
issn 1868-3207 Vol. 11 Issue 2/2010 implants · Cosme Gay-Escoda I user report 10 Use of an X-ray...
52
2 2010 issn 1868-3207 Vol. 11 • Issue 2/2010 | case report Immediate implant placement and temporisation in the aesthetic zone | user report Use of an X-ray phantom in dental 3-D diagnostics in digital volume tomographs | meetings 6 th Arab-German Implantology Meeting of DGZI implants international magazine of oral implantology
Transcript of issn 1868-3207 Vol. 11 Issue 2/2010 implants · Cosme Gay-Escoda I user report 10 Use of an X-ray...
22010
i s sn 1868-3207 Vol. 11 • Issue 2/2010
| case reportImmediate implant placement and temporisationin the aesthetic zone
| user reportUse of an X-ray phantom in dental 3-D diagnostics in digital volume tomographs
| meetings6th Arab-German Implantology Meeting of DGZI
implantsinternational magazine of oral implantology

A program menu that covers all stages of implantation and is easy to use.
A motor with sensitive power control that feels supremely comfortable in the
hand. An aesthetic design with attractive clear shapes. A price / performance
ratio that will give you a pleasant surprise.
An additional feature: the new endodontics function allows retrograde root apex
resections of the root canal to be prepared in an orthograde manner – without
having to change to an endodontic device. That's rather intelligent, isn't it?
wh.com
Intelligent design shows in the details.
A program menu that covers all stages of implantation and is easy to use.
A motor with sensitive power control that feels supremely comfortable in the
hand. An aesthetic design with attractive clear shapes. A price / performance
ratio that will give you a pleasant surprise.
An additional feature: the new endodontics function allows retrograde root apex
resections of the root canal to be prepared in an orthograde manner – without
having to change to an endodontic device. That's rather intelligent, isn't it?
wh.com
A program menu that covers all stages of implantation and is easy to use.
Intelligent design shows in the details.
People have Priority! W&H supports the humanitarian organization SOS Children’s Villages. Get involved! Further information at wh.com
120 Years W
&H.
Help us support SOS Child
ren’s Villages!

Sincerely
Dr Rolf Vollmer
editorial _ implants I
implants2_2010
Dr Rolf Vollmer
_I am seeing more and more misadventures dealing with complex implant cases. In particular, in thelast several months I have seen numerous loading problems dealing with full arch restorations. By and large,the vast majority of these issues relate to a failure in the initial diagnosis. We know from our experience incontinuing education courses that diagnosis and decision-making are always the most difficult things toteach and convey. Implant dentistry is now an integral part of many dental practices, however most den-tists receive their education in implant dentistry after graduation, with little emphasis on the identifica-tion of the complexity and risks of treatment.
I recently became interested in a concept called the SAC classification. SAC stands for Straightforward,Advanced, and Complex. The SAC classification was first described by Sailer and Pajarola in 1999 as amethod to categorize degrees of difficulty in oral surgery. In 2003 SAC underwent extensive review andwas adapted for implant dentistry; it was also the topic of the ITI Consensus Conference in 2007 to stan-dardize their application.
The basis of the SAC classification is that clinical situations in implant dentistry present with varyingdegrees of complexity. The SAC classification has applications in esthetical, restorative and surgical situa-tions but can also be helpful in all forms of implant dentistry. Knowing in advance how complex an implantcase is can ensure there are no surprises in the course of treatment, or if necessary, can allow you to referthe case to someone who is better able to perform the risky portion and return the case to you for the easytreatment. Usage of the SAC classification can assist practitioners in avoiding difficulties in implant andprosthetic cases as well.
It is, therefore, vitally important that we as practitioners are willing to acknowledge that some cases aremore complex or difficult than others, and that we may need experts to deal with such cases. Finding anappropriately qualified colleague to manage a particularly complex case can prevent the case developingcatastrophic complications and can avert a poor outcome.
Complex cases simply cannot be treated with a straightforward approach of “open the flap and see whatwe can do”. For these types of cases more of a “reverse planning” approach is recommended—i.e. determinethe plan of treatment by starting at the end-point. Generally, working forward from today incorporatesneither resource implications nor integration needs. We are mentally so accustomed to the traditional formof thinking that we overlook important items and needs, and make subconscious assumptions that are notnecessarily valid. Instead, periodic “reality checks” of the content of our plan of action and its implemen-tation should occur. Regardless of how well planned cases are, ‘things’ never work out quite as envisaged— all too often real-time developments lead to detours. To minimise such occurrences, modern implantol-ogy diagnostic tools like DVT and computer assisted planning are very helpful in complex cases.
Establish the goal, begin at the end and work backward! If done correctly, we will have an ever-evolv-ing, reality-based, integrated plan that will actually work to achieve our patients aims.
Currently we, as an expert scientific implant association, are happy to offer our colleagues the possi-bility of undertaking company-independent implant training courses including masters programs at uni-versities. Many dentists involved in the surgical or restorative aspects of implant care obtain continuingeducation in implant dentistry and belong to professional implant organizations like the German Associ-ation of Dental Implantology (DGZI). Our continuing education programs (e.g. our basic curriculum andour Annual Meetings) are some of the best I have ever attended, nationally or internationally.
I hope to see many of you later this year in Berlin from the 1st to 2nd of October to celebrate our fortiethanniversary with an outstanding scientific and social program.
Straight forward orbackward planning?

