Welcome to the CPNP 2011 Town Hall Meeting. CPNP Walks for NAMI.
Upload
emmalee-anslowCategory
view
217download
0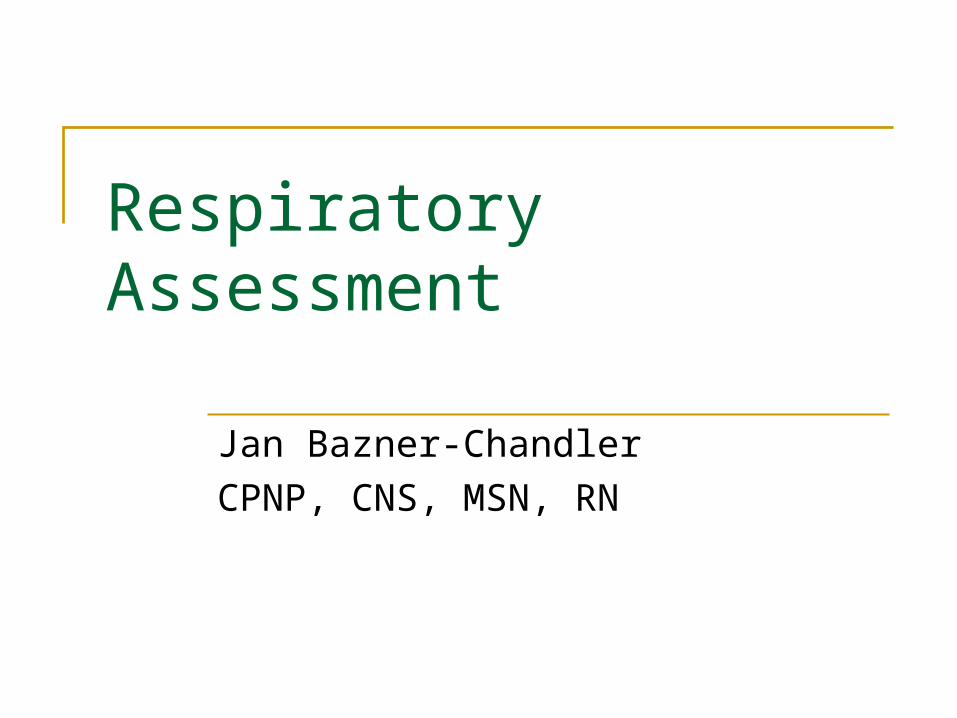
Jan Bazner-Chandler
CPNP, CNS, MSN, RN
Respiratory Assessment
Respiratory
Bifurcation of trachea Change in chest wall shape
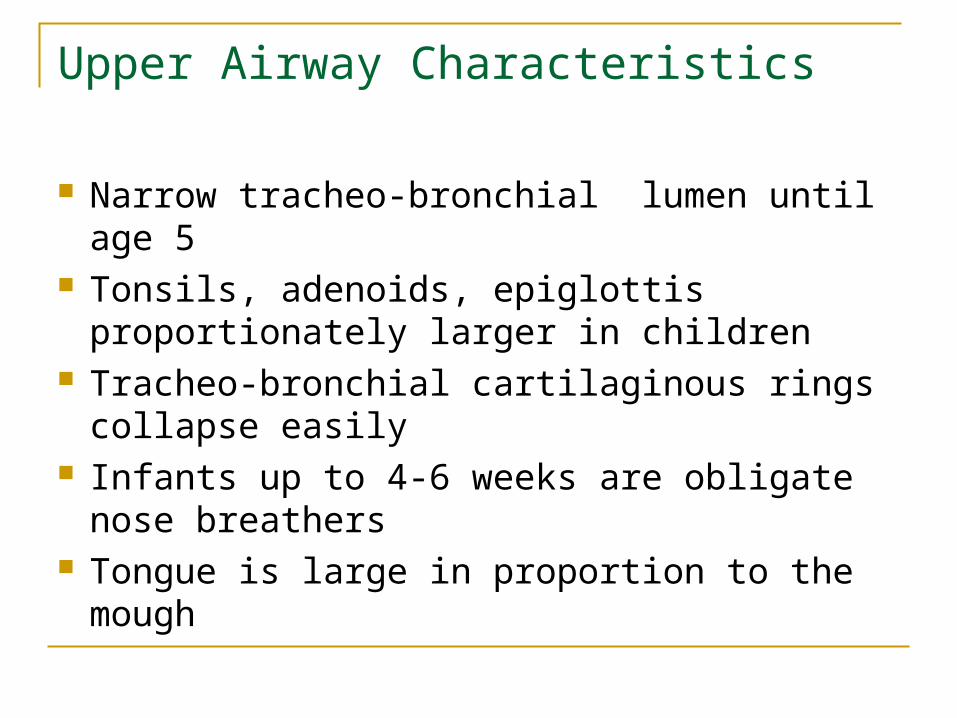
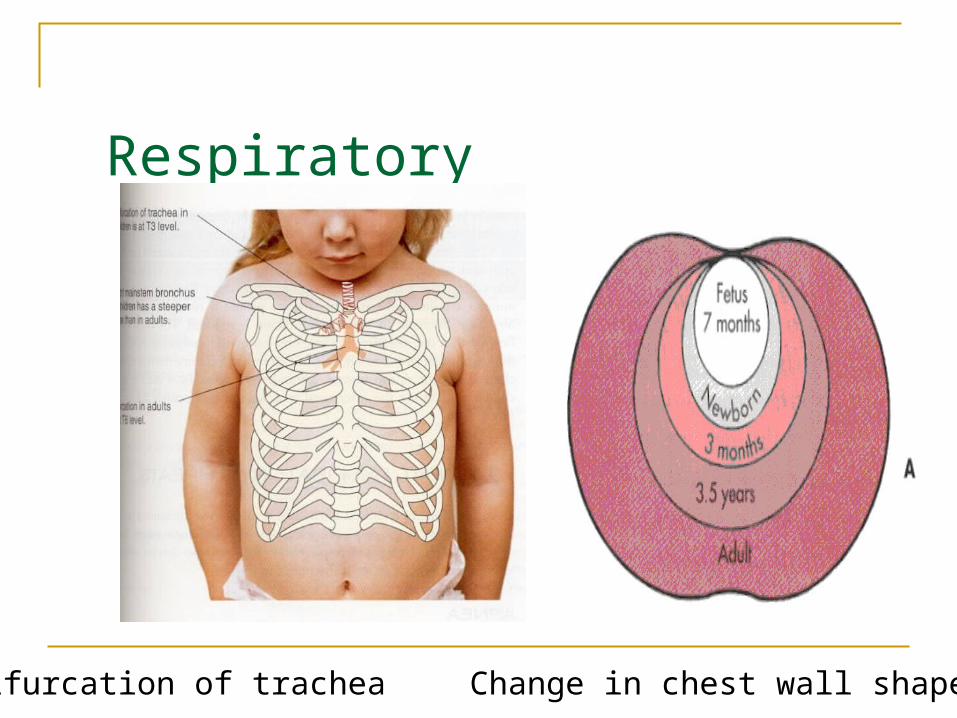
Upper Airway Characteristics
Narrow tracheo-bronchial lumen until age 5 Tonsils, adenoids, epiglottis proportionately
larger in children Tracheo-bronchial cartilaginous rings
collapse easily Infants up to 4-6 weeks are obligate nose
breathers Tongue is large in proportion to the mough
Lower Airway Characteristics Lack of firm bony structure to ribs/chest make
child more prone to retractions when in respiratory distress
Fewer alveoli in the neonate Poor quality of alveoli until age 8 Lack of surfactant that lines the alveoli in the
premature infant Inhibits alveolar collapse at end of expiration
Focused Health History
Reason for the visit Include questions about the environment
What makes condition worse – triggers Allergies
Past medical history: birth history, previous health problems, childhood illness, immunizations
Family medial history: respiratory illness – genetic link
Focused Physical Assessment
Types of breathing: Less than 7 years abdominal breathing
Greater than 7 years abdominal breathing can indicate problems
Respiratory Rate
Inspiratory phase slightly longer or equal to expiratory phase Prolonged expiratory phase = asthma Prolonged inspiratory phase = upper airway
obstruction Croup Foreign body

Color
Observe color of face, trunk, and nail beds
Cyanosis = inadequate oxygenation
Clubbing of nails = chronic hypoxemia
Respiratory Distress
Grunting = impending respiratory failure Severe retractions Diminished or absent breath sounds Apnea or gasping respirations Poor systemic perfusion / mottling Tachycardia to bradycardia Decrease oxygen saturations

Chest Muscle Retraction
Chest Retractions
Retractions suggest an obstruction to inspiration at any point in the respiratory tract.
