Item 11 - Nurse Staffing Annual Report...Trust Board Report Cover Sheet Agenda Item: 11 Date of...
168
Trust Board Report Cover Sheet Agenda Item: 11 Date of Meeting: Wednesday 28 th June 2017 Report Title: Nurse Staffing Annual Capacity & Capability Report Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing for QE Gateshead. Decision: ☐ Discussion: ☐ Assurance: ☒ Information: ☐ Corporate Objectives report relates to: (Including reference to any specific risk) Corporate Objective 4: Delivering patient centred and co-ordinated care ensuring better outcomes as described in the NHS Outcomes Framework. Recommendations: (Action required by Board of Directors) The Board is asked to receive the report for assurance and information. Financial Implications: Yes Risk Management Implications: Yes Human Resource Implications: Yes Diversity and Inclusion Implications: No Author: Mrs H Lloyd, Director of Nursing, Midwifery & Quality & Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality Presented by: Mrs H Lloyd, Director of Nursing, Midwifery & Quality
Transcript of Item 11 - Nurse Staffing Annual Report...Trust Board Report Cover Sheet Agenda Item: 11 Date of...

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
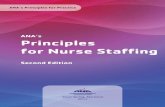
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality

Trust Board
Report Cover Sheet Agenda Item: 11
Date of Meeting:
Wednesday 28th
June 2017
Report Title:
Nurse Staffing Annual Capacity & Capability Report
Purpose of Report: To provide a comprehensive review of inpatient / ward nurse staffing
for QE Gateshead.
Decision:
☐☐☐☐
Discussion:
☐☐☐☐
Assurance:
☒☒☒☒
Information:
☐☐☐☐ Corporate Objectives
report relates to:
(Including reference to
any specific risk)
Corporate Objective 4: Delivering patient centred and co-ordinated
care ensuring better outcomes as described in the NHS Outcomes
Framework.
Recommendations:
(Action required by
Board of Directors)
The Board is asked to receive the report for assurance and
information.
Financial
Implications:
Yes
Risk Management
Implications:
Yes
Human Resource
Implications:
Yes
Diversity and Inclusion
Implications:
No
Author:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality &
Mrs A Lowery, Deputy Director of Nursing, Midwifery & Quality
Presented by:
Mrs H Lloyd, Director of Nursing, Midwifery & Quality

2
Gateshead Health NHS Foundation Trust
‘Safer Staffing’ Nursing Review
1. Introduction
This detailed annual report provides a comprehensive review of inpatient / ward nurse
staffing for QE Gateshead. It is in line with the requirements set out by the National Quality
Board (NQB): Supporting NHS providers to deliver the right staff, with the right skills, in the
right place at the right time- safe, sustainable and productive staffing (July 2016).
In December 2016 NHSI published a draft staffing improvement resource for adult
inpatient wards in acute hospitals which aligns to the NQB guidance. It outlined a
systematic approach for identifying the organisational, managerial and wards factors that
support safe staffing and builds upon the NICE safe staffing guidance. The approach we
have taken to this staffing review is line with the recommendations.
Recent changes to ward configurations have resulted in an increase in bed numbers in
some areas, ward relocations with resultant changes to ward layout/environment, as well
as changes to service delivery models, all of which have had an impact upon the nurse
staffing requirements.
A detailed review of nurse and midwifery staffing took place between February and April
for all acute inpatient areas, Emergency Care Centre, Maternity and community nursing.
This was led by the Director and Deputy Director of Nursing, Midwifery and Quality working
closely with the Associate Directors, Service Line Managers, Matrons and Ward
Sister/Charge Nurses to determine establishment / workforce requirements for the next 12
months ahead.
A review of staffing establishments for Paediatrics and Mental Health will be undertaken
separately and reported to the Board in September.
2. Review of staffing establishments
National guidance recommends that ward nurse staffing is determined using a validated,
evidence based methodology. The nurse staffing review for acute in patient areas and ECC
was undertaken utilising the following comprehensive evidence based methodology:
• Nurse per occupied bed days
• Safer Nursing Care Tool (SNCT)
• NQB / NICE Guidance
• Quality Indicators
• Review of agreed staffing levels
• Professional Judgement
• Review of current establishments
• Nurse per occupied bed day
The initial step in the methodology for calculating nurse staffing is currently based
on the nurse per occupied bed day methodology (NPOB). The number of nursing
staff required for each ward has previously been calculated based on the nurse per
occupied beds ratio as set out below.
Number of beds X 0.9 + 21% uplift