implants2_2010
I editorial
03 Straight forward or backward planning?| Dr Rolf Vollmer
I case report
06 Immediate implant placement and temporisation in the aesthetic zone| Dr Philip J. Friel
14 Bone Harvesting—nice and easy| Dr Steffen Hohl & Dr Anne Sophie Brandt Petersen
I research
18 The concept of “platform switching”in implant dentistry—Part II| Dr Virgil Koszegi Stoianov
24 Rehabilitation of atrophic maxillas usingzygomatic implants| Joan Pi-Urgell, Javier Mir-Mari, Rui Figueiredo & Cosme Gay-Escoda
I user report
10 Use of an X-ray phantom in dental3-D diagnostics in digital volume tomographs| Dr Georg Bach, Christian Müller & Alexander Rottler
II meetings
32 International events 2010/2011
34 25th Anniversary of the Academy of Osseointegration| Dr Rolf Vollmer & Dr Rainer Valentin
36 6th Arab-German Implantology Meeting of DGZI
41 ITI World Symposium 2010
42 Interdisciplinary insights from theory to practice
I implants
33 DGZI’s anatomy weekend a full success!| Dr Christian Ehrensberger
I news
44 Manufacturer news
48 Congratulations and Happy Birthdayto all DGZI-members around the world
I about the publisher
50 | imprint
case report 06 case report 14 research 18
Cover image: SEM scan of PD VitalOs Cement after hardening.
Image courtesy of Produits Dentaires SA (www.vitalos.com).
user report 10 implants 33 meetings 34

TiUnite® surface and Groovy™to enhance osseointegration.
Implant design that replicates the shape of natural tooth roots.
Internal tri-channel connection for accurate and secure prosthetic restorations.
Color-coded system for accu rate and fast component
identification and ease of use.
Color-coding: step-by-step drilling protocol for predictable
surgical procedures.
NobelReplaceTM
The world’s most used implant system.*
* Source: Millennium Research Group
Disclaimer: Some products may not be regulatory cleared/released for sale in all markets. Please contact the local Nobel Biocare sales office for current product assortment and availability.
Versatility, ease-of-use and predict-ability have made NobelReplace Tapered the most widely used implant design in the world.*NobelReplace Tapered is a general use, two-piece implant system that performs both in soft and hard bone, one- and two-stage surgical proce-dures, while consistently delivering
optimal initial stability. NobelReplace Tapered is a system that grows to meet the surgical and restorative needs of clinicians and their patients – from single-tooth restorations to more advanced multi-unit solutions. Whether clinicians are just starting or are experienced implant users, they will benefit from a system that
is unique in flexibility and breadth of application. Nobel Biocare is the world leader in innovative and evidence-based dental solutions. For more information, visit our website.
www.nobelbiocare.com
10 YEARS WITH
TIUNITE® SURFACE
New data confi rm
long-term stability.
© N
ob
el B
ioca
re S
ervi
ces
AG
, 2
01
0.
All
rig
hts
res
erve
d.
No
bel
Bio
care
, th
e N
ob
el B
ioca
re lo
go
typ
e an
d a
ll o
ther
tra
dem
arks
are
, if
no
thin
g e
lse
is s
tate
d o
r is
evi
den
t fr
om
th
e co
nte
xt in
a c
erta
in c
ase,
tra
dem
arks
of
No
bel
Bio
care
.

implants2_2010
_The success of dental restorations can bemeasured in terms of biological stability overtime. With regards to dental implantology, thechallenge is no longer one of integration, morelong term aesthetic stability of the final restora-tion. Nowhere is this biological and aestheticstability more important than in the aestheticzone.
Teeth and their roots have a supportive role tothe alveolar bone in which they are retained. Thisbone in turn gives support to the gingival tissueoverlying it, and the level of this bone directly af-fects the position of this gingival tissue.1 Follow-ing tooth loss, this support is lost, and both thehard and soft tissue begin a process of remodel-ling. This process invariably results in the loss ofbone, and an alteration in the gingival position.While it is possible to replace this support withthe use of bone grafting or collagen plug tech-niques, this can involve a number of surgicalprocedures in order to achieve the final result.Original protocols in implantology required thatimplants be placed into healed edentulousridges. Implants can, however, be placed at thetime of tooth extraction.2 Such techniques canbe used with simultaneous augmentation to
preserve ridge width, decreasing total treatmenttime. This paper, and its case presentation, out-line a technique which allows, in the right con-ditions, the replacement of the support of a lostroot, and consequently prevents major bone re-modelling and subsequent alteration of soft tis-sue position. The following case is one of manycompleted, ranging from the single tooth tomultiple units, all of which have a minimum oftwelve months follow-up, and the results ofwhich will be collectively published in the nearfuture. The illustrated case involves a 63 year old,retired female patient who was referred to theclinic timeously by her general dental practi-tioner following root fracture affecting the up-per left lateral incisor. Her chief complaint wasone of poor aesthetics affecting this tooth (Fig. 1). The condition of this tooth had declinedgradually, following placement of a compositecrown three years previously. The compositecrown had been placed, retained by a temporarypost, following failed root canal therapy duringwhich an endodontic instrument was fracturedin the tooth (Fig. 2). The patient was in goodhealth, a regular dental attendee with an ade-quate oral hygiene regime. A full dental assess-ment was undertaken to include assessment of
Immediate implant place-ment and temporisation inthe aesthetic zoneAuthor_ Dr Philip J. Friel, Great Britain
Fig. 1 Fig. 2 Fig. 3 Fig. 4

