
Journal Of Anesthesiology MP State Vol 1
37
ANAESTHESIOLOGY ANAESTHESIOLOGY M.P. M.P. Editor: Dr. Meenu Chadha Co-editor: Dr. Alok Biyani ? October 2015 Volume 1 ? ? issue 1
-
Upload
cardiacanesthesia -
Category
Documents
-
view
13 -
download
6
description
ISA MP State Chapter Journal of ANesthesiology journal of Madhya Pradesh State ISA Chapter Volume 1
Transcript of Journal Of Anesthesiology MP State Vol 1

ANAESTHESIOLOGY ANAESTHESIOLOGY ANAESTHESIOLOGYM.P.M.P.
Editor: Dr. Meenu ChadhaCo-editor: Dr. Alok Biyani
? October 2015 Volume 1 ? ? issue 1

Anaesthesiology M.P. 1
CONTENTSANAESTHESIOLOGY
M.P.
Dr. Meenu Chadha
Editorial - Pain Physican - Learning Dilemma
21
Dr. Anil K Sharma, Ann Maresca PA-C
Review Article - Chronic Spinal Pain - Diagnosis
32
Prof. Poonam Malhotra Kapoor
Nuances of Social Media in Medical Journalism
103
Dr. Neelima Tandon, Dr. Suman Gupta, Dr. Preeti Goyal,
Dr. Bhanu Choudhary
CASE REPORT - Commencement of Early and Uninterrupted Chest only Compression CPR is the Failsafe technique in Sudden Cardiac Arrest 134
CASE REPORT - Unusual Case of Consecutive Snake bite of three Persons
165
Dr Ashish Sethi, Miltan Debbarma, Neeraj Narang,Anudeep Saxena, Mamta Mahobia
Correlation of Goal- Directed Preoperative Optimization with Clinical outcone in Emergency Abdominal Surgery
196
Dr. Priya Shenwani, Dr. Pradeep Meshram, Dr. Neeraj Narang
CASE REPORT - Case of Uncorrected Tetralogy of Fallot Posted for closed reduction and Hip Spica Application for Fracture of Shaft of Femur 267
Dr. Meenu Chadha, Dr. Dharna Jain
CASE REPORT- Flexometallic Endotrachel Tubes Are They Really Safe?
298
Submission Guidelines
329
EDITOR
Dr. Meenu Chadha
CO-EDITOR
Dr. Alok Biyani
EDITORIAl BOARD
Dr. Mayank Kulshreshtha
Dr. Ashwin Soni
Dr. Suman Gupta
Dr. Ruchi Tandon
Dr. Ashish Sethi
Dr. Harsh Mangal
ADVISORS
Dr. T.C. Kriplani
Dr. V.M. Agnihotri
Dr. R.C. Agarwal
Dr. V.K. Joshi
Dr. M.M. Neema
Dr. Bhanu Ved
Dr. K.G. Vijayan
Dr. K.K. Arora
Dr. Shikha Mehrotra
Dr. Aditya Agarwal
Dr. Dilip Kothari
Dr. Sadhana Sanwatsarkar
Dr. Sudhakar Diwedi
Dr. Manorama Singh
Dr. Rajnish Jain
Dr. S.R. Lad
Dr. Maj USSV Meher, Gradee Specialist (Anesthesiology)
Chief Anaesthetist, Pain Physician & OT SuprintendentVishesh Hospital [email protected] 9977161035
ConsultantApollo Hospitals [email protected]

PAIN PHYSCIAN - LEARNING DILEMMAhe anaesthesiologist has played a primary role since beginning in pain Tmedicine. Late John J Bonica an anaesthesiologist was the first to develop his career
promoting multidisciplinary pain care and formal training of a specialist. The International
Association for the Study of Pain (IASP) was founded in 1974. Interventional pain medicine is evolving as a distinct discipline that requires detailed
knowledge and expertise. Familiarity with radiographic anatomy for image guided injections
and the minor surgical skills needed to implant devices such as spinal cord stimulators and
implanted delivery systems are just a few of the techniques that many of us have master for pain
management. To introduce new interventional techniques to our own pain practice, how can we
ensure that we have been properly trained to conduct these techniques with safety & success?
Adequate exposure to these newer interventions/treatment alternatives is certainly necessary
to ensure its appropriate application & to optimize patient outcomes. We do not have scientific
data to define the average minimum level of experience that will be needed to achieve
competence especially for complex procedures that are associated with significant risks. New techniques are evolving at a staggering rate & we cannot rely solely on pain training
programs to provide all the technical training needed. Higher standards for minimal training are
needed.So the question is where we do stand as pain practitioners. It is time that the parent body
helps in giving insights into formulating some protocols for starting pain practice. In the mean time few considerations that can be kept in the mind of the practitioners are
suggested below:- Study the new techniques- Thoroughly study the published literature to gain a detailed
knowledge of all aspects of the technique.Attend a workshop- Preferably a hands on cadaveric workshop that allows introduction to
the techniques in a realistic setting. Plan and give adequate time for your initial procedure Get help during the initial conduct of the procedure- perhaps another experienced
practitioner ,an invited expert or team up with a colleague in a related discipline.Inform your patients- In detail about the procedure as to what to expect and what would be
the probable outcomes and also obtain written consent for the same.Examine your outcomes- Careful self audit in the initial stages of using any new technique
and comparing them with those of your colleagues or published literature.Hippocratic oath” Primum non nocerum” i.e. First do no harm should be our goal.So need of the hour is that all pain physicians should be involved not only in research and in
publications, but in formulation of protocols for diagnosis, investigation and evidence based
treatment algorithm. Meenu Chadhal
Anaesthesiology M.P.2
E d i t o r i a l

1. President, Spine & Pain Centre NJ & NY. Director, Pain Management Monmouth Medical Centre NJ, USA.
2. Certified Physician Assistant.
Chronic Pain
Spinal Interventional Techniques
Chronic pain is defined as a pain that persists 6
months after an injury and/or beyond the usual
course of an acute disease or a reasonable time for
a comparable injury to heal. It is associated with
chronic pathologic processes that cause
continuous or intermittent pain for months or
years and may continue in the presence or
absence of demonstrable pathology and may not
be amenable to routine pain control methods with 2,7healing never occurring.
However, chronic pain must not be confused 7with chronic pain syndrome which is defined as a
complex pain condit ion with physical ,
psychological, emotional and social components.
While chronic pain and chronic pain syndrome
may appear similar and may at times coexist,
chronic pain syndrome encompasses the added
components of certain psychological ,
socioeconomic influences and psychological
behavioral patterns.
Chronic spinal pain is a complex and
multifactorial phenomenon. There is high
prevalence of chronic spinal pain and there are
numerous modalit ies of treatments in
management of the problem. Despite its
commonality, both in primary care and tertiary
care, it is often difficult to reach a definite diagnosis
of the origin of spinal pain. Interventional Pain
Management techniques are based on the
philosophy of a neurophysiologic and anatomical
basis, in that when present, a structural origin of
pain is important and blocking that structure with
an anesthetic will relieve the pain. A major source
of growth in treatment modalities and their failure
is because of lack of accurate diagnosis. In the
absence of accurate diagnosis, treatment fails
resulting in wasted health care dollars, and
diversion of essential health care resources.
Fundamental to proper treatment is accurate
diagnosis, which is based on the reliability of the
test used to make the diagnosis. There are no
universally accepted gold standards for the
diagnosis of spinal pain, regardless of the 1,2,3,4,5,6,7,8,9,10suspected source. . Controlled studies
have established intervertebral disc, facet joints,
and sacroiliac joints as potential sources of low 2,3,4,9,11,12,13,28back pain. Accurate diagnosis can be
17made by interventional techniques in diagnosing
the source of pain due to intervertebral discs, facet
joints and sacroiliac joint . For some patients there
can be multiple pain generators.
Based on history, physical examination,
imaging, and nerve conduction studies in non-
radicular pain, a precise cause of pain may be
Controlled Diagnostic Injection Techniques
CHRONIC SPINAL PAIN- DIAGNOSIS
l 1 2Dr. Anil K Sharma Ann Maresca PA-C
Anaesthesiology M.P. 3
REVIEW ARTICLE

identified in only approximately 15% of patients.
However, it has been described that with
application of controlled diagnostic interventional
techniques, a diagnosis may become a reality in 3,4,5, 6,9,14,1585% of the patients rather than 15%.
In order to determine the pathophysiology of
clinical pain, the site of nociception, and the
pathway of afferent neural signals, precision
diagnostic blocks are utilized. Provocation
discography, sacroiliac joint injections, and facet
joint injections are part of the armamentarium of
diagnostic techniques with proven accuracy.
Controlled diagnostic blocks have a theoretical
basis that if a patient has legitimate pain from a
specific targeted structure, complete or near
complete relief of that particular pain should be
obtained consistently whenever that structure is
anesthetized. Accuracy can be obtained by
repeating the diagnostic block with different
anesthetizing agents, rendering a consistent
response.
For a diagnostic block to have face validity it
must be shown that the block actually does what it
is supposed to do in an anatomical and a 15, 16physiological sense. The targeted structure
must be proven to have been anesthetized and
that a documented result was either produced or
not produced. Face validity can be tested and
established either by a study whose results can be
replicated in each and every case. Other options to
establish face validity are injecting a contrast
agent utilizing radiographic imaging or by a
physiological approach utilizing a detectable and
testable function other than pain, such as distal
extremity temperature monitoring with a
sympathetic block.
Construct validity establishes if the test
actually achieves what it is supposed to achieve by
measuring the extent to which a test correctly
distinguishes the presence, but also the absence,
of the condition that the test is supposed to detect.
Construct validity measures if the test actually 15,16works or not, and how well it works.
There is no standard criterion for diagnostic
interventional techniques, such as imaging
findings, operative findings, or pathological
findings. For certain types of blocks, long-term
relief, however, may be used to provide standard 15criterion. Thus, Bogduk has developed testing for
construct validity of diagnostic blocks by other
means. Features such as the false-positive rates
can be estimated by determining how often a
diagnostic block is positive in patients who should
not, or demonstrably do not, have the condition in
question. Once the false- positive rates are known,
the specificity of the test can be derived as the
complement of the false-positive rates.
A protocol requiring a series of three blocks
utilizing a placebo may be utilized as one form of
control. The first block must involve an active
agent, in order to establish that the targeted
structure was indeed the pain generator. The other
2 agents are administered on a randomized
double-blind basis. Given these conditions, a true-
positive response would be yielded on every
occasion the active agent was used and no
response when the inactive agent was used.
A second approach, most commonly utilized in
the United States because it is also a more
pragmatic approach, is to use comparative local
anesthetic blocks. The blocks are performed on
separate occasions using local anesthetic agents 15,16,17with different durations of action. The
consistency and duration of the response are
tested in this approach. Inconsistency is
established if there is failure to respond to the
second block, thus indicating a false positive with
the first block. A positive response occurs if the
response is concordant with the expected duration
of action of the anesthetizing agent.
Anaesthesiology M.P.4

discography screening can decrease the number of
unnecessary operations. The discrepancy in
opinions is based on the lack of positive outcomes
with surgical interventions for discogenic pain.
Proponents of discography also argue that it is
the only diagnostic modality that attempts to
correlate pathology with symptoms. This point is
reasonable given the fact that close to two-thirds
of asymptomatic subjects have been found to have
abnormal findings on MRI and CT scans of their 16,18,27lumbar spines, As a means to reduce the high
false-positive rates associated with provocation
discography in certain subgroups, the use of
anesthetic discography has recently generated
significant interest.
The evidence for provocation discography is
fair. Due to ongoing debate on the accuracy of this
test and the lack of outcome parameters in
patients undergoing surgical interventions, the
evidence is subject to other interpretation. There is
limited evidence supporting functional anesthetic
discography.
Lumbar facet joints are pairs of joints that
stabilize and guide motion in the spine. Lumbar
facet joints are a well-recognized source of low
back and referred pain in the lower extremity
above the knees in patients with chronic low back 2, 3, 11, 12, 13, 28pain. Facet joints are innervated by the
3medial branches of the dorsal rami.
Degenerative spinal changes observed on
radiologic imaging studies, including radiographs,
MRI, CT scanning, single photon emission
computed tomography (SPECT), and radionuclide 28, 30, 31bone scanning are common and do not point
out to a specific pain generator. There is ongoing
debate about whether there is association
between degenerative changes in the lumbar facet
joints and symptomatic low back pain.
Lumbar Facet Joint Pain
Diagnosis of Chronic Low Back Pain
Diagnostic Selective Nerve Root Blocks
Lumbar Discography
Lumbosacral selective nerve root blocks
and/or transforaminal epidural injections are used
for the diagnosis and treatment of different
disorders causing lower extremity pain: however,
a clear consensus on the use of selective nerve
root injections as a diagnostic tool does not 6,20currently exist. Though, if a particular spinal
nerve is thought to be responsible for causing or
mediating a patients' symptoms, then
theoretically anesthetizing that nerve should
provide temporary pain relief, thereby creating
the rationale behind the diagnostic spinal nerve
block. Based on the present comprehensive 6,21,22evaluation of the available literature,
diagnostic selective nerve root blocks may be
recommended with limited evidence.
Discography is a procedure that is used to
characterize the pathoanatomy/architecture of
the intervertebral disc and to determine if the
intervertebral disc is a source of chronic low back 23pain. Basic and clinical studies have shown that
the lumbar discs are innervated and can be a 24source of pain.
Chronic low back pain patients with suspected
discogenic etiology, who are willing to consider
surgery and other less invasive options should be
the only patient population considered for this
invasive diagnostic test. There is data that it can
accelerate the degenerative process as well as can
cause herniation, so this should not be performed
just to find the pain generator.
Opponents of discography contend that
escalating numbers of unnecessary fusions have
been performed in the United States each year for 25,26indications of discogenic pain. However,
proponents argue that when properly utilized,
Anaesthesiology M.P. 5

