j.1528-1167.2012.03622.x
12
Causes of status epil epti cus Eugen Tr inka, Juli a Ho ¨ fler, and Al exander Zerbs Depar tment of Neur ology, Chri stian Doppl er Klinik , Parac elsus Medica l Unive rsity Salzbu rg, Salzbu rg, Austr ia SUMMARY Status epilepticus (SE) is the most extreme form of epilepsy. It describes a prolonged seizure that may occur in patients with previous epilepsy or in acute disorders of the central nervous system. It is one of the mos t commonneurolo gic eme rge ncie s, with an incidence of up to 41 per 100,000 per year and an esti mated mort ali ty is 20%. The three major determinants of prognosis are the duration of SE, patient age, and the underlying cause. Com- mon and easily recognized causes of SE include cer ebrovascular disorders, brain trauma, infec- tions, and low antiepileptic drug levels in patients with epile psy. Les s common causes pr esent a clini- cal and diagnostic challenge, but are major deter- minants of prognosis. Among them, inflammatory causes and inb orn errors of metabolis m have gai ned wide int ere st; recent insights into the se causes have con tributed to a better unders tanding of the pathophysiology of SE and its appropriate tre atment . This rev iew focuses on the different etiologies of SE and emphasizes the importance of prompt recognition and treatment of the underly- ing causes . KEY WORDS: Status epi lepticus – eti ology, Tre at- ment, Progn osis. Statu s epilepticu s (SE) is a term used to descr ibe a pro- longed and self-sustaining seizure that may have overt, subtle, or almost no behavioral manifestations. It may be regarded as the most extreme form of epilepsy, or as an expression of an acute and often life-threatening brain dis- order, such as stroke, encephalitis, or trauma. Mortality asso cia ted wit h SE is up to 20% (Sh orv on, 1994; Log ros cin o et al., 1997, 2005). Less than 50% of people in SE have had previous seizures or epilepsy (DeLorenzo et al., 1996; Hes dor ffer et al. , 199 8; Coe yta ux et al. , 2000; Kna ke et al., 2001; Vignatelli et al., 2003). SE is one of the most common neurologic emergency, with an overall annual incidence of 10–41 per 100,000 (DeLo renzo et al., 1996; Hes dor ffer et al., 1998; Coe yta ux et al. , 2000; Kna ke et al., 2001; Vigna telli et al., 2 003). Up to 287,000 patien ts per year are affected in Europe. Not all forms of status are life-threatening and, given the variety of its clinical pre- sentations, the management must be tailored according to the type of SE and the underlying cause. Three major factors determine an increased risk of mortality and mor- bidity associated with SE: (1) certain etiologies, (2) age >60 yea rs, and (3) long dur atio n of SE (To wne et al. , 1994; DeLorenzo et al., 1996; Wu et al., 2002; Rossetti et al., 2006). This review focuses on the various causes of SE, since etiology is increasingly recognized as one of the most important factors for prognosis and outcome. There- fore, identifying and treating the underlying cause of SE is at least as important as prompt and effective treatment with early termination of seizures. Definition and Classification of Status Epilepticus Status epilepticus (SE) has been recognized for centu- rie s (Shorvon, 1994; Wolf et al., 2009). He nri Gas taut (1970) recognized SE as a prolonged seizure with as many forms as there were types of epileptic seizures. Therefore, SE classification mirrored exactly the seizure classifica- tion. In the International League against Epilepsy (ILAE) 1981 Classification, SE was defined as ‘‘ a seizure that per- sists for a sufficient length of time, or repeated frequen tly enough that re cove ry between at tacks do [does] not occur’’ (Commission on Cla ssif ica tion , ILAE, 198 1). Gen eralized ton ic–clonic seizures usuall y do not las t longer than 2–3 min (Theodore et al., 1994); the risk of a seizure becoming self-sustaining increases as the duration reaches 5 min or more (Lowenstein et al., 1999). For the purpose of this review, we use a clinical classification Address correspondence to Eugen Trinka, Department of Neurology, Christi an Dopple r Klinik, Parace lsus Medical Unive rsity, Ignaz Harrer Straße 79, 5020 Salzbu rg, Austri a. E-mail : [email protected] Wiley Perio dical s, Inc. ª 2012 Intern ationa l Leagu e Agains t Epilep sy Epilepsia, 53( Suppl. 4): 127– 138, 2012 doi: 10.1111/j.1528-1167.2012.03622.x SEIZURES IN SPECIAL AND SEVERE SITUATIONS 127
-
Upload
alex-gasnas -
Category
Documents
-
view
220 -
download
0
Transcript of j.1528-1167.2012.03622.x

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 1/12
Causes of status epilepticusEugen Trinka, Julia Hofler, and Alexander Zerbs
Department of Neurology, Christian Doppler Klinik, Paracelsus Medical University Salzburg, Salzburg, Austria
SUMMARY
Status epilepticus (SE) is the most extreme form
of epilepsy. It describes a prolonged seizure that
may occur in patients with previous epilepsy or in
acute disorders of the central nervous system. It is
one of the most common neurologic emergencies,
with an incidence of up to 41 per 100,000 per year
and an estimated mortality is 20%. The three
major determinants of prognosis are the duration
of SE, patient age, and the underlying cause. Com-
mon and easily recognized causes of SE include
cerebrovascular disorders, brain trauma, infec-
tions, and low antiepileptic drug levels in patients
with epilepsy. Less common causes present a clini-
cal and diagnostic challenge, but are major deter-
minants of prognosis. Among them, inflammatory
causes and inborn errors of metabolism have
gained wide interest; recent insights into these
causes have contributed to a better understanding
of the pathophysiology of SE and its appropriate
treatment. This review focuses on the different
etiologies of SE and emphasizes the importance of
prompt recognition and treatment of the underly-
ing causes.
KEY WORDS: Status epilepticus – etiology, Treat-
ment, Prognosis.
Status epilepticus (SE) is a term used to describe a pro-
longed and self-sustaining seizure that may have overt,
subtle, or almost no behavioral manifestations. It may beregarded as the most extreme form of epilepsy, or as an
expression of an acute and often life-threatening brain dis-
order, such as stroke, encephalitis, or trauma. Mortality
associated with SE is up to 20% (Shorvon, 1994; Logroscino
et al., 1997, 2005). Less than 50% of people in SE have
had previous seizures or epilepsy (DeLorenzo et al., 1996;
Hesdorffer et al., 1998; Coeytaux et al., 2000; Knake
et al., 2001; Vignatelli et al., 2003). SE is one of the most
common neurologic emergency, with an overall annual
incidence of 10–41 per 100,000 (DeLorenzo et al., 1996;
Hesdorffer et al., 1998; Coeytaux et al., 2000; Knake
et al., 2001; Vignatelli et al., 2003). Up to 287,000 patients
per year are affected in Europe. Not all forms of status are
life-threatening and, given the variety of its clinical pre-
sentations, the management must be tailored according to
the type of SE and the underlying cause. Three major
factors determine an increased risk of mortality and mor-
bidity associated with SE: (1) certain etiologies, (2) age
>60 years, and (3) long duration of SE (Towne et al.,
1994; DeLorenzo et al., 1996; Wu et al., 2002; Rossetti
et al., 2006). This review focuses on the various causes of SE, since etiology is increasingly recognized as one of the
most important factors for prognosis and outcome. There-
fore, identifying and treating the underlying cause of SE is
at least as important as prompt and effective treatment
with early termination of seizures.
Definition andClassification
of Status Epilepticus
Status epilepticus (SE) has been recognized for centu-
ries (Shorvon, 1994; Wolf et al., 2009). Henri Gastaut
(1970) recognized SE as a prolonged seizure with as manyforms as there were types of epileptic seizures. Therefore,
SE classification mirrored exactly the seizure classifica-
tion. In the International League against Epilepsy (ILAE)
1981 Classification, SE was defined as ‘‘a seizure that per-
sists for a sufficient length of time, or repeated frequently
enough that recovery between attacks do [does] not
occur’’ (Commission on Classification, ILAE, 1981).
