
Jason Persoff, M.D., S.F.H.M. - CEConsultants,...
26
Jason Persoff, M.D., S.F.H.M. • None • Mo’va’onal Disclosures • Controversies in current management o Does the airway even matter? o What drugs work (hint: none)? o Monitoring for perfusion during a code • Post-cardiac arrest treatment o Therapeutic hypothermia o Prognosis 3 • Events leading up to cardiac arrest o Dispel myths about who benefits and who doesn’t from CPR o Advanced directives o Clues to imminent cardiac arrest in hospitalized patients • Treatment during early cardiac arrest o Pathophysiology o Code leadership
-
Upload
phungxuyen -
Category
Documents
-
view
214 -
download
1
Transcript of Jason Persoff, M.D., S.F.H.M. - CEConsultants,...
Jason Persoff, M.D., S.F.H.M.
• None • Mo'va'onal Disclosures
• Controversies in current management o Does the airway even matter? o What drugs work (hint: none)? o Monitoring for perfusion during
a code
• Post-cardiac arrest treatment o Therapeutic hypothermia o Prognosis
3
• Events leading up to cardiac arrest o Dispel myths about who
benefits and who doesn’t from CPR
o Advanced directives o Clues to imminent cardiac
arrest in hospitalized patients
• Treatment during early cardiac arrest o Pathophysiology o Code leadership
4
• Identify knowledge gaps • Improve delivery of emergency cardiac care • Stir the pot of controversies in resuscitation • Recommend further improvements in clinical
practice
5
6
• Knowledge Gaps o Age and resuscitation outcome o Cancer diagnosis and resuscitation outcome o Overall prognosis in resuscitation
• Controversies o In whom is CPR/ACLS futile?
7
8
• Knowledge Gaps o Vital signs most predictive of imminent cardiopulmonary arrest
• Improving Care o Rapid response teams and improvements in code status discussion o Changing culture of vital sign derangements o Predictive models for the Electronic Medical Record
• Controversies o Why don’t people call for help?
9

10
• How much 'me did that video take? o Exactly 82 seconds
• In the hospital, how long does it take to recognize cardiac arrest?
Herlitz et al. Resuscitation 2001. Herlitz et al. Resuscitation 2001.
• Eberle confirmed our skills at pulse check • Sensi'vity 90% • Specificity 55% • Accuracy 65%
