Japan’s Healthcare System and Its Outlook (updated: 2014 April)
26
Japan’s Healthcare System and Its Outlook (updated: 2014 April) www.japanmacroadvisors.com [email protected]
description
Japan’s Healthcare System and Its Outlook (updated: 2014 April). www.japanmacroadvisors.com [email protected]. Executive Summary. - PowerPoint PPT Presentation
Transcript of Japan’s Healthcare System and Its Outlook (updated: 2014 April)

Executive Summary
2
A participation to public insurance system is mandatory to all residents in Japan. The prices of medical treatment and subscribed pills are regulated under the fee-for-service system. Patients directly pay 10-30% of the services they receive while insurers pay the reminder.
The quality of the healthcare in Japan is considered to be high. Japan boost one of the longest life expectancy and one of the lowest infant mortality. At the same time, the system has been cost effective. Despite the recent rise, the per capita healthcare expenditure is below OECD average.
However, its medical expenditure is growing fast in recent years. The total cost of public healthcare has risen from 4.9% of GDP in 1984 to 9.9% of GDP in 2011. A government study estimates that the cost will further rise by 3% to GDP by 2025, mostly due to the demographic change.
While reforms are underway to restrain the rise, a rise of 2% to GDP seems inevitable, in our view.

3
Overview
Outlook
Reform Measures under discussion

Healthcare system in Japan
4
The healthcare system in Japan is characterized by two principles:
100% public insurance coverage
• All residents and below must join one of the two public insurance systems regardless of whether or not they have private health insurance.
Fee-for-Service.
• In principle, all medical treatments and pills are covered under the public insurance system. Patients pay portion of treatments and medicines (10-30% depending on age), and the rest is paid directly to medical service providers by the insurers. There is a cap on patient’s burden in all insurance systems – patients can seek reimbursement for payment above the cap.
• Fees are regulated. The government has a control over what is deemed as medical treatment and their fees .

Japanese Public Insurance System
5
There are three category in the public insurance system: The elderly over the age of 75 is covered under a universal insurance. For working age and below, they need to subscribe to either National Insurance, if they are self employed, or Employee’s Health Insurance, if they are employed.
The Latter-Stage Elderly Insurance System (14.7 million people under coverage)
National Health Insurance
(38.3 million people)
Employee Health Insurance*
(73.7 million people)
Source: Ministry of Health, Labour and Welfare. The number of insured is as of March 31, 2012. * For simplicity, includes mutual associations for public officials and teachers.
75
20
Age
Note: 02e.pdf

Japanese Public Insurance System
6
There are two public insurance systems for the working age: National Health Insurance and Employee’s Health Insurance.
Employee’s Health Insurance
• Employers deduct insurance premium from salaries of their employees, match them, and pay the whole premium to insurers.
• Corporations and industry associations build health insurance insures.
National Health Insurance
• Self-employed, non-salary workers, non-workers are covered by the National Insurance.

Separate System for the Elder
7
In 2008, “Medical Care System for the Latter-Stage Elderly” was established for medical needs for those Age 75+.
• Those age 75 and above will pay 10% of fees for medical services, while their premium is automatically deducted from the pension money they receive from the government.
• Additional premium paid by those between Age 65 to 74 will be set aside by insurers for the Age 75 and above. EHI and NHI also pay some money annually to Age 75+.
• In principle, summarizing, 50% is be funded by the national government, 10% by the elderly, and 40% by the working age population.
A measure to levy additional insurance premium for high income earning elderly is under consideration.
• This change for the elderly could raise 230 billion yen for the public insurance system.

8
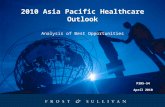
Infant Mortality Rate (deaths per 1000 live births)
Quality of Japan’s healthcare is Japan’s Infant mortality rate is one of the lowest in the world, 2.3 per 1000 live births.
Source: OECD Stats812013161P1G014
Infant Mortality Rate
India
South Africa
IndonesiaBrazil
MexicoChina
Russian Fed.
TurkeyChile
United States
New Zealand
Canada
Hungary
Slovak R
ep.
Poland
United Kingdom
OECD (34)
Australia
Switzerla
nd
Denmark
Germany
Austria
Netherlands
Ireland
Israel
France
Luxembourg ¹
Greece Italy
BelgiumSpain
Portugal
Korea
Slovenia
Czech
Rep.
Estonia
Finland
Norway
Japan
Sweden
Iceland ¹
0.0
10.0
20.0
30.0
40.0
50.0

