
အမည္ - ေအဂ်င္စီ - IEP · PDF fileသီးျခားပညာေရးအစီအစဥ္ (iep) ေမရီလန္းျပည္နယ္ပညာေရးဌာန
Upload
bahlinnmCategory
view
249download
0
Level I Compliance 2015
Isolated head injuries linked to shock and hypotension
According to current ATLS guide-
lines, “For all practical purposes,
shock does not result from isolat-
ed brain injuries.”(1) Following
these guidelines, when shock is
identified, immediate resuscita-
tion with fluid boluses followed
by blood products as needed.
Shock associated with trauma is
often thought to be hemorrhagic
but emerging evidence is suggest-
ing that it could also be associated
with isolated head injuries (IHI).
One study set out to identify if
presenting hypotension could
indeed be associated with ISI.
The study was able to utilize 2009
data from the National Trauma
Data Bank (NTDB) and extract
78,673 patients with relevant data
recorded. (2)
Their results concluded that
among patients with IHI, the
rates of hypotension were greatest
in the 0-4 years of age grouping.
In fact, researchers found that
within this age group, one third
of hypotension was associated
with IHI as opposed to one fifth
with hemorrhagic injury and only
one hundredth with spinal cord
injury.
Several causes of this finding were
hypothesized including a possible
neurogenic response similar to
spinal shock or an autonomic
process with increased vagal tone
or poor sympathetic tone.
Because of the association of
increased cerebral edema with
large volumes of isotonic fluids,
providers may have to adjust their
treatment plans to include less
volume resuscitation and early
administration of vasopressors to
increase sympathetic tone or atro-
pine to block increased vagal
tone.
M O N R O E C A R E L L J R . C H I L D R E N ’ S H O S P I T A L A T V A N D E R B I L T
January 20, 2016
Volume 4, Issue 1
Pediatric Trauma Service IEP Special points of
interest:
Remember after re-
viewing the IEP con-
tent, you must suc-
cessfully pass the
post-test in order to
receive assigned CME
credit of 1.5 hr.
Inside this issue:
WBCT scanning in adult and pediatric centers
2
Benefits of protocol utilization in association with abdominal trauma
2
MCJCHV Abdominal Trauma Work-Up Algorithm
3
MCJCHV Chest Trauma Work-Up Algorithm
3
MCJCHV CHI ≥2 yo Work-Up Algorithm
4
MCJCHV CHI <2 yo Work-Up Algorithm
5
Vascular injuries in pediatric
6
References 6
Jan Feb Mar Apr May Jun Jul Aug Sept Oct Nov Dec Total
Total 9 8 8 10 16 13 17 10 15 4 7 16 133
Present 8 6 7 10 12 12 15 8 15 3 5 12 113
No show 1 2 2 1 1 2 1 1 4 15
Time not 1 1
Past time 1 2 1 4
Percentage 86% 75% 88% 100% 82% 92% 88% 80% 100% 75% 71% 75% 85%
For Level I activations, attendings &/or fellows have 15 minutes to respond to the bedside from time of arrival.
Per ACS, Level I facilities must maintain 80% or greater

Over the last 20 years, there has been a
fivefold increase in the utilization of CT
scans in pediatric patients who present
to the emergency department, with head
injury being the most frequent
indication that prompts CT scan use.
(3) With the rising awareness of
radiation-induced malignancy, a
nationwide push towards limiting the
use of CT scans has been observed since
2008. In the pediatric population,
physicians often rely on these radiology
studies since physical exam may be an
unreliable means of identifying injuries.
One study examined the frequency of
CT utilization, specifically whole body
computed tomography (WBCT), in
adult versus pediatric trauma centers.
Utilizing the National Trauma Data
Bank (NTDB), they were able to identify
30,667 patients to include in the study,
of which 38.3% were managed at a
designated pediatric trauma center. (3)
The following factors were linked to
the use of WBCT scanning: age ≥ 6
years, male gender, intoxication, GCS
score ≤ 8, hypotension and tachycardia
on presentation, blunt injury, motor
cycle collision, head, thoracic or
abdominal AIS ≥ 3, injury severity
score ≥ 25 and management in an
ATC. After adjusting for age, GCS
score, admission vital parameters,
mechanism, type and severity of injury,
patients who presented in an ATC
were 1.8 times more likely to undergo
a WBCT scan ultimately increasing
their risk of radiation without a
difference in outcomes. There was no
noted difference in hospital and ICU
length of stay as well as hospital
disposition between adult and
pediatric center patients that received
WBCTs.
