Journal Club vesico ureteral reflux
50
Journal club Vesicoureteric re ux in children fl Kjell Tullus Lancet 2015; 385: 371–79
-
Upload
jiten-jaipuria -
Category
Documents
-
view
226 -
download
0
description
VUR latest journal club
Transcript of Journal Club vesico ureteral reflux

Journal club
Vesicoureteric reflux in children
Kjell TullusLancet 2015; 385: 371–79

introduction
• VUR – febrile UTI and post infection scarring• Trends are changing with accumulating evidence

spearheaders
UK National Institute for Health and Care Excellence and theAmerican Academy of Pediatrics no longer recommendradiological investigations to detect vesicoureteric reflux
Worldover MCUGs are being done less and less

Epidemiology
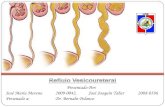
• Vesicoureteric reflux is defined as the back flow of urine from the urinary bladder into one or both ureters, the renal pelvises, or both. Severity is graded in different ways.

International Reflux Study in Children

What should rt grade 3 and left grade 4 reflux be graded as• 3• 4• 3+4/2• 3 and 4

Is VUR common / uncommon / rare
What could be the community incidence of VUR in healthy children?1%, 10%, 20%, 30%

• MCUG data from 102 urologically normal infants and children from 1967 showed that as many as 65% of the infants displayed reflux in the first 6 months of life.• The rate gradually decreased until at the age of 5 years none of the
investigated children showed vesicoureteric reflux.

What about data from patients with UTI

Further surprises

What about siblings?

Final verdict on prevalence of VUR
• 25%-40%

Cause of VUR
• Physiological?• Vesicoureteric reflux can be caused by abnormal positioning of the
ureteral orifice, which seems to arise from abnormal ureteric budding, dysfunctional interaction between the ureteric bud and metanephric mesenchyme, or both.
• Genetically heterogeneous• Chr 1

Secondary VUR – lower urinary tract dysfunction?• Considerations• Cause / effect• prognosis

Investigations?
• VCUG/MCUG – gold standard• How soon should it be done after UTI?

Radionuclide studies
• 74% sensitive 91% specific• Indirect studies - Only to be done in toilet trained children• Direct studies – non toilet trained infants/neonates• MAG 3• No anatomical detail

USG
• Best initial investigation to direct further investigations• To detect VUR … SF6
• Sensitivity – 57-100%• Specificity – 85-100%

Ureteric Doppler waveforms• Sensitivity/specificity – 88.5/82.3 compared to urosonography

Discussion on mechanisms working at VUJ

Renal scarring and VUR
Vesicoureteric reflux, especially of a high grade, is clearly associated with renal parenchymal damage.IVP vs DMSACongenital dysplasia vs scarsWhich one dominatesBoys vs girls

Long term consequences of scarring?• Progression to ESRD• I case of ESRD/10,000 UTI episodes

Effect on kidney function

Blood pressure

Complications of pregnancy….• Conflicting data

Final verdict
• Long term consequences are lower than thought

Natural history of VUR – 38 vs 156

Timing of imaging
• When to do VCUGAAPMCUG should not be performed routinely after the first febrile urinary tract infection in children aged 2 months to 2 years unless ultrasonography reveals hydronephrosis, scarring or other findings suggestive of high-grade vesicoureteric reflux or obstructive uropathy or other atypical or complex clinical disorders.


EAU
• < 2 yrs + first febrile UTI
• Top down approach??

Which approach best?


treatment
• Aim of treatment?• Most will initially favour conservative therapy

Prophylactic antibiotics
• Evidence from RCT’s weak and conflicting


Swedish reflux trial



RIVUR study

Meta analyses

Risk of resistance and choice of antibiotic• Niftran??

BBD??

Final verdict – EAU and AUA
• European Association of Urology state that antibiotic prophylaxis is indicated only in cases of UTI with specific risk factors such as young age, high-grade reflux, lower urinary tract dysfunction, circumcision status, female gender, and status of toilet-training.
• AUA - CAP recommended <1 yr + febrile UTI <1yr + dilating VUR >1 yr + BBD, recurrent UTI or renal cortical abnormalities CAP optional <1 yr + non dilating VUR

Ureteric reimplantation
• Success 92-98%• Meta-analyses – CAP vs Surgery


Bulking agents – agents and technique

Bulking agents - repetition

Bulking agents - considerations
• Duplicated ureter• Neurogenic bladder• BBDPredictors of obstructionThese include dysfunctional voiding, myelomeningocelewith neurogenic bladder, ureteral duplications,transplanted kidneys, and dilated obstructive ureters inthe absence of diagnosis

circumcision
• Circumcision of healthy infant boys has been associated with significantly reduced numbers of cases of acute pyelonephritis, which can lead to renal scarring.• A metaanalysis of more than 400 000 boys showed that the odds
ratio for circumcised boys was 0·13 (95% CI 0·08–0·20).
• The data are much weaker in children with urological malformations, such as high-grade vesicoureteric reflux, but do still suggest a benefit.

Sibling screening
• EAU – no need in toilet trained• AUA - recommends screening of siblings who have evidence of renal
cortical abnormalities, renal size asymmetry, or a sibling with a urinary tract infection.• Optional to observe in toilet trained

Thank you