Standard clinical features and examination are
unreliable in diagnosing lumbar zygapophysial
(facet) joint pain. For the diagnosis of low back
pain, there is no universal gold standard, no
matter what the suspected source, i.e. facet
joint(s), intervertebral disc(s), or sacroiliac joint(s).
Controlled local anesthetic blocks continue to be
the best available tool to identify facet joint(s), or
sacroiliac joint(s) as the source of low back pain.
Controlled diagnostic blocks of a lumbar facet or
zygapophysial joint can be performed by
anesthetizing the medial branches of the dorsal
rami that innervate the target joint, (keeping in
mind that 2 nerves have to be blocked for each
joint). The false-negative rate of diagnostic facet
joint blocks was shown to be 8% due to
unrecognized intravascular injection of local 29anesthetic. The gold standard would include a
placebo-controlled technique, but due to cost
implications and to the ethical and logistical issues
of designing a true placebo, there is limited clinical
utility for this technique.
There was only one study evaluating 50% to 74%
relief as criterion standard with a single block 12showed the prevalence of 48%, 4 studies
evaluated 75% to 100% relief as the criterion
standard with a single block showed a prevalence of 32,3331% to 61%, 5 studies evaluated 50% to 74%
relief as the criterion standard with controlled
diagnostic blocks with the prevalence of 15% to 33 1361%, and studies evaluated 75% to 100% relief as
the criterion standard with controlled blocks with a
prevalence of 25% to 45% in heterogeneous 13,19,34,35 populations. The evidence is good for
utilization of 75% to 100% pain relief with
controlled diagnostic blocks as the criterion
standard with a prevalence of 25% to 45%.
The sacroiliac joint is accepted as a potential
source of low back and /or buttock pain with or
Sacroiliac Joint Pain
13,36without lower extremity pain. The sacroiliac
joint receives innervation from the lumbosacral
nerve roots. There is no universally accepted gold
standard for the diagnosis of low back pain
originating from the sacroiliac joints. A
combination of provocative manipulations tends
to be useful in localizing the sacroiliac joint as the
pain generator for patients with symptoms below
the fifth lumbar vertebra.
38,39The sacroiliac joint is well-innervated with
nociceptors and proprioceptors, even though the
pattern of innervation is the subject of much
controversy. There are no non-invasive tests to
make the diagnosis of sacroiliac joint-mediated
pain, sacroiliac joint blocks appear to be the
evaluation of choice.
There were 2 studies evaluating 50% to 74% 41,44relief with dual blocks. the prevalence of SI joint
pain was 38% with 50% relief and 26.6 % with 70%
relief.
There were a total of 8 studies meeting the
inclusion criteria evaluating sacroiliac joint pain
using a cutoff threshold between 75% and 100% 12,37,40,42,43relief following a single block. The
prevalence in this group ranged from a low of 10%
to a high of 62%.
There were a total of 7 studies meeting the
inclusion criteria with 75% to 100% relief with dual 10,13 blocks, Using the 75% and 100% pain relief with
dual blocks as the criterion standard the
prevalence ranged from 10% to 44.4% and has
been advocated by some as the most rigorous 2, 28means for diagnosing sacroiliac joint pain.
1. Manchikanti L, Singh V, Bakhit CE Fellows B.
Interventional techniques in the management
of chronic pain. Part 1.0. Pain Physician
2000:3:7-42.
2. Manchikanti L, Bosell MV, Singh V, Benyamin
References
Anaesthesiology M.P.6

RM, Fellows B, Abdi S, uenaventua RM, Conn
A, Datta S, Derby R, Falco FJE, Erhart S, Diwan
S, Hayek SM, Helem S, Parr AT, Schultz DM,
S m i t h H S , Wo l fe r L R , H i r s c h J A .
Comprehensive evidence-based guidelines
for interventional techniques in the
management of chronic spinal pain. Pain
Physician 2009:12:699-802.
3. Falco FJE, Manchikanti L, Datta S, Sehgal N,
Geffert S, Onyewu O, Singh V, Bryce DA,
Benyamin RM, Simopoulos TT, Vallejo R,
Gupta S, Ward SP, Hirsch JA. An update of the
systematic assessment of the diagnostic
accuracy of lumbar facet joint nerve blocks.
Pain Physician 2012;15:E869-E907.
4. Falco FJE, Datta S, Manchikanti L, Sehgal N,
Geffert S, Singh V, Smith HS, Boswell MV. An
updated review of diagnostic utility of
cervical facet joint injections. Pain Physician
2012;15:E807-E838.
5. Atluri S, Singh V, Datta S, Geffert S, Sehgal N,
Falco FJE. Diagnostic accuracy of thoracic
facet joint nerve blocks: An update of the
assessment of evidence. Pain Physician
2012;E483-E496.
6. Datta S, Manchikanti L, Falco FJE, Calodney
AK, Atluri S, Benyamin RM, Buenaventura R,
Cohen SP. Diagnostic utility of selective nerve
root blocks in the diagnosis of lumbosacral
radicular pain: Systematic review and update
of current evidence. Pain Physician
2013;16:SE145-SE172.
7. Manchikanti L, Singh V, Datta S, Cohen SP,
Hirsch JA. Comprehensive review of
epidemiology, scope, and impact of spinal
pain. Pain Physician 2009:12:E35-E70.
8. Centers for Disease Control and Prevention.
CDC grand rounds: Prescription drug
overdoses- a U.S. epidemic. MMWR Morb
Mortal Wkly Rep 2012;61:10-13.
9. Manchikanti L, Datta S, Derby R, Wolfer LR,
Benyamin RM, Hirsch JA. A critical review of
the American Pain Society clinical practice
guidelines for interventional techniques: Part
1. Diagnostic interventions. Pain Physician
2010; 13:E141-E174.
10. Laplante BL, Ketchum JM, Saullo TR, DePalma
MJ. Multivariable analysis of the relationship
between pain referral paterns and the source
of chronic low back pain. Pain Physician
2012;15:171-178.
11. Hancock MJ, Maher CG, Latimer J, Spindler MF,
McAuley JH, Laslett M, Bogduk N. Systmatic
review of tests to identify the disc, SIJ or facet
joint as the source of low back pain. Eur Spine J
2007;16:1539-1550.
12. Pang WW, Mok MS, Lin ML, Chang DP, Hwang
MH. Application of spinal pain mapping in the
diagnosis o flow back pain- analysis of 104
cases. ActaAnasthesiol Sin 1998;36:71-74.
13. Manchikanti L, Singh V, Pampti V, Damron K,
Barnhill R, Beyer C, Cash K. Evaluation of the
relative contributions of various structures in
chronic low back pain. Pain Physician
2001;4:308-316.
14. Bogduk N. Principles of diagnostic blocks. In:
Slipman C, Derby R, Simeone FA, Mayer
TG(eds). Interventional Spine: An Algorithmic
Approach. Saunders Elsevier, Philadelphia,
2008, pp 187-192.
15. Bogduk N. On diagnostic blocks for lumbar
zygapophysial joint pain. F1000 Med Rep
2010;2:57.
16. Derby R, Lee SH, Lee JE, Lee Sh. Comparison of
pressure controlled provocation discography
using automated versus manual syringe pump
manometry in patients with chronic low back
Anaesthesiology M.P. 7

pain. Pain Med 2011;12:18-26.
17. Buckley FP. Regional anesthesia with local
anesthetics. In: Loeser JD (ed). Bonica's
Management of Pain. 3rd Edition. Lippincott
Williams & Wilkins, Philadelphia, 2001, pp
1893-1952.
18. Jarvik JG, Hollingworth W, Heagerty PJ,
Haynor DR, Boyko EJ, Deyo RA. Three
yearincicence of low back pain in an initially
asymptomatic cohort: Clinical and imaging
risk factors. Spine (Phila Pa 1976)
2005;30:1541-1548; discussion 1549.
19. Manchikanti L, Manchukonda R, Pampati V,
Damron KS, McManus CD. Prevalence of facet
joint pain in chronic low back pain in
postsurgical patients by control led
comparative local anesthetic blocks. Arch
Phys Med Rehabil 2007;88:449-455.
20. Shah RV. The problem with diagnostic
selective nerve root blocks. Spine(Phila Pa
1976) 2012;37:1991-1993.
21. VanAkkerveeken PF. The diagnostic value of
n e r v e r o o t s h e a t h i n f i l i t r a t i o n .
ActaOrthopScandSuppl 1993;251:61-63.
22. Yeom JS, Lee JW, Park KW, Chang BS, Lee CK,
Buchowski JM, Riew KD. Value of diagnostic
lumbar selective nerve root block: A
prospective controlled study. AJNR Am J
Neuroradiol 2008; 29: 1017-1023.
23. Kuslich SD, Ulstrom CL, Michael CJ. The tissue
origin of low back pain and sciatica: A report
of pain response to tissue stimulation during
operation on the lumbar spine using local
a n e st h e s i a . O r t h o p C l i n N o r t h A m
1991;221:181-187.
24. Freemont AJ, Peacock TE, Goupille P,
HoylandJA , O'Brien J, Jayson MI. Nerve
ingrowth into diseased intervertebral disc in
chronic back pain. Lancet 1997;350:178-181.
25. Madan S, Gundanna M, Harley JM, Boeree NR,
Sampson M. Does provactive discography
screening of discogenic back pain improve
surgical outcome? J Spinal Disord Tech
2002;15:245-253.
26. Maghout-Juratli S, Franklin GM, Mirza SK,
Wickizer TM, Fulton-Kohe D. Lumbar Fusion
outcomes in Washington state worker's
compensation. Spine (Phila Pa 1976)
2006;31:2715-2723.
27. Takatalo J, Karppinen J, Niinimaki J, Taimela S,
Nayha S, Jarvelin MR, Kyllonen E, Tervonen O.
Pervalence of degenerative imaging findings
in Lumbar magnetic resonance imaging
among young adults. Spine (Phila Pa 1976)
2009;34:1716-1721.
28. DattaS, LeeM,Falco FJE, BryceDA, HayekSM.
Systematicassess ment of diagnostic accuracy
and the rapeuticutility o£ luinbarfacetjoint
interventions. Pain Physician 2009;12:437-
460.
29. Dreyfuss P, Schwarzer AC, Lau P, Bogduk N.
Specificity of lumbar medial branch and L5
dorsal ramus blocks. Spine(Phila Pa 1976)
1997;22:895-902.
30. Makki D, Khazim R, Zaidan AA, Ravi K, Toma T.
Single photon emission computerized
tomography (SPECT) scan positive facet joints
and other spinal structures in a hospital-wide
population with spinal pain. Spine J
2010;10:58-62.
31. De Maeseneer M, Lenchik L, Everaert H,
Marcelis S, Bossuyt A, Osteaux M, Beeckman
P. Evaluation of lower back pain with bone
scintigraphy and SPECT. Radiographics
1999;19:901-912; discussion 912-914.
Anaesthesiology M.P.8

