Joints Chapter 8. Joints (Articulations) Articulation—site where two or more bones meet Functions...
72
Joints Chapter 8
-
Upload
brandon-armstrong -
Category
Documents
-
view
241 -
download
0
Transcript of Joints Chapter 8. Joints (Articulations) Articulation—site where two or more bones meet Functions...

JointsChapter 8
Joints (Articulations)
• Articulation—site where two or more bones meet
• Functions of joints:– Give skeleton mobility– Hold skeleton together

Functional Classification of Joints
• Based on amount of movement allowed by the joint
• Three functional classifications:– Synarthroses—immovable – Amphiarthroses—slightly movable – Diarthroses—freely movable

Structural Classification of Joints
• Based on binding material and joint cavity• Three structural classifications:– Fibrous– Cartilaginous – Synovial

Fibrous Joints
• Bones joined by dense fibrous connective tissue
• No joint cavity• Most are synarthrotic (immovable)• Three types:– Sutures– Syndesmoses– Gomphoses

Fibrous Joints: Sutures
• Rigid, interlocking joints containing short connective tissue fibers
• Allow for growth during youth
• In middle age, sutures ossify and are called synostoses

Fibrous Joints: Syndesmoses
• Bones connected by ligaments
• Movement varies from immovable to slightly movable
• Examples: – Synarthrotic distal
tibiofibular joint– Diarthrotic interosseous
connection between radius and ulna

Fibrous Joints: Gomphoses
• Peg-in-socket joints of teeth in alveolar sockets
• Fibrous connection is the periodontal ligament

Cartilaginous Joints
• Bones united by cartilage• No joint cavity• Two types:– Synchondroses– Symphyses

Cartilaginous Joints: Synchondroses
• A bar or plate of hyaline cartilage unites the bones
• All are synarthrotic

Cartilaginous Joints: Symphyses
• Hyaline cartilage covers the articulating surfaces and is fused to an intervening pad of fibrocartilage
• Strong, flexible amphiarthroses

Synovial Joints
• All are diarthrotic• Include all limb joints; most joints of the body• Distinguishing features:
1. Articular cartilage: hyaline cartilage2. Joint (synovial) cavity: small potential space3. Articular (joint) capsule: outer fibrous capsule of dense
irregular connective tissue, inner synovial membrane of loose connective tissue
4. Synovial fluid: viscous slippery filtrate of plasma + hyaluronic acid – lubricates and nourished articular cartilage

Figure 8.3
Periosteum
Ligament
Fibrouscapsule
Synovialmembrane
Joint cavity(containssynovial fluid)
Articular (hyaline)cartilage
Articularcapsule

Synovial Joints
Distinguishing features cont:5. Three possible types of reinforcing ligaments:• Capsular (intrinsic)—part of the fibrous capsule• Extracapsular—outside the capsule• Intracapsular—deep to capsule; covered by synovial
membrane
6. Rich nerve and blood vessel supply:• Nerve fibers detect pain, monitor joint position and stretch• Capillary beds produce filtrate for synovial fluid

Synovial Joints: Friction-Reducing Structures
• Bursae:– Flattened, fibrous sacs lined with synovial
membranes – Contain synovial
fluid

Synovial Joints: Friction-Reducing Structures
• Tendon sheath:– Elongated bursa that wraps completely around a
tendon

Stabilizing Factors at Synovial Joints
• Shapes of articular surfaces (minor role)• Ligament number and location (limited role)• Muscle tone– Extremely important in reinforcing shoulder and
knee joints and arches of the foot

Synovial Joints: Movement
• Muscle attachments across a joint:– Origin—attachment to the immovable bone– Insertion—attachment to the movable bone
• Muscle contraction causes the insertion to move toward the origin
• Movements occur along transverse, frontal, or sagittal planes

Synovial Joints: Range of Motion
• Nonaxial—slipping movements only• Uniaxial—movement in one plane• Biaxial—movement in two planes• Multiaxial—movement in or around all three
planes

Synovial Joint Movement:
• Gliding: one flat bone surface glides or slips over another similar surface
• Examples:– Intercarpal joints– Intertarsal joints– Between articular processes of vertebrae

Synovial Joint Movement:
• Angular: (1)movements that occur along the sagittal plane:– Flexion—decreases the angle of the joint– Extension— increases the angle of the joint– Hyperextension—excessive extension beyond
normal range of motion