3
The 21% uplift is for annual leave (13%); study leave (4%); sickness (4%). Latest
guidance from NHS Improvement related to nurse rostering suggests that uplift
should be between 22% and 25%. The Trust will review the uplift, but will continue
to utilise 21% uplift for the purpose of this staffing review.
The methodology is applied to all wards regardless of size, but is recognised as
being less accurate in predicting required staffing for small wards as staffing can
only be provided in whole numbers, making small wards less efficient in the
utilisation of nursing staff.
In the future we will no longer utilise the nurse per occupied bed day calculation,
however this approach of incorporating a 21% uplift, that allows for efficient and
responsible management of planned and unplanned leave, will be included in our
agreed evidence based methodology moving forward. The 21% uplift is included
within our staffing calculation and the SNCT, a more up to date and sensitive
method of using multipliers taking account of patient acuity and dependency.
• Safer Nursing Care Tool
The Safer Nursing Care Tool (SNCT) was developed to help NHS staff measure
patient acuity and dependency in acute hospital wards to inform evidence based
decision making on staffing and workforce. It is widely recognised by NICE and NHSI
as the ratified tool for measuring staffing requirements.
The Trust has utilised the Safer Nursing Care Tool for some time, collecting data
twice per year, as per national guidance. In April 2016, for improved accuracy, we
moved to monthly measurement which enables us to use the data to monitor
trends over time for every ward. The information acts as an acuity and dependency
‘thermometer’ and is triangulated with other measures to make decisions on
staffing establishments.
The SNCT is based on the critical care patient classification (Comprehensive Critical
Care, DH 2000) as set out in Table 1.
Table 1 SNCT descriptors
Levels of
Care
Descriptor
0 Patient requires hospitalisation. Needs met by provision of normal
ward cares
1a Acutely ill patients requiring intervention or those who are unstable
with a greater potential to deteriorate
1b Patients who are in a stable condition but are dependent on nursing
care to meet most or all of the activities of daily living
2 Patients who can be managed within clearly identified, designated
beds, resources with the required expertise and staffing level OR
may require transfer to a dedicated Level 2 facility/ unit.
3 Patients needing advanced respiratory support and /or therapeutic
support of multiple organs.
For one week each month every ward collects data – this involves scoring each
patient to an acuity and dependency care level as described above. Staffing

4
multipliers are applied for each acuity and dependency care level. These multipliers
factor in nursing time spent on:
• Direct and indirect care;
• Ward management;
• Education/training;
• Staff performance review;
• Official and unofficial staff breaks;
• Associated work such as administration and clerical;
• Bed occupancy.
Uplift for annual leave, sickness cover and maternity leave is added to the
multiplier. The graphs below provide an example of how the resultant SNCT data is
presented and compared to current funded establishment. In this way variation in
patient acuity and dependency can be monitored and taken into consideration with
other data when reviewing nursing establishments.
• Nurse Sensitive Quality Indicators
It is important for any staffing review to take into consideration the quality of care,
patient experience and capability of the workforce. A number of quality indicators
can be linked to nursing care. These are considered for each ward as part of the
staffing review to help ensure staffing levels are sufficient to achieve best patient
care. The table below provides an example for Ward 9.
Patient Acuity & Dependency Level Ward 9 (Surgery)
0.00 0.00
24.4322.40
12.0014.00
17.00
0.00 0.00 0.29 1.20
3.86
1.00 1.500.00 0.00
3.71 3.60
11.71
5.757.67
0.00 0.00 0.29 0.00 0.14 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00
31.2029.72
37.24
24.87
31.7529.53 29.53 29.53 29.53 29.53 29.53 29.53
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)
Patient Acuity & Dependency Level Ward 1 (General Medicine)
3.835.67
10.40
13.8612.00
14.33
8.50
5.67
1.500.40 0.14 0.00
5.33
0.25
14.6716.50
12.80
8.71
11.80
4.00
15.00
0.00 0.00 0.00 0.00 0.00 0.00 0.000.00 0.00 0.00 0.00 0.00 0.00 0.00
36.45 35.66
32.50
28.59
31.82
28.15
34.17
25.94 25.94 25.94 25.94 25.94 25.94 25.94
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
40.00
Apr May Jun Jul Aug Sep Oct
Level 0 Level 1a Level 1b Level 2 Level 3 SNCT Establishments Funded Establishments (WTE)

