
IVF Packet Section 5 (FY17 Final) - University of Utah … July2016 To our patients undergoing IVF:...
7
Updated July2016 Section V IVF Resources Contact Numbers: Main Phone: 801-581-3834 To reach our IVF Nurses for non-emergencies or on weekends please call 801.581.4837 Send us a MyChart message at https://mychart.med.utah.edu/mychart/ (Sign up Required) To pay for your cycle please call 801.587.3721 or 801.213.3871 We, at the Utah Center for Reproductive Medicine, appreciate the fact that infertility is a stressful experience for patients and the emotional strain for an advanced reproductive technology (ART) cycle is considerable. It is not uncommon for patients to have difficulties dealing with the many emotional issues associated with the ART process. Undergoing the ART process sometimes evokes feelings, emotions, and interactions that are troublesome for patients. We encourage you to work with a counselor who can best address the emotional aspects of fertility treatment. Here at UCRM, we recommend: Laura A. Czajkowski, Ph.D. (801) 585-5873 Resources for information on assisted reproductive technology: Web sites: www.healthcare.utah.edu/ucrm https://www.sartcorsonline.com/rptCSR_PublicMultYear.aspx?ClinicPKID=2334 http://www.reproductivefacts.org/ http://www.cdc.gov/ART/index.htm http://www.fertilityguide.com/home.html www.fertilitylifelines.com Book: TAKING CHARGE OF YOUR FERTILITY – The definitive guide to Natural Birth Control and Pregnancy Achievement.
-
Upload
phamnguyet -
Category
Documents
-
view
217 -
download
3
Transcript of IVF Packet Section 5 (FY17 Final) - University of Utah … July2016 To our patients undergoing IVF:...
Updated July2016
Section V
IVF Resources
Contact Numbers: Main Phone: 801-581-3834 To reach our IVF Nurses for non-emergencies or on weekends please call 801.581.4837 Send us a MyChart message at https://mychart.med.utah.edu/mychart/ (Sign up Required) To pay for your cycle please call 801.587.3721 or 801.213.3871 We, at the Utah Center for Reproductive Medicine, appreciate the fact that infertility is a stressful experience for patients and the emotional strain for an advanced reproductive technology (ART) cycle is considerable. It is not uncommon for patients to have difficulties dealing with the many emotional issues associated with the ART process. Undergoing the ART process sometimes evokes feelings, emotions, and interactions that are troublesome for patients. We encourage you to work with a counselor who can best address the emotional aspects of fertility treatment. Here at UCRM, we recommend: Laura A. Czajkowski, Ph.D. (801) 585-5873 Resources for information on assisted reproductive technology: Web sites:
www.healthcare.utah.edu/ucrm https://www.sartcorsonline.com/rptCSR_PublicMultYear.aspx?ClinicPKID=2334 http://www.reproductivefacts.org/ http://www.cdc.gov/ART/index.htm http://www.fertilityguide.com/home.html www.fertilitylifelines.com
Book:
TAKING CHARGE OF YOUR FERTILITY – The definitive guide to Natural Birth Control and Pregnancy Achievement.

Updated July2016
To our patients undergoing IVF: We understand that there is a growing interest in the use of acupuncture during embryo transfer. Reviews and individual studies on the benefits of acupuncture show conflicting results, and at present, there are no clearly defined benefits with regards to deliveries. While we do not encourage acupuncture, we would like to be able to accommodate those who wish to pursue it. However, acupuncture during embryo transfer may require extended use of the procedure room. This affects our ability to care for other patients in a timely fashion. Thus, we ask that you please notify us prior to your transfer date that you are planning to have acupuncture during your procedure so we can schedule appropriately. You will be assessed an hourly room fee for your time in the room used solely for acupuncture (time for the actual transfer and recovery are excluded, please ask for details). Thank you so much for your understanding in this issue, and we wish you the best in your endeavors. The Staff at UCRM References El-Toukhy T, et al. A systematic review and meta-analysis of acupuncture in in vitro fertilisation. British Journal of Obstetrics and Gynecology. 2008 Sep;115(10):1203-13. So EW, et al. A randomized double blind comparison of real and placebo acupuncture in IVF treatment. Human Reproduction (Oxford, England) 2009;24:341-8.