Synovial Joint Movement
• Angular: (2)movements that occur along the frontal plane:– Abduction—movement
away from the midline– Adduction—movement
toward the midline– Circumduction

Synovial Joint Movement
• Rotation: The turning of a bone around its own long axis– Examples:• Between C1 and C2
vertebrae• Rotation of humerus and
femur

Synovial Joints: Special Movements
• Movements of radius around ulna:– Supination (turning hand
backward)– Pronation (turning hand forward)
• Movements of the foot:– Dorsiflexion (upward movement) – Plantar flexion (downward
movement)

Synovial Joints: Special Movements
• Movements of the foot:– Inversion (turn sole medially)– Eversion (turn sole laterally)
• Movements in a transverse plane:– Protraction (anterior
movement)– Retraction (posterior
movement)

Synovial Joints: Special Movements
• Elevation (lifting a body part superiorly)
• Depression (moving a body part inferiorly)
• Opposition of the thumb– Movement in the saddle
joint so that the thumb touches the tips of the other fingers

Classification of Synovial Joints
• Six types, based on shape of articular surfaces:– Plane– Hinge– Pivot– Condyloid– Saddle– Ball and socket

Plane Joints
• Nonaxial joints• Flat articular surfaces• Short gliding movements

Hinge Joints
• Uniaxial joints • Motion along a single plane• Flexion and extension only

Pivot Joints
• Rounded end of one bone conforms to a “sleeve,” or ring of another bone
• Uniaxial movement only

Condyloid (Ellipsoidal) Joints
• Biaxial joints• Both articular surfaces are oval• Permit all angular movements

Saddle Joints
• Biaxial• Allow greater freedom
of movement than condyloid joints
• Each articular surface has both concave and convex areas

Ball-and-Socket Joints
• Multiaxial joints• The most freely moving synovial joints

Knee Joint• Largest, most complex joint of body• Three joints surrounded by a single joint cavity:– (1)Femoropatellar joint:• Plane joint• Allows gliding motion during knee flexion
– (2,3)Lateral and medial tibiofemoral joints between the femoral condyles and the C-shaped lateral and medial menisci (semilunar cartilages) of the tibia• Allow flexion, extension, and some rotation when knee
is partly flexed

Figure 8.8a
(a) Sagittal section through the right knee joint
Femur
Tendon ofquadricepsfemoris
SuprapatellarbursaPatellaSubcutaneousprepatellar bursaSynovial cavityLateral meniscus
Posteriorcruciateligament
Infrapatellarfat pad Deep infrapatellarbursaPatellar ligament
Articularcapsule
Lateralmeniscus
AnteriorcruciateligamentTibia

Figure 8.8b
(b) Superior view of the right tibia in the knee joint, showing the menisci and cruciate ligaments
Medialmeniscus
Articularcartilageon medialtibialcondyle
Anterior
Anteriorcruciateligament
Articularcartilage onlateral tibialcondyle
Lateralmeniscus
Posteriorcruciateligament

Knee Joint
• At least 12 associated bursae• Capsule is reinforced by muscle tendons:– E.g., quadriceps and semimembranosus tendons
• Joint capsule is thin and absent anteriorly• Anteriorly, the quadriceps tendon gives rise to:– Lateral and medial patellar retinacula– Patellar ligament

Figure 8.8c
Quadricepsfemoris muscle
Tendon ofquadricepsfemoris muscle
Patella
Lateral patellarretinaculum
Medial patellarretinaculum
Tibial collateralligament
Tibia
Fibularcollateralligament
Fibula
(c) Anterior view of right knee
Patellar ligament

Knee Joint
• Capsular and extracapsular ligaments– Help prevent hyperextension
• Intracapsular ligaments: – Anterior and posterior cruciate ligaments– Prevent anterior-posterior displacement– Reside outside the synovial cavity

Figure 8.8d
Articular capsule
Oblique poplitealligament
Lateral head ofgastrocnemiusmuscle
Fibular collateralligament
Arcuate poplitealligament
Tibia
Femur
Medial head ofgastrocnemiusmuscle
Tendon ofsemimembranosusmuscle
(d) Posterior view of the joint capsule,including ligaments
Popliteusmuscle (cut)
Tendon ofadductor magnus
Bursa
Tibial collateralligament

