Issues of Women Returning from Combat Harold Kudler, M. D. Elizabeth Marks LCDR Erin Simmons Kristy...
89
Issues of Women Returning from Combat Harold Kudler, M. D. Elizabeth Marks LCDR Erin Simmons Kristy Straits-Troster, Ph.D., ABPP
-
Upload
sherman-tyler -
Category
Documents
-
view
216 -
download
1
Transcript of Issues of Women Returning from Combat Harold Kudler, M. D. Elizabeth Marks LCDR Erin Simmons Kristy...

Issues of Women Returning from Combat
Harold Kudler, M. D.Elizabeth Marks
LCDR Erin SimmonsKristy Straits-Troster, Ph.D., ABPP

“When I come to feeling overwhelmed…I want a one-on-one talk with a trained psychiatrist who’s either been to war or understands war.”
--Staff Sgt. Gladys Santos, who attempted suicide after three tours in Iraq.
Newsweek February 11, 2008
Introduction
2

“For the first time in American history, 90% of wounded (soldiers) survive their injuries”
(Alive Day Memories: Home from Iraq HBO documentary
“A greater percentage of men and women are coming home with …TBI and severe Posttraumatic Stress.”
Introduction
3

IntroductionHow many of you are:• Current or former Service Members? • Spouses of a Current or Former
Service Member?• Other family of a Current or Former
Service Member?
4

IntroductionHow many of you are:• Psychiatrists/Physicians?• Psychologists?• Social workers?• Licensed Counselors?
• Substance Abuse?• Marriage and Family?
• Nurses?• Others?
5

• Length of current combat operations– As of November 27, 2006, war in Iraq
has been going on longer than WWII.• An all volunteer force = multiple
deployments
Scope of the Issue
6

Scope of the Issue
• 1 ½ million service members have served in Iraq and Afghanistan
• “The war in Iraq remains very personal. Over 75% of Soldiers and Marines surveyed reported being in situations where they could be seriously injured or killed; 62-66% knew someone seriously injured or killed; more than one third described an event that caused them intense fear, helplessness or horror.”
--From the Office of Surgeon General Mental Health Advisory Team (MHAT) IV, Final Report, Nov 06
7

Scope of the Issue• “The challenges are enormous and the
consequences of non-performance are significant. Data…indicate that 38% of Soldiers and 31% of Marines report psychological symptoms. Among members of the National Guard, the figure rises to 49%. Further, psychological concerns are significantly higher among those with repeated deployments, a rapidly growing cohort.
--Report of the DoD Task Force on Mental Health, June 2007
8

Scope of the Issue
• Psychological concerns among family members of deployed and returning OEF/OIF veterans, while yet to be fully quantified, are also an area of concern. Hundreds of thousands of children have experienced the deployment of a parent…”
--Report of the DoD Task Force on Mental Health, June 2007
9

Who VA Serves
• Of 23.4 million Veterans currently alive, nearly three-quarters served during a war or an official period of conflict
• Women account for 8% of all Veterans (roughly 1.8 million Women Veterans)
• VA currently provides health care to 5.5 million Veterans (roughly 1 in 5 Veterans)
• Roughly 11% of VA users are Women
http://www.va.gov/10
Care Access Points• 153 medical centers
– At least one per state, Puerto Rico and the District of Columbia
• 909 ambulatory care and community-based outpatient clinics
• 47 residential rehabilitation treatment programs
• 232 Veterans Centers• 108 comprehensive home-care programs• 4 DoD/VA Polytrauma Centers• My HealtheVet http://www.myhealth.va.gov/• 21 Veterans Integrated Service Networks
(VISNs)11

Mental Health Among OEF/OIF Veterans
• Possible mental health problems reported among 44% (162,044) of the 371,123 eligible OEF/OIF veterans who have presented to VA
• Provisional MH diagnoses include:• PTSD 83,865
– (23% of all who presented to VA)• Nondependent Abuse of Drugs: 68,009• Depressive Disorder: 56,492• Affective Psychoses 32,065• Neurotic Disorders: 44,899• Alcohol Dependence: 14,396• Drug Dependence: 6,543
12