HA
ONE VING HEALTHY BABIES
AT A TIMEHow many embryos should I transfer to have one baby?
During in vitro fertilization (IVF), you can transfer one embryo (single embryo transfer, or SET) or two embryos (double embryo transfer, or DET). If you are a good candidate for single embryo transfer, your chance of having a baby after two single embryo transfers is as good as your chance of having a baby after one double embryo transfer. That’s important to know because twin pregnancies are risky for baby and mother.
The chart below compares the percentage of women who had single babies or twins after single and double embryo transfers among good candidates for single embryo transfer. These women were good candidates for single embryo transfer because they were using IVF for the first time and were (1) younger than 38, transferring fresh embryos created from their own eggs, and freezing at least one embryo or (2) any age and transferring fresh embryos created from donor eggs.
•
•
•
1 SET (fresh): transfer of one fresh embryo for the first IVF cycle.
1 SET (fresh) + 1 SET (frozen): transfer of one fresh embryo for the first IVF cycle, followed by transfer of one frozen embryo, if the first fresh embryo transfer does not lead to having a baby.
1 DET (fresh): transfer of two fresh embryos for the first IVF cycle.
Embryo Stage
(Day of Transfer)
EMBRYO TRANSFER OPTION
1 SET (fresh) 1 SET (fresh) + 1 SET (frozen) 1 DET (fresh)
Cleavage
(2-3 days)
At least one baby: 38%
Twins: Less than 1%
At least one baby: 55%
Twins: Less than 1%
At least one baby: 49%
Twins: 16%
Blastocyst
(5-6 days)
At least one baby: 51%
Twins: Less than 1%
At least one baby: 66%
Twins: 1%
At least one baby: 60%
Twins: 27%
Source: Centers for Disease Control and Prevention, National Assisted Reproductive Technology Surveillance System (NASS), 2010-2012.
For women who are good candidates for single embryo transfer, transferring one fresh embryo followed by one frozen embryo, if a second transfer is needed, offers the best chance of having a baby without increasing the chance for twins.
CS2
5712
4

HA
ONE VING HEALTHY BABIES
AT A TIMEWhy are we worried about twin pregnancies?
We know that you are ready to start or add to your family. You may be concerned about your chances of having a baby using in vitro fertilization (IVF) or how much cycles of IVF cost. These concerns are common and may lead you to think about transferring more than one embryo during your IVF procedure. However, transferring more than one embryo increases your chances of having twins or more. Twin pregnancy is risky for baby and mother, whether or not IVF is used. Some of these risks include:
Almost 3 out of 5 twin babies are born preterm, or at less than 37 weeks of pregnancy. Twin babies are nearly 6 times as likely to be born preterm as single babies.
About 1 out of 4 twin babies are admitted to the neonatal intensive care unit (NICU). Twin babies are more than 5 times as likely to be admitted to the NICU as single babies.
About 7 out of 1,000 twin babies have cerebral palsy. Twin babies are more than 4 times as likely to have cerebral palsy as single babies.
Twin babies are more likely to be stillborn, experience neonatal death, have birth defects of the brain, heart, face, limbs, muscles, or digestive system, and have autism than single babies.
Almost 1 out of 10 women carrying twins gets pregnancy-related high blood pressure. Women carrying twins are twice as likely to get pregnancy-related high blood pressure as women carrying single babies.
Almost 1 out of 20 women carrying twins gets gestational diabetes. Women carrying twins are 1.5 times as likely to get gestational diabetes as women carrying single babies.
The best way to reduce the chance of twins from IVF is to reduce the number of embryos transferred.
Research shows that, for some women, transferring one fresh embryo followed by one frozen embryo, if a second transfer is needed, offers the best chance of having a baby without increasing the chance for twins.
See the other side for details.
CS2
5712
4

HAVING HEALTHY BABIES
ONE AT A TIMEHow many embryos should I transfer to have one baby?
