IX CURSO DE AVANCES EN - AGIDEIagidei.org/wp-content/uploads/2014/12/cbm-2015-06strinicio.pdf · IX...
36
Javier de la Fuente Aguado S. M. Interna. H. POVISA. Vigo. IX CURSO DE AVANCES EN INFECCIÓN POR VIH Y HEPATITIS VIRALES TERAPIA DEL PACIENTE NAIVE CON UN RÉGIMEN ANTIRRETROVIRAL STR La Coruña 30 y 31 de Enero 2015
Transcript of IX CURSO DE AVANCES EN - AGIDEIagidei.org/wp-content/uploads/2014/12/cbm-2015-06strinicio.pdf · IX...

Javier de la Fuente AguadoS. M. Interna. H. POVISA. Vigo.
IX CURSO DE
AVANCES EN
INFECCIÓN POR VIH
Y HEPATITIS
VIRALES
TERAPIA DEL PACIENTE NAIVE CON UN RÉGIMEN ANTIRRETROVIRAL STR
La Coruña 30 y 31 de Enero 2015

Éxito TAR adherencia
• La adherencia es un factor predictor de:
– Supresión viral mantenida
– Reducción riesgo de desarrollar resistencias
– Menor progresión de infección
– Menor tasa de hospitalización
– Mayor supervivencia

Factores relacionados con la adherencia
complejidad, efectos adversos e interacciones
mala relación médico‐paciente
toxicomanías
enfermedad mental, deterioro neurocognitivo
bajo nivel educativo
barrera idiomática,
falta de apoyo social

STR
STR APROBADOS POR FDA/EMA
EFV/TDF/FTC RPV/TDF/FTC
EVG/COB/TDF/FTCDTG/ABC/3TC

EFV/TDF/FTC
• Comparador habitual
– STARTMRK
– SINGLE
• Eficacia y tolerancia predecibles
• Interrupciones usualmente ligadas a EA
• Dos tercios de las prescripciones en naive

clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
STaR: RPV/TDF/FTC vs EFV/TDF/FTC in Treatment-Naive Pts � Randomized, open-label phase IIIB study
� Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
Treatment naive;HIV-1 RNA > 2500 c/mL;susceptible to EFV, FTC,
RPV, TDF(N = 786)
RPV/TDF/FTC(n = 394)
EFV/TDF/FTC QD(n = 392)
Wk 96Wk 48
Cohen C, et al. AIDS 2014. Abstract WEPE064.

clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
STaR Study: RPV/TDF/FTC Noninferior to EFV/TDF/FTC in Tx-Naive Pts at Wk 96
4.1%-1.1% 9.2%
-0.6% 5.5% 11.5%Wk 96
Wk 48
0-12% 12%
FavorsEFV/TDF/FTC
FavorsRPV/TDF/FTC
Pts
(%
)
Wk 48 Wk 96 Wk 48 Wk 96 Wk 48 Wk 96
Cohen C, et al. AIDS 2014. Abstract WEPE064.
RPV/TDF/FTC (n = 394)
EFV/TDF/FTC (n = 392)
*HIV-1 RNA < 50 copies/mL as defined by FDA Snapshot algorithm.
7.2%1.1% 13.4%
0.2% 7.6% 15.1%Wk 96
Wk 48
All Pts
BL VL ≤ 100,000 c/mL
Wk 96
Wk 48
BL VL > 100,000 c/mL
-11.1% -1.8% 7.5%
-8.7% 11.6%
86 82 7872
8 6 9 6 39
3.511.3
100
60
40
20
0
80
Virologic Success* Virologic Failure D/c due to AEs
1.5%
95% CI for Difference
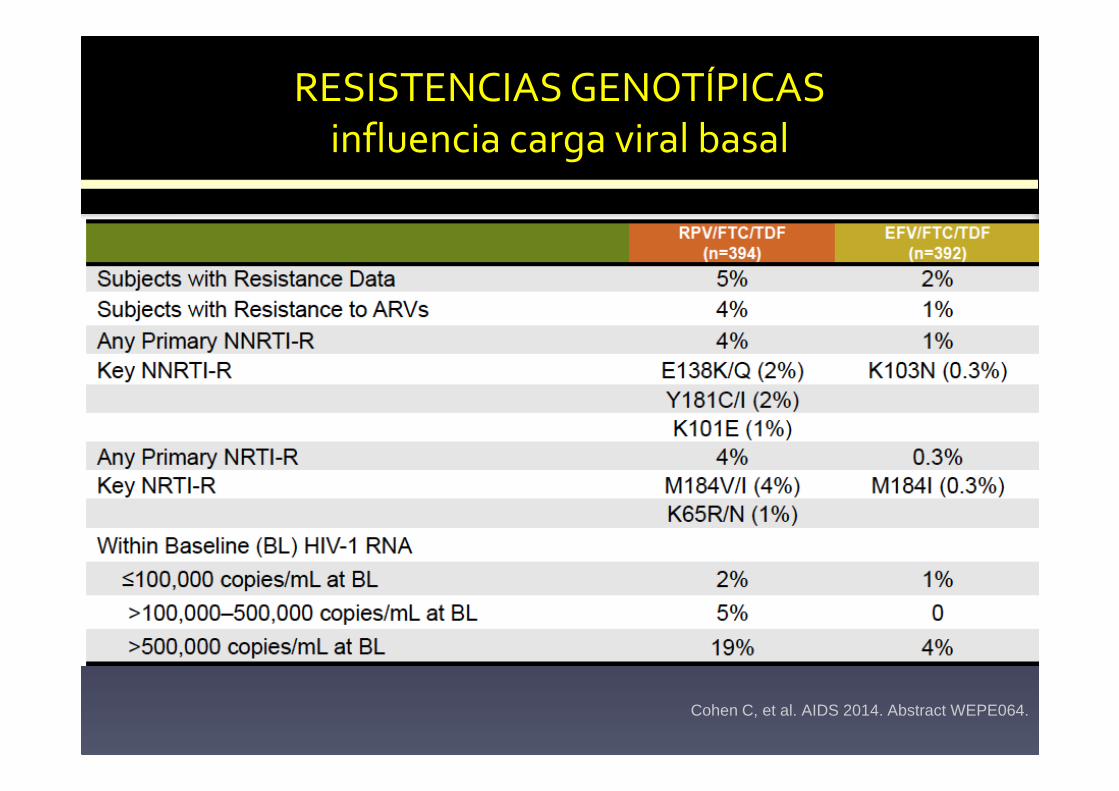
RESISTENCIAS GENOTÍPICAS influencia carga viral basal
Cohen C, et al. AIDS 2014. Abstract WEPE064.
clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
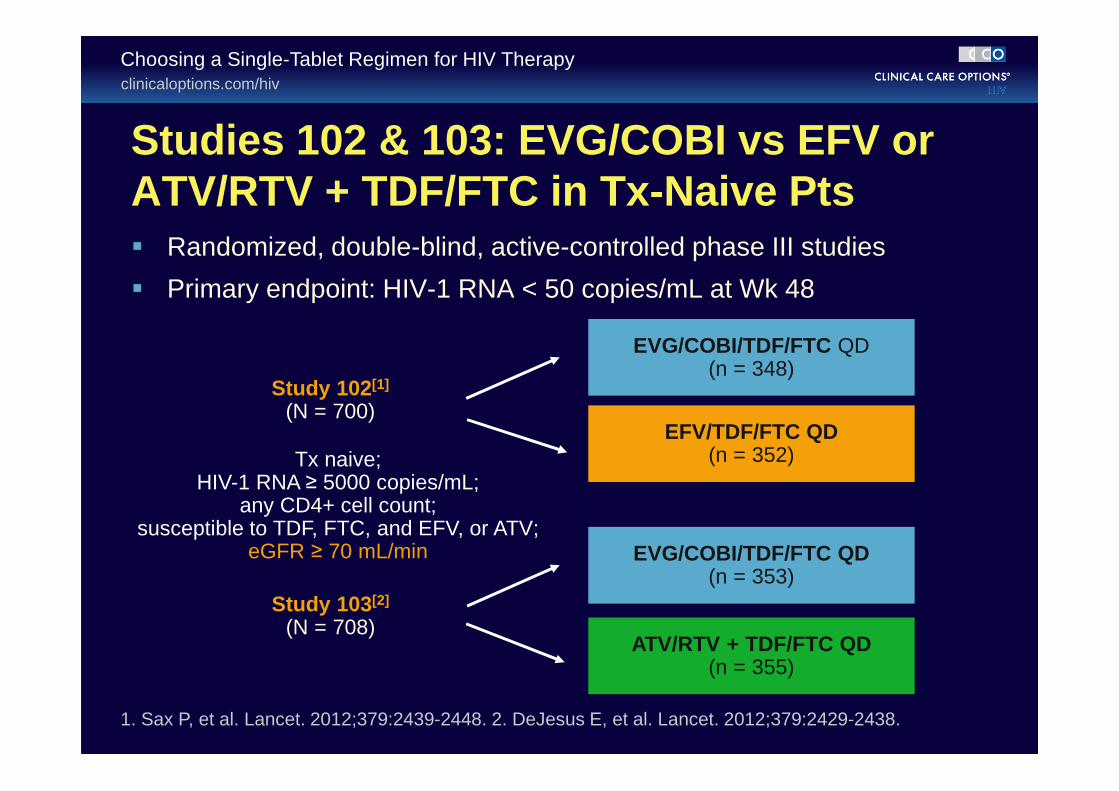
Studies 102 & 103: EVG/COBI vs EFV or ATV/RTV + TDF/FTC in Tx-Naive Pts� Randomized, double-blind, active-controlled phase III studies
� Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
1. Sax P, et al. Lancet. 2012;379:2439-2448. 2. DeJesus E, et al. Lancet. 2012;379:2429-2438.
Tx naive;HIV-1 RNA ≥ 5000 copies/mL;
any CD4+ cell count;susceptible to TDF, FTC, and EFV, or ATV;
eGFR ≥ 70 mL/min
Study 102[1]
(N = 700)
Study 103[2]
(N = 708)
EVG/COBI/TDF/FTC QD(n = 348)
EFV/TDF/FTC QD(n = 352)
EVG/COBI/TDF/FTC QD(n = 353)
ATV/RTV + TDF/FTC QD(n = 355)

clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
1. Sax PE, et al. Lancet. 2012;379:2439-2448. 2. Zolopa A, et al. J Acquir Immune Defic Syndr. 2013;63:96-100. 3. Wohl D, et al. ICAAC 2013. Abstract H-672a.
Wk 48 144
EVG/COBI/TDF/FTC (n = 348)
EFV/TDF/FTC (n = 352)
8075
Pts
(%
)
8884 8482
96
7 7 6 8 7 104 5 5
7 6 7
48 14496 48 14496
Virologic Success* Virologic Failure D/c due to AEs
95% CI for Difference
Wk 48[1]
Wk 96[2]
Wk 144[3]
-12% 12%0
Favors EFV
Favors EVG/COBI
-1.3% 11.1%
4.9%
3.6%
8.8%2.7%
-1.6%
-2.9%
*HIV-1 RNA < 50 copies/mL as defined by FDA Snapshot algorithm.
Study 102: EVG/COBI/TDF/FTC Noninferior to EFV/TDF/FTC in Tx-Naive Pts to Wk 144
8.3%
0
20
40
60
80
100

clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
1. De Jesus E, et al. Lancet. 2012;379:2429-2438. 2. Rockstroh J, et al. J Acquir Immune Defic Syndr. 2013;62:483-486. 3. Clumeck N, et al. EACS 2013. Abstract LBPS7/2.
ATV/RTV + TDF/FTC (n = 355)
78 75
90 87
Wk 48 1440
20
40
60
80
100
96 48 14496 48 14496
83 82
5 5 47 7 78 5 4 6 6 9
Favors ATV/RTV
Favors EVG/COBI
-3.2% 9.4%
3.1%
2.7%
7.5%1.1%
6.7%
-2.1%
-4.5%
95% CI for DifferenceEVG/COBI/TDF/FTC (n = 353)
Pts
(%
)Study 103: EVG/COBI/TDF/FTC Noninferior to ATV/RTV + TDF/FTC in Naive Pts to Wk 144
Virologic Success* Virologic Failure D/c due to AEs
*HIV-1 RNA < 50 copies/mL as defined by FDA Snapshot algorithm.
-12% 12%0
Wk 48[1]
Wk 96[2]
Wk 144[3]