implants2_2010
soft and hard tissue, remaining dentition, occlu-sion and parafunction, current and required oralhygiene and maintenance. The patient wasnoted to have a high smile line, clearly showingthe dentogingival complex in function. A full dis-cussion outlined the options available to the pa-tient, who after consideration, elected a fixedoption, with implant restoration being her solu-tion of choice. The patient was fully aware of therisks and alternatives to the procedure, andgiven her very recent root fracture affecting thetooth, surgery was scheduled for the same week.Mounted study models were produced, uponwhich, two vaccum formed stents were madeover the tooth in question. Full radiographic as-sessment was undertaken to determine the con-dition of the remaining root, adjacent teeth androots, while assessing the area dimensionally forimplant placement. The patient was prepared forsurgery following pre operative consent and an-tibiotics together with repeated pre operativerinsing with chlorhexidine gluconate 0.2 %.Standard surgical scrub and drapes were em-ployed. The upper left lateral incisor tooth wascarefully extracted using periotomes to preserveboth hard and soft tissue around the socket.3 Thistechnique facilitates tooth removal withouttraumatising the alveolar bone of the socket orsurrounding gingival tissue. The technique canbe performed for any extraction, but it is of par-ticular importance when the subsequent place-ment of dental implants is envisaged.
Following atraumatic tooth removal, thesocket was thoroughly irrigated, debrided andfully assessed (Fig. 3). The socket was found to beintact, stable and formed from solid bone. The
buccal crestal bone was found to be intact, at agood level and supporting the thick gingivalgenotype overlying it. Having fully assessed thesocket, the implant osteotomy was undertaken,following a flapless surgery protocol with bothexternal and internal irrigation, and using thesurgical stent as a guide to the final required po-sition. Bone removed during the procedure washarvested (Fig. 4). The osteotomy was preparedand the fixture placed slightly towards thepalatal plane. The implant was seated to the de-sired vertical position to allow ideal soft tissueposition after healing. The implant (Nobel Bio-care RST 16 mm NP) was inserted and torqued to35Ncm (Fig. 5). After implant placement, thesocket was then reassessed. As expected therewas found to be a slight void between implantand buccal plate. The harvested bone was packedinto this defect, as an adjunctive graft, in orderto support the buccal plate and its overlying gin-givae.4 Having placed the implant and harvestgraft, the bony socket was now supporting itsoverlying hard and soft tissues once more. At-tention then turns towards gaining support forthe crestal soft tissues. An immediate temporaryabutment was torqued on to the implant againto 35 Ncm, and a Teflon cap placed over this (Fig. 6). Using the second vaccum formed stent,a temporary crown was constructed using aflowable composite resin, and light cured beforebeing removed. Following removal, the crown isadded to and carefully polished, especially in thecervical area, to give a highly polished, er-gonomic temporary restoration which is ade-quately supportive to the cervical gingival tis-sues, providing a circumferencial seal aroundthe marginal area. Following final polishing, the
Fig. 9 Fig. 10 Fig. 11
Fig. 5 Fig. 6 Fig. 8Fig. 7

implants2_2010
temporary crown is luted to the temporary abut-ment using a temporary cement. The post opera-tive radiograph (Fig. 7) shows this situation andhighlights a small excess of temporary cementwhich can be easily removed with floss. The tem-porary restoration is kept clear of the occlusion.Given the implant is placed directly into the ex-traction socket, and that the adequately support-ive temporary crown provides an excellent crestalgingival seal, no flap is required and consequently,no sutures are used in this procedure. Standardpost operative protocols are followed. As a resultof this flapless approach , the trauma of surgery islessened, and review one week post surgery showsan excellent recovery (Fig. 8), with very little signof any trauma, swelling or alteration of the sur-rounding gingival tissue, which largely remainsunchanged. After a five to six month healing pe-riod, during which regular review is undertaken,the temporary crown is removed using a crownremover. The temporary abutment is removed andthe socket irrigated. A standard open tray impres-sion technique is used to record the position of theimplant, and the temporary abutment and crownreplaced. The subsequently produced model isused to construct an abutment and crown, repli-cating the exact support given by the temporaryset up. The case is completed by final abutmentplacement and torque to 35 Ncm. Following trialfit, and approval of the definitive restoration, theocclusion is checked and adjusted as required . TheZirconia crown is cemented using a resin cement,with care being taken to minimally load the ce-ment and remove any excess prior to and aftercure. Occlusion is again assessed and adjusted asrequired. The success of the restoration is evidentimmediately after cementation (Fig. 9), at 3 month(Fig. 10) , six month (Fig. 11) and 18 month review(Fig. 12 a & b). In order to successfully perform theprocedure outlined above, timing is essential, par-ticularly in the case of the root fractured tooth. Inthese cases, if such treatment is not initiated ingood time, the area can become infected with cor-responding sinus formation and inevitable loss ofthe buccal plate of bone. This would entail re-assessment and treatment using a multi-staged,delayed placement regime. In order to perform
flapless surgery, the operator must have suitableexperience, and be competent in the procedure.Added to this, as with any surgery, a full knowl-edge and appreciation of the anatomy surround-ing the surgical site is essential to ensure a suc-cessful outcome. It is sometimes necessary tocarry out further special tests or procedures dur-ing the planning stages, to ascertain further in-formation prior to commencement of treatment.These may include CT scanning or ridge mappingof the proposed surgical site. Following atrau-matic tooth extraction and socket assessment itmay, occasionally, not be possible to proceed withimmediate implant placement for a number ofreasons. In such cases proper planning is essentialto ensure that an alternative treatment optionmay be undertaken. While flapless surgery incursdecreased trauma and faster healing, during anyflapless procedure, it must be remembered thatthe operator can, at any time, raise a flap, if at allconcerned with regards to surgical progress. Bio-logical stability has been maintained from re-moval of the damaged root right through to ce-mentation of the definitive restoration. By re-specting and understanding the natural tissues inthis way, predictably excellent results can beachieved time after time.
The clinical photographs and case discussionare included with the expressed permission of thepatient involved. All of the laboratory stages forthe case were completed by Lincoln Ceramics,Glasgow.
_References
1. Gargiulo et al J.Periodontol,1961,31:261–267.2. Lazzara R J. Immediate implant placement intio extractionsites: surgical and restorative advantages. Int J PeriodontRest Dent 1989;9:332–343.3. Quayle A. Atraumatic removal of teeth and root fragmentsin Dental Implantology. Int J Oral Maxillofac Implants1990;5:293–296.4. Botticelli et al. The jumping distance revisited : An experi-mental study in the dog. Clin Oral Implants Res2003;14(1):35–42.
First published in Scottish Dentist March-April2008._
Fig. 12a Fig. 12b
Dr Philip J. FrielPhilip Friel Advanced Dentistry170 Hyndland RoadG12 9HZ Glasgow, Great Britain
_contact implants

