ISSUE 2 Infl ammation and Pain Control in Cataract...
9
To obtain CME credit for this activity, go to http://cme.ufl.edu/toai Supported by an unrestricted educational grant from Bausch + Lomb, Inc. Inflammation and Pain Control in Cataract Surgery e human eye has evolved to be relatively intolerant of inflammation: the clarity of media and the integrity of ocular microstructures are jeopardized by the swelling and release of chemical mediators that characterize the body’s inflammatory response. 1 Among ocular tissues, the uvea (the iris, ciliary body, and choroid) mounts the most pronounced inflamma- tory response—and even routine, uneventful cataract surgery cases involve some uveal trauma, typically at the ciliary body. Of particular visual importance is the cornea, which can become edematous and lose clarity with the inflammation induced by cataract surgery. is trauma initiates the release of cell membrane phos- pholipids that trigger the arachidonic acid-mediated inflam- matory cascade, leading to the formation of prostaglandins. Prostaglandins cause vasodilation and increased vascular permeability, as well as iris smooth muscle constriction. 2 Corticosteroids inhibit the formation of prostaglandins early in the cascade—by blocking the enzyme phospholipase A2, which is required for the initial release of phospholipids. Nonsteroidal antiinflammatory drugs (NSAIDs) act later in the cascade, blocking the cyclooxygenase enzymes required for prostaglandin synthesis. 2 e clinical and visual consequences of uncontrolled post- operative inflammation can be significant, and antiinflamma- tory drug therapy has long been a mainstay of postoperative management in cataract surgery, as has the off-label preop- erative use of these drugs. e ultimate outcome of cataract surgery depends as much on the patient’s healing response as on the procedure itself, making modulation of that response a critical part of the overall surgical process. Surgeons’ abil- ity to modulate that healing depends upon two things: drug selection and patient cooperation. EVOLVING SURGERY AND EXPECTATIONS Cataract surgery has evolved steadily over the last few decades, becoming safer and less traumatic as the years have FIGURE 1 Injection and anterior chamber inflammation 1 day after cataract surgery. (Image courtesy of Uday Devgan, MD.) ISSUE 2 UDAY DEVGAN, MD, FACS, FRCS Although a continuous series of incremental improvements in surgical technology has made cataract extraction less traumatic than ever before, tissue manipulation remains significant enough to trigger an inflammatory response. Cautious prophylaxis and tight control of inflammation in the early postoperative period improves patients’ subjective experience and reduces the risk of vision-threatening inflammatory sequelae. A CONTINUING MEDICAL EDUCATION PUBLICATION CME C O NTINUIN G M ED IC A L E D U C A TIO N
Transcript of ISSUE 2 Infl ammation and Pain Control in Cataract...
To obtain CME credit for this activity, go to http://cme.ufl .edu/toai Topics in OCULAR ANTIINFLAMMATORIES 1Supported by an unrestricted educational grant from Bausch + Lomb, Inc.
Infl ammation and Pain Control in Cataract Surgery
� e human eye has evolved to be relatively intolerant of in� ammation: the clarity of media and the integrity of ocular microstructures are jeopardized by the swelling and release of chemical mediators that characterize the body’s in� ammatory response.1 Among ocular tissues, the uvea (the iris, ciliary body, and choroid) mounts the most pronounced in� amma-tory response—and even routine, uneventful cataract surgery cases involve some uveal trauma, typically at the ciliary body. Of particular visual importance is the cornea, which can become edematous and lose clarity with the in� ammation induced by cataract surgery.
� is trauma initiates the release of cell membrane phos-pholipids that trigger the arachidonic acid-mediated in� am-matory cascade, leading to the formation of prostaglandins. Prostaglandins cause vasodilation and increased vascular permeability, as well as iris smooth muscle constriction.2 Corticosteroids inhibit the formation of prostaglandins early in the cascade—by blocking the enzyme phospholipase A2, which is required for the initial release of phospholipids.
Nonsteroidal antiin� ammatory drugs (NSAIDs) act later in the cascade, blocking the cyclooxygenase enzymes required for prostaglandin synthesis.2
� e clinical and visual consequences of uncontrolled post-operative in� ammation can be signi� cant, and antiin� amma-tory drug therapy has long been a mainstay of postoperative management in cataract surgery, as has the o� -label preop-erative use of these drugs. � e ultimate outcome of cataract surgery depends as much on the patient’s healing response as on the procedure itself, making modulation of that response a critical part of the overall surgical process. Surgeons’ abil-ity to modulate that healing depends upon two things: drug selection and patient cooperation.
EVOLVING SURGERY AND EXPECTATIONSCataract surgery has evolved steadily over the last few
decades, becoming safer and less traumatic as the years have
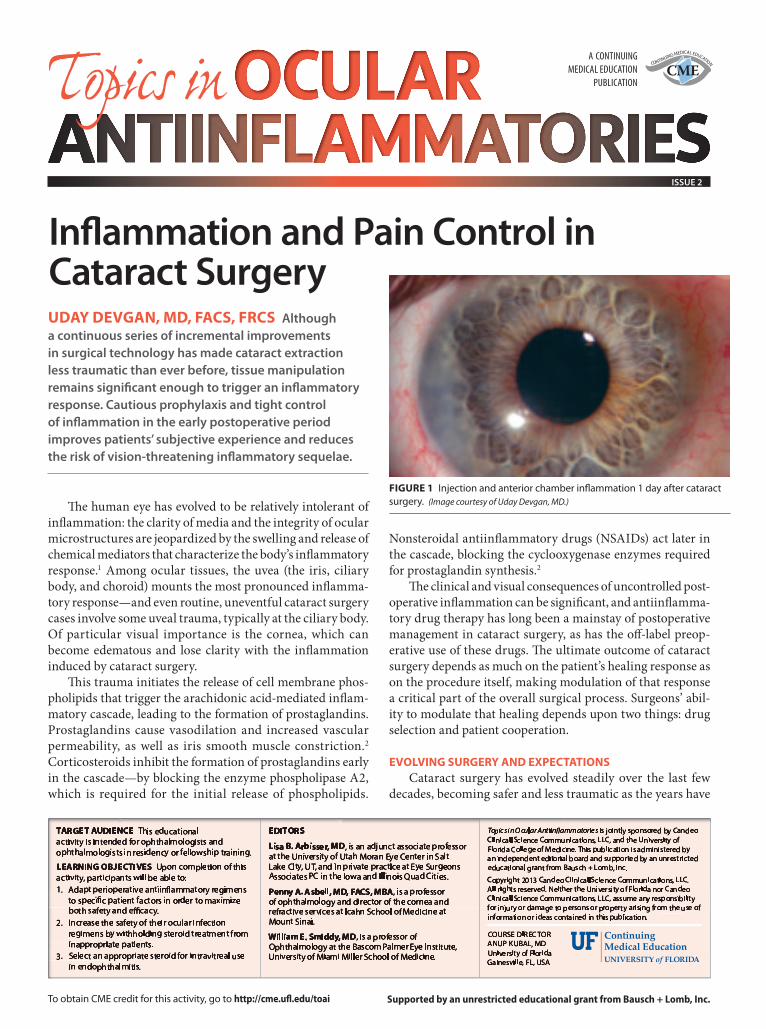
FIGURE 1 Injection and anterior chamber infl ammation 1 day after cataract surgery. (Image courtesy of Uday Devgan, MD.)
