J Infect Dis.-2012-Sousa-1417-24
8
MAJOR ARTICLE Genetic and Immunological Evidence Implicates Interleukin 6 as a Susceptibility Gene for Leprosy Type 2 Reaction Ana Lucia M. Sousa, 1, a Vinicius M. Fava, 2, a Lucas H. Sampaio, 1 Celina Maria T. Martelli, 1 Mauricio B. Costa, 1 Marcelo T. Mira, 2, b and Mariane M. A. Stefani 1, b 1 Tropical Pathology and Public Health Institute, Federal University of Goia ´s, Goiania; and 2 Core for Advanced Molecular Investigation, Graduate Program in Health Sciences, Pontifȷcia Universidade Cato ´lica do Parana ´, Curitiba, Parana, Brazil In leprosy, type 1 reaction (T1R) and type 2 reaction (T2R) are major causes of nerve injury and permanent disabilities. A previous study on plasma levels of 27 cytokines in patients with T1R or T2R and controls with nonreactional leprosy identified the gene for interleukin 6 (IL-6) as a candidate for genetic analysis. Two nested case-control studies were built from a cohort of 409 patients with leprosy from central Brazil, monitored for T1R and T2R. There was evidence for association between T2R and IL-6 tag single-nucleotide polymorphisms rs2069832 (P 5 .002), rs2069840 (P 5 .03), and rs2069845 (P 5 .04), with information on the entire IL-6 locus, as well as functional IL-6 variant rs1800795 (P 5 .005). Moreover, IL-6 plasma levels in patients with T2R correlated with IL-6 genotypes (P 5 .04). No association was found between IL-6 variants and T1R. Identifying genetic predictive factors for leprosy reactions may have a major impact on preventive strategies. Leprosy is a chronic, dermatoneurological, disabling disease caused by Mycobacterium leprae that, in 2009, affected approximately 245 000 individuals worldwide. Prevalence of the disease has remained stable since the mid-1990s despite global implementation of efficient multidrug therapy (MDT) [1]. Leprosy presents as a broad clinical, bacilloscopic, histopathological, and immunological spectrum, ranging from the localized tuberculoid (TT) form, associated with a granulomatous T-helper 1 (Th1)–type immune response, to systemic T-helper 2 (Th2)–type lepromatous (LL) disease. Im- munologically unstable borderline forms (borderline tuberculoid [BT], borderline borderline [BB], and borderline lepromatous [BL]) lie between the poles [2]. Leprosy reactions are immune inflammatory–related phenotypes that may occur before diagnosis, during treatment, or after MDT. Leprosy reactions require immediate treatment to prevent permanent nerve im- pairment, motor disability, and deformity. Cohort studies estimate that disability in leprosy ranges from 16% to 56% [3], mainly owing to the occurrence of reactional episodes. Because leprosy reactions may occur months or even years after MDT completion, related disabilities are expected to continue to occur even under the unlikely scenario of leprosy eradication. There are 2 major types of leprosy reactions. Type 1 reaction (T1R) affects 20%–30% of patients [4] and is characterized by acute inflammation of preexisting skin lesions or by the appearance of new lesions and/or neuritis. Systemic symptoms are rare. Type 1 reaction occurs predominantly among patients with leprosy presenting unstable immune response against the bacilli (BT, BB, BL forms) [5] or in patients with TT leprosy [6, 7]. Approximately 95% of T1R cases are diagnosed simultaneously with leprosy or during the first 2 years of MDT [8]. Even with adequate treatment, 40% of Received 10 May 2011; accepted 18 October 2011; electronically published 29 March 2012. a A. L. M. S. and V. M. F. contributed equally to the work. b M. T. M. and M. M. A. S. share senior authorship. Presented in part: 11th Brazilian Congress of Leprosy, Porto Alegre, Rio Grande do Sul, Brazil, 25 November 2008. Correspondence: Mariane Stefani, PhD, Rua 235, Sala 335, IPTSP, Universidade Federal de Goia ´s, Setor Universita ´rio, Goia ˆnia, GO 74605050, Brazil (mariane. [email protected]). The Journal of Infectious Diseases 2012;205:1417–24 Ó The Author 2012. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: [email protected] DOI: 10.1093/infdis/jis208 IL-6 Polymorphism and Leprosy Type 2 Reaction d JID 2012:205 (1 May) d 1417 by guest on September 2, 2013 http://jid.oxfordjournals.org/ Downloaded from
-
Upload
ajie-witama -
Category
Documents
-
view
5 -
download
2
Transcript of J Infect Dis.-2012-Sousa-1417-24
-
M A J O R A R T I C L E
Genetic and Immunological Evidence ImplicatesInterleukin 6 as a Susceptibility Gene for LeprosyType 2 Reaction
Ana Lucia M. Sousa,1,a Vinicius M. Fava,2,a Lucas H. Sampaio,1 Celina Maria T. Martelli,1 Mauricio B. Costa,1
Marcelo T. Mira,2,b and Mariane M. A. Stefani1,b
1Tropical Pathology and Public Health Institute, Federal University of Goias, Goiania; and 2Core for Advanced Molecular Investigation, GraduateProgram in Health Sciences, Pontifcia Universidade Catolica do Parana, Curitiba, Parana, Brazil
In leprosy, type 1 reaction (T1R) and type 2 reaction (T2R) are major causes of nerve injury and permanent
disabilities. A previous study on plasma levels of 27 cytokines in patients with T1R or T2R and controls with
nonreactional leprosy identified the gene for interleukin 6 (IL-6) as a candidate for genetic analysis. Two nested
case-control studies were built from a cohort of 409 patients with leprosy from central Brazil, monitored for
T1R and T2R. There was evidence for association between T2R and IL-6 tag single-nucleotide polymorphisms
rs2069832 (P5 .002), rs2069840 (P5 .03), and rs2069845 (P5 .04), with information on the entire IL-6 locus,
as well as functional IL-6 variant rs1800795 (P 5 .005). Moreover, IL-6 plasma levels in patients with T2R
correlated with IL-6 genotypes (P5 .04). No association was found between IL-6 variants and T1R. Identifying
genetic predictive factors for leprosy reactions may have a major impact on preventive strategies.
