IVIG-mediated protection against necrotizing pneumonia ... · INFECTIOUS DISEASE IVIG-mediated...
14
INFECTIOUS DISEASE IVIG-mediated protection against necrotizing pneumonia caused by MRSA Binh An Diep, 1 * † Vien T. M. Le, 1† Cedric Badiou, 2,3 Hoan N. Le, 1 Marcos Gabriel Pinheiro, 1,4 Au H. Duong, 1 Xing Wang, 1 Etyene Castro Dip, 1 Fábio Aguiar-Alves, 1,4 Li Basuino, 1 Helene Marbach, 1 Thuy T. Mai, 1 Marie N. Sarda, 5 Osamu Kajikawa, 6 Gustavo Matute-Bello, 6 Christine Tkaczyk, 7 Jean-Philippe Rasigade, 2,3 Bret R. Sellman, 7 Henry F. Chambers, 1 Gerard Lina 2,3 * New therapeutic approaches are urgently needed to improve survival outcomes for patients with necrotizing pneu- monia caused by Staphylococcus aureus. One such approach is adjunctive treatment with intravenous immunoglobulin (IVIG), but clinical practice guidelines offer conflicting recommendations. In a preclinical rabbit model, prophylaxis with IVIG conferred protection against necrotizing pneumonia caused by five different epidemic strains of community- associated methicillin-resistant S. aureus (MRSA) as well as a widespread strain of hospital-associated MRSA. Treatment with IVIG, either alone or in combination with vancomycin or linezolid, improved survival outcomes in this rabbit model. Two specific IVIG antibodies that neutralized the toxic effects of a-hemolysin (Hla) and Panton-Valentine leukocidin (PVL) conferred protection against necrotizing pneumonia in the rabbit model. This mechanism of action of IVIG was un- covered by analyzing loss-of-function mutant bacterial strains containing deletions in 17 genes encoding staphylococcal exotoxins, which revealed only Hla and PVL as having an impact on necrotizing pneumonia. These results demonstrate the potential clinical utility of IVIG in the treatment of severe pneumonia induced by S. aureus. INTRODUCTION Community-associated pneumonia caused by methicillin-resistant Staphylococcus aureus (MRSA) has been reported worldwide (1). The best treatment for this potentially life-threatening infection has not been clearly defined. Controversies persist among national clinical guidelines on the treatment of severe community-associated MRSA pneumonia. Intra- venous immunoglobulin (IVIG), which contains pooled human polyclonal antibodies that neutralize lung-damaging toxins produced by MRSA (2), is recommended as adjunctive therapy for treatment of severe community- associated MRSA pneumonia by the U.K. and Canadian clinical practice guidelines (3, 4). In contrast, IVIG is not routinely recommended by the Infectious Diseases Society of America (IDSA) clinical practice guidelines because empirical evidence supporting its use is lacking (5). Current use of IVIG for the treatment of community-associated MRSA pneumonia is supported only by in vitro data showing that it con- tains antitoxin antibodies (2) and by anecdotal case reports (6–9). Ran- domized clinical trials to test the efficacy of IVIG as adjunctive therapy may be impractical because community-associated MRSA necrotizing pneumonia occurs sporadically and is rapidly fatal; moreover, it may be unethical to withhold a potentially life-saving intervention for a severe infection with a mortality rate of 30 to 75% (6–9). However, it should be noted that protective effects of IVIG as adjunctive therapy in patients with bacterial sepsis or septic shock have been conflicting, with some clinical trials showing significant reductions in mortality in adults with sepsis when treated with IVIG compared to placebo or no intervention, but this benefit was not observed in trials with low risk of bias or in neonates (10). Direct evidence that IVIG protects against severe pneumonia caused by community- or hospital-associated MRSA strains is needed. Here, we conducted a series of experiments in a rabbit model of S. aureus–induced acute, necrotizing pneumonia to determine whether treatment with IVIG reduced mortality. This model mimics the rapidly fatal course of infection that occurs in humans, including severe hypox- emia, leukopenia, lung necrosis, pulmonary edema, alveolar hemorrhage, hemoptysis, and death ( 11). Rabbits are similar to humans in their exquisite sensitivity to two key lung-damaging staphylococcal toxins, a-hemolysin (Hla) and Panton-Valentine leukocidin (PVL), whereas other species, in- cluding mouse, rat, and monkey, are resistant to the leukolytic effects of PVL ( 11–13). We found that IVIG improved survival of rabbits infected by each of the major epidemic clones of Hla- and PVL-producing community- associated MRSA, including the North American clone USA300, U.S. Midwest clone USA400, Asian/Pacific clone USA1000, Southwest Pacific clone USA1100, and European/North African clone ST80. IVIG also im- proved survival of rabbits infected with the Hla-producing (but not PVL- producing) hospital-associated MRSA clone USA100 (14). Hla and PVL were shown to be critical for the pathogenesis of necrotizing pneumonia, and small amounts of anti-Hla– and anti-PVL–neutralizing antibodies in IVIG were necessary and sufficient for its protective efficacy in rabbits. RESULTS IVIG-mediated protection against lethal necrotizing pneumonia in a rabbit model The optimal dosage of IVIG for the treatment of community-associated MRSA pneumonia is not clearly defined, although a high-dose IVIG of 2 g/kg is thought to be needed to achieve protective titers because staph- ylococcal toxins are not neutralized as efficiently as streptococcal toxins by IVIG (15). Here, we show that a commercial preparation of human 1 Division of HIV, Infectious Diseases, and Global Medicine, Department of Medicine, Univer- sity of California, San Francisco, San Francisco, CA 94110, USA. 2 INSERM U1111, Université Lyon 1, CNRS UMR5308, ENS Lyon, Lyon, France. 3 Centre National de Référence des Staphylo- coques, Hospices Civils de Lyon, Bron, France. 4 Pathology Program, Fluminense Federal University, Niterói, RJ, Brazil. 5 Laboratory of Immunology, Centre Hospitalier Lyon Sud, Hos- pices Civils de Lyon, Lyon, France. 6 Division of Pulmonary and Critical Care Medicine, De- partment of Medicine, University of Washington School of Medicine, Seattle, WA 98109, USA. 7 Department of Infectious Diseases, MedImmune, LLC, Gaithersburg, MD 20878, USA. *Corresponding author. Email: [email protected] (B.A.D.); [email protected] (G.L.) †These authors contributed equally to this work. RESEARCH ARTICLE www.ScienceTranslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 1 by guest on May 19, 2020 http://stm.sciencemag.org/ Downloaded from
Transcript of IVIG-mediated protection against necrotizing pneumonia ... · INFECTIOUS DISEASE IVIG-mediated...

R E S EARCH ART I C L E
I N FECT IOUS D I S EASE
hD
ownloaded from
IVIG-mediated protection against necrotizingpneumonia caused by MRSABinh An Diep,1*† Vien T. M. Le,1† Cedric Badiou,2,3 Hoan N. Le,1 Marcos Gabriel Pinheiro,1,4
Au H. Duong,1 Xing Wang,1 Etyene Castro Dip,1 Fábio Aguiar-Alves,1,4 Li Basuino,1
Helene Marbach,1 Thuy T. Mai,1 Marie N. Sarda,5 Osamu Kajikawa,6
Gustavo Matute-Bello,6 Christine Tkaczyk,7 Jean-Philippe Rasigade,2,3
Bret R. Sellman,7 Henry F. Chambers,1 Gerard Lina2,3*
New therapeutic approaches are urgently needed to improve survival outcomes for patients with necrotizing pneu-monia caused by Staphylococcus aureus. One such approach is adjunctive treatmentwith intravenous immunoglobulin(IVIG), but clinical practice guidelines offer conflicting recommendations. In a preclinical rabbitmodel, prophylaxis withIVIG conferred protection against necrotizing pneumonia caused by five different epidemic strains of community-associated methicillin-resistant S. aureus (MRSA) as well as a widespread strain of hospital-associated MRSA. Treatmentwith IVIG, either alone or in combinationwith vancomycin or linezolid, improved survival outcomes in this rabbitmodel.Two specific IVIG antibodies that neutralized the toxic effects of a-hemolysin (Hla) and Panton-Valentine leukocidin(PVL) conferred protection against necrotizing pneumonia in the rabbit model. This mechanism of action of IVIG was un-coveredby analyzing loss-of-functionmutant bacterial strains containing deletions in 17genes encoding staphylococcalexotoxins, which revealed only Hla and PVL as having an impact on necrotizing pneumonia. These results demonstratethe potential clinical utility of IVIG in the treatment of severe pneumonia induced by S. aureus.
ttp
by guest on May 19, 2020://stm
.sciencemag.org/
INTRODUCTION
Community-associated pneumonia caused by methicillin-resistantStaphylococcus aureus (MRSA) has been reported worldwide (1). Thebest treatment for this potentially life-threatening infection has not beenclearly defined. Controversies persist among national clinical guidelineson the treatmentof severe community-associatedMRSApneumonia. Intra-venous immunoglobulin (IVIG), which contains pooled human polyclonalantibodies that neutralize lung-damaging toxins produced byMRSA (2),is recommended as adjunctive therapy for treatment of severe community-associatedMRSA pneumonia by theU.K. andCanadian clinical practiceguidelines (3, 4). In contrast, IVIG is not routinely recommended by theInfectious Diseases Society of America (IDSA) clinical practice guidelinesbecause empirical evidence supporting its use is lacking (5).