ISSUE 2
UDAY DEVGAN, MD, FACS, FRCS Although a continuous series of incremental improvements in surgical technology has made cataract extraction less traumatic than ever before, tissue manipulation remains signifi cant enough to trigger an infl ammatory response. Cautious prophylaxis and tight control of infl ammation in the early postoperative period improves patients’ subjective experience and reduces the risk of vision-threatening infl ammatory sequelae.
A CONTINUINGMEDICAL EDUCATION
PUBLICATIONCME
CONTINUING MEDICAL EDUCATION

2 Topics in OCULAR ANTIINFLAMMATORIES To obtain CME credit for this activity, go to http://cme.ufl .edu/toai
STATEMENT OF NEEDThe indications for topical ophthalmic antiinfl ammatory drugs (both steroidal and nonsteroidal) are evolving rapidly, as new agents and new applications emerge. Many of these are novel—eg, the perioperative use of nonsteroidal antiinfl ammatory drugs (NSAIDs) to prevent cystoid macular edema—and/or fl y in the face of older thinking—eg, the use of steroids to calm infl ammation and reduce the risk of melting or scarring from infection. Neither of these important applications is on-label.
In addition, new steroidal and nonsteroidal agents continue to come to market, expanding the utility of both classes. Antiinfl ammatory drugs are now used for: the treatment of ocular surface disease and allergic conjunctivitis; prevention of perioperative pain and infl ammation in ocular surgery; infection management; cystoid macular edema prophylaxis following cataract surgery; haze prevention in PRK; and much more.
What has regrettably not followed this expansion of indications, formulations, and new molecular entities are protocols for drug selection and use.1 These are vital because signifi cant diff erences in safety, tolerability, and effi cacy exist between and within both antiinfl ammatory drug classes. C-20 ester steroids, for example, have a demonstrated lower risk of intraocular pressure (IOP) elevation than ketone steroids.2,3 Since a range of steroid formulations and concentrations is available, clinicians need up-to-date information about the indications and optimum uses for each.3
Although topical NSAID formulations have been associated with signifi cant adverse events (keratopathy ranging from superfi cial punctate keratitis to corneal melt), recent work shows these to be uncommon and less severe with newer formulations.4 Indeed, novel NSAIDs make use of lower concentrations and less frequent dosing, potentially impacting safety profi les and reducing risk from long-term use.5
Although both are “antiinfl ammatory,” steroids and NSAIDs act at diff erent points in the infl ammatory cascade, and thus off er opportunities for physicians to fi ne-tune their drug selection. And although they are frequently used together, whether or not the two drug classes can act synergistically is controversial. In the context of recent clinical data, a clear mechanistic understanding of each drug class generally—and of newer formulations specifi cally—will equip clinicians to make eff ective, evidence-based prescribing decisions across the many situations that call for ocular infl ammation control.
REFERENCES1. Dua HS, Attre R. Treatment of post-operative
infl ammation following cataract surgery —a review. European Ophthalmic Review. 2012;6(2):98-103.
2. Comstock TL, DeCory H. Advances in corticosteroid therapy for ocular infl ammation: loteprednol etabonate. International Journal of Infl ammation. 2012; doi:10.1155/2012/789623.
3. Fong R, Leitritz M, Siou-Mermet R, Erb T. Loteprednol etabonate gel 0.5% for postoperative pain and infl ammation after cataract surgery: results of a multicenter trial. Clin Ophthalmol. 2012;6:1113-24.
4. Singer M, Cid MD, Luth J, et al. Incidence of corneal melt in clinical practice: our experience vs a meta-analysis of the literature. Clin Exp Ophthalmol. 2012;S1:003.
5. Cable M. Comparison of bromfenac 0.09% QD to nepafenac 0.1% TID after cataract surgery: pilot evaluation of visual acuity, macular volume, and retinal thickness at a single site. Clin Ophthalmol. 2012;6:997-1004.
OFFLABEL USE STATEMENT This work discusses off -label uses of antiinfl ammatory medications.
GENERAL INFORMATION This CME activity is sponsored by the University of Florida College of Medicine and is supported by an unrestricted educational grant from Bausch + Lomb, Inc.
Directions: Select one answer to each question in the exam (questions 1–10) and in the evaluation (questions 11–16). The University of Florida College of Medicine designates this activity for a maximum of 1.0 AMA PRA Category 1 Credit™. There is no fee to participate in this activity. In order to receive CME credit, participants should read the report, and then take the posttest. A score of 80% is required to qualify for CME credit. Estimated time to complete the activity is 60 minutes. On completion, tear out or photocopy the answer sheet and send it to:
University of Florida CME Offi cePO Box 100233, Gainesville, FL 32610-0233PHONE: 352-733-0064 FAX: 352-733-0007
Or you can take the test online at http://cme.ufl .edu/toaiSystem requirements for this activity are: For PC users: Windows® 2000, XP, 2003 Server, or Vista; Internet Explorer® 6.0 or newer, or Mozilla® Firefox® 2.0 or newer (JavaScript™ and Java™ enabled). For Mac® users: Mac OS® X 10.4 (Tiger®) or newer; Safari™ 3.0 or newer, Mozilla® Firefox® 2.0 or newer; (JavaScript™ and Java™ enabled).
Internet connection required: Cable modem, DSL, or better.
DATE OF ORIGINAL RELEASE September 2013. Approved for a period of 12 months.
ACCREDITATION STATEMENT This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of the University of Florida College of Medicine and Candeo Clinical/Science Communications, LLC. The University of Florida College of Medicine is accredited by the ACCME to provide continuing medical education for physicians.
CREDIT DESIGNATION STATEMENT The University of Florida College of Medicine designates this enduring material for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should only claim the credit commensurate with the extent of their participation in the activity.
FACULTY AND DISCLOSURE STATEMENTS Lisa B. Arbisser, MD (Faculty Advisor), is an adjunct associate professor at the University of Utah Moran Eye Center in Salt Lake City, UT, and an ophthalmologist at Eye Surgeons Associates PC in Bettendorf, IA. She states that in the past 12 months, she has participated in a stand-alone Bausch + Lomb advisory board meeting.
Penny A. Asbell, MD, FACS, MBA (Faculty Advisor), is a professor of ophthalmology and director of the cornea and refractive services at Icahn School of Medicine at Mount Sinai. She states that in the past 12 months, she has been as consultant for R-tech, Senju, and Bausch + Lomb, has given CME lectures for Merck, and has received a research grant from Alcon.
William E. Smiddy, MD (Faculty Advisor), is a professor of Ophthalmology at the Bascom Palmer Eye Institute, University of Miami Miller School of Medicine. He states that in the past 12 months, he has attended a steering committee meeting of Alimera Scientifi c.