Figure 8.8e
Fibularcollateralligament
Posterior cruciateligament
Medial condyle
Tibial collateralligament
Anterior cruciateligament
Medial meniscus
Patellar ligament
Patella
Quadriceps tendon
Lateral condyleof femur
Lateralmeniscus
Fibula
Tibia
(e) Anterior view of flexed knee, showing the cruciateligaments (articular capsule removed, and quadricepstendon cut and reflected distally)

Figure 8.9
Lateral Medial
Patella(outline)
Tibial collateralligament(torn)
Medialmeniscus (torn)
Anteriorcruciateligament (torn)
Hockey puck

Shoulder (Glenohumeral) Joint
• Ball-and-socket joint: head of humerus and glenoid fossa of the scapula
• Stability is sacrificed for greater freedom of movement

Figure 8.10a
Acromionof scapula
Synovial membraneFibrous capsule
Hyalinecartilage
CoracoacromialligamentSubacromialbursa
Fibrousarticular capsuleTendonsheath
Tendon oflong headof bicepsbrachii muscle
Synovial cavityof the glenoidcavity containingsynovial fluid
Humerus
(a) Frontal section through right shoulder joint

Shoulder Joint
• Reinforcing ligaments:– Coracohumeral ligament—helps support the
weight of the upper limb– Three glenohumeral ligaments—somewhat weak
anterior reinforcements

Shoulder joint• Reinforcing muscle tendons:–Tendon of the long head of biceps:• Travels through the intertubercular
groove • Secures the humerus to the glenoid
cavity– Four rotator cuff tendons encircle the
shoulder joint:• Subscapularis• Supraspinatus• Infraspinatus• Teres minor
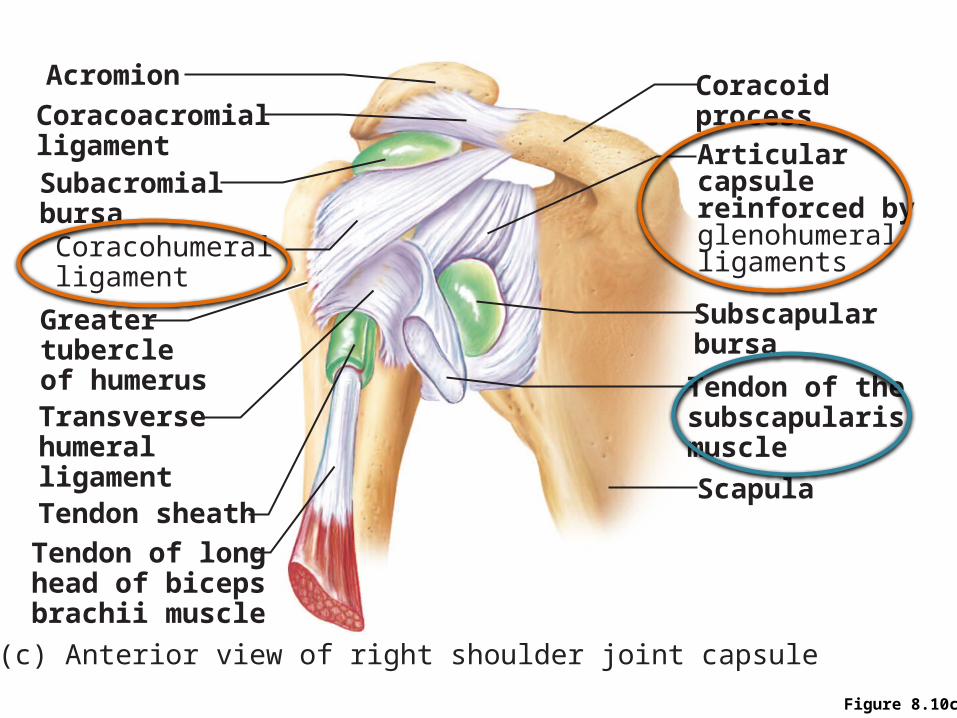
Figure 8.10c
Acromion
CoracoacromialligamentSubacromialbursaCoracohumeralligament
Greatertubercleof humerusTransversehumeralligamentTendon sheath
Tendon of longhead of bicepsbrachii muscle
Articularcapsulereinforced byglenohumeralligaments
Subscapularbursa
Tendon of thesubscapularismuscle
Scapula
Coracoidprocess
(c) Anterior view of right shoulder joint capsule