o Median 'me needed to iden'fy presence or absence of pulse: • 24 seconds overall, 32 seconds for pulse absent pa5ents
• In 2009, Tibbells confirmed we’d only goMen a liMle beMer • Sensi'vity 86% • Specificity 64% • Accuracy 78%
• BoMom line: in controlled circumstances, we don’t know if a pa'ent has a pulse or not
Eberle et al. Resuscitation 1996 (33) Tibballs J and Russell Philip. Resuscitation
2009; 80: 61 Eberle et al. Resuscitation 1996 (33)
Tibballs J and Russell Philip. Resuscitation 2009; 80: 61

• A code blue is called while you’re on the unmonitored unit of the hospital. As you enter the room, the nurses wheel in the code cart.
14

Neurologically Intact Survival (CPC 0-1)
Survival to Hospital Discharge
Return of Spontaneous Circulation
Death
CPC Status
• 0 Normal • 1 Good • 2 Mod Disability • 3 Major Disability • 4 Persistent Vegetative State • Brain Death
88% of all In-Hospital Cardiac Arrests Occur on Patients with DNR Status
Hodgetts et al. Resuscitation 54: 2002
Neurologically Intact Survival (CPC 0-1)
Survival to Hospital Discharge
Return of Spontaneous Circulation
Death
CPC Status
• 0 Normal • 1 Good • 2 Mod Disability • 3 Major Disability • 4 Persistent Vegetative State • Brain Death
54-76%
17-57%
58-75%
14-27% of Pediatric In-Hospital Arrests
24% of Adult In-Hospital Arrests Samson et al. NEJM 354: 2006
Nadkarni, et al. JAMA 295: 2006
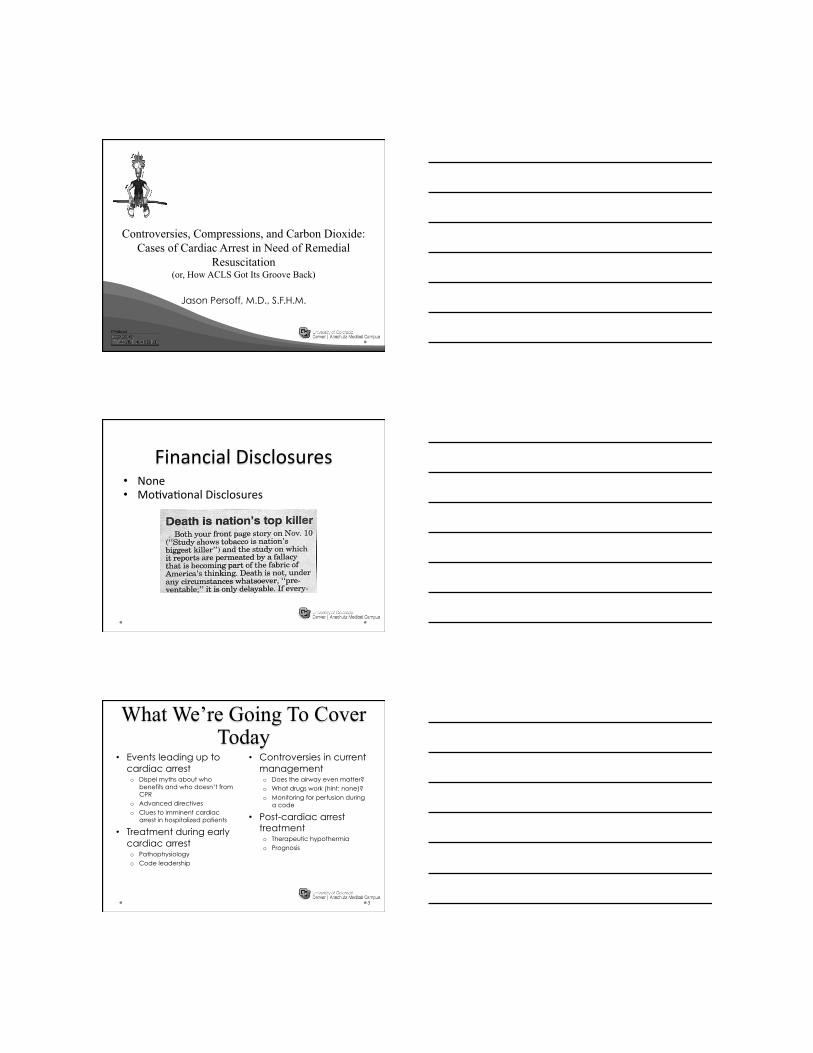
Total Surviving Neurologically Intact ~12%
Neurologically Intact Survival (CPC 0-1)
Survival to Hospital Discharge
Return of Spontaneous Circulation
Death
CPC Status
• 0 Normal • 1 Good • 2 Mod Disability • 3 Major Disability • 4 Persistent Vegetative State • Brain Death
53-52%
10-20%
61-62%
Usually preceded up to 8 hours prior to arrest by marked changes in SBP, HR, or oxygen saturation
Skrifvars et al. Resuscitation 70: 2006
Nadkarni, et al. JAMA 295: 2006
Total Surviving Neurologically Intact ~6.8%
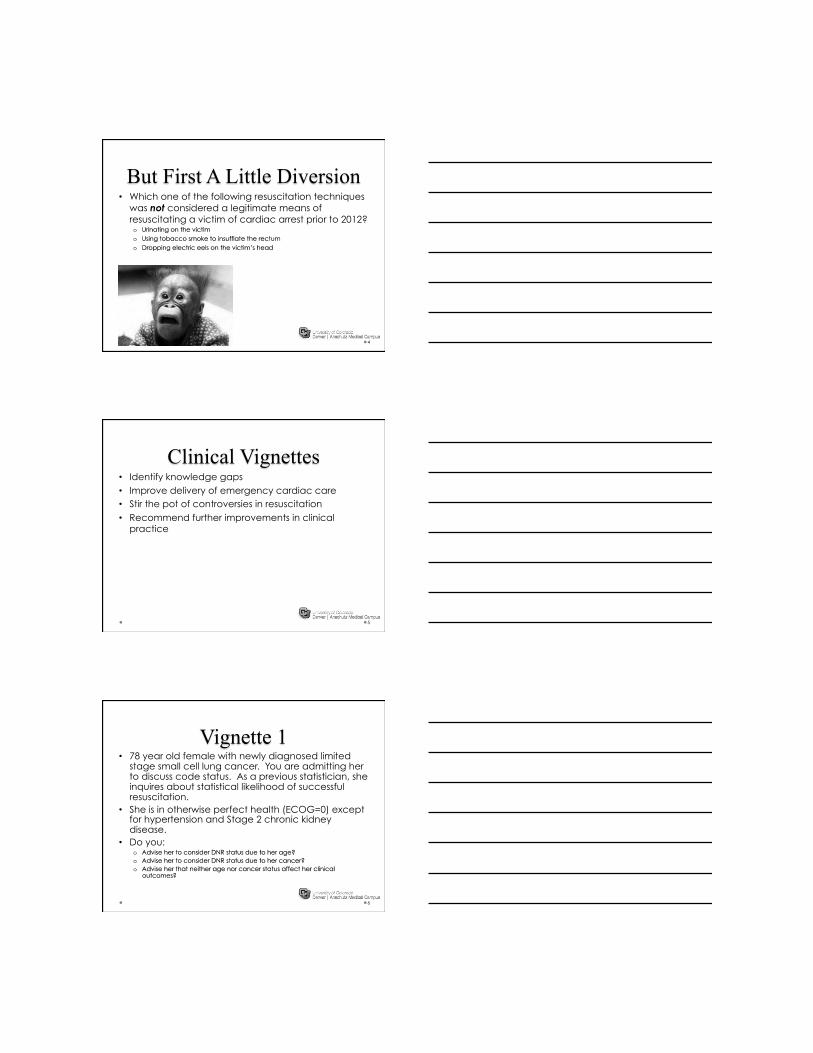
Untreated V-Fib/VT
Electrical Phase
0-4 minutes
High Countershock Receptivity
Circulatory Phase
4-10 minutes
CPR Needed Before Shock
Metabolic Phase
10+ minutes
Comprehensive Multisystem Approach
After Mader T, Resuscitation 2007
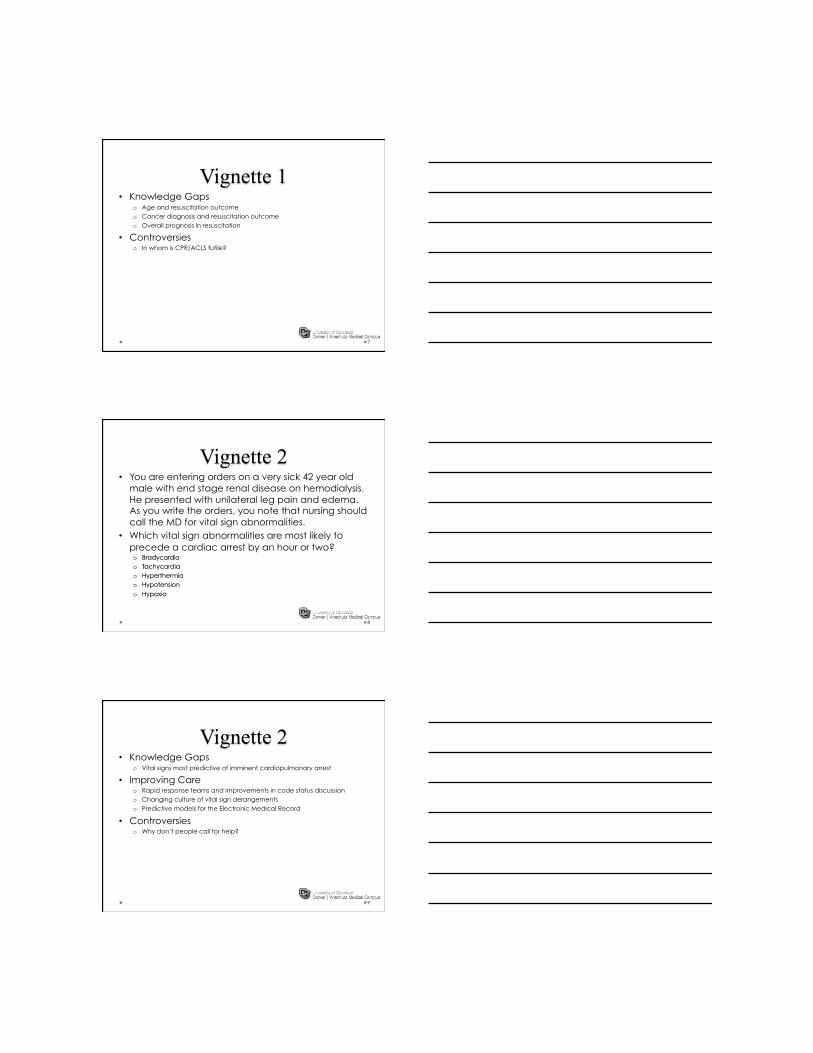
Circulatory Collapse 0-3 Mins
• Pulse Check? • Call Code? • CPR?