Uday Devgan, MD, FACS, FRCS, practices at Devgan Eye Surgery, serves as chief of ophthalmology at Olive View UCLA Medical Center, and is associate clinical professor at the Jules Stein Eye Institute at the University of California, Los Angeles, School of Medicine. He reports the following fi nancial disclosures in the past 12 months: consultant to Aaren, Alcon, Bausch + Lomb, Gerson Lehman, LensGen, Omeros, and Optimedia; speaker for Alcon, Bausch + Lomb, Slack/OSN; stockholder in Specialty Surgical; and royalties from Accutome.
Thomas M. Lietman, MD, is Pearl and Samuel Kimura Professor of ophthalmology and professor of epidemiology and biostatistics at the University of California, San Francisco (UCSF) in San Francisco, CA. He is also the Director of the Proctor International Center and Associate Director of the F. I. Proctor Foundation, UCSF. He states that in the past 12 months, he has not had a fi nancial relationship with any commercial organization that produces, markets, re-sells, or distributes healthcare goods or services consumed by or used on patients.
John D. Sheppard, MD, is professor of ophthalmology, clinical director of the Lee Center for Ocular Pharmacology at Eastern Virginia Medical School. He is also Medical Director of the Lions Eye Bank, and president of Virginia Eye Consultants. He states that in the past 12 months, he has been a consultant and speakers bureau member for Alcon, Allergan, Abbott , Bausch + Lomb, and Merck.
DISCLAIMER Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and professional development. The information presented in this activity is not meant to serve as a guideline for patient care. Procedures, medications, and other courses of diagnosis and treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patients’ conditions and possible contraindications or dangers in use, applicable manufacturer’s product information, and comparison with recommendations of other authorities.
COMMERCIAL SUPPORTERS This activity is supported by an unrestricted educational grant from Bausch + Lomb, Inc.
TOPICS IN OCULAR ANTIINFLAMMATORIES, ISSUE 2
gone by. The incision size required for extracapsular cataract extraction was cut in half with the advent of phacoemulsi� cation, and advances in intraocular lens (IOL) technology have allowed surgery to be performed with even smaller incisions.3
In addition, phacoemulsification technology and surgical technique have bene� ted from a continuous stream of incremental re� nements. � ese have, for example, reduced the amount of ultrasound energy available to do col-lateral damage to delicate tissues in the vicinity of the lens, most notably the corneal endothelium. This has been accomplished by, among other things, delivering ultrasound in smaller pulses of energy, remaining e� ective but mini-mizing tissue trauma.3
� e advent of femtosecond laser-assis ted cataract surgery has the poten-tial to reduce the phaco energy delivered to the eye still further by using precisely targeted laser energy to pre-fragment or so� en the lens; it may even be possible to reduce ultrasound time to near zero in some cases.4 As experience with femto-second technology grows, we will be able to compare the impact of various laser fragmentation patterns on phaco energy use and determine whether the technol-ogy can produce a meaningful reduction in postoperative in� ammation.
� e � ip side of better outcomes from less traumatic surgery is a heightened level of patient expectations. � e days when a long recovery from cataract sur-gery was the norm are over, and patients now expect to enjoy LASIK-like results from cataract surgery on postoperative day 1. For surgeons to deliver on these expectations requires not only excel-lent surgical technique but also highly e� ective management of healing and in� ammation.
CLINICAL FEATURES Typical signs of inflammation in
the immediate postoperative period are cells and � are in the anterior chamber, which is evidence of compromise to the blood-aqueous barrier (Figure 1). Symp-toms a� er a routine cataract procedure are, fortunately, typically manageable, and pain tends to be low. Patients o� en
To obtain CME credit for this activity, go to http://cme.ufl .edu/toai Topics in OCULAR ANTIINFLAMMATORIES 3
risk cases. For all my cataract patients, I prescribe preoperative medications (including NSAID, steroid, and an antibiotic) starting 3 days before surgery. First, this helps to ensure a steady state of drug in the anterior chamber. Some of the available NSAIDs, particularly those that are dosed once a day, are long-acting, and a couple of doses may help to achieve a su� cient level of drug.
In addition, starting drugs 3 days out helps ensure my patients obtain their medications and get into the habit of us-ing them before their lives are disrupted by the surgery. If a patient is scheduled for surgery on a Monday, one of the days on which I typically operate, I do not want him to wait until Sunday to drop o� his prescription, only to � nd it cannot be � lled same-day. Requiring the patient to � ll the prescription on Friday increases the likelihood of our getting prophylactic drops into the eye as planned.
In selecting agents for inf lammation control around cataract surgery, I evaluate e� cacy, safety, and complexity of dosing regimen. I have streamlined my own perioperative medication regimens into two channels: one for patients who are able to purchase brand-name drugs, and one for patients who need generics. I help patients understand that there are di� erences between the two, and I provide a straightforward and simple reference form for each regimen downloadable from my practice’s website.
DRUG SELECTION: STEROIDTopical corticosteroids have long been a mainstay of
post-cataract surgery in� ammation control. A range of drugs and formulations are available today, each with risk/bene� t pro� les that should be evaluated for individual patients. � e
report general soreness and a feeling of fatigue about the eye and periocular area, as well as some degree of light sensitivity, due to uveal in� ammation.
Indeed, pain scores are among standard measures of ef-� cacy in clinical trials of topical ophthalmic antiin� ammatory drugs; and while the use of a study drug tends to result in more pain-free subjects than placebo, a striking proportion of the untreated placebo group experience no pain.5,6 Beyond discomfort, the potential consequences of uncontrolled post-cataract surgery in� ammation, including cystoid macular edema (CME) and posterior capsular � brosis, can negatively impact postoperative vision.7
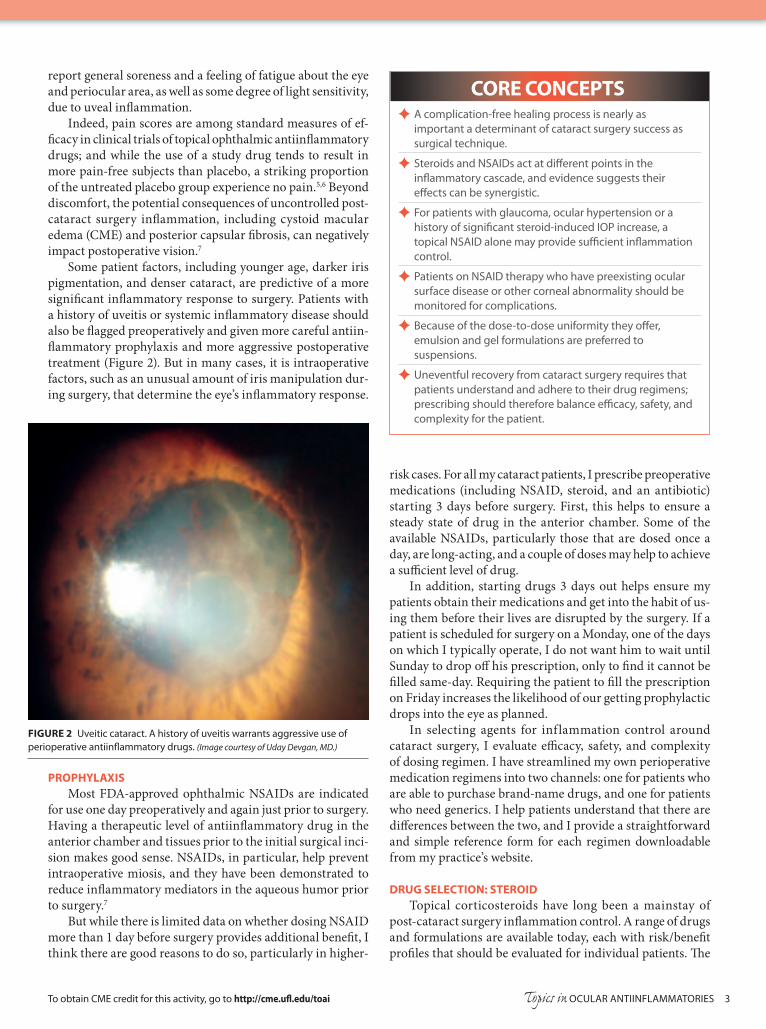
Some patient factors, including younger age, darker iris pigmentation, and denser cataract, are predictive of a more signi� cant in� ammatory response to surgery. Patients with a history of uveitis or systemic in� ammatory disease should also be � agged preoperatively and given more careful antiin-� ammatory prophylaxis and more aggressive postoperative treatment (Figure 2). But in many cases, it is intraoperative factors, such as an unusual amount of iris manipulation dur-ing surgery, that determine the eye’s in� ammatory response.
