![Journal Name: International Journal of Hepatobiliary and … · 2018. 12. 7. · 96 Endoscopic retrograde cholangiopancreatography [ERCP] ... 98 biopsy and confirm the diagnosis.](https://static.fdocuments.net/doc/165x107/60d37e520da2ff39e45fd202/journal-name-international-journal-of-hepatobiliary-and-2018-12-7-96-endoscopic.jpg)
Journal Name: International Journal of Hepatobiliary and … · 2018. 12. 7. · 36 Endoscopic...
12
Manuscript Accepted Early View Article Page 1 of 12 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD) Type of Article: Case Report Title: Subcapsular Left Hepatic Lobe Hematoma: A potentially life-threatening post-ERCP complication. Case report Authors: Alzubaidi AM, Alshadadi AA, Atta MF, Alsareii SA doi: To be assigned Early view version published: May 9, 2017 How to cite the article: Alzubaidi AM, Alshadadi AA, Atta MF, Alsareii SA. Subcapsular Left Hepatic Lobe Hematoma: A potentially life-threatening post-ERCP complication. Case report. International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD). Forthcoming 2017. Disclaimer: This manuscript has been accepted for publication. This is a pdf file of the Early View Article. The Early View Article is an online published version of an accepted article before publication in the final form. The proof of this manuscript will be sent to the authors for corrections after which this manuscript will undergo content check, copyediting/proofreading and content formatting to conform to journal’s requirements. Please note that during the above publication processes errors in content or presentation may be discovered which will be rectified during manuscript processing. These errors may affect the contents of this manuscript and final published version of this manuscript may be extensively different in content and layout than this Early View Article.
Transcript of Journal Name: International Journal of Hepatobiliary and … · 2018. 12. 7. · 36 Endoscopic...
-
Manuscript Accepted Early View Article
Page 1 of 12
Early View Article: Online published version of an accepted article before publication in the
final form.
Journal Name: International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD)
Type of Article: Case Report
Title: Subcapsular Left Hepatic Lobe Hematoma: A potentially life-threatening post-ERCP
complication. Case report
Authors: Alzubaidi AM, Alshadadi AA, Atta MF, Alsareii SA
doi: To be assigned
Early view version published: May 9, 2017
How to cite the article: Alzubaidi AM, Alshadadi AA, Atta MF, Alsareii SA. Subcapsular
Left Hepatic Lobe Hematoma: A potentially life-threatening post-ERCP complication. Case
report. International Journal of Hepatobiliary and Pancreatic Diseases (IJHPD).
Forthcoming 2017.
Disclaimer: This manuscript has been accepted for publication. This is a pdf file of the
Early View Article. The Early View Article is an online published version of an accepted
article before publication in the final form. The proof of this manuscript will be sent to the
authors for corrections after which this manuscript will undergo content check,
copyediting/proofreading and content formatting to conform to journal’s requirements.
Please note that during the above publication processes errors in content or presentation
may be discovered which will be rectified during manuscript processing. These errors may
affect the contents of this manuscript and final published version of this manuscript may
be extensively different in content and layout than this Early View Article.