Code Team Arrival
3-6 Mins
• How quickly does the team arrive and who leads?
CPR, Drugs, Intubation 6-10 Mins
• Arrhythmia Recognition?
• Airway, Breathing • Shocks • Drugs
Code Team Begins to Integrate 10+ Mins
• Kitchen Sink • Txfr or
Pronounced
Acute VF Arrest
Metabolic Phase
Electrical Phase
Circulatory Phase
Fibrillating myocardium deplete of ATP
Weisfeldt ML and Becher LB. JAMA 2002;
288: 3035.
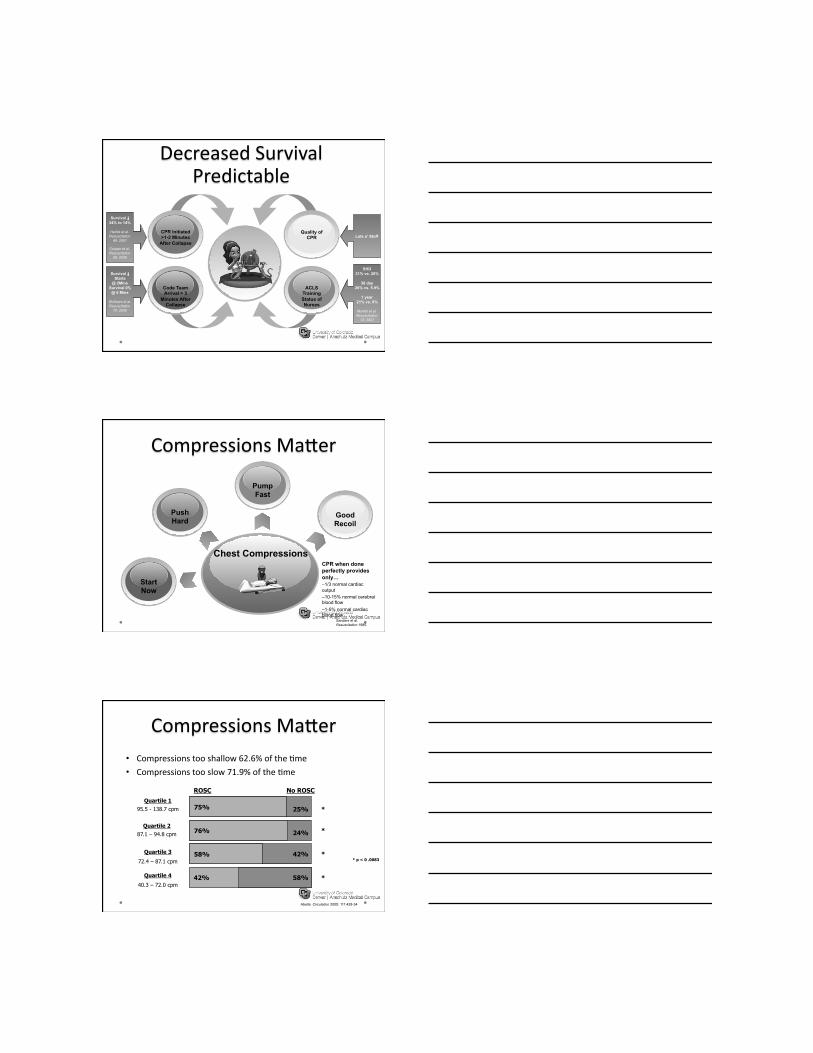
CPR Initiated >1-2 Minutes
After Collapse
Survival ↓ 34% to 14%
Herlitz et al. Resuscitation
49: 2001
Cooper et al. Resuscitation
68: 2006
Code Team Arrival > 3
Minutes After Collapse
Survival ↓ Starts
@ 2Mins Survival 0%
@ 6 Mins
Skrifvars et al. Resuscitation
70: 2006
ACLS Training Status of Nurses
SHD 31% vs. 20%
30 day 26% vs. 5.9%
1 year 21% vs. 0%
Moretti et al. Resuscitation
72: 2007
Quality of CPR Lots o’ Stuff
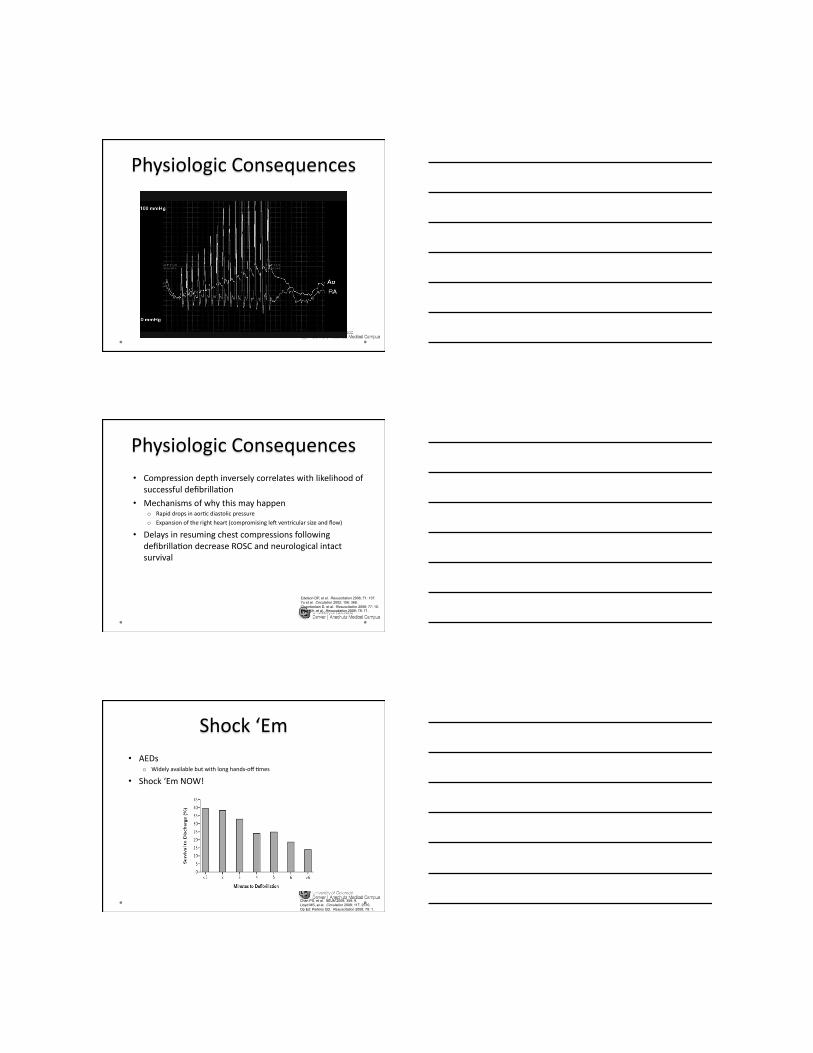
Chest Compressions
Start Now
Good Recoil
Push Hard
Pump Fast
CPR when done perfectly provides only… – 1/3 normal cardiac output – 10-15% normal cerebral blood flow – 1-5% normal cardiac blood flow
Sanders et al. Resuscitation 1985.