SIMPLY BETTERSTRAUMANN® SLActive
Straumann® SLActive – The next generation in surface technology
Higher security and faster osseointegration for every indication Reduced healing times from 6–8 weeks
down to 3–4 weeks Increased treatment predictability in critical protocols
Please contact us at +41 (0)61 965 1111 More information on www.straumann.com
Based on the following studies: preclinical: Buser et al. (2004), Schwarz et al. (2006/2007) clinical: Zöllner et al. (2007), Oates et al. (2007) internal data on file
...over1
million implant
s
sold
!
Straumann® SLActive
10 I
I user report _ 3-D diagnostics
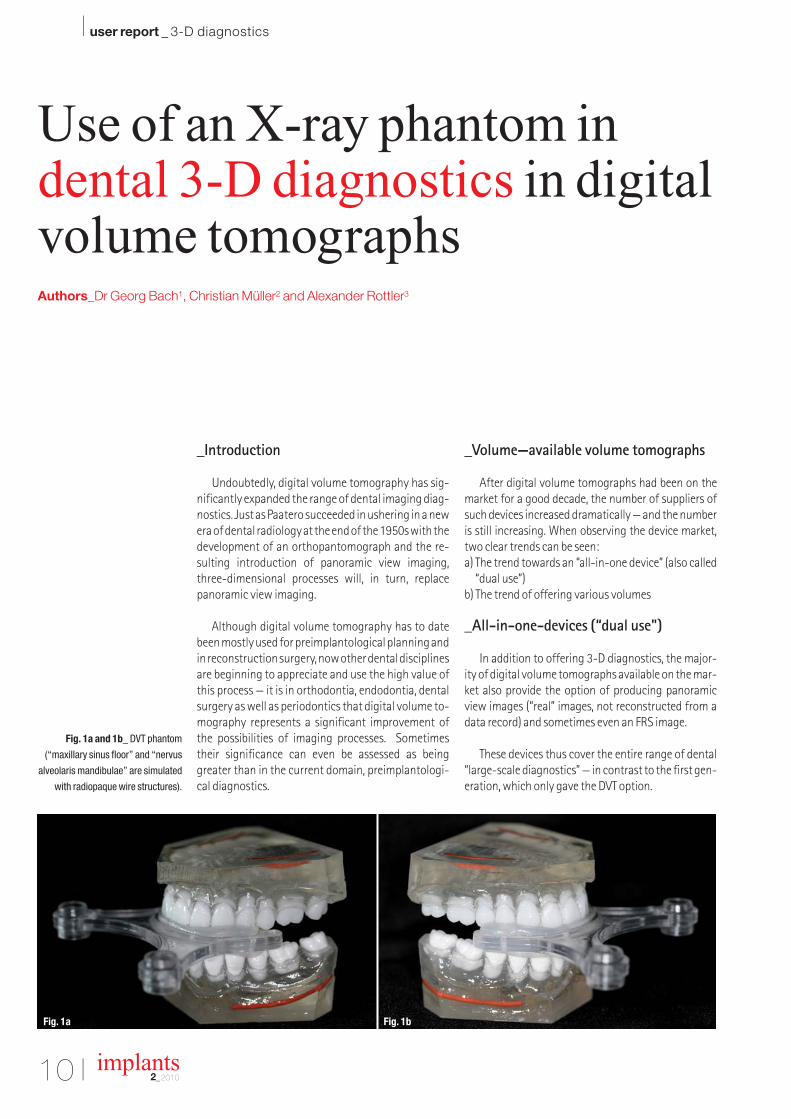
Fig. 1a and 1b_ DVT phantom
(“maxillary sinus floor” and “nervus
alveolaris mandibulae” are simulated
with radiopaque wire structures).
implants2_2010
_Introduction
Undoubtedly, digital volume tomography has sig-nificantly expanded the range of dental imaging diag-nostics. Just as Paatero succeeded in ushering in a newera of dental radiology at the end of the 1950s with thedevelopment of an orthopantomograph and the re-sulting introduction of panoramic view imaging,three-dimensional processes will, in turn, replacepanoramic view imaging.
Although digital volume tomography has to datebeen mostly used for preimplantological planning andin reconstruction surgery, now other dental disciplinesare beginning to appreciate and use the high value ofthis process — it is in orthodontia, endodontia, dentalsurgery as well as periodontics that digital volume to-mography represents a significant improvement ofthe possibilities of imaging processes. Sometimestheir significance can even be assessed as beinggreater than in the current domain, preimplantologi-cal diagnostics.
_Volume—available volume tomographs
After digital volume tomographs had been on themarket for a good decade, the number of suppliers ofsuch devices increased dramatically — and the numberis still increasing. When observing the device market,two clear trends can be seen:a) The trend towards an “all-in-one device” (also called
“dual use”)b) The trend of offering various volumes
_All-in-one-devices (“dual use")
In addition to offering 3-D diagnostics, the major-ity of digital volume tomographs available on the mar-ket also provide the option of producing panoramicview images (“real” images, not reconstructed from adata record) and sometimes even an FRS image.
These devices thus cover the entire range of dental“large-scale diagnostics” — in contrast to the first gen-eration, which only gave the DVT option.
Use of an X-ray phantom in dental 3-D diagnostics in digitalvolume tomographsAuthors_Dr Georg Bach1, Christian Müller2 and Alexander Rottler3
Fig. 1a Fig. 1b
The DVT devices of today’s generation are oftensimilar in design and appearance to traditional digi-tal volume tomographs; the position of the patientwith these and other “frame” devices is typicallystanding or sitting, while the once dominant supinepatient position of the first device generation is passéexcept for one manufacturer.
_Various volumes
Such first-generation devices featured very largevolumes which required time-consuming reworkingof the immense data record for problems beyondlarge and reconstruction surgery in order to be ableto evaluate the “relevant” data and/or regions in atarget-oriented manner. Today numerous manufac-turers offer devices with mid-size and small volumes.Three types of devices are available:_Devices with a large volume (18 x 20 cm and higher)
for oral surgery and reconstruction._Devices with a medium volume (8 x 10 cm and
higher) for oral surgery and reconstruction._Devices with a small volume (4 x 5 cm) for oral sur-
gery and dental procedures.
_Problems with devices with small andmedium volume
Devices with small and medium volume are gen-erally used in oral surgery and dental practices; theyare mostly used for preimplantological diagnostics,for oral surgery and orthodontic and endodonticprocedures.
The “finiteness” of the volume size requires care-ful device setting and patient positioning so that therelevant structure is also depicted and/or “encoun-tered”; it must also be “well targeted.”
For new users and those colleagues who only dovolume tomographies once in a while, this correctsetting can pose difficulties.
This was our motivation to develop a DVT phan-tom which can be used for training purposes as wellas for direct preparation of an image with a patient.
_The DVT phantom and its application
The DVT phantom is an X-ray phantom which de-picts a medium-sized mandibular and maxillar den-tal arch; the teeth are positioned in ideal denticula-tion.
The divided phantom (mandible and maxilla) ismounted on the individual biting or positioningaid/support of the respective device. Barium sulfateis added to the plastic teeth so that they are visible in
easy
-gra
ft®C
RY
STA
L
Bip
hasi
c co
mpo
site
sub
stitu
te, 6
0 %
HA
/ 40
% ß
-TC
P, P
LGA
coa
ted
Bip
h
Degradable Solutions AGWagistrasse 23CH-8952 SchlierenPhone: +41 43 433 62 [email protected]
Simple handling and accelerated osteocon-duction for long-term volume preservation.
Order your free test sample over the internet!
bio
nic
st
icky
gra
nule
s AD