PROPHYLAXISMost FDA-approved ophthalmic NSAIDs are indicated
for use one day preoperatively and again just prior to surgery. Having a therapeutic level of antiin� ammatory drug in the anterior chamber and tissues prior to the initial surgical inci-sion makes good sense. NSAIDs, in particular, help prevent intraoperative miosis, and they have been demonstrated to reduce in� ammatory mediators in the aqueous humor prior to surgery.7
But while there is limited data on whether dosing NSAID more than 1 day before surgery provides additional bene� t, I think there are good reasons to do so, particularly in higher-
CORE CONCEPTS ✦ A complication-free healing process is nearly as
important a determinant of cataract surgery success as surgical technique.
✦ Steroids and NSAIDs act at diff erent points in the infl ammatory cascade, and evidence suggests their eff ects can be synergistic.
✦ For patients with glaucoma, ocular hypertension or a history of signifi cant steroid-induced IOP increase, a topical NSAID alone may provide suffi cient infl ammation control.
✦ Patients on NSAID therapy who have preexisting ocular surface disease or other corneal abnormality should be monitored for complications.
✦ Because of the dose-to-dose uniformity they off er, emulsion and gel formulations are preferred to suspensions.
✦ Uneventful recovery from cataract surgery requires that patients understand and adhere to their drug regimens; prescribing should therefore balance effi cacy, safety, and complexity for the patient.
FIGURE 2 Uveitic cataract. A history of uveitis warrants aggressive use of perioperative antiinfl ammatory drugs. (Image courtesy of Uday Devgan, MD.)

4 Topics in OCULAR ANTIINFLAMMATORIES To obtain CME credit for this activity, go to http://cme.ufl .edu/toai
potency of “strong” steroids, such as prednisolone acetate, di� uprednate, and dexamethasone, is balanced by a higher risk of intraocular pressure (IOP) increases, as compared to steroids such as loteprednol etabonate and � uorometholone. However, this dose- and duration-dependant e� ect can be mitigated by careful patient selection and using the briefest e� ective duration of therapy.8
Steroid formulation is also an important consideration, particularly in the early postoperative period. Many topical ophthalmic steroids are formulated as suspensions, which require vigorous shaking prior to use in order to ensure that active drug, as well as the vehicle, is instilled in the eye.
Research measuring actual drug concentrations in drops of ophthalmic steroid suspensions, dispensed a� er shaking or failing to shake the bottle, has shown that concentrations can vary wildly—even a� er shaking for 5 seconds, drops of branded prednisolone acetate 1% were within 15% of the declared concentration less than half of the time.9 So when prescribing suspension formulations, clear and emphatic patient instruction is required. I like to use the analogy of an oil-and-vinegar salad dressing: it only tastes right when shaken vigorously immediately before pouring.
Two fairly recently introduced topical steroid formulations overcome this problem: di� uprednate 0.05% is formulated as an emulsion, and loteprednol etabonate 0.5% is available as a gel. Both o� er consistent and uniform dosing.9,10 Loteprednol etabonate 0.5% is also available as an ointment; but while ointments do not require shaking, they are di� cult to place properly in the eye (especially for older and less dexterous patients) and may cause visual blurring. � e gel formulation of loteprednol etabonate is very well tolerated by patients and is not associated with signi� cant visual blurring.
Because they operate at di� erent points on the in� am-matory cascade, topical steroids and NSAIDs appear to have synergistic antiin� ammatory e� ects, and studies have shown additional bene� t from adding an NSAID to the postoperative steroid regimen—even in patients considered at low risk for in� ammatory complications like CME.11 Combining the two may also allow for a shorter duration of steroid treatment, thus limiting the associated risks.
DRUG SELECTION: NSAIDIn a topical NSAID, I look for a newer-generation product
with a good record of e� cacy in randomized, placebo-con-trolled trials. Success in a clinical trial, in which the NSAID is the only antiin� ammatory medication provided to the patient, is a good predictor of success in a real-world setting, in which a corticosteroid is available to augment the NSAID’s antiin� ammatory action.
Good corneal penetration is critical for NSAID e� cacy a� er cataract surgery. In� ammation control is most needed in the anterior chamber—not on the ocular surface—and though they are rare, the adverse e� ects most worrisome with NSAID use involve the cornea, ranging from punctate keratitis to corneal melt.12
Advances in NSAID development have therefore focused
on enhancing penetration into the eye as well as potency (ability to bind the cyclooxygenase enzymes and inhibit pros-taglandin synthesis). Nepafenac ophthalmic suspension (0.3% or 0.1%) is a pro-drug, which is hydrolyzed a� er penetrating the cornea into the more potent amfenac, achieving good drug concentration in target tissues of the anterior chamber and leaving little on the surface.7
Bromfenac ophthalmic solution (0.09%) is another potent NSAID which has been available in the United States since 2005. � e bromfenac molecule is structurally similar to am-fenac, but it is distinguished by halogenation with a bromine atom, which improves its potency.13 A new ophthalmic formu-lation of bromfenac has recently been approved with a lower concentration of drug (0.07%) and a lower pH (7.8, reduced from 8.3), increasing the drug’s penetration into the anterior chamber and resulting in higher levels of drug in the iris and ciliary body than are achieved with the higher concentration.14
SPECIAL CONSIDERATIONSRisk factors for a signi� cant IOP increase in response
to steroid therapy include history of glaucoma or glaucoma suspects, older age, a � rst-degree family history of primary open-angle glaucoma, and high myopia.8 Patients with a history of glaucoma or ocular hypertension should be given steroid therapy only in a controlled and cautiously monitored manner. For such patients in my own practice, I may consider giving only NSAID therapy to resolve postoperative in� am-mation, or perhaps a very brief (3-day) course of steroids fol-lowed by prolonged NSAID treatment. Even in non-steroid responders, because I routinely put patients on both a steroid and an NSAID a� er cataract surgery, I o� en reduce the steroid dosing from the labeled 4 drops/day regimen to just twice a day, particularly if the surgery was uneventful.
