855 1.355 0.176
Table 3. Extracellular fluid to total body fluid of the lower limb preoperatively (pre-OPE) and seventh day postoperatively (POD7) in the lymph node dissection (LND; n=12) and control (n=6) groups.
20 Journal of Lymphoedema, 2013, Vol 8, No 2

Practice development
Journal of Lymphoedema, 2013, Vol 8, No 2 21
Polymnia Nikolaidis, Katarina Karlsson
Evidence and tradition in conflict: The Swedish experience of lymphoedema treatment and care
The treatment of chronic oedema and lymphoedema varies around the world. The availability of
treatment varies and is determined by the patient’s distance from the therapist and the number of trained lympheodema therapists at a given facility. Cost is a further barrier to receiving optimal treatment.
Clinicians in different countries often choose different treatments and strategies. At the recent International Society of Lymphology congresses in Rome and Malmö (16–20 September 2013 and 19–23 September 2011, respectively) the variations were evident.
Global variationsIn parts of the world where filariasis is the common cause of secondary lymphoedema (e.g. India, Thailand, and other parts of Asia, as well as South America), patients do not present until their condition is significant in terms of swelling. Health care is reactive and the focus is more on functional issues.
Generally, the main goals of treatment are to increase the individual’s mobility, promote return to work (where applicable), and restore the person’s ability to support themselves. Of course, there is also the need to better control of the vectors (i.e. mosquitoes in the case of filariasis) to achieve prevention.
Lymphoedema therapists are generally fully responsible for initiating and evaluating the lymphoedema treatment plan. This includes the ordering and fitting of compression garments and stockings. This is an advantage as the therapist follows the person from diagnosis to endpoint and can continue to monitor, manage, and evaluate the patient.
Follow-up visits with patients after lymph node surgery are routine. This includes patients with malignant melanoma. Patients are provided with preventive information early (usually the day after surgery) and are normally followed-up 4–5 weeks later by a physiotherapist/lymphoedema therapist, either individually or in a group.
At the follow-up visit, an assessment of joint mobility is conducted and the patient is informed about the basic functioning of the lymphatic system, skin care, and the importance of performing some kind of physical activity. These individuals are encouraged to begin their physical activities as soon as possible, preferably 2–3 weeks postsurgery.
People who were previously physically inactive are advised to take up some kind of exercise for the upper body – such as swimming, pole walking (Nordic walking), weight lifting, cross country
Abstract
The basis of Swedish lymphoedema treatment programmes were first developed in Germany early last century. The treatment principles remained the same until recent years and are based on manual lymph drainage, compression, skin care, and exercise. However, our experience is that it is important to assess patients holistically and therefore other approaches to treatment may be better. We suggest that less emphasis be placed on manual lymph drainage and more on compression, exercise, and weight reduction.
Key words
Lymphoedema therapist, patient expectation, communication, patient organisation
Polymnia Nikolaidis and Katarina Karlsson, Physiotherapists and Lymphoedema Therapists, Department of Cancer Rehabilitation, Karolinska University Hospital, Stockholm, Sweden
Declaration of interest: None.
In a developed country like Sweden, patients generally present early, the oedema volume is usually low, and oedema is mainly related to cancer treatment. Knowledge of cancer-related oedemas is important. These are often recognised at an early stage and the lymphoedema treatment is an integrated part of rehabilitation.
However, access to care may vary, particularly due to geography and clinician availability. The goal of lymphoedema treatment is not only to reduce and/or improve function, but also to improve patients’ quality of life and – for those at risk of developing lymohoedema – deliver education on prevention.
Swedish lymphoedema careStockholm, with a population of around 1.5 million, currently has 53 registered lymphoedema therapists in primary care, and 17 in home and palliative care teams. There are also a couple of private rehabilitation clinics out of which 12 therapists operate. This means that there is one therapist per 18 750 inhabitants.
In Sweden, a doctor’s referral is not required for a consultation with a lymphoedema therapist and patients often contact lymphoedema therapists in primary care directly.

Practice development
22 Journal of Lymphoedema, 2013, Vol 8, No 2
skiing, or rowing – in order to stimulate the lymphatic and blood circulation. In the case of inguinal clearance, cycling and swimming are recommended. At this visit the therapist will measure the limb and order compression stockings or sleeves, in case oedema should develop.
