Guillermo Garcia-Manero, MD1; Ehab Atallah, MD2; Samer K ...
Upload
ross-wellsCategory
view
221download
0
January, 20141
Innovation for Neonatal Care at Philips Research
Dr Louis AtallahSenior Scientist, Patient Care SolutionsPhilips Research, EindhovenJanuary 2014

January, 20142
Philips Research: Innovation around the GlobeMore than 1500 scientists, cooperating with ~250 universities/institutes
Briarcliff Clinical sites HealthcareLighting
CambridgeHome & OralHealthcare
Paris Healthcare
Eindhoven HealthcareLighting Lifestyle
Bangalore Emerging Markets HealthcareLighting
HamburgHealthcare
Shanghai Emerging Markets HealthcareLighting, Lifestyle

January, 20143
Patient Care SolutionsEnhancing patient care through smart sensor solutions
VisionSmart patient care solutions will increasingly support hospital staff in clinical decision making in various care settings. New solutions for lower acuity care will reduce the workload in the ICU. This will also enable use in the home, aiming to improve quality of life and further drive down the cost of healthcare.
MissionThrough collaboration with clinical experts we deliver innovative technology solutions for Patient Care in the fields of Physiological Monitoring, Respiratory & Emergency care, assisting caregivers both in hospital and home.
January, 20144
Why neonatal care?• 15 million babies are born preterm every year (WHO)• Many babies (not only preterm) have problems and require care in
the NICU (Sweden: 10%). • Term babies could also be challenging as their problems require quick
diagnosis and treatment.• Very ill babies need more observation and care and often have longer
stays in NICUs than preterm babies.
January, 20145
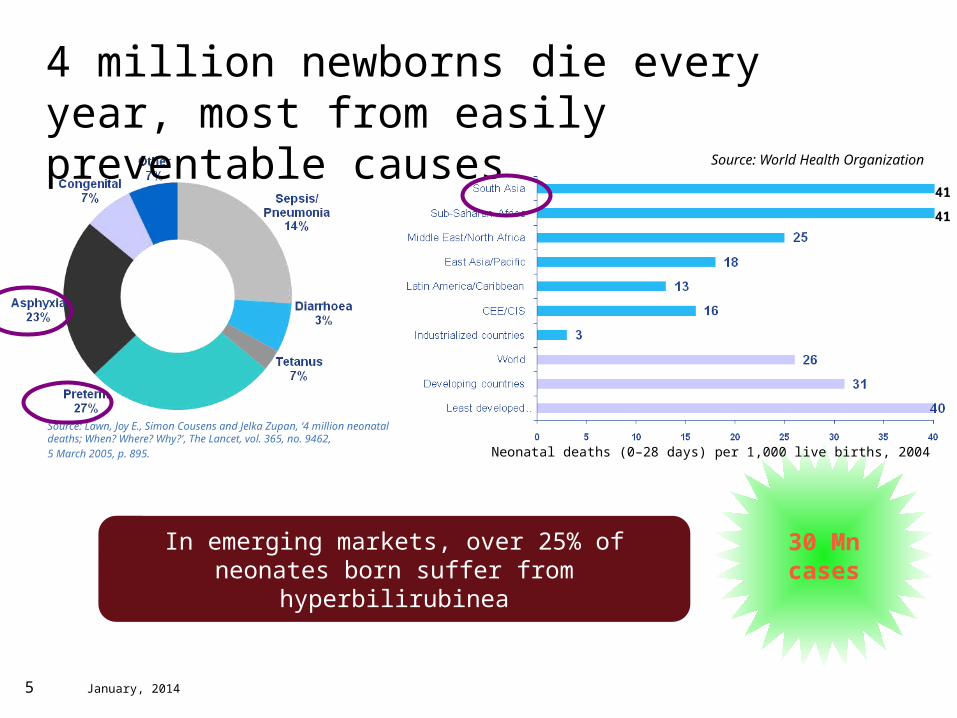
4 million newborns die every year, most from easily preventable causes
Source: Lawn, Joy E., Simon Cousens and Jelka Zupan, ‘4 million neonatal deaths; When? Where? Why?', The Lancet, vol. 365, no. 9462,5 March 2005, p. 895.
Source: World Health Organization
41
41
30 Mncases
In emerging markets, over 25% of neonates born suffer from hyperbilirubinea
Neonatal deaths (0–28 days) per 1,000 live births, 2004
January, 20146
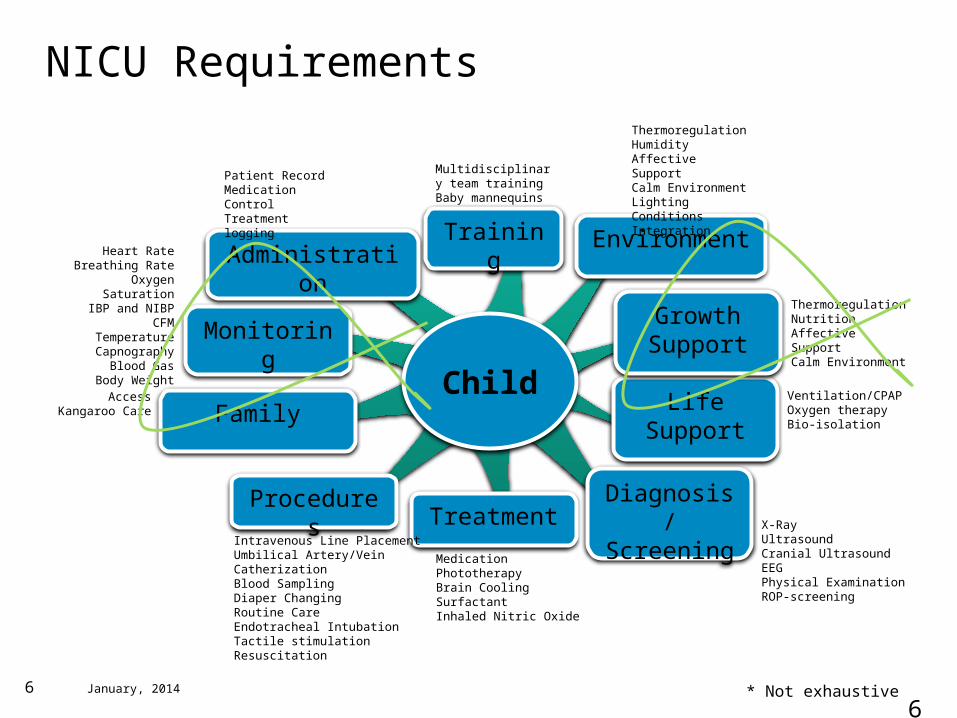
NICU Requirements
6
Child
Monitoring
Family
Procedures Diagnosis/Screening
Life Support
ThermoregulationNutritionAffective SupportCalm Environment
Ventilation/CPAPOxygen therapyBio-isolation
GrowthSupport
Treatment
AccessKangaroo Care
X-RayUltrasoundCranial UltrasoundEEGPhysical ExaminationROP-screening
MedicationPhototherapyBrain CoolingSurfactantInhaled Nitric Oxide
Heart RateBreathing Rate
Oxygen SaturationIBP and NIBP
CFMTemperatureCapnography
Blood GasBody Weight
Intravenous Line PlacementUmbilical Artery/Vein CatherizationBlood SamplingDiaper ChangingRoutine CareEndotracheal IntubationTactile stimulationResuscitation
* Not exhaustive
AdministrationTraining Environment
ThermoregulationHumidityAffective SupportCalm EnvironmentLighting ConditionsIntegration
Multidisciplinary team trainingBaby mannequins
Patient RecordMedication ControlTreatment logging
January, 20147
This presentationEnhancing neonatal care through smart sensor solutions
Focus on:• Thermoregulation and unobtrusive
temperature measurement• Unobtrusive ECG monitoring• Can monitoring help us predict
complications and prevent them earlier?
January, 20148
8
Thermoregulation and core temperature measurement