32. Revel ME, Listrat VM, Chevalier XJ, Dougados
M, N'Guyen MP, Vallee C, Wybier M, Gires F,
Amor B. Facet Joint block for low back pain:
Identifying predictors of a good response.
Arch Phys Med Rehabil 1992;73:824-828.
33. Manchikanti L, Pampati V, Fellows B, Baha A.
The inability of the clinical picture to
characterize pain from facet joints. Pain
Physician 2000;3:158-166.
34. Laslett M, Oberg B, Aprill CN, McDonald B.
Zygapophysial joint blocks in chronic low back
pain: A test Revel's model as a screening test.
BMC MusculoskelatalDisord 2004;5:43-48.
35. Laslett M, McDonald B, Aprill CN, Tropp H,
Oberg B. Clinical predictors of screening
lumbar zygapophysia l jo int blocks:
Development of clinical prediction rules.
Spine J 2006;6:370-379.
36. Kennedy DJ, Shokat M, Visco CJ. Sacroiliac
joint and lumbar zygapophysial joint
corticosteroid injections. Phys Med
RehabilClin N Am 2010;21:835-842.
37. Schwarzer AC, Aprill CN, Bogduk M. The
sacroiliac joint in chronic low back pain. Spine
(Phila Pa 1976)1995;20:31-37.
38. Cohen SP, Chen Y, Neufeld NJ. Sacroiliac joint
p a i n : A co m p re h e n s i ve rev i ew o f
epidemiology, diagnosis and treatment.
Expert Rev Neurother 2013;13:99-116.
39. Vilensky JA, O'Connor BL, Fortin JD, Merkel GJ,
Jimenez AM, Scofield BA, Kleiner JB. Histologic
analysis of neural elements in the human
sacroiliac joint. Spine (Phila Pa 1976)
2002;37:1202-1207.
40. Dreyfuss P, Michaelsen M, Pauza K, Mclarty J,
Bogduk N. The value of medical history and
physical examination in diagnosising sacroiliac
j o i nt p a i n . S p i n e ( P h i l a Pa 1 9 7 6 )
1996;21:2594-2602.
41. Van der Wuff P, Buijs EJ, Groen GJ. A multitest
regimen of pain provocation tests as an aid to
reduce unnecessary minimally invasive
sacroiliac joint procedures. Arch Phys Med
Rehabil 2006;87:10-14.
42. Slipman CW, Sterenfeld EB Chou LH, Herzog R,
Vresilovic E. The value of radionuclide imaging
in the diagnosis of sacroiliac joint syndrome.
Spine (Phila Pa 1976) 1996;21-2251-2254.
43. Laslett M, Aprill CN, McDonald B, Young SB.
Diagnosis of sacroiliac joint pain: A validity of
individual provocation tests and composites
of tests. Man Ther 2005;10:207-218.
44. Irin RW, Watson T, Minick RP, Ambrosius WT.
Age, body mass index, and gender differences
in sacroiliac joint pathology. Am J Phys Med
Rehabil 2007; 86:37-44.
Anaesthesiology M.P. 9

1. Department of Cardiac Anaesthesia, CNC, AIIMS, New Delhi
NUANCES OF SOCIAL MEDIA IN MEDICAL JOURNALISM *
l 1Prof. Poonam Malhotra Kapoor
o one in today's era of technology wants to be
belonging to past dawns, but wants to move Nahead to the noon of the future. Today, social
media is being used aggressively by medical
publishers to promote knowledge, spread ideas
and create platforms, where they can
communicate their message. Social media helps
guide them to create discussions amongst
colleagues and across the globe on latest topics in
their fields of medicine. It helps journals increase
their scope by broadening the readership with a
larger population viewing the recent journal
articles. Social media has seen rapid growth in
popularity in the last few years. There is
widespread use of sites such as facebook and
twitter amongst medical journals and a growing
number of well-established blogs and internet
forums that are aimed specifically at medical
journals such as that for Circulation, British
Medical Journal, New England Journal of Medicine,
Lancet, JCVA etc. Cobwebbed, by the desires to
reach the masses, most established as well as
upcoming journals, put their best foot forward and
leave no stone unturned in putting the journal
articles for enhanced viewership. None of them,
but don't realize that further down, there is a trap! !
In promoting the journal, we are spending time,
energy, money to be seen online and stay hooked
on to the social media for very fast journal article
updates! But, are we gaining or loosing?
THE PROS OF SOCIAL MEDIA
Explosion of Social Media
It's hard to oppose the social media blitzkrieg
adoption of newer technology all of which are
great drivers of change in medicine. Social Media
is one such technology which has had a massive
effect on making die world increasingly shrink to
become a hub of global knowledge reach more
people and increase readership. This makes us all
medical professionals across the world, sail in the
same boat of social, international knowledge but
which is not without paradoxes! It's hard to
oppose the social media storm, but we need to
focus at least half as much attention on a quietly
worsening viewership crisis!!
The online information environment has
evolved from a world in which users searched
information (web 1 .0) to a world where they are
now able to generate and spread information
themselves (web 2.0). This has shifted the focus
from content-centric to user-centric information
environment, leading to no explicit direction of
information flow, with the reader interacting
through social media with all three namely the
sources, the medium and importantly with each
other and leading to no contact with the direct
supplier!!
A lot of work by the researchers needs to
frame the implications of the explosion of new
REPUBLICATION
* From Annals of Cardiac Anaesthesia ISSN 0971-8561/Volume18/Issue3.
Anaesthesiology M.P.10

social media and web technologies in the specific
context of risk and benefit to the journal status.
It is important at all times to be aware of the
journals online image and how it can impact its
professional standing.
Social media applications like Facebook.
Twitter. Linkedln. and Youtube are extremely
popular and its use is growing exponentially
[Figure I]. However, it is time-consuming. It has
replaced human meetings and behavior and
interactions. Thus, though being online is an
advertisement, it has led to the offline basic
intricacies woven around human emotions and
bonds going for a toss! "Googling emotions" and
"sharing them online" is weakening human
bonds, and one shudders that the "hard copy"
replaced by a "soft copy" of the journal, brings
about a fission of fear of deterioration in "active
journal" reading without a "hardcopy" in hand.
The budget being used while putting a
medical journal on social media is of utmost
importance. Dr. Ryan in a Google interview on 1"The scope" said about the famous journal
Circulation going on the Facebook and Twitter
with the aim of improving the scope of readership
that most readers felt that a low budget strategy
was not a good platform to read an article. An
article may be hit by thousands, but read only by a
few tweets. The viewers get the message, but the
primary article as it is, is safely stored in their
phones and never read!! And the journal has
spent effort and money to put it on the phone!
Social media opens the era of citizen and
collaborative journalism, wherein professional
journalism can both create new medical news
collaboratively and interactively with the public,
THE CONS OF SOCIAL MEDIA
THE CONS OF SOCIAL MEDIA
SOCIAL MEDIA - A PARADOX
but it also uses the latter as "feat - on the streets"
eye - witness reporters, whether it is with social
bookmarking or twitters hash-tags! Effective
social media communication requires clear
identification and thorough understanding of the
target audiences. It needs appropriate
management of information provision, so that it
optimally enhances the journals status amongst
the readers.
2The American Medical Association and the 3Federation of State Medical Boards provide basic
instructive guidelines for the use of social media,
in which it emphasizes the need to protect patient
privacy and confidentially and to maintain a
professional journalism discipline. It is imperative
for a medical journal to keep professional and
personal activity separate. Facebook users have
no control over what the readers may post about
them! It is important to remain within their
professional ethics and discipline to enhance its
image.
A personal and professional touch to the social
media campaign is required for all "online
MAINTAIN PROFESSIONAL BOUNDARIES ON
SOCIAL MEDIA
FUTURE CHALLENGES IN MEDICAL JOURNALISM
USE OF SOCIAL MEDIA
Figure 1: Networking of social media application
Anaesthesiology M.P. 11

important to establish dual online identities, to
separate personal and professional identities.
An evolved and ethical use of social media will
take medical journalism UP Sky High for as told by
Buddha "Thousands of candles can be lighted from
a single candle, but the life of a candle will not be
shortened."
Medical education shared on social media too
is like the candle that never decreases by being
shared.
1. Dr. Ryan. Health care insider: Surprising
findings from a study about using social media
to promote journal article. An Interview.
2. http://www.ama-assn.org /ama/ pub /
physician-resources / medicalethics / code-
medical-ethics / opinion9124.
3. Model Policy Guidelines for the Appropriate
Use of Social Media and Social Networking in
Medical Practice. Federation of state medical
boards, http://www.fsmb.org/ pdf/pub-
social-media-guidelines.pdf.
4. https://www.wsma.org/Media/Legal-pdfs /
Social_media_WSMA % 20 Statement _
20130821 .pdf.
5. Leiker M. When to "friend" a patient: Social
media tips for health care professionals. WMJ
2011;110: 42e3.
REFERENCES
success" without a personal face to it. Instant
interaction with the "reader's online queries"
whether on the blog or on a tweet is the need of
the hour. Engaging the readers in a journal
accounts conversation involving multiple
organizations helps bring more authors to spread
more research knowledge and take it up also on
public health issues. Involving the public is
important Researches in medical fraternity must
be explained to the masses through social media.
All this is what will make medical journalism savvy 4on the social media.
The mannerism in which one delivers the PDF
on the gadgets is important too! Lengthy pages,
small fonts are not the preferred technique by the
viewers. What is seeked in an article is
minipodcasts through brief interviews, short video
commentaries or through infographics as well.
Most readers follow only much evolved strategies
on social media and most of them, may read the
journal online or in the mailbox. This paradox is
challenging.
Awareness and interest in social media, though
it has hit medical journalism like a bulwak in recent
years, is still in its infancy. A prompt call for social
media guidelines to prevent unprofessional
content and breaches in patient confidentiality is
the need of the hour. Further research is essential
to harmonise the ethical aspects of clinical
manuscripts, being seen on Facebook and other 5sites, for which as suggested by Leiker et al., it is
CONCLUSION
Anaesthesiology M.P.12

1. Associate Professor Dept. of Anaesthesiology GRMC, Gwalior
2. Assistant Professor Dept. of Anaesthesiology GRMC, Gwalior
3. Associate Professor Dept. of Anaesthesiology GRMC, Gwalior
4. Professor & Head Dept. of Anaesthesiology GRMC, Gwalior
COMMENCEMENT OF EARLY AND UNINTERRUPTED CHEST ONLY
COMPRESSION CPR IS THE FAILSAFE TECHNIQUE IN SUDDEN CARDIAC
ARRESTl
1 2 3 4Dr. Neelima Tandon , Dr. Suman Gupta , Dr. Preeti Goyal Dr. Bhanu Choudhary ,
Case Report
Abstract:
Introduction:
Cardiopulmonary resuscitation is a versatile
term which encompasses so many techniques
which are updated every five years by the American
Heart Association. When suddenly confronted to
do so, it storms one's brain before we actually put
in efforts to do so because of complexity of its steps
and urgency to execute it immediately without
delay for it to be effective. Chest compressions are
the good means to maintain blood flow to victims
brain, heart and other vital organs .Here we
illustrate a true life story of how an out of hospital
cardiac arrest was managed by chest compression
CPR only.
Cardiac arrest is a condition in which the heart 1abruptly stops pumping blood. A Standard
cardiopulmonary Resuscitation (CPR) involves
alternating chest compression with rescue
breathing. For >50 years this combination of chest
compression and rescue breathing has been a 2 standard CPR.
Out of Hospital Cardiac arrest is a major public
health problem, affecting approximately 300,000 3individuals in the united states annually
In India-no definite survey been carried out to
reveal data related to cardiac pulmonary
resuscitation.
It's a great horror when you self visualizes a
faint of heart .At such times, it is better to do some
CPR rather than doing nothing, even if you are not
trained or certified provider .We need to alter the
mind set of trained personnel as well as layman
that chest only compression CPR (COCCPR) can be
executed by anybody whom so ever witnesses
circumstances of sudden cardiac arrest.
Here we report a real life incidence of sudden
cardiac arrest , revived as a result of only chest
compression CPR . A 74 years elderly woman was
about to retire to bed. Suddenly she grumbled
loudly that the bystander rushed to her and found
her to be unresponsive bystander. Bustander being
anaesthesiologist tried to palpate carotid but
failed. Mouth to mouth was difficult as she was
edentulous. She Immediately bared her chest and
Case –report
Anaesthesiology M.P. 13

