Journal Club On Combination Flap Surgery with Resin-Modified Glass Ionomer for the Treatment of...
37
-
Upload
shilpa-shiv -
Category
Health & Medicine
-
view
462 -
download
0
Transcript of Journal Club On Combination Flap Surgery with Resin-Modified Glass Ionomer for the Treatment of...


Combination Flap Surgery with Resin-Modified Glass Ionomer for the Treatment of Radicular Lesions: A Long-Term Follow-upLuis A et al, Int J Periodontics Restorative Dent 2013.
Shilpa Shivanand
II MDS

Introduction • Subgingival radicular lesions and non-carious cervical lesions
(NCCLs) present a great challenge to clinicians.
• Current treatment for NCCLs varies from conservative subgingival restoration to a more advanced periodontal flap.
• Nonsurgical treatment of subgingival lesions is challenging due to limited visualization and moisture contamination of restorative materials.
• Amalgam and composite resin, although frequently elected as the restorative materials to treat subgingival lesions, elicit a severe gingival inflammatory response and do not allow periodontal attachment on their surface.
Gomes SC, Miranda LA et al, 2005.

Introduction….
• Periodontal attachment loss and furcation involvement are common adverse side effects of using restorative materials that are not biocompatible.
Valderhaug J, 1980
• Surgical crown lengthening compromises periodontal attachment and the overall esthetic results.
• As a result, some of these teeth affected by radicular lesions may be extracted because of the overwhelming restorative and surgical challenges of saving the tooth.

Why RMGI ?
• Resin-modified glass ionomer has been advocated for treating radicular lesions.
• This material consists of a hybrid of traditional glass ionomer with a small portion of light-curing composite resin, resulting in intermediate properties between glass ionomers and resins.
Sidhu SK, Watson TF 1995
• RMGI was developed to overcome the problems of low initial mechanical strength and moisture sensitivity exhibited by conventional glass ionomers.
Burgess JO et al 1993, Hinoura K et al 1991

Why RMGI ? ..
• Resistance to microleakage of RMGI is an important feature in a surgical field where contamination with blood and oral fluid is inevitable.
Tjan AH, Dunn JR 1990, Sidhu SK 1992
• RMGI possesses antibacterial properties through its fluoride release that contribute to the prevention of recurrent caries which is particularly important in a subgingival environment where plaque control is difficult.
Williams et al JA 2001, Dhondt CL et al 2001
• Moreover, periodontal attachment through long junctional epithelium and hemidesmosomes to this material has been shown.
Dragoo MR 1997

Aim
• The present clinical study was undertaken to evaluate the clinical effectiveness and biocompatibility of RMGI in conjunction with flap surgery to treat subgingival radicular lesions.

Materials and Methods
• A review of clinical cases pertaining to the use of an RMGI was performed.
• Patients were treated in a private practice between 1997 and 2010.
• All surgical and restorative procedures as well as clinical measurements were performed by two periodontists.
• This study was approved by the University of Michigan Health Sciences Institutional Review Board.

Clinical Measurements
• Demographic data and clinical parameters were recorded including probing pocket depth (PPD), gingival recession, clinical attachment level (CAL), bleeding on probing (BOP)- as present / absent within 30 sec after probing.
• All measurements were performed using a Marquis periodontal probe (Marquis Dental) and were rounded up to the nearest millimeter.
• The retention of the RMGI in the restorative cavity was also recorded as present or absent.
• All measurements were recorded at baseline (ie, prior to surgery) and at follow-up (ie, following surgery).

Surgical Procedure
• Surgical procedures performed were categorized as either open flap debridement (OFD) or coronallyadvanced flap with or without connective tissue graft (CAF ± CTG).
• CAF ± CTG was performed in cases that exhibited gingival recession with minimal keratinized gingiva and attached gingiva.
• All procedures were performed following the same basic surgical protocol.

Surgical procedure…
• Subjects were anesthetized with a local anesthetic containing vasoconstrictor.
• A full-thickness mucoperiosteal flap was reflected following sulcular incision.
• The radicular defect was reshaped using round carbide burs to remove caries if present and to decontaminate the root surface.
• Hemostasis of the surgical site was achieved using the local anesthetic.
• The RMGI (Geristore, Den-Mat) was placed according to the manufacturer’s recommendations.

Surgical procedure…
• Acid etching with phosphoric acid gel was applied on the root surface for 30 seconds and rinsed off with every attempt to prevent the gel from contacting the bone and connective tissue.
• Multipurpose bonding system (Den-Mat) was applied prior to placement of the RMGI.
• A and B paste were mixed with a syringe tip and gun.
• The material was placed using a plastic instrument while ensuring that all margins were well sealed.
• RMGI was then light cured using a conventional halogen light for 30 seconds.

Surgical procedure…
• Finishing and polishing of the restoration were achieved with a fine-grit flame-shaped diamond bur and curettes.
• The flap was either replaced at its original position in the OFD group or coronally positioned in the CAF ± CTG group and sutured with 4-0 silk and 5-0 gut sutures.
• N-butyl cyanoacrylate was used as needed to achieve additional flap closure and stability.