Figure 8.10d
Acromion
Coracoid process
Articular capsule
Glenoid cavity
Glenoid labrum
Tendon of long headof biceps brachii muscle
Glenohumeral ligaments
Tendon of thesubscapularis muscle
ScapulaPosterior Anterior
(d) Lateral view of socket of right shoulder joint,humerus removed

Elbow Joint
• Radius and ulna articulate with the humerus• Hinge joint formed mainly by trochlear notch
of ulna and trochlea of humerus• Flexion and extension only

Figure 8.11a
Articularcapsule
Synovialmembrane
Synovial cavity
Articular cartilage
Coronoid process
Tendon ofbrachialis muscle
Ulna
Humerus
Fat pad
Tendon oftricepsmuscle
Bursa
Trochlea
Articular cartilageof the trochlearnotch
(a) Median sagittal section through right elbow (lateral view)

Elbow Joint
• Anular ligament—surrounds head of radius• Two capsular ligaments restrict side-to-side
movement:– Ulnar collateral ligament– Radial collateral ligament

Figure 8.11b
Humerus
Lateralepicondyle
Articularcapsule
Radialcollateralligament
Olecranonprocess
Anularligament
Radius
Ulna
(b) Lateral view of right elbow joint

Figure 8.11d
Articularcapsule
Anularligament
Coronoidprocess
(d) Medial view of right elbow
Radius
Humerus
Medialepicondyle
Ulnarcollateralligament
Ulna

Hip (Coxal) Joint
• Ball-and-socket joint• Head of the femur articulates with the
acetabulum• Good range of motion, but limited by the deep
socket • Acetabular labrum—enhances depth of socket

Figure 8.12a
Articular cartilage
Coxal (hip) bone
Ligament ofthe head of the femur (ligamentum teres)
Synovial cavity
Articular capsule
Acetabularlabrum
Femur
(a) Frontal section through the right hip joint

Hip Joint
Reinforcing ligaments:• Iliofemoral ligament• Pubofemoral ligament• Ischiofemoral ligament• Ligamentum teres

Figure 8.12c
Ischium
Iliofemoralligament
Ischiofemoralligament
Greatertrochanterof femur
(c) Posterior view of right hip joint, capsule in place

Figure 8.12d
Anterior inferioriliac spine
Iliofemoralligament
Pubofemoralligament
Greatertrochanter
(d) Anterior view of right hip joint, capsule in place

Temporomandibular Joint (TMJ)
• Mandibular condyle articulates with the temporal bone
• Two types of movement– Hinge—depression and elevation of mandible– Gliding—e.g. side-to-side (lateral excursion)
grinding of teeth• Most easily dislocated joint in the body

Figure 8.13a
Zygomatic process
Mandibular fossaArticular tubercle
Infratemporal fossa
Externalacousticmeatus
Articularcapsule
Ramus ofmandible
Lateralligament
(a) Location of the joint in the skull

Figure 8.13b
Articularcapsule
Mandibularfossa
Articular discArticulartubercle
Superiorjointcavity
Inferior jointcavity
Mandibularcondyle
Ramus ofmandible
Synovialmembranes
(b) Enlargement of a sagittal section through the joint