Generalized tonic–clonic seizures usually do not last
longer than 2–3 min (Theodore et al., 1994); the risk of a
seizure becoming self-sustaining increases as the duration
reaches 5 min or more (Lowenstein et al., 1999). For the
purpose of this review, we use a clinical classification
Address correspondence to Eugen Trinka, Department of Neurology,Christian Doppler Klinik, Paracelsus Medical University, Ignaz HarrerStraße 79, 5020 Salzburg, Austria. E-mail: [email protected]
Wiley Periodicals, Inc.ª 2012 International League Against Epilepsy
Epilepsia, 53(Suppl. 4):127–138, 2012
doi: 10.1111/j.1528-1167.2012.03622.x
SEIZURES IN SPECIAL AND SEVERE SITUATIONS
127

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 2/12
along two taxonomic criteria: the presence (or absence) of
motor symptoms and the impairment (or retention) of con-
sciousness. Therefore, one can distinguish (A) SE types
with prominent motor symptoms, such as convulsive SE,
and (B) SE types without prominent motor symptoms,
summarized as nonconvulsive SE (NCSE). NCSE canoccur with or without coma; this has important etiologic
implications and determines its treatment. A third cate-
gory (C) comprises the boundary syndromes, including
epileptic encephalopathies and acute forms of coma with
status-like electroencephalography (EEG) patterns.
Table 1 briefly outlines this tentative classification. For a
more detailed discussion of SE classification, refer to:
(Shorvon, 1994; Walker et al., 2005; Bauer & Trinka,
2006, 2009; Berg et al., 2010). However, the definitions
and classifications are in flux and an ILAE Task force is
currently developing a new draft classification of SE, fol-
lowing the concepts of the ILAE’s new classification pro-posal of seizures and syndromes (Berg et al., 2010).
Causes of Convulsive Status
Epilepticus in Adults
Most population-based studies have used a traditional
30-min duration of SE, and so the numbers given are the
lowest estimates. Using the 5-min definition, determining
the time from onset to starting emergency treatment, the
incidence in clinical practice is much higher than in the
epidemiologic studies. Convulsive SE comprises 37–70%
of all forms of status, and its annual incidence is up to 40
per 100,000 (Waterhouse, 2008). In adults with preexist-
ing epilepsy, the most common etiologies are low antiepi-
leptic drug (AED) levels (accounting for at least one
fourth of SE [Fig. 1]), remote symptomatic etiologies, and
stroke (DeLorenzo et al., 1995, 1996). This subgroup with
epilepsy and low AED levels has a good prognosis, with a
low mortality of 4.0–8.6% (Towne et al., 1994; DeLorenzo
et al., 1995). Overall, acute symptomatic causes are the
most common etiology, accounting for 48–63% of all SE
cases (Hesdorffer et al., 1998; Coeytaux et al., 2000;
Knake et al., 2001). Stroke is the leading cause among theacute symptomatic cases, accounting for 14–22% of SE in
adults (DeLorenzo et al., 1995; Knake et al., 2001). In
older adults, remote stroke is a major cause. Knake et al.
(2001) found that remote stroke caused 36% of SE in
patients older than 56 years. In the Richmond Virginia
Status Epilepticus Study, 41% of adults and 61% of the
elderly had acute or remote ischemic and hemorrhagic
strokes as cause of status (DeLorenzo et al., 1995).
In the context of epilepsy, SE may develop in those with
a previous diagnosis of epilepsy or de novo, as its initial
manifestation. Approximately 15% of patients with epi-
lepsy have had at least one episode of status during theirlifetime. Most often, the SE is due to the epilepsy itself,
triggered by medication nonadherence, resulting in sub-
therapeutic AED levels (Aminoff & Simon, 1980) or by
inappropriate drug treatment (Thomas et al., 2006a,b).
The clinical features of SE in these patients depend on the
underlying epilepsy syndrome. In the context of idiopathic
generalized epilepsy, status is most often nonconvulsive
(Shorvon & Walker, 2005); in the context of juvenile
myoclonic epilepsy it may be myoclonic (Thomas et al.,
2006a,b; Larch et al., 2009). Myoclonic status may also
develop in progressive myoclonic epilepsy, Lennox-
Gastaut syndrome, or epilepsy with myoclonic absences.
Table 1. Proposed classification of seizure
types according to their semiology, along two
taxonomic criteria: motor symptoms and
impairment of consciousness
With prominent motor symptoms
Convulsive SE (syn.: tonic–clonic SE)
Myoclonic SE (prominent epileptic myoclonic jerks)
Focal motor (including EPC )
Tonic SE
Hyperkinetic SE
Without prominent motor symptoms (i.e., NCSE)
NCSE with coma
NCSE without coma
Generalized
Focal
Boundary syndromes
Epileptic encephalopathy
Acute forms of coma with status-like EEG pattern
Epileptic behavioral disturbance and psychosis
Confusional states, or delirium with epileptiform EEG changes
Figure 1.
Etiology of status epilepticus in adults, with associatedmortality for each category. Based on data from
DeLorenzo et al., 1995. AED, antiepileptic drugs; CNS,central nervous system.Epilepsia ILAE
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
128
E. Trinka et al.

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 3/12
However, the precise incidence of convulsive status or
myoclonic status in these syndromes is not known.
Approximately 12% of patients who eventually develop
epilepsy have presented with SE as their first clinical man-
ifestation (Hauser, 1990; Hesdorffer et al., 1998). In these
patients, SE may be an intrinsic manifestation of disease,sometimes with recurrent episodes, or the epilepsy may be
the consequence of a prolonged SE, with neuronal death
and alteration of networks causing recurrent seizures after
the initial event. During a 10-year follow-up, epilepsy
developed in 42% of patients who had acute symptomatic
SE and in 14% of patients who had acute symptomatic
seizures (Hesdorffer et al., 1998). The development of
subsequent epilepsy is more likely if the status is refrac-
tory to treatment (Holtkamp et al., 2005), supporting the
hypothesis that SE contributes to epileptogenesis by
enhancing hyperexcitable networks.
Nonconvulsive Status
Epilepticus
NCSE may be defined as ‘‘an enduring epileptic condi-
tion with reduced or altered consciousness, behavioral and
vegetative abnormalities, or merely subjective symptoms
without major convulsive movements’’ (Drislane, 2000).
This umbrella term includes a wide spectrum of disorders,
ranging from benign conditions, such as absence status in
idiopathic generalized epilepsy, to severe life-threatening
conditions, such as subtle SE or coma with generalized
epileptiform discharges (coma-GEDs). Therefore, it is
important to subdivide this category according to thedegree of unresponsiveness or to the depth of coma
(Fig. 2). Consciousness, which notoriously resists defini-
tion, becomes a taxonomic criterion for subdividing
NCSE (Bauer & Trinka, 2009). Consciousness itself can
be categorized into quantitative and qualitative conscious-
ness. The quantitative element depends upon the patient’s
level of consciousness and arousability, which in turn
depends upon the integrity of the ponto-mesodiencephalic
reticular pathways and the thalamocortical projections.
Qualitative consciousness, on the other hand, depends
upon the content of consciousness, experience, emotions,
and sensations, known only to patients themselves. Itreflects the inner monologue and it is essential for any
meaningful interaction with the environment. Qualitative
consciousness is associated with awareness, enabling the
patient either to focus on and interact with the environ-
ment or to engage in an inner monologue. Table 2
describes the different types of NCSE.
The incidence of NCSE, based on epidemiologic stud-
ies, ranges from 40.0 to 66.9% (DeLorenzo et al., 1995;
Hesdorffer et al., 1998; Coeytaux et al., 2000; Knake
et al., 2001; Vignatelli et al., 2003). Like convulsive sta-
tus, NCSE may occur in acute central nervous system
(CNS) disorders or may be a part of certain electroclinical
syndromes. We do not know the precise incidence of
NCSE in the epilepsy population. In our own audit (1975
to 2003) at the University Hospital Innsbruck, 220 patients
with epilepsy (140 women, median age 45 years [range 2–
89]) had at least one episode of NCSE either during their
Figure 2.