Current use of IVIG for the treatment of community-associatedMRSApneumonia is supportedonly by in vitro data showing that it con-tains antitoxin antibodies (2) and by anecdotal case reports (6–9). Ran-domized clinical trials to test the efficacy of IVIG as adjunctive therapymay be impractical because community-associatedMRSAnecrotizingpneumonia occurs sporadically and is rapidly fatal; moreover, it may beunethical to withhold a potentially life-saving intervention for a severeinfectionwith amortality rate of 30 to 75% (6–9). However, it should benoted that protective effects of IVIGas adjunctive therapy inpatientswithbacterial sepsis or septic shock have been conflicting, with some clinicaltrials showing significant reductions in mortality in adults with sepsis
1Division of HIV, Infectious Diseases, and Global Medicine, Department of Medicine, Univer-sity of California, San Francisco, San Francisco, CA 94110, USA. 2INSERM U1111, UniversitéLyon 1, CNRS UMR5308, ENS Lyon, Lyon, France. 3Centre National de Référence des Staphylo-coques, Hospices Civils de Lyon, Bron, France. 4Pathology Program, Fluminense FederalUniversity, Niterói, RJ, Brazil. 5Laboratory of Immunology, Centre Hospitalier Lyon Sud, Hos-pices Civils de Lyon, Lyon, France. 6Division of Pulmonary and Critical Care Medicine, De-partment of Medicine, University of Washington School of Medicine, Seattle, WA 98109,USA. 7Department of Infectious Diseases, MedImmune, LLC, Gaithersburg, MD 20878, USA.*Corresponding author. Email: [email protected] (B.A.D.); [email protected] (G.L.)†These authors contributed equally to this work.
www.ScienceTra
when treated with IVIG compared to placebo or no intervention, but thisbenefit was not observed in trialswith low risk of bias or in neonates (10).Direct evidence that IVIG protects against severe pneumonia caused bycommunity- or hospital-associated MRSA strains is needed.
Here, we conducted a series of experiments in a rabbit model of S.aureus–induced acute, necrotizing pneumonia to determine whethertreatment with IVIG reduced mortality. This model mimics the rapidlyfatal course of infection that occurs in humans, including severe hypox-emia, leukopenia, lung necrosis, pulmonary edema, alveolar hemorrhage,hemoptysis, anddeath (11). Rabbits are similar tohumans in their exquisitesensitivity to two key lung-damaging staphylococcal toxins,a-hemolysin(Hla) and Panton-Valentine leukocidin (PVL), whereas other species, in-cludingmouse, rat, andmonkey, are resistant to the leukolytic effects ofPVL (11–13).We found that IVIG improved survival of rabbits infected byeachof themajor epidemic clones ofHla- andPVL-producing community-associated MRSA, including the North American clone USA300, U.S.Midwest cloneUSA400, Asian/Pacific cloneUSA1000, Southwest Pacificclone USA1100, and European/North African clone ST80. IVIG also im-proved survival of rabbits infected with theHla-producing (but not PVL-producing) hospital-associated MRSA clone USA100 (14). Hla and PVLwere shown to be critical for the pathogenesis of necrotizing pneumonia,and small amounts of anti-Hla– and anti-PVL–neutralizing antibodies inIVIG were necessary and sufficient for its protective efficacy in rabbits.
RESULTS
IVIG-mediated protection against lethal necrotizingpneumonia in a rabbit modelThe optimal dosage of IVIG for the treatment of community-associatedMRSA pneumonia is not clearly defined, although a high-dose IVIG of2 g/kg is thought to be needed to achieve protective titers because staph-ylococcal toxins are not neutralized as efficiently as streptococcal toxinsby IVIG (15). Here, we show that a commercial preparation of human
nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 1

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
IVIG, ClairYg, contained antibodies that neutralized the cytotoxic effectsof PVL against human polymorphonuclear leukocytes (PMNs) and Hlaagainst rabbit red blood cells (Fig. 1,A toE). Twodifferent lots ofClairYgexhibited similar neutralizing activities against PVL (Fig. 1, B andC) andHla (Fig. 1E).
A pharmacokinetic study in rabbits further showed that intravenousadministration of 1/10 of the recommended human dose, 200 mg/kg, ofIVIG achieved serum concentrations of 3.4 ± 1.0 mg/ml at 2 hours and1.8 ± 0.1mg/ml at 48 hours after dosing. These concentrationswere three-to sixfold higher than 0.5 mg/ml of IVIG that was sufficient to neutralizethe cytotoxic effects of PVL and Hla in vitro (Fig. 2, A to C).
To evaluate the protective efficacy of IVIG, either alone or in com-bination with vancomycin, which is recommended in clinical practiceguidelines as a first-line agent for the treatment of MRSA pneumonia(3–5), rabbits were randomized for treatment with (i) saline; (ii) vanco-mycin (30 mg/kg, twice daily), a dosing regimen that yields peak serumconcentrations of 36.1 ± 4.2 mg/ml at 1 hour after dosing (16); (iii) IVIG(200 mg/kg) alone; or (iv) an IVIG + vancomycin combination, which
www.ScienceTra
was administered at 1.5 hours postinfection (hpi) with the USA300/SF8300 epidemic clone of community-associated MRSA in the rabbitmodel of necrotizing pneumonia (11). Overall survival rateswere 7% foranimals treated with saline, compared to 7% for those treated with van-comycin alone (P = 0.23 versus saline by one-sided log-rank test), 50%for those treated with IVIG alone (P = 0.010 versus saline), and 71% forthose treated with the IVIG-vancomycin combination (P < 0.001 versussaline) (Fig. 2D).Animals treatedwith the IVIG-vancomycin combinationshowed greater survival than those treatedwith IVIG alone (P= 0.14) orvancomycin alone (P<0.001).All infected animals had severe pulmonaryedema, as evidenced by lungwet weight–to–bodyweight (LW/BW) ratiosexceeding the normal range of 4 to 5 for uninfected lungs, althoughthere were no between-group differences (Fig. 2E). A significant reduc-tion in bacterial count in the lungs was observed in animals treated withthe IVIG-vancomycin combination but not IVIG alone or vancomycinalone (Fig. 2F).
Linezolid, a protein synthesis inhibitor recommended in clinical prac-tice guidelines as an acceptable alternative to vancomycin for treatment of
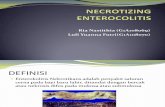
Fig. 1. Human IVIG contains neutralizing antibodies to PVL and Hla.(A) Kinetics of pore formation in human PMNs determined by uptake of propi-
inducedmembranepore formation in response tohuman IVIG,whichwasaddedat the indicated times after PVL was mixed with human PMNs. (E) Two different
dium iodide (PI) in response to the S. aureus toxins LukS-PV and LukF-PV (PVL) atbiologically relevant concentrations (see also Fig. 5G). (B andC) Two different lotsof IVIG {ClairYg lot nos. 11L00258 [IVIG(L8)] and 11L00443 [IVIG(L3)]} blocked PVL-induced pore formation in human PMNs. (D) Kinetics of neutralization of PVL-
lots of IVIG exhibited similar inhibition of rabbit red blood cell lysis in response tovarying concentrations of Hla. Results in (A) to (D) are representative of two in-dependentexperimentswith threehumanblooddonors, and those in (E) are repre-sentativeof three independentexperimentswithasinglebatchof rabbiterythrocytes.
nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 2

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
MRSApneumonia (3–5), has been shown to be superior to vancomycinfor the treatment of necrotizingpneumonia in the rabbitmodel (16).Here,we evaluated the protective efficacy of IVIG alone or in combinationwithlinezolid. Rabbitswere randomized for treatmentwith (i) a negative controlhuman IVIGantibodypreparationdepletedof anti-PVLandanti-Hla anti-bodies (200mg/kg; IVIG-depleted); (ii) linezolid (50mg/kg, three timesdaily), a dosing regimen that yielded a peak serumconcentrationof 10.5±
www.ScienceTra
2.3 mg/ml at 1 hour after dosing (16); (iii) IVIG (200mg/kg) alone; or (iv)an IVIG+ linezolid combination, whichwas administered at 1.5 hpi withtheUSA300/SF8300MRSA strain (11). Overall survival rateswere 0% foranimals treatedwith IVIG-depleted, compared to47%for those treatedwithIVIG alone (P < 0.001 versus IVIG-depleted), 67% for those treatedwith linezolid (P<0.001versus IVIG-depleted), and93% for those treatedwith the IVIG-linezolid combination (P < 0.001 versus IVIG-depleted)
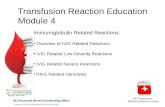
Fig. 2. Human IVIG, either aloneor in combinationwithvancomy-
cin or linezolid, confers protectionin a rabbit model of necrotizingpneumonia. (A) Total human IgG,(B) anti-PVLhuman IgG, and (C) anti-Hla human IgG in the serum of rab-bits takenat the indicated timeafterintravenous administrationofhumanIVIG (200mg/kg). Error bars indicateSEM. AU, arbitrary units. (D) Kaplan-Meiersurvivalcurves, (E)LW/BW(×103)ratio, and (F) bacterial densities, log10(CFU per lung) for animals treated in-travenouslywithIVIG(200mg/kg)onceat1.5hpi (n=14rabbits); vancomycin(30 mg/kg) four times at 1.5, 13, 25,and37hpi (n=15rabbits); IVIG+van-comycin (n = 13 rabbits); or saline at1.5 hpi (n= 14 rabbits) with 5.4 × 109CFU of the SF8300 WT strain. One-sided log-rank (Mantel-Cox) testwasused to test hypothesis that survivalofanimalstreatedwithsalineisshorterthan survival of those treated withIVIG, vancomycin,or thecombinationof IVIG + vancomycin, as well as thehypothesis that survival of animalstreatedwith IVIGaloneorwithvanco-mycin alone is shorter than thosetreated with the combination ofIVIG + vancomycin, with P < 0.010(significance level of 0.05 dividedby five different comparisons) beingconsidered statistically significant toaccount for multiple comparisonsusingBonferronimethod. (G) Kaplan-Meier survival curves, (H) LW/BW(×103) ratio, and (I)bacterialdensities,log10 (CFU/lung) for animals treatedwith IVIG(L3) (200 mg/kg) intra-venously once at 1.5 hpi (n = 15rabbits), linezolid (50 mg/kg) sub-cutaneously four times at 1.5, 10,18, and26hpi (n=15 rabbits), IVIG+linezolid (n = 15 rabbits), or IVIG(200 mg/kg) depleted of anti-HlaIgG and anti-LukS/LukF IgG intra-
venously once at 1.5 hpi (n = 15 rabbits) with 5.3 × 109 CFU of the SF8300 WTstrain. One-sided log-rank (Mantel-Cox) test was used to test the hypothesis thatsurvival of animals treated with saline is shorter than survival of those treatedwith IVIG, linezolid, or the combination of IVIG+ linezolid, aswell as the hypoth-esis that survival of animals treated with IVIG alone or with linezolid alone isshorter than those treated with the combination of IVIG + linezolid, with P <0.010 (significance level of 0.05 dividedby five different comparisons) being con-sideredstatisticallysignificant toaccount formultiplecomparisonsusingBonferronimethod. (E andH) LW/BW (×103) ratio and (F and I) bacterial densities, log10 (CFUper lung), for saline-treated animals were compared to those of each of the otherthree treatment groups by nonparametric one-way analysis of variance (ANOVA)with Kruskal-Wallis test followed by Dunn’s multiple comparisons test. Filledsymbols representdata fromdeadanimals, andopensymbols representdata fromsurviving animals that were euthanized at 48 hpi (E and F) or 96 hpi (H and I).
nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 3

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
(Fig. 2G). Animals treated with the IVIG-linezolid combination showed greater sur-vival than those treated with IVIG alone(P = 0.003) or linezolid alone (P = 0.037by one-sided log-rank test), although thelatter was not statistically significant be-cause the Bonferroni-corrected significancethreshold after accounting for multiplecomparisons was 0.01 (Fig. 2G). The var-ious treatmentmodalities did not have anyeffect on LW/BW ratios (Fig. 2H), sug-gesting that IVIG and/or linezolid did notreduce acute lung injury when comparedto LW/BW ratios for the IVIG-depletedcontrol, although theyprevented respiratorydysfunction and death to at least 96 hpi(Fig. 2G). Consistent with our previousfindings in the same rabbit model that line-zolid reduced bacterial counts in lungs of
Fig. 3. Prophylaxis with IVIG protectsagainst lethalnecrotizingpneumoniacaused
by five clinical community-associatedMRSAstrains. Eight rabbits per experimental groupwere randomized to receive either saline orIVIG(L8)/IVIG(L3) (200 mg/kg) at 24 hoursbefore infection (hbi) with 5.8 × 109 CFU ofUSA300/SF8300 (A to C), 5.7 × 109 CFU ofUSA400 (D to F), 1.5 × 109 CFU of USA1000(G to I), 6.3 × 109 CFU of USA1100 (J to L), and6.8 × 109 CFU of ST80 (M to O). One rabbitrandomized for prophylaxis with IVIG(L3) hadanesthesia-related death before challengewith the ST80 strain (M to O). Kaplan-Meiersurvival curveswere comparedwith one-sidedlog-rank (Mantel-Cox) test to evaluate the hy-pothesis that survival of animals pretreatedwith saline is shorter than survival of thosepretreated with IVIG, with P < 0.05 being con-sidered statistically significant. LW/BW ratioand log10 (CFU per lung) for saline-pretreatedanimals were compared to those pretreatedwith IVIG by nonparametric Mann-WhitneyU test. Filled symbols represent data fromdead animals, and open symbols representdata from surviving animals that were eutha-nized at 48 hpi.www.ScienceTranslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 4

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
infected animals (16), linezolid, whenadministered either alone or in combina-tion with IVIG at 1.5 hpi, also significant-ly reduced log10 [colony-forming unit(CFU) per lung] (P < 0.001; Fig. 2I).
To further test whether prophylaxiswith IVIG protected against necrotizingpneumonia, IVIG (200 mg/kg) was ad-ministered 24 hours before challengewith notonlyUSA300/SF8300butalso fourother community-associated MRSAstrains: USA400/MW2, USA1000,USA1100, and ST80 (Fig. 3). Comparedwith saline control, prophylaxis withIVIG resulted in a statistically significantmortality reduction of 63% for challengewithUSA300/SF8300 (P= 0.022 by one-sided log-rank test; Fig. 3,A toC), 75%forUSA400/MW2 (P = 0.003; Fig. 3, D to F),50% forUSA1000 (P=0.013; Fig. 3, G to I),75% forUSA1100 (P=0.001; Fig. 3, J to L),and 63% for strain ST80 (P < 0.001; Fig. 3,MtoO).Preexposureprophylaxis or post-exposure treatment with IVIG [Figs. 2 (F
and I) and 3 (C, F, I, and O)] did not influence bacterial count in thelungs of animals challenged with USA300/SF8300, USA400, USA1000,and ST80 (the exception being that IVIG resulted in a reduction in bac-www.ScienceTra
terial count in the lungs of animals challenged with USA1100; Fig. 3L).These data suggested that the mechanism of action of IVIG-mediatedprotection was not due to enhanced opsonophagocytic killing.
Fig. 4. Effects of major staphylococcalexotoxins in acute lung injury. Comparison
of (A to C) LW/BW (×103) and (D to F) log10CFU per lung for rabbits (n = 9 animals perexperimental group) euthanized at 9 hpiwithSF8300 WT or isogenic mutants containingdeletion of genes encoding PVL (DlukSF),Dpsm-a,Dhla,DhlgABC,DlukED,DlukGH (alsoknown as leukocidin A and B), Dseq/sek, andDselx. (G to J) Concentrationsof IL-8 andMCP-1 in the lungs and plasma of rabbits eutha-nizedat9hpiwithSF8300WT,orDpsm-a,Dhla,andDlukSFmutant strains.Nonparametric one-wayANOVAwith Kruskal-Wallis test followedbyDunn’smultiplecomparisonstestwereusedto evaluate differences betweenWT and eachof the mutant strains. (K) Photographs depictgross pathology of representative lungs har-vested from rabbits at 9 hpi with the four iso-genic SF8300 strains: WT, Dpsm-a, Dhla, andDlukSFmutant strains.nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 5

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
Characterization of the relative contributions of toxinsin the pathogenesis of community-associatedMRSA pneumoniaIn clinical settings, IVIG (1000 to 2000mg/kg) is typically used becausethis high-dose regimen is needed to exert an anti-inflammatory responsein the patient. Because even a low-dose regimen of IVIG (200 mg/kg)was protective in the rabbit pneumonia model, it seemed unlikely thatIVIG’s protective effect involved dampening of acute lung inflammation.Instead, on thebasis of our data (Fig. 1) andother in vitro studies (2,15,17),themechanismof IVIG-mediatedprotection seemed tobedue to thepres-ence of specific antibodies in IVIG that neutralized some of the toxinsproducedby S. aureus.One approach todetermine themechanismofpro-tection would be to affinity-purify the different antitoxin antibodies fromIVIG and evaluate individual protective effects of each specific antibodypreparation in the rabbit model. However, this approach would be costprohibitive because S. aureus produces many toxins. Thus, we took agenetic approach to systematically characterize those toxins that havebeen implicated in S. aureusnecrotizing pneumonia in our rabbitmodelto identify those that were most potent. Then, we evaluated whetheraffinity-purified antibodies that neutralized those specific toxins wereprotective in our rabbit model.
In-frame deletions of 17 different genes at eight different chromo-somal loci that encode staphylococcal exotoxins were constructed in aUSA300/SF8300 clinical strain (tables S1 and S2). Although these toxingenes have demonstrated roles in disease pathogenesis in one or moreanimal models, only the PVL mutant has been shown previously to beseverely attenuated in the New Zealand white rabbit model of necrotiz-ing pneumonia (11). In this rabbit model, deletion of the gene encodingPVL (DlukSF) or Dhla attenuated the capacity of the mutant bacteria tocause acute lung injury at 9 hpi, as evidenced by significantly decreasedLW/BW ratios (P < 0.001; Fig. 4A). In contrast, deletion of genes en-coding phenol-soluble modulin a types 1 to 4 (Dpsm-a), g-hemolysin(DhlgABC), leukocidin E andD (DlukED), leukocidinG andH (DlukGH)(also known as leukocidin A and B), staphylococcal enterotoxin Q and K(Dseq/sek), and staphylococcal enterotoxin-likeX (DselX) did not result insignificant reduction in LW/BW ratios (Fig. 4, A to C). Bacterial countsin lungs of animals at 9 hpiwith the SF8300wild-type (WT) strain did notdiffer from those infectedwith any of the othermutant strains (Fig. 4, D toF). Lungs of animals infected with Dhla and DlukSFmutants were grosslydifferent from those infected with the SF8300 WT parental strain, withextensive areas of necrosis and severe pulmonary edema (Fig. 4K). Com-pared to the SF8300 WT parental strain, the Dpsm-a, Dhla, and DlukSFmutants provoked a reduction in interleukin-8 (IL-8) in rabbit lungs (Fig.4G), which resulted in a concomitant reduction in leakage of IL-8 into theblood (Fig. 4H). In contrast, only theDlukSFmutant, but notDpsm-a andDhla mutants, provoked a reduction in monocyte chemotactic protein1 (MCP-1) (Fig. 4, I and J). Reduced IL-8 in rabbit lungs and bloodhas been shown previously to result in a reduced influx of neutrophils,which are known to play a central role in mediating acute lung injuryand inflammation in the rabbit pneumonia model (11).