Of note, head CT rates did not differ
between adult and pediatric trauma
centers, however the use of thoracic and
abdominal CTs were significantly higher
in the adult programs. (3) This may be
attributed to the utilization of
guidelines and prediction models put in
place at pediatric trauma centers. These
guidelines recommend selective imaging
based on mechanism of injury, physical
examination, and laboratory studies.
At MCJCHV, liaisons from PEM,
PICU, Trauma, NSGY, Ortho, ANES,
and Radiology have collaborated to
establish recommended radiology work-
ups for trauma patients presenting with
blunt chest, blunt abdominal, and
closed head injuries. These are
included in this issue for your review.
should take into account the patient’s GCS, reliability of an abdominal exam, and the presence of abdominal wall bruising.
One designated pediatric trauma center instituted their own protocol in hopes of decreasing the negative CT rate and the cost of laboratory studies utilized in the evaluation of abdominal trauma. (5) After institut-ing their evidenced based protocol, the rate of positive CT scan findings increased from 23% to 49%. For them, protocol deviation occurred most frequently in the conscious, reliable exam group (40%) with the scans being obtained in the absence of abdominal tenderness/pain or lack of surgery consult prior to the scan.
When evaluating pediatric patients, assessing for abdominal trauma can be challenging due to few external signs, unreliable communication, difficulty obtaining an accurate abdominal exam, a physiological reserve that maintains normotension despite ongoing volume loss, and injury patterns specific to cer-tain age groups. (5) CTs of the abdo-men and pelvis are routinely obtained for adult patients if the physical exam is unreliable. However with children, current data suggests judicious use of CT radiation due to the increased can-cer risk. Many institutions have report-ed overuse of CT scanning in pediatrics, especially when evaluating for ab-dominal trauma. Guidelines determin-ing the diagnostic work up in children
Only 8% of patients had clinically sig-nificant scans when the protocol was not followed as opposed to 31% when the protocol was followed.
This protocol also led to the reduction of total laboratory costs of 39%. The protocol specified ordering a HGB/HCT and AST/ALT instead of a CBC and CMP or liver panel.
The majority of studies covering the topic recommend a combination of specific laboratory studies and physical exam in determining the need for CT. Specifically hematuria and elevated ALT with an abnormal abdominal exam are the best predictors of intra-abdominal injury.
Utilization of whole body CT scans in adult and pediatric trauma centers
The benefits of protocol utilization in abdominal trauma
Page 2
Pediatric Trauma Service IEP
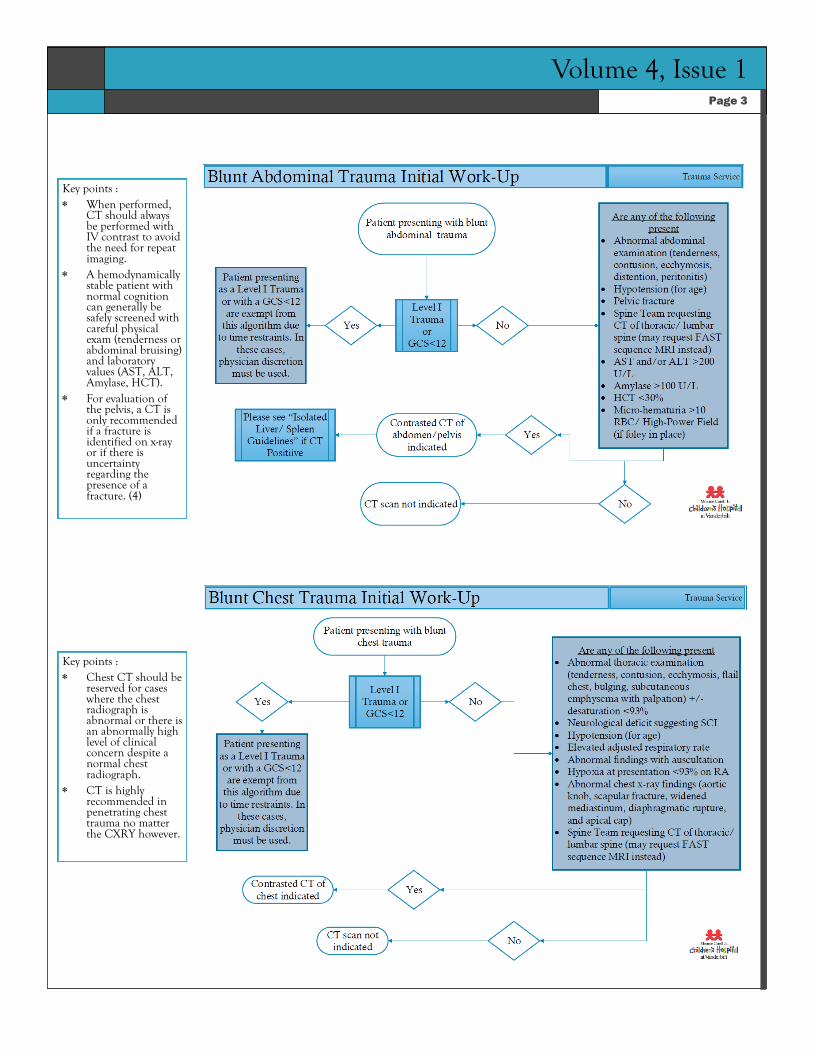
Key points : When performed,
CT should always be performed with IV contrast to avoid the need for repeat imaging.