The Centers for Disease Control and Prevention (CDC) tracks success rates for women who receive IVF. For the years 2010 to 2012, CDC found that transferring one embryo at a time can lead to a better chance of having at least one baby while reducing the chance of having twins. These success rates are only for patients who tried IVF for the first time using fresh (not frozen and thawed) embryos, and who were either
•
•
Younger than 38, using embryos created from their own eggs, and with more than one embryo available for transfer.
Any age, using embryos created from donor eggs.
The rates below are shown by day of embryo transfer, which can affect success.
What are my chances of having at least one baby or twins if I transfer one fresh embryo?
•
•
When a fresh embryo was transferred 2-3 days after retrieval, 38% of women had at least one baby, and less than 1% had twins.
When a fresh embryo was transferred 5-6 days after retrieval, 51% of women had at least one baby, and less than 1% had twins.
What if I transfer one fresh embryo but don’t have a baby?
During your fresh cycle, your doctor can freeze extra embryos for you to use later. If you don’t get pregnant or have a baby during your fresh cycle, you can do a frozen cycle. In a frozen cycle, the frozen embryos are thawed and transferred.
•
•
When a fresh embryo was transferred 2-3 days after retrieval, and then a frozen and thawed embryo was transferred later if needed, 55% of women had at least one baby, and less than 1% had twins.
When a fresh embryo was transferred 5-6 days after retrieval, and then a frozen and thawed embryo was transferred later if needed, 66% of women had at least one baby, and less than 1% had twins.
What are my chances of having at least one baby or twins if I transfer two fresh embryos?
•
•
When two embryos were transferred 2-3 days after retrieval, 49% of women had at least one baby, and 16% had twins.
When two embryos were transferred 5-6 days after retrieval, 60% of women had at least one baby, and 27% had twins.
The option to transfer one fresh embryo followed by one thawed embryo, if needed, offers the highest chance for some IVF patients to have a baby without increasing the chance for twins. Talk with your doctor about which embryo transfer option is right for you.
The Society for Assisted Reproductive Technology (SART) has developed a tool that can help you figure out your chance of success based on your characteristics. To use this calculator, go to: https://www.sartcorsonline.com/Predictor/Patient For more information about IVF, see www.cdc.gov/art

Fact Sheet From ReproductiveFacts.org
The Patient Education Website of the American Society for Reproductive Medicine
In vitro fertilization (IVF): what are the risks?IVF is a method of assisted reproduction in which a man’s sperm and a woman’s eggs are combined outside of the body in a laboratory dish. One or more fertilized eggs (embryos) may be transferred into the woman’s uterus, where they may implant in the uterine lining and develop. Serious complications from IVF medicines and procedures are rare. As with all medical treatments, however, there are some risks. This document discusses the most common risks.What kind of side effects can occur with IVF medicines?Usually, injectable fertility medications (gonadotropins) are used for an IVF cycle. These medicines help stimulate a number of follicles with eggs to grow in the ovaries. A more detailed discussion of fertility medications can be found in the ASRM booklet, Medications for inducing ovulation.
Possible side effects of injectable fertility medicines include:• Mild bruising and soreness at the injection site (using different sites
for the injections can help) • Nausea and, occasionally, vomiting• Temporary allergic reactions, such as skin reddening and/or itching
at the injection site• Breast tenderness and increased vaginal discharge• Mood swings and fatigue• Ovarian hyperstimulation syndrome (OHSS)
Most symptoms of OHSS (nausea, bloating, ovarian discomfort) are mild. They usually go away without treatment within a few days after the egg collection. In severe cases,OHSScancause largeamountsof fluid tobuild up in the abdomen (belly) and lungs. This can cause very enlarged ovaries, dehydration, trouble breathing, and severe abdominal pain. Very rarely (in less than 1% of women having egg retrieval for IVF), OHSS can lead to blood clots and kidney failure. For more information about OHSS, see the ASRM fact sheet Ovarian hyperstimulation syndrome (OHSS). Earlier reports from several decades ago suggested a link between ovarian cancer and the use of fertility medicines. However, more recent and well done studies no longer show clear associations between ovarian cancer and the use of fertility medications. What are the risks of the egg retrieval?During the egg retrieval, your doctor uses vaginal ultrasound to guide the insertion of a long, thin needle through your vagina into the ovary and then into each follicle to retrieve eggs. Possible risks for this procedure include:• Mild to moderate pelvic and abdominal pain (during or after). In
most cases, the pain disappears within a day or two and can be managed with over-the-counter pain medications.