As intrapleural pressure becomes increasingly negative, the musculature “pulls back” in an effort to overcome the blockage.
The degree and level of retraction depend on the extent and level of the obstruction.
Diagnostic Tests
Detects abnormalities of chest or lungs Chest x-ray Sweat chloride Test MRI Laryngoscope / bronchoscopy CT Scan
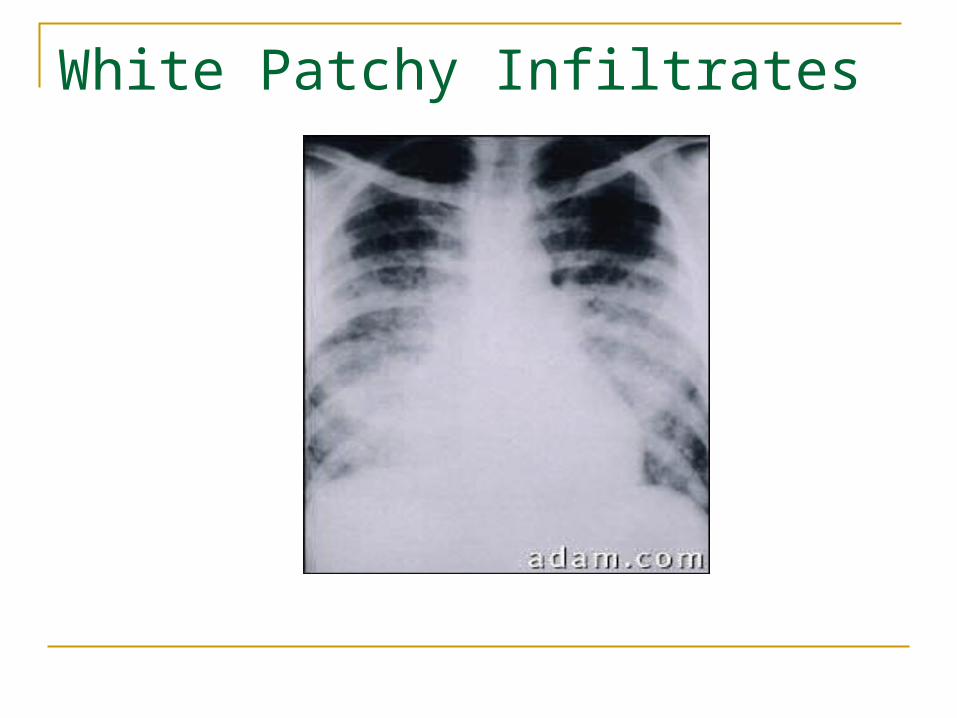
White Patchy Infiltrates
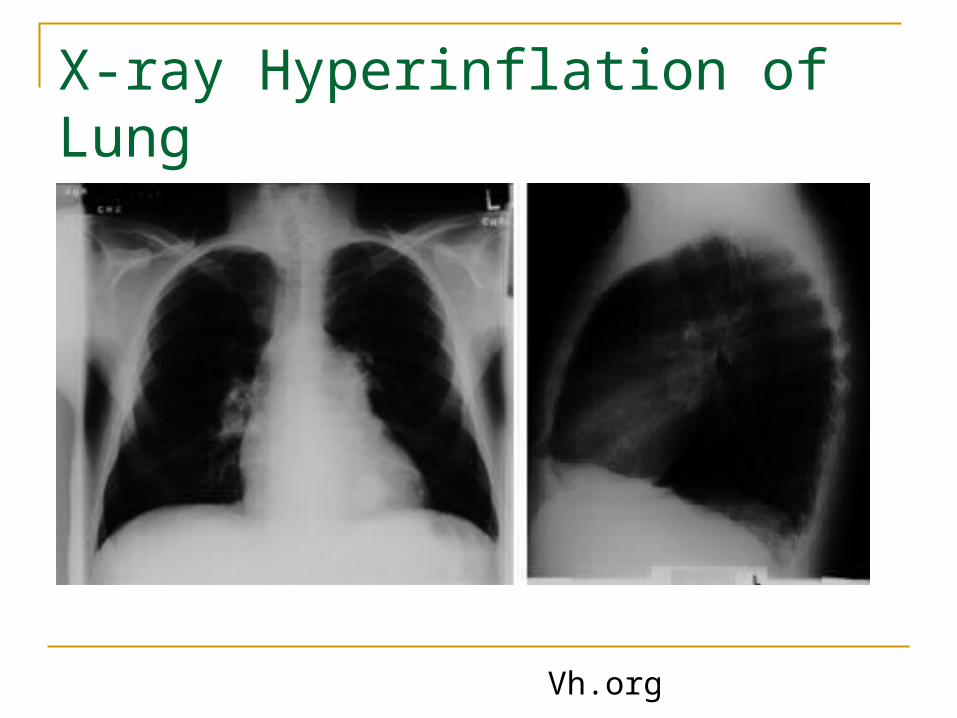
X-ray Hyperinflation of Lung
Vh.org

Pleural Effusion
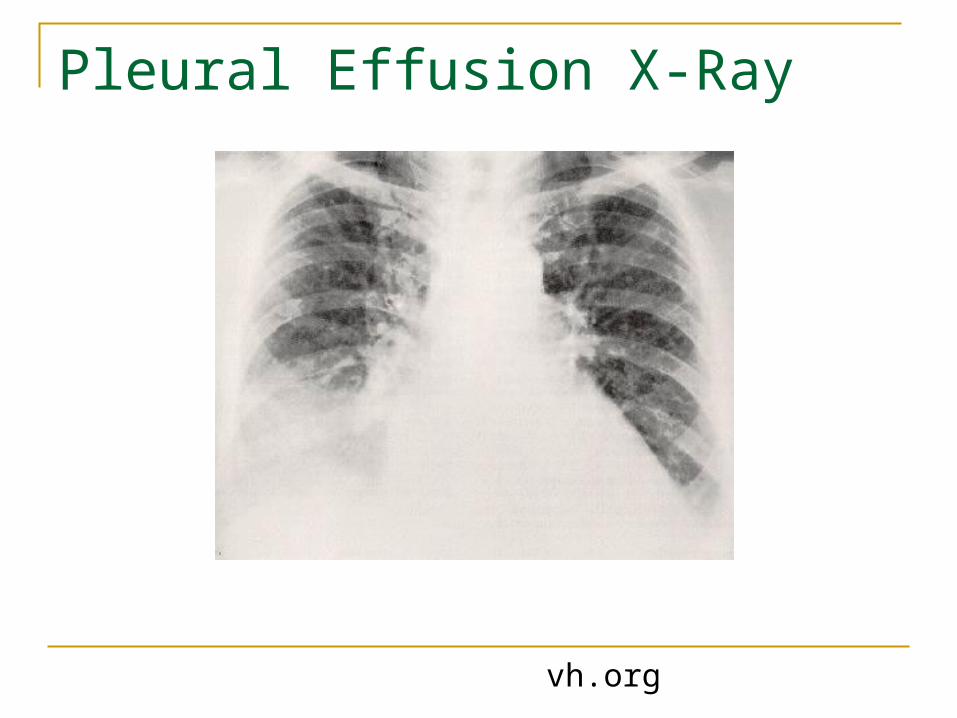
Pleural Effusion X-Ray
vh.org
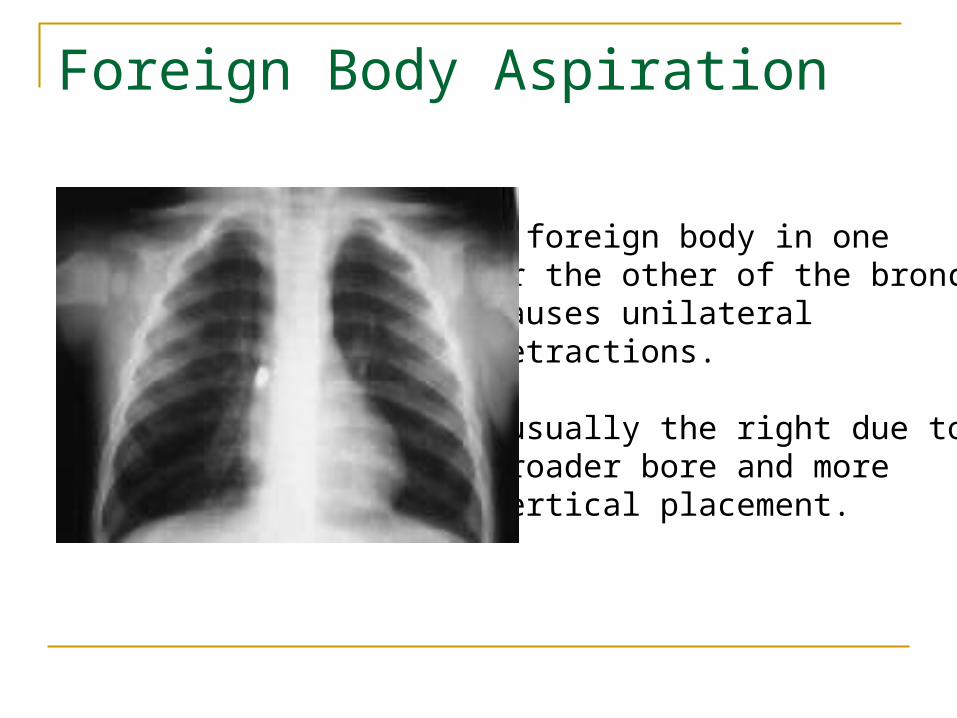
Foreign Body Aspiration
A foreign body in oneor the other of the bronchicauses unilateral retractions.