Similarly, while the risks are low for serious corneal com-plications with topical NSAIDs, patients with preexisting ocu-lar surface disease, as well as those with diabetes or rheumatoid arthritis, may warrant greater care and close monitoring on NSAID therapy—or may be provided steroid therapy alone.15
Intraocular lens selection can also in� uence antiin� am-matory protocols, with some models being more susceptible to refractive changes with capsular bag � brosis and contraction. Again, to keep things simple and to maximize in� ammation control for my patients, I provide a uniform set of postoperative regimens for most of my patients. But in some cases, as with an accommodating IOL that requires precise centration and po-sitioning to perform well, greater antiin� ammatory coverage may provide additional protection against capsular � brosis, which could shi� the lens position. Likewise, multifocal IOLs are especially sensitive to optical aberrations of the corneal surface or visual distortions due to swelling in the macula; so the stakes may be somewhat higher for in� ammation control with advanced-technology IOLs.
CONCLUSIONDevising a pre- and postoperative antiinf lammatory
regimen for cataract surgery involves balancing drug potency,

To obtain CME credit for this activity, go to http://cme.ufl .edu/toai Topics in OCULAR ANTIINFLAMMATORIES 5
safety, real-world e� cacy, and ease of administration. Patient compliance with postoperative medications tends to be highest in the � rst week a� er surgery, when the experience and physi-cian instructions are freshest in the mind. Helping patients understand that the eye continues to heal and recover from cataract surgery well a� er the immediate discomfort has sub-sided—and making them feel invested in their postoperative care—are essential to ensuring the procedure’s ultimate success.
Uday Devgan, MD, FACS, FRCS, practices at Devgan Eye Surgery, serves as chief of ophthalmology at Olive View UCLA Medical Center, and is associate clinical professor at the Jules Stein Eye Institute at the University of California, Los Angeles, School of Medicine. He reports the following fi nancial disclosures in the past 12 months: consultant to Aaren, Alcon, Bausch + Lomb, Gerson Lehman, LensGen, Omeros, and Optimedia; speaker for Alcon, Bausch + Lomb, Slack/OSN; stockholder in Specialty Surgical; and royalties from Accutome. Managing editor Jennifer Zweibel assisted in the preparation of this article.
REFERENCES 1. Streilein WJ. Ocular immune privilege: the eye takes a dim but practical view
of immunity and infl ammation. J Leukocyte Biol. 2003;74:179-85. 2. Ahuja M, Dhake AS, Sharma SK, et al. Topical ocular delivery of NSAIDs.
AAPS J. 2008 April. http://link.springer.com/article/10.1208/s12248-008-9024-9/fulltext.html Accessed July 24 2013.
3. Devgan U. Surgical techniques in phacoemulsifi cation. Curr Opin Ophthalmol. 2007;18:19-22.
4. Abell RG, Kerr NM, Vote BJ. Toward zero eff ective phacoemulsifi cation time using femtosecond laser pretreatment. Ophthalmology. 2013;120:942-8.
5. Donnenfeld ED, Holland EJ, Stewart RH, et al. Bromfenac ophthalmic solution 0.09% (Xibrom) for postoperative ocular pain and infl ammation. Ophthalmology. 2007;114:1653-62.
6. Fong R, Leitritz M, Siou-Mermet R, et al. Loteprednol etabonate gel 0.5% for postoperative pain and infl ammation after cataract surgery: results of a multicenter trial. Clin Ophthalmol. 2012;6:1113-24.
7. Walters T, Raizman M, Ernest P, et al. In vivo pharmacokinetics and in vitro pharmacodynamics of nepafenac, amfenac, ketorolac, and bromfenac. J Cataract Refract Surg. 2007;33:1539-45.
8. Kersey JP, Broadway DC. Corticosteroid-induced glaucoma: a review of the literature. Eye. 2006;20:407-16.
9. Stringer W, Bryant R. Dose uniformity of topical corticosteroid preparations: difl uprednate ophthalmic emulsion 0.05% versus branded and generic pred-nisolone acetate ophthalmic suspension 1%. Clin Ophthalmol. 2010;4:119-24.
10. Coff ey MJ, DeCory HH, Lane SS. Development of a non-settling gel formula-tion of 0.5% loteprednol etabonate for anti-infl ammatory use as an ophthalmic drop. Clin Ophthalmol. 2013;7:299-312.
11. Wittpenn JR, Silverstein S, Heier J, et al. A randomized, masked comparison of topical ketorolac 0.4% plus steroid vs steroid alone in low-risk cataract surgery patients. Am J Ophthalmol. 2008;146:554-60.
12. Congdon NG, Schein OD, von Kulajta P, et al. Corneal complications associ-ated with topical ophthalmic use of nonsteroidal antiinfl ammatory drugs. J Cataract Refract Surg. 2001;27:622-31.
13. Baklayan GA, Patterson HM, Song CK, et al. 24-hour evaluation of the ocular distribution of 14C-labeled bromfenac following topical instillation into the eyes of New Zealand white rabbits. J Ocul Pharmacol � er. 2008;24(4):392-8.
14. Padilla A, Baklayan G; inventors. Bromfenac bioavailability. United States patent US 2013/0096199 A1. April 18, 2013.
15. Kim SJ, Flach AJ, Jampol LM. Nonsteroidal anti-infl ammatory drugs in ophthalmology. Surv Ophthalmol. 2010;55(2):108-33.
6 Topics in OCULAR ANTIINFLAMMATORIES To obtain CME credit for this activity, go to http://cme.ufl .edu/toai
a satisfactory visual outcome. � ere is a good chance that a “cured” patient will be le� visually impaired or blind due to vision-limiting corneal opaci� cation and signi� cant distortion from axial ectasia and irregular astigmatism. Af-ter “successful” treatment of contact lens related microbial keratitis, roughly half of the patients are le� with a best
corrected visual acuity worse than 20/60, and a quarter are 20/200 or worse.9
� e scarring that occurs is part of the “healing” process; and the residual opaci� cation it may leave is caused more by the host immune response than by the infection itself. � is sug-gests a role for steroids to prevent scar formation and improve visual outcomes. Suppressing the in� ammatory response, however, may also bring harm, especially in infections where the host defense plays a critical role in eliminating the organ-ism, such as in fungal or amoebic infections.