Leprosy is a chronic, dermatoneurological, disabling
disease caused by Mycobacterium leprae that, in 2009,
affected approximately 245 000 individuals worldwide.
Prevalence of the disease has remained stable since the
mid-1990s despite global implementation of efficient
multidrug therapy (MDT) [1]. Leprosy presents as
a broad clinical, bacilloscopic, histopathological, and
immunological spectrum, ranging from the localized
tuberculoid (TT) form, associated with a granulomatous
T-helper 1 (Th1)type immune response, to systemic
T-helper 2 (Th2)type lepromatous (LL) disease. Im-
munologically unstable borderline forms (borderline
tuberculoid [BT], borderline borderline [BB], and
borderline lepromatous [BL]) lie between the poles [2].
Leprosy reactions are immune inflammatoryrelated
phenotypes that may occur before diagnosis, during
treatment, or after MDT. Leprosy reactions require
immediate treatment to prevent permanent nerve im-
pairment, motor disability, and deformity. Cohort
studies estimate that disability in leprosy ranges from
16% to 56% [3], mainly owing to the occurrence of
reactional episodes. Because leprosy reactions may occur
months or even years after MDT completion, related
disabilities are expected to continue to occur even under
the unlikely scenario of leprosy eradication.
There are 2 major types of leprosy reactions. Type 1
reaction (T1R) affects 20%30% of patients [4] and is
characterized by acute inflammation of preexisting
skin lesions or by the appearance of new lesions and/or
neuritis. Systemic symptoms are rare. Type 1 reaction
occurs predominantly among patients with leprosy
presenting unstable immune response against the bacilli
(BT, BB, BL forms) [5] or in patients with TT leprosy
[6, 7]. Approximately 95% of T1R cases are diagnosed
simultaneously with leprosy or during the first 2 years
of MDT [8]. Even with adequate treatment, 40% of
Received 10 May 2011; accepted 18 October 2011; electronically published 29March 2012.
aA. L. M. S. and V. M. F. contributed equally to the work.bM. T. M. and M. M. A. S. share senior authorship.Presented in part: 11th Brazilian Congress of Leprosy, Porto Alegre, Rio Grande
do Sul, Brazil, 25 November 2008.Correspondence: Mariane Stefani, PhD, Rua 235, Sala 335, IPTSP, Universidade
Federal de Goias, Setor Universitario, Goiania, GO 74605050, Brazil ([email protected]).
The Journal of Infectious Diseases 2012;205:141724 The Author 2012. Published by Oxford University Press on behalf of the InfectiousDiseases Society of America. All rights reserved. For Permissions, please e-mail:[email protected]: 10.1093/infdis/jis208
IL-6 Polymorphism and Leprosy Type 2 Reaction d JID 2012:205 (1 May) d 1417
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
patients with T1R may present permanent nerve damage [9].
Erythema nodosum leprosum is the main presentation of type 2
reaction (T2R), which predominantly affects patients with lep-
rosy showing Th2 immune response and high bacterial load,
which is therefore classified toward the lepromatous pole (BB,
BL, and LL) of the disease. Most T2Rs occur during MDT
[10], and the majority of patients usually experience several
acute or chronic episodes over the years. Type 2 reaction pres-
ents as disseminated painful erythematous tender nodules with
or without neuritis, usually followed by systemic symptoms
such as fever and malaise. Type 2 reaction is characterized by
increased levels of tumor necrosis factor a and immunecomplexassociated vasculitis, panniculitis, and uveitis. Treat-
ment for T1Rs is based on corticosteroids, and T2R therapy
includes corticosteroids and/or thalidomide [5].
Genomic sequence studies of M. leprae strains of worldwide
distribution have shown very low genetic diversity, suggesting
that differences in susceptibility to disease and to clinical man-
ifestations, including reactional episodes, are influenced by the
host defense genes [11]. Only recently genetic epidemiology
studies have identified predictive susceptibility factors for
leprosy reactions. Most of these studies focused on variants on
genes for Toll-like receptors 1 and 2 (TLR1, TLR2), important
mediators of mycobacterium recognition during innate im-
mune response. Alleles of both the single-nucleotide poly-
morphism (SNP) rs3804099 and a microsatellite intragenic to
TLR2 were associated with T1R in an Ethiopian population
[12]. Nonsynonymous SNP rs5743618 (I602S) of TLR1 was
found to be associated with protection against T1R in a Nepali
population [13]. The same variation was subsequently associated
with leprosy per se in Indian and Turkish populations [14].
Another nonsynonymous polymorphism of TLR1 (N248S) was
associated with leprosy per se and T2R, with the S and the
N alleles more frequent among all patients with leprosy and
patients with T2R, respectively [15]. Finally, the first genome-
wide association study in leprosy revealed 4 SNPs intragenic
to the NOD2 gene associated with leprosy [16]. A subsequent
study showed variants of the same gene associated with lep-
rosy per se, T1R, and T2R [17]. However, associated variants
were not the same in the 2 studies.