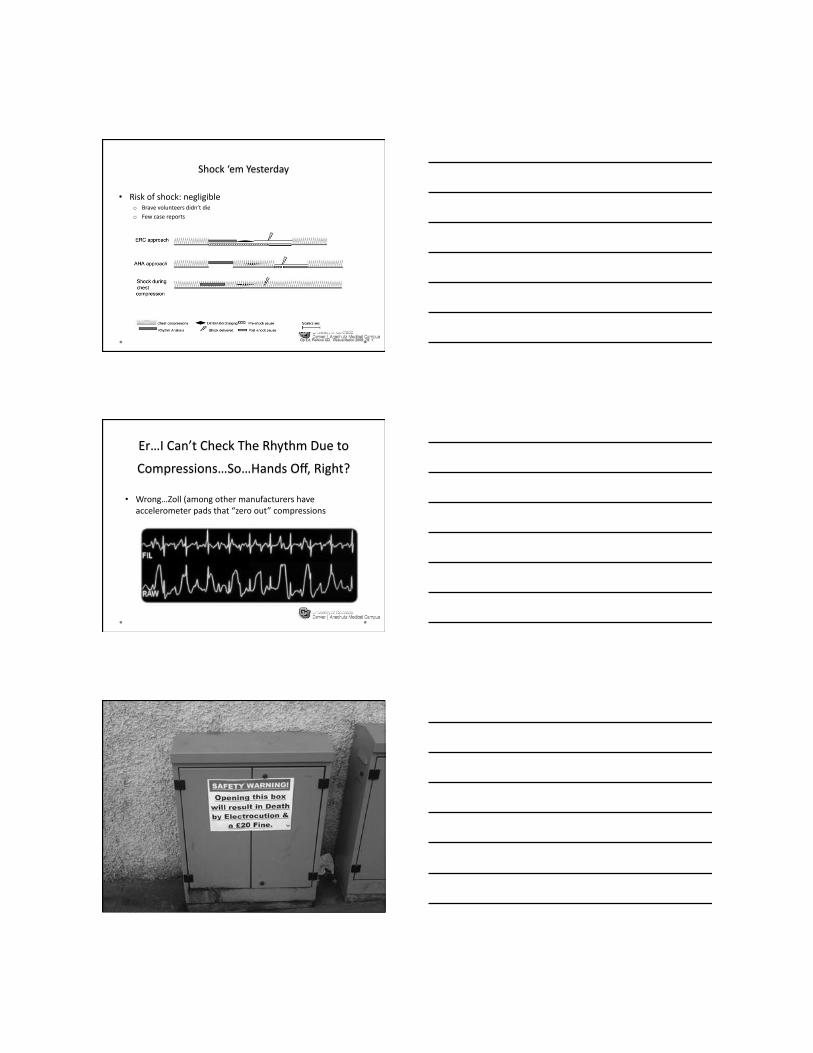
• Compressions too shallow 62.6% of the 'me
• Compressions too slow 71.9% of the 'me
* p < 0 .0083
* 75% 25%
ROSC No ROSC Quartile 1
95.5 - 138.7 cpm
* 24% 76% Quartile 2
87.1 – 94.8 cpm
58% 42% Quartile 3
72.4 – 87.1 cpm
* 42% 58% Quartile 4
40.3 – 72.0 cpm
Abella. Circulation 2005; 111:428-34
*

62%
0%
42%
0% 20% 40% 60% 80%
% Too Shallow
% Too Deep
% Incomplete
Release
Wik et al. JAMA 2005: 293:299-304
Yu et al. Circulation 2002; 106:368-72
• Compression depth inversely correlates with likelihood of successful defibrilla'on
• Mechanisms of why this may happen o Rapid drops in aor'c diastolic pressure
o Expansion of the right heart (compromising leW ventricular size and flow)
• Delays in resuming chest compressions following defibrilla'on decrease ROSC and neurological intact survival
Edelson DP, et al. Resuscitation 2006; 71: 137. Yu et al. Circulation 2002; 106: 368. Chamberlain D, et al. Resuscitation 2008; 77: 10. Berg RA, et al. Resuscitation 2008; 78: 71.
• AEDs o Widely available but with long hands-‐off 'mes
• Shock ‘Em NOW!
Chan PS, et al. NEJM 2008; 358: 9. Lloyd MS, et al. Circulation 2008; 117: 2510. Op Ed: Perkins GD. Resuscitation 2008; 79: 1.
• Risk of shock: negligible o Brave volunteers didn’t die
o Few case reports
Op Ed: Perkins GD. Resuscitation 2008; 79: 1.
• Wrong…Zoll (among other manufacturers have accelerometer pads that “zero out” compressions

• Delayed defibrilla'on o Black race associated with delays in defibrilla'on (p<0.001)
o Small hospital size (<250 beds)
o “AWer hours” (nights/weekends)
o Non-‐monitored bed
Chan PS, et al. NEJM 2008; 358: 9. Herlitz et al. Resuscitation 2001.