9
Life Expectancy (Total population at birth)
Japan’s life expectancy is one of the longest in the world. It rose to 83 years approx. in 2011 from 72 years in 1970.
Life Expectancy at Birth
Source: OECD Stats812013161P1G001
Switzerla
ndJapan
ItalySpain
Iceland
France
Australia
SwedenIsr
ael
Norway
Netherlands
New Zealand
Luxembourg
Austria
United Kingdom
Korea
Canada
Germany
Greece
Portugal
Finland
Ireland
Belgium
Slovenia
OECD (34)
Denmark
United States
Chile
Czech
Rep.
Poland
Estonia
Slovak R
ep.
HungaryTurke
y
MexicoChina
Brazil
Indonesia
Russian Fed.
India
South Africa
015
30
4560
7590
2011 1970

Health Expenditure
10
Japan’s health care system seem cost-effective. Its healthcare expenditure per capita is USD 3,213 (purchase power parity), slightly below the OECD average of USD 3,322.
Health Expenditure Per Capita, 2011 (or nearest year)
Source: OECD “Health at Glance 2013.”
-
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
US
Nor
way
Switz
erla
nd
Net
herla
nd
Aust
ria
Cana
da
Germ
any
Denm
ark
Luxe
mbo
urg
Fran
ce
Belg
ium
Swed
en
Aust
ralia
Irela
nd UK
Finl
and
Icel
and
Japa
n
New
Zea
land
Spai
n
Italy
Port
ugal
Slov
enia
Gree
ce
Isra
el
Kore
a
Czec
h Re
p
Slov
ak R
ep
Hung
ary
Chile
Pola
nd
Russ
ia
Esto
nia
Braz
il
Mex
ico
S. A
fric
a
Turk
ey
Chin
a
Indi
a
Indo
nesia
Note:812013161P1G150

Health Expenditure
11
In terms of % GDP, Japan is on a par with the OECD average. (health and long term care combined)
Health Expenditure as % GDP, 2011 (or nearest year)
Source: OECD “Health at Glance 2013.”
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
Uni
ted
Stat
es
Net
herla
nds
Fran
ce
Denm
ark
Swed
en
Cana
da
Switz
erla
nd
Belg
ium
Ger
man
y
Aust
ria
New
Zea
land
Nor
way
Japa
n
Finl
and
Icel
and
Port
ugal
Spai
n
Slov
enia
Uni
ted
King
dom
Gre
ece
Isra
el
Hung
ary
Kore
a
Luxe
mbo
urg
Czec
h Re
publ
ic
Pola
nd
Esto
nia
Long-term care
Health
Note: 812013161P1G185-combined exp

12
Current Status
Outlook
Measures

Medical Expenditure Growth
13
The per capita medical expenditure is increasing as the society ages. Despite the narrower coverage after 2007, the medical expenditure for the elderly continues to raise as a portion of the total expenditure.
Source: (left) Ministry of Health, Labour and Welfare. National Institute of Population and Social Security Research. (right) Ministry of Health, Labour and Welfare. “Annual Health, Labour and Welfare Report 2012-2013”
Health Expenditure Per Capita and % Age 65+ Population
-
50.00
100.00
150.00
200.00
250.00
300.00
350.00
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
1954
1957
1960
1963
1966
1969
1972
1975
1978
1981
1984
1987
1990
1993
1996
1999
2002
2005
2008
2011
Population % 65+
Per Capita
Health Expenditure Used by the Elderly (%)
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
45.0%
1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
2003-2007 Coverage Change: Age 70+ ⇒Age 75+
Note: toukei 20140408

Healthcare Expenditure
14
Currently, the government pays approximately 40% of the medical expenditure. Their burden is expected to continue increasing as the total expenditure grows.
Government, 38.4%
Employers, 20.2%
Employees, 28.4%
Patients, 12.3%
Others , 0.7%
Source: Ministry of Health, Labour and Welfare. *Data is for FY2011. ** From [White Paper 2013]
Medical Expenditure by Payers* Payment by the National Government**
-
2,000
4,000
6,000
8,000
10,000
12,000
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
(JPY bn)
Note: toukei 20140408