A hemodynamically stable patient with normal cognition can generally be safely screened with careful physical exam (tenderness or abdominal bruising) and laboratory values (AST, ALT, Amylase, HCT).
For evaluation of the pelvis, a CT is only recommended if a fracture is identified on x-ray or if there is uncertainty regarding the presence of a fracture. (4)
Page 3
Volume 4, Issue 1
Key points : Chest CT should be
reserved for cases where the chest radiograph is abnormal or there is an abnormally high level of clinical concern despite a normal chest radiograph.
CT is highly recommended in penetrating chest trauma no matter the CXRY however.

Pediatric Trauma Service IEP

Volume 4, Issue 1

Epidemiology Account for only 0.6%-1.4% of all pediatric injuries. Upper extremity injuries most common in 2-6 years of age. Lower extremity injuries most common in >12 years of age. Brachial artery injuries occur in 53% of cases followed by
popliteal at 9.5%, and the common femoral arties at 5.9%.
Fallon, S., Delemos, D., Akikuotu, A., Christopher, D., & Naik-Mathuria, B. (2016). The use of an institutional pediatric abdominal trauma protocol improves resource use. Journal of Trauma and Acute Care Surgery, 80(1), 57-63.
Gardner, A., Diz, D., Tooze, J., Miller, C., & Petty, J. (2015). Injury patterns associated with hypotension in pediatric trauma patients: A national trauma database review. Journal of Trauma and Acute Care Surgery, 78(6), 1143-1148.
Pandit, V., Michailidou, M., Rhee, P., Zangbar, B., Kulvatunyou, N., Khalil, M., . . . Joseph, B. (2015). The use of whole body computed tomography scans in pediatric trauma patients: Are there differences among adults and pediatric centers? Journal of Pediatric Surgery.
Pierce, D., Mangona, K., Bisset, G., & Naik-Mathuria, B. (2015). Computed tomography in the evaluation of pediatric trauma. Clinical Pediatric Emergency Medicine, 16(4), 220-229.
Wahlgren, C., & Kragsterman, B. (2015). Management and outcome of pediatric vascular injuries. Journal of Trauma and Acute Care Surgery, 79(4), 563-567.
References
Pediatric Trauma Service IEP
Vascular injuries
Operative techniques Repair techniques include interposition graft (24%),
patch (19%), primary repair- lateral suture/direct anastomosis (12%), bypass (9.5%), endovascular techniques (3.7%), and miscellaneous- i.e., thrombectomy, thrombendarterectomy, ligation(8.1%)
Exploration or release of artery was performed 23% of the time.
Vein is the leading graft material followed by synthetics. In younger patients (≤10 years), patch repair techniques
were more common (28% vs. 9.6%). In the older pediatric population (11-15 years),
reconstruction with interposition and bypass grafts was more common (49% vs. 23%).
Complications and follow-up Arterial occlusion/thrombosis most common
postoperative complication. Amputations are associated with occluded vein grafts in
reconstructions at the level of the femoral artery.
CME instructions


