Relationship between depth and coma (x-axis), prog-nosis (x-axis), degree of structural brain damage (red y-
axis), and epileptic brain dysfunction (blue y-axis) dueto status epilepticus. Clinical entities depicted in theupper part of the graph are arranged along the x-axiswithout distinct positions, in recognition that largeborder zones and overlaps between the conditionsmay exist. With permission from Bauer & Trinka, 2009.AS, absence status epilepticus; EPC, epilepsia partialiscontinua; GEDs, generalized epileptiform discharges;IGE, idiopathic generalized epilepsy; LEDs, lateralizedepileptiform discharges; NCSE, nonconvulsive statusepilepticus.Epilepsia ILAE
Table 2. Categories of NCSE, classified
according to the degree of disturbed
consciousness
NCSE with coma
NCSE withoutcoma
Generalized
Typical absence status
Atypical absence status
Myoclonic absence status
Focal
Aura continua
With vegetative symptoms
With sensory symptoms
With visual symptoms
With olfactory symptoms
With gustatory symptoms
With emotional symptoms
AphasicSE
SE with dyscognitive symptoms
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
129
Causes of Status Epilepticus

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 4/12
disease or at their initial presentation (Bauer G, Trinka E,
unpublished data). The cause of NCSE was remote symp-
tomatic in 47%, idiopathic in 45%, and remained
unknown (cryptogenic) in 48%. Forty-six percent had
focal SE, 21% had a generalized NCSE in the context of
idiopathic (or genetic) generalized epilepsies, and 22%
had atypical absence status in the context of Lennox-Gas-
taut syndrome. Table 3 details their different types of sta-
tus epilepticus.
Causes of Absence Status
Epilepticus
Absence status (AS) is best described as ‘‘a confusional
state of variable intensity, ranging from simple cognitive
slowing to catatonic stupor, lasting for hours to days or
weeks’’ (Andermann & Robb, 1972). The EEG shows
bilateral rhythmic, synchronous, and mostly symmetric
paroxysmal activity, which can be continuous or discon-
tinuous (Bauer & Trinka, 2010; Fig. 3). It is important to
recognize that AS is a heterogeneous condition, whichmay occur in patients with preexisting idiopathic general-
ized epilepsy (‘‘typical’’ AS) or during the course of
chronic symptomatic generalized epilepsy, such as Len-
nox-Gastaut syndrome (‘‘atypical’’ AS). Of interest, some
Table 3. Types of NCSE in 220 patients with
epilepsy and a history of NCSE (Bauer &
Trinka, data on file)
n %
Generalized (106 = 48.2%)
Typical absence SE 57 25.9
Atypical absence SE 49 22.3
Localized/lateralized (100 = 45.5%)
Focal simple (58 = 26.4%)
Aura continua 11 5.0
Vegetative 8 3.6
Aphasic 27 12.3
Pure frontal 9 4.1
Psychosis 3 1.4
Focal complex (42 = 19.1%)
Continuous 30 13.7
Discontinuous 12 5.5
Unclassified 14 6.3
Total 220 100.1
Figure 3.
Typical absence status epilepticus in an older patient (V.J., female, 74 years. tc 0.3 F30). This patient had scatteredgeneralized tonic–clonic seizures since age of 54 years. Her EEG showed periodically repeated generalized 3/s spikeand wave, with no major diffuse slow activity between periods (note the reduced time calibration). EEG kindlyprovided by Prof. Dr. G. Bauer, Innsbruck. The patient displayed discontinuous psychic functions, and was amnesicfor the abnormal condition. Recovery was immediate after intravenous diazepam.Epilepsia ILAE
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
130
E. Trinka et al.

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 5/12
patients develop AS later in life, occasionally de novo
(Andermann & Robb, 1972; Thomas et al., 1992), or it
may occur as a late exacerbation of an idiopathic general-
ized epilepsy syndrome (Bauer et al., 2007). There may
also be a fourth group of AS, comprising ‘‘absences’’ with
very clear focal characteristics. This group may be consid-ered as a transitional form between AS and dyscognitive
focal SE of frontal origin (Bauer et al., 2006; Thomas,
2011).
Many cases of AS have nonspecific precipitating fac-
tors. The most important are antiepileptic drug (AED)
withdrawal or impaired adherence, alcohol, sleep depriva-
tion, and sleep–wake cycle disturbance. Other nonspecific
factors include stress, fatigue, fever, mild head trauma, or
metabolic derangement after surgery (Thomas & Zifkin,
2008; Thomas & Gelisse, 2009).
Several idiopathic generalized epilepsy syndromes may
be aggravated by inappropriate AEDs: carbamazepine,phenytoin, tiagabine, or other c-aminobutyric acid
(GABA)ergic medications (Snead & Hosey, 1985; Knake
et al., 1999; Thomas et al., 2006a,b; Trinka et al., 2002).
Thomas et al. reported 14 patients with idiopathic general-
ized epilepsy treated with either carbamazepine alone or
with other potentially aggravating drugs, for example,
phenytoin, vigabatrin, or gabapentin. Ten of these cases
developed AS; in half, the AS was atypical. All their
patients had a clear seizure aggravation, with development
of new seizure types before AS developed (Thomas et al.,
2006a,b). The prognosis was invariably good with full sei-
zure control in all patients after switching to appropriate
drugs.In late-onset AS, other drug-related factors play an
important clinical role (Thomas et al., 1992; Thomas &
Andermann, 1994). Most importantly, psychotropic medi-
cation — or its withdrawal — may provoke late-onset AS
(Fernandez-Torre, 2001). In addition, many other drugs,
for example, theophylline, baclofen, metformin, and
cimetidine, may exacerbate absences later in life (for a
review see Thomas & Snead, 2007).
There are metabolic and toxic factors in many patients,
although the precise incidence is not known. Examples
include hyponatremia, hypoglycemia decompensated
chronic renal failure, hepatic failure, and hypocalcemia(for review see Thomas & Snead, 2007). There have been
several cases of AS following the use of contrast-enhanc-
ing products during myelography or carotid angiography
(Pritchard & O’Neil, 1984; Vollmer et al., 1985; Coeytaux
et al., 2000). Some cases of transient global amnesia after
angiography may in fact also be epileptic in nature (Bauer
et al., 2005).
AS probably occurs most frequently in the context of
electroclinical syndromes. Aside from childhood
absence epilepsy, juvenile absence epilepsy, and juve-
nile myoclonic epilepsy, there are other syndromes asso-
ciated with AS as a key clinical feature: AS may occur
in eyelid myoclonia with absences (Jeavons syndrome)
(Yang et al., 2008), idiopathic generalized epilepsy with
phantom absences (Panayiotopoulos et al., 2001), per-
ioral myoclonias with absences (Agathonikou et al., 1998),
or absences status epilepsy (Genton et al., 2008). The
prognosis in these syndromes (not yet fully accepted inthe ILAE classification) is generally good, and patients
respond well to appropriate AEDs — valproate in most
cases. However, this is not true of AS associated with
ring chromosome 20, where prolonged confusional
states are notoriously resistant to AEDs and there have
been lethal cases (Jacobs et al., 2008). The EEG shows
bilateral high-voltage slow waves, sometimes with inter-
mingled spikes and frontal accentuation. There is no
typical clinical picture, except for mild cognitive impair-
ment (Fig. 4).
Causes of FocalNonconvulsiveStatus Epilepticus
Focal NCSE (as with AS) encompasses a wide range of
clinical symptoms. Previously the term ‘‘complex focal or
complex partial’’ SE was used, which may be replaced in
future by ‘‘dyscognitive SE.’’ These forms usually have
structural abnormalities and clinical focal signs that must
be identified to guide appropriate drug treatment (Fig. 2).
Most of the published literature concerns patients with
temporal or extratemporal lobe epilepsy of remote symp-
tomatic cause, whose NCSE is either as the presenting
symptom or develops during the course of the disease
(Tomson et al., 1992, Kaplan et al., 1996; Scholtes et al.,
1996). As with AS, there are often nonspecific risk factors,
but more often status occurs in these patients without spe-
cific provoking factors. In a review of 70 patients with
focal NCSE of frontal origin, more than one fourth had no
history of epilepsy. Forty-five percent had a focal frontal
Figure 4.
Clinical course of convulsive status epilepticus.Epilepsia ILAE
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
131
Causes of Status Epilepticus
7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 6/12
lesion. The etiology was most often a brain tumor (benign
or malignant), or a posttraumatic or a postsurgical lesion
(Thomas & Zifkin, 2008).