IntroductionThe V6 MIRECC in collaboration with VA’s
Environmental Epidemiology Service (EES) analyzed DoD & VA data on over 54,000 female & 398,000 male OEF/OIF Veterans in order to determine their risk for PTSD
Among the factors considered were gender, age, military rank, military branch, Active Duty vs. Reserve status, marital status & race
This first look at gender-specific risk for PTSD among OEF/OIF Veterans offers new direction for research, outreach & clinical initiatives
13

Methods• These administrative data have to be interpreted with
caution because they only apply to OEF/OIF Veterans who have accessed VHA health care due to a current health question
• These data do not represent the total group of over one million OEF/OIF Veterans who have become eligible for VA healthcare since FY 2002 or the approximately 1.8 million troops who have served in the two theaters of operation since the beginning of the conflicts in Iraq and Afghanistan
• At the MIRECC’s request, EES ran a series of logistic regression analyses on PTSD by gender based on 2nd QTR FY09 data
14

What About Women OEF/OIF Veterans Seen in VA (as of 2nd Qtr FY2009)?
• Number of Female OEF/OIF VA Users = 45,152
• 12% of the total number of OEF/OIF VA Users (371,123) are women
• This closely mirrors the overall percentage of women among OEF/OIF veterans eligible to use VA (11%)
15

Women Veterans Are More Likely Than Male Veterans to Be:
• Black – 28.8% vs. 15%
• Younger – 66.1% are 29 or younger vs. 57.1% of men
• Active Duty rather than Reserve Component – 54% vs. 51%
• This may or may not be a significant difference but seems to reflect historical enlistment trends
16

Dx Combined Female Male
PTSD 23% 19% 23%Non-Dependent Sub. Abuse
18% 13% 19%
Depressive Disorder 15% 20% 15%
Affective Psychosis 9% 12% 8%
Neurotic Disorder 12% 15% 12%
Alcohol Dep. 4% 2% 4%
Drug Dep. 2% 1% 2%
Personality Disorder 2% 2% 1%
Mental Health Diagnoses Among OEF/OIF Veterans By Gender
17

Factors Associated with PTSD Among 54,275 Women Veterans
• Reserve Component at greater risk than Active Duty (Odds Ratio (OR) 1.13)*
• Enlisted members at greater risk than Officers (OR 1.41)*
• Army members at greatest risk among Service Branches*
• Women older than 30 at greater risk
* Same Among Both Men and Women 18

Factors Associated with PTSD Among 54,275 Female Veterans• No clear relationship to level of education
(but if remove Rank from analyses, you find greater risk among women with less education)
• Divorced or Legally Separated Veterans at greater risk than married or single (not so for widowed)*
• No significant difference by race
* Same Among Both Men and Women19

Factors Associated with PTSD Among 398,228 Male Veterans(Differences Only)
• Men under 40 are at greater risk for PTSD• Education lower than a BA at greater risk• Single Men at significantly lower risk than
married (OR 0.76)• Black Men at greater risk and Hispanic
Men at lower risk than White Men
20
Possible Gender Issues Affecting Presentation AND Diagnosis• Women may have less exposure to
combat or may be exposed to a different range of danger situations during deployment resulting in different rates of MH diagnoses• Need to compare number, length,
frequency and intensity of deployments and/or traumatic experiences by gender
• Race, ethnicity, age or rank differences and/or differences in early life trauma among men and women may account for differing rates of dx
21

Possible Gender Issues Affecting Presentation AND Diagnosis
• Men and women may have different standards about when and how to present MH problems such that there are only apparent differences between them
• Men and women may have different concerns about the career impact of reporting a mental health problem in service or in VA
22

Possible Gender Issues Affecting Presentation AND Diagnosis
• Clinicians may have gender-specific biases in making MH diagnoses• Less likely to dx PTSD in women?• More likely to dx personality disorder
in women?• Might women OEF/OIF Veterans have
different tendencies to seek help outside of DoD and VA than men?
• Will providers outside of DoD and VA be prepared to understand and engage Women OEF/OIF Veterans?
23

Mental Health Among Female OEF/OIF Veterans
• Remember that 44% of all eligible OEF/OIF veterans presenting to VA report possible mental health problems
• Among women, 42% report possible mental health problems vs. 44% among men
24