There are many benefits of early diagnosis and treatment (Ramos et al, 1999; Johansson and Branje, 2010). Patients can either eliminate minor oedema or reduce it to a level that does not affect their activities.
In terms of rehabilitation, at Karolinska University Hospital in Stockholm, patients are educated to recognise the early signs of lymphoedema and usually present early with minimal oedema (stage 0–2).
For breast cancer patients, compression garments or bandaging are recommended for a few days in most cases to reduce oedema, if needed, and thereafter measure and fit a compression garment.
Manual lymph drainage (MLD) performed by the lymphoedema therapist is never the first choice of treatment. Patients are informed about the lack of evidence for MLD, but are encouraged to undertake self massage for a short period to evaluate its effects. Where self massage is ineffectual, the patient can discontinue and focus on wearing compression garments and being physically active. Patients are encouraged to begin some form of exercise for improving circulation (Schmitz et al, 2010; Kwan et al, 2011).
In cases of advanced cancer, the treatment plan is different and depends on factors such as venous obstruction, medication-related oedema, levels of plasma protein, activity, oncological treatment, and oedema status. Treatment is mainly aimed at improving function and comfort.
Treatment expectationsPatients may have different goals, motivations, and expectations of treatment. For a patient with high levels of oedema, a reduction in oedema may mean that they can return to work, for another, even a small volume of oedema may negatively impact self confidence and self esteem with the accompanying psycho–social consequences. Thus, patient expectations may not always coincide with the lymphoedema therapist’s goals and expectations of treatment.
differently to both compression and physical activity.
Often the lymphoedema therapist has to assess which therapies work best for the individual. At times, it can be a “try and see” approach, where one change is made at a time and its effect is measured.
Primary lymphoedema is relatively rare and commonly underdiagnosed, which contributes to the fact that this group of patients usually presents at a later stage than those with oedema related to breast cancer treatment. This late presentation makes the treatment more extensive and difficult and is compounded by the lack of doctors specialising in lymphoedema. This often means that a complicated patient is assessed solely by a lymphoedema therapist. Experience is critical in providing targeted and appropriate treatments to optimise outcomes. Fortunately, complex cases are becoming rarer, since knowledge about lymphoedema and its treatment are becoming more well known.
However, in Sweden, the authors know from experience that many newly trained lymphoedema therapists often do not have access to patients’ medical records and do not have an experienced supervisor or mentor to ask for advice. This can compromise patient care and result in suboptimal treatment.
A further problem is that a physical therapist or lymphoedema therapist working in primary care will mainly treat other groups of patients, such as those with orthopedic, neurological, or muscle-related disorders. The therapist may actually assess, treat, and follow-up very few lymphoedema patients. It may take many years to gain clinical experience of the various types of oedemas and lymphoedemas, and of the optimal treatments. In an oncology setting, this does not pose such a problem as many patients are similar in terms of their treatment and present for therapy relatively early.
Education issues Some lymphoedema therapist education programmes are short (sometimes only a few days in duration) and their targets are primarily cosmetologists and beauticians. In Sweden, longer courses (4–6 weeks) are only open to clinicians such as physiotherapists, nurses, and occupational therapists.
A shift in careTraditionally, the main outcome measure of successful lymphoedema treatment has been reduced oedema volume. Treatment has been focused on MLD. However, based on more recent research, a paradigm shift in therapy is underway. In the future, therapists will most likely emphasise holistic care, favouring compression therapy and physical activity over MLD.
In recent years, there has been contradictory evidence of the value of MLD. Research is not always convincing, and MLD has not proven to reduce the volume of lymphoedema (Kärki et al, 2009; Huang et al, 2013).
Physical activity in cancer care is important because it has been shown to reduce the side effects of treatment (e.g. pain, fatigue, and nausea) and improve quality of life, physical strength, and mobility (McNeely et al, 2006).
Lymphoedema therapists need to examine how we can accelerate change in our approach to oedema management and how this should be integrated into health care systems.
Patient responsibilityThe level of responsibility the patient is expected to take is different around the world. In some countries, the patient is passive – they expect the therapist to take full responsibility for their oedema treatment and they willingly place themselves in the hands of the therapists. In other countries, emphasis is given to the patient accepting responsibility for their treatment and the therapist has a more guiding role.