Rare causes of focal NCSE include intravenous contrast
media, or drugs such as ciprofloxacin, lithium intoxica-
tion, theophylline, vigabatrin, tiagabine, or crack cocaine(Thomas et al., 2006b). Mesial temporal focal NCSE can
also be the presenting symptom of the increasingly recog-
nized nonparaneoplastic limbic encephalitis, related to
voltage-dependent potassium channels (VGKC/LGI1)
(Irani et al., 2010), NMDA receptors (Vincent & Bien,
2008), or antibodies against glutamic acid decarboxylase
(Malter et al., 2010). Some of them lead to a specific sei-
zure type (e.g., faciobrachial dystonic seizures associated
with anti-VGKC/LGI1 antibodies), preceding the onset of
the limbic encephalitis (Irani et al., 2011a,b). It is impor-
tant to note that paraneoplastic limbic encephalitis may
also present with focal NCSE (Dalmau et al., 2008), indi-cating the need for a comprehensive search and rigorous
treatment of any underlying primary neoplasm. We do not
yet know the full spectrum of this new group of immune-
mediated encephalopathies (Table 4).
The outcome for focal NCSE is less favorable than that
for AS. Long-lasting focal status, especially of temporal
lobe origin, may cause brain edema identifiable on mag-
netic resonance imaging (MRI) (Bauer et al., 2006). These
patients may also have severe and prolonged amnesia
(Engel et al., 1978; Treiman et al., 1981). However, many
patients presenting with focal NCSE have acute or remote
symptomatic epileptogenic lesions, making it difficult to
disentangle the dysfunction due to the epileptic activityfrom the effect of the structural lesion (Hilkens & De
Weerd, 1995; Kaplan, 1996; Trinka et al., 2002). How-
ever, focal NCSE occurring with an acute lesion most
likely contributes substantially to the associated neuro-
logic dysfunction (Hilkens & De Weerd, 1995; Bauer &
Trinka, 2010). Therefore, patients with focal NCSE need
prompt and vigorous treatment, tailored to the underlying
cause.
Causes of Comatose
Nonconvulsive Status
Epilepticus
Comatose forms of NCSE need further attention. It is
important from the clinical standpoint (1) to clarifywhether the coma is caused by the epileptic seizure or sta-
tus, or by the brain disorder itself, (2) to assess the contri-
bution of epileptic activity to the depth of coma, (3) to
consider whether treatment improves prognosis in these
patients or not, and (4) to implement an appropriate treat-
ment in these critically ill patients. Unlike in other forms
of NCSE, the cause of the comatose patient’s SE can
sometimes only be identified from the history, the tempo-
ral pattern of coma, and the neurologic signs. The epileptic
etiology is most often confirmed only by the presence of
continuous or discontinuous epileptiform discharges on
the EEG (Lowenstein & Aminoff, 1992; Jordan, 1999;Brenner, 2005). A frequently used, but not universally
accepted, classification of patients in comatose status uses
the dichotomy of generalized versus focal or lateralized
EEG discharges (Brenner, 2004). The EEG is absolutely
necessary to make this distinction. In this review we used
the terms ‘‘coma with generalized epileptiform dis-
charges’’ (or coma-GED) and ‘‘coma with lateralized epi-
leptiform discharges’’ (or coma-LED) (Bauer & Trinka,
2009). The etiology in these patients is almost always
acute symptomatic, encompassing a wide variety of
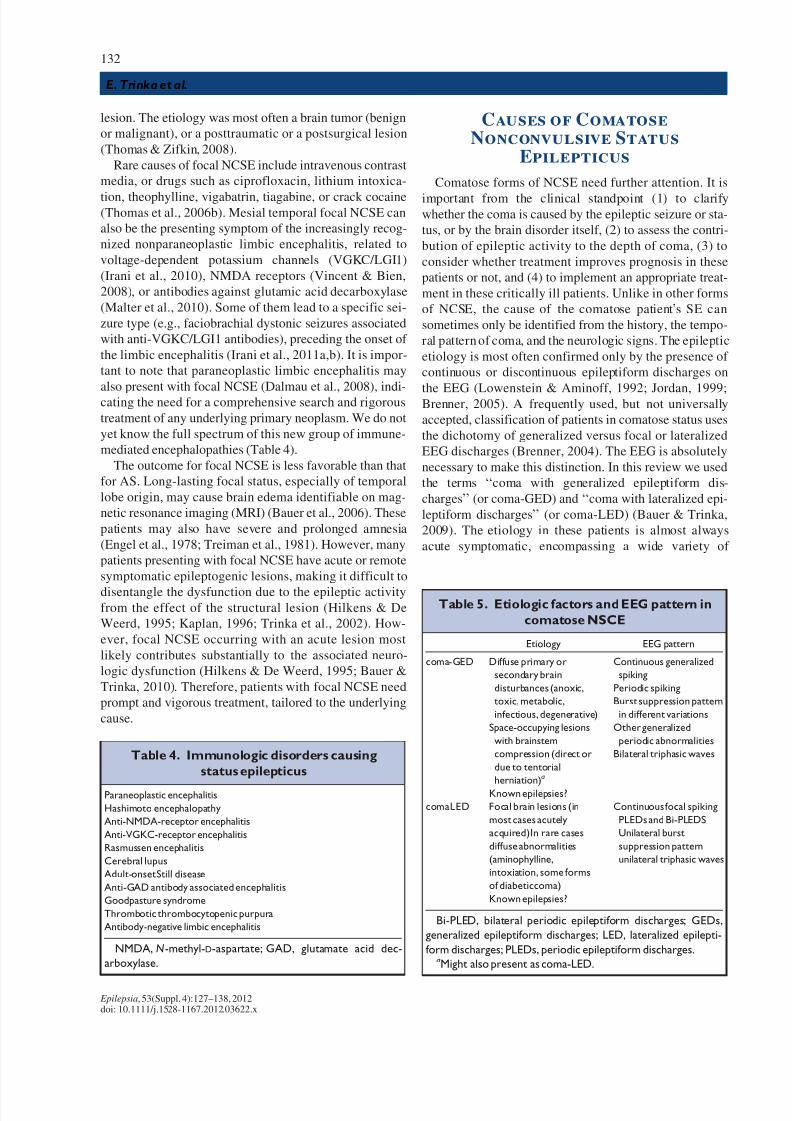
Table 5. Etiologic factors and EEG pattern in
comatose NSCE
Etiology EEG pattern
coma-GED Diffuse primary or
secondary brain
disturbances (anoxic,
toxic, metabolic,
infectious, degenerative)
Space-occupying lesions
with brainstem
compression (direct or
due to tentorial
herniation)
a
Known epilepsies?
Continuous generalized
spiking
Periodic spiking
Burst suppression pattern
in different variations
Other generalized
periodic abnormalities
Bilateral triphasic waves
comaLED Focal brain lesions (in
most cases acutely
acquired)In rare cases
diffuse abnormalities
(aminophylline,
intoxiation, some forms
of diabeticcoma)
Known epilepsies?
Continuous focal spiking
PLEDs and Bi-PLEDS
Unilateral burst
suppression pattern
unilateral triphasic waves
Bi-PLED, bilateral periodic epileptiform discharges; GEDs,
generalized epileptiform discharges; LED, lateralized epilepti-
form discharges; PLEDs, periodic epileptiform discharges.aMight also present as coma-LED.
Table 4. Immunologic disorders causing
status epilepticus
Paraneoplastic encephalitis
Hashimoto encephalopathy
Anti-NMDA-receptor encephalitis
Anti-VGKC-receptor encephalitis
Rasmussen encephalitis
Cerebral lupus
Adult-onset Still disease
Anti-GAD antibody associated encephalitis
Goodpasture syndrome
Thrombotic thrombocytopenic purpura
Antibody-negative limbic encephalitis
NMDA, N-methyl-D-aspartate; GAD, glutamate acid dec-
arboxylase.