Conventional OFD + RMGI

CAF ± CTG + RMGI

Post-op Instructions
• Patients were instructed to take analgesics (400 mg ibuprofen every 4 to 6 hours for 3 days) and to discontinue oral hygiene, including tooth brushing and flossing around the surgical areas, for 10 days.
• No antibiotics were prescribed.
• Patients were instructed to rinse twice daily with 0.12% chlorhexidine mouthwash for 2 weeks.
• Sutures were removed after 10 days.
• Periodontal maintenance was performed every 3 to 4 months.

• Cases were considered successful if they exhibited the following:
• (1) periodontal pocket depth ≤ 4 mm
• (2) no progressive clinical attachment loss of more than 2 mm between baseline and follow-up
• (3) absence of symptoms and
• (4) retention of the restorative material.

Statistical Analysis
• Descriptive statistics were expressed as means ±standard error (SE) for parameters collected at baseline and follow-up.
• Radicular lesions were used as the unit of measurement.
• The t test was performed on all clinical parameters (ie, PPD, recession, CAL, BOP) to compare values at baseline to follow-up. (P < 0.05 - statistically significant)
• Chi-square test was used to compare success rates for individual practitioners as well as the association between baseline and follow-up clinical parameters (ie, PPD, CAL, and BOP) with success of the cases.

Results
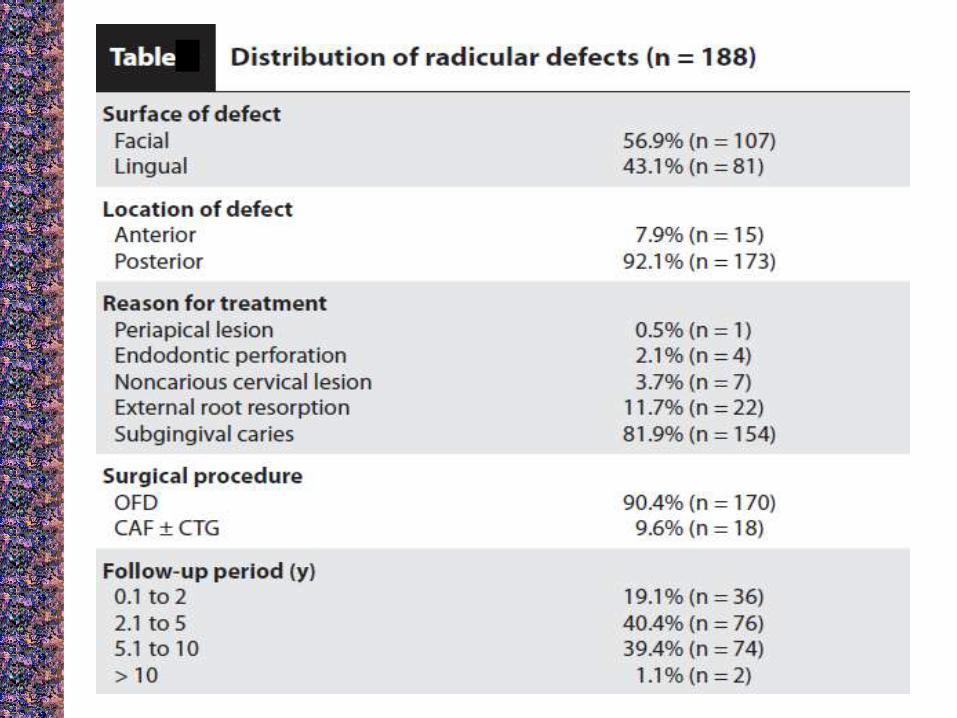
• The study population consisted of 142 patients (66 men and 76 women, mean age: 63.0 ― 0.9 years) with 188 subgingival radicular defects including external root resorption, root caries, endodontic perforation, periapical lesions, and non-carious cervical lesions.
• Patients were followed up for a mean of 4.2 ±0.2 years (up to 13.4 years).
• No adverse events were reported during the observation period.

Results…
• Of the patients, 30.3% (n = 43) were smokers and 14.1% (n = 20) were diagnosed with diabetes.
• OFD alone was used to treat 90.4% (n = 170) of cases, and 9.6% (n = 18) of the cases were treated using the CAF ± CTG approach.

Results…
• After a mean follow-up of 4.2 years, 77.7% (n = 146) of cases treated with OFD were successful and 94.4% (n = 17) of cases treated with CAF ± CTG were successful.
• The overall success rate was 86.7% (163/188) based on the total number of radicular defects.
• When patient is used as the unit of analysis, the overall success rate was 82.4% (117/142).
• Success rates among all operators were similar with no significant differences.


Results…
• Of the 25 cases that failed, 7 (28.0%) were replaced with RMGI, 2 (8.0%) were replaced with another restorative material other than RMGI, and 16 (64.0%) were extracted due to either recurrent caries, vertical fracture, or a devitalized tooth.
• Hence, 9 (36.0%) cases failed due to a loss of retention of the restoration.