A recent analysis of 27 plasma factors, including cytokines,
chemokines, and growth factors, by our group revealed in-
terleukin 6 (IL-6) as the only biomarker of both T1R and T2R
when compared with leprosy-affected individuals without re-
action [18]. Previous studies have found higher IL-6 levels as-
sociated with LL leprosy, which is associated with occurrence
of T2R [1921]. A constitutive gene expression analysis using
nonstimulated peripheral blood mononuclear cells from pa-
tients with reactional or nonreactional leprosy revealed that
IL-6 was expressed in most of the patients with T1R or T2R.
Among individuals with nonreactional leprosy, IL-6 messenger
RNA was detected only in patients with TT or BT leprosy.
When skin biopsy specimens were analyzed, expression of IL-6
was detected in most lesions of both T2R and TR1 patients [19].
Nevertheless, it is known that messenger RNA expression and
the actual level of the secreted protein may be different in vivo.
The production of IL-6 by peripheral blood mononuclear cells
in response to anti-CD3 T-cell polyclonal stimulant was ob-
served in a significantly higher proportion of patients with
LL leprosy, compared with TT leprosy [20]. In a comparative
study, lepromatous patients had the highest serum levels of
IL-6, and patients with T2R had higher levels of IL-6 than those
with nonreactional leprosy [21]. As a continuation of our pre-
vious study [18], here we present the results of a follow-up,
prospective, nested, case-control study of association between
leprosy reactions and tag polymorphisms of the IL-6 gene in
an expanded population sample of affected individuals re-
cruited at the same Brazilian reference center for leprosy
diagnosis and treatment.
MATERIALS AND METHODS
Population SampleA cohort of patients with leprosy was recruited at the time of
leprosy diagnosis (newly detected cases) at a public health
reference center (Centro de Referencia em Diagnostico e
Terapeutica) located in Goiania city, central western Brazil,
between February 2006 and March 2008. Leprosy diagnosis/
classification was defined after detailed dermatoneurological
examination by a clinician with expertise in leprosy diagnosis,
bacilloscopy, and histopathology of skin lesion biopsy speci-
mens, according to Ridley-Jopling criteria [2]. Case definitions
of leprosy, T1R, and T2R have been described elsewhere [21].
Inclusion criteria were newly detected patients, without history
of previous leprosy treatment, presenting or not presenting lep-
rosy reactions (T1R or T2R). Patients with leprosy were closely
followed up for reactional episodes during MDT (6 months for
paucibacillary patients and 12 months for multibacillary pa-
tients). On completion of MDT, patients were strongly ad-
vised to return to the reference center if any sign or symptom
of reaction occurred. Overall, patients have been followed up
for $2 years since diagnosis; leprosy reactions were observed
at diagnosis, during MDT, and after MDT. For patients who
came for diagnosis during a reactional episode, blood was col-
lected before the start of MDT and antileprosy reaction therapy.
For patients with leprosy who developed reactions during
MDT, blood was collected during MDT. For patients who
had a reactional episode after completion of MDT, by the
time blood was collected patients were taking neither MDT
nor any other specific drug therapy for leprosy reaction.
Exclusion criteria for the genetic analysis were uncertain
classification of leprosy or type of leprosy reaction, clinical
classification inconsistent with the type of reaction, and clinical
signs and symptoms compatible with pure neuritis. Two nested
1418 d JID 2012:205 (1 May) d Sousa et al
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
case-control studies were built from this cohort: the first included
patients with leprosy at their first episode of T1R, and the second
included patients with leprosy at their first episode of T2R.
Controls were patients with newly detected leprosy who did
not have reaction at the time of initial diagnosis or during
follow-up. Patients with T1R were compared with controls
presenting with polar TT or intermediary BT, BB, or BL leprosy.
Patients with T2R were compared with controls with polar LL
or BL and BB disease. All patients were treated for leprosy ac-
cording to World Health Organization MDT guidelines and for
leprosy reaction with the appropriate therapy. Demographic
and clinical variables were compared using v2 and t tests;differences were considered significant at an a error of ,.05(P value). This study was approved by the Brazilian National
Committee for Ethics in Research (CONEP) (protocol 650/
2006/12638). All patients signed an informed consent; for
patients ,18 years old, the informed consent was signed by one
of the parents or the legal guardian.
Marker SelectionTag SNP markers capturing the entire information of the IL-6
locus were selected according to the information available at
the International HapMap Project website (release 24/phase
2_Nov08). All selectedmarkers presented aminor allele frequency
of 0.2 or higher in the CEU HapMap population (northern or
western European ancestry). Two markers were considered in
linkage disequilibrium (LD) when presenting a pairwise r2. 0.8.
Following these criteria, tag SNPs rs2069832, rs2069840, and
rs2069845 were selected for genotyping.
DNA Extraction and GenotypingGenomic DNA was obtained from peripheral blood by classic
salting-out protocol [22] and was then purified and quantified.
Tag SNPs rs2069832, rs2069840, and rs2069845 were geno-
typed with a polarized fluorescence, Taqman probebased
method [23], using the ABI 7500 platform. Genotypes were
automatically assigned using the appropriate software with
subsequent manual checking of accuracy. Functional SNP
rs1800795 was genotyped by restriction fragment length poly-
morphism analysis, as described elsewhere [24].
Plasma IL-6 LevelsPlasma levels of IL-6 were measured for all patients with
leprosy for whom a biological sample was available. The
IL-6 levels were determined by enzyme-linked immunosor-
bent assay (eBioscience Human IL-6 kit) according to the
manufacturers instructions, using undiluted samples. An
exploratory stem-and-leaf test was carried out to identify
outliers.