A good clinical outcome is more likely to be achieved if the therapist and patient agree on treatment goals and the patient’s obligations (i.e. some form of contract exists). The therapist must be clear about what is required of the patient and encourage them to ask themselves: “What have I done for my oedema/limb today?”
It is also important to enhance and reinforce the patient’s ability to cope with everyday oedema care, which may be tiresome for some people (Piller, 2012).
Some oedemas are complex and this is particularly true of lower-limb oedema. Few secondary lymphoedemas are solely of lymphatic origin and there is usually venous insufficiency present to some degree. This means that patients respond

Practice development
Journal of Lymphoedema, 2013, Vol 8, No 2 23
Nonetheless, the therapist in the shorter education programmes will often receive a certificate stating that they have received some degree of lymph therapist education. In Sweden, holding this type of certificate can mean a clinician is allowed to treat patients with secondary lymphoedema. Often this leads to people treating patients without possessing any basic knowledge of oncology or pathophysiology. Ideally, no person without a basic clinical qualification should be accepted for a lymphoedema therapy training programme.
The title “lymphoedema therapist” is not one of the professions covered by the Patient Safety Act in Sweden. This means that while lymphoedema therapists with no medical qualifications are not allowed to work and treat patients within the public healthcare system, they can still treat lymphoedema patients at private clinics. This must be borne in mind to ensure the limitations of knowledge and practice can be addressed.
As previously mentioned, therapists’ backgrounds vary and so does their therapeutic focus. For example, in England, nurses initially treat lymphoedema patients, and their main focus is on the skin and skin-related issues. While in Sweden, for the most part, physiotherapists treat lymphoedema. Therefore, the body’s musculoskeletal system and function and activity limitations are focused on. Fewer skin problems are also encountered by clinicians since patients are treated earlier in the process.
Self-care is keyThe significance placed on physical activity in the treatment of lymphoedema in Sweden means that a large proportion of patients are required not only to take care of their skin and compression therapy, but also to exercise regularly. Thus, patients spend a lot of time managing their oedema treatment.
The lymphoedema therapist’s role in treatment is to guide, motivate, and empower patients, helping them take an active role in treating their oedema.
From clinical experience, the authors note that many patients choose to end their contact with the lymphoedema therapist. The reasons may vary, and we know from experience that some early oedemas decrease with time or disappear
collective knowledge of oedema, and often, importantly, what others think of available therapists. An important part of the work of these organisations is, therefore, to provide objective and evidence-based information to their members as well as convey to them the fact that not every method is appropriate in every case.
The research into lymphoedema treatment is limited. Not every therapy has a high level of evidence and there will often be contradictory reports. Presenting and acknowledging the balance is critical in ensuring therapists, patients, and patient organisations work together for the best outcomes. Communication is a critical part of this process. The interaction between the lymphoedema therapist and these organisations needs examining.
ConclusionLymphoedema treatment in Sweden is not perfect, but there is a great opportunity to make it better. A paradigm shift in treatment can more easily be implemented by greater holistic thinking and working in close cooperation with patient organisations.
References
Huang TW, Tseng SH, Lin CC et al (2013) Effects of manual lymphatic drainage on breast cancer-related lymphoedema: a systematic review and meta-analysis of randomized controlled trials. World J Surg Oncol 11: 15
Johansson K, Branje E (2010) Arm lymphoedema in a cohort of breast cancer survivors 10 years after diagnosis. Acta Oncol 49(2): 166–73
Kärki A, Anttila H, Tasmuth T, Rautakorpi UM (2009) Lymphoedema therapy in breast cancer patients: a systematic review on effectiveness and survey of current practices and costs in Finland. Acta Oncol 48(6): 850–9
Kwan ML, Cohn JC, Armer JM et al (2011) Exercise in patients with lymphoedema: a systematic review of the contemporary literature. J Cancer Surviv 5(4): 320–36
McNeely ML, Campbell KL, Rowe BH et al (2006) Effects of exercise on breast cancer patients and survivors: a systematic review and meta-analysis. CMAJ 175(1): 34–41
Piller N (2012) We need to help patients to help themselves. Journal of Lymphoedema 7(1): 6
Ramos SM, O’Donnell LS, Knight G (1999) Edema volume, not timing, is the key to success in lymphoedema treatment. Am J Surg178(4): 311–5
Schmitz KH, Ahmed RL, Troxel AB et al (2010) Weight lifting for women at risk for breast cancer-related lymphedema: a randomized trial. JAMA 304(24): 2699–705
completely and so the patient no longer needs or seeks any input from the lymphoedema therapist.