January, 20149
9
Thermoregulation
• Thermoregulation is the ability to balance between heat production and heat loss in order to maintain body temperature within a certain normal range.
• Need for thermoregulation: – To protect enzyme function
– To maximize metabolic efficiency– To reduce oxygen use– To reduce calorie expenditure – To promote growth and development
• New born babies are highly susceptible for heat loss and its adverse consequences (hypothermia) immediately after birth and during first few days of life.
January, 201410
10
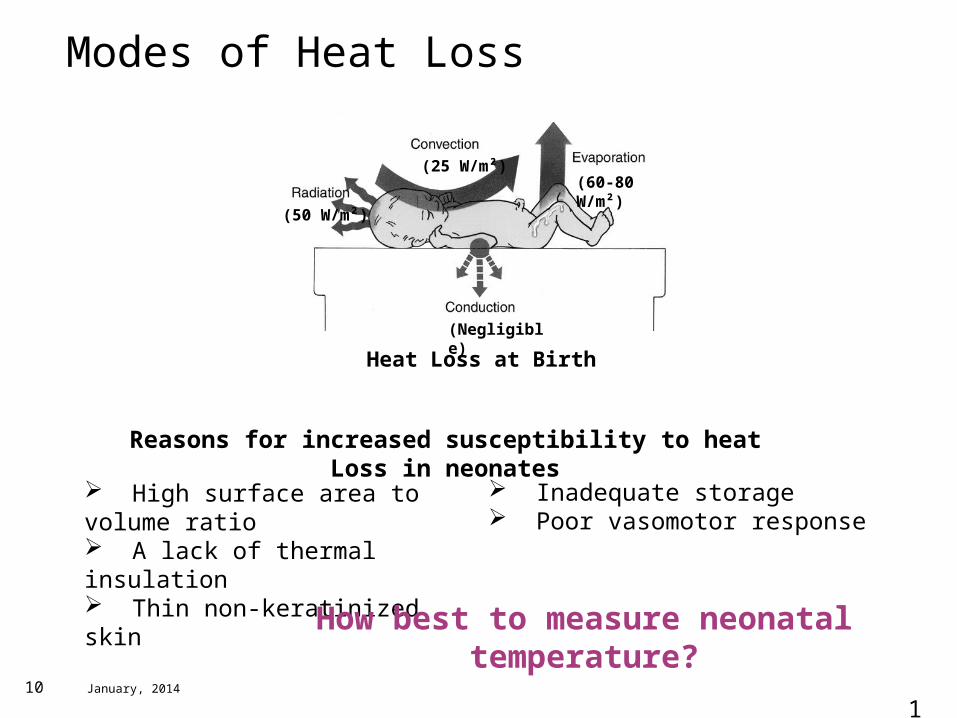
Modes of Heat Loss
High surface area to volume ratio A lack of thermal insulation Thin non-keratinized skin
(60-80 W/m²)(25 W/m²)
(50 W/m²)
(Negligible)
Heat Loss at Birth
Inadequate storage Poor vasomotor response
Reasons for increased susceptibility to heat Loss in neonates
How best to measure neonatal temperature?
January, 201411
Several methods for measuring temperatureContinuous, accurate?
• Spot-check temperature measurements (axillary)• Sensors in the diaper (isolated)• Rectal temperatures?• Do they really represent core temperature?
• Esophageal Temperature:– Surrogate for core temperature– Temperature changes can be sudden and
dramatic, not reflected by spot-check measurements.
Philips InnerSense Esophageal Temperature Probe+ Feeding Tube