• Injury to organs near the ovaries, such as the bladder, bowel, or blood vessels. Very rarely, bowel or blood vessel injury can require emergency surgery and, occasionally, blood transfusions.
• Pelvic infection (mild to severe). Pelvic infections following egg retrieval or embryo transfer are now uncommon because antibiotic medicines are usually given at the time of egg collection. Severe infection may require hospitalization and/or treatment with intravenous antibiotics.
• Rarely, to manage a severe infection, surgery may be required to remove one or both of the ovaries and tubes and/or uterus. Women who have had pelvic infections or endometriosis involving the ovaries are more likely to get IVF-related infections.
What are the risks associated with the embryo transfer?A catheter containing the embryos is used to gently place them into the uterus (womb). Women may feel mild cramping when the catheter is inserted through the cervix or they may have vaginal spotting (slight bleeding) afterward. Very rarely, an infection may develop, which can usually be treated with antibiotics.
If I conceive with IVF, will my pregnancy be more complicated (than if I conceived on my own)?Having a multiple pregnancy (pregnancy with more than one baby) is more likely with IVF, particularly when more than one embyro is transferred. Thesepregnanciescarrysignificantrisks,including:• Preterm labor and/or delivery: premature babies (regardless of
whether or not they were conceived naturally or with IVF) are at higher risk for health complications such as lung development problems, intestinal infections, cerebral palsy, learning disabilities, language delay, and behavior problems
• Maternal hemorrhage• Delivery by cesarean section (C-section)• Pregnancy-related high blood pressure• Gestational diabetes
The more embryos that are transferred into the uterus, the greater the risk. Your doctor should transfer the minimum number of embryos necessary to provide a high likelihood of pregnancy with the lowest risk of multiple pregnancy. For more information about multiple pregnancy, see the ASRM booklet titled Multiple pregnancy and birth: twins, triplets and high-order multiples. One way to avoid multiple pregnancy is to choose to transfer only one embryo at a time. For more information about this, see the ASRM fact sheet Single embryo transfer.Will IVF increase the risk of my child having a birth defect?The risk of birth defects in the general population is 2%-3%, and is slightly higher among infertile patients. Most of this risk is due to delayed conception and the underlying cause of infertility. Whether or not IVF alone is responsible for birth defects remains under debate and study. However, when