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
132
E. Trinka et al.

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 7/12
Table 6. Causes of epilepsia partialis continua (according to Tan et al., 2010)
Age period EPC type1 (staticcause) Diagnostictest
EPC type 2 (progressive
cause) Diagnostic test
Infancy Hemimegalencephaly Mitochondrial disease
(Alper disease)
Serum and cerebrospinal
fluid lactate, musclebiopsy biopsy,
mitochondrial DNA
(mutation of POLG1)
Childhood Focal corticaldysplasia
Sturge-Weber
syndrome focal cortical
dysplasia
Rasmussen s yndrome Cerebrospinal fl uid
oligoclonal banding,
immunoglobulin G index
Tuberoussclerosis Repeated ski n
examination
Mitochondrial
encephalomyopathy, lactic
acidosis and stroke-like episodes
(MELAS)
Serum and cerebrospinal
fluid lactate, muscle
biopsy, mitochondrial
DNA
Neurocysticerosis Immunoelectrotransfer
blotassay
Delayed type of measles
encephalitis (complication of
measlesin
immunocompromised children)
Immunosuppresive
treatment, contact with
measles
(Tick-borne) encephalitis Cerebrospinal fluid study
serologic test for virus
Gliomatosis cerebri
Other foreign tissue
lesions Nonketotic
(ketotic) hyperglycemia
Serum glucose, urinary
ketones
Adults Cerebrovascular
disorders (stroke;
intracranial bleeding,
cerebral venous
thrombosis, vasculitis)
Adult-onset Rasmussen’s
syndrome
Cerebrospinal fluid
oligoclonal banding,
immunoglobulin G index
Nonketotic (ketotic)
hyperglycemia
Serum glucose Creutzfeldt-Jakob disease 14-3-3 protein in
cerebrospinal fiuid
Focal cortical dysplasia Myoclonus epilepsy with ragged
redfibers (MERRFs)
Serum and cerebrospinal
fluid lactate, musclebiopsy, mitochondrial
DNA
Paraneoplastic limbic
encephalopathy
Cerebrospinal fluid study,
chest computed
tomography, anti-Hu
test
Kuf’s disease Skin or rectal mucosal
biopsy
Neoplasms
Tuberculous meningitis
(tuberculoma)
(Tick-borne) encephalitis
Cerebrospinal fluid study,
chest XR, tuberculin skintest
Cerebrospinal fluid
study,serologictest for
virus
Autoimmune thyroid
encephalopathy
Thyroid function tests,
antithyroglobulin
antibody,antimicrosomal antibody
Behcet di sease Neuroimaging, recurrent
oral and genital
ulceration, skin lesions,
HLA-B5 positivity
Sjogrensyndrome Hypergammaglobulinemia
positive antinuclear
antibody, anti-SSA, SSB,
rheumatoid factor
Multiplesclerosis Cerebrospinal fluid
oligoclonal banding
HIV encephalopathy
Immunoglobulin G index
Serologic test for HIV
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
133
Causes of Status Epilepticus

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 8/12
systemic diseases or CNS disorders. Table 5 shows the eti-
ologic factors and EEG patterns found in coma-GED and
coma-LED. Unlike in AS and focal NCSE, these patients
are often resistant to treatment, and the prognosis depends
entirely on the course of the underlying disorder.
Advanced convulsive SE becomes oligosymptomatic withfewer motor symptoms; deep coma is the leading symp-
tom, hence the term ‘‘subtle status’’ (Treiman et al., 1984).
The causes are identical to convulsive SE.
Causes of Epilepsia Partialis
Continua
Epilepsia partialis continua (EPC) is a special type of
focal status epilepticus (Table 1), first described by
Kojewnikov in 1894; he considered it as a ‘‘peculiar form
of cortical epilepsy.’’ EPC is characterized by ‘‘spontane-
ous regular or irregular clonic muscle twitching of cere-bral cortical origin, sometime aggravated by action or
sensory stimuli, confined to one part of the body, and
continuing for a period hours days, or weeks’’ (Obeso
et al., 1985). EPC, also called Kojewnikov syndrome,
occurred in patients with Russian spring–summer tick-
borne encephalitis; EPC typically develops 2–3 weeks
after the end of the acute illness (Zemskaya et al., 1991).
EPC was later recognized to occur in several neurologic
disorders, with age of onset ranging from infancy to adult-
hood, and even in the elderly. The prevalence, based on
the EPC case registry of the British Neurological Surveil-
lance Unit, is <1 per million (Cockerell et al., 1996).
The reported causes of EPC are extremely diverse, and
include metabolic disorders (nonketotic hyperglycemia ormitochondrial encephalopathy), cerebrovascular disor-
ders, inflammation (especially Creutzfeldt–Jakob disease,
progressive multifocal leukoencephalopathy from HIV
infection, multiple sclerosis, neurocysticercosis and oth-
ers), neoplasms (astrocytoma, hemangioma, lymphoma
and metastasis), and cortical dysplasia (focal cortical
dysplasia and hemimegalencephaly) (Oguni et al., 1991;
Veggiotti et al., 1995; Lee et al., 2000; Placidi et al., 2001;
Pandian et al., 2002; Huang et al., 2005; Wieser & Chauvel,
2005; Aydin-Ozdemir et al., 2006; Kinirons et al., 2006;
Sinha & Satischandra, 2007; Bien & Elger, 2008; Yeh &
Wu, 2008; Mameniskiene et al., 2011). The most commonetiologies are cerebrovascular disorders (24–28%), inflam-
matory causes (15–19%), neoplasms (5–16%), and meta-
bolic disorders (6–14%). Despite full neurologic work-up,
19–28% of EPC cases have no identifiable cause (Thomas
et al., 1977; Cockerell et al., 1996; Sinha & Satischandra,
2007). Table 6 gives an overview of the causes of EPC.
Bancaud divided EPC into two types: type 1, caused by
focal static lesions of the sensorimotor cortex, and type 2,
caused by progressive cerebral lesions with neurologic
and intellectual deterioration (Bancaud, 1992). Type 2
most often reflects mitochondrial diseases and inflamma-
tory causes, such as Rasmussen syndrome or Creutzfeldt–
Jakob disease.
UncommonCauses of Status
Epilepticus
The uncommon causes of SE deserve consideration. In
many cases of drug-resistant SE, the underlying disorder
remains untreated, because rare causes may be over-
looked. We do not know the frequency of these rare
Table 8. Uncommon infectious disease causing status epilepticus
Atypical bacterial infections Viral infections Prion disease Other infections
Bartonella/cat-scratch disease HIV and HIV-related infections Creutzfeldt-Jakob disease Paracoccidioidomycosis
Coxiella burnett (Q fever) West Nile encephalitis Paragonimiasis
Neurosyphilis JC virus ( progressive multifocal
leukoencephalopathy)
Mucormycosis
Scrub typhus Parvovirus B19
Shigellosis Varicella encephalitis
Mycoplasmapneumonia Subacutesclerosing panencephalitis
Chl amydophilapsittaci Measles encephalitis
Rubella encephalitis
Rous sarcoma virus
(RSV) associated SE
Polioencephalomyelitis
St. Louis encephalitis
Table 7. Mitochondrial diseases causing
status epilepticus
Alpers disease
Occipital lobe epilepsy/mitochondrial spinocerebellar ataxia and
epilepsy (MSCAE)
Mitochondrial encephalopathy, lacticacidosis, and stroke-like episodes
(MELAS)
Leigh syndrome
Myoclonic encephalopathy with ragged red fibers (MERRF)
Neuropathy, ataxia, and retinitis pigmentosa (NARP)
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
134
E. Trinka et al.

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 9/12
causes, and the available literature is mostly confined to
single case reports or small case series. This overview is
based on a systematic search of all available English liter-
ature between 1990 and 2008 (Tan et al., 2010). The
authors identified 181 causes of SE after reviewing 513
articles. The causes fell into five categorical groups:
1. Immunologically mediated disorders (Table 4).2. Mitochondrial diseases (Table 7).
3. Uncommon infective disorders (Table 8).
4. Genetic disorders (Table 9).
5. Drugs or toxins.
Table 10 lists other uncommon causes of SE. It cannot
be overemphasized that the knowledge of the range of
conditions is important to clinical practice; the underlying
disorder must be treated to achieve full seizure control.
The tables are derived from the article by Tan et al. (2010)
and reflect the current state of knowledge on these causes
of SE.