12 I
I user report _ 3-D diagnostics
Fig. 2_ DVT phantom in a volume
tomograph (Kodak 9000 3d, small
volume) fixated on the original patient
biting aid.
Fig. 3_ Device settings: With the aid
of the light visors, a volume is placed
on the region to be depicted (here
region 26 and maxillary sinus floor).
Fig. 4_ DVT phantom image of the
maxilla with the X-ray phantom.
Fig. 5_ DVT phantom image of the
mandible with the X-ray phantom.
implants2_2010
the X-ray image; these teeth have been made by themanufacturer especially for X-ray applications.
The DVT platform is now mounted in the devicewith the original biting aid/support instead of a pa-tient. The device setting can occur in two differentways:a) The desired volume is preset using the device pro-
gram and then manually fine-tuned.b) The device is manually set directly on the region to
be depicted with the aid of the light visors.Then the set positioning is saved.
_Using the DVT phantom for training and practice purposes
With the aid of the DVT phantom and the above-mentioned setting techniques, new users or col-leagues seeking technical qualifications can learnhow to set the device for the regions to be examined,generate one or more individual images using the“preview function” and check to see if the settingwas correct. In the event of incorrect settings, a bet-ter image can be immediately generated so thatthere is a direct learning curve.
_Using the DVT phantom for preparinga patient image
Time-consuming and tedious setting (“aiming”)of the volume on a patient who is already in the de-vice is not something that will generally meet with
the patient’s whole-hearted agreement. This iswhere presetting the device with the aid of the DVTphantom comes in handy. The desired region is de-picted with the phantom and, if needed, is checkedwith the preview function. Then the phantom is re-moved, and the patient is fetched and positioned inthe device. Generally, only one device setting for thepatient’s body size and small fine-tuning are re-quired and the image is set.
_How to obtain a DVT phantom
Such a DVT phantom can be produced in cooper-ation with practicing dental technicians, the bariumsulfate-containing plastic teeth are available on themarket and a phantom can be made in the mannerdescribed above. An easier option is to send a DVTpositioning aid of your device to www.dtcm-freiburg.de or [email protected]. Master Den-tal Technician Christian Müller will then mount aprepared DVT phantom on your positioning aid. In-dustrially manufactured barium-sulfate-contain-ing plastic teeth (SR Vivo Tac/SR Ortho Tac, IvoclarVivadent) will be used which are then incorporatedinto a mandibular and maxillar model made of trans-parent plastic.
The authors of this article hope that the fascinat-ing field of 3-D diagnostics will establish itself quicklyin dentistry and that it will remain an imaging proce-dure that significantly expands upon the hithertorange of dental X-ray diagnostics in the long term._
Fig. 2 Fig. 3
Fig. 4 Fig. 5
Dr Georg BachRathausgasse 3679098 Freiburg im Breisgau, GermanyE-mail: [email protected]
1 DDS; specialist in oral sur-gery
2 Diploma Master DentalTechnician
3 Bachelor Dental Techni-cian
_contact implants

a perfect fit ©
NEW IMPLANTS, NEW ABUTMENTS
LIBERTY OF CHOICENATURALLY FROM CAMLOG
Reliable implants, patented Tube-in-TubeTM connection, and from now on as an option: platform switching. Camlog offers more. More information: www.camlog.com

implants2_2010
Figs. 1 & 2_Initial situation in region
031,041. State 3 months after the
removal of the teeth 31, 41. In region
041 the vestibular lamella has
completely collapsed.
Fig. 3_Noticeably visible three wall
bone defect in region 031 vestibular.
Fig. 4_After drilling the implant
shafts, region 031 showed to be
significantly atrophied.
Fig. 5_The implant shafts are dilated
using condensers and the periim-
plantational bone is condensed.
Fig. 6_Implant insertion in the
regions 031, 041. In region 031 it is
visible that a vestibular augmentation
must take place.
_Introduction
The desire to use bone from your own body tobuild new bone in another place is almost as oldas humanity itself. We call this procedure autolo-gous bone grafting.
In the case of autologous bone grafting thebone is removed from the same organism that thegraft is to be incorporated in. The body’s own bonecells have the greatest potency for rebuilding ofbones and are the gold standard in oral augmen-tation surgery. Donor areas are: the tuber maxil-lae, the retromolar space, the chin region or theiliac crest, the ribs or the shin. Gaining the re-quired quantity is sometimes elaborate (large
surgical interventions, in patient stay) and af-flicted with particular problems, especially whenit comes from regions far away from the oral cav-ity (e.g. the iliac crest). The extraction of autolo-gous bone grafts from the retromolar space findthe best acceptance with patients.
Particularly in implantology lateral augmenta-tions are necessary in more than 75 per cent ofcases. These augmentative measures mostly re-quire low bone volumes of less than 0.3 mg. If thedecision is made intraoperatively, that the pa-tient’s own bone must be used, as a rule the fol-lowing question must be asked: “Which regionshould the bone be taken from and how can it beremoved quickly?”
Bone Harvesting—nice and easyAuthors_Dr Steffen Hohl, Germany & Dr Anne Sophie Brandt Petersen, Denmark
Fig. 1 Fig. 2 Fig. 3
Fig. 4 Fig. 5 Fig. 6