THE STEROID CONTROVERSY
Whether the adjunctive use of topical steroids provides any bene� t in managing ulcerative keratitis has been debated for decades. While proponents of steroid therapy believe that antiin� ammatory agents can help minimize immune-
What is the Role of Steroids in Treating Ocular Infection?
Acute in� ammation is a natural and essential host tissue response to microbial infection and other harmful stimuli. Although acute in� ammation is a protective mechanism aimed at eliminating invading organisms and restoring tissue integrity, when in� ammation becomes excessive or persistent it can be more destructive than the infection itself. In theory, taming this in� ammatory response—while simultaneously bringing the infectious process under control—should im-prove clinical outcomes.
Corticosteroids, a mainstay of antiin� ammatory treat-ment, can reduce immune-mediated tissue damage and thus, it is suggested, play a useful role in infectious disease manage-ment. However, steroids are associated with a variety of adverse side e� ects, including inhibition of the immune response and potentiation of infection.
� e possible advantages of adding steroid therapy to ef-fective antimicrobial treatment has been addressed in ocular toxoplasmosis and heavily studied in certain systemic infec-tions.1-3 In the ophthalmology literature, however, there is a paucity of clinical evidence to support corticosteroids’ theo-retical bene� t in the treatment of serious ocular infections such as infectious keratitis and postoperative endophthalmitis. In this article we will examine the controversial role of topical steroids in light of recent studies.
CHALLENGE IN TREATING CORNEAL INFECTIONInfectious keratitis is a leading cause of blindness world-
wide. In the US, reported annual incidence varies from 11 to 27 per 100,000 persons/year.4,5 � e incidence in developing countries is at least ten times higher.6-8 Bacterial infection is the most common cause of a corneal ulcer, although in some parts of the world, such as south India and Nepal, fungal ulcers are as common as bacterial ones.
� e goals of infectious keratitis treatment are to elimi-nate the causative organisms and to restore ocular function. By using newer broad-spectrum antibiotics, such as the C8 methoxy � uoroquinolones, or a multi-drug regimen of forti-� ed antibiotics, clinicians can now eliminate infection before perforation in the vast majority of cases.
E� ective antibiotic treatment, however, does not guarantee
THOMAS M. LIETMAN, MD AND JOHN D. SHEPPARD, MD In theory, adding topical corticosteroids to other measures for the treatment of ocular infection could reduce scaring and improve visual outcomes, but this potential benefi t has yet to be clearly demonstrated in clinical studies. In any case, corticosteroids should be used only in the presence of eff ective antimicrobial treatment and used with caution to minimize potential risks.
CORE CONCEPTS ✦ Infl ammation is a two-edged sword: it is essential to
infectious organism eradication but when excessive or persistent can cause severe ocular tissue damage.
✦ In ocular infection, optimal visual prognosis requires control of both the infection and the infl ammatory response.
✦ Topical steroids are the treatment mainstay for ocular infl ammatory conditions. Adjunctive steroid therapy may have a role in managing ocular infection by attenuating infl ammatory damage to ocular tissues.
✦ With appropriate antibiotic coverage, topical steroids are safe for the treatment of bacterial corneal ulcers, but there is little evidence that they provide signifi cant clinical benefi t.
✦ Steroids are not recommended for fungal keratitis, and should be used with great caution in Acanthamoeba infection.
✦ Current use of intravitreal steroid in postoperative endophthalmitis is empirical. No clinical study has clearly established that adjunctive steroid therapy is of benefi t.
CORE CONCEPTS

To obtain CME credit for this activity, go to http://cme.ufl .edu/toai Topics in OCULAR ANTIINFLAMMATORIES 7
mediated damage and prevent corneal scarring, others assert that the steroids may hamper re-epithelialization and prolong the infection.
� e controversy has endured so long in part because of the absence of evidence from large scale, prospective clinical tri-als aimed at determining the e� cacy of steroid therapy. Most studies found in the literature have been either retrospective or anecdotal.10
Over the last 10 or 15 years, however, cornea specialists in the US have gravitated toward adding topical steroid therapy to their bacterial keratitis treatment regimens, reasoning that because the antibiotic is able to eliminate the infection, slowing the immune response down may reduce the scarring without prolonging infection. But is this true?
SCUT: FINDINGS AND IMPLICATIONS
� e Steroids for Corneal Ulcers Trial (SCUT), initiated in 2007, is the � rst and only large-scaled, randomized, con-trolled clinical trial aimed at determining whether a topical steroid in combination with antibiotic treatment improves the visual outcomes of bacterial ulcer treatment.11 Unlike the prior inconclusive trials that were limited by sample size, the multicenter SCUT included 500 cases of bacterial ulcers, a sample size powered to detect a di� erence in visual acuity outcome of as little as one line.12-14
Overall, the SCUT researchers found no obvious bene� t in using steroids as adjunctive therapy. � ere was no statistically signi� cant di� erence in visual acuity or scar size between the steroid and placebo groups at 3 weeks or 3 months. Second-ary subgroup analyses of SCUT, however, did show several interesting sub-group analyses.
First, steroids appear to be associated with worse outcomes in Nocardia corneal ulcers.15 � is suggests that use of steroids should be avoided in patients with Nocardia ulcers. It also implies that steroids might have been mildly bene� cial in ul-cers caused by other bacteria. Secondly, ulcers with the most severe presentation (poor vision or large, central in� ltrates), such as Pseudomonas aeruginosa corneal ulcers, appeared to respond better to steroids.16 � ird, steroid treatment may be more likely to improve outcome when given early in the course of infection.
As with the secondary results of other clinical trials, these suggestive � ndings should serve to generate new testable hy-potheses rather than be taken as absolute treatment guides. In SCUT, steroids were given no less than 48 hours following antibiotic treatment. (In some cases, they were given as late as 7 days a� er the initial antibiotic treatment.) A small but e� cient clinical trial that examines the e� ect of earlier ste-roid treatment on visual outcomes in the most severe ulcers would be worthwhile and could conceivably generate more positive results.
STEROID THERAPY AFTER SCUT� e SCUT certainly did not settle the debate over adjunc-
tive use of steroids in the treatment of bacterial keratitis. While
the primary study result was that steroids made no di� erence in visual outcome, neither did the adjunctive treatment cause any additional harm. One major concern with steroid use is increased intraocular pressure (IOP). But the steroid group in SCUT actually had fewer pressure spikes than the placebo group, suggesting that in� ammation, rather than steroid treat-ment, is a more likely cause of elevated IOP, at least in the � rst 3 weeks of treatment.
All in all, there may not be as much at stake in the steroid debate as was previously thought: on the one hand, steroids are safer for bacterial ulcers than many feared; but on the other hand, steroids are not so clearly e� ective that clinicians are obliged to use adjunctive steroid therapy.
� e results of SCUT apply only to bacterial ulcers; the trial required a positive bacterial culture, a negative fungal culture, and no evidence of Acanthamoeba or herpetic infection for en-rollment. In cases of fungal or Acanthamoeba ulcers, where the infection is o� en tenacious because the organisms are di� cult to kill with drugs, the host immune response is particularly important for infection control, and suppressing the immune reactions might lead to catastrophic results.