January, 201412
Philips InnerSense Esophageal Temperature Probe+ Feeding Tube
Unobtrusive core temperature measurement
• A feeding tube containing temperature sensors to reliably measure core temperature.
• Temperature can be measured, displayed on the patient monitor and used for trend analysis.
• Recent study we did on 12 babies showed that this sensor is more stable than a skin sensor placed in the diaper especially during motion and kangaroo care.

January, 201413
13
Contactless ECG

January, 201414
NICU| Environment
• Many procedures are necessary and standard, and have reduced viability to 24 weeks. However, these same procedures can have side effects!
• Skin is incompletely developed (not until 34 weeks that the skin is functionally competent). Scars prevail in 10% of neonates in the NICU.
• ECG is important in observing neonatal conditions and can indicate life threatening events such as sepsis (infection).
• A closer look….
Adhesive electrodes
14
January, 201415
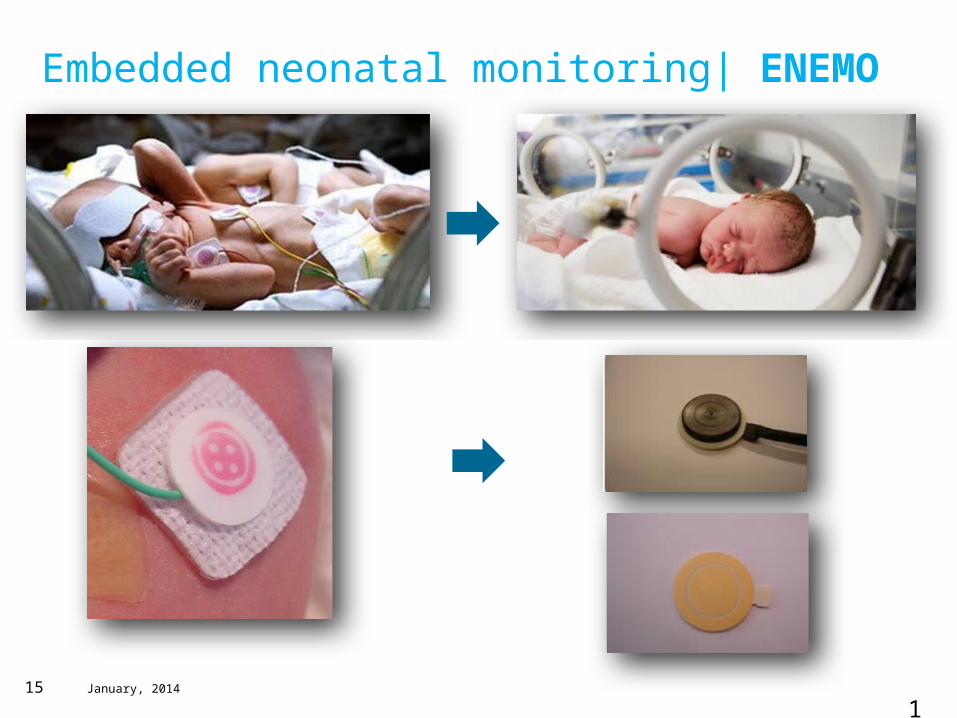
Neonate: improved comfort (less scars and pain)
Caregiver: less preparation time
Parents: improved parent-child bonding
Embedded neonatal monitoring| ENEMO
15
January, 201416
16
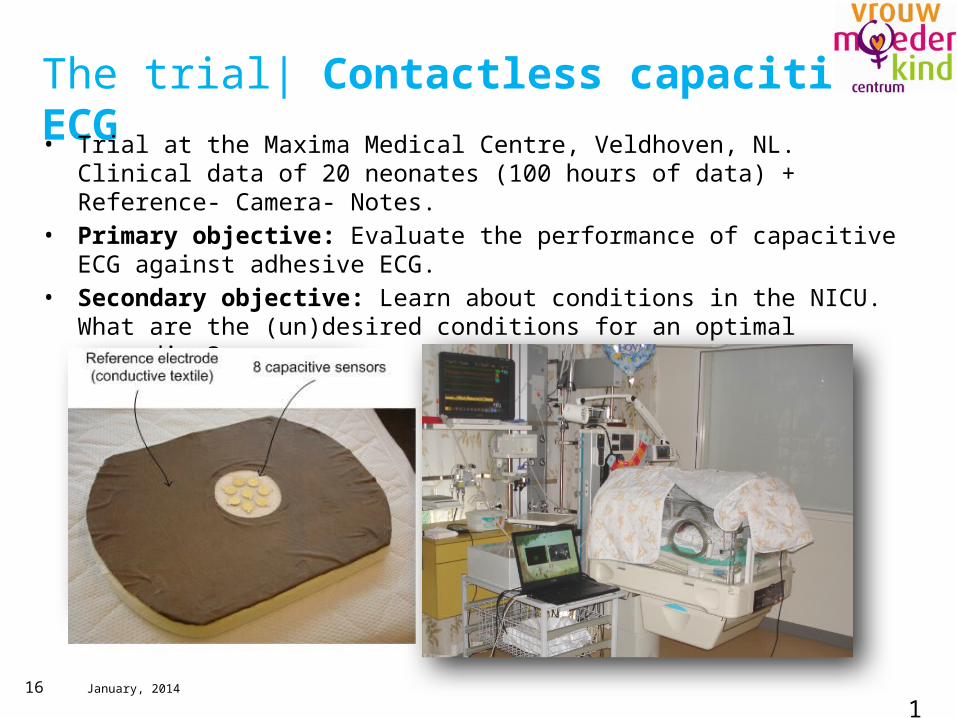
The trial| Contactless capacitive ECG• Trial at the Maxima Medical Centre, Veldhoven, NL. Clinical data of 20 neonates (100
hours of data) + Reference- Camera- Notes.• Primary objective: Evaluate the performance of capacitive ECG against adhesive ECG.• Secondary objective: Learn about conditions in the NICU. What are the (un)desired
conditions for an optimal recording?
January, 201417
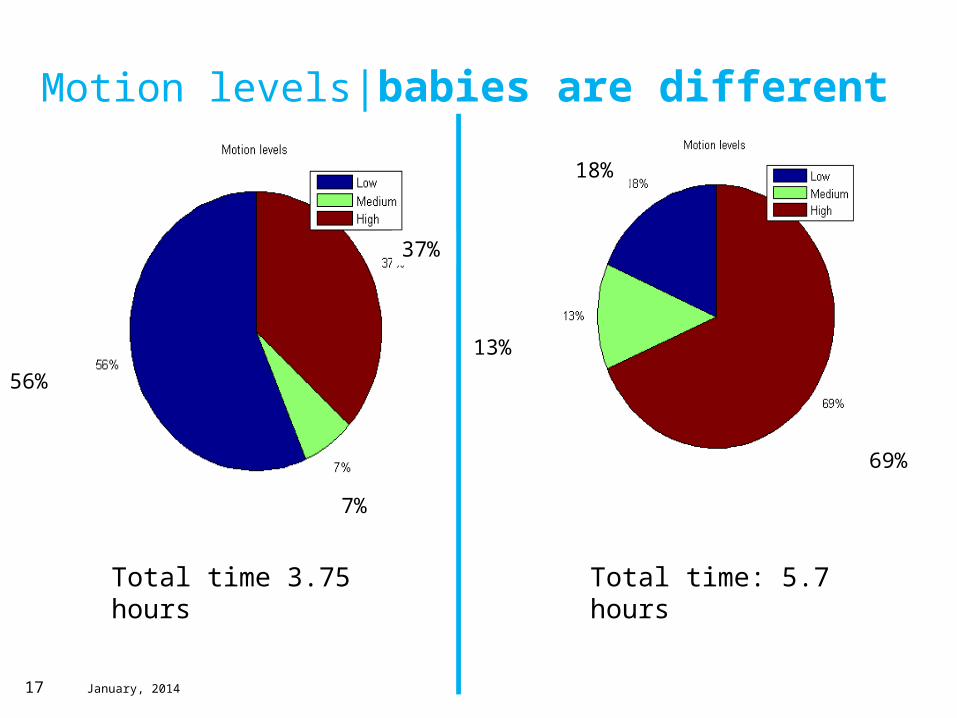
Motion levels|babies are different
Total time 3.75 hours Total time: 5.7 hours
37%
7%
56%
18%
13%
69%