Observations about Women OEF/OIF Veterans From SHEP, Focus Group Studies, NC CareLine Findings• Women OEF/OIF Veterans may be at
greater risk for MH problems (Based on MH component responses on SF-12) (SHEP)
• Better mental health scores were associated with more education, male gender and lower AUDIT C scores (SHEP)
• No gender differences in education in alcohol abuse (as per AUDIT C in SHEP)
• No significant difference in overall satisfaction with VA Care
• Women were, however, more satisfied than men with continuity of VA care (SHEP)
25

Observations about Women OEF/OIF Veterans From SHEP, Focus Group Studies, NC CareLine Findings• Women are concerned about possible
fertility problems related to disrupted menstrual cycles and/or exposure to environmental toxins in country (Focus)
• 34% of the 5,785 calls received by NC CareLine regarding veterans services were from women
• A Marketing Survey conducted by the American Psychoanalytic Association found that women decide who in the household will seek mental health services
26

Conclusions• Men and Women are equal but not
the same• There is a clear need for gender-
specific approaches to the readjustment and health of Women Veterans
27

28
Basic Training – Military Culture
Painting a Moving Train 28
Understanding the nature of the military culture, combat and the stresses of living and working in a war zone are critical to establishing credibility with your clients.

29
Basic Training – Military Culture
Painting a Moving Train 29
Understanding the nature of the military culture, combat and the stresses of living and working in a war zone are critical to establishing credibility with your clients.

30
Basic Training – Military Culture
• Army– Army National Guard
• Navy• Marine Corps• Air Force
– Air National Guard• Coast Guard*
Painting a Moving Train 30

31
Basic Training – Military Culture
• High standard of discipline that helps organize and structure the armed forces
• Professional ethos of loyalty and self-sacrifice that maintains order during battle
• Distinct set of ceremony and etiquette that create shared rituals and common identities
• Emphasis on group cohesion & esprit de corps that connect service members to each other.
Painting a Moving Train 31

Integration1993: Congress opens combat ships to women.1993-5: First female pilots in all branches.2005: First woman awarded the Silver Star for combat action. 2008: First woman promoted to rank of 4-star General (U.S. Army).
Women are still restricted from the following warfare specialties (with exceptions):
• Air Force: Pararescue, Combat Controllers• Army: Infantry, Armor, Artillery, Special Forces, Combat Engineering • Marine Corps: Infantry, Armor, Artillery, Combat Engineering,
Reconnaissance, Riverine Assault Craft• Navy: Submarines, SEALs
32

33
Basic Training – Military Culture
• A word about lingo…
Painting a Moving Train 33

Veterans’ Perspectives on Post-Deployment Needs:
Focus Group Results
Kristy Straits-Tröster, Ph.D., Patrick Calhoun, Ph.D., Harold Kudler, M.D.

Methods• Designed to complement medical record data
with direct input from interviews• Participants recruited by telephone to fill 6
focus groups with 12 participants each:2- Active Component (Active Duty or Separated), 2- National Guard or Reserve Component1- Female Veterans1- Female Spouses
• Informed consent obtained by investigators on site
The OEF/OIF Focus Groups

Confidential Neutral Setting

• Focus group leaders utilized a moderator’s guide
• All sessions were audiotaped and later transcribed, coded for themes
• Information collected:– Deployment Health Concerns– Family Concerns and Support– Preferences for healthcare services & info– Barriers to care– Recommendations
The OEF/OIF Focus Groups

Focus Group Participants• Time since last deployment
– Mean = 27 months (SD 11) – Most had returned 2004-2005
• 23 of 54 veterans had accessed VA services (43%)
• Most served in Army or Marines• Women veterans’ duties included Military
Police Corps, finances, laundry, pharmacy tech, supply provision, military intelligence, air support control

Health concerns while deployed--all Veterans: • Safety and effectiveness of chemoprophylaxis• Chemical exposures• Burn pit smoke exposure• Unhygienic latrines• Food safety
Women Veterans• Disrupted menstrual cycles• Exposure to prisoners and foreign animals• Sexual harrassment and assault• Combat-related fear of death
Focus Group Findings