• Con'nuous capnography o Increasingly appears to be predic've of excellent perfusion
o Markers of perfusion include a sudden increase in PCO2
o Ven'la'ons can be 'trated to accommodate for EtCO2 of 35-‐40mmHg
Oxygen is Rapidly
Consumed
• 2-4 Minutes • Asymmetric distribution
Switch to Anaerobic Metabolism
• Hepatic perfusion necessary to clear • pKa, pH and other
changes change medication effects
CO2 Rapidly Rises
• Adds to acid burden • Needs lung perfusion
and ventilation to clear
Low Flow
• Functional reductions in compression-
assisted forward flow • Arteriole failure with
low effective blood volumes
Hypoxia
Circulatory Collapse
Lactic Acidosis
Hypercarbia
“The Drain”
• “Iatrogenic hypotension” – Over-zealous BVM use due to
• Desire to correct hypoxia • Belief that hyperventilation will correct acid-base derangements
• What is the appropriate tidal volume for a patient in cardiopulmonary arrest?
• Roughly 750cc
• What is the volume of an adult bag-valve-mask?
• 1.5 liters • Designed for 1-handed operation
New Paradigm: CCR
Michard F. Anesthesiology 2005

• Phenomenon of auto-‐PEEP usually referred to pa'ents on a ven'lator
• Rate exceeded at least 60.9% of the 'me in humans
• In swine models, hyperven'la'on results in… • …increased intrathoracic pressure • …decreased coronary perfusion pressures • …lower survival
• Abella. Circulation 2005; 111:428-34.
• Aufderheide, et al. Resuscitation 2004.

• Contraindicated in conscious pa'ents o Can premote retching and laryngospasm
o Trauma
• Pa'ents gasp during cardiac arrest • Gasping…
o …is a forceful agonal respira'on
o …is a marker of improved prognosis
o …increases cerebral blood flow
o …decreases intracranial pressure
o …improves upper airway patency
o …generates cardiac output
• Yang, et al. Crit Care Med 1994; 22: 879.
• Ristagno G, et al. Resuscitation 2007; 75: 366.
• Xie J, et al. Crit Care Med 2004; 32:238.
• Srinivasan V, et al. Resuscitation 2006; 69: 329.
• Ewy GA and Kern KB. J Am Coll of Cardiol 2009; 53:147.
Rats! A hemorrhagic
model of PEA in rats
Suzuki M, et al. Resuscitation 2009; 80:109.
• Why hypothermia? o Superoxide genera'on post-‐resuscita'on o Calcium influx into cells o Decreased available glucose o Increased oxida've phosphoryla'on o Cooling preserves mitochondria
o The only “brain preserving” therapy post-‐arrest • Hazards
o Coagulopathy o Impaired WBC func'on o Decrease in cardiac index o Hyperglycemia (Real)
• Requires o Con'nuous bladder or central monitoring of temperature o Target 32-‐34°C
A. Aguila et al. / Resuscitation 81 (2010) 1621–1626
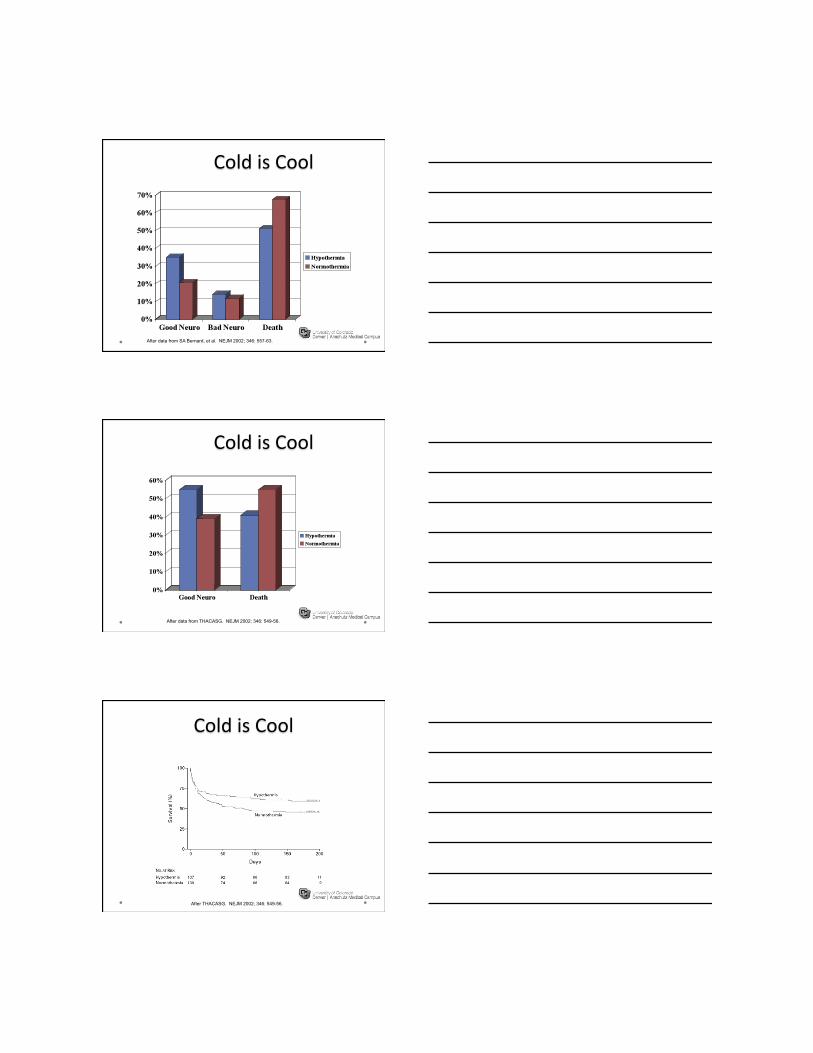
After data from SA Bernard, et al. NEJM 2002; 346: 557-63.