5
Table 2 Quality Indicators
Quality Outcomes May to Oct 2016 Ward 9
Friends and Family Test -
Recommend Rate 93.3%
Number of Falls (Monthly
Average of incidence)
29
(4.8)
Patient Experience Score
(Maximum score = 6) 5.67
Safety Thermometer – New
Catheter UTI 1
Safety Thermometer Pressure
Ulcers (Grade 2-4) prevalence 1
Safety Thermometer - New
VTE 0
Validated Category 2 Pressure
Damage (Monthly Average of
incidence )
0 .16 Staffing Incidents reported
via Datix 0
Safety Thermometer – Falls-
prevalence 0
• Agreed staffing levels
In April 2014, the NQB mandated that all hospitals have in place a process to enable
staffing establishments to be met on a shift by shift basis. In line with this we
agreed planned levels of staffing on a shift by shift basis across the Trust and both
planned and actual nurse staffing levels are publically displayed on all wards.
We have used these recommendations to ensure that staffing establishments are
able to meet the required shift by shift staffing levels for each ward, maintaining a
minimum of 1:8 qualified nurses to patient ratio, and an optimal level of 1:8 plus a
qualified nurse co-ordinator for each early shift.
Finally, Ward Sister/Charge Nurse and Matron’s professional judgement, local
context, with working knowledge of the clinical area and patient needs determines
the number of staff required to safely deliver patient care.
• Review of current establishments
Once the new staffing levels were identified, the required establishments were
calculated and compared to the current funded establishments to determine
whether any adjustments to funding and skill mix were required. This was especially
important due to the reconfiguration of wards and the increase in bed base across
the Trust.
3. Collaborative Approach to Safer Staffing
Workshops were held with ward sister/charge nurses and Matrons to review a range of
information that included the NPOBD establishments, previously agreed staffing levels,
SNCT data and quality indicators. These involved detailed discussions, debate and
challenge to enable robust decisions to be made regarding staffing levels moving forward.
Meetings were held with both the Medical and Surgical Business Units led by the Director
of Nursing, Midwifery and Quality involving the Associate Directors and Matrons. The
purpose was to analyse, scrutinise and challenge the staffing proposals and to come to an
agreement on safe staffing levels to ensure the continuity of safe patient care.
• (Proposed) Agreed Staffing Levels
Table 3 (Medicine - Wards) and Table 4 (Surgery) provide the proposed planned
staffing numbers on a shift by shift basis and rationale for proposed changes. These

6
staffing levels have been set using the described methodology and are based on the
ratio of 1:8 qualified nurse to patient (plus the co-ordinator for an early shift) and a
minimum ratio of 1:8 for the late shift.
The information in Table 3 includes the non-invasive ventilation nurses on Ward 9,
stroke nurses Ward 4 and the chest pain nurse on Ward 8 who are identified as +1
in the agreed staffing numbers table 3. Allowances have been made in the budgets
for these staff.
Where there has been an increase in beds there will be a requirement for an uplift
in funded establishment and work is currently being undertaken with finance to
determine these new establishments.
4. Efficient Rostering
Significant work on efficient nurse rostering has been undertaken in line with the
recommendations made within the Lord Carter review. The working group led by the
Deputy Director of Nursing Midwifery and Quality has developed a rostering policy, and
standards for ward managers and these are being rolled out across all acute inpatient ward
areas.
Our establishments are based upon the most efficient shift system being in place for full
time staff and comprise of:
• 2 x 6 hours 45mins shift
• 2x 12 hours shift
This shift pattern enables each full time member of staff to cover 6 shifts per week. This is
in contrast to the traditional shift pattern of five 7.5 hours per shift. They do not include
additional management time for Ward Sister/ Charge Nurses however it is anticipated that
this will be incorporated into the co-ordinators role. A suite of performance indicators
have been identified and reports are being developed at business unit and ward level to
enable measurement of compliance with the standards and assess the impact of this
quality and efficiency work.

7
Table 3 Planned Staffing Levels Medicine on a shift by shift basis
Ward Beds Early Late Nights
Now Pre RN HCA Ratio RN HCA Ratio RN HCA
Ward 1 24 17 4 3 3.4 3 3 4 2 2 Numbers lowered as this ward relocated from ward 12 to
ward 1 and is now excludes PIU patients.
Ward 4 30 24 5+1 4 3.3 4+1 3 4.2 2 3 Increase in HCAs for nights as ward relocated from ward
22 to ward 4. Layout of ward requires three nursing
teams per shift. Higher risk of patient falls.
Ward 8 21 21 5+1 2 3 4+1 2 3.5 2+1 1 No change in numbers
Ward 9 36 24 6+1 4 3.6 5+1 4 4 2+1 3 Over time have increased from 24 to 27 to 36 beds.
SNCT reflects the proportion of high acuity patients in
this area. Higher risk of falls.
Ward 11 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of patients with increased
acuity and dependency. Complex patient group.
Ward 22 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
SNCT indicates high proportion of more dependent
patients. Higher risk of patient falls.
Ward 23 24 24 4 3 3.4 3 3 4 2 2 Dual Care Ward. No change in numbers. HCA’s were
increased in 16/17 following approval of business case.
Ward 24 29 24 5 4 3.2 4 3 4.1 2 2 Increase in HCA numbers due to increase to 29 beds (+5).
Higher risk of patient falls.
Ward 25 30 24 5 4 3.3 4 3 4.2 2 2 Increase in HCA numbers due to increase to 29 beds (+6).
Higher risk of patient falls.
St Bedes 10 10 3 2 2 2 2 2.5 2 1 No change in numbers.