Focus Group Findings
Post-Deployment Problems--all Veterans:• Social avoidance• Noise sensitivity, jumpiness• Anger, irritability, lack of patience• Sleep problems • Chronic joint pain • Trouble concentrating, memory lapses• Drinking or smoking too much• Personality changes, emotionally labile• Digestive and bowel problems, weight changes• Hearing loss
Women Veterans• Fertility, miscarriages• Lack of sexual interest

“I had this anger problem [after returning from deployment], the least little bitty thing I would be ready to snap. . . I’ve been on an emotional rollercoaster since I got back.”
---- Female Veteran
Focus Group Findings

Post-Deployment Family Problems—all Veterans:
• Marital problems, divorce• Dealing with distressed children and spouses• Easily angered, jumpy in family setting• Restless sleep problems • Difficulty adjusting to running household together,
being together again• Body image problems due to weight gain• Employment problems, anger at work
Women Veterans• Overprotective of children
Focus Group Findings

“I don’t think there’s enough emphasis on women coming home. Like a lot of the videos they show and things they talk about, they all show men’s problems…they don’t show women coming home that don’t look as good as they used to or that their hair is all falling out or anything. It’s all about men.
---- Female Veteran
Focus Group Findings

Services used and preferences—all Veterans:• Mixed report of VA experiences• Mixed report of TriCare experiences• Community providers confused about fee
basis process, dental • Churches helped families, prayer• Buddies helped• Working out, martial arts• Also reported drinking, smoking, driving to
relax
Women Veterans• Faith in God• Family support (especially parents)
What Helped?

• Pride, beliefs that “I should handle it”• Stigma associated with MH treatment• Concern about being “labeled” and its impact
on military promotion or security clearance• Too much red tape and paperwork• Frustrated waiting on phones, noisy waiting
areas, parking• No options outside VA • Don’t like lectures and large groups• Beliefs that treatments “don’t work anyway”
Women veterans• Being surrounded by men at the VA• Feeling guilty seeing more needy/injured
veterans• Denial
Barriers to Care

• Help dealing with anger, stress• Information about benefits and services• Job and school counseling• Marriage and family counseling
Top Five Areas of Interest

Recommendations from Veterans/Spouses:• More education after demobilization• More web-based information• Knowledgeable unit liaisons• Easier VA appointment access• More caring staff• Decrease stigma• Offer evening and weekend clinics• Use peer supports
Focus Group Findings

Web-Based Resources
• Collaborative development of self-help resources with assessment, tailored feedback, intervention and self-monitoring
• Information clearinghouses and regional resources

Focus on Self-Management

Programs on Afterdeployment.org
New programs to launch in Feb 2010



Issues Unique to Women VeteransSexual and Reproductive Issues: • Military Sexual Trauma
No one will believe me Will be branded a “slut” Still have to work with perpetrator Fear of retaliation Might be transferred to another unit or more
dangerous duty Could end military career
• Pregnancy No sex policy in theater -- punishable Intentional pregnancies, resentment Stigma-decreases manpower in combat zone
• Abortion Prohibited in military hospitals Dangerous self-abortions in combat zone

Physical Challenges of Combat Strength/endurance less than men Must work harder, prove self Weight of battle gear/ equipment/
weapons harder on female body Can’t stop for bathroom-risk of
dehydration, UTI Cleanliness during period
Issues Unique to Women Veterans

Issues Unique to Women Veterans
Psychological Challenges of Military Life Don’t show any form of weakness Segregation from men can result in less social
support and hard to develop friendships Competition/suspicion between femailes in unit Dealing with flirting, sexual advances, teasing Hard to identify best role to fit in Don’t want to stand out/ emphasize inequality Sacrificing femininity, morals, gender role beliefs
to fit in

Reintegration to Workforce--Career Challenges Women don’t benefit as much from military
service in the civilian workforce Women’s combat duty often doubted Getting used to working with women again in
civilian environment May be assumed you are lesbian or antisocial “Boys’ club” of higher echelons Greater opportunities for minority women in the
military compared to the civilian world
Issues Unique to Women Veterans