TherapeuticConsiderations
Given the wide variety of clinical presentations of SE,
ranging from life-threatening conditions to seemingly
harmless ones, it is important to tailor the treatment to the
type of status and to the underlying disorder. The clinical
presentation of SE determines the aggressiveness treat-
ment. All treatment concepts on convulsive SE are based
on a staged approach (Fig. 4). In the early phase of convul-
sive SE, large randomized controlled trials support the use
of intravenous benzodiazepines. Alternatively, the intra-
muscular route is effective in the prehospital setting
(Silbergleit et al., 2012). In stage two, AEDs were used,
but it must be emphasized that there are no clinical trials
to inform the best drug treatment at this stage (Cock and
ESETT Group, 2011). Phenytoin, levetiracetam, and valp-
roic acid are most often used (Shorvon et al,. 2008). The
newer AED lacosamide has also gained acceptance in the
community, but data on its effectiveness in convulsive
Table 9. Status epilepticus due to genetic diseases
Chromosomal aberrations
Inborn errors of
metabolism
Malformations of
cortical development
Neurocutaneous
syndromes Others
Ring chromosome 20 Porphyria Focal cortical
dysplasias
Sturge-Weber
syndrome
Rett’s syndrome
Angelmansyndrome Menke’s disease Hemimegalencephaly Tuberous sclerosis Dravet syndrome and
SCN1A gene mutation
spectrum
Wolf-Hirschhorn s yndrome Wilson’s disease Polymicrogyria Migrating partial seizures
in infancy
Fragile X syndrome Alexander’s disease Heterotopias Pyeridoxine dependency
X-linked mentalretardation
syndrome
Gobalamin C/D
deficiency
Schizencephaly Familial hemiplegic
migraine
Ringchromosome 17 Ornithine transcarbamylase
(OTC) deficiency
Hyperprolinemia
Maple-syrup urine disease
3-Methylcrotonyl CoA
carboxylase deficiency
Lysinuric protein intoleranceHydroxyglutaric aciduria
Metachromatic
leukodystrophy
Kuf’s disease
Late infantile ceroid
lipofuscinosis
Beta-ureidopropionase
deficiency
Lafora’s disease
Dentato-rubro-pallido-luysian
atrophy
Infantile-onset
spinocerebellar ataxia
Wrinkly-skin syndrome
Neurocutaneousmelanomatosis
Neuroserpin mutation
Wolfram syndrome
Autosomal recessive
hyperekplexia
Cockayne syndrome
Cerebral autosomal
dominant arterio-pathy
with subcortical infarcts
and leuko
encephalopathy
(CADASIL)
3-Hydroxyaxyl
CoA dehydrogenase
deficiencyCarnitine
palmitoyltransferase
Succinic semildehyde
dehydrogenase deficiency
Jeavons syndrome
Robinow syndromeLYK5 mutation
MECP2 mutation
Malignant hyperpyrexia
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
135
Causes of Status Epilepticus

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 10/12
status are limited (Hçfler et al., 2011; Trinka, 2011). From
stage three onward, intensive care unit treatment and gen-
eral anesthesia are the mainstays of drug treatment. Again,
there are no randomized controlled trials informing the
effectiveness of individual drugs in this stage. Midazolam
seems to be better tolerated than pentobarbital/thiopental
and propofol (Shorvon & Ferlisi, 2012). A fourth stage of
status was recently introduced (Shorvon & Trinka, 2011),
and a treatment protocol was proposed by Shorvon and
Ferlisi (2011). Needless to say, all general measures for
intensive care treatment have to be applied at the begin-
ning of status (Shorvon et al., 2008). There is general
agreement that AS, dyscognitive status and other forms of
focal nonconvulsive SE do not require the same aggres-
sive treatment as convulsive SE. Most patients in AS
respond promptly to a benzodiazepine or valproic acid. In
focal NCSE the potential risks of treatment, especially
intubation and sedation, must be weighed against the ben-
efits of seizure control in preventing neuronal damage and
long-term consequences.
Disclosure of Conflict
of Interest
AZ has no conflict of interest to declare. JH has received speaker’shonoraria from UCB and travel grants from UCB, Eisai, and Gerot. EThas acted as a paid consultant to Eisai, Medtronics, Bial, and UCB. Hehasreceived research fundingfrom UCB, Biogen-Idec, and Sanofi-Aven-tis, and speakers’ honoraria from Bial, Cyberonics, Desitin Pharma, Eisai,Gerot, Bçhringer, Sanofi, Medis, and UCB. We confirm that we haveread the Journal’s position on issues involved in ethical publication andaffirm that this report is consistent with those guidelines.
References
Agathonikou A, Panayiotopoulos CP, Giannakodimos S, Koutroumani-dis M. (1998) Typical absence status in adults: diagnostic and syndro-mic considerations. Epilepsia 39:1265–1276.
Aminoff MJ, Simon RP. (1980) Status epilepticus causes, clinical fea-tures and consequences in 98 patients. Am J Med 69:657–666.
Andermann F, Robb JP. (1972) Absence status: a reappraisal followingreview of thirty-eight patients. Epilepsia 13:177–187.
Aydin-Ozdemir Z, Tüzün E, Baykan B. (2006) Autoimmune thyroidencephalopathy presenting with epilepsia partialis continua. ClinEEG Neurosci 37:204–209.
Bancaud J. (1992) Kojewnikov’s syndrome (epilepsia partialis continua)in children. In Roger J, Dravet C, Bureau M, Dreifuss FE, Wolf P(Eds) Epileptic syndromes in infancy, childhood and adolescence.2nd edn.John Libbey Eurotext, London, pp. 363–379.
Bauer G, Trinka E. (2006) Seizures, syndromes and classifications.
Epileptic Disord 8:162–163.
Table 10. Other causes of status epilepticus
Iatrogenic Other medical conditions
Electroconvulsive therapy
Temporal lobectomy and
other neurosurgeryInsertion of intracranialelectrode
Ventriculoperitoneal shunt
Blood transfusion
Carotid angioplasty and stenting
Multiple sclerosis
Hypertension-induced posterior
reversible encephalopathysyndrome
Panayiotopoulos syndrome
Thyroid disease
Pyridoxine-dependent seizure
Neuroleptic malignant syndrome
Ulcerative colitis
Behcet syndrome
Celiac disease
Cobalamin deficiency
Folinicacid responsive seizures
Renal arterystenosis
Pituitary apoplexy
Renal arterydissection
Hypomelanosis of Ito
Cerebral palsyHemophagocytic
lymphohistiocytosis
Anhidrotic ectodermal dysplasia
Methemoglobinemia
Figure 5.
Staged approach to the treatment of convulsive statusepilepticus. *There is currently limited evidence for theuse of lacosamide in SE (see Hofler et al., 2011) Modi-fied after Trinka, 2007; Shorvon et al., 2008.
Epilepsia ILAE
Figure 6.
Treatment algorithm for superrefractory statusepilepticus. Modified after Shorvon & Ferlisi, 2011.Epilepsia ILAE
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
136
E. Trinka et al.

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 11/12
Bauer G, Trinka E. (2010) Nonconvulsive status epilepticus and coma.
Epilepsia 51:177–190.Bauer G, Benke T, Unterberger I, Schmutzhard E, Trinka E. (2005) Tran-
sient global amnesia or transient epileptic amnesia? QJM 98:383;author reply 383–384.
Bauer G, Dobesberger J, Bauer R, Embacher N, Benke T, Unterberger I,Walser G, Luef G, Trinka E. (2006) Prefrontal disturbances as the
sole manifestation of simple partial nonconvulsive status epilepticus.Epilepsy Behav 8:22–225.
Bauer G, Bauer R, Dobesberger J, Benke T, Walser G, Trinka E. (2007)Absence status in the elderly as a late complication of idiopathic gen-eralized epilepsies. Epileptic Disord 9:39–42.
Berg AT, Berkovic SF, Brodie MJ, Buchhalter J, Cross JH, van EmdeBoas W, Engel J, French J, Glauser TA, Mathern GW, MoshØ SL,Nordli D, Plouin P, Scheffer IE. (2010) Revised terminology andconcepts for organization of seizures and epilepsies: report of theILAE Commission on Classification and Terminology, 2005–2009.Epilepsia 51:676–685.
Bien CG, Elger CE. (2008) Epilepsia partialis continua: semiology anddifferential diagnoses. Epilept Disord 10:3–7.
BrennerRP. (2004) EEGin convulsiveand nonconvulsive status epilepti-cus. J Clin Neurophysiol 21:319–331.
Brenner RP. (2005) The interpretation of the EEG in stupor and coma.
Neurologist 11:271–284.Cock HR, ESETT Group. (2011) Established status epilepticus treatmenttrial (ESETT). Epilepsia 52(Suppl. 8):50–52.
Cockerell OC, Rothwell J, Thompson PD, Marsden CD, Shorvon SD.(1996) Clinical and physiological features of epilepsia partial con-tinua: cases ascertained in the UK. Brain 119:393–407.
Coeytaux A, Reverdin A, Jallon P, Nahory A. (1999) Non-convulsivesta-tus epilepticus following intrathecal fluorescein injection. Acta Neu-rol Scand 100:278–280.
Coeytaux A, Jallon P, Galobardes B, Morabia A. (2000) Incidence of status epilepticus in French-speaking Switzerland: EPISTAR.