8
Table 4 Planned Staffing Levels Surgery on a shift by shift basis
Ward Beds
Early Late Nights Commentary
RN HCA Ratio RN HCA Ratio RN HCA
Ward 12 27
5 3 3.3 4 3 3.8 2 2 Agreed change in skill mix for night duty. This ward has
relocated from ward 9 to ward 12.
Ward 14a 32 5 4 3.5 4 4 4 2 3 No change in agreed numbers.
Ward 21 18 3 2 3.6 3 2 3.6 2 1 No change to agreed numbers.
Level 1 30 5 3 3.7 4 3 4.2 2 2 No change in agreed numbers.
Level 2 30 5 4 3.3 4 4 3.7 2 2 No change in agreed numbers.
CCU 14 12 2 1 or 2 12 2 1 or 2 11 1 No change in agreed numbers.
5. Review of staffing ECC
Table 5 Planned Staffing Levels of ECC
Ward Beds Early Late Nights
Commentary
now pre RN HCA RN HCA RN HCA
EAU 24 24 7 2 7 2 7 2 Numbers required to meet 1: 4 ratio per POD for qualified nurse. 2
Nursing assistants required across 3 PODs per shift. One qualified co-
ordinator per shift. Reflects the high activity, turnover and length of stay.
SSU 24 24 4 2 3 2 3 2 Increase in qualified at night due to increase in admissions.
A&E Majors 10 2 11 2 9 2 These numbers are required to provide the following staff to patient ratios
2:1 in Resus, 1:4 Majors . 2 qualified staff in triage and 2 in Minors 2.
Urgent Care
Centre
4 Nurse Practitioners. Shift pattern start times are
staggered over the day to provide cover across
extended hours.
Now open 8am until 12 midnight seven days per week.

9
6. Review of Staffing within Maternity
A review of midwifery staffing has also been undertaken in collaboration with the
Head of Midwifery and the following staffing levels have been agreed for Delivery
Suite, Antenatal/Postnatal Ward, Special Care Baby Unit (SCBU) and Pregnancy
assessment unit. These are set out in tables 6 to 9.
Within Delivery Suite ‘Birth Rate Acuity’ an acuity and dependency tool, has recently
been implemented to enable us to assess and monitor the acuity of our mothers
over set periods of the day and indicate whether staffing levels meet their needs.
This data will be analysed and built into our staffing review methodology moving
forward.
Table 6
Delivery Suite /
Theatres Mon Tues Wed Thurs Fri Sat Sun
Early Q *5 *5 *5 *5 *5 4 4
U 2 2 2 2 2 2 2
Late Q 4 4 4 4 4 4 4
U 2 2 2 2 2 2 2
Night Q 4 4 4 4 4 4 4
U 1 1 1 1 1 1 1
* accommodate elective theatre staffing Monday to Friday
Table 7
AN/PN Ward Mon Tues Wed Thurs Fri Sat Sun
Early Q 3 3 3 3 3 2 2
U 2 2 2 2 2 2 2
Late Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Night Q 2 2 2 2 2 2 2
U 2 2 2 2 2 2 2
Table 8
Special Care
BABY Unit Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1