January, 201418
Framework| The Vectorcardiogram
A graphic representation of the magnitude and direction of the electrical currents in the heart as a vector loop.
Vectorcardiogram (VCG)
January, 201419
VCG construction
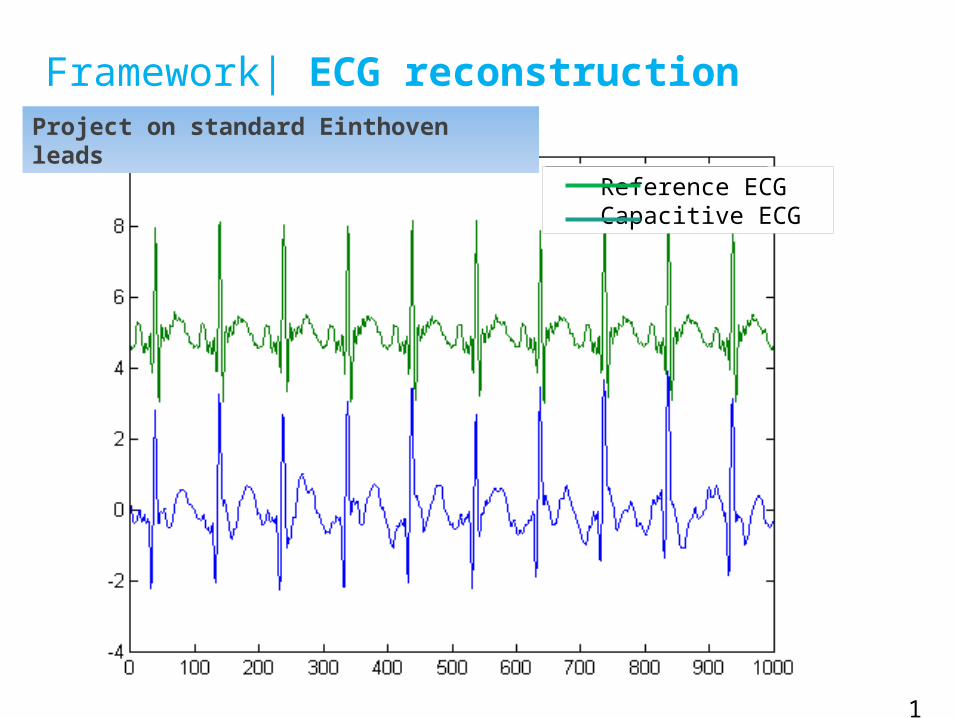
Framework| ECG reconstruction
Pre-processing/ subtracting motion artefacts
VCG Projection
ECG R-peak identification using wavelet techniques
Kalman filtering of channels (knowing beat locations)
VCG Projection (again)
Project on standard Einthoven leads
19
Reference ECGCapacitive ECG
January, 201420
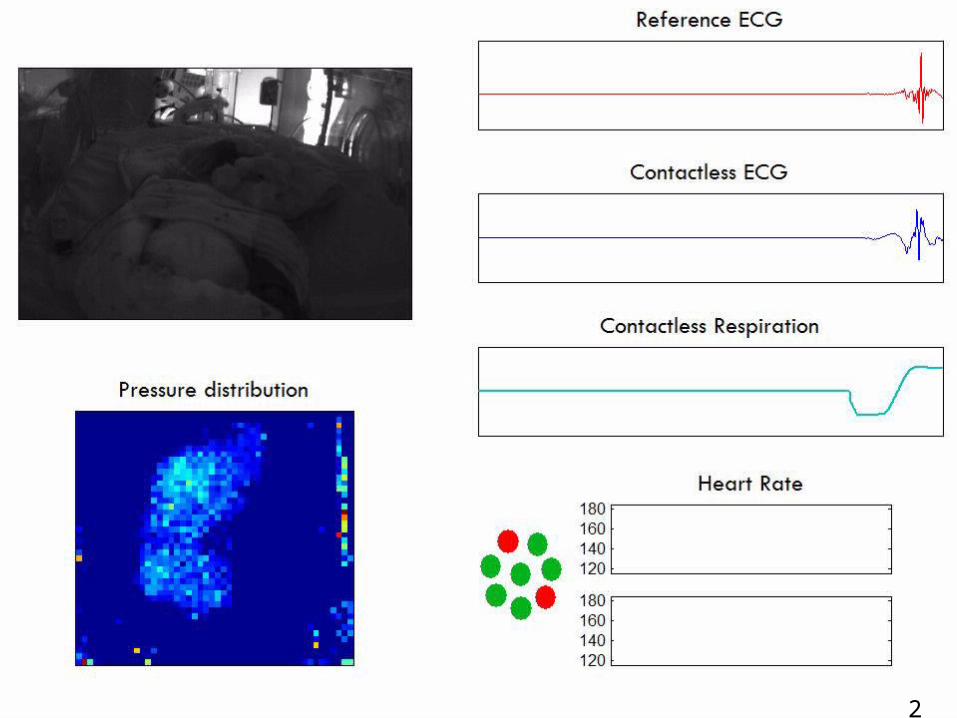
Framework| In real time…
20