Discussion-
Multifactorial efforts have been launched to
encourage bystanders to use compression only
CPR (COCCPR) because this approach is easier to
teach ,learn, remember and perform than
conventional CPR with rescue breathing. There are
multiple reasons of COCCPR being advantageous
over conventional CPR technique, including the
rapid deterioration of blood flow that occurs
during even with brief disruptions of chest
compressions, the long ramp up time to return to
adequate blood flow after resuming chest
compression, the complexity of conventional CPR,
the significant time required to perform the
breaths and the critical importance of cerebral and 4coronary circulation during arrest.
When a person has a cardiac arrest because of a
cardiac cause , such individual normally has plenty
of oxygen reserve in the body, thus rescue
breathings aren't as vital to survival as trying to 5keep blood flowing as regularly as possible.
Studies comparing survival rates of cardiac arrest
victims in the light of the kind of rescue efforts
performed by the bystanders has concluded that
chances of leaving the hospital alive were actually 6higher for patients who received COCCPR.
Rescue breathing is so difficult to perform that 7it can interrupt chest compressions. Minimizing
interruptions in chest compressions during
resuscitation attempts by bystanders might be
associated with increase in survival compared with 8conventional CPR. The reduction in venous return
during positive pressure ventilation also can be
associated with a worse outcome in those 9receiving conventional CPR.
Thus for a successful continuous –chest
–compression CPR, a certain steps can be followed 11as shown in the Table
started chest compression hard and fast
simultaneously calling for help ,knowing that it
might take several minutes for help to arrive. Only
chest compression CPR was continued, without
interrupting it for any period of time; until they
reached Intensive Care Unit (ICU) and continued
thereafter also. In ICU trachea was intubated and
ventilation started with 100 % oxygen with
continuing Chest Compression. All the routine
investigations as per ICU Protocol were done
(Arterial Blood Gases , Cardiac markers, Hbgm%,
Total Count, Serum Urea, Creatinine ,blood sugar
etc.).Monitors i.e. Electrocardiogram(ECG) ,Non
invasive blood pressure ( NIBP), Pulse oximeter (
SpO2) were applied and it revealed Asystole in
ECG. Immediately Inj. Adrenaline 1:1000 dilute in
10 ml Normal Saline was administered
intravenously without interruptions of chest
compressions in subsequence she had ventricular
fibrillation following which heart was shocked
with 120 joule biphasically along with CPR. Forty
five minutes elapsed till now, finally she reverted
back to sinus rhythm with occasional Ventricular
prematures contractions (VPC's ) per minute.
Inj.Amiodarone was administered 300 mg I.V
bolus followed by its infusion. She was kept on
ventilator for next two days with supportive
treatment with vasopressors. Slowly she was
weaned off and shifted to High dependency unit
(HDU) for next 5 days for observation and
discharged thereafter. Echocardiography shows
extensive anterior wall Myocardial Infarction with
EF 25% , akinetic and regional wall abnormality.
Coronary angiography done after a month showed
blockade in proximal LAD 80% , Distal LAD 50-60%
and RCA plaque. Stenting was done as mode of
treatment .Now she is asymptomatic and actively
doing her day to day activities . Hence chest
compression only CPR turned out to be the Best
CPR than conventional CPR to help victims of
sudden cardiac arrest.
Anaesthesiology M.P.14

Table 1. Steps for Continuous Chest
Compression CPR
Conclusion:
1. Call for help on 108 by yourself or ask someone
to do the same.
2. Position the patient on the floor ,face up. Bare
patient chest . Place the heel of one hand on the
center of the chest with the heel of the other
hand on top of the first .Lock your elbows so
that your arms are straight. Position your
shoulders directly above the center of the
patient's chest and fall so that the weight of
your upper body compresses the patient's
chest . Perform fast , forceful chest
compressions at more than 100/ min,
compressing the chest 1.5 to 2 inch. Allow time
for decompression
3. If an automated external defibrillator is
available ,open the patient's shirt and attach
the pads to the skin in the positions indicated
on the automated external defibrillator and
follow the machine's voice instructions .Keep
interruptions of chest compressions to a
minimum.
Hence COCCPR is easy to teach, learn, 7 ,10remember and perform But in our clinical
perspectives , there is nothing like all in one law
in most of the cases where lack of oxygen is the
primary cause of respiratory arrest like drug
overdose, alcohol intoxication, carbon
monooxide poisoning, severe asthma attack
,drowning, choking, conventional CPR with
mouth to mouth breathing remains the 1appropriate rescue technique.
We conclude that COCCPR is more effective
over conventional CPR in conditions of cardiac
arrest .Any interruptions in chest compression ,in
order to attempt rescue breathing will hamper the
blood flow to vital organs and lower the chances of
survival . Also COCCPR is less complex ,easier to
learn and remember, hence it should be
encouraged while doing Basic Life Support.
Note- In the present case report the bystander
was author herself and the victim was her mother.
1. C i r c u l a t i o n . 2 0 0 7 ; 11 6 : e 5 6 6 - e 5 6 8 doi:10.1161/CIRCULATIONAHA.107.740779
2. Safar P,Escarraga L A,Elam J O. N.Engl J.Med.1958:258:671-677
3. http://phys.org/news 205515381.html
4. http://phys.org/News 205515381.html
5. h t t p : / p h y s . o r g / n e w s / 2 0 1 0 - 1 0 - c h e s t -compression-only cpr-survival-cardiac.html
6. cardiopulmonary resuscitation by Bystanders with chest compression only(SOS-KANTO): an observational study: Lanset 2007; 369:920-926
7. Sayre MR, Berg RA, Cave DM , Page RL ,Potts J ,White RD: American Heart Association Emergency Cardiovascular Care Committee H a n d s - o n l y ( c o m p r e s s i o n -only)cardiopulmonary resuscitation :a call to action for bystander response to adults who experience out of hospital sudden cardiac arrest : a science advisory for the public from the American 2167.Heart Association Emergency Cardiovascular Care Committee Circulation.2008;117:2162-
8. Bobrow BJ, Clark LL, Ewy GA, Chikani V. Sanders AB, Berg RA, Richman PB, Kern KB. Minimally interrupted cardiac resuscitation by emergency medical services for out of hospital cardiac arrest JAMA 200;299:1158-1165.
9. AUfderheide TP, Sigurdsson G Pirrallo RG, Yannopoulos D, Mcknite S, von Briesen C, Sparks CW. Conrad CJ, Provo TA, Lurie KG. Hyperventilation-induced hypotension during cardiopulmonary resuscitation. Circulation 2004;109: 1960-1965.
10. 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation.2010-122;5639-5946
REFERENCES:
Anaesthesiology M.P. 15

1. Deparment of Anaesthesia and crtitical care, Military Hospital Gwalior, Morar Cantt.
Abstract:
Background:
A case of Three NCC cadets bitten by the same
snake while sleeping in their tent at their NCC
camp. This interesting and unusual case occurred
in the rural area of Gwalior, M.P, and India. The
uniqueness of the case lies in the fact that all
three boys were bitten by the same snake.
Further, with negligible local signs of
Envenomation, two of the patients presented
with classical signs of neurotoxicity. The third
patient suffered no ill-effects and was kept under
observation in the ICU. Notwithstanding the
numerous superstitions associated with snake
bite, all of them were rushed to our hospital
immediately and made a complete and
uneventful recovery.
Since time immemorial, snakes have inspired
an awe mixed with fear in our mind. In India,
these reptiles are greatly feared and hence
worshipped. In India, snakes are found
everywhere from the icy heights of the Himalayas
down to Andaman island.
India is inhabited by more than 60 species of
venomous snakes out of which only four have
been popularly known to be dangerously
poisonous to man; cobra, common krait, Russell
1viper and Saw Scaled Viper . In India each year
approximately 200,000 number of cases of snake
bite are reported, out of which 45,000 to 50,000 2succumb to death . India is recognized as having
the highest snakebite mortality in the world. Most
of the fatalities are due to the victim not reaching
the hospital in time and are preventable. This
instance of multiple envenomation with
neurotoxicity by the same snake has not been
reported often in scientific journals.
Three NCC cadets aged between 17-20 years
were sleeping in their tent at their campsite on the
outskirts of Gwalior. All three were asleep when
they were allegedly bitten by a snake. The first boy
was bitten on his left ear.by the time he was alert
and pushed it away realizing it was a snake, he was
bitten again on his right hand also. the snake bit
the second boy who was sleeping on his right
upper arm. The third boy was bitten on his right
leg, however, with no fang marks or skin break.
Since they were in an organized camp, an alarm
was raised and the cadets shown to the
paramedical staff (Nursing assistant) present at
the camp site. A loose tourniquet was applied
(handkerchief) and immobilization of the affected
areas of all the three patients was done. The
Case presentation:
UNUSUAL CASE OF CONSECUTIVE SNAKE BITE IN THREE PERSONS
Case Report
l 1Dr. Maj USSV Meher, Graded Specialist (Anesthesiology)
Anaesthesiology M.P.16

further evaluation.
(b) The second cadet presented with c/o bulbar
symptoms with pupils mid-dilated. Fang marks
were clearly visible on right hand with no local
reaction. ASV 100 ml given over 1 hr. Adjunct
therapy including Dexmedetomidine infusion, IV
antibiotics, PPI inhibitors, Inj Neostigmine with
glycopyrrolate was given as for the first cadet. The
same evening, the patient developed stridor with
acute onset respiratory distress with worsened
bulbar symptoms with pooling of secretions.
ABG showed Co2 retention with fall in SP02. In
view of the above, the patient was placed on
ventilator support. SCMV mode initial FIO2 – 70 %.
He was reassessed after 24 hrs, when he had a
power of grade 4/5 and ptosis was markedly
reduced. He had normal eye opening to command.
He was put on T-piece support. He was extubated
the same evening after 24 hrs of ventilation. He
made a complete recovery and was discharged
after seven days of hospital admission.
(c) The third patient had no signs of
envenomation or any other signs of neurotoxicity.
He was placed in ICU for observation and shifted to
medical ward after 48 hrs.
Snakebites remain a public health problem in
many countries. The snake venom consists of
different enzymatic and non-enzymatic
components. The nature of the symptoms in our
scenario indicates the neurotoxic nature of the
venom. Neurotoxic envenomation has the potency
to cause a broad spectrum presentation ranging
from ptosis and opthalmoplegia to respiratory
arrest. Timely administered anti-venom and
ventilator assistance can prevent the mortality and
morbidity of the victims. The use of anti-
cholinesterase therapy helped accelerate the
clinical recovery by combating post-synaptic toxins
released by the snake venom.
Discussion:
cadets were rushed to the Accident &Emergency
room of Military hospital Gwalior, Morar Cantt.
They reached here at 0420 hrs.
According to the history given by the cadets on
admission the snake managed to crawl away.
Hence the snake was not available to identify its
species.
(a) The first cadet presented with c/o problems
in swallowing and difficulty in opening eyes, pain
and numbness in the body. He had some classic
signs of neurotoxicity, viz.Ptosis, Bulbar symptoms
like drooling of saliva, sluggishness, apathy,
disorientation, slurring of speech, and difficulty in
respiration . GCS 15/15 On examination of bite site,
there was slight redness on left ear without any
features of swelling, bruising, blistering, local
bleeding, etc. Arterial blood gas was normal. ICU
protocol including clott ing profi le was
ordered.ASV was started 5 vials ASV reconstituted
with 100 ml D/W was administered with 5 vials
repeated 6 hrly.over after premedication with Inj
Hydrocortisone/Avil. However, patient had an
attack of severe bronchospasm with rapid
desaturation. He was immediately intubated and
placed on ventilator support on Galileo Gold. He
was put on SCMV mode withFio2 @ 50 %. Inj
Neostigmine 0.05 mg/kg with 0.6 mg Atropine was
given I.M and repeated every6 hrs. he was put on
Dexmedetomidine 0.5 mcg/kg hrly infusion. The
adjunct therapy included antibiotic, PPI inhibitors,
iv. fluids etc. This standard treatment continued for
24 hrs. He was reassessed subsequently Fio2
decreased to 40 %. Power improved to grade 4/5.
He was then put on T-piece with marked
improvement in eye opening and was extubated
after 36 hours and later monitored. The patient
made a remarkable recovery and was discharged
without any sequelae after seven days of hospital
admission. He was asked to report after 1 week for
Signs and symptoms:
Anaesthesiology M.P. 17