Neurology 55:693–697.Commission on Classification and Terminology of the International
League Against Epilepsy. (1981) Proposal for revised clinicaland electroencephalographic classification of epileptic seizures.Epilepsia 22:489–501.
Dalmau J, Gleichman AJ, Hughes EG. (2008) Anti-NMDA-receptor
encephalitis: case series and analysis of the effects of antibodies. Lancet Neurol 7:1091–1098.
DeLorenzo RJ, Pellock JM, Towne AR, Boggs JG. (1995) Epidemiologyof status epilepticus. J Clin Neurophysiol 12:316–325.
DeLorenzo RJ, Hauser WA, Towne AR. (1996) A prospective, popula-tion-based epidemiologic study of status epilepticus in Richmond,Virginia. Neurology 46:1029–1035.
Drislane FW. (2000) Presentation, evaluation, and treatment of noncon-vulsivestatus epilepticus. Epilepsy Behav 1:301–314.
Engel J, Ludwig B, Fetell M. (1978) Prolonged partial complex statusepilepticus: EEG and behavioral observations. Neurology 28:863–869.
Fernandez-Torre JL. (2001) De novo absence status of late onset follow-ing withdrawal of lorazepam: a case report. Seizure 10:433–437.
Gastaut H. (1970) Clinical and electroencephalographic classification of epileptic seizures. Epilepsia 11:102–113.
Genton P, Ferlazzo E, Thomas P. (2008) Absence status epilepsy: delin-eation of an adult idopathic generalized epilepsy syndrome. Epilepsia49:642–649.
Hauser WA. (1990) Status epilepticus: epidemiology considerations. Neurology 40(Suppl. 2):9–12.
Hesdorffer DC, Logroscino G, Cascino G, Annegers JF, Hauser WA.(1998) Incidence of status epilepticus in Rochester, Minnesota,1965–1984. Neurology 50:735–741.
Hilkens PHE, De Weerd AW. (1995) Non-convulsive status epilepticusas cause for focal neurological deficit. Acta Neurol Scand 92:193–197.
Hçfler J, Unterberger I, Dobesberger J, Kuchukhidze G, Walser G,Trinka E. (2011) Intravenous lacosamide in status epilepticus and sei-zure clusters. Epilepsia 52:e148–e152.
Holtkamp M, Othman J, Buchheim K, Meierkord H. (2005) Predictorsand prognosis of refractory status epilepticus treated in a neurologicalintensive care unit. J Neurol Neurosurg Psychiatry 76:534–539.
Huang CW, Hsieh YY, Pai MC, Tsai JJ, Huang CC. (2005) Nonketotichyperglycemia-related epilepsia partialis continua with ictal unilat-eral parietal hyperperfusion. Epilepsia 46:1843–1844.
Irani SR, Alexander S, Waters P, Kleopa KA, Pettingill P, Zuliani L,Peles E, Buckley C, Lang B, Vincent A. (2010) Antibodies to Kv1potassium channel-complex proteins leucine-rich, glioma inactivated1 protein and contactin-associated protein-2 in limbic encephalitis,
Morvan’s syndrome and acquired neuromyotonia. Brain 133:2734–2748.
Irani SR, Michell AW, Lang B, Pettingill P, Waters P, Johnson MR,Schott JM, Armstrong RJ, S Zagami A, Bleasel A, Somerville ER,Smith SM, Vincent A. (2011a) Faciobrachial dystonic seizuresprecede Lgi1 antibody limbic encephalitis. Ann Neurol 69:892–900.
Irani SR,SchottJM, Vincent A, Smith SJ.(2011b) Tonic seizures: a diag-nostic clue of anti-LGI1 encephalitis? Neurology 77:2140–2141;author reply 2141-3.
Jacobs J, Bernard G, Andermann E, Dubeau F, Andermann F. (2008)Refractory and lethal status epilepticus in a patient with ring chromo-some 20 syndrome. Epileptic Disord 10:254–259.
Jordan KG.(1999)Nonconvulsive status epilepticus in acute brain injury. J Clin Neurophysiol 16:332–340.
Kaplan PW. (1996) Nonconvulsive status epilepticus in the emergencyroom. Epilepsia 37:643–650.
Kinirons P, O’Dwyer JP,Connolly S, HutchinsonM. (2006) Paraneoplas-tic limbic encephalitis presenting as lingual epilepsia partialis con-
tinua. J Neurol 253:256–257.
Knake S, Hamer HM, Schomburg U, Oertel WH, Rosenow F. (1999)Tiagabine-induced absence status in idiopathic generalized epilepsy.
Seizure 8:314–317.Knake S, Rosenow F, Vescovi M, Oertel WH, Mueller HH, Wirbatz A,
Katsarou N, Hamer HM, Status Epilepticus Study Group Hessen(SESGH). (2001) Incidence of status epilepticus in adults in Ger-many: a prospective, population-based study. Epilepsia 40:759–762.
Larch J, Unterberger I, Bauer G, Reichsoellner J, Kuchukhidze G, TrinkaE. (2009) Myoclonic status epilepticus in juvenile myoclonicepilepsy. Epileptic Disord 11:309–314.
Lee K, Haight E, Olejniczak P. (2000) Epilepsia partialis continua inCreuzfeldt-Jacob disease. Acta Neurol Scand 102:398–402.
Logroscino G, Hesdorffer DC, Cascino G, Annegers JF, Hauser WA.
(1997) Short-term mortality after a first episode of status epilepticus.
Epilepsia 38:1344–1349.Logroscino G, Hesdorffer DC, Cascino G, Hauser WA, Coeytaux A,
Galobardes B, Morabia A, Jallon P. (2005) Mortality after a first epi-sode of status epilepticus in the United States and Europe. Epilepsia46(Suppl. 11):46–48.
Lowenstein DH, Aminoff MJ. (1992) Clinical, EEG features of statusepilepticus in comatose patients. Neurology 42:100–104.
Lowenstein DH, Bleck T, Macdonald RL. (1999) It’s time to revisetorevise the definitionof status epilepticus. Epilepsia 40:120–122.
Malter MP, Helmstaedter C, Urbach H, Vincent A, Bien CG. (2010)Antibodies to glutamic acid decarboxylase define a form of limbicencephalitis. Ann Neurol 67:470–478.
Mameniskiene R, Bast T, Bentes C, Canevini MP, Dimova P, Granata T,Høgenhaven H, Jakubi BJ, Marusic P, Melikyan G, Michelucci R,Mukhin KY, Oehl B, Ragona F, Rossetti AO, Rubboli G, Schubert S,Stephani U, Strobel J, Vignoli A, Zarubova J, Wolf P. (2011) Clinical
course and variability of non-Rasmussen, nonstroke motor and sen-sory epilepsia partialis continua: a European survey and analysis of 65 cases. Epilepsia 52:1168–1176.
Obeso JA, Rothwell JC, Marsden CD. (1985) The spectrum of corticalmyclonus: from focal reflex jerks to spontaneous motor epilepsy.
Brain 108:193–224.Oguni H, Andermann F, Rasmussen T. (1991) The natural history of the
syndrome of chronic encephalitis and epilepsy: a study of the MNIseries of forty-eight cases. In Andermann F (Ed.) Chronic encephali-tis and epilepsy: Rasmussens's syndrome. Butterworth-Heinermann,Boston,MA, pp. 7–35.
Panayiotopoulos CP, Ferrie CD, Koutroumanidis M, Rowlinson S, Sand-ers S. (2001) Idiopathic generalized epilepsy with phantom absencesand absencestatusin a child. Epileptic Disord 3:63–66.
Pandian JD, Thomas SV, Santoshkumar B. (2002) Epilepsia partialis
continua: a clinical and electroencephalography study. Seizure11:437–441.
Epilepsia, 53(Suppl. 4):127–138, 2012doi: 10.1111/j.1528-1167.2012.03622.x
137
Causes of Status Epilepticus

7/27/2019 j.1528-1167.2012.03622.x
http://slidepdf.com/reader/full/j1528-1167201203622x 12/12
Placidi F, Floris R, Bozzao A. (2001) Ketotic hyperglycemia and epilep-sia partialis continua. Neurology 57:534–537.
Pritchard PB III, O’Neal DB. (1984) Nonconvulsive status epilepticusfollowing metrizamide myelography. Ann Neurol 16:252–254.