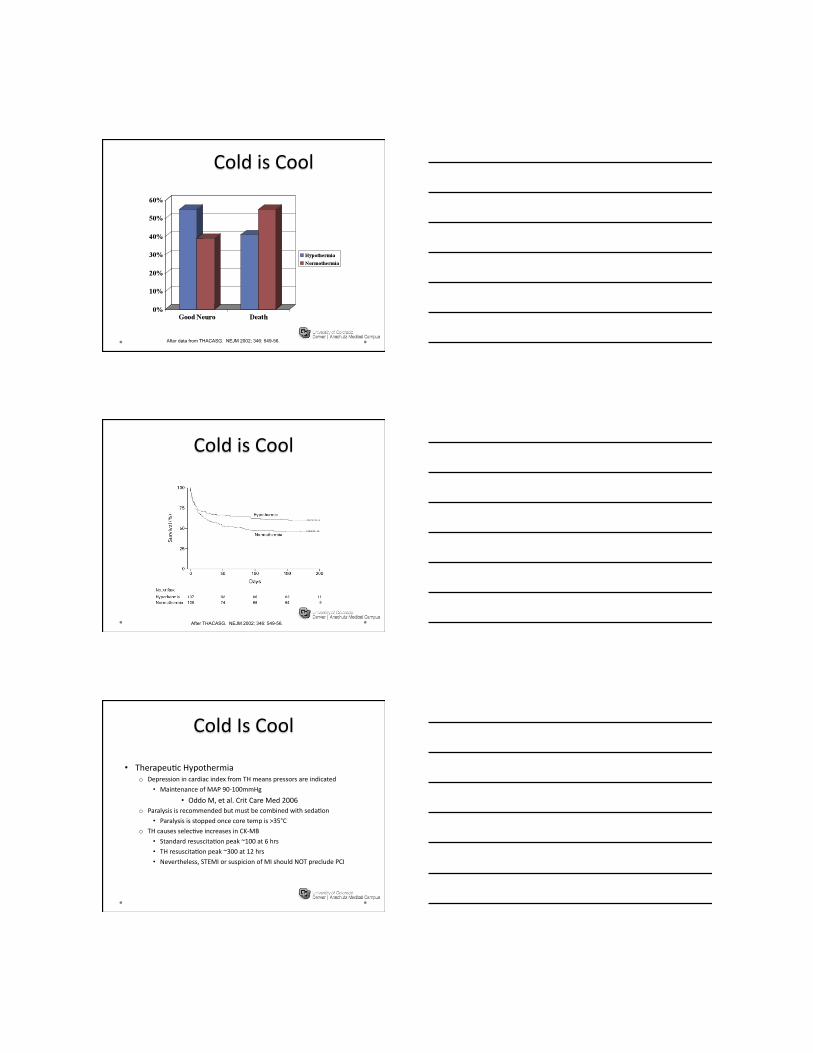
After data from THACASG. NEJM 2002; 346: 549-56.
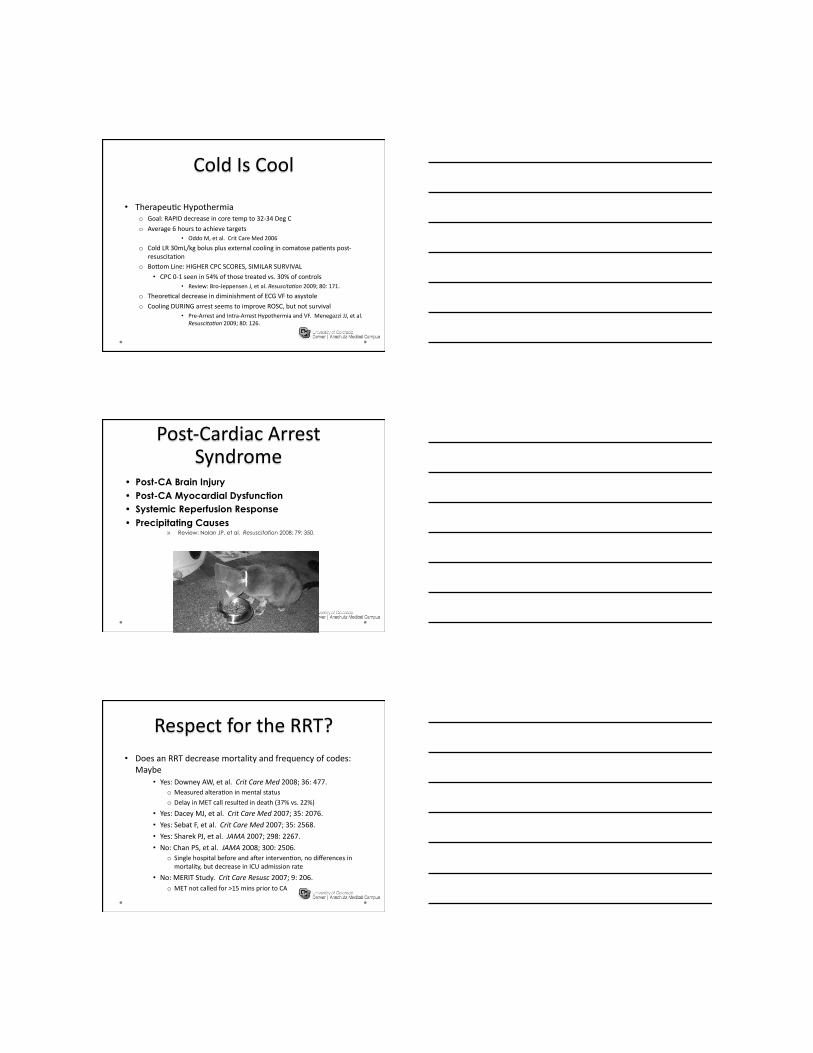
After THACASG. NEJM 2002; 346: 549-56.

• Therapeu'c Hypothermia o Depression in cardiac index from TH means pressors are indicated
• Maintenance of MAP 90-‐100mmHg
• Oddo M, et al. Crit Care Med 2006 o Paralysis is recommended but must be combined with seda'on
• Paralysis is stopped once core temp is >35°C
o TH causes selec've increases in CK-‐MB
• Standard resuscita'on peak ~100 at 6 hrs • TH resuscita'on peak ~300 at 12 hrs • Nevertheless, STEMI or suspicion of MI should NOT preclude PCI
• Therapeu'c Hypothermia o Goal: RAPID decrease in core temp to 32-‐34 Deg C
o Average 6 hours to achieve targets • Oddo M, et al. Crit Care Med 2006
o Cold LR 30mL/kg bolus plus external cooling in comatose pa'ents post-‐resuscita'on
o BoMom Line: HIGHER CPC SCORES, SIMILAR SURVIVAL
• CPC 0-‐1 seen in 54% of those treated vs. 30% of controls • Review: Bro-‐Jeppensen J, et al. Resuscita*on 2009; 80: 171.
o Theore'cal decrease in diminishment of ECG VF to asystole
o Cooling DURING arrest seems to improve ROSC, but not survival • Pre-‐Arrest and Intra-‐Arrest Hypothermia and VF. Menegazzi JJ, et al.