QUAD: EVG/COBI/TDF/FTC

clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
ARIA: Fixed-Dose DTG/ABC/3TC vs ATV/RTV + TDF/FTC in ART-Naive Women� Ongoing, randomized, open-label phase IIIb study
– Primary endpoint: HIV-1 RNA < 50 copies/mL at Wk 48
ART-naive womenHIV-1 RNA ≥ 500 copies/mL
HLA-B*5701 negative(N = 474)
DTG/ABC/3TC(n = 237)
ATV/RTV + TDF/FTC(n = 237)
Wk 48
ClinicalTrials.gov. NCT01910402.

clinicaloptions.com/hivFinding the Fit With Fixed-Dose Combination Antiretroviral Regimens
SINGLE: DTG + ABC/3TC Superior to EFV/TDF/FTC Through Wk 144
HIV
-1 R
NA
< 5
0 co
pie
s/m
L (%
)
8881
DTG + ABC/3TC (n = 414)
EFV/TDF/FTC(n = 419)
0
20
40
60
80
100
8072
Wk 48 Wk 96
∆ 8.0%(2.3% to 13.8%)
∆ 7.4% (2.5% to 12.3%)
Pappa K, et al. ICAAC 2014. Abstract H-647a.
7163
∆ 8.3%(2.0% to 14.6%)
Wk 144
All Pts HIV-1 RNA (c/mL)
CD4+ Cell Count(cells/mm3)
204/280
185/288
92/134
80/131
262/357
230/357
34/57
35/62
≤ 100,000 > 100,000 > 200 ≤ 200
HIV
-1 R
NA
< 5
0 co
pie
s/m
L (%
)
0
20
40
60
80
100
7364 69
61
7364
60 56

clinicaloptions.com/hivFinding the Fit With Fixed-Dose Combination Antiretroviral Regimens
DHHS and IAS-USA Guidelines: 2014 Recommended Regimens for First-line ART
1. DHHS Guidelines. May 2014. 2. Günthard HF, et al. JAMA. 2014;312:410-425.
Class
DHHS[1]
IAS-USA[2]Regardless of BL VL or CD4+ Count
Pts With Pre-ARTVL < 100,000 c/mL
NNRTI � EFV/TDF/FTC � EFV + ABC/3TC*� RPV/TDF/FTC�
� EFV/TDF/FTC or� EFV + ABC/3TC*‡ or� RPV/TDF/FTC‡
Boosted PI � ATV/RTV + TDF/FTC � DRV/RTV + TDF/FTC
� ATV/RTV + ABC/3TC* � ATV/RTV + TDF/FTC or� ATV/RTV + ABC/3TC*‡
� DRV/RTV + TDF/FTC
INSTI � RAL + TDF/FTC � EVG/COBI/TDF/FTC║
� DTG + ABC/3TC*§
� DTG + TDF/FTC
� RAL + TDF/FTC � EVG/COBI/TDF/FTC║
� DTG + ABC/3TC*§
� DTG + TDF/FTC
*Only for pts who are HLA-B*5701 negative. �Only for those with CD4+ cell counts > 200 cells/mm3.‡Not recommended in pts with baseline HIV-1 RNA > 100,000 copies/mL.║Only for pts with pre-ART CrCl > 70 mL/min.§Publication of these guidelines preceded the availability of DTG/ABC/3TC as a single-tablet regimen.


Combinaciones de TAR de inicio recomendadas Documento de consenso de GeSida/PNS sobre TAR
(enero 2015)
PREFERENTES
INI
ABC/3TC+DTG
TDF/FTC+DTG
TDF/FTC+RAL
ALTERNATIVAS
INNTITDF/FTC/EFV
TDF/FTC/RPV
INIABC/3TC + RAL
TDF/FTC/EVG/COBI
IP/rTDF/FTC+DRV/r o DRV/COBITDF/FTC+ATV/r o ATV/COBIABC/3TC+ATV/r o ATV/COBI

Combinaciones de TAR de inicio recomendadas Documento de consenso de GeSida/PNS sobre TAR
(enero 2015)
PREFERENTES
INI
ABC/3TC+DTG
TDF/FTC+DTG
TDF/FTC+RAL
ALTERNATIVAS
INNTITDF/FTC/EFV
TDF/FTC/RPV
INIABC/3TC + RAL
TDF/FTC/EVG/COBI
IP/rTDF/FTC+DRV/r o DRV/COBITDF/FTC+ATV/r o ATV/COBIABC/3TC+ATV/r o ATV/COBI