Some patients who have low volume oedemas request regular MLD. Those who live in the Stockholm area are able to receive such treatment from the many lymphoedema therapists in the city. Unfortunately, the wide availability of lymphoedema therapists may mean that some patients are over-treated with MLD, use compression when they do not actually need it, or become dependant on the lymphoedema therapist rather than independent.
Patients are sometimes frustrated when they cannot receive MLD in the way they did earlier in their treatment, or from what they know other similar patients have received. People also want other complementary techniques, such as laser therapy, compression pumps, and other methods they have heard about. Therefore, some patients are sometimes disappointed that the healthcare system is too evidence-based and does not use complementary methods to the extent they would like.
This leaves a number of important questions unanswered. Is it outcomes other than reduced oedema volume that some patients expect from treatment? How well can lymphoedema therapists meet these patients’ needs? Is the patient asking for MLD for reasons other than oedema/volume reduction? Is it perhaps the touch/tactile stimulation or the soothing effect of the MLD? Should this additional demand be met by lymphoedema therapists, or should these patients seek a private massage therapist?
A new approach to careWe need to consider if therapists need to be more holistic in their approach and integrate and accept other professions into the management of the patient. For instance, in some circumstances, could cognitive behavioural therapy help the patient better handle cancer, the impacts of its treatment, and the symptoms of the lymphoedema? Perhaps body awareness training, mindfulness, or yoga might help?
Patients frequently seek out patient organisations to meet other people in the same situation, gain knowledge from other patients’ experiences, actively questioning treatments, share their

Case report
24 Journal of Lymphoedema, 2013, Vol 8, No 2
Malou van Zanten, Beth Kean
Use of a two-layer compression system in severe bilateral leg lymphoedema with ulceration: A case report
R esearch into the benefits of compression on venous congestion and associated ulceration has been
widely documented (Milic et al, 2010; Stucker et al, 2013). However, research into the correct level of compression for lymphoedema is difficult to obtain, most likely due to a lack of inclusion of rigorous undergarment pressure measurements in reports. The preferred method of lymphoedema treatment is usually compression of the limb, due to its ability to enhance venous return, reduce capillary filtration, and increase lymphatic reabsorption and the breakdown of fibrotic tissue (Moffatt et al, 2011; Muldoon and Charles, 2013).
It is vital that, during the intensive treatment phase for lymphoedema, the compression garment does not hinder an individual’s range of movement to ensure maximum lymph flow from the affected area. It has been documented that muscle contraction while wearing compression produces a higher peak in blood and lymph flow velocity (Partsch and Moffatt, 2012).
Australian community (Barker and Weller, 2010). Chronic leg ulcers are believed to affect more than 3% of the population aged ≥65 years, with a 56% chance of reoccurrence within 3 months of healing (Barker, 2010).
Case studyA 61-year-old Caucasian male (Patient X) presented at the Lymphoedema Research Unit at Flinders University in April 2013 with severe bilateral lymphoedema, that had persisted since 2009. He had received several intensive reduction treatments since that time; however, due to high treatment costs, he ceased them in early 2011.
The patient reported that in March 2008 he had multiple fibromas removed from the groin. The fibromas penetrated deeper than initially anticipated. Within 2 days of surgery, the postoperative deep tissue wounds had become infected, and the participant was admitted for multiple daily dressing changes. Three days later, the wounds showed signs of continued breakdown and an increase in necrotic tissue. Patient X was immediately admitted to
Abstract
Background: In this case report the authors present an individual with a medical history of severe bilateral leg lymphoedema, multiple bilateral ulceration, type 2 diabetes, and morbid obesity. Aim: To determine the efficacy of a commercially available compression system (Coban™ 2 Compression System; 3M) on an individual with severe bilateral leg lymphoedema, and multiple bilateral ulceration. Methods: Employing the Coban 2 Compression System toe-boot bandaging technique, objective and subjective data on leg volume, tissue compositional changes and wound healing were collected at baseline and three times per week over a 4-week follow-up period. Under-bandage pressures were controlled using a pressure monitor during bandage application. Results: The patient’s total limb volume decreased during treatment; circumference volume measurements showed a 3 L reduction in the left leg, and a 1.3 L reduction in the right leg. Limb volume decreased by 2.1 L in the left leg, and 2.1 L in the right. Bioimpedance spectroscopy data measured a reduction of 3.2 L in the left leg and 3.0 L in the right leg. Tissue fluids reduced by 55% in the superficial tissue of both calves during the intervention period. The reduction of the total wound size was 21.7 cm2 in the left leg and 19.95 cm2 in the right leg. Conclusion: Treatment with Coban 2 Compression System improved wound healing and decreased leg volume in the present case.