Most cornea specialists do not use steroids in cases of fungal keratitis. For Acanthamoeba infection, most clinicians prefer to wait a number of weeks before using steroids, if they use them at all. Traditionally, ophthalmologists emphasized the importance of identifying the bacterial species as a guide to antibiotic selection, but for decisions about steroid use, the critical issue is to determine whether or not the infection is bacterial. Steroids should never be given before the possibility of a fungal, Acanthamoeba, or herpetic infection is excluded; and when given they should always be accompanied by ap-propriate antimicrobial treatment.
STEROIDS IN ENDOPHTHALMITIS TREATMENTEndophthalmitis is a dreaded postoperative complica-
tion because of its devastating e� ects on the eye and vision. � e majority of postoperative endophthalmitis cases occur a� er cataract surgery. � e incidence of post-cataract surgery endophthalmitis was recently reported to be about 0.1%.17 But with so many cataract surgeries performed each year (nearly 4 million cases in the US alone), even a tiny incidence can produce a signi� cant number of cases.
� e endophthalmitis vitrectomy study (EVS) has estab-lished that intravitreal antibiotics are the best approach to treatment of postoperative endophthalmitis, and immediate vitrectomy is of substantial bene� t only for patients with the worst vision loss.18 � e study did not evaluate concomitant steroid use, but over the years simultaneous or subsequent in-travitreal steroid injections have become increasingly popular as adjunctive therapy to control the in� ammatory damage.
CLINICAL EVIDENCEBecause of the extreme di� culty in organizing and ex-
ecuting a viable prospective randomized clinical trial, there is little scienti� cally balanced data in the literature supporting

8 Topics in OCULAR ANTIINFLAMMATORIES To obtain CME credit for this activity, go to http://cme.ufl .edu/toai
the bene� t of steroids in the treatment of postoperative endo-phthalmitis. A small study (N = 29) by Gan and colleagues was the first randomized, placebo-controlled study that demonstrated a trend towards better vision with adjunctive use of intravitreal steroid, though the results were not statisti-cally signi� cant.19
Most recently, Albrecht and colleagues reported a pro-spective, randomized, placebo-controlled clinical trial of 62 postoperative endophthalmitis cases in which they compared adjunctive intravitreal dexamethasone with intravitreal an-tibiotics alone.20 � e post-cataract subgroup showed a trend toward improved visual outcomes with dexamethasone, although statistical signi� cance was not achieved. � is South African study data, however, is reassuring to those who elect to use intravitreal steroids in endophthalmitis treatment be-cause steroid use also had no deleterious side e� ects in their study population.
CURRENT STATEPeyman and colleagues � rst reported use of intravitreal
steroid in the treatment of bacterial endophthalmitis in 1974.21 Almost four decades later, there is still no agreement on the adjunctive use of steroids in managing endophthalmitis. Currently the administration of steroids for patients with endophthalmitis is primarily empirical and le� to the judg-ment of the clinician.
Most clinicians feel more comfortable giving the steroids when the organisms have been identi� ed, although gram-positive bacteria are known to be the most frequent cause of endophthalmitis with a typically acute onset. Some choose to administer steroid empirically at the time of the initial injec-tion of paired antibiotics such as vancomycin and ce� azidime, particularly when severe in� ammation is present. But, if for any reason an unusual organism is suspected—if, for example, the patient is immunocompromised, diabetic, or the endo-phthalmitis had a delayed onset—steroid therapy is withheld.
In the US dexamethasone, which is available in a preser-vative-free solution, is the most commonly used intravitreal steroid for treatment of infectious endophthalmitis. A short-acting steroid, it is preferred in this setting to minimize the risk of potentiating the infection. If the initial steroid therapy turns out to be e� ective, then a longer-acting intravitreal agent, usually triamcinolone, may be indicated.
CONCLUSIONTopical and intravitreal steroids may have a role in ocular
infection management. New clinical evidence supports the safety of adjunctive steroid therapy in the treatment of both bacterial keratitis and postoperative endophthalmitis, always in the context of sound clinical judgment. But whether or not steroids are of bene� t—and, if so, in which cases—remains in question.
� omas M. Lietman, MD, is Pearl and Samuel Kimura Professor of oph-thalmology and professor of epidemiology and biostatistics at the University
of California, San Francisco (UCSF) in San Francisco, CA. He is also the director of the Proctor International Center and associate director of the F. I. Proctor Foundation, UCSF. He states that in the past 12 months, he has not had a fi nancial relationship with any commercial organization that produces, markets, re-sells, or distributes healthcare goods or services consumed by or used on patients. John D. Sheppard, MD, is professor of ophthalmology, clinical director of the Lee Center for Ocular Pharmacology at Eastern Virginia Medi-cal School. He is also medical director of the Lions Eye Bank, and president of Virginia Eye Consultants. He states that in the past 12 months, he has been a consultant and speakers bureau member for Alcon, Allergan, Abbott , Bausch + Lomb, and Merck. Medical writer Ying Guo, MBBS, PhD, assisted in the preparation of this article.
REFERENCES 1. Holland GN, Lewis KG. An update on current practices in the management
of ocular toxoplasmosis. Am J Ophthalmol. 2002;134(1):102-14. 2. Chaudhuri A. Adjunctive dexamethasone treatment in acute bacterial men-
ingitis. Lancet Neurol. 2004;3(1):54-62. 3. de Gans J, van de Beek D; European Dexamethasone in Adulthood Bacte-
rial Meningitis Study Investigators. Dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347(20):1549-56.
4. Erie JC, Nevitt MP, Hodge DO, et al. Incidence of ulcerative keratitis in a defi ned population from 1950 through 1988. Arch Ophthalmol. 1993;111:1665-71.
5. Jeng BH, Gritz DC, Kumar AB. Epidemiology of ulcerative keratitis in Northern California. Arch Ophthalmol. 2010;128(8):1022-8.
6. Gonzales CA, Srinivasan M, Whitcher JP, et al. Incidence of corneal ulcer-ation in Madurai district, South India. Ophthalmic Epidemiol. 1996;3:159-66.
7. Basak SK, Basak S, Mohanta A, Bhowmick A. Epidemiological and micro-biological diagnosis of suppurative keratitis in Gangetic West Bengal, eastern India. Indian J Ophthalmol. 2005; 53(1): 17-22.
8. Upadhyay MP, Karmacharya PC, Koirala S, et al. � e Bhaktapur eye study: ocular trauma and antibiotic prophylaxis for prevention of corneal ulceration in Nepal. Br J Ophthalmol. 2001;85:388-92.
9. Wilhelmus KR. Indecision about corticosteroids for bacterial keratitis: an evidence-based update. Ophthalmology. 2002;109(5):835-42.
10. Suwan-Apichon O, Reyes JM, Herretes S, et al. Topical corticosteroids as adjunctive therapy for bacterial keratitis. Cochrane Database Syst Rev. 2007;(4):CD005430.