Consistentwith their reduced capacity to cause acute lung injury, theDhla mutant, the DlukSF mutant, as well as the DhlaDlukSF doublemutant caused significantly lower mortality rates compared to the SF8300WTparental strain (P=0.007 andP<0.001; Fig. 5A).TheDpsm-amutantalso exhibited reduced capacity to cause lethal infection compared toSF8300WT, althoughP= 0.024 by one-sided log-rank test is considerednot statistically significant using the Bonferroni-corrected significancethreshold of 0.0125 to account for multiple comparisons. The attenuated
www.ScienceTra
virulence of the DlukSF and DhlaDlukSF was evident also in the signifi-cantly reducedLW/BWratio and bacterial counts in lungs (all significant,P < 0.01; Fig. 5, B and C).
Because SElXwas previously shown to be important in anAmericanDutch belted rabbit pneumonia model (18) using the USA300/LACstrain, we constructed an in-frame deletion of the selx gene in this strainand then compared survival of animals infectedwith the isogenic strainsin ourNewZealandwhite rabbitmodel of necrotizing pneumonia. No dif-ference in mortality was observed between the LAC WT and LACDselxmutant (fig. S1, A toD), which is consistentwith the lack of any differencesin acute lung injury at 9 hpi with SF8300WTand SF8300Dselx (Fig. 4C)in our rabbitmodel. The discrepancies between the null result in ourNewZealandwhite rabbitmodel and the positive result in theAmericanDutchbelted rabbitmodel (18) could be due to the use of different rabbit strains,an explanation thatmay be supported by the fact thatmore recent studiesby the same group did not show any differences between USA400/MW2WT and theMW2Dselxmutant in a New Zealand white rabbit model ofinfective endocarditis (19).
Inasmuch as the major clones of community-associated MRSA areknown to up-regulate production of Hla and PVL (20), we comparedhere their pathogenic capacity in the rabbit model and determined theamounts of toxin produced in vivo. USA300, USA1000, USA1100,USA400, and ST80 strains were relatively similar in their capacity tocause rapidly lethal necrotizing pneumonia, with 34 of 35 rabbits chal-lenged with these five strains succumbing to infection (Fig. 5, D to F).The ST80 strain caused more rapidly lethal infection than the USA300/SF8300 strain (P = 0.006 by two-sided log-rank test), although bothstrains caused lethality in 100% of challenged animals (Fig. 5D). Thesecommunity-associatedMRSA clones produced PVL and Hla above theenzyme-linked immunosorbent assay (ELISA) detection limit in 94 and69% of the 35 infected lungs, respectively (Fig. 5, G and H). PVL pro-duction in the lungs varied among the different community-associatedMRSA strains, from a low concentration of 0.53 mg per lung byUSA1000 to a high concentration of 5.07 mg per lung by USA1100(Fig. 5G). Hla production in the lungs also exhibited strain-to-strainvariability, from a low concentration of 0.28 mg per lung by USA400to a high concentration of 3.24 mg per lung by USA1000 (Fig. 5H). Con-centrations of these toxins produced in the lungs of many of the animalsexceeded the toxic concentrations of PVL and Hla produced againstmammalian cell targets in vitro (see Fig. 1, A and E).
Mechanisms of protection by IVIGHaving shown that Hla and PVL are the principal toxins mediating le-thal necrotizing pneumonia in the rabbit model, we next tested whetherthe protective efficacy of IVIG was due to specific antibodies that neu-tralized these toxins. RecombinantHla andPVL subunits, LukS-PVandLukF-PV, were used in affinity column chromatography to selectivelycapture toxin-specific antibodies. Affinity-purified anti–LukS-PV andanti–LukF-PV antibodies neutralized PVL-induced pore formation inneutrophils (fig. S2, A and B), whereas the anti-Hla antibodies neutra-lized Hla-induced lysis of red blood cells (fig. S2C). Because IVIG alsohas anti-inflammatory activities that could confer protection independentof specific antitoxin antibodies, we controlled for this possibility by pre-paring IVIG depleted of its anti–LukS-PV, anti–LukF-PV, and anti-Hlaantibodies throughnegative selectionon affinity columnchromatography.The IVIG-depleted preparation was deficient in its toxin-neutralizingactivity against PVL-induced pore formation in neutrophils and Hla-induced red blood cell lysis (fig. S2, A to C).
nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 6

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
Fig. 5. Staphylococcal necrotizing pneumoniais mediated principally by two toxins, PVL andHla. Comparison of Kaplan-Meier survival curves(A), LW/BW ratio (×103) (B), and log10 CFU per lung(C) for rabbits challengedwith USA300/SF8300WTstrain, or isogenicmutant strainsDpsm-a,Dhla,DlukSF,or thedoublemutantstrainDhlaDlukSF (n=12animalsper experimental group). One-sided log-rank (Mantel-Cox) testwas used to test the hypothesis that survivalof animals challengedwith SF8300WT is shorter thansurvival of thosechallengedwitheachof the fourmu-tant strains Dpsm-a, Dhla, DlukSF, or DhlaDlukSFwithP < 0.0125 (significance level of 0.05 divided by fourdifferent comparisons) being considered statisticallysignificant to account for multiple comparisons usingthe Bonferroni method. Comparison of Kaplan-Meiersurvival curves (D), LW/BW ratio (×103) (E), and log10
www.ScienceTranslationalMedicine.org
CFU per lung (F) of rabbits challenged with WT strains belonging to the epidemic community-associated MRSA strains USA300/SF8300 (ST8), USA400/MW2 (ST1),USA1000 (ST59), USA1100 (ST30), and ST80 (n = 7 animals per experimental group). Amounts of LukS-PV (G) and Hla (H) produced in the lungs of infected animals.Two-sided log-rank (Mantel-Cox) test was used to test the hypothesis that survival of animals challenged with SF8300 WT is not different from survival of thosechallenged with each of the other four community-associated MRSA strains, with P < 0.0125 (significance level of 0.05 divided by four different comparisons) beingconsidered statistically significant toaccount formultiple comparisonsusing theBonferronimethod. The following log-rank testPvalues are for comparisonof SF8300WT versus each of the other community-associatedMRSA strains: P= 0.20 for SF8300 versus USA400, P= 0.19 for SF8300 versus USA1000, P= 0.46 for SF8300 versusUSA1100, and P = 0.006 for SF8300 versus ST80. For both studies, the LW/BW ratio (×103), bacterial densities in lungs, and toxin concentrations in lungs for animalschallenged with SF8300 were compared to each of the four other strains by nonparametric one-way ANOVA with Kruskal-Wallis test followed by Dunn’s multiplecomparisons test. Filled symbols represent data from dead animals, and open symbols represent data from surviving animals that were euthanized at 36 hpi.
21 September 2016 Vol 8 Issue 357 357ra124 7

R E S EARCH ART I C L E
Prophylaxis with affinity-purified anti-LukS/F-PVantibodies (1mg/kg),anti-Hla antibodies (1mg/kg), or IVIG (200mg/kg) demonstrated a similarprotective efficacy in reducing mortality after challenge with the USA300/SF8300 WT strain compared to saline control (Fig. 6, A to C). Using aBonferroni-corrected significance threshold of 0.0125 to account formultiple comparisons, P = 0.010 for saline versus IVIG and P = 0.006
www.ScienceTra
for saline versus anti-Hla immunoglobulin G (IgG), by one-sided log-rank test, were considered statistically significant, whereas P = 0.014 forsaline versus anti-LukF/S IgG was not statistically significant (Fig. 6A).Administration of depleted IVIG (200mg/kg) did not confer significantprotection compared to the saline-treated animals (P=0.12; Fig. 6A). Serafrom animals treated with IVIG exhibited similar neutralization activities
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
tel-Cox) test was used to test the hypothesis that survival of animals pretreatedwith depleted IVIG is shorter than
Fig. 6. Anti-Hla and anti-PVL antibo-dies affinity purified from human IVIG
protect against USA300 community-associated MRSA necrotizing pneumo-nia. Comparisonof Kaplan-Meier survivalcurves (A), LW/BW ratio (×103) (B), andlog10CFUper lung (C) of rabbitspretreatedat 1.5 hours before infectionwith 6.4 × 109CFU of SF8300 WT strain with the fol-lowing regimens: saline (n = 10 rabbits),IVIG(L8) (200mg/kg;n=12 rabbits), IVIG(L8)(200mg/kg) depleted of anti-Hla IgG andanti-LukS/LukF IgG (n = 9 rabbits), anti-Hla IgG (1mg/kg)affinity-purified fromIVIG(n=8 rabbits), anti-LukS IgG (1mg/kg), andanti-LukF IgG(1mg/kg)affinity-purifiedfromIVIG (n = 8 rabbits). One-sided log-rank(Mantel-Cox) testwas used to test the hy-pothesis that survival of animalspretreatedwith saline is shorter than survival of thosepretreatedwitheachof fourantibodyprep-arations,with P < 0.0125 (significance levelof 0.05 divided by four different compari-sons) being considered statistically signifi-cant to account for multiple comparisonsusing the Bonferroni method. LW/BW ratio(×103) and log10 CFU per lung for animalschallenged with SF8300 were comparedto each of the four other strains by non-parametric one-way ANOVAwith Kruskal-Wallis test followed by Dunn’s multiplecomparisons test. Comparison of Kaplan-Meier survival curves (D), LW/BW ratio(×103) (E), and log10 CFU per lung (F) ofrabbits pretreated at 1.5 hours before in-fection with 5.1 × 109 CFU of SF8300 WTwith depleted IVIG(L3) (200 mg/kg) orIVIG(L3) (200mg/kg) (eight rabbits per ex-perimental group). Comparison of Kaplan-Meier survival curves (G), LW/BW ratio(×103) (H), and log10 CFU per lung (I) ofrabbits pretreated at 1.5 hours before in-fection with 5.3 × 109 CFU of SF8300 WTwith depleted IVIG(L3) (200 mg/kg) oranti-Hla IgG (4 mg/kg) (eight rabbits perexperimentalgroup).ComparisonofKaplan-Meier survival curves (J), LW/BW ratio (×103)(K), and log10 CFU per lung (L) of rabbitspretreated at 1.5 hours before infectionwith 5.4 × 109 CFUof SF8300WTwith de-pleted IVIG(L3) (200 mg/kg) or anti-LukS/LukF IgG (4 mg/kg) (eight rabbits per ex-
perimental group). One-sided log-rank (Mansurvival of those pretreated with the other antibody preparations, with P < 0.05 being considered statistically significant. Filled symbols represent data fromdead animals, and open symbols represent data from surviving animals that were euthanized at 48 hpi. LW/BW ratio (×103) and bacterial densities in rabbitlung for the different pairwise comparisons were evaluated with the nonparametric Mann-Whitney U test.nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 8

R E S EARCH ART I C L E
Dow
nlo
to sera fromanimals treatedwith specific antitoxin antibodies in thePVL-induced human neutrophil pore formation assay and the Hla-inducedrabbit red blood cell hemolysis assay (fig. S2, D to F).