intracytoplasmic sperm injection (ICSI) is done along with IVF, there may be an increased risk of birth defects. In addition, there may be a slight increased risk of sex chromosome (X or Y chromosome) abnormalities with ICSI. However, it is uncertain if these risks are due to the ICSI procedure itself or to problems with the sperm themselves. Men with sperm defects are more likely to have chromosomal abnormalities, which can be transmitted to their children. However, these disorders are extremely rare. Rare genetic syndromes called imprinting disorders may be slightly increased wtih IVF.Miscarriage and ectopic pregnancyThe rate of miscarriage after IVF is similar to the rate following natural conception, with the risk going up with the mother’s age. The rate of miscarriage may be as low as 15% for women in their 20s to more than 50% for women in their 40s. There is a small risk (1%) of an ectopic (tubal) pregnancy with IVF; however, this rate is similar to women with a history of infertility. If an ectopic pregnancy occurs, a woman may be given medicines to end the pregnancy or surgery to remove it. If you are pregnant and experience a sharp, stabbing pain; vaginal spotting or bleeding; dizziness or fainting; lower back pain; or low blood pressure (from blood loss), and have not hadanultrasoundconfirmingthatthepregnancyisintheuterus,callyourdoctor immediately. These are all signs of a possible ectopic pregnancy. There is a 1% risk for a heterotopic pregnancy after IVF. This is when an embryo implants and grows in the uterus while another embryo implants in the tube, leading to a simultaneous ectopic pregnancy. Heterotopic pregnancies usually require surgery (to remove the ectopic pregnancy). In most cases, the pregnancy in the womb can continue to develop and grow safely after the tubal pregnancy is removed. Revised 2015
For more information on this and other reproductive health topics, visit www.ReproductiveFacts.org
AMERICAN SOCIETY FOR REPRODUCTIVE MEDICINE • 1209 Montgomery Highway • Birmingham, Alabama 35216-2809TEL (205) 978-5000 • FAX (205) 978-5005 • E-MAIL [email protected] • URL www.asrm.org
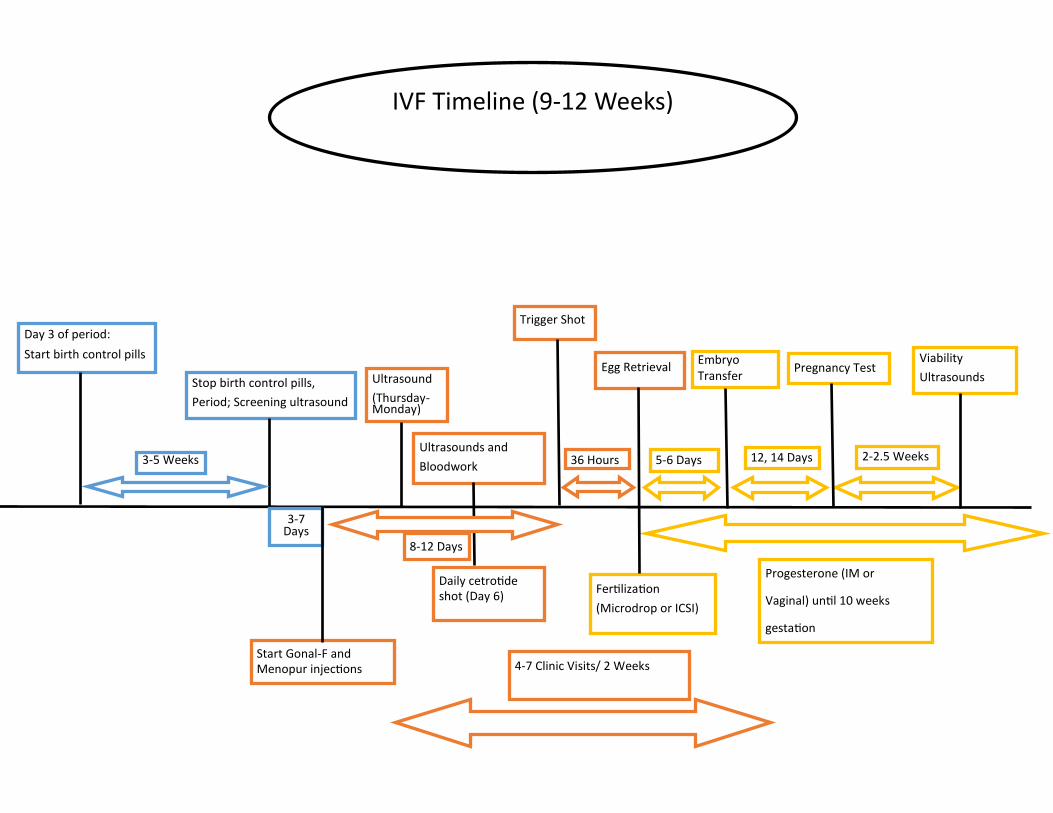
Day 3 of period:
Start birth control pills
3-5 Weeks
Stop birth control pills,
Period; Screening ultrasound
Ultrasound
(Thursday-Monday)
Ultrasounds and
Bloodwork
Trigger Shot
3-7 Days
8-12 Days
Start Gonal-F and Menopur injections
Egg Retrieval Embryo Transfer
Pregnancy Test
36 Hours 5-6 Days 12, 14 Days 2-2.5 Weeks
Viability
Ultrasounds
Fertilization
(Microdrop or ICSI)
Progesterone (IM or
Vaginal) until 10 weeks
gestation
IVF Timeline (9-12 Weeks)
Daily cetrotide shot (Day 6)
4-7 Clinic Visits/ 2 Weeks


