Barriers to Women’s Access to Healthcare and other services
Many don’t apply for benefits even though served in a combat zone
Don’t think of themselves as “veterans” VA hospitals and clinics have been slow to become woman-
friendly (privacy concerns, exam tables facing doors, few baby changing tables)
Homeless women veterans (over 13,000) often are parents of young children (23%)
Most resources for homeless are not geared for families and alternate versions of homelessness (friend’s couch)
Don’t want to be perceived as bad mother with PTSD Few resources for dual military couples No resources for male civilian spouses
Issues Unique to Women Veterans

TRICAREYour Military Health Plan
PP
411B
EC
1106
3W
Introduction to TRICARE
Presented by Health Net Federal Services
Brian Corlett, TRICARE Service Center Manager

What is TRICARE?• Health care program for 9.2 million
military beneficiaries – active duty, retired, families
• Integrated health care delivery system– Military treatment facilities (MTFs)– Civilian health care facilities
• TRICARE Prime
• TRICARE Extra
• TRICARE Standard
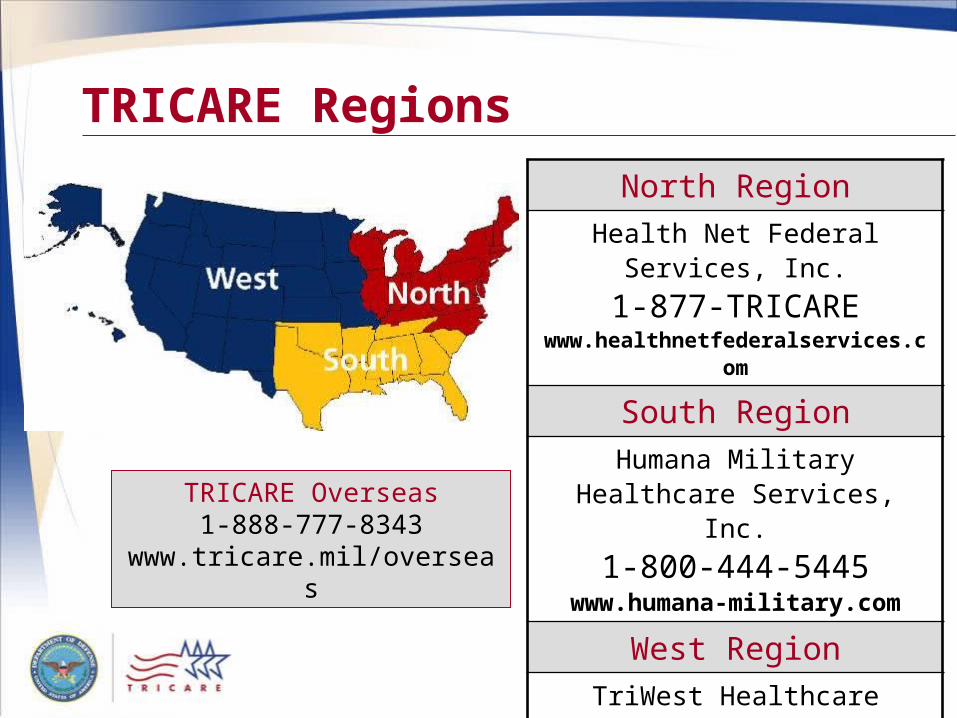
TRICARE Regions
North RegionHealth Net Federal Services,
Inc.1-877-TRICARE
www.healthnetfederalservices.com
South RegionHumana Military Healthcare
Services, Inc.1-800-444-5445
www.humana-military.com
West RegionTriWest Healthcare Alliance
1-888-TRIWESTwww.triwest.com
TRICARE Overseas1-888-777-8343
www.tricare.mil/overseas

TRICARE Prime• Comparable to an HMO
• Enrollment required
• Most care received from or through primary care manager
• Referrals for all specialty care
• Pre-negotiated rates to providers

TRICARE Standard• Enrollment not required
• Care from non-network TRICARE-authorized providers or TRICARE network providers
• Referrals not required for specialty care
• Some services may require prior authorization
TRICARE Extra• Functions more like PPO
• Similar to TRICARE Standard
• Care encouraged from TRICARE network providers– Lower cost-shares than TRICARE Standard– Providers accept TRICARE negotiated rate

TRICARE Pharmacy Program• Available to all eligible beneficiaries
• Large, uniform formulary
• Affordable costs to beneficiaries
• Local pharmacy providers (network and non-network), mail order, military treatment facility
Visit www.tricare.mil/pharmacy for more information.