Resuscita*on 2009; 80: 126.
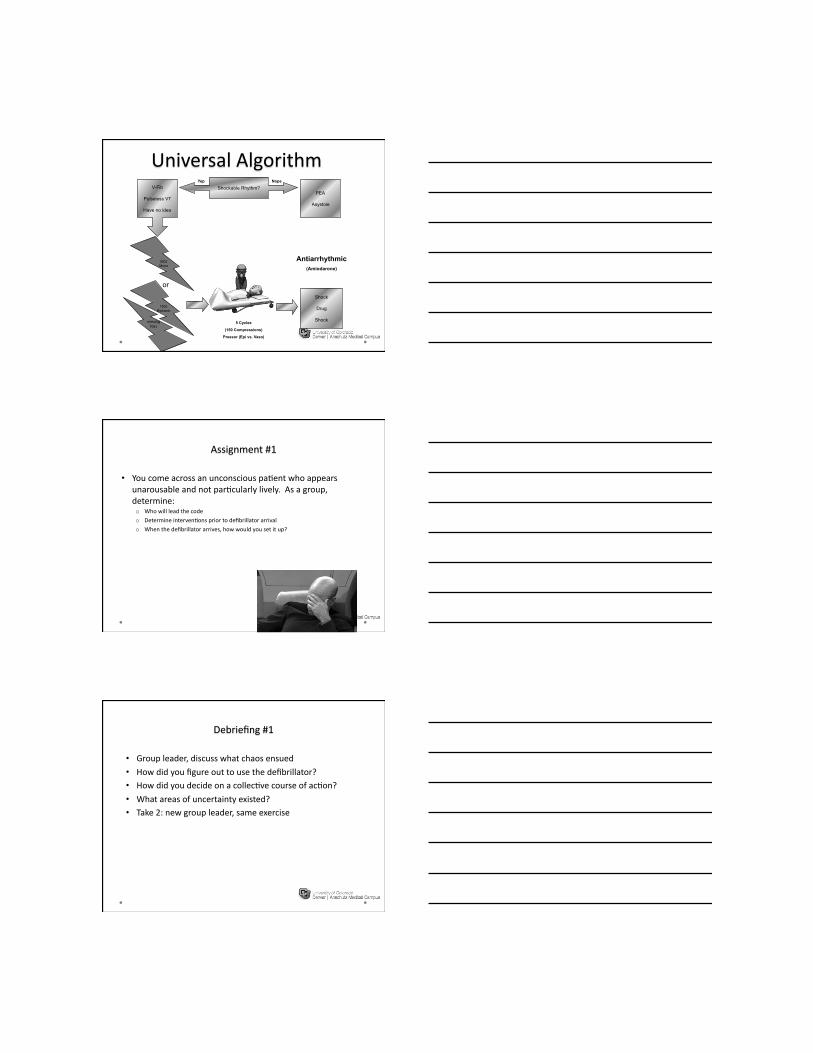
Shockable Rhythm? Yep
V-Fib
Pulseless VT
Have no idea
Nope
PEA
Asystole
360J Mono
150J Biphasic
150J Biphasic
or
5 Cycles
(150 Compressions)
Pressor (Epi vs. Vaso)
Shock
Drug
Shock
Antiarrhythmic (Amiodarone)
• You come across an unconscious pa'ent who appears unarousable and not par'cularly lively. As a group, determine: o Who will lead the code
o Determine interven'ons prior to defibrillator arrival
o When the defibrillator arrives, how would you set it up?
• Group leader, discuss what chaos ensued • How did you figure out to use the defibrillator? • How did you decide on a collec've course of ac'on? • What areas of uncertainty existed? • Take 2: new group leader, same exercise

• Peripheral vs. Central Lines • Precordial Thumps • Cough CPR • Pulse Checks
Shockable Rhythm? Yep
V-Fib
Pulseless VT
Have no idea
Nope
PEA
Asystole
360J Mono
150J Biphasic
150J Biphasic
or
5 Cycles
(150 Compressions)
Pressor (Epi vs. Vaso)
Shock
Drug
Shock
Antiarrhythmic (Amiodarone)
Desbiens NA, Crit Care Med 2008; 36:391.

• All pa'ents in PEA should receive: o IVF wide open to “fill the tank”
• Pa'ents will go into vascular collapse commonly as shock ensues increasing the rela've vascular volume by many liters
o Oxygen • Systemic hypoxia causes vasoconstric'on of the pulmonary arteries leading to RV dysfunc'on and thus decreases in LV preload
o Epinephrine • Peripheral alpha-‐agonist can clamp down the vessels effec'vely but will also increase myocardial workload via beta-‐agonist effects. This is a short-‐term fix
o Chest Compressions • Already discussed
• Your team arrives on a pa'ent who is agonally breathing but appears to have a very faint, rapid pulse. o At what point would you ins'tute chest compressions?
o What interven'ons should you ini'ate immediately and why?
o Name some immediate causes that could have led to this collapse
• What were the difficul'es this go around in deciding course of ac'on?
• Ul'mately, what did your group decide was the e'ology for the collapse and how did you approach it?
• What algorithms do you think may have helped you perform beMer?

• Effect of CCR on Alveolar Collapse and Recruitment o More Atelectasis
o More Hypoxemia
o Worse Hemodynamics
o Effects Persist Even AWer Resump'on of IPPV
o But…the pigs used were anesthe*zed
• Markstaller K, et al. Resuscita*on 2008; 79: 125.