11. Srinivasan M, Mascarenhas J, Rajaraman R, at al. Corticosteroids for bacterial keratitis: the Steroids for Corneal Ulcers Trial (SCUT). Arch Ophthalmol. 2012;130(2):143-50.
12. Carmichael TR, Gelfand Y, Welsh NH. Topical steroids in the treatment of central and paracentral corneal ulcers. Br J Ophthalmol. 1990;74(9):528-31.
13. Srinivasan M, Lalitha P, Mahalakshmi R, et al. Corticosteroids for bacterial corneal ulcers. Br J Ophthalmol. 2009;93(2):198-202.
14. Blair J, Hodge W, Al-Ghamdi S, et al. Comparison of antibiotic-only and antibiotic-steroid combination treatment in corneal ulcer patients: double-blinded randomized clinical trial. Can J Ophthalmol. 2011;46(1):40-5.
15. Lalitha P, Srinivasan M, Rajaraman R, et al. Nocardia keratitis: clinical course and eff ect of corticosteroids. Am J Ophthalmol. 2012;154(6):934-9.
16. Sy A, Srinivasan M, Mascarenhas J, et al. Pseudomonas aeruginosa keratitis: outcomes and response to corticosteroid treatment. Invest Ophthalmol Vis Sci. 2012;53(1):267-72.
17. Keay L, Gower EW, Cassard SD, et al. Postcataract surgery endophthalmitis in the United States: analysis of the complete 2003 to 2004 Medicare database of cataract surgeries. Ophthalmology. 2012;119(5):914-22.
18. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Endophthalmitis Vitrectomy Study Group. Arch Ophthalmol. 1995;113(12):1479-96.
19. Gan IM, Ugahary LC, van Dissel JT, et al. Intravitreal dexamethasone as adjuvant in the treatment of postoperative endophthalmitis: a prospective randomized trial. Graefe’s Arch Clin Exp Ophthalmol. 2005;243:1200-5.
20. Albrecht E, Richards JC, Pollock T, et al. Adjunctive use of intravitreal dexamethasone in presumed bacterial endophthalmitis: a randomised trial. Br J Ophthalmol. 2011;95(10):1385-8.
21. Peyman GA, Herbst R. Bacterial endophthalmitis. Treatment with in-traocular injection of gentamicin and dexamethasone. Arch Ophthalmol. 1974;91:416-8.
To obtain CME credit for this activity, go to http://cme.ufl .edu/toai Topics in OCULAR ANTIINFLAMMATORIES 9
1. Which of the following is NOT a risk factor for steroid-induced IOP increase?A. Type II diabetesB. Ocular hypertension C. High myopiaD. First-degree relative with
glaucoma
2. Steroid use was associated with poorer outcomes in:A. Streptococcus ulcersB. Pseudomonas ulcersC . Nocardia ulcersD. Moraxella ulcers
3. What was the primary outcome of SCUT regarding treatment of bacterial corneal ulcers? A. Steroids signi� cantly improve
visual outcome B. Steroids signi� cantly relieve pain
and shorten the time course of the condition
C. Steroids should be given more than 72 hours a� er antimicrobial treatment
D. None of the above is correct
EXAMINATION ANSWER SHEET TOPICS IN OCULAR ANTIINFLAMMATORIES | ISSUE 2
EVALUATION:1=Poor 2=Fair 3=Satisfactory 4=Good 5=Outstanding
11. Extent to which the activity met the identifi ed Objective 1: 1 2 3 4 5 Objective 2: 1 2 3 4 5 Objective 3: 1 2 3 4 5
12. Rate the overall eff ectiveness of how the activity: Related to my practice: 1 2 3 4 5 Will infl uence how I practice: 1 2 3 4 5 Will help me improve patient care: 1 2 3 4 5 Stimulated my intellectual curiosity: 1 2 3 4 5 Overall quality of material: 1 2 3 4 5 Overall met my expectations: 1 2 3 4 5 Avoided commercial bias/infl uence: 1 2 3 4 5
13. Will the information presented cause you to make any changes in your practice? Yes No
14. If yes, please describe: __________________________
________________________________________________
15. How committed are you to making these changes? 1 2 3 4 5
16. Are future activities on this topic important to you? Yes No
If you wish to receive credit for this activity, please fi ll in the following information. Retain a copy for your records. PLEASE PRINT CLEARLY
________________________________________________________________FIRST NAME LAST NAME DEGREE
________________________________________________________________ORGANIZATION/INSTITUTE
________________________________________________________________ADDRESS LINE 1
________________________________________________________________ADDRESS LINE 2
________________________________________________________________CITY STATE ZIP
________________________________________________________________PHONE FAX
________________________________________________________________EMAIL ADDRESS
This CME activity is jointly sponsored by the University of Florida and Candeo Clinical/Science Communications, LLC, and supported by an unrestricted educational grant from Bausch + Lomb, Inc. Mail to: University of Florida CME Offi ce, PO Box 100233, Gainesville, FL 32610-0233. DIRECTIONS: Select the one best answer for each ques-tion in the exam above (Questions 1–10). Participants must score at least 80% on the questions and complete the entire Evaluation (Questions 11–16) to receive CME credit. CME exam expires August 31, 2014.
1. A B C D
2. A B C D
3. A B C D
4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
ANSWERS:
4. Topical corticosteroids work by blocking:A. Prostaglandin E2B. Phospholipase A2C. Phospholipid transfer proteinD. All of the above
5. Which of the following is the route frequently employed by clinicians to administer steroids for in� ammation control in endophthalmitis? A. Oral medication B. Intravenous injection C. Intravitreal injection D. Subconjunctival injection
6. Which of the following is most likely to be a complication of topical NSAID use? A. Hypotony B. Sudden IOP spikeC. Mild uveitisD. Punctate keratitis
7. Which of the following is associated with increased in� ammation a� er cataract surgery?A. Older ageB. Dietary de� ciencies C. Darkly pigmented iridesD. Hyperopia
8. In the SCUT, the e� ect of steroid on IOP was:A. Pronounced B. Not signi� cantC. Forced early conclusion of the trialD. Meaningful only in Acanthamoeba
ulcers
9. Intravitreal steroids should be withheld in postoperative endophthalmitis treatment when: A. � e condition had a delayed onsetB. � e patient is youngC. � e patient is immunocompetentD. All of the above are correct
10. A suspension formulation: A. O� ers excellent drop-to-drop
consistency B. Must always be refrigeratedC. Requires vigorous shakingD. Enhances drug penetration
This CME program is sponsored by the University of Florida College of Medicine and supported by an unrestricted educational grant from Bausch + Lomb, Inc. Directions: Select the one best answer to each question in the exam (Questions 1–10) and in the evaluation (Questions 11–16) below by circling one letter for each answer. Participants must score at least 80% on the questions and complete the entire Evaluation section on the form below. The University of Florida College of Medicine designates this enduring material for a maximum of 1.0 AMA PRA Category 1 Credit™. There is no fee to participate in this activity. You can take the test online at http://cme.ufl .edu/toai.
EXAMINATION QUESTIONS TOPICS IN OCULAR ANTIINFLAMMATORIES | ISSUE 2