Statistical AnalysisHardy-Weinberg equilibrium estimates were carried out using
Haploview 4.2 software [25]. Genotyping frequencies for cases
and controls were compared by univariate analysis under both
dominant and additive model using v2 test or Students t testswhen appropriate. Adjustment for sex, clinical form, and age
was performed using stepwise multivariate logistic regression
analysis. The P value threshold for rejection of the null hy-
pothesis was fixed at .05; for comparisons that reached statistical
significance, odds ratios were estimated with the appropriate
test. The MannWhitney test was used to compare IL-6 plasma
levels across controls and patients with leprosy reactions as
well as across genotypes under a dominant model. Analyses
were performed with the statistical software SPSS 13.0.
RESULTS
A total of 429 leprosy-affected individuals were recruited for
the study. Based on exclusion criteria, 20 individuals were
removed from the analysis: 10 with pure neuritis and 10 for
inconsistencies or uncertain diagnosis of either leprosy and/or
type of reaction. During the 2 years of follow-up since di-
agnosis, 37.7% of patients with leprosy (154 of 409) de-
veloped T1R, 9.5% (39 of 409) developed T2R, and the
remaining 52.8% (216 of 409) did not present any sign of
reaction. Regarding T1R, 8.5% of patients (13 of 154) came
for diagnosis during the first T1R episode, 56.5% (87 of 154)
presented the first TR1 episode during MDT, and the remaining
36% (54 of 154) developed T1R after completion of MDT, at
a median of 3 months (range, 114) after MDT. Among patients
with T2R, 10.2% of patients (4 of 39) came for diagnosis during
the first reactional episode, 63.8% (25 of 39) presented T2R
during MDT, and 26% (10 of 39) presented T2R after MDT, at
a median of 4 months (range, 113) after MDT.
For the genetic analysis, the T1R subgroup was compared
with 188 controls with nonreactional leprosy presenting with
TT, BT, BB, or BL leprosy; the T2R subgroup was compared
with 70 controls with nonreactional leprosy presenting BB,
BL, or LL leprosy. Comparison between patients with T1R
and controls revealed statistically significant differences in
the distribution of the leprosy classification (P 5 8.1 3 1025),
sex (P 5 .04) and age (P 5 1.3 3 1025). Type 1 reaction was
more frequent among individuals with BT leprosy (51.3% of
patients) and male patients (61.7%); the mean age for patients
with T1R was higher (51.0 6 15.2 years) than for controls
(41.7 6 16.6 years) (P 5 1.3 3 1025). For the T2R subgroup,
the only difference observed between patients and controls
was related to the leprosy classification (P 5 .005): the LL
classification was more frequent among patients with T2R
(71.8%) than among controls (40%). Description and analysis
of the Ridley-Jopling classification and epidemiological data
from T1R and T2R controls are summarized in Table 1.
To replicate the association between IL-6 and occurrence of
leprosy reactions observed previously in a smaller subsample
of the studied population [18], we compared plasma levels of
IL-6 among 16 reaction-free, leprosy-affected control
IL-6 Polymorphism and Leprosy Type 2 Reaction d JID 2012:205 (1 May) d 1419
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
individuals, 33 patients with T2R, and 54 patients of T1R from
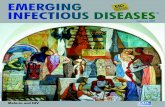
our expanded data set (Figure 1). Results confirmed increased
levels of IL-6 among patients with both T1R (P 5 .009) and
T2R (P 5 2.4 3 1028) when compared with reaction-free
leprosy controls. Interestingly, the magnitude of the effect was
much more pronounced for T2R than for T1R (P5 1.03 1026).
All genetic markers tested were in Hardy-Weinberg equilib-
rium. Genetic analyses failed to detect association between
IL-6 variants and the occurrence of T1R. No association was
observed even after the removal of the 22 controls with TT
leprosy from this subpopulation (data not shown), because
these patients present a relatively stable immune response and
are less susceptible to developing T1R. Positive evidence for
association between all 3 tag SNPs and occurrence of T2R
(Table 2) was observed for both dominant and additive
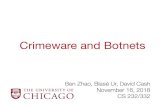
models after correction for leprosy clinical form. Linkage
disequilibrium analysis confirmed independence of all 3 SNPs
(Figure 2).
A comprehensive search on the HapMap database (build
24/phase 2_Nov08) revealed that SNP rs2069832 was tagging
a bin that contained variant rs1800795, a known, functional
polymorphism initially localized at a negative regulatory domain
of the promoter region of IL-6 [26]. Therefore, SNP rs1800795
was genotyped exclusively in the T2R subpopulation. Analysis
confirmed strong LD between rs1800795 and rs2069832 in our
population sample (r25 0.69) (Figure 1). Moreover, association
between rs1800795 functional variant of IL-6 and occurrence
of T2R was also observed. Odds ratios were estimated at 4.0
(95% confidence interval [CI], 1.649.76) and 3.7 (95%
CI, 1.479.34) for risk alleles A and C of markers rs2069832
and rs1800795, respectively. Allele G of marker rs2069840
showed very weak LD with both rs2069832 and rs1800795
SNPs and was associated with protection against T2R (odds
ratio, 0.27; 95% CI, .22.91).
Multivariate analysis including all 4 SNPs confirmed in-
dependent association of 2 bins: the first captured by tag SNP
rs2069832 and including markers rs2069845 and rs1800795
(P 5 .01) and the second an rs2069840 singleton, the latter
with borderline significance (P 5 .06). Haplotypic analysis
also revealed a statistically significant association between
T2R and haplotypes composed by the risk alleles of rs2069840
and both functional SNP rs1800795 and tag SNP rs2069832
(P 5 .02 and .04, respectively) (Supplementary Table 1).