January, 201421
Results| Instantaneous Heart Rate coverage
21
Perc
ent c
over
age
Baby number
Coverage: Total time with a good match.
Peak detection used to calculate true positives and negatives leading to Sensitivity and PPV.
Reference ECGCapacitive ECG
Coverage Low number of layers, mostly chest position, good sensor alignment
Very bad sensor alignment, side positioning
Perc
ent c
over
age
Baby number

January, 201422
Good conditions
Results| Effect of layers and positioningBaby 9
4 layers of cloth, side positioning 1 layer removed, chest positioning
22
Bad conditions
January, 201423
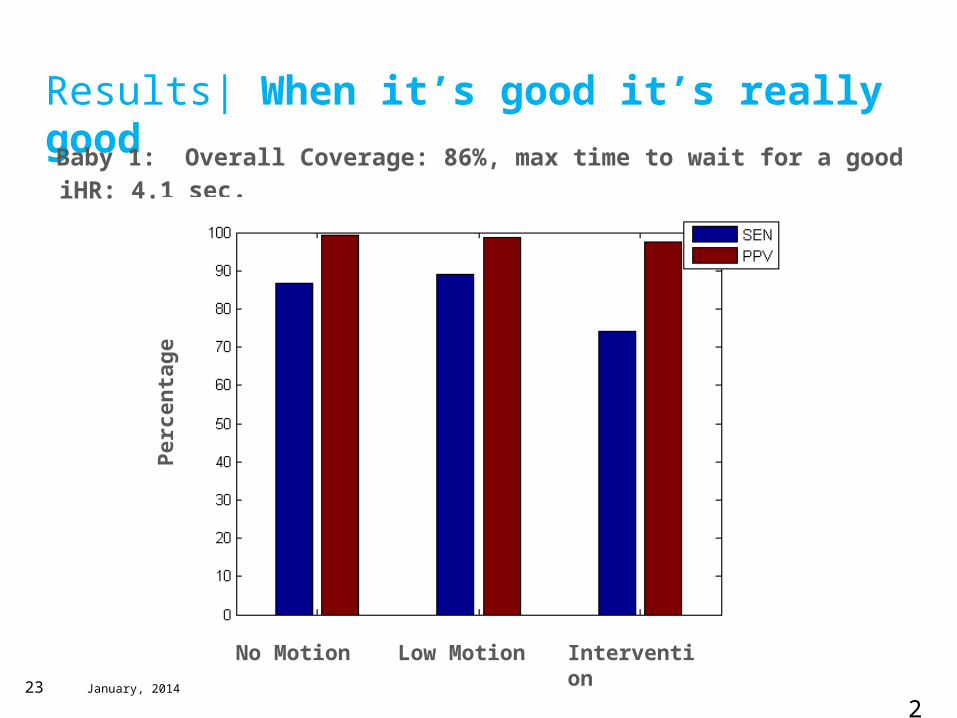
Results| When it’s good it’s really good
Baby 1: Overall Coverage: 86%, max time to wait for a good iHR: 4.1 sec.
No Motion Low Motion Intervention
Per
cen
tag
e
23