Key words
Chronic ulcer, compression, lymphoedema, wound healing
Malou van Zanten, Research Officer and PhD candidate, Lymphoedema Research Unit, Department of Surgery, School of Medicine, Flinders University, South Australia, Australia. Beth Kean, Lymphoedema Research Unit Coordinator, Lymphoedema Research Unit, Department of Surgery, School of Medicine, Flinders University, South Australia, Australia
Declaration of interest: None.
The Coban™ 2 Compression System (3M) is a two-layer, latex-free, self-adherent compression bandage. Its rigidity and inelastic properties ensure a high working pressure and low resting pressure. The Coban 2 Compression System has been shown to be useful in lymphoedema reduction and venous ulcer healing in multicentre, randomised, controlled trial settings (3M, 2011; Moffatt et al, 2011; Morgan et al, 2011). These studies account for the user-friendliness of the application for the clinician, as well as monitoring slippage, patient comfort, and mobility.
The burden of chronic woundsChronic nonhealing wounds frequently occur in the latter stages of lymphoedema. They are especially problematic in the lower legs due to their dependency. Chronic wounds can be costly and are a major public health problem in addition to significantly reducing the quality of life of the affected person (Agale, 2013). A high incidence of venous ulcers and recurrence has been reported within the

Case report
Journal of Lymphoedema, 2013, Vol 8, No 2 25
emergency surgery to prevent the spread of gangrene. The extent of soft tissue trauma, major infection, and possibly lymphatic vessel disruption is likely to have evoked the onset of lymphoedema in 2009.
In October 2012, a lymphoscintigram showed functional lymphatic insufficiency, but no indication of dermal backflow. Lymph drainage from both legs was within normal limits. Deep vein thrombosis was discounted and a chest X-ray did not show overt cardiac failure.
With a history of morbid obesity, hypertension, and type 2 diabetes, the skin on the patient’s lower legs showed signs of dryness, fissures, and weeping ulcers. He also suffered recurrent episodes of erysipelas, further compounding the lymphoedema. A lower-back injury prevented him from wearing a compression garment. To manage his condition and to respond to frequent flare ups, he visited the emergency department on a weekly basis for dressing changes and antibiotics, if needed. Wound dressings alone did not facilitate wound healing, with limb volumes and his wounds continuing to worsen, so it was decided that an intensive compression therapy programme would be initiated, with the main aims being to reduce lymphoedema and associated wound discomfort.
Clinical presentation lymphoedemaPatient X presented with extremely dry and scaly skin, and pitting on the lower legs and dorsal surfaces of both feet. The upper legs and knees seemed unaffected and bilateral positive Stemmer’s sign was present. Skin changes, hyper pigmentation on both lower limbs, papillomatosis on the base of the toes, and fibrotic tissue in the mid area of the tibia (bilateral) were also present. The limbs were categorised as stage III lymphoedema, as per International Society of Lymphology consensus (2009). There were no signs of neuropathy, despite the individual having diabetes.
Patient X is retired and resides with his
measurements being taken. The limb was then bandaged with Coban 2 Compression System, using the toe-boot application method (3M, 2011). Bandage slippage was monitored with a simple mark on the skin with a marker pen and measured with measuring tape upon return appointments. While applying bandages in the supine position, 42 mmHg–45 mmHg was required to reach the desired 50 mmHhg of under-bandage pressure when standing.
Site-specific tissue fluid was measured at anterior mid-thigh (15 cm proximal from patella), posterior mid-thigh (15 cm proximal from knee crease), and posterior lower limb (15 cm distal from knee crease). A bilateral dorsal site measurement was also taken (medium probe, 2.5 mm–5 mm in skin), 5 cm from the base of the toes using the MoistureMeter D.