*usually the right due tobroader bore and more vertical placement.
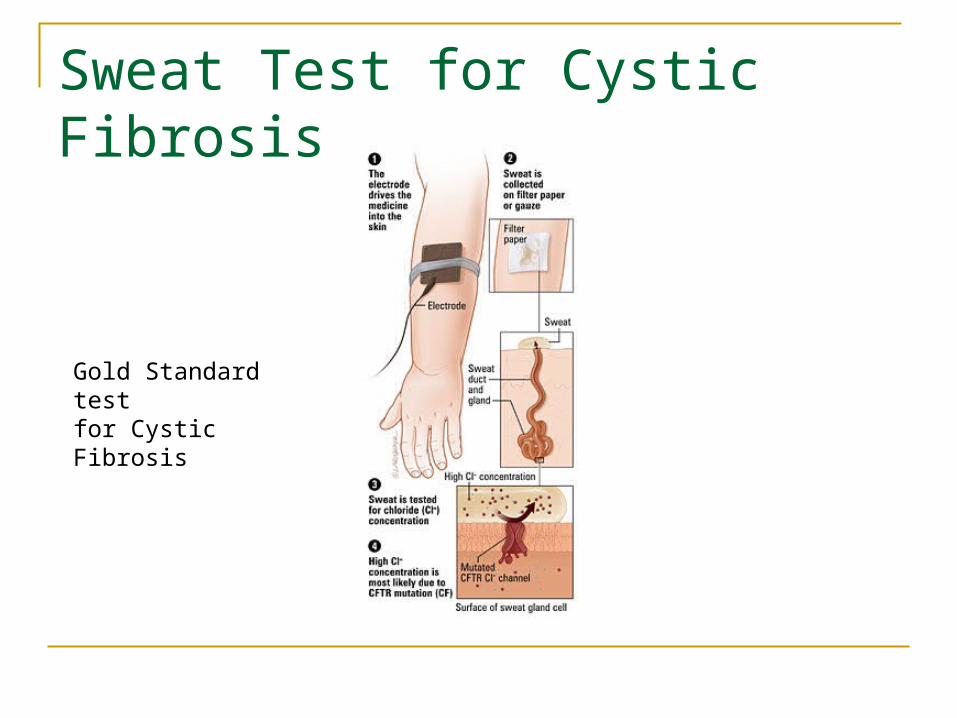
Sweat Test for Cystic Fibrosis
Gold Standard testfor Cystic Fibrosis

Oxygen Therapy: Nursing Interventions Proper concentration
Adequate humidity: make sure there is fluid in the bottle
Make sure prongs are in nose and that the nares are patent – suction out nares to increase oxygen flow
Monitor oxygen SATS: if alarm keeps on going off but the infant / child looks good, check the device
Monitor activity level or infant / child
Aerosol Therapy
Respiratory Therapist will do the treatment Communicate with therapist – eliminated