Global (11)
Adherencia
2.9% (1%-4,8%)
CV<50
2,2% (-1.2% – 2.5%)
Global (11)
Adherencia
2.9% (1%-4,8%)
CV<50
2,2% (-1.2% – 2.5%)
Naives (5)
1927 pacientes
Adherencia
4,4%
(1,8%-7%)
RV
5,7%
(0,7%-10,8%)
Pretratados (6)
1102 pacientes
Adherencia
1%
(-0,8%-2.8%)
RV
-0,7%
(-5,3-3.8%)
Parienti et al. Clin Infect Dis 2009Nachega et al. Clin Infect Dis 2014


clinicaloptions.com/hiv
Choosing a Single-Tablet Regimen for HIV Therapy
Summary: Observational Studies of STRs vs Multicomponent RegimensStudy Main Finding
LifeLink Database[1]
(N = 7073)STRs associated with higher rate of adherence and lower risk of hospitalization
Commercially insured US HIV pts[2]
(N = 6938)
Non STRs associated with 1.5 x risk of incomplete dosing; partial adherence associated with increased rate of hospitalization
Quebec Cohort[3]
(N = 4996)Higher proportion of STR pts adherent to therapy; STRs also associated with lower rate of hospitalization and healthcare utilization
VA Cohort[4]
(n = 15,602)STRs associated with significantly better adherence, lower hospitalization rate
CANOC Cohort[5]
(N = 2965)RAL + 2 NRTIs had lower risk of discontinuation vs EFV/TDF/FTC
� Limitation: cannot control for all factors leading to selection of STRs that may also be associated with good outcomes (first-line regimens, lack of psychiatric disease/substance abuse, provider-perceived good adherence, low risk of resistance)
1. Sax PE, et al. PLoS One. 2012;7:e31591. 2. Cohen C, et al. J Int AIDS Soc. 2012;56(suppl 4):18060. Abstract P1. 3. Lachaine J, et al. ICAAC 2013. Abstract H-663. 4. Rao GA, et al. ICAAC 2013. Abstract H-1464. 5. Machouf N, et al. IAC 2014. Abstract WEPDB0103.

Tasas de no adherencia total o selectivaEFECTO DE RÉGIMEN TAR
Cohen C, et al. HIV11; Glasgow, Scotland; November 11-15, 2012; Abst. P001.

0
20
40
60
80
100
STR IP INNTI INI
NO ADH SELECTIVA NO ADH CD4 > 500 CV < 50
COMPACT STUDYNo adherencia selectiva
Antinori et al. JIAS 2012

No adherencia selectiva‐completa RIESGO DE HOSPITALIZACIÓN
Cohen C, et al. HIV11; Glasgow, Scotland; November 11-15, 2012; Abst. P001.
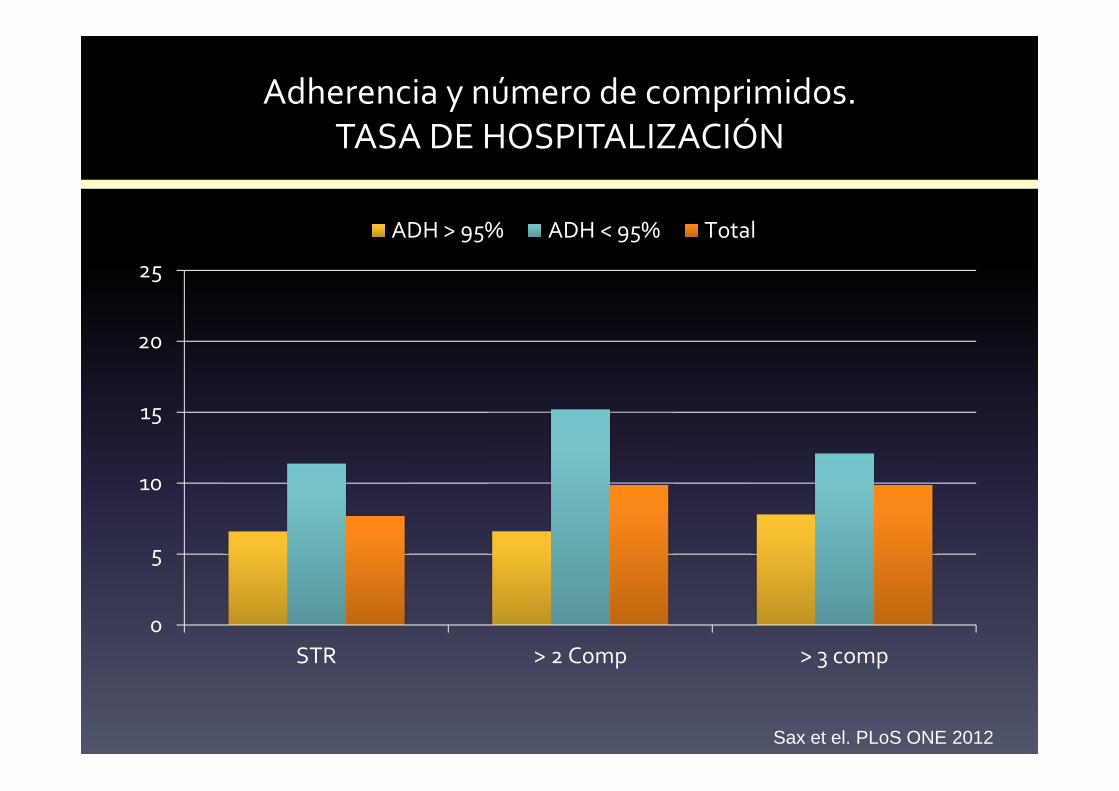
Adherencia y número de comprimidos.TASA DE HOSPITALIZACIÓN
0
5
10
15
20
25
STR > 2 Comp > 3 comp
ADH > 95% ADH < 95% Total
Sax et el. PLoS ONE 2012