ResultsTreatment with the Coban2 Compression System over 4 weeks significantly decreased Patient X’s total limb volume. During the active bandaging time (between baseline and final visit) limb volume as measured by the Perometer was reduced by 2.1 L in the left leg and 2.1 L in the right leg. The right leg increased in volume from week four to follow up by 0.4 L and the left leg increased by 0.1 L, which was expected as active intervention had ceased.
Lower extremity total volumes were calculated from the circumference measurements using the truncated cone formula; a limb volume reduction of 3.1 L in the left leg and 1.7 L in the right leg was observed. During the active bandaging period (4 weeks), the Bioimpedance Spectroscopy (InBody) measurement showed a reduction of 3.2 L in the left leg and 3.0 L in the right leg. At the follow-up appointment, further fluid reduction was measured, despite no active intervention (Patient X was wearing bilateral compression garments).
Multiple wounds were present bilaterally, on the distal posteriors of the lower limbs. At baseline, the left leg had a total wound size of 25.8 cm² and right leg was 29.7 cm². Patient X’s wound size reduced by 21.7 cm² in the left leg and 17.7 cm² in the right leg between baseline and final visit. It was observed at follow up (4 weeks post treatment) that no wounds were present on the left leg, while the right leg wounds had continued to decrease in size by 2.25 cm², giving a total reduction of 19.95 cm² (Figure 2).
The TEWL readings fluctuated during the taking of measurements. This could be due to
sibling. He explained he is very fond of computer games and can spend hours sitting on a computer chair without laying supine for a night’s rest.
Both legs had multiple wounds with excess yellowish-clear exudate. Granulation tissue was visible, but all wounds were covered with debris and showed signs of infection (Figure 1).
MaterialsPatient X’s lower legs were bandaged using a toe-boot application with the Coban 2 Compression System. This intervention was applied every second day for a duration of 4 weeks due to leakage of the wound areas.
The following bilateral duplicated measurements were obtained at every clinic visit:• Wound size and perimeter using a Visitrak
wound measurement grid (Smith & Nephew).
• Limb circumferences using a Perometer 350S (Pero-System Messgeräte) every 3.7 mm and a standard tape measure every 4 cm.
• Total body water (intracellular and extracellular), limb fluid volumes, fat and muscle masses using a whole-body Bioimpedance Spectroscopy Unit (InBody)
• Site-specific tissue fluid (MoistureMeter D; Delfin Technnologies).
• Undergarment pressure in supine position (Kikuhime; mediGroup) on the lateral side of lower limb, large probe.
• Transepidermal water loss (TEWL; VapoMeter).
• Tissue resistance using an indurometer (Flinders Biomedical Engineering).
• A quality of life questionnaire was also completed and photos taken (Keeley et al, 2010).
MethodsPatient X’s lower legs, including the feet and toes, were cleansed with lukewarm water and a surgical sponge (Medisponge, Filtrona Porous Technologies) and dried prior to all
Figure 1. Patient X’s legs at baseline in (a) anterior and (b) posterior views, and detailed images of the patient’s (c) left and (d) right leg wounds.
(a) (b) (c) (d)

Case report
26 Journal of Lymphoedema, 2013, Vol 8, No 2
the bandaging material being removed and cleansing of the legs before the measurements were taken. The authors waited for the skin to cool and dry, however, the lower limbs were often damp with perspiration. Higher TEWL readings in the right leg suggested a loss of barrier function. This was consistent with the authors’ prediction, as the wounds on the right leg were larger and harder to heal than those present on the left leg.
A 55% reduction in fluids in the superficial tissue of both calves (mean 34.4 units of calf area) was measured
be attributed to both the bandaging and the regular friendly contact of the authors. Patient X was compliant in wearing bandages throughout the 4-week treatment regimen. Although he reported some heat-induced discomfort at night, he found the bandages comfortable and noninvasive. ConclusionThe compression bandaging used in this case report proved effective in reducing Patient X’s lymphoedema fluids, subsequently resolving his wounds. The removal of this fluid is essential for wound healing. Early detection is crucial to prevent further progression in lymphoedema, including skin breakdown and the appearance of chronic wounds. Cost is often a factor for both patient and clinician in treatment options and bandaging may prove a more cost-effective intervention that may halt wound progression. Bandaging must be applied correctly, with the right pressure and pressure gradient, and adapted to each patient’s needs, including mobility, comfort, and cost.