To further confirm the mechanisms of IVIG-mediated protectionagainst lethal pneumonia, three additional independent studies wereconducted. Prophylaxis with IVIG (200 mg/kg) resulted in 63% reduc-tion inmortalitywhen compared todepleted IVIG (200mg/kg) (P=0.002by one-sided log-rank test; Fig. 6, D to F). Similarly, prophylaxis with anti-Hla antibodies (4mg/kg) resulted in 88%reduction inmortality (P<0.001byone-sided log-rank test; Fig. 6,G to I) or anti-LukS/F antibodies (4mg/kg)(P < 0.001 by one-sided log-rank test; Fig. 6, J to L) when compared todepleted IVIG (200 mg/kg).
The generalizability of these results on the mechanisms of action ofIVIG was further strengthened by comparing protective efficacies ofIVIG-depleted and IVIG using two additional clinical strains, the lessercommunity-associatedMRSA strainUSA400/MW2 found in theMidwestof the United States (14) and Alaska (21) and the predominantmultidrug-resistant hospital-associated MRSA strain USA100/NRS382 found inhealth care facilities throughout the United States (14). When compared
www.ScienceTra
to IVIG-depleted (200mg/kg), prophylaxiswith IVIG(200mg/kg) resultedin 100% reduction in mortality with the USA400 strain (P < 0.001 byone-sided log-rank test; Fig. 7, A to C) and 50% reduction in mortalitywith theUSA100 strain (P= 0.022; Fig. 7, D andE). Together, these dataindicate that IVIG may protect against lethal infection through its spe-cific antitoxin antibodies.
DISCUSSION
Necrotizing pneumonia caused by community-associated MRSAstrains is associated clinicallywith a rapid andhighmortality rate, despiteappropriate antibiotic treatment (1). There is an urgent need for newtherapeutic approaches that would supplement current antibiotic therapyto improve survival during the acute phase of the infection.Anumber ofcase reports have documented the use of IVIG as an effective adjunct toantimicrobial therapy to treat severe cases of staphylococcal pneumonia(6–9). By demonstrating that IVIG administration protects againstdeath in a rabbit model of necrotizing pneumonia using five different
by guest on May 19, 2020
http://stm.sciencem
ag.org/aded from
Fig. 7. Human IVIGprotects against pneumonia caused by community-associatedMRSA strain USA400 and hospital-associatedMRSA strain
NRS382 WT strain with depleted IVIG(L3) (200 mg/kg) or IVIG(L3) (200 mg/kg)(eight rabbits per experimental group). One-sided log-rank (Mantel-Cox) test
USA100. Comparison of Kaplan-Meier survival curves (A), LW/BW ratio(×103) (B), and log10 CFUper lung (C) of rabbits pretreated at 1.5 hours beforeinfection with 5.5 × 109 CFU of USA400 WT strain with IVIG(L3) (200 mg/kg)depletedof anti-Hla IgGandanti-LukS/LukF IgGor complete IVIG(L3) (200mg/kg)(eight rabbits per experimental group). Comparison of Kaplan-Meier surviv-al curves (D), LW/BW ratio (×103) (E), and log10 CFU per lung (F) of rabbitspretreated at 1.5 hours before infection with 5.6 × 109 CFU of USA100/
was used to test the hypothesis that survival of animals pretreated with de-pleted IVIG is shorter than survival of those pretreated with the other antibodypreparations, with P < 0.05 being considered statistically significant. Filledsymbols represent data from dead animals, and open symbols represent datafrom surviving animals that were euthanized at 96 hpi. LW/BW ratio (×103) andbacterial densities in rabbit lung for the different pairwise comparisons wereevaluated with the nonparametric Mann-Whitney U test.
nslationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 9

R E S EARCH ART I C L E
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
community-associated MRSA clinical strains and one predominanthospital-associatedMRSAclinical strain and by unraveling themechanismof this protective effect, our study provides preclinical evidence that IVIGmay have a role to play in the treatment of severe MRSA pneumonia.
Several hypotheses regarding themechanism of action of IVIG havebeen proposed. Our working hypothesis was that IVIG protects againstMRSA necrotizing pneumonia by neutralizing S. aureus toxins that areinvolved in disease pathogenesis. It was based on previous observationsthat IVIG contains neutralizing antibodies against several S. aureus vir-ulence factors, such as superantigens (22), pore-forming toxins (2, 23),and microbial surface components recognizing adhesive matrix mole-cules (24). Thus, we first attempted to identify which S. aureus virulencefactors may be involved in the rabbit model of necrotizing pneumonia.A comprehensive analysis of the relative contributions of various toxinssecreted by USA300 revealed that only Hla and PVL, and to a lesserextent PSM-a, had a significant impact on acute lung injury and survivaloutcomes in the rabbit model of necrotizing pneumonia (Figs. 4 and 5).Hla and PVL were produced at toxic levels in the lungs of many of therabbits infected with the five major epidemic community-associatedMRSA strains, indicating that they also contributed to the pathogenesisof necrotizing pneumonia caused by not only USA300 but also otherprevalent CA-MRSA clones. Finally, the absence of lethality inducedby the USA300 DhlaDlukSF double mutant confirmed the importanceof these two toxins in the pathogenesis of necrotizing pneumonia (Fig. 5A).
The presence of neutralizing antibodies against Hla and PVL in IVIGwas shown previously (2, 23) and confirmed herein for the two differentbatches of IVIG used in the rabbit studies (Fig. 1, A to E). Pharmaco-kinetic analysis in rabbits indicated that administrationof IVIG (200mg/kg)resulted in serum titers sufficient to neutralize Hla and PVL secreted by thebacteria in rabbit lungs for at least 48hours (Fig. 2,A toC). ProphylaxiswithIVIGreducedmortality compared to saline control in the rabbit pneumoniamodel using five different community-associated MRSA strains thatproduced bothHla and PVL (Fig. 3, A toO). The roles of neutralizing anti-bodies against these two toxins were confirmed by demonstrating thataffinity-purified anti-Hla and anti-PVL antibodies protected against lethalinfection, whereas IVIG depleted of these neutralizing antibodies did notsignificantly improve animal survival [Figs. 2 (G to I), 6 (A to L), and 7 (Ato F)].Given that the bicomponent toxinsPVL (LukSF), LukED,HlgABC,and LukGH/LukAB are antigenically related, we suspect that most anti-bodies against PVL in IVIG could be attributed to previous exposure toone of these toxins, and we cannot rule out possible cross-neutralizationafforded by affinity-purified antibodies.However, itmay have little impactin our rabbit model because the deletion of genes encoding the otherbicomponent toxins did not have a significant impact on acute lung injury(Fig. 4).
Given that the distinctions between community-associated MRSAandhospital-associatedMRSA strains are blurred by cross-transmissionof these strains into and out of health care facilities (25), it was importantto determine whether IVIG also protected against a hospital-associatedMRSA strain. Clinical studies are conflicting as to whether S. aureusstrains with high cytotoxic activities are associated with more severe dis-ease. Rose et al. (26) reported paradoxically that MRSA strains with lowcytotoxic activity were associated with increased mortality rates becauseof nosocomial pneumonia. Stulik et al. (27) reported that higha-hemolysincytotoxic activity was associated with ventilator-associated pneumonia forinfection with methicillin-susceptible S. aureus strains but not MRSAstrains. It is not clear whether the USA100/NRS382 clinical strain usedin our study would be classified as having high or low cytotoxic activity
www.ScienceTran
because this strain belongs to clonal complex 5 that tends to exhibit widevariation in cytotoxicity (26). Nonetheless, the USA100/NRS382 clinicalstrain is representative of the hospital-associated MRSA lineage that iswidespread in health care facilities across the United States (14). In therabbit pneumonia model, USA100/NRS382 caused rapidly fatal pneu-monia in animals administered depleted IVIG, whereas those animalsadministered IVIG had a 50% reduction in overall mortality rate (P <0.022; Fig. 7D), indicating that IVIGprotected against pneumonia causedby not only community-associated MRSA strains but also a hospital-associated MRSA strain.