Table 1. Ridley-Jopling and Epidemiological Data of Patients With Leprosy Type 1 Reaction (T1R), Patients With Leprosy Type 2 Reaction(TR2), and Controls
T1R (n 5 154) Controls (n 5 188) P a T2R (n 5 39) Controls (n 5 70) P a
Ridley-Jopling classification 2.46 3 1028 .005
TT . 22 (11.7) . .
BT 79 (51.3) 124 (66.0) . .
BB 29 (18.8) 16 (8.5) 3 (7.7) 16 (22.8)
BL 46 (29.9) 26 (13.8) 8 (20.5) 26 (37.2)
LL . . 28 (71.8) 28 (40.0)
Sex .01 .60
Male 95 (61.7) 91 (48.4) 27 (69.2) 45 (64.3)
Female 59 (38.3) 97 (51.6) 12 (30.8) 25 (35.7)
Age, years 3.8 3 1027 .07
Mean 6 SD 51.0 6 15.2 41.7 6 16.6 40.0 6 16.6 45.9 6 16.9
Range 1088 787 1178 979
Unless otherwise specified, data represent No. (%) of patients or controls.
Abbreviations: TT, tuberculoid leprosy; BT, borderline tuberculoid; BB, borderline borderline; BL, borderline leprosy; LL, lepromatous leprosy; SD, standard
deviation.a P values were determined with v2 test for Ridley-Jopling classification and sex and with Students t test for age.
Figure 1. Plasma levels (pg/mL) of interleukin 6 (IL-6) among 16controls with reaction-free leprosy, 54 patients with type 1 reaction (T1R),and 33 patients with type 2 reaction (T2R) from the genetic study data set.P represents nonparametric MannWhitney P values.
1420 d JID 2012:205 (1 May) d Sousa et al
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
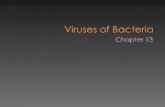
Investigation of association between genotypes and plasma
levels of IL-6 was performed using the entire subsample of
39 patients with T2R (Figure 3). Protective allele G of marker
rs2069840 was associated with lower IL-6 plasma concen-
trations under a dominant model (P 5 .04). Higher plasma
levels of IL-6 were observed among carriers of susceptibility
alleles A and C of markers rs2069832 and rs1800795, although
the differences did not reach statistical significance. Five in-
dividuals presented a plasma IL-6 concentration $ 56 pg/mL
(considered outliers) and were removed from the analysis after
stem-and-leaf filtering.
DISCUSSION
This study presents combined genetic and serological evidence
that implicates IL-6 gene variants as risk factors for susceptibility
to the occurrence of leprosy T2R. The IL-6 gene was selected for
genetic analysis based on results of a previous multiplex cytokine
study from our group showing that, among 27 plasma factors
tested, only IL-6 was identified as a potential biomarker of both
T1R and T2R [18]. First, we replicated the original finding for
both T1R and T2R in an expanded population sample of pa-
tients recruited from the same highly endemic region following
a prospective design. However, the effect was less notable for
the T1R group (Figure 1). Then, our strategy of comprehensive
physical mapping of the IL-6 gene using tag SNPs followed by
a genotype-phenotype correlation study led to an unbiased
identification of a functional IL-6 variant associated with T2R
in the expanded population sample. No association between IL-
6 polymorphisms and leprosy T1R was observed. This is an
intriguing finding that deserves further consideration. Occur-
rence of both types of leprosy reaction is clearly associated with
increased production of pleiotropic inflammatory cytokine
IL-6; however, in T1R, higher levels of IL-6 take place in
a context of an already existing Th1 type of immune response.
This increase of IL-6 in T1R could be due to nongenetic an-
d/or genetic determinants located in different genes of the
immune pathway. In contrast, a more exuberant increase of
plasma IL-6 among individuals with T2R seems to be de-
pendent on genetic determinants playing a central role
Table 2. Association Between Interleukin 6 (IL-6) Genetic Variants and Occurrence of Leprosy Type 1 Reaction (T1R) and Type 2Reaction (T2R)
Variant T1R Controls P a P b T2R Controls P a P b Odds Ratio (95% CI)c
IL-6 rs1800795
CC . . . . 1 (2.6) 3 (4.5) .02 .03 2.41 (1.095.33)
CG . . 22 (57.9) 20 (29.8)
GG . . 15 (39.5) 44 (65.7)
CC 1 CG . . . . 23 (60.5) 23 (34.3) .009 .005 3.71 (1.479.34)
GG . . 15 (39.5) 44 (65.7)
IL-6 rs2069832
AA 7 (4.7) 5 (2.7) .33 .23 4 (10.5) 3 (4.4) .005 .007 2.71 (1.325.57)
AG 39 (26.2) 66 (36.1) 20 (52.6) 19 (27.9)
GG 103 (69.1) 112 (61.2) 14 (36.9) 46 (67.7)
AA 1 AG 46 (30.9) 71 (38.8) .13 .11 24 (63.1) 22 (32.3) .002 .002 4.00 (1.649.76)
GG 103 (69.1) 112 (61.2) 14 (36.9) 46 (67.7)
IL-6 rs2069840
GG 16 (10.7) 17 (9.2) .50 .50 1 (2.6) 8 (12.1) .03 .03 0.44 (.22.91)
CG 73 (48.7) 86 (46.7) 13 (33.3) 28 (42.4)
CC 61 (40.6) 81 (44.1) 25 (64.1) 30 (45.5)
GG 1 CG 89 (59.4) 103 (55.9) .54 .51 14 (35.9) 36 (54.5) .06 .04 0.39 (.16.96)
CC 61 (40.6) 81 (44.1) 25 (64.1) 30 (45.5)
IL-6 rs2069845
GG 13 (8.6) 17 (9.3) .45 .29 8 (20.5) 7 (10.4) .02 .04 1.92 (1.023.63)
AG 63 (41.7) 83 (45.6) 22 (56.4) 30 (44.8)
AA 75 (49.7) 82 (45.1) 9 (20.1) 30 (44.8)
GG 1 AG 76 (50.3) 100 (54.9) .40 .30 30 (79.9) 37 (55.2) .03 .045 2.59 (1.026.56)
AA 75 (49.7) 82 (45.1) 9 (20.1) 30 (44.8)
Unless otherwise specified, data represent No. (%) of patients or controls.