Multiple snake bites are relatively common.
However, instances of successive bites by the same
creature at the same instance are relatively
unheard of.
Consent:
Written informed consent was obtained from
the patient for publication of this Case report and
any accompanying images.
Figure 1
Figure 2
Images :- 1& 2: Patient victims of multiple envenomation from a single snake bite, admitted in our ICU
with typical neurotoxic symptoms pre & post convalescence.
References:
1. Mohapatra B,Warreil DA,Suraweera W,Bhatia P,Dhingra N,Jotkar RM,Rodriguez PS,Mishra
K,Whitaker R,Jha P,Million death study.
Collabarators.Snake bite mortality in india:A nationally representative mortality survey, PLoS, Negi
Trop Dis. 2011 Apr 12;5(4):e1018.
2. WHO SEARO (2010): Guidelines on management of Snake-bite New Delhi: WHO Regional office for
South- East Asia.
3. National Snake bite management protocol,2009.
4. Anjum Arshad et al. The Pan African Medical Journal - ISSN 1937-8688: A snake bite on scrotum-a
case report. http://www.panafrican-med-journal.com/content/article/10/25/full/.
Anaesthesiology M.P.18
1. Department of Anaesthesiology and Critical Care, Netaji Subhash Chandra Bose Medical College, Jabalpur
CORRELATION OF GOAL- DIRECTED PREOPERATIVE OPTIMIZATION WITH CLINICAL OUTCOME IN EMERGENCY
ABDOMINAL SURGERY
l 1Dr. Ashish Sethi, Miltan Debbarma, Neeraj Narang,Anudeep Saxena, Mamta Mahobia.
Peritonitis is inflammation of the peritoneum
and is most commonly due to a localized or
generalized infection. It can be primary, secondary
or tertiary based on the source and nature of
microbial contamination.Secondary Peritonitis which is due to
perforation of the hollow viscus continues to be
one of the most common surgical emergencies.
Risk factors among the general population include
among others, helicobacter pylori infection,
indiscriminate use of steroids and non steroidal
anti inflammatory agents, and enteric fever in
addition to several other less common causes. This
condition most of the times needs an emergency
surgical intervention. Since there is lack of data in
India regarding its prognostic indicators, morbidity 1and mortality patterns, application of a scoring
system, is needed to stratify patients to assess the
type and level of care required for a particular
patient.
The management protocols include surgical
intervention, broad spectrum antimicrobial
therapy and intensive care support. Despite this,
management of peritonitis is highly demanding 2and complex. This group of patients invariably
present with features of sepsis on admission, and
thus the management of sepsis has to be primarily
incorporated in the perioperative management
protocol.
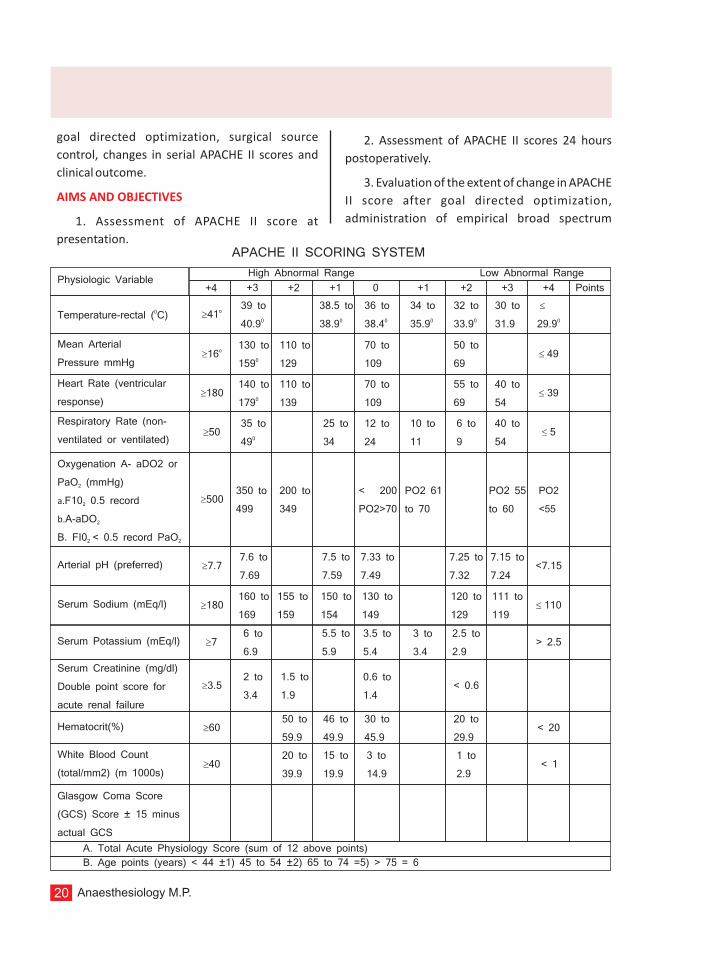
There are various scoring indices such as Acute
Physiology and Chronic Health Evaluation
(APACHE) score (based on 34 Physiological 3,4,5parameters) , the multi organ failure (MOF)
3,4score , and the Mannheim Peritonitis Index 3,6,7,8,9,10(MPI) , for risk stratification in patients of
perforation peritonitis. APACHE II was later
developed as a simplified and clinically useful 11system using 12 physiological variables. The
score can be translated to a mortality risk level that
correlates with observed mortality with
reasonable accuracy.
APACHE II scoring system has been found to be
superior in the prediction of outcome in critically ill
patients with perforation peritonitis in some 12studies. This system is able to stratify a wide
variety of patients prognostically because of the
strong and consistent underlying relationship
between acute physiologic derangement and the
risk of death during acute illness. Acute
Physiological score of APACHE II tends to change in
conditions leading to deranged homeostasis.
This study has taken into account the APACHE II
score and tried to establish a relationship between
Anaesthesiology M.P. 19
goal directed optimization, surgical source
control, changes in serial APACHE II scores and
clinical outcome.
1. Assessment of APACHE II score at
presentation.
AIMS AND OBJECTIVES
2. Assessment of APACHE II scores 24 hours
postoperatively.
3. Evaluation of the extent of change in APACHE
II score after goal directed optimization,
administration of empirical broad spectrum
APACHE II SCORING SYSTEM
Physiologic Variable
0Temperature-rectal ( C)
Mean Arterial
Pressure mmHg
Heart Rate (ventricular
response)
Respiratory Rate (non-
ventilated or ventilated)
Oxygenation A- aDO2 or
PaO (mmHg)2
a.F10 0.5 record2
b.A-aDO2
B. FI0 < 0.5 record PaO2 2
Arterial pH (preferred)
Serum Sodium (mEq/l)
Serum Potassium (mEq/l)
Serum Creatinine (mg/dl)
Double point score for
acute renal failure
Hematocrit(%)
White Blood Count
(total/mm2) (m 1000s)
Glasgow Coma Score
(GCS) Score ± 15 minus
actual GCS
A. Total Acute Physiology Score (sum of 12 above points)
B. Age points (years) < 44 ±1) 45 to 54 ±2) 65 to 74 =5) > 75 = 6
+4 +3 +2 +1 0 +1 +2 +3 +4 Points
o³41
o³16
³180
³50
³500
³7.7
³180
³7
³3.5
³60
³40
39 to
040.9
38.5 to
038.9
36 to
038.4
34 to
035.9
32 to
033.9
30 to
31.9
£
029.9
130 to
0159
110 to
129
70 to
109
50 to
69 £ 49
140 to
0179
110 to
139
70 to
109
55 to
69
40 to
54 £ 39
35 to
049
25 to
34
12 to
24
10 to
11
6 to
9
40 to
54 £ 5
350 to
499
200 to
349
< 200
PO2>70
PO2 61
to 70
PO2 55
to 60
PO2
<55
7.6 to
7.69
7.5 to
7.59
7.33 to
7.49
7.25 to
7.32
7.15 to
7.24<7.15
160 to
169
155 to
159
150 to
154
130 to
149
120 to
129
111 to
119 £ 110
6 to
6.9
5.5 to
5.9
3.5 to
5.4
3 to
3.4
2.5 to
2.9> 2.5
2 to
3.4
1.5 to
1.9
0.6 to
1.4< 0.6
50 to
59.9
46 to
49.9
30 to
45.9
20 to
29.9< 20
20 to
39.9
15 to
19.9
3 to
14.9
1 to
2.9< 1
High Abnormal Range Low Abnormal Range
Anaesthesiology M.P.20

antibiotics and definitive source control.
4. To observe the outcome in terms of duration
of hospital stay and mortality in both the groups.
After obtaining clearance from the institutional
ethics committee and informed consent the study
was carried out in the Department of
Anaesthesiology and Critical Care, Netaji Subhash
Chandra Bose Medical College, Jabalpur.
100 patients 16 years and above, of ASA
physical status I and II E with clinical diagnosis of
perforation peritonitis.
Group I (Case): 50 patients optimized by goal
directed optimization protocol in the pre operative
holding room by anaesthesiology residents.
Group II (Control): 50 patients managed by
surgery residents in the surgical wards without any
fixed algorithm.
* Spontaneous Bacterial Peritonitis
* Malignancy
* Negative Allen's test
* Anticoagulant therapy
* Patients requiring mechanical ventilation
pre or post operatively.
Patients with abdominal emergencies admitted
to general surgery units were prescreened and
were included in the study only after a clinical
diagnosis of perforation peritonitis was made with
reasonable certainty. Assessment of APACHE II
score was done as a first step and patients were
randomly assigned to one of the two groups, case
group(S) and control group (C). Patients of the case
group received standardized, algorithmic
METHODOLOGY
Selection of cases:
Criteria for exclusion:
STUDY PROTOCOL
management in the preoperative holding room.
Central venous cannulation was performed and
goal directed optimization of these patients was
carried out by the anaesthesiology resident on call.
Those in the control group were managed in the
surgery wards by the surgical resident on call.
Patients assigned to the case group were
optimized till the following targets were achieved
central venous pressure (CVP) between 8 and 12
cmH2O, mean arterial pressure (MAP) of 65 mmHg
or above, and urine output equal to or greater than
0.5 ml.kg-1 hr-1.
The protocol for goal-directed optimization
was as follows. Boluses of 0.9% saline (20-30 ml/kg
body weight) were given every 30 minute to
achieve the first goal (CVP 8 to 12 cmH2O). If MAP
was less than 65 mmHg after reaching the first
goal, vasopressor (nor epinephrine infusion) was
given to achieve and maintain the second goal
(MAP > 65 mmHg). Our third goal was to ensure a
urine output of > 0.5 ml/kg/hr.
In contrast, the patients in control group were
managed according to the clinical judgment
without any fixed algorithm. Empirical broad
spectrum antibiotic cover was given to all the
patients in both the groups.
Patients in the case group were taken up for
surgery after objectively achieving all three three
goals (end points of resuscitation) while those in
the control group were taken up for surgery after
subjective hemodynamic stabilization.
All patients received standard general
endotracheal anaesthesia. Intraoperatively
electrocardiogram (ECG), heart rate, oxygen
saturation (SPO2), non invasive blood pressure
(NIBP) and end tidal carbon dioxide (EtCO2), urine
output monitored.
Decision to extubate the patients or to
continue ventilation was based on the patient's
Anaesthesiology M.P. 21

Table 1APACHE II SCORE ON ADMISSION
Group
Case
Control
Mean
6.8
7.1
SD
3.7
2.6
clinical condition and immediate postoperative
blood gas parameters.
Patients were closely monitored in post
operative recovery room for the next 72 hrs.
APACHE II scoring was repeated 24 hr
postoperatively. Patients were shifted to
postoperative ward after 72 hrs and followed up
till discharge from hospital. In hospital mortality
was taken as the outcome.
All case report forms were checked for
completeness and inappropriate or illogical
responses. The forms were entered using
Microsoft 2007 Excel worksheet. The data bases
were validated and all inconsistencies and
differences were resolved. Statistical analyses
were performed using STATA 12 for Windows
(Stata Corp E.P., Texas, USA). Categorical data are
presented as frequency counts (percent) and
compared using the chi-square or Fisher's exact
statistics as appropriate
OBSERVATIONS AND RESULTS
The mean APACHE II score on admission in case
group is 6.8 ± 3.7 and in the control group is 7.1 ±
2.6. There was no significant difference between
the two study groups.
There is a significant lowering of serial APACHE II
scores in case group as compared to control group
(p < 0.001).
There was significant lowering of mean duration
of hospital stay seen in case group (9.8 ± 1.7 days) as
compared to control group (11.26 ± 3.2 days) p <
0.005.
Table 2APACHE II SCORE, 24 HRS
Group
Case
Control
Mean
2.2
4.5
SD
3.2
3.2
Table 3DURATION OF HOSPITAL STAY (DAYS
Study
Case
Control
Mean
9.8
11.26
SD
1.7
3.2
Table 4
TYPE OF OPERATION DONE
Operation done
Primary Repair of ileal perforation withproximal ileostomy
Omentopexy of pre pyloric perforation
Primary repair of ileal perforation
Total
Case
22(44%)
27(54%)
1(2%)
50
Control
18(36%)
27(54%)
27(54%)
50
Total
40(40%)
54(54%)
6(6%)
100
Anaesthesiology M.P.22