implants2_2010
The retromolar space is chosen here in morethan 70 per cent of cases. Until now exclusivelyblock grafts have been used.
_Case description
The 36 year old patient wants the gaps in histeeth in the regions 031, 041 to be filled with im-plants due to his otherwise intact dentition. How-ever in this situation the question is raised ofwhether implantation and necessary augmenta-tion of the crestal jaw line can occur synchro-nously. It was planned for the patient to have au-tologous bone adhered in the region of the 031
vestibular. Hereby the right retromolar spaceand the right tuber area were considered asdonor areas. The patient could be assured pre-operatively that an extraction defect of bone ex-traction would only involve few complaintsymptoms. Interoperatively the crestal incisionwas begun in the areas 031 and 041. After form-ing a minimally invasive mucoperiosteal flap, inparticular region 031 showed strong vestibularatrophies. Initially implant drilling was carriedout and the bore shaft was extended using bonecondenser, i.e. the periimplantational bone wascondensed. Subsequently, the implant bodies wereinserted. Here it became obvious that the implant
Fig. 7_the implant body in region 031
must be vestibularly covered with au-
tologous bone over approx. 2/3 of its
surface.
Fig. 8_Retromolar stab incision with
an 11 scalpel.
Fig. 9_A conventional implant drill is
used to drill directly in the area of the
linea obliqua through the stab inci-
sion. A “two spade drill” is excel-
lently suited to bone extraction.
Fig. 10_Bone excavation via simple
shaft drilling with the conventional
“two spade drill”.
Fig. 8 Fig. 9Fig. 7
Fig. 11 Fig. 12Fig. 10
Fig. 14 Fig. 15Fig. 13
Fig. 17 Fig. 18Fig. 16

implants2_2010
Fig. 11_additional bone excavation
by hollowing out the shaft drill hole in
the linea obliqua with the excavator.
Fig. 12_Implants and autologous
bone augmentation in situ. In order to
achieve this result it was only neces-
sary to drill into the retromolar!
Fig. 13_Covering the implants
and augmentations with a simple
collagen membrane.
Figs. 14 & 15_The stab incision of
the retromolar extraction region is
glued with cyanoacrylate. Hereby the
patient only incurs a microscopic
extraction defect.
Figs. 16 & 17_The soft tissue in the
implant region is closed with ab-
sorbable suture material. The neigh-
bouring teeth 43,42,32,33 are
lingually cauterised.
Figs. 18 & 19_Insertion of a Mary-
land provisional prosthesis, directly
after the augmentative-implantologi-
cal intervention.
Fig. 20_ DVT of excavation defect.
was 2/3 exposed on its vestibular side in region031. Both implants were primarily stable. Aftermeasuring the missing bone volume, a stab incisionwas made in the right retromolar. Then a conven-tional implant drill was driven through the gumsand drilled precisely 9 mm deep. When withdraw-ing the drill the bone meal was already able to be re-tained. Additionally further spongiose bone wasextracted with a mini-excavator.
The transplant bone was able to be adsorbed intothe implant body in an ideal manner. Finally a thingcollagen membrane was applied for complete cov-erage. The soft tissue defects were closed with ab-sorbable materials. The stab incision in the retro-molar was glued with cyanoacrylate. In regions031/041 the wound closure was carried out usingabsorbable suture material and horizontal mat-tress stitches.
Finally as a provisional restoration a Marylandtemporary prosthesis was affixed, which addition-ally ensured a good soft tissue stabilisation. A dig-ital volume tomography (DVT) was produced in or-der to evaluate the removal defect and documentthe augmentative result.
_Summary
Autologous bone grafting represents the goldstandard in augmentation surgery. Particularly withimplant operations it is often only shown intraop-eratively that a small quantity of autologous boneis needed for augmentation. In this situation quick
reaction is often indicated. The retromolar space isfrequented most often for this purpose. As the pa-tient should have the least possible discomfort dueto the bone extraction, minimally invasive proce-dures are the means of choice.
The technique presented above is a new methodwhich is impressive due to its minimally invasiveand simple characteristics. The shown procedure isespecially ideal for augmentation planning withvolumes up to 0.5 mg. Of course larger bone vol-umes can also be extracted using this minimally in-vasive method. Soft tissues can be closed discreetlyand so that they are hardly noticeable to the patientusing adhesive techniques. Minimally invasive pro-cedures in implantology can be perfectly plannedand executed by including modern 3-D-diagnostics(DVT)._
Dr Dr Steffen HohlDIC Dental Implant CompetenceEstetalstr. 121614 Buxtehude, Germanywww.dr-hohl.de
Dr Anne Sophie Brandt PetersenTandlaegerne i KogadeKogade 46270 Tonder, Denmarkwww.dentist.dk
_contact implants
Fig. 22
Fig. 19 Fig. 20 Fig. 21