10
Table 9
Pregnancy
Assessment Mon Tues Wed Thurs Fri Sat Sun
Early Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Late Q 2 2 2 2 2 2 2
U 1 1 1 1 1 1 1
Night Q
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
1+ 1 twilight
U N/A N/A N/A N/A N/A N/A N/A
7. Community Nursing Services
The current community nursing staff of 170 WTE was TUPE transferred from South
Tyneside Foundation Trust in October 2016 following the Gateshead Care
Partnership’s successful bid to deliver community services for the patients in
Gateshead. NHS Improvement published draft guidance in March 2017 on
community staffing as part of a suite of guidance currently being developed for
various care settings and specialities. The resource acknowledges and sets out
comprehensively the different considerations that need to be factored in when
planning the district nursing workforce compared to acute settings. The guidance
refers to safer caseloads in district nursing services rather than safer staffing as this
better reflects the complexity of determining the required staffing levels. The
resource is based on the NQB (2016) three expectations right staff, right skills, right
place and time and provides a set of principles under these key areas.
Some key areas of note include:
• What does good care look like? – the guide recommends Maybin et al ( 2016)
quality framework as a basis for an assessment tool for measuring the quality
of district nursing services.
• The district nursing caseload – there is an acknowledgment that the approach
to determining a safe caseload is not based on nurse to patient ratios due to
caseloads varying in size and complexity and geographical distribution of
patients.
• Determining safe caseloads – should involve assessment of current and
projected population and the skills within the team at strategic level. At an
operational level it requires an assessment of needs of patients at a service
and team level to determining how staff are deployed. The importance of
investing in technology to support safe caseload management is emphasised.
Having reviewed this guidance it is our intention to undertake a full workforce
review and development plan within the parameters of the community
transformation agenda ensuring our approach is aligned to the recommendations
made within this new staffing guidance.

11
8. Capability and Quality
It is important for any staffing review to take into consideration the quality of the
care provided, patient experience and capability of the work force as well as the
capacity. Table 7 provides a breakdown by ward of the following information:
• Patient experience – the Friends and Family Test
• Patient Experience- Real Time survey
• Percentage of harm free care – the Safety Thermometer
• Percentage of staff who have completed mandatory training
• Percentage of staff who have had an appraisal in the last 12 months
There are local action plans in the areas that have not achieved over 80% for
mandatory training and appraisals as well as Trust wide plans for F&FT and the safety
thermometer.
Table 10 Quality and capability indicators
Business
Unit Specialty Ward / Dept
Patient
F&FT
Patient
Experience
(average
score / 6)
Safety
Thermometer
(harm free)
Mandatory
Training Appraisal
Medicine Elderly Ward 22 100.00% 5.84 95.83% 87.50% 88.89%
Medicine Respiratory Ward 9 97.56% no survey 96.97% 88.57% 81.40%
Medicine Cardiology Ward 8 100.00% 6.00 100.00% 90.63% 75.00%
Medicine Gastro Ward 11 100.00% 5.87 96.55% 95.24% 100.00%
Medicine Medicine Ward 1 100.00% 6.00 88.24% 90.63% 97.06%
Medicine Stroke Ward 4 91.67% 5.99 96.00% 83.78% 86.05%
Medicine Elderly Ward 23 100.00% no survey 87.50% 87.50% 89.29%
Medicine Elderly Ward 24 100.00% no survey 100.00% 88.46% 79.41%
Medicine Elderly Ward 25 100.00% 5.99 93.33% 61.54% 82.35%
Medicine Palliative St Bedes - 6.00 71.43% 95.83% 92.00%
Medicine Emergency
Care
Ward 2
Short Stay 98.53% no survey 80.00% 73.08% 96.77%
Medicine Emergency
Care
ECC
Assessment 98.57% 5.61 92.86% 87.10% 79.07%
Medicine Mental
Health Cragside - no survey 100.00% 74.07% 81.48%
Medicine Mental
Health Sunniside - no survey 100.00% 73.68% 89.47%
Medicine Rehabilitation ICAR 100.00% no survey 90.00% 100.00% 92.59%
Surgery Gen Surgery Ward 12 97.56% 5.84 100.00% 85.19% 90.91%
Surgery Orthopaedics Ward 14 81.82% 5.93 82.76% 64.71% 92.86%
Surgery Gynaeonc Ward 21 97.30% 5.99 100.00% 92.00% 85.71%
Surgery Orthopaedics PSSC 1 98.72% 5.80 100.00% 84.38% 87.50%
Surgery Gen Surgery PSSC 2 98.15% 5.77 100.00% 93.10% 91.43%
Surgery Critical Care Critical Care 100.00% 6.00 100.00% 98.80% 95.45%
Surgery Maternity AN/PN 98.81% no survey 100.00% 82.61% 87.50%
9. Conclusion
This report provides assurance to the Board on staffing capacity and capability. It
provides a clear methodology for agreeing nursing and midwifery staffing numbers
and establishments. It provides information on the agreed number of staff needed

12
on a shift by shift basis on each ward and meets the requirement set out in
expectations set out by the NQB and provides assurance that the Trust has robust
systems in place to safeguard the quality of care provided to patients. This report will
be published on the Trust website for our patients and the public.
10. Recommendations
The Board is asked to receive this report for information and assurance.
Hilary Lloyd Avril Lowery
Director of Nursing, Deputy Director of Nursing,
Midwifery and Quality Midwifery and Quality