The number of deaths in case group was 4%,
while that in the control group was 16%.
There was significant decline in death rate in
case group as compared to control group.
Majority of perforation peritonitis patients
present late with sepsis which further increases
morbidity and mortality. Both sepsis and third
space loss of fluid due to perforation leads to
imbalance between oxygen demand and delivery
resulting in tissue hypoxia and subsequent
multiple organ failure. Several studies support the
concept that persistent shock has an adverse
impact on survival in a time dependent manner
and therapeutic strategies involving early
recognition and rapid reversal of shock improves
survival.
Perforation peritonitis is a frequently
encountered surgical emergency in tropical
countries like India. It affects mostly the young.1,2
Despite advances in management protocols it
poses a formidable challenge for perioperative
physicians.2 Majority of cases present late with
features of sepsis and septic shock.13 Therefore
for such a setting there is enough justification in
favor of goal directed optimization which has
evidence based role in improving outcomes in
sepsis and septic shock as established after the
landmark study by Rivers et al.16
In this study, we found that majority of
DISCUSSION
patients had upper gastrointestinal tract
perforation; i.e. 54% suffered from pre-pyloric
perforation and rest had ileal perforation. This
concurs with earlier studies of R.S. Jhobta et al2,
and M.L. Ramchandran et al.14 which showed
greater percentage of perforation cases involving
upper gastrointestinal tract in India.
APACHE II (Acute Physiology and Chronic
Health Evaluation II) is a severity of disease
classification system (Knaus et al), 15 among one
of the several ICU scoring systems. It is applied
within 24 hours of admission in an intensive care
unit (ICU), an integer score from 0 to 71 is
computed based on several measurements;
higher scores correspond to more severe disease
and a higher risk of death.
We observed that majority of the patients in
case group showed features of sepsis; notably,
tachycardia (pulse rate > 90/min), tachypnoea
(respiratory rate > 20), hypotension (SBP < 90 0mmHg) and temperature > 38 C. Such patients
underwent a Goal Directed Optimization as per
our study protocol. Boluses of 0.9% saline (20- 30
ml/kg body weight) were given every 30 minutes
to achieve the first goal (CVP 8 to 12cmH2O). If
MAP was less than 65 mmHg after reaching the
first goal, vasopressor (norepinephrine infusion)
was instituted to achieve and maintain the second
goal (MAP > 65 mmHg). Our third goal was to
ensure a urine output of > 0.5 ml/kg/hr.
The initial APACHE II score taken at admission
was comparable in both case and control groups
(6.8 ± 3.7 vs. 7.1 ± 2.6), whereas there was a
significant reduction in APACHE II score 24 hours
post operatively in both the groups (2.2 vs. 4.5) (p
< 0.0001 vs. p < 0.001)
After optimization the surgeon proceeded
with definitive source control. The surgeries
performed in majority of patients were primary
repair of pre-pyloric perforation with omentopexy
Table 5
FINAL OUTCOME
Outcome
Death
Discharge
Total
Case
2(4%)
48(60%)
50
Control
8(16%)
42(84%)
50
Anaesthesiology M.P. 23

(case 54% control 54%). This study is in agreement
with the study of M.L. Ramchandra et al.14
There was unanimity in mean duration of
hospital stay in this study as seen in the past
studies. Rivers E. et al 16 showed that there was
significant reduction in duration of hospital stay
among those who were treated by goal directed
optimization. In accordance, we found that
optimized patients in case group were discharged
early (9.8 ± 1.7) as compared to control group
(11.26 ± 3.2) (p<0.005).
The study of Han et al17 observed that early
shock reversal by adequate fluid resuscitation was
associated with improved outcome and each hour
of delay in resuscitation was associated with 50%
increased odds of mortality.
Another study of Whalen et al18 showed that
aggressive fluid resuscitation early in the
treatment course led to a decreased occurrence of
persistent shock and subsequently improved
survival of patients with septic shock.
In this study we observed a lower mortality
rate in the case group (4%) as compared to the
control group (16%) (p < 0.05). This study is
inspired by and broadly follows the principles
established in the landmark Rivers study, with
variations and modifications such as exclusion of
central venous saturation (ScvO2) measurement
largely due to resource limitations and feasibility
considerations prevalent in the day to day practice
in a government medical college hospital setting.
1. Sharma L, Gupta S, Soin AS, Sikora S,
Kapoor V. Generalised peritonitis in India- the
tropical spectrum. Jpn J Surg. 1991; 21:272-7.
2. Jhobta RS, Attri AK, Kaushik R, Sharma R,
Jhobta A. Spectrum of perforation peritonitis in
India-review of 504 consecutive cases. World J
Emerg Surg. 2006; 1:26.
REFERENCES
3. Notash AY, Salimi J, Rahimian H,
Fesharaki MS, Abbasi A. Evaluation of Mannheim
peritonitis index and multiple organ failure score
in patients with peritonitis. India J Gastroenterol.
2005; 24:197-200.
4. Rogy M, Fugger R, Schemper M, Koss G,
Schulz F. The value of two distinct prognosis score
in patients with peritonitis. The Mannheim
Peritonitis Index versus the APACHE Score,
Chirurg, 1990; 61:297-300.
5. Lee FY, Leung KL, Lai BS, Ng SS, Dexter S,
Lau WY, Predicting mortality and morbidity of
patients operated on for perforated peptic ulcers.
Arch Surg. 2001; 136:90-4.
6. Billing A, Frohlich D, Schildberg FW.
Prediction of outcome using the Mannheim
peritonitis index in 2003 patients. Br. J. Surg. 1994;
81:209-13.
7. Bosscha K,Reijnders K. Hulstacrt PF, Algra
A. van der Werken C. Prognostic scoring systems
to predict outcome in peritonitis and intra
abdominal sepsis. Br. J. Surg. 1987; 4:1532-4.
8. Kologlu M, Elker D, Altun H, Sayek I.
Validation of MPI and PIA II in two different groups
of patients with secondary peritonitis.
Heptogastroenterology. 2001:48:147-51.
9. Goris RJ, Boekhorst TP, Nuytinck JK,
Gimbrare JS. Multiple-organ failure: Generalised
autodestructive inflammation? Arch Surg. 1985;
44:937-46.
10. Makela JT, Kiviniemi H, Ohtonen P,
Laitinen SO. Factors that predict morbidity and
mortality in patients with perforated peptic
ulcers. Eur J Surg. 2002; 168:446-51.
11. Knaus WA, Draper EA, Wagner DP,
Zimmerman JE. APAC HE II acute physiology and
chronic health evaluation: a severity of disease
classification system. Crit Care Med. 1985;
Anaesthesiology M.P.24

13:818-29.
12. Samir Delibegovic, Dragana Markovic et
al. Apache II Scoring System Is Superior in the
Prediction of the Outcome in Critically III Patients
with Perforative Peritonitis in Pakistan: 300 cases.
Eastern experience. World J Emerg Surg 2008;
3:31.
13. Ersumo T, W/Meskel Y, Kotisso B.
Perforated peptic ulcer in Tikur Anbessa Hospital;
a review of 74 cases. Ethiop Med. J. 2005; 43:9-13.
14. Methikere Lingaiah Ramachandra,
Bellary Jagadesh, Sathees B.C. Chandra: Clinical
Study and Management of Secondary Peritonitis
due to Perforated Hollow Viscous; Arch Med Sci
2007; 3:1:61-68.
15. Knaus WA, Draper EA, Wagner DP,
Zimmerman JE. APAC HE II – acute physiology and
chronic health evaluation: a severity of disease
classification system. Crit Care Med. 1985;
13:818-29.
16. Rivers E, Nguyen B, Havstad S, Ressler J,
Muzzin A, Knoblich B, Peterson E, Tomlanovich M:
Early goal directed therapy in the treatment of
severe sepsis and septic shock. N. Engl J Med
345:1368Y1377, 2001.
17. Han YY, Carcillo JA, Dragotta MA: Early
reversal of pediatric neonatal septic shock by
community physicians is associated with
improved outcome. Pediatrics 112:793-799,
2003.
18. Whalen MJ, Doughty LA, Carlos TM:
Intercellular adhesion molecule-1 and vascular
cell adhesion molecule-1 are increased in the
plasma of children with sepsis induced multiple
organ failure. Crit Care Med 28:2600-2607, 2000.
Anaesthesiology M.P. 25

Abstract:
Introduction
Congenital heart disease is one of the
commonest birth defect.Advancement of
medical and surgical skills have increased the
survival to adulthood. Hence, we encounter many
such children reporting for various disorders
requiring anesthesia for non-cardiac surgical
corrections. They pose a challenge for anesthesia
because perioperative morbidity and mortality is
greater compared with other children. The
anatomy and pathophysiology of defect of each
patient is different resulting in a varied response
during management. Hence, it is arduous to
manage these cases in basic set up without
invasive monitoring. We report a case of
uncorrected Tetralogy of Fallot posted for closed
reduction under anesthesia.
Key-words: uncorrected Tetralogy of Fallot,
shunt operation, right to left shunt, anesthetic
management, phenylephrine
Cyanotic Congenital Heart Disease (cCHD) is
characterized by intracardiac right-to-left
shunting of unsaturated blood and its distribution
into the systemic circulation resulting in arterial 1hypoxemia . Tetralogy Of Fallot is one of the most
common forms of cyanotic congenital heart
1. Department of Anaeshesiology, NSCB Medical College, Jabalpur
CASE OF UNCORRECTED TETRALOGY OF FALLOT POSTED FOR CLOSED
REDUCTION AND HIP SPICA APPLICATION FOR FRACTURE OF SHAFT OF FEMUR
l 1 2 3Dr. Priya Shenwani , Dr. Pradeep Meshram , Dr. Neeraj Narang
2disease . Most patients experience cyanosis at
birth and die in childhood without surgical
intervention. The rate of survival at 40 years 3without surgical correction is only 3% . The main
causes of death are chronic congestive heart
failure, secondary to the long-standing pressure
overload and consequent pathological changes in 4the right ventricle and arrhythmias . The
treatment consists of palliative procedures like
systemic-pulmonary (s/p) arterial shunts and
balloon dilatation of pulmonic valve; or definitive
surgical correction. Central shunt is a type of s/p
shunt in which artificial graft tube is placed in
between aorta and pulmonary artery.
We report a case of 6 year old boy weighing 15
kgs who reported in our hospital for pain and
swelling in right thigh and inability to move the
limb. He gave a history of fall on the ground while
playing. He was diagnosed with closed fracture of
proximal third shaft of femur right side. He was
posted for closed reduction of fracture and
application of hip spica under anesthesia.
The child was examined carefully as he had
marked central cyanosis and grade IV clubbing.
There was presence of loud systolic murmur and
click in the aortic area. Chest X-ray showed an
Case history
Case Report
Anaesthesiology M.P.26

titrated as per response. We noted that saturation increased after giving phenylephrine, but was fixed at 88%. There was no further rise in SpO2 despite increasing rate of phenylephrine.
After completion of the procedure, child was
shifted to the ICU for recovery and monitoring. He
was discharged from ICU the next day, with
uneventful course of events.
The children suffering from Tetralogy of Fallot,
which is one of the most common type of
congenital cyanotic heart disease, are chronically
hypoxemic. They have easy fatigability and become
breathless. They are also susceptible to recurrent
fever and chest infections. Usually they may have
growth retardation, delayed milestones, severe
metabolic derangements, multi-organ failure, and
major neurological deficits. They are prone for
vascular stroke, brain abscess, arrhythmias, heart 5, 6blocks, and infective endocarditis . Hence, it's
prudent to administer prophylactic antibiotics 6before any intervention in the operating room .
Cases with uncorrected defects are intricate,
but palliative correction makes them relatively
simpler. The ultimate goal of conducting such cases
is maintaining pulmonary blood flow and
hydration. There are many recognized factors
known to affect the direction of shunt flow and the
degree of shunting. Hence the main goal of
induction in a cyanotic patient is to establish
balanced anesthesia without increasing right-to-
left shunt fraction. The main objectives are to
maintain SVR, or even rise in SVR is favorable (by
using adrenergic agonists like phenylephrine) as it 7increases pulmonary blood flow . We should try to
decrease PVR to improve and maintain pulmonary
blood flow by hypocarbia, alkalosis, high oxygen 7concentrations, inhaled nitric oxide, etc .
Ketamine is an excellent inducing agent for
cyanoticheart disease, because it decreases PVR,
Discussion
enlarged boot shaped heart with pulmonary
oligaemia. ECG suggested of right ventricular
hypertrophy and right axis deviation. On
echocardiography, there was dilated right
ventricle, with over-riding of aorta, large VSD and a
shunt was seen in aorta. Detailed history,
examination and investigations revealed that he
was a case of congenital cyanotic heart disease. 3
Hb levels were 16.9 gm%, TLC was 8000 cells/mm , 3and platelet count was 1.95 lac / mm . He was
taking Tab. Aspirin 50 mg and tab. Propanolol
2.5mg daily.
Two years ago, he underwent shunt surgery
(central s/p shunt between aorta and right
pulmonary artery ) for palliation of symptoms as
he suffered from Tetralogy of Fallot with
pulmonary atresia and patent ductus arteriosus.
After explaining high risk and taking a written
informed consent, he was taken in the operating
room. Basic monitors were connected like NIBP,
SpO2, and ECG. Peripheral venous access was
obtained with 22G intracath using aseptic
precautions. We avoided inadvertent flushing and
performed judicious drug administration to
prevent air bubbles from entering the circulation.
Ringer lactate (RL) was administered at 4mL/kg
and prophylactic i.v. antibiotics (inj. Ceftriaxone-
sulbactum) given as per body weight.
On air saturation was 55%, heart rate was 88
beats/min, and NIBP was 98/58 mmHg. Inj. i.v.
glycopyrrolate 0.2mg was given. Induction was
done by using i.m. Ketamine 100mg (7mg/kg)and
100% oxygen was given via facemask using Ayre's
T-piece.
Closed reduction and hip spica application was
done. Vitals were stable and recorded after every
5min.
Saturation increased to 63% after giving 100% oxygen, Heart rate was 106/min. . Phenylephrine infusion at rate of 0.5-5 ìg/kg/min was started and
Anaesthesiology M.P. 27