TRICARE
• Myth – TRICARE involvement is a long, difficult process for providers
• Reality – TRICARE provider participation involves a simple form and less that 1 month for acceptance (TRICARE Prime requires longer period of time and a signed contract.)

TRICARE
• Myth – TRICARE reimbursement is slow
• Reality – TRICARE electronic reimbursement usually occurs within 30 day of submission

TRICARE
• Myth – TRICARE pays less to providers than Medicare reimbursement
• Reality – TRICARE reimbursement is tied to Medicare rates – TRICARE Prime pays slightly less than Medicare

TRICAREYour Military Health Plan
PP
411B
EC
1106
3W
1
TRICAREYour Military Health Plan
Behavioral Health Care Services
BR
4128
02B
ET
0505
W

TRICARE: Behavioral Health Care ServicesVersion 2 (Revision: 05/31/05)
TRICARE Prime Beneficiaries(Except Active Duty)• Entitled to eight (8) initial outpatient
visits per fiscal year (Oct. 1–Sept. 30)
• No prior authorization required
• No primary care manager (PCM) referral is needed
• Must seek care from a TRICARE network provider
• Prior authorization is required after the eighth (8th) visit
BR
4128
02B
ET
0505
W

TRICARE: Behavioral Health Care ServicesVersion 2 (Revision: 05/31/05)
TRICARE Standard andTRICARE Extra Beneficiaries
• No referrals required for any outpatient visits
• Entitled to eight (8) initial outpatient visits per fiscal year without authorization
• Prior authorization is required after the eighth (8th) visit
• Seeking care from a TRICARE network provider will reduce the patients out-of-pocket costs
BR
4128
02B
ET
0505
W

TRICARE: Behavioral Health Care ServicesVersion 2 (Revision: 05/31/05)
Behavioral Health Care Providers• Psychiatrists (M.D., D.O.)• Clinical Psychologists (Ph.D.)• Certified psychiatric nurse specialists (PNS)• Master’s-level clinical social workers (LCSW)• Certified marriage and family therapists (LMFT)• Licensed Professional Counselors (LPC’s) *
*with physician referral and supervision
All providers require a Medicare # except LMFT’s & LPC’s
PA’s & NP’s are not recognized TRICARE Behavioral Provider’s and cannot bill codes 90801-90899
BR
4128
02B
ET
0505
W

TRICARE: Behavioral Health Care ServicesVersion 2 (Revision: 05/31/05)
TRICARE Covered Outpatient Services
• Outpatient Services– Individual Therapy– Family Therapy– Collateral Visits– Play Therapy– Psychoanalysis*– Psychological Testing (max. 6 unit
benefit/yr)*
*Prior authorization required
Prior auth not required for Psych Testing, but providers need to verify yearly limit has not been exhausted.
BR
4128
02B
ET
0505
W

TRICARE: Behavioral Health Care ServicesVersion 2 (Revision: 05/31/05)
TRICARE Covered Inpatient Services
• Inpatient Services– Acute Inpatient Psychiatric Care
• Ages 19+ (30 day IP limit per fiscal year)• Ages 18 and below (45 day IP limit per fiscal year)
– Psychiatric Partial Hospitalization (60 day limit)– Residential Treatment Center (RTC) Care (150 day
limit)– Substance Abuse*
• Detoxification (7 day limit)• Rehabilitation (21 day limit)
* Substance Abuse days cont toward yearly IP limit
BR
4128
02B
ET
0505
W