-
Manuscript Accepted Early View Article
Page 2 of 12
TYPE OF ARTICLE: Case Report 1
2
TITLE: Subcapsular Left Hepatic Lobe Hematoma: A potentially life-threatening 3
post-ERCP complication. Case report 4
5
AUTHORS: 6
Alzubaidi AM1, Alshadadi AA 1, Atta MF1, Alsareii SA2 7
8
AFFILIATIONS: 9 1King Khalid Hospital –Najran/Gastroenterology /Saudi Arabia 10 2Faculty of Medicine –Surgical Department -Najran University /Saudi Arabia 11
12
CORRESPONDING AUTHOR DETAILS 13
Dr.Ali Mothanna Saleh Al-zubaidi 14
Consultant Gastroenterology & Hepatology King Khalid hospital –Najran 15
Clinical Assistant Professor Faculty of Medicine/Najran University /Saudi Arabia 16
Email: [email protected] 17
18
Short Running Title: NOT GIVEN 19
20
Guarantor of Submission : The corresponding author is the guarantor of 21
submission. 22
23
24
25
26
27
28
29
30
31
-
Manuscript Accepted Early View Article
Page 3 of 12
TITLE: Subcapsular Left Hepatic Lobe Hematoma: A potentially life-threatening 32
post-ERCP complication. Case report 33
34
ABSTRACT 35
Endoscopic retrograde cholangiopancreatography (ERCP) is minimally invasive 36
procedure commonly performed for biliary and pancreatic diseases. According to the 37
literature, the most common related complication are: pancreatitis, post-38
sphincterotomy bleeding, perforation and cholangitis, This is rare and exceptional 39
ERCP complication and only few cases have been reported.We report a case of 40
rare post-ERCP complication, subcapsular liver hematoma that was diagnosed 16 41
hour post-ERCP in 28-year old lady with intra-abdominal collection, U/S guided 42
drainage of suspected bile leak was done ,but the drained fluid was bloody, with 43
total amount of 900ml in the first 36 hours (Analysis its blood mixed with bile), 44
Patient received 2unit packed RBCs and she maintain her vital sign and 45
Hemoglobin at 8.5g/dl. 46
CT Abdomen was done and revealed large left hepatic lobe subcapsular hematoma 47
16 x7 x 12 cm with no active bleeding causing compression of the left hepatic 48
vessels. 49
On the basis of laboratory, clinical, and hemodynamic parameters the patient was 50
hemodynamically stable. She was managed conservatively with only U/S guided 51
drained of abdominal collection and no any radiological or surgical intervention 52
needed for the hematoma. 53
54
Keywords: Endoscopic Retrograde cholangiopancreatography, Subcapsular 55
hematoma, post-ERCP complication. 56
57
58
59
60
61
62
-
Manuscript Accepted Early View Article
Page 4 of 12
TITLE: Subcapsular Left Hepatic Lobe Hematoma: A potentially life-threatening 63
post-ERCP complication. Case report 64
65
INTRODUCTION 66
Endoscopic retrograde cholangiopancreatography (ERCP) is one of the most 67
frequently performed therapeutic procedures for biliary and pancreatic diseases. 68
ERCP-related complications around 2.5% to 9%, with a mortality rate ranging from 69
0.6% to 1 %.[1]. Post-ERCP Pancreatitis, perforation, cholangitis and post-70
sphincterotomy bleeding are the most frequently described complications 71
[2,3].Rare unexpected post-ERCP complication such as Subcapsular hepatic 72
hematoma was firstly described in 2000 [4].although it's rare but its potential life 73
threatening condition.We report an unusual case of left hepatic lobe subcapsular 74
hematoma after ERCP presenting with a drop in hemoglobin, tachycardia and intra-75
abdominal collection. 76
77
CASE REPORT 78
A 28-year-old female patient was referred to us as a case of obstructive jaundice 79
caused by common hepatic duct stricture misdiagnosed as choledocholithiasis by 80
ultrasound abdomen. She was admitted for ERCP. Proper biliary drainage was done 81
after dilatation of common hepatic duct stricture by dilator catheter up to 10 French 82
with the placement of plastic stent 10french 10cm length without immediate 83