January, 201424
Results| ECG shape analysisParameter Mean difference (std)
in ms
RR distance -0.35(7.94)
QRS distance -6.1 (6.71)
PR distance 19.78(11.24)
QT distance -33.56(30.65)
Reference
Capacitive
R
P T
QS
R
P
T
Q
S
24
For more results see: PR-TN 2012/00614Capacitive ECG sensing in the NICU - design and results of the clinical feasibility study
Baby 1
January, 201425
25
NICU| ECG relevance• 7 Dutch and 10 international NICUs (UK, Spain, Ireland, USA,
Belgium) responded to a survey we sent.• ECG an important tool for screening: 90% of participants check it
regularly whereas 10% of participants check it only once in a while.
• In order of importance: HR, HR variation, Respiration rate, QRS shape variation.
• Instantaneous heart rate (iHR) an important parameter for Sepsis detection1. Sepsis is the most common cause of death for infants beyond 1 week of age.
1. Early non invasive diagnosis of sepsis in preterm infants (Griffin Ped Research 2003; Griffin Pediatrics 2005; Moorman IEEE 2006, Fairchild 2012).
January, 201426
26
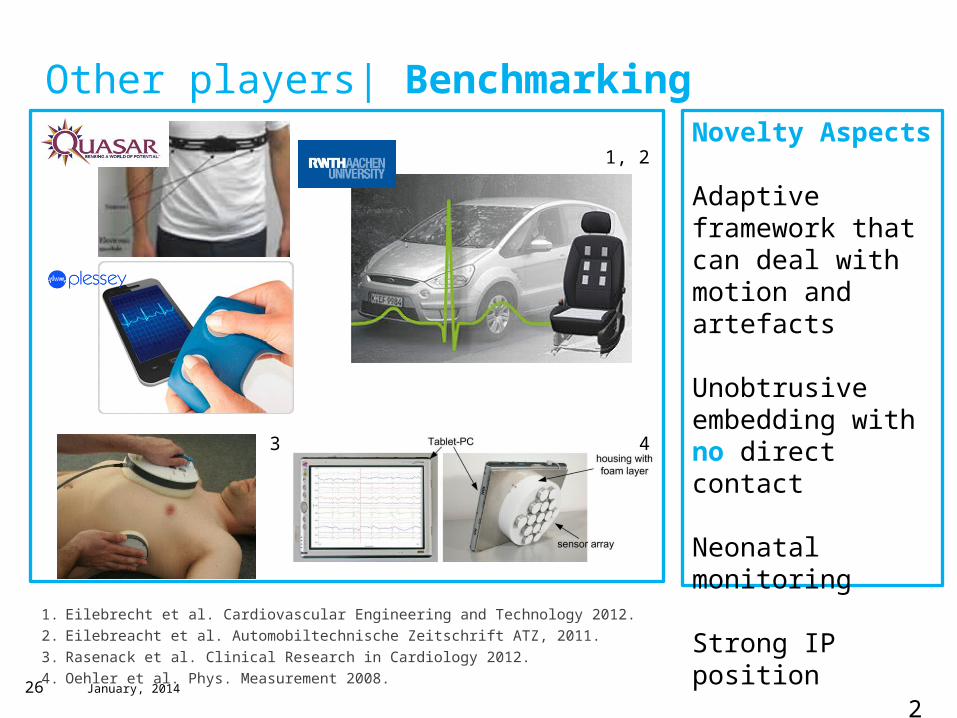
Other players| Benchmarking
1. Eilebrecht et al. Cardiovascular Engineering and Technology 2012.2. Eilebreacht et al. Automobiltechnische Zeitschrift ATZ, 2011.3. Rasenack et al. Clinical Research in Cardiology 2012.4. Oehler et al. Phys. Measurement 2008.
Novelty Aspects
Adaptive framework that can deal with motion and artefacts
Unobtrusive embedding with no direct contact
Neonatal monitoring
Strong IP position
3 4
1, 2
January, 201427
27
What can we do with instantaneous heart rate?