IVIG has been used clinically for its autoimmune-inhibiting and anti-inflammatory therapeutic effects (28). In the rabbit model of necrotizingpneumonia, it is possible that IVIG-mediated protection was due to itsanti-inflammatory effects that lessened the severity of host-mediatedacute lung injury (11). However, high-dose IVIG, 2 g/kg, is generally re-quired for IVIG’s anti-inflammatory effects, whereas protection in therabbit model of necrotizing pneumonia was achieved using 1/10 of thehuman dose, 200 mg/kg. If there was an anti-inflammatory effect inthe rabbit model, then it was likely to be minimal because 59 of 64(92%) rabbits administered IVIG (200 mg/kg) depleted of anti-Hlaand anti-PVL antibodies did not survive (Figs. 2G, 6 (A, D, G, and J),and 7 (A and D)] compared to a similar mortality rate of 84% (53 of 63)for rabbits administered saline [Figs. 2D, 3 (A, D, G, J, andM), and 6A].
The role of IVIG in enhancing in vitro opsonophagocytic killing of S.aureus has been debated (29–33). Notably, rabbits administered IVIGdepleted of its antitoxin antibodies did not differ in lung bacterial countsfrom those treatedwith saline (Fig. 6C), suggesting that themyriad otherantibodies in IVIG did not enhance in vivo opsonophagocytic killing ofS. aureus. In support of this, six of seven studies inwhich IVIGwas com-pared to saline in the rabbitmodel also showed no significant differencesin lung bacterial counts [Figs. 2F and 3 (C, F, I, andO)], with the exceptionbeing the one study in which rabbits were challenged with the USA1100strain, which yielded mean log10 CFU of 8.39 and 5.52 (P = 0.007) forthose animals pretreated with saline and IVIG, respectively (Fig. 3L). Al-though this exception could be due to IVIG enhancing bacterial killing ofUSA1100 strain, another potential explanation is that IVIG protected allinfected animals fromacute death (Fig. 3J), thereby allowing those animalsthat lived longer a correspondingly greater period of time for clearance ofbacteria from the lungs (Fig. 3L). Accordingly, the two USA1100-infectedrabbits, which were treated with saline and survived, also had fewer lungbacterial counts (log10 CFU of 5.04 and 7.27; Fig. 3L).
Linezolid, a protein synthesis inhibitor, is recommended in the IDSAclinical practice guidelines as an acceptable alternative to vancomycin fortreatment of MRSA pneumonia (5). We have shown previously (16) aswell as herein (Fig. 2, D to I) that linezolid, but not vancomycin, pro-tected against lethal necrotizing pneumonia in rabbits. Combinationtreatment with IVIG-vancomycin resulted in an overall survival rateof 71% (Fig. 2D), whereas combination treatment with IVIG-linezolidresulted in a higher overall survival rate of 93% (Fig. 2G). Linezolid wasshown previously to inhibit production of PVL and Hla in the rabbitlungs (16). The combined antitoxin properties of linezolid, which inhibitsproduction of bacterial toxins, and IVIG, which neutralizes preformedtoxins and prevents their cytotoxic effects on host cells, conferred thegreatest protection in the rabbit model. Comparative data such as theseare important for demonstrating a potential benefit of using a protein syn-thesis inhibitor, like linezolid, over vancomycin in combinationwith IVIG.
Our study has certain limitations. IVIG, either alone or in combina-tion with vancomycin or linezolid, was administered at a single time
slationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 10

R E S EARCH ART I C L E
by guest onhttp://stm
.sciencemag.org/
Dow
nloaded from
point, 1.5 hpi. We have shown previously in the same rabbit model ofnecrotizing pneumonia that delaying treatmentwith linezolid to 4 or 9 hpidecreased or abolished its protective effects (16). Whether these narrowwindows of efficacy in themodel translate into a time frame within whichapatient is clinically likely topresent andbediagnosedwith staphylococcalpneumonia is not known, a practical limitation of the rabbit model due tothe acute nature of this experimental infection (16). The combination oflinezolid and IVIGdemonstrated the greatest protective effects (Fig. 2), yetwhether it can extend the treatment window and confer protection whenadministered at a later stage of infection remains to be determined. Ourstudy is also limited by the fact that only a single commercial IVIG prep-aration, ClairYg produced by Laboratoire Français du Fractionnementet des Biotechnologies (LFB), was evaluated for protective efficacies in therabbit model. Although different commercial IVIG preparations mayvary in their concentrations of specific antitoxin antibodies, it is beyondthe scope of this work to determine the in vitro and in vivo antitoxin pro-perties of IVIG from the different companies. However, the two lots ofClairYg evaluated herein showed similar concentrations of anti-Hla andanti-LukS/F neutralizing antibodies (Fig. 1) and protective efficaciesin vivo (Figs. 2, 3, and 6).Adifferent commercial IVIGpreparation, Tégé-line produced by LFB, was shown previously to contain high titers of anti-LukS/F antibodies (2). The difference in neutralizing activities of differentcommercial IVIG preparations against staphylococcal and streptococcalsuperantigens has been shown to be relatively small, ranging from 6 to11% (15). It should be noted that even a low dose of IVIG (200 mg/kg),which is 1/10 of the recommended dose for use in humans, demonstratedprotective efficacies in our rabbit studies. It remains to be seen whetherany differences in neutralization potencies of different commercial IVIGpreparations, especially when used at the recommended high dose of2 g/kg, would affect clinical efficacy.
In conclusion, IVIGwas protective against lethal S. aureusnecrotizingpneumonia in a rabbit model because of the presence of specific polyclo-nal antibodies that neutralized the two key lung-damaging toxins, Hlaand PVL. The results demonstrate the potential clinical utility of IVIGas an adjunct therapy for treating S. aureus necrotizing pneumonia.
May 19, 2020
MATERIALS AND METHODS
Study designProtective effects of IVIG, alone or in combination with vancomycin orlinezolid, were determined in preexposure prophylaxis studies and post-exposure treatment studies in a rabbitmodel of necrotizing pneumonia.IVIG dosing in rabbits was determined empirically on the basis of serumconcentrations of human IVIG in rabbits and in vitro toxin neutraliza-tion titers. To determine whether specific antibodies in IVIG conferredprotection, we affinity-purified anti-PVL and anti-Hla antibodies fromIVIG. IVIG also has opsonophagocytic killing and anti-inflammatoryactivities that could confer protection independent of specific antitoxinantibodies. To control for these possibilities, IVIG depleted of its anti-PVL and anti-Hla antibodies was also used. The various IVIG-derivedantibody constructswere compared for protective efficacies in the rabbitpneumonia model using five different community-associated MRSAclinical strains and one predominant hospital-associatedMRSA clinicalstrain. Unraveling the mechanism of IVIG-mediated protection wasfacilitated by comparing virulence of S. aureusWT and isogenic mu-tants deficient in various secreted toxins (table S1 and S2). The rabbitexperimental pneumonia protocol was reviewed and approved by the
www.ScienceTran
University of California, San Francisco (UCSF) Institutional AnimalCare and Use Committee and conducted in a facility accredited bytheAssociation forAssessment andAccreditation of LaboratoryAnimalCare International. Infected animals were monitored every 2 to 3 hoursfor the first 30 hpi and then three times daily thereafter for clinicalsigns of pulmonary dysfunction, defined as abnormal respiratory rate>75 breaths/min, cough, and cyanosis. Animals euthanized for pulmo-nary dysfunction were recorded as nonsurvivors. Sample sizes were es-timated using log-rank test with 5% type I error rate and 80%power. Allpathogenesis studies for the comparison of WT and isogenic mutantstrains were conducted as blinded, randomized experiments. Althoughanimals were randomized for treatment studies, these studies cannot beconducted in a blindedmanner because of differences in administrationof various treatment modalities.
Rabbit model of necrotizing pneumoniaTo establish necrotizing pneumonia in the rabbit model, a 1.5-ml instil-late containing various bacterial strains was delivered directly into thelungs of anesthetizedNewZealandwhite outbred rabbits througha 2.5-mmpediatric endotracheal tube as previously described (11). We used 8- to12-week-old rabbits, weighing 2.0 to 2.8 kg. For the mortality studies,rabbits were monitored every 2 to 3 hours for the first 30 hpi and thenthree times daily thereafter, and survivors were euthanized at either36, 48, or 96 hpi. For the time-killed studies, rabbits were euthanizedat 9 hpi to determine the extent of acute lung injury. Lungs were removedaseptically from euthanized rabbits or those that were found dead. Lungswere cut into <0.5-cm pieces. Part of the lung sample was homogenizedin 0.9% saline and titered by plating serial dilutions on blood agar todetermine the number of CFUs.
The following regimens were administered intravenously at the in-dicated doses via the marginal ear vein of the rabbits for either pre-exposure prophylaxis (24 and 1.5 hours before induction of experimentalpneumonia) or postexposure treatment (1.5 hours after induction of ex-perimental pneumonia): IVIG (200 mg/kg; ClairYg, LFB), vancomycin(30 mg/kg), IVIG (200 mg/kg) depleted of anti-LukS/F-PV and anti-HlaIgG, affinity-purified anti-LukS/F-PV IgG (1 or 4 mg/kg), and affinity-purified anti-Hla IgG (1 or 4 mg/kg). Two different lots of IVIG, IVIG(L3)and IVIG(L8), were used in various experimental studies. Linezolidwas dissolved in 5% cyclodextrin to 12 mg/ml and administered at50 mg/kg subcutaneously.