complications(Figure1Arrow A), the Second day after the procedure the patient 84
complained of mild abdominal pain and fullness in the epigastric area. She 85
developed tachycardia (PR 115 beats per minute & BP = 100/60mmHg) with a drop 86
of hemoglobin of 2g/dl without melena or hematemesis. 87
Laboratory tests revealed a normal white blood cell count (8.5× 109/L) and drop in 88
hemoglobin level (from 9 to7 g/dL),platelets = 243,INR = 1.4 ,total bilirubin = 214 89
umol/L, direct bilirubin = 176 umol, AST = 55 u/L , ALT = 60 u/l,ALP = 174 u/L, GGT 90
= 90 u/L and Normal S.Amylase level. 91
Abdominal U/S Showed free fluid in the abdomen with a subscapular liver collection. 92
U/S guided drainage of suspected bile leak was done it drained (Figure1Arrow b). 93
Bloody fluid with a total amount of 900ml drained in the first 36 hours (Analysis its 94
-
Manuscript Accepted Early View Article
Page 5 of 12
blood mixed with bile), four days there after the drain became dry after which the 95
abdominal catheter was removed. The patient received 2 unit of packed RBCs and 96
she maintained her vital signs and Hb around 8.5g/dl. CT Abdomen was done and 97
revealed large left hepatic lobe subcapsular hematoma 16*7*12 cm with no active 98
bleeding causing compression of the left hepatic vein with capsule tension (Figure2). 99
The patient was kept on broad spectrum antibiotics. On the third day, she 100
complained of abdominal discomfort and vomiting which could be attributed to 101
compression of the stomach and proximal duodenum by the hematoma as shown in 102
(Figure3). 103
On the basis of the laboratory, clinical, and hemodynamic parameters; the patient 104
was hemodynamically stable. She was managed conservatively with only U/S guided 105
drained of abdominal collection and no any radiological or surgical intervention 106
needed for the hematoma. 107
Her follow-up CT abdomen at day 8 showed most of the hematoma organized 108
(Figure4). And patient discharged home at day 20 of hospitalization with close follow-109
up in OPD. 110
111
DISCUSSION 112
Subcapsular hepatic hematoma is a rare unexpected and potentially life-threatening 113
complication after ERCP. It was firstly described by Ortega et al.[ 4 ]in 2000 who 114
diagnosed subcapsular hematoma in 81-year-old man with abdominal pain after 115
ERCP for CBD stone. 116
The etiology of the hematoma is not entirely clear. Most of the authors claimed that it 117
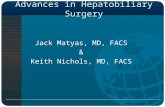
is caused by rupture of small caliber vessels due to the guide wire trauma [5,6,7 ]. In 118
our case guide, wire is the most probable cause as it appears in (Figure5). 119
Abdominal pain associated with hypotension and tachycardia after ERCP should 120
raise the suspicion of intrahepatic bleeding with capsule distension. Different 121
symptoms are described in literature: abdominal pain (91%), hypotension (39.1%), 122
anemia (39.1%), fever (21.7%) and peritonism (13%) [8 ].In our case patient has 123
epigastric pain, anemia, tachycardia and vomiting which could be attributed to 124
stomach & duodenal compression. CT and ultrasound are the gold standard 125
radiological modalities for diagnosis and surveillance of this complication [9]. 126
-
Manuscript Accepted Early View Article
Page 6 of 12
No laboratory test provide reliable indicators of the development of a subcapsular 127
hepatic hematoma, except for a decrease in the hemoglobin level[10.11].The 128
Management is conservative for most of the cases as we did in our case. As the 129
Glisson’s capsule of the liver-confined the hematoma and prevents more bleeding. 130
However large hematomas may require percutaneous drainage for symptomatic 131
relief [12,7]. Management of the 25 cases reported up to now (41.5% cases 132
conservative, percutaneous drainage (25%), Embolization (21%), and surgical 133