Healthcare Expenditure Forecast
15
Japan’s healthcare expenditure (medical and long term care combined) has been increasing.
Healthcare Expenditure : Historical and Forecast(Medical and Nursing Expenditure Combined)
Source: Ministry of Health, Labour and Welfare. The figure includes nursing expenditure after 2000. Forecast is from the Comprehensive Reform of Social Security and Tax. Forecasts made in March 2012, included in the final report.
(JPY trn)
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2015
2020
2025
Forecast
Note: toukei 20140408

Healthcare Expenditure Forecast
16
The healthcare expenditure (medical plus nursing) is expected to increase both in nominal numbers and as a percentage of GDP. 40% of the increase (in amount) is from nursing.
Source: The Comprehensive Reform of Social Security and Tax. Forecasts made in March 2012, included in the final report.
Healthcare Expenditure: Historical and Forecast(Medical and Nursing Expenditure Combined)
(JPY trn)
2011 2012 2015 2020 2025
GDP 484.0 479.6 509.8 558.0 610.6
Medical Expenditure 39.0 35.1 39.5 46.9 54.0 Elderly Nursing Expenditure 9.0 8.4 10.5 14.9 19.8
Total as % GDP 9.9% 9.1% 9.8% 11.1% 12.1%
Note: toukei 20140408

Healthcare Expenditure Forecast
17
Even if only the cost-cutting measures are taken, the total expenditure is expected to increase by 1.5% of GDP.
Source: The Comprehensive Reform of Social Security and Tax. Forecasts made in March 2012, included in the final report.
Healthcare Expenditure: Historical and Forecast(Medical and Nursing Expenditure Combined)
2015 2025As Is Reformed As Is Reformed
Health Expenditure 39.1 39.5 53.3 54.0 Elderly Nursing Expenditure 9.9 10.5 16.4 19.8
Impact of Reform 0.2% 0.7%
<+> 0.5% 2.1%Improving in-hospital care 1.5 6.5 Transferring in-hospital patients to out-hospital 0.3 1.1 Improving nursing care 0.9 5.3 <-> -0.3% -1.4%Shortening in-hospital stay 1.1- 5.9- Decreasing hospital visits 0.3- 1.5- Increasing home-care 0.2- 0.8- Prevention 0.1- 0.6-
1.0 4.10
Impact as % of GDP
Impact as % of GDP
(JPY trn)
Note: toukei 20140408

Medical Expenditure Growth
18
The speed of Japan’s health expenditure increase outpaces other countries.
Annual Average Growth Rate of Per Capita Health Expenditure 2000-2011
Source: OECD “Health at Glance 2013.”
-14.0%-12.0%-10.0%
-8.0%-6.0%-4.0%-2.0%0.0%2.0%4.0%6.0%8.0%
Gre
ece
Irela
nd
Icel
and
Esto
nia
Port
ugal UK
Denm
ark
Slov
enia
Cxec
h Re
p
Spai
n
Italy
Aust
ralia
Aust
ria
Nor
way
Belg
ium
Mex
ico
Fran
ce
Cana
da
New
Zea
land
Net
herla
nds
Pola
nd US
Switz
erla
nd
Finl
and
Swed
en
Ger
man
y
Hung
ary
Slov
ak R
ep
Isra
el
Japa
n
Chile
¹
Kore
a
Note: 8120131P1G151

19
Current Status
Outlook
Measures

Deterrence of Unnecessary Access
20
On average, a Japanese visits doctors 13 times per year. Introduction of general practitioners (GPs) as gatekeeper may be able to reduce the burden of doctors, and hence decrease the total number of visits.
Number of Annual Doctor Consultation Per Capita 2011
Source: OECD “Health at Glance 2013.”
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
Kore
a
Japa
n
Hung
ary
Czec
h Re
publ
ic
Slov
ak R
epub
lic
Ger
man
y
Russ
ian
Fed.
Turk
ey
Belg
ium
Cana
da
Spai
n
Aust
ria
Fran
ce
Pola
nd
Aust
ralia
Luxe
mbo
urg
Net
herla
nds
Slov
enia
Esto
nia
Isra
el
Icel
and
Nor
way
Uni
ted
King
dom
Denm
ark
Finl
and
Port
ugal
Uni
ted
Stat
es
Switz
erla
nd
Irela
nd
New
Zea
land
Chile
Swed
en
Mex
ico
Braz
il
Sout
h Af
rica
Note: 812013161P1G1065-doctor consultation