8TRICARE: Behavioral Health Care ServicesVersion 2 (Revision: 05/31/05)
Overview of Costs and Fees
BR
4128
02B
ET
0505
W
N/A$0$0TPR/TPRADFM
Cost-share after deductible is met25% of allowable charge
Cost-share after deductible is met20% of negotiated rate
N/AStandard
Cost-share after deductible is met20% of allowable charge
Cost-share after deductible is met 15% of negotiated rate
N/AExtra
No deductible$25 copayment
No deductibleNo copayment
$0Prime
Retirees and othersActive Duty Family Member
Active Duty Costs
Program
N/A$0$0TPR/TPRADFM
Cost-share after deductible is met25% of allowable charge
Cost-share after deductible is met20% of negotiated rate
N/AStandard
Cost-share after deductible is met20% of allowable charge
Cost-share after deductible is met 15% of negotiated rate
N/AExtra
No deductible$25 copayment
No deductibleNo copayment
$0Prime
Retirees and othersActive Duty Family Member
Active Duty Costs
Program

TRICAREYour Military Health Plan
PP
411B
EC
1106
3W
TRICARE Reserve Select
Available October 1, 2007New Rates Effective 1-1-2010

TRICARE Reserve Select (TRS)• Premium-based health plan that
qualified National Guard and Reserve members may purchase for duration of service
• Similar coverage to TRICARE Standard and TRICARE Extra
• Monthly premium payment (DoD pays 72%) is $49.62 for member or $197.65 for family
• Coverage for survivors may continue 6 months after member’s death

In Conclusion…• TRICARE is an insurance provider for a large
cadre of the patient population – the entire military community and families
• TRICARE may be the only health insurance for a whole population component, dependent on their military service status
• TRICARE is mandated to provide coverage to the military community and is dependent on civilian providers to do so
• www.tricare.mil
Call to Action

Beyond the DoD/VA Continuum
• Ideally MH problems among OEF/OIF veterans of either gender will be picked up somewhere within the DoD/VA continuum of care but:– If only 40% of All OEF/OIF Veterans
eligible for VA care have come to VA where are the other 60%?
• There is a “silent majority” of OEF/OIF veterans not coming to VA
80

Comparison to the National Vietnam Veterans Readjustment Study
• Only 20% of the Vietnam Veterans with PTSD at the time of the study had EVER gone to VA for Mental Health Care yet:
• 62% of all Vietnam Veterans with PTSD had sought MH care at some point
Kulka et al. 1990 p. 228
81

Thinking About The Silent Majority• Who among them do we want to reach?• What intervention(s) would be most
appropriate?• How would we reach these veterans?• At what point do we reach them?• What about their families?
– Family support predicts resilience– Families have needs of their own
• Are there gender differences among them?82

Public Health Model• Most war fighters/veterans will not
develop a mental illness but all war fighters/veterans and their families face important readjustment issues
• This population-based approach is less about making diagnoses than about helping individuals and families retain a healthy balance despite the stress of deployment
83

Public Health Model• The public health approach requires a
progressively engaging, phase-appropriate integration of services
• This program must: – Be driven by the needs of the Service Member/
veteran and his/her family rather than by DoD and VA traditions
– Meet prospective users where they live rather than wait for them to find their way to the right mix of our services
– Increase access and reduce stigma
84

The Public Health Model and Women Veterans• Women may face different stigmata
then do men• Might women OEF/OIF have different
tendencies to seek help outside of DoD and VA than men?
• Will providers outside of DoD and VA be prepared to understand and engage women OEF/OIF veterans?
85

Next Steps• Further analyses to adjust for
demographics and trauma exposure• Expand gender-specific needs
assessment and outreach among Service Members, Veterans and providers
• Develop gender-informed provider training, outreach and treatment
• Study/Address gender-specific stigma• Transform the post deployment
health system
86

QUESTIONS?

Contact InformationHarold Kudler, M.D.
Elizabeth Marks [email protected]
Erin Simmons, Ph.D., LCDR. MSC, USN
Kristy Straits-Troster, Ph.D. , [email protected]
88

LIONESSA feature documentary by
Meg McLagan and Daria Sommers
The story of five women soldiers who served together for a year in Iraq and returned home as part of this country’s first generation
of women combat veterans.
To order LIONESS on dvd go to:
www.lionessthefilm.com
To inquire about screenings contact:
LIONESS © Copyright Team Lioness LLC