Rossetti AO, Hurwitz S, Logroscino G, Bromfield EB. (2006) Prognosis of status epilepticus: role of aetiology, age, and consciousness impaire-ment at presentation. J Neurol Neurosurg Psychiatry 77:611–615.
Scholtes FB, Renie WO, Meinardi HM. (1996) Non-convulsive statusepilepticus: causes, treatment, outcome in 65 patients. J Neurol
Neurosurg 61:93–95.Shorvon S. (1994) Status epilepticus: its clinical features and treatment
in children and adults. University Press, Cambridge.Shorvon S, Ferlisi M. (2011) The treatment of super-refractory status
epilepticus: a critical review of available therapies and a clinicaltreatment protocol. Brain 134(Pt 10):2802–2818.
Shorvon S, Ferlisi M. (2012) The outcome of therapies in refractory andsuper-refractory convulsive status epilepticus and recommendationsfor therapy. Brain May 9 [Epubahead of print].
Shorvon S, Trinka E. (2011) Status epilepticus – making progress.Epilepsia 52(Suppl. 8):1–2.
Shorvon S, Walker M. (2005) Status epilepticus in idiopathic generalizedepilepsy. Epilepsia 46(Suppl. 9):73–79.
Shorvon S, Baulac M, Cross H, Trinka E, Walker M. (2008) The drug
treatment of status epilepticus in Europe: censensus document from aworkshop at the first London Colloquium on Status Epilepticus.
Epilepsia 49:1277–1285.
Silbergleit R, Durkalski V, Lowenstein D, Conwit R, Pancioli A, PaleschY, Barsan W. (2012) Intramuscular versus intravenous therapy forprehospital status epilepticus. N EnglJ Med 366:591–600.
Sinha S, Satischandra P. (2007) Epilepsia partialis continua over last14 years: experience from a tertiary care center from south India.Epilepsy Res 74:55–59.
Snead OC, Hosey LC. (1985) Exacerbation of seizures in children bycarbamazepine. N EnglJ Med 313:916–921.
Tan R, Neligan A, Shorvon SD. (2010) Uncommon causes of statusepilepticus. Epilepsy Res 91:11–22.
Theodore WH, Porter RJ, Albert P. (1994) The secondarily generalizedtonic-clonic seizure: a videotape analysis. Neurology 44:1401–1407.
Thomas P. (2011) Causes of non-convulsive status epilepticus in adults.
In Shorvon S, Andermann F, Guerrini R (Eds) The causes of epilepsy.
Cambridge University Press,Cambridge, pp. 752–758.Thomas P, Andermann F. (1994) Late-onset absence status epilepticus is
most often situation-related. In Malafosse A, Genton P, Hirsch E,Marescaux C, Broglin D, Bernasconi R (Eds) Idiopahtic generalized epilepsies. John Libbey, London,pp. 95–109.
Thomas P, Gelisse P. (2009) Nonconvulsive status epilepticus. Rev Neurol (Paris). 165:380–389.
Thomas P, Snead OC III. (2007) Absence status epilepticus. In Engel J,Pedley T (Eds) Epilepsy: a comprehensive textbook , 2nd ed. Lippin-cott William and Wilkins, Philadelphia, pp. 693–703.
Thomas P, Zifkin B. (2008) Frontal lobe non convulsive status epilepti-cus. In Kaplan PWA, Dislane F (Eds) Non convulsive status epilepti-cus. Demos Biomedical, New York, pp. 91–101.
Thomas JE, Reagan TJ, Klass DW. (1977) Epilepsia partialis continua:a reviewof 32 cases. Arch Neurol 34:266–275.
Thomas P, Beaumanoir A, Genton P, Dolisi C, Chatel M. (1992) De novo
absence status:reportof 11 cases. Neurology 42:105–110.Thomas P, Valton L, Genton P. (2006a) Absence and myoclonic statusepilepticus precipitated by antiepileptic drugs in idiopathic general-ized epilepsy. Brain 129:1281–1292.
Thomas P, Zifkin B, Andermann F. (2006b) Complex partialstatus epilepticus. In Wasterlain CG, Treiman DM (Eds) Status epi-lepticus: mechanism and management . MIT Press, Cambridge, pp.69–90.
Tomson T, LindbomU, NilssonBY. (1992) Non-convulsve status epilep-ticus in adults: thirty-two consecutive patients from a general hospitalpopulation. Epilepsia 33:829–835.
Towne AR, Pellock JM, Ko D, DeLorenzo RJ. (1994) Determinants of mortality in status epilepticus. Epilepsia 35:27–34.
Treiman DM, Delgado-Escueta AV, Clark MA. (1981) Impairment of memory following complex partial status epilepticus. Neurology31:109.
Treiman DM, DeGiorgio CMA, Salisbury SM, Wickboldt CL.(1984) Subtle generalized convulsive status epilepticus. Epilepsia25:653.
Trinka E. (2007) Notfälle im Bereich der Epilepsien: was tun und waslassen? Nervenheilkunde 26:953–1072.
Trinka E. (2011) What is the evidence to use new intravenous AEDs instatus epilepticus? Epilepsia 52(Suppl. 8):35–38.
Trinka E, Dilitz E, Unterberger I. (2002) Non-convulsive status epilepti-cus after replacement of valproate with lamotrigine. J Neurol249:1417–1422.
Veggiotti P, Colamaria V, Dalla Bernardina B. (1995) Epilepsia partialis
continua in a case of MELAS: clinical and neurophysiological study. Neurophysiol Clin 25:158–166.Vignatelli L, Tonon C, D’Alessandro R. (2003) Incidence and short-term
prognosis of status epilepticus in adults in Bologna, Italy. Epilepsia44:964–968.
Vincent A, Bien CG. (2008) Anti-NMDA-receptor encephalitis: a causeof psychiatric, seizure, and movement disorders in young adults.
Lancet Neurol 7:1091–1098.Vollmer ME, Weiss H, Beanland C, Krumholz A. (1985) Prolonged con-
fusion due to absence status following metrizamide myelography. Arch Neurol 42:1005–1007.
Walker M, Cross H, Smith S. (2005) Nonconvulsive status epilepticus:Epilepsy Research Foundation workshop reports. Epilept Disord 7:253–296.
WaterhouseE. (2008) Theepidemiology of status epilepticus. In DrislaneR, Kaplan P (Eds) Nonconvulsive status epilepticus. Demos Medical
Publishing, New York, pp. 23–40.
Wieser HG, Chauvel P. (2005) Simple partial status epilepticus and epi-lepsia partialis continua of Koshevnikov. In Engel J Jr, Pedley TA(Eds) Epilepsy: a comprehensive textbook . Lippincott-Raven, Phila-delphia, PA,pp. 705–724.
Wolf NI,Rahman S, SchmittB. (2009) Status epilepticus in children withAlpers disease caused by POLG1 mutations: EEG and MRI features.Epilepsia 50:1596–1607.
Wu YW, Shek DW, Garcia PA, Zhao S, Johnston SC. (2002) Incidenceand mortality of generalized convulsive status epilepticus in Califor-nia. Neurology 58:1070–1076.
Yang T, Liu Y, Liu L. (2008) Absence status epilepticus in monozygotictwins Jeavons syndrome. Epileptic Disord 10:227–230.
Yeh SJ, Wu RM. (2008) Neurocysticerosis presenting with epilepsiapartialis continua: a clinicopathologic report and literature review.
J Formos Med Assoc 108:576–581.Zemskaya AG,YatsukSL, Samoilov VI.(1991) Intractable or partial epi-
lepsy of infectious or inflammatory etiology: recent-surgical experi-ence in the USSR. In Andermann F (Ed) Chronic encephaltis and
epilepsy: Rasmussens's syndrome. Butterworth-Heinemann, Boston,MA,pp. 271–279.
Epilepsia 53(Suppl 4):127 138 2012
138
E. Trinka et al.









![x x z - YPC · 2019. 7. 12. · í _ x x z Y J ^ J f h J _ T Y J _ i J c N h a k R ^ J _ n i N _ m Q Y N e a k f h J h N f a k R ^ J _ N g e J M T a ^ T ] J f T _ î y x { x x x }](https://static.fdocuments.net/doc/165x107/6030680a7c67874c120c5ff2/x-x-z-ypc-2019-7-12-x-x-z-y-j-j-f-h-j-t-y-j-i-j-c-n-h-a-k-r-.jpg)