Discussion
• Successful treatment of subgingival radicular lesions depends greatly on excellent combined restorative and periodontal procedures.
• Favorable properties of the RMGI were demonstrated by previous in vitro and histologic studies, including its biocompatibility and ability to obtain an attachment through long junctional epithelium and hemidesmosomes.
Dragoo MR 1997, Al-Sabek F et al 2005.

Discussion…
• The current study supports the idea that the attachment on restored roots can be maintained over a mean period of 4.2 years as demonstrated by shallow PPD and CAL gain despite its subgingival location.
• The soft tissue healing of successful cases showed significantly less inflammation, as demonstrated by the decreased BOP at follow-up.
• The presence of BOP in failed cases could be attributed to plaque accumulation on the restorative material, which exacerbates gingival inflammation.
• However, Plaque Index was not measured in this study and, therefore, oral hygiene performance could not be assessed.

Discussion…
• Previous studies have shown good retention of the RMGI in treating Class V lesions.
Santamaria MP et al 2009, Adballa AI 1997
• In this study, 36.0% of failed cases were due to loss of retention of the restoration.
• Within the context of subgingival defects, where access is difficult and contamination is frequent, the combination therapy generated a success rate of 86.7% and is a good alternative to extracting the tooth.
Discussion…
• Furthermore, the CAF ± CTG group generated a success rate of 94.4%, which suggests that it is a valuable technique when presenting options available to treat radicular lesions, despite the smaller number of patients belonging to this group.
• The authors speculate that retention of the RMGI is enhanced with a CAF compared to an OFD due to the formation of a hemidesmosomal attachment to the RMGI and, hence, the inability to damage the subgingival RMGI with instrumentation.
• Whereas in the OFD group, the risk of dislodging the RMGI increases due to mechanical instrumentation during maintenance therapy, which contributes to its lower success rate compared to the CAF ± CTG group.

Conclusion
• This study confirms the successful placement of RMGI onto the root surface to restore function and esthetics in teeth that previously would have been non-restorable.
• The overall success rate of this treatment modality was 86.7%.
• The possibility of achieving clinical attachment gain can be attributed to the advantageous clinical features of this material such as biocompatibility.
• The favorable results of this treatment modality were maintained over a mean period of 4.2 years with a maximum follow-up of 13 years.

Critical Evaluation
• No indices to measure oral hygiene plaque index
• No histologic evaluation done to evaluate soft tissue attachment
• Not considered etiologic factors of patients causing the radicular lesion

Cross References

I. Periodontal Tissue Response to Coverage of Root Cavities Restored With Resin Materials: A
Histomorphometric Study in DogsThiago M.et al, JOP 2007.
AIM: The purpose of this study was to histomorphometrically evaluate the response of periodontal tissues covering Class V resin restorations in dogs.
METHOD: After raising a mucoperiosteal flap, bony defects measuring 5*5 mm were created on the buccal aspect of the canines of five dogs followed by cavity preparations on the root surface measuring 3*3*1 mm. Before repositioning the flap to cover the bone defect, the cavities were restored with composite resin (CR) or resin-modified glass ionomer cement (RMGIC) or were left unrestored as control (C). The dogs were euthanized 90 days after surgery. Specimens comprising the tooth and periodontal tissues were removed, processed routinely, cut into longitudinal serial sections in the buccolingual direction, and stained with hematoxylin and eosin (H&E) or Masson’s trichrome. The most central sections were selected for histomorphometric analysis.

• RESULTS: Histomorphometric analysis revealed apical migration of epithelial tissue onto the restorative materials (RMGIC and CR). The C group presented significantly longer connective tissue attachment (P <0.05) than the RMGIC and CR groups and significantly higher bone regeneration (P <0.05) compared to the RMGIC group. Histologically, the cervical third (CT) of all groups had the most marked chronic inflammatory infiltrate.
• CONCLUSION: Within the limits of this study, it can be concluded that the restorative materials used exhibit biocompatibility; however, both materials interfered with the development of new bone and the connective tissue attachment process.

II. Preferential Attachment of Human Gingival Fibroblasts to the Resin Ionomer Geristore
Al Sabek et al , J Endodontics 2005.
ABSTRACT: The resin ionomer Geristore has been used extensively for root perforation repairs. The purpose of this study was to evaluate oral in vitro biocompatibility of the resin ionomer Geristore compared to two other dental perforation repair materials, Ketac-Fil and Immediate Restorative Material (IRM). Growth and morphology of human gingival fibroblasts (HGFs) was determined using scanning electron microscopy (SEM) of HGFs cells grown on test materials as well as cytotoxicity assays using elutes from test materials.

CONCLUSION: SEM analysis showed that HGFs attached and spread well over Geristore with relatively normal morphology. SEM showed that fibroblasts did not attach and spread well over Ketac-Fil or IRM as cells appeared much fewer with rounded and different morphology than fibroblasts grown on Geristore. Cytotoxicity assays indicated that HGFs proliferated in the presence of Geristore elutes and not in the presence of Ketac-Fil or IRM elutes. In vitro interpretation indicates that Geristore is less cytotoxic to gingival fibroblasts.