January, 201428
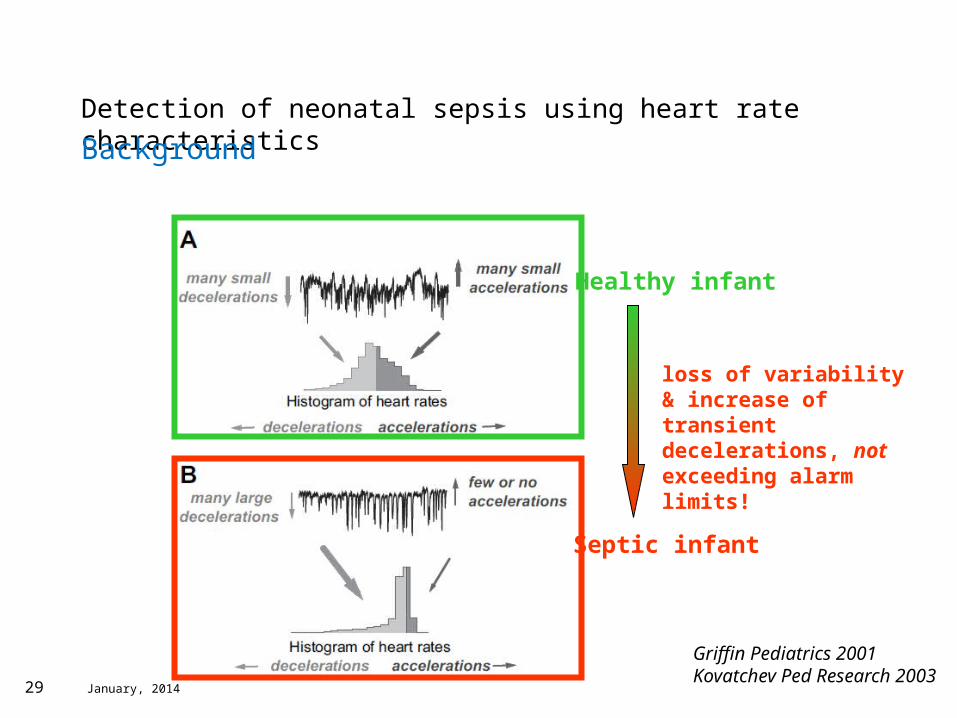
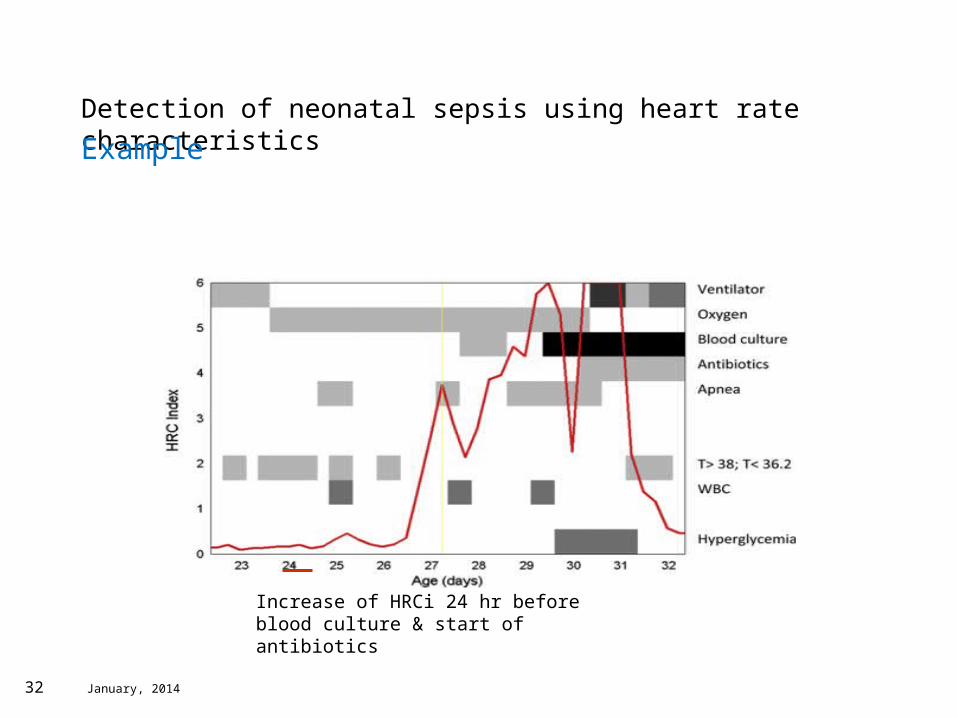
Detection of neonatal sepsis using heart rate characteristics
Background
• Late-onset sepsis (onset > 72 hr after birth): 30% of preterm very low birth weight infants experience sepsis during their NICU stay (Stoll 2002)
• Sepsis is the most common cause of death among preterm infants beyond the first week of life.
• Heart rate characteristics monitoring (e.g changes in heart rate pattern) have shown to aid in the early non invasive diagnosis of sepsis in preterm infants (Griffin Ped Research 2003; Griffin Pediatrics 2005; Moorman IEEE 2006).
January, 201429
Griffin Pediatrics 2001Kovatchev Ped Research 2003
Healthy infant
Septic infant
loss of variability & increase of transient decelerations, not exceeding alarm limits!
Detection of neonatal sepsis using heart rate characteristics
Background
January, 201430
• The HRCi is derived from regression modeling and uses measures of standard deviation (SD), sample symmetry (R1 and R2), and SampEn to estimate the risk of upcoming sepsis and sepsis-like illness.
• The formula for the HRC index is: HRCi = [exp(A) / 1+exp(A)]where: A = intercept + β1(SD) + β2(R1) + β3(R2) + β4(SampEn)
• The intercept and coefficients β are estimated from epidemiologic data on sepsis and sepsis-like illness in the NICU (training set)
Detection of neonatal sepsis using heart rate characteristics
Algorithm