PIEZON-MASTER-SURGERY.COM
TOUCH
’N’
GO

implants2_2010
_Discussion
There is an association between bone and softtissue preservation around implants with directinfluence on aesthetics.
Some authors have proposed different meth-ods to maintain supporting bone: improved im-plant micro-geometry and implant surfacetreatment, improved implant abutment connec-tion (elimination of bacterial reservoir, absenceof movements under bending forces) as well asthe use of wide implants with smaller sized abut-ments (platform switching concept).
An alternative in preserving marginal bonelevels around implants is the platform switchingconcept that refers to the use of a smaller diam-eter abutment on a larger diameter implant plat-form. This connection shifts the perimeter of theimplant—abutment junction (IAJ) inward to-wards the central implant axis.
Lazzara and Porter demonstrated that the in-ward movement of IAJ also shifts the inflamma-tory cell infiltrate inward and away from the
bone implant interface, creating a horizontal bi-ologic width that will limit bone resorptionaround the coronal aspect of the implant.
From a biomechanical perspective, stress inthe bone is concentrated around the crestal re-gion because of the difference in modulus ofelasticity between bone and implant, as demon-strated in photo - elastic and finite elementanalysis studies.14
Peak bone stresses occurring in marginalbone have been hypothesized to cause bone mi-cro-fracture and may be responsible, at leastpartially for peri-implant bone loss with saucer-ization patterns after prosthetic loading.
The issue of whether platform switching mayaffect stress patterns by minimizing peak bonestresses in the marginal bone has not beendemonstrated yet.
The original criteria established for assessingimplant success and survival6 identified mar-ginal bone levels as an important indicator formeasuring the response of the peri-implant tis-sues to functional loading.
More recent studies have considered the ef-fect of stresses established in bone by the directinfluence of non passive prosthetic work to be acausative factor in marginal bone loss.7, 8
Another more recent explanation of marginalbone loss is the theory of establishing the bio-logic width directly related to the position of theimplant-abutment microgap and its associatedmicrobial flora.9, 10
The concept of “platform switching” inimplant dentistryA literature review—Part II
Author_ Dr Virgil Koszegi Stoianov, Romania
implants2_2010
In addition, some studies have shown thatcertain designs in the geometry of implant coro-nal part may contribute to bone loss, while otherstudies have indicated that such bone loss can beprevented by incorporating a biomechanicalstable connection and a more retentive surfaceon the implant collar.11, 12
Prevention of horizontal and vertical mar-ginal peri-implant bone resorption during thepost-loading period is fundamental in maintain-ing stable gingival levels around implant-sup-ported restorations.13 It has been demonstratedthat peri-implant marginal bone loss is time-re-lated with significantly more acute bone lossduring the preloading period than in the follow-ing loading phases (two years after surgery) andalso during the first year after loading (sixmonths to one year after surgery) than in thesecond one (one year to two years after surgery).
Aesthetic outcomes cannot be attributed to asingle parameter. They are the result of a numberof important factors, especially in the aestheticarea.
Both biologic width and the integration ofplatform switching concept are of utmost sig-nificance in preserving a stable marginal bonelevel around implant neck. It is important to un-derstand mainly the meaning of biologic width.
Hence, the stable bone serves as a support forthe soft tissue determining the long-term aes-thetic and functional treatment, the outcomestability being ensured in this manner.
The following points should be noted: _ The use of a single post for temporary and final
prosthetic work;_ As long as the frequent replacement of parts is
not avoided, repeated destruction of the con-nective-tissue attachment of the biologicwidth occurs increasing the risk of bone re-sorption;
_A special implant and abutment design (a ledgeand integration of the biologic width/taperedshape of the post) facilitates nonsurgicallengthening and thickening of the peri-implantsoft tissue.
This leads to the establishment of a wider andmore resistant zone of connective tissue. A mi-cro-rough and nano-rough titanium surface ex-tending to the implant shoulder in conjunctionwith the platform switching concept providesosseous integration along the entire length ofthe implant.
A fine thread optimally distributes the masti-catory forces in the region of the implant neck,avoiding further bone loss in this region.15
Possible interactions amongst factors con-tributing to peri - implant bone loss.
These factors include:_Surgical and anatomical considerations such
as mucoperiosteal flap design, thickness ofbuccal and lingual cortical plates of bone re-maining after osteotomy preparation, bonequality, healing technique submerged or non-submerged, early unintentional cover screwexposure by mucosal dehiscence and amountof keratinized Gingiva;
_Patient risk factors such as medical and phar-macological status, habits including cigarettesmoking, poor oral hygiene, excessive alcoholconsumption, mucosal erosive pathology likelichen planus, previous or present periodontitis(chronic or aggressive);
_Biologic width related factors such as level ofthe micro-gap, platform switching and im-plant-tooth or implant-implant distance;
_Implant design including geometry, surface,length and diameter;
_Biomechanical factors including time of load-ing, type of loading, type of prosthesis, habitslike bruxism.
Flap designIt was reported in the literature long time
ago32 that, whenever a mucoperiosteal flap is re-flected about a tooth, some crestal bone resorp-tion will occur. Similarly elevating a flap to placea dental implant will lead to crestal bone loss andthere is evidence suggesting a direct relation-ship between size of full thickness flap and theresulting post op bone loss.
Other studies33 reported no statistically sig-nificant differences using more traditional his-tological evaluation of retrieved specimens aftertwelve weeks of site healing. Becker reported thesame magnitude of difference in buccal vertical