Deterrence of Unnecessary Access
21
Approximately 70% is spent on services at hospitals and clinic.
In Patient , 37.3%
Out Parient , 34.8%
Dental, 6.9%
Medicine, 17.2%
Hospital Living Cost,
2.1%
Nurse Visits, 0.2%
Aftercare, 1.5%
Source: Ministry of Health, Labour and Welfare. Data is for FY2011.
Health Expenditure by Usage
Note: toukei 20140408

Deterrence of Unnecessary Access
22
Japanese in-patients tend to stay in hospitals for a longer period of time than those in other OECD countries. If then can stay at home under care of local community and practitioners, the expenditure may decrease.
Average Length of Stay in Hospital 2011
Source: OECD “Health at Glance 2013.”
0.02.04.06.08.0
10.012.014.016.018.020.0
Japa
n¹
Kore
a
Russ
ian
Fed.
Finl
and
Chin
a
Hung
ary
Czec
h Re
publ
ic
Germ
any
Switz
erla
nd
Fran
ce
Port
ugal
Luxe
mbo
urg
New
Zea
land
Belg
ium
Italy
Slov
ak R
epub
lic
Aust
ria
Cana
da¹
Esto
nia
Spai
n
Pola
nd
Slov
enia
Unite
d Ki
ngdo
m
Nor
way
Gree
ce
Irela
nd
Icel
and
Unite
d St
ates
Chile
Isra
el
Aust
ralia
Net
herla
nds¹
Sout
h Af
rica
Swed
en
Denm
ark
Indo
nesia
Mex
ico
Turk
ey
Note: 812013161P1G077-length of stay in hosp

Separate System for the Elder
23
In 2008, “Medical Care System for the Latter-Stage Elderly” was established for medical needs for those Age 75+.
• Those age 75 and above will pay 10% of fees for medical services, while their premium is automatically deducted from the pension money they receive from the government.
• Additional premium paid by those between Age 65 to 74 will be set aside by insurers for the Age 75 and above. EHI and NHI also pay some money annually to Age 75+.
• In principle, summarizing, 50% is be funded by the national government, 10% by the elderly, and 40% by the working age population.
A measure to levy additional insurance premium for high income earning elderly is under consideration.
• This change for the elderly could raise 230 billion yen for the public insurance system.

Generics and Prevention
24
More use of generics will help Japan contain medical costs. Generics use in Japan is about half of the OECD average in value and volume. Prevention is also likely to help minimize the number of patients with adult diseases that require frequent and continuous services.
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
45.0
By Value By Volume
OECD19 Average
Japan
Share of Generics in Total Pharmaceutical Market 2011
Source: OECD “Health at Glance 2013.” Note: 812013161P1G094-generics

Mixed Treatment
25
Patients may become allowed to be treated under the insurance and out of their own pocket simultaneously. This will increase the welfare of patients by choice, while this may potentially save the government some money.
• The original plan was to allow mixed treatment so that patients of difficult disease will have more options. However, recently, the ministry is showing unwillingness to allow it.
• As a compromise, it is likely that a new rule will be set up regarding the mixed treatment. • Written proposal describing different treatment options for patients must be
submitted by doctors to patients. • Medical moral hazard (i.e. doctors suggesting unnecessary treatments) must be
avoided.

IMPORTANT DISCLAIMERIMPORTANT DISCLAIMER: The information herein is not intended to be an offer to buy or sell, or a solicitation of an offer to buy or sell, any securities and including any expression of opinion, has been obtained from or is based upon sources believed to be reliable but is not guaranteed as to accuracy or completeness although Japan Macro Advisors (“JMA”) believe it to be clear, fair and not misleading. Each author of this report is not permitted to trade in or hold any of the investments or related investments which are the subject of this document. The views of JMA reflected in this document may change without notice. To the maximum extent possible at law, JMA does not accept any liability whatsoever arising from the use of the material or information contained herein. This research document is not intended for use by or targeted at retail customers. Should a retail customer obtain a copy of this report they should not base their investment decisions solely on the basis of this document but must seek independent financial advice.
26