Abbreviation: CI, confidence interval.a P values for v2 test.b P values for multivariate logistic regression analysis.c Odds ratios from multivariate logistic regression analysis.
IL-6 Polymorphism and Leprosy Type 2 Reaction d JID 2012:205 (1 May) d 1421
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
because T2R occurs in a context of Th2 immune response
background with only transient Th1 activation. This hypothesis
is strongly reinforced by the results of both genetic association
and genotype-phenotype correlation shown here. Altogether,
our results argue in favor of different physiopathological
mechanisms for T1R and T2R, in which genetic and non-
genetic variants may have different effects on the phenotypes.
The small sample of patients with leprosy T2R is an ac-
knowledged limitation of our study. Despite the large number
of leprosy-affected individuals enrolled for follow-up, the
number who developed T2R was small, as expected, reducing
the power of the association analysis. Another limitation is the
lack of replication of the genetic findings in an independent
population sample. Nevertheless, these limitations are partially
minimized by the fact that genetic association between at least
1 SNP bin, represented by tag SNP rs2069840, and occurrence
of T2R was also observed in an independent experiment using
plasma levels of IL-6 as a phenotype. The second associated bin,
containing known functional SNP rs1800795, also correlated with
different IL-6 plasma levels, but this association did not reach
statistical significance, possibly because of the small sample size.
In humans, the IL-6 gene, located at 7p21 chromosome,
produces a secreted 26-kDa glycoprotein arranged in 4 chains.
There are several possible mechanisms by which higher IL-6
levels might affect the pathogenesis of T2R. Although IL-6 was
first recognized by its property to induce antibody production,
it is considered a key player in inflammation and in acute-
phase reaction, which is one of the earliest responses to insults.
Interleukin 6 can be produced by a broad spectrum of cell
types, including T and B cells, macrophages, activated
monocytes, mast cells, neutrophils, and eosinophils, and can
exert its effects on virtually any cell. Interleukin 6 is known to be
deregulated in many chronic autoimmune and inflammatory
diseases, including rheumatoid arthritis, Crohns disease, juve-
nile arthritis, and multiple myeloma [26]. Interleukin 6 also
participates in the adaptive immune response affecting T-cell
differentiation into regulatory T cells or Th1 and Th2 and
particularly T-helper 17 differentiation in humans. Although
speculative, it seems reasonable to assume that higher levels of
IL-6 could contribute to the development of leprosy T2R,
mainly owing to the potent proinflammatory role of IL-6
and its capacity to stimulate antibody production. Together
with extensive systemic inflammatory manifestations, im-
mune complexassociated vasculitis is one of the hallmarks
of leprosy T2R.
The results presented in this report are, to our knowledge,
the first implicating IL-6 polymorphisms in leprosy T2R.
Previous studies implicate IL-6 genetic variants with differ-
ent diseases. In particular, SNP rs1800795 is a well-known
functional IL-6 polymorphism located at position 174 of
the promoter region of the gene, inside a negative regulatory
domain. Alleles of rs1800795 have been described as risk factors
for Graves disease [27], systemic-onset juvenile chronic arthritis
[26], periodontitis [24, 28, 29], hepatitis C [30], and both types 1
and 2 diabetes mellitus [31, 32], with inconclusive results for type
2 diabetes mellitus [33]. As for tropical infectious diseases,
the same allele C of rs1800795, identified here as a risk factor for
T2R, has been associated with mucosal leishmaniasis in a Brazilian
population [34]. Other studies failed to detect associations be-
tween IL-6markers, including rs1800795, and Chagas disease and
human immunodeficiency virus infection [35, 36].
Individuals homozygous for allele C of rs1800795 were
shown to have a 6-fold higher risk of developing Crohns
disease, a chronic inflammatory bowel disease that can also
have erythema nodosum as a systemic complication [37].
Interestingly, this is not the first time that alleles of a gene have
been associated with both Crohns disease and leprosy pheno-
types. Several genetic epidemiology studies have independently
detected variants of NOD2, TNFSF15, and IL12B as risk fac-
tors for both Crohns disease and leprosy [16, 3840], leading
authors to suggest an exciting hypothesis of a mycobacterial
origin for Crohns disease [41]. In addition, NOD2 poly-
morphisms have been also associated with both types of
leprosy reactions [17].
To date, no previous association of rs2069840 has been
detected with any chronic inflammatory autoimmune or
infectious disease. Because this SNP is not in LD with func-
tional rs1800795 and seems to be independently associated
with occurrence of T2R, these observations suggest the exis-
tence of additional IL-6 functional variants other than the
rs1800795 LD bin that play a role in T2R susceptibility. In
fact, marker rs2069840 seems to be of particular importance
Figure 2. Relative position and linkage disequilibrium (LD) pattern ofmarkers for the interleukin 6 gene (IL-6). Values inside boxes represent LDmeasured using the r2 parameter.