needless paging for treatments Treatment should be done before the infant
eats When you make your morning rounds assess
if there is any infant / child that needs an immediate treatment

Home Teaching Inhaled Medications Correct dosage Prescribed time Proper use of inhaler No OTC drugs Encourage fluids When to call physician
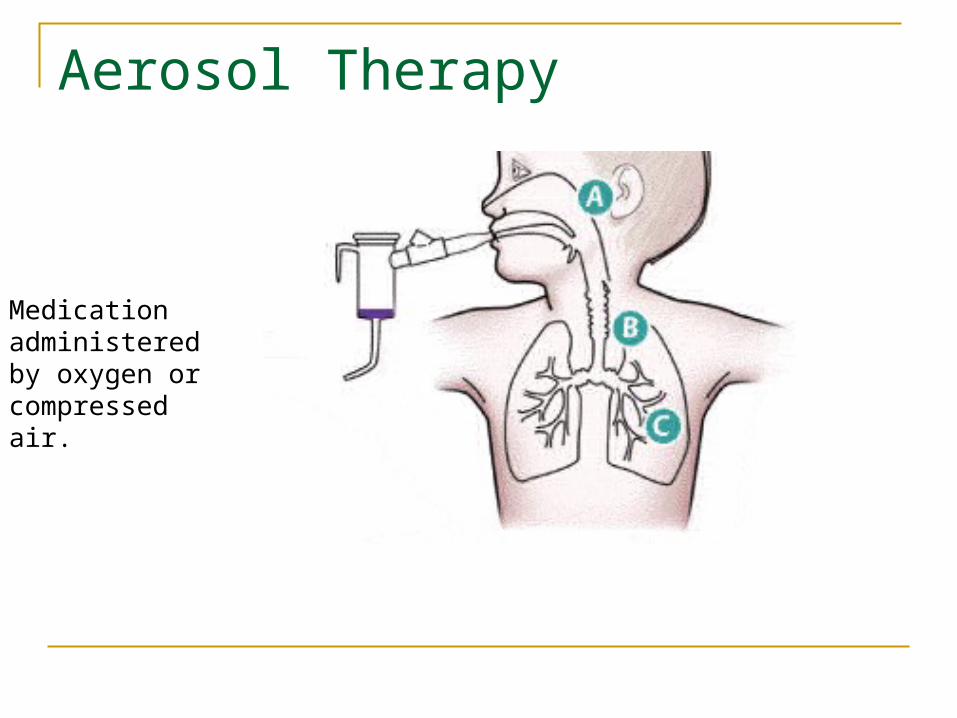
Aerosol Therapy
Medicationadministeredby oxygen or compressedair.

Outpatient Aerosol Treatment
Postural Drainage and Percussion In the small child you can position on your lap Do first thing in the AM Do before meals or one hour after Do after the aerosol treatment since the
treatment will help open the airways and loosen the mucous
Suction the infant after treatment – teach parents to do bulb suction

Percussion and postural drainage

Mechanical Ventilation

Alterations in Respiratory Function

Severe Respiratory Distress
• Nasal flaring and grunting• Severe retractions• Diminished breath sounds• Hypotonia• Decreased oxygen saturations
What to do if infant / child in respiratory distress! Stimulate the infant / child - remember crying or
activity will help mobilize secretions and expand lungs
Have the older child sit up take deep breaths and cough
Chest percussion to loosen secretions Give oxygen Assess if interventions work Call for help if you need it – pull the emergency cord
– yell for help