References
3M (2011) Training Manual Lymphoedema Intensive Therapy. 3M Health Care, Australia
Agale SV (2013) Chronic Leg Ulcers: Epidemiology, Aetiopathogenesis, and Management. Available at: http://bit.ly/1b4akc5 (accessed on 27.11.2013)
Barker J, Weller C (2010) Developing clinical practice guidelines for the prevention and management of venous leg ulcers. Wound Pract Res 18(2): 62–71
Keeley V, Crooks S, Locke J et al (2010) A quality of life measure for limb lymphoedema (LYMQOL). Journal of Lymphoedema 5(1): 26–37
Lymphoedema Framework (2006) Compression Therapy: A Position Document on Compression Bandaging. International Consensus. MEP Ltd, London: 12–23
Milic DJ, Zivic SS, Bogdanovic et al (2010) The influence on different sub-bandage pressure values on venous ulcer healing when treated with compression therapy. J Vasc Surg 51(3): 655–61
Moffatt CJ, Franks PJ, Hardy D et al (2011) A preliminary randomized controlled study to determine the application frequency of a new lymphoedema bandaging system. British Journal of Dermatology 166(3): 624–32
Morgan PA, Murray S, Moffatt CJ, Young H (2011) The experience of patients with lymphoedema undergoing a period of compression bandaging in the UK and Canada using the 3M Coban 2 compression sytem. Int Wound J 8(6): 586–98
Muldoon J, Charles H (2013) Clinical effectiveness and patient considerations in oedema management. Journal of Lymphoedema 8(1): 51–2
Stücker M, Link K, Reich-Schupke S et al (2013) Compression and venous ulcers. Phlebology 28 (Suppl 1): 68–72
by MositureMeter D between baseline and final appointment. At the follow-up appointment it was noted that all fluid levels had increased again, which is to be expected given that the compression garment did not provide as high a pressure as the bandage did. A correlation was discovered between the thigh area measurement fluid increase and the indurometer data measured at baseline and follow up.
The indurometer showed a higher reading within the thigh areas, possibly indicating that fluid has been pushed up from the calf areas due to the compression bandaging and has made the upper-leg tissue softer. There were no significant indurometer findings at the other measurement sites (Figure 3).
Quality of life There was no change in Patient X’s quality of life score over the case study period, with the participant rating 8 on a scale of 10 (0 = no quality of life, 10 = highest quality of life; Keeley et al, 2010). However, at week four, he reported less difficulty in areas such as walking, bending, and undertaking housework, in comparison to baseline. Patient X also reported that the swelling did not affect how he felt about himself “at all” by week four, compared to “a little” at baseline.
Overall, the Patient X reported an increase in ease of living from baseline to week four. However, at follow up, his answers were similar to baseline. At follow up, Patient X marked the same subjective scale numbers as baseline, however, he commented that his quality of life had improved. Patient X had “enjoyed coming for appointments” and discussing lifestyle and daily events with the researchers. The increase in quality of life throughout the treatment phase could
Figure 2. Patient X’s (a) left and (b) right posterior leg wounds following 4 weeks’ treatment with the Coban™ 2 Compression System (3M).
Figure 3. Patient X’s legs at follow-up, (a) anterior and (b) posterior views.
(a)
(b)
(a) (b)

Instructions for authors
Journal of Lymphoedema, 2013, Vol 8, No 2 27
Journal of Lymphoedema welcomes submissions for publication in the following four categories:ReviewResearch and auditPractice development Case report
Title pageThe title page should include:Title of the article (approx. 10 words)The full names of the authorsFull details of each author’s current appointments
including place of workName, address, phone, fax and e-mail of the
corresponding author.
Abstract/SummaryThis is typeset in bold at the beginning of the article. As a general guide, articles in the Research/Audit section of the journal have abstracts, while those in the other sections (Practice developement/Review) have a summary.The Abstract should be no longer than 180 words
in length and should contain the following headings: Background, Aims, Methods, Results, Conclusions, Declaration of interest.
The summary should be a very concise (no more than 90 words) accurate statement that captures the reader’s interest by setting the scene for the article.