maintains SVR and is the safest agent for cyanotic 8patients .
The children with Tetralogy of Fallot are at an
increased risk for significant hypoxia (tet spells/
blue spells/ cyanotic spells), characterized by
sudden cyanosis and syncope. This happens by
increased shunting of blood due to decrease in
systemic vascular resistance and increase in
venous return. It can be prevented by
maintaining adequate hydration, avoid exposure
to cold, adequate glucose intake and oral
Propanolol 0.5-1 mg/kg/ 6hrly.
Management of a hypercyanotic spell intra-
operatively should include general measures to
reduce infundibular spasm, improve oxygenation
and increase cardiac output, and specific
measures to reduce right to left shunt and/or
infundibular spasm: Increase inspired oxygen,
fluid bolus 10-20 ml.kg-1, deepen anaesthesia,
fentanyl bolus 1 mcg.kg-1 Phenylephrine 1
mcg.kg-1 bolus up to 5-10mcg.kg-1 can be given.
It is advisable to perform an ABG to rule out
metabolic acidosis pre-operatively, and to treat
the same in case of severe cyanotic spells.
A vigilant eye is required throughout the
procedure to detect and manage any
complications namely hypoxia, hypotension,
acidosis, etc. Good analgesia will reduce
sympathetic stimulation and hemodynamic
instability. Postoperative care includes intensive
monitoring, appropriate fluid management, and 9, 10good control of pain .
We would appreciate your feedback on this
case report. This was done to the best of our
abilities although unavailability of invasive
monitoring was a concern.
1. Abhijeet Raha, Pragati Ganjoo, Amay Singh,
Monica S. Tandon, and Daljit Singh J Pediatr
References
Neurosci. 2012 Jan-Apr; 7(1): 23–26
2..Tanaka K, Kitahata H, Kawahito S, Nozaki J,
Tomiyama Y, Oshita S. Phenylephrine increases
pulmonary blood flow in children with tetralogy of
Fallot. Can J Anaesthe 2003 Nov 50(():926-9
3. Cerebral Abscess in 8 years old with
uncorrected Tetralogy of Fallot: Anesthetic
challenge
Sidharth Sraban Routray, Khageswar Raut ,
Debasis Mishra, Rajib Mishra IJBAR (2013) 04 (11)
4. Kaplan JA, cardiac anesthesia 4thed .
Philadelphia : WB Saunders, 1999:812
5. Anwar AM, Nosir YF, Anjam A, Mushtaq M,
Alama MN, Chamsi-Pasha H: Multivalvular
infective endocarditis in a tetralogy of Fallot.
Echocardiography 2008, 25:88–90.
6. Freed MD: Infective endocarditis in the adult
with congenital heart disease. Cardiol Clin 1993,
11:589–602.
7. Shahani JM. Anesthetic considerations in
children with congenital heart disease undergoing
non-cardiac surgery. Indian J Anaesth
2012;56:491-5.
rd8. Lake CL, pediatric cardiac anesthesia 3 ed.
Stamford, CT :Appleton & Lange, 1998:223-229
9. Yumul R, Emdadi A, Nassim M. Anesthesia
for non cardiac surgery in children with congenital
heart disease. Semin Cardiothorac Vasc Anesth.
2003;7:153–65.
10. White MC. Anesthetic implications of
congenital heart disease for children undergoing
non-cardiac surgery. Anaesth Intensive Care Med.
2009;10:504–9.
Anaesthesiology M.P.28

ABSTRACT:
INTRODUCTION:
CASE REPORT :
We present a case of 37 years male American
Society Of Anesthesiologists Grade I who
underwent C1 – C2 posterior cervical fusion for
atlanto – axial dislocation under general
anaesthesia with flexometallic endotracheal
tube in prone position. Entire surgical procedure
and anaesthesia was uneventful but before
extubation patient bit the tube and the tube was
cut into two pieces connected only by a thin wire.
Although the lacerated tube was removed using
Magill's forceps without any complications but it
taught us a lesson and made to think – Are these
tubes really safe to use?
Since last few years, anaesthesia has
considerably advanced to safer techniques.
Flexometallic endotracheal tubes are one of
these safer techniques and now are being
increasingly used in routine anaesthetic practice
as a safer and preventive option in certain cases
where kinking and compression of endotracheal
tube intraoperatively is anticipated.1
A 37-year male, American society of
anesthesiologists Grade I, with diagnosis of
atlanto – axial dislocation was posted for C1-C2
posterior fusion. Routine blood investigations
including complete blood count, serum
creatinine, blood urea nitrogen, random blood
sugar, serum electrolytes, bleeding time, clotting
time, Chest X-ray and electrocardiogram were
within normal limits. Preanaesthetic examination
revealed no systemic illness and airway was
Mallampatti Grade I. Patient was premedicated
with intramuscular injection. Glycopyrollate 0.2
mg half an hour before taking to operation
theatre. Patient was taken in operation theatre
after obtaining intravenous access,and was
m o n i t o r e d w i t h p u l s e o x i m e t e r ,
electrocardiogram, non invasive blood pressure
and end tidal carbon-di-oxide. Induction was done
with intraveneous injection fentanyl 2 mcg/kg and
intraveneous injection Propofol 2 mg/kg, muscle
relaxation was achieved with intraveneous
injection Rocuronium 0.9 mg/kg. Patient was
intubated with Flexometallic endotracheal tube of
internal diameter 8.5 mm. After securing the tube
with adhesive tapes along with Guedel's airway,
patient was made prone for surgery. Anesthesia
was maintained with O2 + N2O in 1:1 ratio with
Isoflurane 1% and injection Atracurium 0.1 mg/kg.
Surgical procedure lasted for approx. 3 hours and
the entire intraoperative anaesthesia course was
uneventful. After completion of surgical
procedure, the patient was made supine &
1. Consultant Anesthesiologist, Pain Consultant and OT Superintendent Vishesh Hospital Indore
FLEXOMETALLIC ENDOTRACHEALTUBES - ARE THEY REALLY SAFE?
l 1 2Dr. Meenu Chadha, Dr. Dharna Jain,
Case Report
2. Sr. Resident, Dept. of Anaesthesia, Vishesh Hospital Indore
Anaesthesiology M.P. 29

anaesthesia was reversed using intraveneous
Injection Myopyrrolate . Oral and endotracheal
tube suctioning was done and when reversal
criteria was accomplished we planned to
extubate the patient but to our surprise after
laryngoscopic suction of the oral cavity with
removal of the oral airway our patient tightly
clenched his teeth and bit the tube to the extent
that the tube got lacerated completely (IMAGE 1)
.
Fortunately the lacerated tube was removed
successfully by our team using Magill's forceps
without aspiration or any other complication but
this incidence taught us a big lesson. Patient was
shifted to intensive care unit in stable condition
and discharged by the surgeon after few days.
Flexometallic endotracheal tubes or spiral
embedded tubes or armoured tubes have
advantage of being resistant to kinking and
compression making them useful in surgeries in
prone position, sitting position, head and neck
surgeries, tracheal surgeries, neurosurgical
procedures and cases where head and neck
manipulation is required intra operatively for
better surgical access.3 These tubes have nylon
or metal spiral wound reinforcing wire covered
DISCUSSION:
both internally and externally by rubber, latex,
poly vinyl chloride or silicone.3
Although these tubes are a boon for certain
surgical procedures they do possess some
problems which cannot be overlooked. Like they
require stylet for insertion and may get rotated on
the stylet during the insertion, possess difficulty
for nasotracheal intubation, and cannot be
shortened, 3, 4, . Overuse and repeated
sterilization of reusable spiral embedded tubes
can predispose them to problems Dynamic
kinking of these tubes by compression with a
Dingmans retractor may lead to ventilatory
problems.5 Latex allows greater flexibility of tube
than the red rubber but it is more susceptible to
deformity on inflation. During light plane of
anaesthesia, patient can bite the tube leading to a
serious complication like permanent deformation
of the tube and thus occlusion of lumen leading to
difficulty in endotracheal suction and life
threatening hypoxia and hypoventilation.1,3
Laceration of tube as happened in our case
may lead to aspiration of tube material which
itself may create a life threatening situation,
fortunately we came out without any of such
complication, but this may not be always the case.
This case reasserts some of the valuable standard
teachings :
Anaesthesiology M.P.30

(a) Keep a bite block /dental prop in place
when a patient has an airway maintaining gadget
in place (endotracheal tube, laryngeal mask
airway etc.
(b) Do not remove bite block/dental prop
during oral suction.
(c) Remove the bite block/dental prop after
removal of the endotracheal tube /laryngeal
mask air way etc
(d) if available, use the tubes with covering at
the bite portion.
1. Dr Dinesh Malhotra, Dr Mehmood Rafiq,
Dr Shagufta Qazi, Dr Satya Dev Gupta-Ventilatory
obstruction with spiral embedded tube- Are they
REFFERNCES:
as safe? IJA 2007;51;5:432-433
2. Dr Sonia Wadhwan, Dr Vibha and Dr
Rakesh Kumar- An uncommon reason for damage
to the intubating laryngeal mask airway (ILMA)
endotracheal tube inflation system. A&A
2004;99:2:624
3. Dr Afzal Azim1, Dr. Prakash Matreja, Dr.
Chandrakant Pandey. Desaturation with
flexometallic endotracheal tube during lumber
spine surgery– A case report. IJA 2003; 47;1:48-49
4. P. Martens: Persistent narrowing of an
armoured tube. Anaesthesia 1992; 47: 716-717
A j a y K u m a r, H . H . D a s h - D y n a m i c
intraoperative kinking of flexometallic tube.
Journal of Neurosurgical Anesthesiology July
2001;13;3:243-245
Anaesthesiology M.P. 31

ll manuscripts must be submitted via email
to [email protected]. AThe submitted manuscripts that are not as per
the “Instructions to Authors” would be returned
to the authors for technical correction, before
they undergo editorial/peer-review. Generally,
the manuscript should be submitted in the form
of two separate files:
1. Title Page/First Page File/covering
letter: This file should provide
a. The type of manuscript (original article,
review article, short communication, Letter to
editor, etc.) title of the manuscript, running title,
names of all authors/ contributors (with their
highest academic degrees, designation and
affiliations) and name(s) of department(s) and/ or
institution(s) to which the work should be
credited, . All information which can reveal your
identity should be here. Use text/rtf/doc files. Do
not zip the files.
b. The total number of pages, total number
of photographs and word counts separately for
abstract and for the text (excluding the
references, tables and abstract), word counts for
introduction + discussion in case of an original
article;
c. Source(s) of support in the form of
grants, equipment, drugs, or all of these;
d. Acknowledgement, if any. One or more
statements should specify 1) contributions that
need acknowledging but do not justify
authorship, such as general support by a
departmental chair; 2) acknowledgments of
technical help; and 3) acknowledgments of
financial and material support, which should
specify the nature of the support. This should be
SUBMISSION GUIDELINESincluded in the title page of the manuscript and
not in the main article file.
e. If the manuscript was presented as part
at a meeting, the organization, place, and exact
date on which it was read. A full statement to the
editor about all submissions and previous reports
that might be regarded as redundant publication
of the same or very similar work. Any such work
should be referred to specifically, and referenced
in the new paper. Copies of such material should
be included with the submitted paper, to help the
editor decide how to handle the matter.
f. Registration number in case of a clinical
trial and where it is registered (name of the registry
and its URL)
g. Conflicts of Interest of each author/
contributor. A statement of financial or other
relationships that might lead to a conflict of
interest, if that information is not included in the
manuscript itself or in an authors' form
h. Criteria for inclusion in the authors'/
contributors' list
i. A statement that the manuscript has
been read and approved by all the authors, that
the requirements for authorship as stated earlier
in this document have been met, and that each
author believes that the manuscript represents
honest work, if that information is not provided in
another form (see below); and
j. The name, address, e-mail, and
telephone number of the corresponding author,
who is responsible for communicating with the
other authors about revisions and final approval of
the proofs, if that information is not included on
the manuscript itself.
Anaesthesiology M.P.32