intervention only in three cases 12.5%). As the guide wire may be sources of 134
infection we recommend prophylactic broad spectrum antibiotics for these patients to 135
prevent hematoma infection and abscess formation. In our case hematoma did not 136
increase and hemodynamics of the patient remained stable, so she did not require 137
embolization or surgical intervention. 138
In the case of hemodynamic instability, different therapeutic approaches including 139
minimally invasive radiological intervention such as selective vessels embolization 140
showed high success rates[13]. Surgical approach consist of hematoma evacuation, 141
local hemostasis with electrocoagulation or hemostatic devices, or packing in case of 142
massive hemorrhage[14] 143
144
CONCLUSION 145
Rare ERCP complications like liver subcapsular hematoma must be kept in mind if 146
the patient complains of right upper quadrant pain or develops hemodynamic 147
instability. Treatment is mostly conservative. As the guide wire may be sources of 148
infection we suggest prophylactic antibiotic because hematoma is liable to get 149
infection and abscess formation, with follow-up by serial CT scans. 150
Hepatic artery embolization and surgery should be performed early in case of 151
hemodynamic instability or increasing size of hematoma. We concluded that guide 152
wire injury of the hepatic vessels is the most probably causative agent and 153
avoidance of deep insertion of the guide wire may decrease the risk of such 154
catastrophic complication. 155
156
157
158
-
Manuscript Accepted Early View Article
Page 7 of 12
CONFLICT OF INTEREST 159
Ali Mothanna Al-zubaidi, Abdulfattah A Alshadadi, Muhammad Farook Atta and 160
Saeed Alsareii declare no conflicts of interests. 161
162
AUTHOR’S CONTRIBUTIONS 163
NOT GIVEN 164
165
REFERENCES 166
1. Zizzo M, Lanaia A, Barbieri I, Zaghi C, Bonilauri S. Subcapsular Hepatic 167
Hematoma After Endoscopic Retrograde Cholangiopancreatography: A Case 168
Report and Review of Literature. Medicine (Baltimore) [Internet]. Wolters 169
Kluwer Health; 2015 Jul [cited 2016 Dec 30]; 94(26):e1041. Available from: 170
http://www.ncbi.nlm.nih.gov/pubmed/26131812 171
2. Cotton PB, Garrow DA, Gallagher J, Romagnuolo J. Risk factors for 172
complications after ERCP: a multivariate analysis of 11,497 procedures over 173
12 years. Gastrointest Endosc [Internet]. 2009 Jul [cited 2016 Dec 30]; 174
70(1):80–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19286178 175
3. Abdel Aziz AM, Lehman GA. Pancreatitis after endoscopic retrograde 176
cholangio-pancreatography. World J Gastroenterol [Internet]. Baishideng 177
Publishing Group Inc; 2007 May 21 [cited 2016 Dec 30]; 13(19):2655–68. 178
Available from: http://www.ncbi.nlm.nih.gov/pubmed/17569133] 179
4. Ortega Deballon P, Fernández Lobato R, García Septiem J, Nieves Vázquez 180
MA, Martínez Santos C, Moreno Azcoita M. Liver hematoma following 181
endoscopic retrograde cholangiopancreatography (ERCP). Surg Endosc 182
[Internet]. 2000 Aug [cited 2016 Dec 30]; 14(8):767. Available from: 183
http://www.ncbi.nlm.nih.gov/pubmed/11287996 184
5. Orellana F, Irarrazaval J, Galindo J, Balbontin P, Manríquez L, Plass R, et al. 185
Subcapsular hepatic hematoma post ERCP: a rare or an underdiagnosed 186
complication? Endoscopy [Internet]. © Georg Thieme Verlag KG; 2012 Apr 4 187
[cited 2016 Dec 30]; 44(S 02):E108–9. Available from: http://www.thieme-188
connect.de/DOI/DOI?10.1055/s-0031-1291493 189
-
Manuscript Accepted Early View Article
Page 8 of 12
6. Petit-Laurent F, Scalone O, Penigaud M. Sub-capsular hepatic hematoma 190
after ERCP: case report and literature review. Gastroenterol Clin Biol. 2007; 191
31:750–2. 192
7. Bhati C, Inston N, Wigmore S. Subcapsular intrahepatic hematoma: an 193
unusual complication of ERCP. Endoscopy [Internet]. © Georg Thieme Verlag 194