Impacto clínico de no adherencia
Cohen C, et al. HIV11; Glasgow, Scotland; November 11-15, 2012; Abst. P001.

Blanco et al. AIDS 2014

STR y QoLPreferencia del paciente
Airoldi et al. Patient Preference and Adherence 2010

Persistencia STR vs MTR
Sweet et al. JIAS 2014

Persistencia diferentes STR y MTR
Sweet et al. JIAS 2014

SSSSingleingleingleingle TTTTablet ablet ablet ablet RRRRegimenegimenegimenegimen
Reducir número comprimidos
Frecuencia de las tomas
Evitar interferencias o restricciones alimenticias
Disminuir las interacciones
Reducir o eliminar efectos secundarios
Errores prescripción o interpretación
Impide toma selectiva
Reducir costes económicos

SSSSingleingleingleingle TTTTablet ablet ablet ablet RRRRegimenegimenegimenegimen
LIMITACIONESLIMITACIONESLIMITACIONESLIMITACIONES ACTUALESACTUALESACTUALESACTUALES
Dosis fijas No permite ajustes de fármacos(Peso, FG, IM..)
Interacciones Citocromo p450
Único combo (FTC/TDF) de INTI Limitaciones de uso en pacientes con nefropatía y EMO
Precio frente a genéricos
Potencia viral o umbral de resistencia en CV elevadas
Toma de IBP o antiácidos ycationes divalentes
RPV, DTG, EVG

FUTURO INMEDIATO
• DGV/ABC/3TC
• TAF/FTC/EVG/COB
• TAF/FTC/DRV/COB
• EFV/ABC/3TC

STR TRATAMIENTO RECOMENDADO EN NAIVE
Class
DHHS[1]
IAS-USA[2]Regardless of
BL VL or CD4+ CountPts With Pre-ARTVL < 100,000 c/mL
NNRTI � EFV/TDF/FTC � EFV + ABC/3TC*� RPV/TDF/FTC�
� EFV/TDF/FTC or� EFV + ABC/3TC*‡ or� RPV/TDF/FTC‡
Boosted PI � ATV/RTV + TDF/FTC � DRV/RTV + TDF/FTC
� ATV/RTV + ABC/3TC* � ATV/RTV + TDF/FTC or� ATV/RTV + ABC/3TC*‡
� DRV/RTV + TDF/FTC
INSTI � RAL + TDF/FTC � EVG/COBI/TDF/FTC║
� DTG + ABC/3TC*§
� DTG + TDF/FTC
� RAL + TDF/FTC � EVG/COBI/TDF/FTC║
� DTG + ABC/3TC*§
� DTG + TDF/FTC
*.