2. Blinded Article file: The manuscript
must not contain any mention of the authors'
names or initials or the institution at which the
study was done or acknowledgements. Page
headers/running title can include the title but not
the authors' names. Manuscripts not in
compliance with The Journal's blinding policy will
be returned to the corresponding author. The
main text of the article, beginning from Abstract
till References (including tables) should be in this
file. Use rtf/doc files. Do not zip the files.
3. Images: Submit good quality color
images. Each image should be less than 4 MB in
size. Size of the image can be reduced by
decreasing the actual height and width of the
images (keep up to 1800 x 1200 pixels or 5-6
inches). Images can be submitted as jpeg files. Do
not zip the files. Legends for the figures/images
should be included at the end of the article file.
4. The contributors' / copyright transfer
form (template provided below) has to be
submitted in original with the signatures of all the
contributors within two weeks of submission .
Manuscripts must be prepared in accordance
with "Uniform requirements for Manuscripts
submitted to Biomedical Journals" developed by
the International Committee of Medical Journal
Editors (October 2006).
These include original research work in
Pharmaceutical sciences, Medicinal/analytical
chemistry, Biotechnology and bioallied sciences.
The text of original articles amounting to up to
2500 words (excluding Abstract, references and
Tables) and The manuscript may have about 25 to
30 references should be divided into sections
with the headings Abstract, Key-words,
Preparation of Manuscripts
Types of Manuscripts
Original articles:
Introduction, Material and Methods, Results and
Discussion,Conclusion, References, Tables and
Figure legends.
The review articles are strictly by invitation
from the Editor. It is expected that these articles
would be written by individuals who have done
substantial work on the subject or are considered
experts in the field and are solicited by the
editorial board. A short summary of the work
done by the contributor(s) in the field of review
should accompany the manuscript.
The prescribed word count is up to 3500 words
excluding tables, references and abstract. The
manuscript may have about 40 to 50 references.
The manuscript should have an unstructured
Abstract (250 words) representing an accurate
summary of the article. The section titles would
depend upon the topic reviewed.
The journal expects the contributors to give
post-publication updates on the subject of review.
The update should be brief, covering the advances
in the field after the publication of the article and
should be sent as a letter to editor, as and when
major development occurs in the field.
New, interesting and rare cases can be
reported. They should be unique, describing a
great anaesthetic challenge and providing a
learning point for the readers. Cases with clinical
significance or implications will be given priority.
These communications could be of up to 1400
words (excluding Abstract and references) and
should have the following headings: Abstract
(unstructured), Key-words, Introduction, Case
report, Discussion,Conclusion, References, Tables
and Legends in that order.
The manuscript could be of up to 1400 words
(excluding references and abstract) and could be
Review Articles:
Case reports:
Anaesthesiology M.P. 33
supported with up 10 to 15 references. Case
Reports could be authored by up to four authors.
The manuscript could be of up to 1000 words
(excluding references),without abstract and
could be supported with up 6 to 8 references and
should have the fo l lowing headings :
Introduction, Case report (for Case reports)
( M e t h o d s a n d r e s u l t s f o r c l i n i c a l
i nve st i gat i o n s ) , D i s c u s s i o n , C o n c l u s i o n ,
References, Tables and Legends in that order
These should be short and decisive
observations. They should preferably be related
to articles previously published in the Journal or
views expressed in the journal. They should not
be preliminary observations that need a later
paper for validation. The letter could have up to
600 words and 6 references. It could be generally
authored by not more than four authors.
The comments,addressed to the
Editor,should include reference of the published
article,should be concise (Max.250 words) with
critical comments to the point, with references in
support.Upto 300 words and not more than 4
references,including the first reference of the
article being commented upon to be included.
Response to Comments: The author is
allowed to present his case/response to the
observations made by the reader, in concise,upto
300 words.
R e f e r e n c e s s h o u l d b e n u m b e r e d
consecutively in the order in which they are first
mentioned in the text (not in alphabetic order).
Identify references in text, tables, and legends by
Arabic numerals in square bracket after the
punctuation marks. References cited only in
Brief communications
Letter to the Editor:
Comments on Published Articles:
References
tables or figure legends should be numbered in
accordance with the sequence established by the
first identification in the text of the particular
table or figure.No references to be used in absract
and Conclusion/ Summary. Use the style of the
examples below, which are based on the formats
used by the NLM in Index Medicus. The titles of
journals should be abbreviated according to the
style used in Index Medicus. Use complete name
of the journal for non-indexed journals. Avoid
using abstracts as references. Information from
manuscripts submitted but not accepted should
be cited in the text as “unpublished observations”
with written permission from the source. Avoid
citing a “personal communication” unless it
provides essential information not available from
a public source, in which case the name of the
person and date of communication should be
cited in parentheses in the text. References from
past issues of IJA of related topics encouraged.
The commonly cited types of references are
shown here, for other types of references such as
newspaper items please refer to ICMJE Guidelines
( h t t p : / / w w w . i c m j e . o r g o r h t t p : / /
www.nlm.nih.gov/bsd/uniform_requirements.ht
ml).
a. Standard journal article (for up to six
authors): Shukla N, Husain N, Agarwal GG, Husain
M. Utility of cysticercus fasciolaris antigen in Dot
ELISA for the diagnosis of neurocysticercosis.
Indian J Med Sci 2008;62:222-7.
b. Standard journal article (for more than
six authors): List the first six contributors followed
by et al.
Nozari Y, Hashemlu A, Hatmi ZN, Sheikhvatan
M, Iravani A, Bazdar A, et al. Outcome of coronary
artery bypass grafting in patients without major
risk factors and patients with at least one major
risk factor for coronary artery disease. Indian J
Articles in Journals
Anaesthesiology M.P.34

Med Sci 2007;61:547-54
c. Volume with supplement:
Shen HM, Zhang QF. Risk assessment of nickel
carcinogenicity and occupational lung cancer.
Environ Health Perspect 1994; 102 Suppl 1:275-
82.
d. Issue with supplement:
Payne DK, Sullivan MD, Massie MJ. Women’s
psychological reactions to breast cancer. Semin
Oncol 1996; 23(1, Suppl 2):89-97.
a. Personal author(s): Ringsven MK, Bond
D. Gerontology and leadership skills for nurses.
2nd ed. Albany (NY): Delmar Publishers; 1996.
b. Editor(s), compiler(s) as author: Norman
IJ, Redfern SJ, editors. Mental health care for
elderly people. New York: Churchill Livingstone;
1996.
c. Chapter in a book: Phillips SJ, Whisnant
JP. Hypertension and stroke. In: Laragh JH,
B r e n n e r B M , e d i t o rs . H y p e r t e n s i o n :
pathophysiology, diagnosis, and management.
2nd ed. New York: Raven Press; 1995. pp. 465-78.
Electronic Sources as reference
Abood S. Quality improvement initiative in
nursing homes: the ANA acts in an advisory role.
Am J Nurs [serial on the Internet]. 2002 Jun [cited
2002 Aug 12];102(6):[about 3 p.]. Available from:
http://www.nursingworld.org/AJN/2002/june/
Wawatch.htm
Foley KM, Gelband H, editors. Improving
palliative care for cancer [monograph on the
Internet]. Washington: National Academy Press;
2001 [cited 2002 Jul 9]. Available from:
http://www.nap.edu/books/0309074029/html/.
Books and Other Monographs
Journal article on the Internet
Monograph on the Internet
Homepage/Web site
Part of a homepage/Web site
Tables
Illustrations (Figures)
Cancer-Pain.org [homepage on the Internet].
New York: Association of Cancer Online
Resources, Inc.; c2000-01 [updated 2002 May 16;
c i t e d 2 0 0 2 J u l 9 ] . A v a i l a b l e f r o m :
http://www.cancer-pain.org/.
American Medical Association [homepage on
the Internet]. Chicago: The Association; c1995-
2002 [updated 2001 Aug 23; cited 2002 Aug 12].
AMA Office of Group Practice Liaison; [about 2
screens]. Available from: http://www.ama-
assn.org/ama/pub/category/1736.html
lTables should be self-explanatory and should
not duplicate textual material.
lTables with more than 10 columns and 25 rows
should be avoided.
lNumber tables, in Arabic numerals,
consecutively in the order of their first citation
in the text and supply a brief title for each.
lPlace explanatory matter in footnotes, not in
the heading.
lExplain in footnotes all non-standard
abbreviations that are used in each table.
lObtain permission for all fully borrowed,
adapted, and modified tables and provide a
credit line in the footnote.
lFor footnotes use the following symbols, in
this sequence: *, †, ‡, §, ||,¶ , **, ††, ‡‡
lTables with their legends should be provided
at the end of the text after the references. The
tables along with their number should be cited
at the relevant place in the text
lUpload the images in JPEG format. The file size
should be within 2 MB in size while uploading.
Anaesthesiology M.P. 35

lFigures should be numbered consecutively
according to the order in which they have
been first cited in the text.
lLabels, numbers, and symbols should be clear
and of uniform size. The lettering for figures
should be large enough to be legible after
reduction to fit the width of a printed column.
lSymbols, arrows, or letters used in
photomicrographs should contrast with the
background and should be marked neatly
with transfer type or by tissue overlay and not
by pen.
lTitles and detailed explanations belong in the
legends for illustrations not on the
illustrations themselves.
lWhen graphs, scatter-grams or histograms
are submitted the numerical data on which
they are based should also be supplied.
lThe photographs and figures should be
trimmed to remove all the unwanted areas.
lIf photographs of individuals are used, their
pictures must be accompanied by written
permission to use the photograph.
lIf a figure has been published elsewhere,
acknowledge the original source and submit
written permission from the copyright holder
to reproduce the material. A credit line should
appear in the legend for such figures.
lLegends for illustrations: Type or print out
legends (maximum 40 words, excluding the
credit line) for illustrations using double
spacing, with Arabic numerals corresponding
to the illustrations. When symbols, arrows,
numbers, or letters are used to identify parts
of the illustrations, identify and explain each
one in the legend. Explain the internal scale
(magnification) and identify the method of
staining in photomicrographs.
lFinal figures for print production: If the
uploaded images are not printable quality, the
publisher office may request for higher
resolution images which can be sent at the
time of acceptance of the manuscript. Send
sharp, glossy, un-mounted, color photographic
prints, with height of 4 inches and width of 6
inches at the time of submitting the revised
manuscript. Print outs of digital photographs
are not acceptable. If digital images are the
only source of images, ensure that the image
has minimum resolution of 300 dpi or 1800 x
1600 pixels in TIFF format. Send the images on
a CD. Each figure should have a label pasted
(avoid use of liquid gum for pasting) on its back
indicating the number of the figure, the
running title, top of the figure and the legends
of the figure. Do not write the contributor/s’
name/s. Do not write on the back of figures,
scratch, or mark them by using paper clips.
lThe Journal reserves the right to crop, rotate,
reduce, or enlarge the photographs to an
acceptable size.
In case of clinical studies which involves patient,
Identifying information should not be published in
written descriptions, photographs, sonograms, CT
scans, etc., and pedigrees unless the information is
essential for scientific purposes and the patient (or
parent or guardian, wherever applicable) gives
written informed consent for publication. Authors
should remove patients' names from figures unless
they have obtained written informed consent from
the patients. When informed consent has been
obtained, it should be indicated in the article and
copy of the consent should be attached with the
covering letter.
Protection of patients Rights to Privacy
Anaesthesiology M.P.36


