KG Stuttgart · New York; 2007 Dec [cited 2016 Dec 30]; 39(S 1):E150–E150. 195
Available from: http://www.thieme-connect.de/DOI/DOI?10.1055/s-2007-196
966241 197
8. Marco Antonio Zappa, Alberto Aiolfi, Ilaria Antonini, Cinzia Domenica 198
Musolino, and Andrea Porta; Subcapsular hepatic haematoma of the right 199
lobe following endoscopic retrograde cholangiopancreatography: Case report 200
and literature review. World J Gastroenterol. 2016 May 7; 22(17): 4411–201
4415. 202
9. Priego P, Rodríguez G, Mena A, Losa N, Aguilera A, Ramiro C, et al. 203
Hematoma subcapsular hepático tras CPRE. Rev Española Enfermedades 204
Dig. Sociedad Española de Patología Digestiva / Arán Ediciones, S.L.; 2007; 205
99(1):53–4. 206
10. Cardenas A, Crespo G, Balderramo D, Bordas JP, Sendino O, Llach J. 207
Subcapsular liver hematoma after Endoscopic Retrograde 208
Cholangiopancreatography in a liver transplant recipient. Ann Hepatol 209
[Internet]. 2008; 7(4):386–8. Available from: 210
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&do211
pt=Citation&list_uids=19034242 212
11. Klímová K, Suárez CP, Asanza CG, Peña AM, Arregui EC, Alonso AH. 213
Subcapsular Hepatic Hematoma after ERCP: A Case Report and Revision of 214
Literature. 2014; (March):161–66. 215
12. Fei B-Y, Li C-H. Subcapsular hepatic haematoma after endoscopic retrograde 216
cholangiopancreatography: an unusual case. World J Gastroenterol [Internet]. 217
2013 Mar 7 [cited 2016 Dec 30]; 19(9):1502–4. Available from: 218
http://www.wjgnet.com/1007-9327/full/v19/i9/1502.htm 219
13. Solmaz A, Gülçiçek O.B, Erçetin C, Yiğitbaş H, Biricik A,Yavuz E, Sevim E, 220
Çelebi F ÇA. SUBCAPSULAR HEPATIC HEMATOMA FOLLOWING 221
-
Manuscript Accepted Early View Article
Page 9 of 12
ENDOSCOPIC RETROGRADE CHOLANGIOPANCREATOGRAPHY. J Case 222
Reports [Internet]. 2016 Jan 30 [cited 2017 Jan 12];6(1):40–3. Available from: 223
http://www.casereports.in/articles/6/1/Subcapsular-Hepatic-Hematoma-224
Following-Endoscopic-Retrograde-Cholangiopancreatography.html 225
14. González-López R, García-Cano E, Espinosa-González O, Cruz-Salgado Á, 226
Montiel-Jarquin Á-J, Hernández-Zamora V. Tratamiento quirúrgico para 227
hematoma subcapsular hepático posterior a colangiografía retrógrada 228
endoscópica; caso inusual. Cir Cir [Internet]. 2015 Nov [cited 2017 Jan 12]; 229
83(6):506–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26319688 230
231
FIGURE LEGENDS 232
233
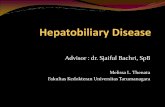
Figure 1: Plain CT shows plastic CBD stent (A)- lobe and intra-abdominal drain (B)- 234
in place 235
236
Figure 2: CT abdomen shows left liver Subcapsular Hematoma (Arrow) 237
238
Figure 3: Shows the hematoma reaching to the left abdominal wall causing 239
compression of the stomach and proximal small bowel. 240
241
Figure 4: Abdominal CT day 8 shows heterogeneous hematoma due to clot 242
formation. 243
244
Figure 5: Deeply inserted ERCP Guide wire 0.035 inch into left liver lobe 245
246
247
248
249
250
251
252
253
-
Manuscript Accepted Early View Article
Page 10 of 12
FIGURES 254
255
256
257
Figure 1: Plain CT shows plastic CBD stent (A)- lobe and intra-abdominal drain (B)- 258
in place 259
260
261
262
Figure 2: CT abdomen shows left liver Subcapsular Hematoma (Arrow) 263
264
A
B
-
Manuscript Accepted Early View Article
Page 11 of 12
265
266
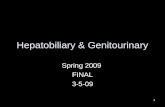
Figure 3: Shows the hematoma reaching to the left abdominal wall causing 267
compression of the stomach and proximal small bowel. 268
269
270
271
Figure 4: Abdominal CT day 8 shows heterogeneous hematoma due to clot 272
formation. 273
274
Liver subcapsular hematoma causing
compression of the stomach
Compressed stomach
-
Manuscript Accepted Early View Article
Page 12 of 12
275
276
Figure 5: Deeply inserted ERCP Guide wire 0.035 inch into left liver lobe 277