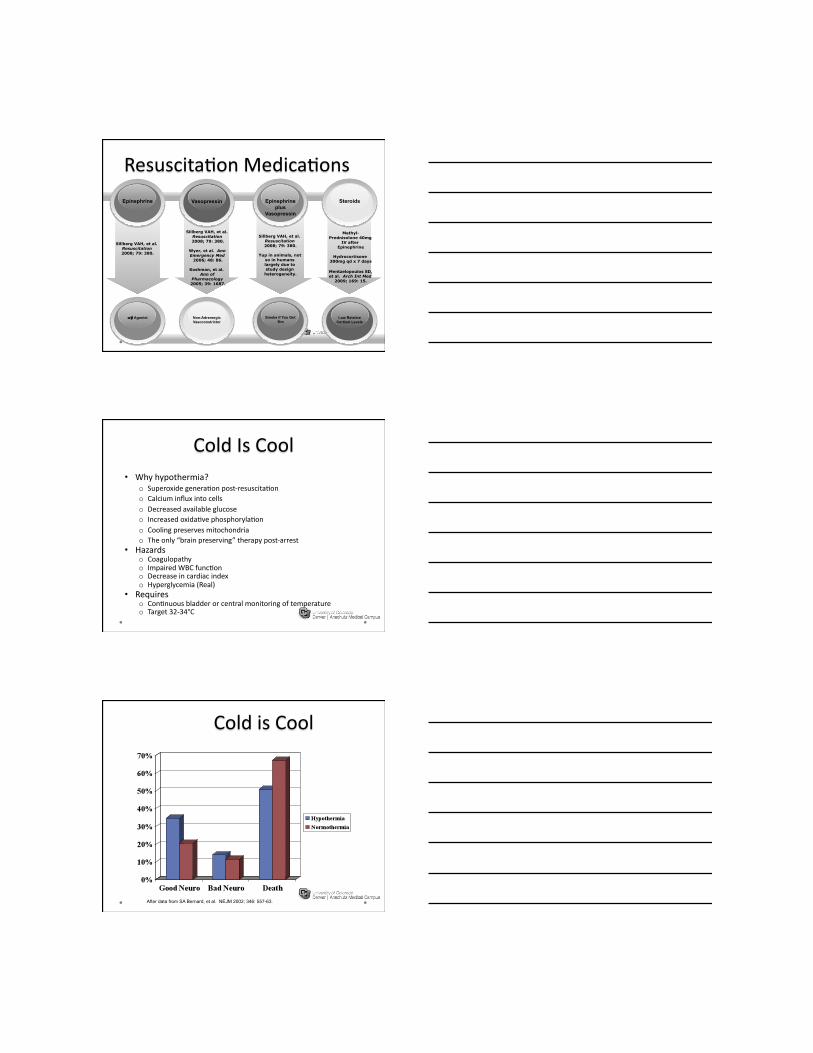
Methyl-Prednisolone 40mg
IV after Epinephrine
Hydrocortisone 300mg qd x 7 days
Mentzelopoulos SD, et al. Arch Int Med
2009; 169: 15.
Steroids
Low Relative Cortisol Levels
Sillberg VAH, et al. Resuscitation 2008; 79: 380.
Wyer, et al. Ann Emergency Med
2006; 48: 86.
Koshman, et al. Ann of
Pharmacology 2005; 39: 1687.
Vasopressin
Non-Adrenergic Vasoconstrictor
Sillberg VAH, et al. Resuscitation 2008; 79: 380.
Yup in animals, not so in humans largely due to study design
heterogeneity.
Epinephrine plus
Vasopressin
Smoke if You Got ‘Em
Sillberg VAH, et al. Resuscitation 2008; 79: 380.
Epinephrine
α/β Agonist
• Why hypothermia? o Superoxide genera'on post-‐resuscita'on o Calcium influx into cells o Decreased available glucose o Increased oxida've phosphoryla'on o Cooling preserves mitochondria o The only “brain preserving” therapy post-‐arrest
• Hazards o Coagulopathy o Impaired WBC func'on o Decrease in cardiac index o Hyperglycemia (Real)
• Requires o Con'nuous bladder or central monitoring of temperature o Target 32-‐34°C
After data from SA Bernard, et al. NEJM 2002; 346: 557-63.
After data from THACASG. NEJM 2002; 346: 549-56.
After THACASG. NEJM 2002; 346: 549-56.
• Therapeu'c Hypothermia o Depression in cardiac index from TH means pressors are indicated
• Maintenance of MAP 90-‐100mmHg
• Oddo M, et al. Crit Care Med 2006 o Paralysis is recommended but must be combined with seda'on
• Paralysis is stopped once core temp is >35°C
o TH causes selec've increases in CK-‐MB
• Standard resuscita'on peak ~100 at 6 hrs • TH resuscita'on peak ~300 at 12 hrs • Nevertheless, STEMI or suspicion of MI should NOT preclude PCI
• Therapeu'c Hypothermia o Goal: RAPID decrease in core temp to 32-‐34 Deg C
o Average 6 hours to achieve targets • Oddo M, et al. Crit Care Med 2006
o Cold LR 30mL/kg bolus plus external cooling in comatose pa'ents post-‐resuscita'on
o BoMom Line: HIGHER CPC SCORES, SIMILAR SURVIVAL
• CPC 0-‐1 seen in 54% of those treated vs. 30% of controls • Review: Bro-‐Jeppensen J, et al. Resuscita*on 2009; 80: 171.
o Theore'cal decrease in diminishment of ECG VF to asystole
o Cooling DURING arrest seems to improve ROSC, but not survival • Pre-‐Arrest and Intra-‐Arrest Hypothermia and VF. Menegazzi JJ, et al.
Resuscita*on 2009; 80: 126.
• Post-CA Brain Injury • Post-CA Myocardial Dysfunction • Systemic Reperfusion Response • Precipitating Causes
» Review: Nolan JP, et al. Resuscitation 2008; 79: 350.
• Does an RRT decrease mortality and frequency of codes: Maybe
• Yes: Downey AW, et al. Crit Care Med 2008; 36: 477. o Measured altera'on in mental status
o Delay in MET call resulted in death (37% vs. 22%)
• Yes: Dacey MJ, et al. Crit Care Med 2007; 35: 2076.
• Yes: Sebat F, et al. Crit Care Med 2007; 35: 2568.
• Yes: Sharek PJ, et al. JAMA 2007; 298: 2267.
• No: Chan PS, et al. JAMA 2008; 300: 2506. o Single hospital before and aWer interven'on, no differences in mortality, but decrease in ICU admission rate
• No: MERIT Study. Crit Care Resusc 2007; 9: 206. o MET not called for >15 mins prior to CA
• “Why doesn’t anyone call for help?” • Buist M. Crit Care Med 2008; 36: 634.
• Implementa'on of an RRT improves vital sign recording • Chen J, et al. Resuscita*on 2009; 80: 35.
Isn’t Orientation over yet????
