Both the Abstract and the Summary should enable the reader to understand the scope and main conclusions of the article without having to read the rest of the paper.
Word countFor all clinical articles, the word count (excluding title page, abstract/summary/tables) should not exceed 4000 words. Case reports should not exceed 2000 words and five references.
Short introductionThe introduction is designed to capture the reader’s interest by putting the article into the context of current clinical practice, quoting key references. It should also give the reader an idea of the objectives and contents of the paper. It should be clear and inviting.
MethodsFor papers describing original work (usually in the Research/audit section), a concise but informative account of all techniques (including statistical methods) used should be provided, in order to enable the reader to reproduce the work if necessary. Published/standard
methods can be referenced; detail is not necessary. However, variations to the published procedure should be described.
ResultsFor papers describing original work (usually in the Research/audit section), a comprehensive and clear description of results with tables, graphs, etc, is required. As well as presenting data in pictorial form, a narrative account should also be given, since the reader should not be expected to interpret results unaided. Where appropriate, statistical procedures should be used to indicate the variability of results and to test the significance of differences.
DiscussionPapers describing original work (usually in the Research/audit section), require a discussion. This should not be a repetition of results. It should summarise and interpret your conclusions and comment on their significance in light or what is already known from the literature. Identify Shortcomings in your work should be identified, and suggestions made as to what can be done to extend/confirm your findings.
ConclusionsFor all papers, the conclusion should be succinct and logically ordered. It should identify gaps in knowledge and suggest future initiatives.
HeadingsThroughout the article, please use plenty of headings to break up the text and to highlight the main points within the paper. Also remember to indicate the importance attached to each one.
Abbreviation and unitsSI units should always be used.
Key words and key pointsPlease provide five key words to appear at the start of your article, and 3–5 key point sentences that summarise the main themes of your paper.
Tables and illustrationsTables and illustrations are helpful to demonstrate key data or points to the reader. It is the author’s responsibility to ensure that permission is received for reproduction. Please do not supply more than 10 tables or 10 figures. Ensure tables and illustrations have a table heading and figure legend, and are cited in the text.
PhotographsNo more than 10 figures (photos should be provided as jpeg or tiff (300dpi), permission for reproduction is the author’s responsibility. All should have legends and should be clearly labelled, and cited in the text.
ReferencesJournal of Lymphoedema uses the Harvard system of referencing (names cited in the text). The number of references should not exceed 35.
In the reference list: References should be listed in alphabetical order. The surname and initials of each author should be
given in full for six or fewer authors; for seven or more, the names and initials of the first three should be given, followed by “et al”. The sequence for a journal reference is author(s), year, title, journal, volume, issue, page range.
Journals:Baker SR, Stacey MC, Jopp Mc Kay AG et al (1991) Epidemiology of chronic venous ulcers. Br J Surg 78(7): 864–7
Books:Goodman LS, Gillman A (1990) Goodman and Gillman’s the Pharmacologial Basis of Therapeutics (8th edn). McGraw Hill, New York, NY
Chapters in books:Saffle JR, Schnebly WA (1994) Burn wound care. In: Richard RL, Stanley MJ (eds) Burn Care and Rehabilitation: Principles and Practice. Davis Co., Philadelphia, PA: 137–9
SubmissionsPlease submit your manuscript online:http://www.epress.ac.uk/jol/webforms/author.php
For further more information, please email the Managing Editor, Lindsey Mathews [email protected]
Writing for the Journal of LymphoedemaJournal of Lymphoedema is a biannual peer-reviewed publication that aims to provide cutting-edge articles and information on the management of lymphoedema for all professionals working in lymphoedema care. Writing for publication in Journal of Lymphoedema can be a useful way to help develop and crystallize ideas about a specific topic, encourage exploration of an area in greater depth, and communicate novel findings to colleagues.

© Journal of Lymphoedema, a division of Schofield Healthcare Media Ltd1–2 Hatfields, London SE1 9PG, UKTel: +44 (0)20 7960 1510 Fax: +44 (0)20 7627 1570
No part of this journal may be reproduced or transmitted in any form, by any means, electronic or mechanic, including photocopying, recording or any information retrieval system, without the publisher’s permission.
www.woundsinternational/resource-centre/lymphoedema.com ISSN 1750-7235