January, 201431
HRCi percentiles correlate with risk for sepsis. Patients are classified into 3 risk categories. Low risk is defined as HRCi < 75th percentile (score <1). Medium risk (light gray boxes) includes infants with HRCi in the 75th to 90th percentile (score 1–2). The highrisk HRC group (dark gray box) has HRCi greater than 90th percentile (score >3).
Reference: Griffin Pediatrics 2005
Detection of neonatal sepsis using heart rate characteristics
HRCi as relative risk
January, 201432
Increase of HRCi 24 hr before blood culture & start of antibiotics
Detection of neonatal sepsis using heart rate characteristics
Example
January, 201433
33
In conclusion…

January, 201434
Conclusion
• Neonates are a very vulnerable population. Research in this area could benefit a lot from:– Unobtrusive and pervasive sensor systems.– Support for neonatal comfort, sleep and growth– Intelligent solutions using the data acquired for
early prediction of deterioration.– Support for nurses and clinicians for more
efficient and easier care.

January, 20143535
Fulfilling our ambitions in Mother and Child CareHolistic comprehensive portfolio
Incubatorsand warmers
OB Ultrasound
NeonatalRespiratory
Support
Fetal and maternal
monitoring
Neonatal patient monitoring
Feeding and
Specialtyproducts
Developmental Care Positioningaids
AventHome apnea monitoring
Jaundice diagnostic and therapy
January, 201436
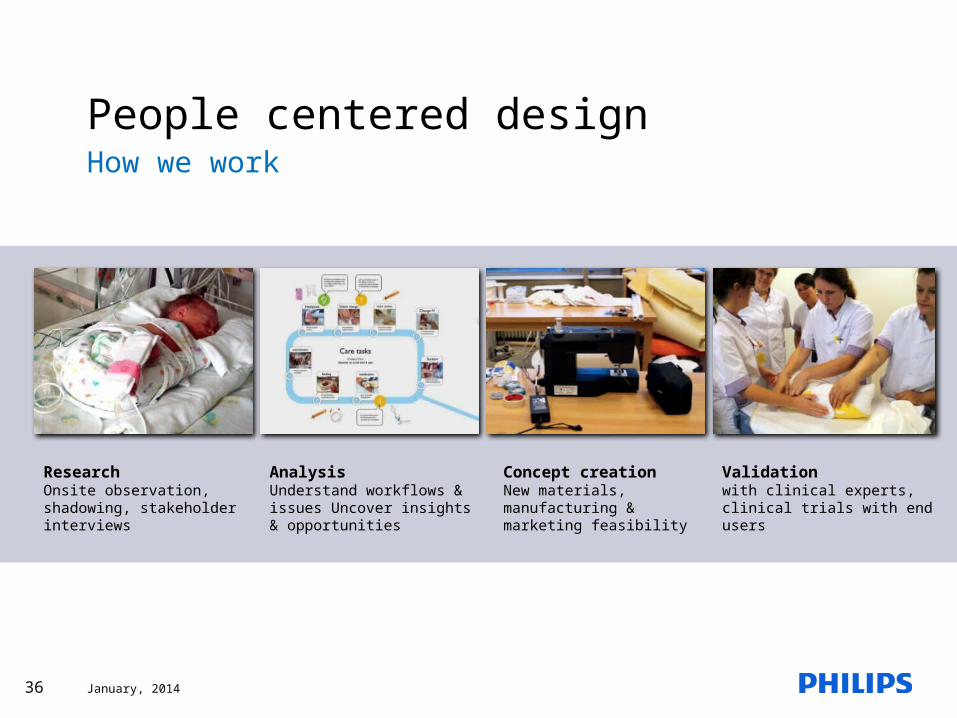
People centered designHow we work
Research Onsite observation, shadowing, stakeholder interviews
AnalysisUnderstand workflows & issues Uncover insights & opportunities
Concept creation New materials, manufacturing & marketing feasibility
Validation with clinical experts, clinical trials with end users

January, 201437
Acknowledgments | The teamCollaborators
• Wei Chen- TU/e
• Loe Feijs-TU/e
• Misha Croes-TU/e
• Dominika Potuzakova-TU/e
• Joanna Pilarczyk-TU/e
• Chris Nederhorst-RHF
• Hugo Zijlmans- AME
• Jos Bax (PINS)
• Mark Bogers (PINS)
Team
• Mohammed Meftah – Philips Research
• Martijn Schellekens- Philips Research
• Aline Serteyn- TU/e
• Rik Vullings-TU/e
• Jan Bergmans –TU/e
• Sidarto Bambang Oetomo- MMC/TU/e
• Astrid Osagiator-MMC
• Edwin Bongers-Philips Research
• Eefje Arts-Hornix- Philips Research
• Marjolein van Lieshout-Philips Research
• Vanessa Sattele-Philips Design
• Anton Janssen-Philips Research
Philips Business
• Siegfried Kaestle
• Amy Phillips
• Leslie Altimier
37

January, 201438