Statistical analysesSurvival curves were generated using the Kaplan-Meier method, andsignificance was assessed by means of the log-rank (Mantel-Cox) test,with Bonferroni correction formultiple comparisonswhere appropriate(GraphPad version 6.0). Normal distribution was not assumed, so LW/BW (×103), log10 CFU, and concentrations of toxins and cytokines werecompared using a nonparametric two-sided Mann-Whitney U test orone-way ANOVA with Kruskal-Wallis test, followed by Dunn’smultiple comparisons post hoc test where appropriate.
SUPPLEMENTARY MATERIALS
www.sciencetranslationalmedicine.org/cgi/content/full/8/357/357ra124/DC1Materials and MethodsFig. S1. SElX does not contribute to lethal infection with USA300/LAC strain in the New Zeal-and white rabbit model of necrotizing pneumonia.
slationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 11

R E S EARCH ART I C L E
Fig. S2. Anti-Hla IgG and anti-LukF/S IgG affinity-purified from IVIG have potent neutralizationactivities.Table S1. Bacterial strains used in the present study.Table S2. Oligonucleotides used for construction of in-frame gene deletions using pKOR1 al-lelic replacement system.References (34–36)
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from
REFERENCES AND NOTES
1. A. I. Hidron, C. E. Low, E. G. Honig, H. M. Blumberg, Emergence of community-acquiredmeticillin-resistant Staphylococcus aureus strain USA300 as a cause of necrotising community-onset pneumonia. Lancet Infect. Dis. 9, 384–392 (2009).
2. V. Gauduchon, G. Cozon, F. Vandenesch, A.-L. Genestier, N. Eyssade, S. Peyrol, J. Etienne,G. Lina, Neutralization of Staphylococcus aureus Panton Valentine leukocidin by intravenousimmunoglobulin in vitro. J. Infect. Dis. 189, 346–353 (2004).
3. D. Nathwani, M. Morgan, R. G. Masterton, M. Dryden, B. D. Cookson, G. French, D. Lewis;British Society for Antimicrobial Chemotherapy Working Party on Community-onset MRSAInfections, Guidelines for UK practice for the diagnosis and management of methicillin-resistant Staphylococcus aureus (MRSA) infections presenting in the community. J. Antimicrob.Chemother. 61, 976–994 (2008).
4. M. Barton, M. Hawkes, D. Moore, J. Conly, L. Nicolle, U. Allen, N. Boyd, J. Embree, L. Van Horne,N. Le Saux, S. Richardson, A. Moore, D. Tran, V. Waters, M. Vearncombe, K. Katz, J. S. Weese,J. Embil, M. Ofner-Agostini, E. L. Ford-Jones; Writing Group of the Expert Panel of CanadianInfectious Disease, Infection Prevention and Control, Public Health Specialists, Guidelinesfor the prevention and management of community-associated methicillin-resistant Staph-ylococcus aureus: A perspective for Canadian health care practitioners. Can. J. Infect. Dis.Med. Microbiol. 17, 4C–24C (2006).
5. C. Liu, A. Bayer, S. E. Cosgrove, R. S. Daum, S. K. Fridkin, R. J. Gorwitz, S. L. Kaplan, A. W. Karchmer,D. P. Levine, B. E. Murray, M. J. Rybak, D. A. Talan, H. F. Chambers, Clinical practice guidelines bythe infectious diseases society of America for the treatment of methicillin-resistant Staphylococcusaureus infections in adults and children: Executive summary. Clin. Infect. Dis. 52, 285–292(2011).
6. N. Rouzic, F. Janvier, N. Libert, E. Javouhey, G. Lina, J.-Y. Nizou, P. Pasquier, D. Stamm, L. Brinquin,C. Pelletier, F. Vandenesch, D. Floret, J. Etienne, Y. Gillet, Prompt and successful toxin-targetingtreatment of three patients with necrotizing pneumonia due to Staphylococcus aureus strainscarrying the Panton-Valentine leukocidin genes. J. Clin. Microbiol. 48, 1952–1955 (2010).
7. N. Libert, E. Batjom, A. Cirodde, S. de Rudnicki, L. Grasser, M. Borne, L. Brinquin, Antitoxintreatments for necrotizing pneumonia due to Panton-Valentine leukocidin-secretingStaphylococcus aureus. Med. Mal. Infect. 39, 14–20 (2009).
8. C. Salliot, V. Zeller, X. Puechal, V. Manceron, S. Sire, N. Varache, J. Etienne, N. Desplaces, J.-M. Ziza,Panton-Valentine leukocidin-producing Staphylococcus aureus infections: Report of 4 Frenchcases. Scand. J. Infect. Dis. 38, 192–195 (2006).
9. F. G. Hampson, S. W. Hancock, R. A. Primhak, Disseminated sepsis due to a Panton-Valentineleukocidin producing strain of community acquired meticillin resistant Staphylococcus aureusand use of intravenous immunoglobulin therapy. Arch. Dis. Child. 91, 201 (2006).
10. M. M. Alejandria, M. A. Lansang, L. F. Dans, J. B. Mantaring III, Intravenous immunoglobulinfor treating sepsis, severe sepsis and septic shock. Cochrane Database Syst. Rev. 9,CD001090 (2013).
11. B. A. Diep, L. Chan, P. Tattevin, O. Kajikawa, T. R. Martin, L. Basuino, T. T. Mai, H. Marbach,K. R. Braughton, A. R. Whitney, D. J. Gardner, X. Fan, C. W. Tseng, G. Y. Liu, C. Badiou, J. Etienne,G. Lina, M. A. Matthay, F. R. DeLeo, H. F. Chambers, Polymorphonuclear leukocytes mediateStaphylococcus aureus Panton-Valentine leukocidin-induced lung inflammation and injury.Proc. Natl. Acad. Sci. U.S.A. 107, 5587–5592 (2010).
12. B. Löffler, M. Hussain, M. Grundmeier, M. Brück, D. Holzinger, G. Varga, J. Roth, B. C. Kahl,R. A. Proctor, G. Peters, Staphylococcus aureus Panton-Valentine leukocidin is a very potentcytotoxic factor for human neutrophils. PLOS Pathog. 6, e1000715 (2010).
13. A. N. Spaan, T. Henry, W. J. van Rooijen, M. Perret, C. Badiou, P. C. Aerts, J. Kemmink, C. J. C. de Haas,K. P. M. van Kessel, F. Vandenesch, G. Lina, J. A. G. van Strijp, The staphylococcal toxinPanton-Valentine leukocidin targets human C5a receptors. Cell Host Microbe 13, 584–594(2013).
14. L. K. McDougal, C. D. Steward, G. E. Killgore, J. M. Chaitram, S. K. McAllister, F. C. Tenover,Pulsed-field gel electrophoresis typing of oxacillin-resistant Staphylococcus aureus isolatesfrom the United States: Establishing a national database. J. Clin. Microbiol. 41, 5113–5120(2003).
15. J. Darenberg, B. Soderquist, B. H. Normark, A. Norrby-Teglund, Differences in potency ofintravenous polyspecific immunoglobulin G against streptococcal and staphylococcalsuperantigens: Implications for therapy of toxic shock syndrome. Clin. Infect. Dis. 38,836–842 (2004).
www.ScienceTran
16. B. A. Diep, A. Afasizheva, H. N. Le, O. Kajikawa, G. Matute-Bello, C. Tkaczyk, B. Sellman,C. Badiou, G. Lina, H. F. Chambers, Effects of linezolid on suppressing in vivo production ofstaphylococcal toxins and improving survival outcomes in a rabbit model of methicillin-resistant Staphylococcus aureus necrotizing pneumonia. J. Infect. Dis. 208, 75–82 (2013).
17. T. Darville, L. B. Milligan, K. K. Laffoon, Intravenous immunoglobulin inhibits staphylococcaltoxin-induced human mononuclear phagocyte tumor necrosis factor alpha production.Infect. Immun. 65, 366–372 (1997).
18. G. J. Wilson, K. S. Seo, R. A. Cartwright, T. Connelley, O. N. Chuang-Smith, J. A. Merriman,C. M. Guinane, J. Y. Park, G. A. Bohach, P. M. Schlievert, W. I. Morrison, J. R. Fitzgerald, Anovel core genome-encoded superantigen contributes to lethality of community-associatedMRSA necrotizing pneumonia. PLOS Pathog. 7, e1002271 (2011).
19. W. Salgado-Pabón, L. Breshears, A. R. Spaulding, J. A. Merriman, C. S. Stach, A. R. Horswill,M. L. Peterson, P. M. Schlievert, Superantigens are critical for Staphylococcus aureus infectiveendocarditis, sepsis, and acute kidney injury. mBio 4, e00494-13 (2013).
20. G. Y. C. Cheung, R. Wang, B. A. Khan, D. E. Sturdevant, M. Otto, Role of the accessory generegulator agr in community-associated methicillin-resistant Staphylococcus aureus patho-genesis. Infect. Immun. 79, 1927–1935 (2011).
21. M. Z. David, K. M. Rudolph, T. W. Hennessy, S. Boyle-Vavra, R. S. Daum, Molecular epidemiologyof methicillin-resistant Staphylococcus aureus, rural southwestern Alaska. Emerg. Infect. Dis. 14,1693–1699 (2008).