Figure 8.13c
Lateral excursion: lateral (side-to-side) movements of the mandible
Outline ofthe mandibularfossa
Superior view
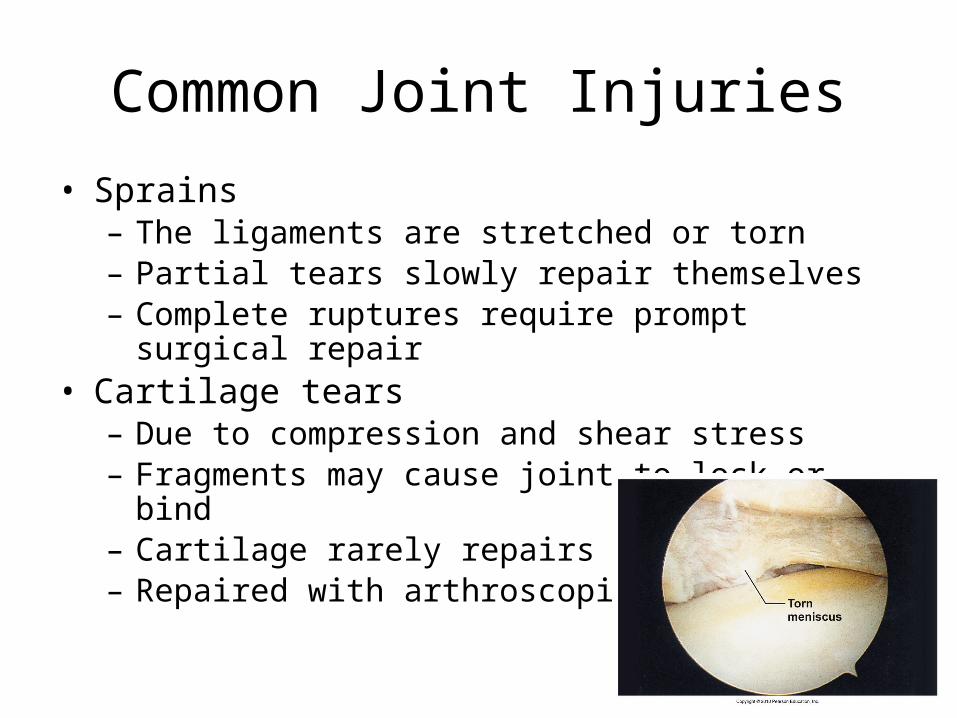
Common Joint Injuries• Sprains– The ligaments are stretched or torn– Partial tears slowly repair themselves– Complete ruptures require prompt surgical repair
• Cartilage tears– Due to compression and shear stress– Fragments may cause joint to lock or bind– Cartilage rarely repairs itself– Repaired with arthroscopic surgery

Common Joint Injuries
• Dislocations (luxations)– Occur when bones are forced out
of alignment– Accompanied by sprains,
inflammation, and joint immobilization
– Caused by serious falls or playing sports
• Subluxation—partial dislocation of a joint

Inflammatory and Degenerative Conditions
• Bursitis– An inflammation of a bursa, usually caused by a
blow or friction– Treated with rest and ice and, if severe, anti-
inflammatory drugs• Tendonitis– Inflammation of tendon sheaths typically caused
by overuse– Symptoms and treatment similar to bursitis

Arthritis
• >100 different types of inflammatory or degenerative diseases that damage joints
• Most widespread crippling disease in the U.S.• Symptoms; pain, stiffness, and swelling of a
joint• Acute forms: caused by bacteria, treated with
antibiotics• Chronic forms: osteoarthritis, rheumatoid
arthritis, and gouty arthritis

Osteoarthritis (OA)
• Common, irreversible, degenerative (“wear-and-tear”) arthritis
• 85% of all Americans develop OA, more women than men
• Probably related to the normal aging process• More cartilage is destroyed than replaced in badly
aligned or overworked joints• Exposed bone ends thicken, enlarge, form bone spurs,
and restrict movement• Treatment: moderate activity, mild pain relievers,
capsaicin creams, glucosamine and chondroitin sulfate

Rheumatoid Arthritis (RA)
• Chronic, inflammatory, autoimmune disease of unknown cause
• Onset: 40 -50 years• 3x more women• Signs and symptoms include joint pain and
swelling (usually bilateral), anemia, osteoporosis, muscle weakness, and cardiovascular problems

Rheumatoid Arthritis
• Synovitis, inflammation, pannus formation, cartilage erosion, scar tissue forms, bones connect (ankylosis)

Gouty Arthritis
• Uric acid crystals in joints and soft tissues, inflammation
• More common in men • Typically affects the joint at the base of the great toe
• In untreated gouty arthritis, the bone ends fuse and immobilize the joint
• Treatment: drugs, plenty of water, avoidance of alcohol

Lyme Disease
• Caused by bacteria transmitted by the bites of ticks
• Symptoms: skin rash, flu-like symptoms, and foggy thinking
• May lead to joint pain and arthritis• Treatment: antibiotics

Developmental Aspects of Joints
• By embryonic week 8, synovial joints resemble adult joints
• A joint’s size, shape, and flexibility are modified by use
• Advancing years take their toll:– Ligaments and tendons shorten and weaken– Intervertebral discs become more likely to
herniate– Most people in their 70s have some degree of OA
• Exercise!!!!!!