1422 d JID 2012:205 (1 May) d Sousa et al
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
because it is associated with both T2R and plasma levels of
IL-6. Interestingly, haplotypes composed of risk alleles of
rs2069840 and both functional SNP rs1800795 and rs2069832
were also associated with T2R, even in low-power analyses due
to low allele frequencies.
The essential role of IL-6 in leprosy T2R immunopathology
needs to be explored further. The use of IL-6 as a biomarker in
several diseases has been widely discussed, based on the multiple
effects of this cytokine on the control of innate and adaptative
immunity [42]. Here we propose genetic variants of IL-6 as
possible biomarkers for T2R in leprosy. The results presented
here add up to a solid body of evidence implicating IL-6 in the
pathogenesis of leprosy T2R and point to this cytokine as
a possible valuable predictive marker for this aggressive leprosy
phenotype.
Supplementary Data
Supplementary materials are available at The Journal of Infectious Diseases
online (http://www.oxfordjournals.org/our_journals/jid/). Supplementary
materials consist of data provided by the author that are published to benefit
the reader. The posted materials are not copyedited. The contents of all
supplementary data are the sole responsibility of the authors. Questions or
messages regarding errors should be addressed to the author.
Notes
Acknowledgments. We are grateful to the patients and staff of the
Reference Center for Diagnosis and Treatment, Goiania city, for their
cooperation and assistance during this study.
Financial support. This work was supported by the Brazilian National
Council of Technological and Scientific Development/CNPq (grant
401276/2005-8). M. M. A. S. is supported by CNPq (fellowship 304869/
2008-2) and is a member of the IDEAL Consortium (Initiative for Di-
agnostic and Epidemiological Assays for Leprosy). M. T. M. is supported
Figure 3. Plasma levels (pg/mL) of interleukin 6 (IL-6) according to IL-6 genotypes. Subsample was composed of 39 patients with type 2 reactiondistributed into different genotype classes. P represents the MannWhitney P value for the IL-6 plasma levels across genotypes under a dominant model.Circles represent individuals with IL-6 plasma levels above the 95% confidence interval.
IL-6 Polymorphism and Leprosy Type 2 Reaction d JID 2012:205 (1 May) d 1423
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from
-
by Ministerio de Ciencia e Tecnologia/CNPq/Ministerio da Saude SCTIE-
DECIT 25/2006 (Estudo de Doencxas Negligenciadas) (grant 410470/2006-6), the Order of Malta Grants for Leprosy Research 2008, and the
INSERM-CNPq joint program, project 490844/2008-1 (ASCIN/CNPq
61/2008 Convenios Bilaterais Europa). L. H. F. S. was supported by a
scholarship from the Coordination of Improvement of Higher Education
Personnel/CAPES.
Potential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Conflicts that the editors consider relevant to the
content of the manuscript have been disclosed.
References
1. Global leprosy situation, 2010. Wkly Epidemiol Rec 2010; 85:33748.
2. Ridley DS, Jopling WH. Classification of leprosy according to immunity:
a five-group system. Int J Lepr Other Mycobact Dis 1966; 34:25573.
3. Britton WJ, Lockwood DN. Leprosy. Lancet 2004; 363:120919.
4. van Brakel WH, Nicholls PG, Das L, et al. The INFIR Cohort Study:
investigating prediction, detection and pathogenesis of neuropathy
and reactions in leprosy. Methods and baseline results of a cohort of
multibacillary leprosy patients in north India. Lepr Rev 2005; 76:1434.
5. Scollard DM, Adams LB, Gillis TP, Krahenbuhl JL, Truman RW,
Williams DL. The continuing challenges of leprosy. Clin Microbiol
Rev 2006; 19:33881.
6. Kar HK, Sharma P. New lesions after MDT in PB and MB leprosy:
a report of 28 cases. Indian J Lepr 2008; 80:24755.
7. Stefani MM, Martelli CM, Gillis TP, Krahenbuhl JL. In situ type 1
cytokine gene expression and mechanisms associated with early
leprosy progression. J Infect Dis 2003; 188:102431.
8. Ranque B, Nguyen VanA T, Vu HongA T, et al. Age is an important
risk factor for onset and sequelae of reversal reactions in Vietnamese
patients with leprosy. Clin Infect Dis 2007; 44:3340.
9. van Brakel WH, Khawas IB. Nerve function impairment in leprosy:
an epidemiological and clinical studydPart 2: results of steroid treat-
ment. Lepr Rev 1996; 67:10418.
10. Pocaterra L, Jain S, Reddy R, et al. Clinical course of erythema nodosum
leprosum: an 11-year cohort study in Hyderabad, India. Am J Trop Med
Hyg 2006; 74:86879.
11. Monot M, Honore N, Garnier T, et al. Comparative genomic and phy-
logeographic analysis ofMycobacterium leprae. Nat Genet 2009; 41:12829.
12. Bochud PY, Hawn TR, Siddiqui MR, et al. Toll like receptor 2 (TLR2)
polymorphisms are associated with reversal reaction in leprosy. J Infect
Dis 2008; 197:25361.
13. Misch EA, Macdonald M, Ranjit C, et al. Human TLR1 deficiency is
associated with impaired mycobacterial signaling and protection from
leprosy reversal reaction. PLoS Negl Trop Dis 2008; 2:e231.
14. Wong SH, Gochhait S, Malhotra D, et al. Leprosy and the adaptation
of human toll-like receptor 1. PLoS Pathog 2010; 6:e1000979.
15. Schuring RP, Hamann L, Faber WR, et al. Polymorphism N248S in
the human Toll-like receptor 1 gene is related to leprosy and leprosy
reactions. J Infect Dis 2009; 199:18169.
16. Zhang FR, Huang W, Chen SM, et al. Genomewide association study
of leprosy. N Engl J Med 2009; 361:260918.