22. S. Takei, Y. K. Arora, S. M. Walker, Intravenous immunoglobulin contains specific antibodiesinhibitory to activation of T cells by staphylococcal toxin superantigens [see comment].J. Clin. Invest. 91, 602–607 (1993).
23. S. Bhakdi, U. Mannhardt, M. Muhly, F. Hugo, H. Ronneberger, K.-D. Hungerer, Human hyper-immune globulin protects against the cytotoxic action of staphylococcal alpha-toxin in vitroand in vivo. Infect. Immun. 57, 3214–3220 (1989).
24. J. H. Vernachio, A. S. Bayer, B. Ames, D. Bryant, B. D. Prater, P. J. Syribeys, E. L. Gorovits,J. M. Patti, Human immunoglobulin G recognizing fibrinogen-binding surface proteinsis protective against both Staphylococcus aureus and Staphylococcus epidermidis infectionsin vivo. Antimicrob. Agents Chemother. 50, 511–518 (2006).
25. U. Seybold, E. V. Kourbatova, J. G. Johnson, S. J. Halvosa, Y. F. Wang, M. D. King, S. M. Ray,H. M. Blumberg, Emergence of community-associated methicillin-resistant Staphylococcusaureus USA300 genotype as a major cause of health care–associated blood stream infec-tions. Clin. Infect. Dis. 42, 647–656 (2006).
26. H. R. Rose, R. S. Holzman, D. R. Altman, D. S. Smyth, G. A. Wasserman, J. M. Kafer, M. Wible,R. E. Mendes, V. J. Torres, B. Shopsin, Cytotoxic virulence predicts mortality in nosocomialpneumonia due to methicillin-resistant Staphylococcus aureus. J. Infect. Dis. 211, 1862–1874(2015).
27. L. Stulik, S. Malafa, J. Hudcova, H. Rouha, B. Z. Henics, D. E. Craven, A. M. Sonnevend, E. Nagy,a-Hemolysin activity of methicillin-susceptible Staphylococcus aureus predicts ventilator-associated pneumonia. Am. J. Respir. Crit. Care Med. 190, 1139–1148 (2014).
28. E. W. Gelfand, Intravenous immune globulin in autoimmune and inflammatory diseases.N. Engl. J. Med. 367, 2015–2025 (2012).
29. L. Maródi, A. Kalmár, L. Karmazsin, Stimulation of the respiratory burst and promotion ofbacterial killing in human granulocytes by intravenous immunoglobulin preparations. Clin.Exp. Immunol. 79, 164–169 (1990).
30. E. Glowalla, B. Tosetti, M. Krönke, O. Krut, Proteomics-based identification of anchorlesscell wall proteins as vaccine candidates against Staphylococcus aureus. Infect. Immun.77, 2719–2729 (2009).
31. C. S. Munro, P. J. Stanley, P. J. Cole, Assessment of biological activity of immunoglobulinpreparations by using opsonized micro-organisms to stimulate neutrophil chemiluminescence.Clin. Exp. Immunol. 61, 183–188 (1985).
32. G. Rajam, G. M. Hammons, G. M. Carlone, J. S. Sampson, E. W. Ades, A novel innate immune-enhancement strategy combined with IVIG rescues mice from fatal Staphylococcus aureussepticemia. Int. J. Microbiol. 2011, 725483 (2011).
33. M.-F. Shaio, K. D. Yang, J. F. Bohnsack, H. R. Hill, Effect of immune globulin intravenous onopsonization of bacteria by classic and alternative complement pathways in prematureserum. Pediatr. Res. 25, 634–640 (1989).
34. T. Bae, O. Schneewind, Allelic replacement in Staphylococcus aureus with induciblecounter-selection. Plasmid 55, 58–63 (2006).
35. F. Vandenesch, T. Naimi, M. C. Enright, G. Lina, G. R. Nimmo, H. Heffernan, N. Liassine, M. Bes,T. Greenland, M. E. Reverdy, J. Etienne, Community-acquired methicillin-resistant Staphylococcusaureus carrying Panton-Valentine leukocidin genes: Worldwide emergence. Emerg. Infect. Dis. 9,978–984 (2003).
36. B. A. Diep, H. A. Carleton, R. F. Chang, G. F. Sensabaugh, F. Perdreau-Remington, Roles of 34virulence genes in the evolution of hospital- and community-associated strains of methicillin-resistant Staphylococcus aureus. J. Infect. Dis. 193, 1495–1503 (2006).
Acknowledgments: We thank the LFB for providing IVIG (ClairYg) and J.-M. Dugua, F. Bettsworth,C. Lamotte, and B. Le Levreur for their technical assistance. Funding: This work was supported inpart by the U.S. Public Health Service grant NIH R01 AI087674 to B.A.D., a UCSF Research Evaluation
slationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 12

R E S EARCH ART I C L E
and Allocation Committee grant to B.A.D., andMedImmune, a member of the AstraZeneca group.Author contributions: B.A.D., H.F.C., and G.L. designed the studies and obtained funding. B.A.D.,V.T.M.L., H.N.L., M.G.P., A.H.D., X.W., E.C.D., F.A.-A., L.B., H.M., T.T.M., and H.F.C. constructed the iso-genicmutants, performed the rabbit studies, and/or analyzed those data. C.B., M.N.S., J.-P.R., and G.L.prepared affinity-purified antibodies and depleted IVIG, performed in vitro toxin neutralizationassays and toxin quantification, and/or analyzed those data. O.K. and G.M.-B. performed cytokinequantification and/or analyzed those data. C.T. and B.R.S. performed toxin quantification and/oranalyzed those data. B.A.D. performed statistical analyses. B.A.D., V.T.M.L., B.R.S., H.F.C., and G.L.wrote the manuscript. Competing interests: B.A.D. received research funding from Arsanis Bio-sciences, Cubist (now a part of Merck), Genentech (now a part of Roche), Integrated BioTherapeu-tics, MedImmune (now a part of AstraZeneca), and Pfizer. C.T. and B.R.S. are employed byMedImmune, a member of the AstraZeneca group, and may hold AstraZeneca stocks or stockoptions. C.T. and B.R.S. are coinventors on patent WO/2012/109285, entitled “Antibodies thatspecifically bind Staphylococcus aureus alpha toxin and methods of use,” which was filed byMedImmune. H.F.C. is a paid consultant for Cubist, AstraZeneca, Theravance, Allergan, Pfizer, and
www.ScienceTran
Genentech. The other authors declare that they have no competing interests. Data andmaterialsavailability: Patent WO/2012/109285 describing MEDI4893* has been filed by MedImmune.MEDI4893*, an anti-Hla human monoclonal antibody, was used as an ELISA reagent for quantifica-tion of toxin levels in rabbit lungs.
Submitted 10 May 2016Accepted 2 September 2016Published 21 September 201610.1126/scitranslmed.aag1153
Citation: B. A. Diep, V. T. M. Le, C. Badiou, H. N. Le, M. G. Pinheiro, A. H. Duong, X. Wang,E. C. Dip, F. Aguiar-Alves, L. Basuino, H. Marbach, T. T. Mai, M. N. Sarda, O. Kajikawa,G. Matute-Bello, C. Tkaczyk, J.-P. Rasigade, B. R. Sellman, H. F. Chambers, G. Lina, IVIG-mediated protection against necrotizing pneumonia caused by MRSA. Sci. Transl. Med. 8,357ra124 (2016).
slationalMedicine.org 21 September 2016 Vol 8 Issue 357 357ra124 13
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from

IVIG-mediated protection against necrotizing pneumonia caused by MRSA
Matute-Bello, Christine Tkaczyk, Jean-Philippe Rasigade, Bret R. Sellman, Henry F. Chambers and Gerard LinaCastro Dip, Fábio Aguiar-Alves, Li Basuino, Helene Marbach, Thuy T. Mai, Marie N. Sarda, Osamu Kajikawa, Gustavo Binh An Diep, Vien T. M. Le, Cedric Badiou, Hoan N. Le, Marcos Gabriel Pinheiro, Au H. Duong, Xing Wang, Etyene
DOI: 10.1126/scitranslmed.aag1153, 357ra124357ra124.8Sci Transl Med
improved survival outcomes in this preclinical animal model.prophylaxis with IVIG, or postexposure treatment with IVIG in combination with either vancomycin or linezolid,sufficient to confer protection against necrotizing pneumonia caused by MRSA in a rabbit model. Preexposure
-hemolysin (Hla) and Panton-Valentine leukocidin (PVL) are necessary andαneutralize the toxic effects of Diep and colleagues now show that, of the myriad antibodies contained in IVIG, only two specific antibodies that
pneumonia because empirical evidence supporting its use is lacking.Staphylococcus aureustreatment for severe Controversies persist about the use of human intravenous immunoglobulin (IVIG) as an adjunctive
Stemming the tide of MRSA-induced pneumonia
ARTICLE TOOLS http://stm.sciencemag.org/content/8/357/357ra124
MATERIALSSUPPLEMENTARY http://stm.sciencemag.org/content/suppl/2016/09/19/8.357.357ra124.DC1
REFERENCES
http://stm.sciencemag.org/content/8/357/357ra124#BIBLThis article cites 36 articles, 10 of which you can access for free
PERMISSIONS http://www.sciencemag.org/help/reprints-and-permissions
Terms of ServiceUse of this article is subject to the
registered trademark of AAAS. is aScience Translational MedicineScience, 1200 New York Avenue NW, Washington, DC 20005. The title
(ISSN 1946-6242) is published by the American Association for the Advancement ofScience Translational Medicine
Copyright © 2016, American Association for the Advancement of Science
by guest on May 19, 2020
http://stm.sciencem
ag.org/D
ownloaded from