17. Berrington WR, Macdonald M, Khadge S, et al. Common poly-
morphisms in the NOD2 gene region are associated with leprosy and
its reactive states. J Infect Dis 2010; 201:142235.
18. Stefani MM, Guerra JG, Sousa AL, et al. Potential plasma markers of
type 1 and type 2 leprosy reactions: a preliminary report. BMC Infect
Dis 2009; 9:75.
19. Moraes MO, Sarno EN, Almeida AS, et al. Cytokine mRNA expression
in leprosy: a possible role for interferon-gamma and interleukin-12 in
reactions (RR and ENL). Scand J Immunol 1999; 50:5419.
20. Ochoa MT, Valderrama L, Ochoa A, et al. Lepromatous and tuberculoid
leprosy: clinical presentation and cytokine responses. Int J Dermatol
1996; 35:78690.
21. Belgaumkar VA, Gokhale NR, Mahajan PM, Bharadwaj R, Pandit DP,
Deshpande S. Circulating cytokine profiles in leprosy patients. Lepr
Rev 2007; 78:22330.
22. John SW, Weitzner G, Rozen R, Scriver CR. A rapid procedure for
extracting genomic DNA from leukocytes. Nucleic Acids Res 1991;
19:408.
23. Lee LG, Connell CR, Bloch W. Allelic discrimination by nick-
translation PCR with fluorogenic probes. Nucleic Acids Res 1993;
21:37616.
24. Trevilatto PC, Scarel-Caminaga RM, de Brito RB Jr, de Souza AP,
Line SR. Polymorphism at position 2174 of IL-6 gene is associatedwith susceptibility to chronic periodontitis in a Caucasian Brazilian
population. J Clin Periodontol 2003; 30:43842.
25. Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visuali-
zation of LD and haplotype maps. Bioinformatics 2005; 21:2635.
26. Fishman D, Faulds G, Jeffery R, et al. The effect of novel poly-
morphisms in the interleukin-6 (IL-6) gene on IL-6 transcription
and plasma IL-6 levels, and an association with systemic-onset juvenile
chronic arthritis. J Clin Invest 1998; 102:136976.
27. Anvari M, Khalilzadeh O, Esteghamati A, et al. Graves disease and
gene polymorphism of TNF-alpha, IL-2, IL-6, IL-12, and IFN-gamma.
Endocrine 2010; 37:3448.
28. Nibali L, Griffiths GS, Donos N, et al. Association between interleukin-
6 promoter haplotypes and aggressive periodontitis. J Clin Periodontol
2008; 35:1938.
29. Nibali L, DAiuto F, Donos N, et al. Association between perio-
dontitis and common variants in the promoter of the interleukin-6
gene. Cytokine 2009; 45:504.
30. Cussigh A, Falleti E, Fabris C, et al. Interleukin 6 promoter poly-
morphisms influence the outcome of chronic hepatitis C. Immu-
nogenetics 2011; 63:3341.
31. Kristiansen OP, Nolse RL, Larsen L, et al. Association of a functional
17 beta-estradiol sensitive IL6-174G/C promoter polymorphism with
early-onset type 1 diabetes in females. Hum Mol Genet 2003; 12:
110110.
32. Gillespie KM, Nolse R, Betin VM, et al. Is puberty an accelerator of
type 1 diabetes in IL6-174CC females? Diabetes 2005; 54:12458.
33. Qi L, van Dam RM, Meigs JB, Manson JE, Hunter D, Hu FB. Genetic
variation in IL6 gene and type 2 diabetes: tagging-SNP haplotype
analysis in large-scale case-control study and meta-analysis. Hum
Mol Genet 2006; 15:191420.
34. Castellucci L, Menezes E, Oliveira J, et al. IL6 -174 G/C promoter
polymorphism influences susceptibility to mucosal but not localized
cutaneous leishmaniasis in Brazil. J Infect Dis 2006; 194:51927.
35. Sobti RC, Berhane N, Mahedi SA, et al. Polymorphisms of IL-6 174
G/C, IL-10 -592 C/A and risk of HIV/AIDS among North Indian
population. Mol Cell Biochem 2010; 337:14552.
36. Torres OA, Calzada JE, Beraun Y, et al. Lack of association between
IL-6-174G/C gene polymorphism and Chagas disease. Tissue Antigens
2010; 76:1314.
37. Guerreiro CS, Ferreira P, Tavares L, et al. Fatty acids, IL6, and TNF
alpha polymorphisms: an example of nutrigenetics in Crohns disease.
Am J Gastroenterol 2009; 104:22419.
38. Barrett JC, Hansoul S, Nicolae DL, et al. Genome-wide association
defines more than 30 distinct susceptibility loci for Crohns disease.
Nat Genet 2008; 40:95562.
39. Le Bourhis L, Benko S, Girardin SE. Nod1 and Nod2 in innate im-
munity and human inflammatory disorders. Biochem Soc Trans 2007;
35:147984.
40. Morahan G, Kaur G, SinghM, et al. Association of variants in the IL12B
gene with leprosy and tuberculosis. Tissue Antigens 2007; 69(Suppl 1):
2346.
41. Behr MA, Schurr E. Mycobacteria in Crohns disease: a persistent hy-
pothesis. Inflamm Bowel Dis 2006; 12:10004.
42. Fisman EZ, Tenenbaum A. The ubiquitous interleukin-6: a time for
reappraisal. Cardiovasc Diabetol 2010; 9:62.
1424 d JID 2012:205 (1 May) d Sousa et al
by guest on September 2, 2013
http://jid.oxfordjournals.org/D
ownloaded from