implants2_2010
bone loss as Jeong, one millimeter less for flap-less approach.
Alveolar bone thicknessThe main blood supply for buccal alveolar
bone is supplied by vessels in the overlyingmuco periosteum34 and is greatly affected by el-evating a full thickness flap to facilitate place-ment of a dental implant. Studies suggest that ifresidual facial bone thickness is less than 2 mmand/or if dehiscences or fenestrations of facialbone occurred during osteotomy preparation,consideration should be given to augmentingfacial bone thickness with GBR procedures.35, 36
Premature exposure of an implant coverscrew through the overlying mucosa may resultwhere mucosal tissues fail to achieve primaryclosure, or are too thin to avoid dehiscence, orhave been traumatized with the transitionalprosthesis. It was reported in the literature thatpatients with prematurely exposed cover screwssuffered 3.9 times greater bone loss than non-exposed ones.37
Quantity of keratinized tissueAdequate keratinized tissue may be more im-
portant around implants than natural teeth forseveral reasons: supracrestal collagen fibers areoriented in a parallel rather than in a perpendi-cular configuration adjacent to transmucosalsurfaces of implants38, providing less resistanceto local trauma and microbial penetration. Peri-implant mucosa may have a reduced capacity toregenerate itself due to compromised number ofcells and poor vascular suply.39
Oral hygiene, smoking, alcohol abusePatients with poor oral hygiene and/or exist-
ing periodontal disease experience greater peri-implant crestal bone loss than patient with goodoral hygiene and stable periodontal status. Both
current and lifetime cigarette are associatedwith deterioration in bone quality and impairedwound healing.40 Smoking has been shown to beone of the most significant factors predisposingto implant failure.41 Individuals who use alcoholin excess may have inadequate nutrition includ-ing vitamin deficits which may compromise ini-tial site healing.42
DiabetesIt is well known that diabetic patients are at
higher risk for developing periodontitis and arealso more prone to infection.43 It is very likelythat performance of dental implant will be af-fected as well. Poor metabolic control in dia-betic patients increases the risk of peri-implan-titis.44
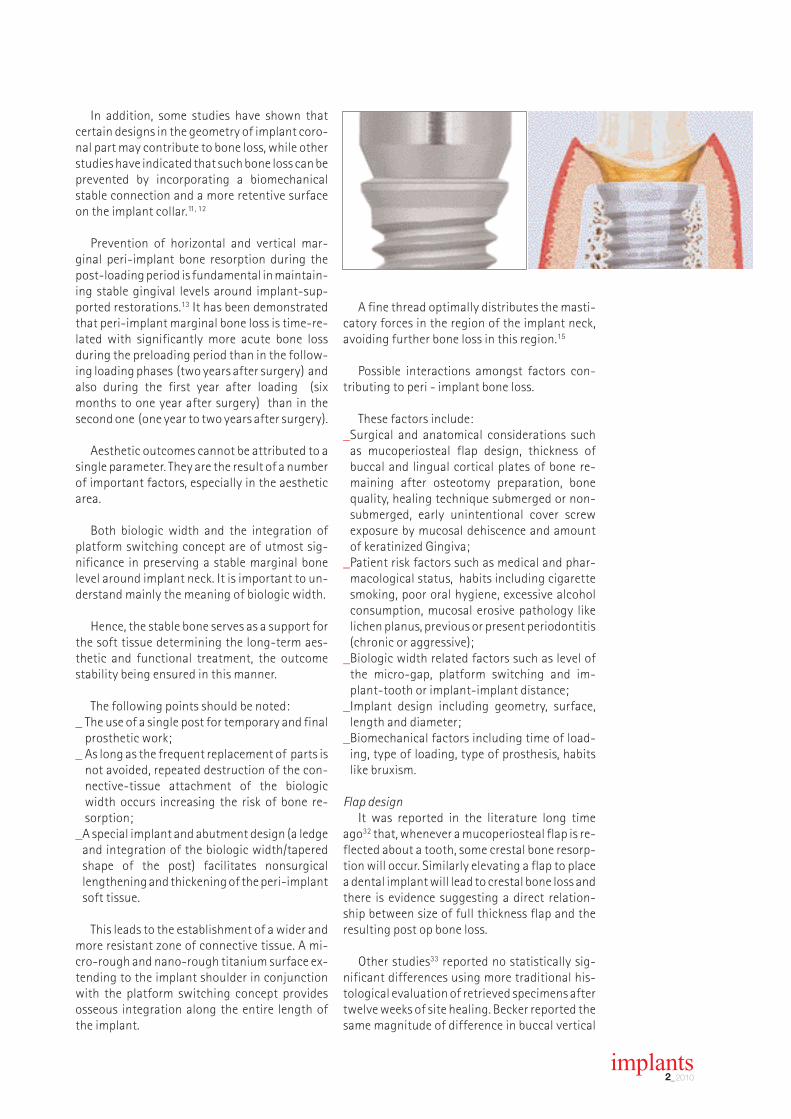
Biologic widthCrestal bone remodeling to establish “bio-
logic width” or soft tissue seal in peri-implantmucosal tissues is considered to be an importantfactor contributing to early crestal bone losswith all types of endosseous dental implants(Fig. 4).45, 46
Factors known to affect this crestal bone lossinclude the level of micro-gap in relation to thebone crest, platform switching achieved eitherby implant body design and/or by using an abut-ment smaller in diameter than the implant bodyand tooth-implant or inter-implant horizontaldistance. Another factor with deleterious effecton crestal bone resorption is considered to be therepeated removal and replacement of abut-ments because of disruption of the soft tissueseal.47
The biologic width has changed horizontallywithin the platform switched implant.
Level of the micro-gapThe connection between implant body and
prosthetic abutment is termed “micro-gap” and,in most cases, it is susceptible to microbial seed-ing and micro-movements between the partsduring clinical function. Both micro-gap and mi-cro-movements may lead to localized inflam-mation and associated crestal bone loss if themicro-gap is within a minimum distance fromthe alveolar crest. Biologic width around theneck of a dental implant constitutes a mucosalseal intended to protect the underlying bone. Itis formed apically to the micro-gap and requiresa minimum of about 1.5 mm of fibrous connec-tive tissue between bone and epithelial attach-ment of the gingival sulcus of the implant (Fig. 5).48, 49

The new kit for success.
www.geistlich-pharma.com LEADING REGENERATION
Geistlich Combi-Kit Collagen – the best kit for successful and predictable results in ridge preservation and minor augmentations.
combined in Geistlich
Combi-Kit Collagen
Geistlich
Bio-Oss® Collagen and
Geistlich Bio-Gide®
From MAY 2010

implants2_2010
Platform switchingThis design feature can be created in an im-
plant body or achieved by the clinician using acompatible abutment of a narrower diameterthan the implant platform. It can be acquiredeven with the healing abutment in case of non-submerged approach. The purpose of platformswitching is to create a horizontal componentfor the total linear distance between micro-gapand bone crest required for biologic width50 andeventually to shift the stress concentration awayfrom the cervical bone-implant interface.51
Generally, the horizontal component createdby platform switching is around 0.5 mm (Fig. 6),sufficient to result in significantly less radiolog-ical detectable crestal bone loss in humans.51, 52
Not only does this concept reduce the risk ofperi-implantitis in the future but also has thebenefit in the aesthetic zone of providing bettersoft tissue support.53
Implant-tooth or inter-implant distanceFor single tooth dental implants, a minimum
horizontal distance of 1.5 mm must be left be-tween the implant and the two approximatingtooth root surfaces in order to avoid crestal boneloss after biologic width accommodation.
When two implants are placed side by side,the crestal bone loss that occurs between themhas a more complicated aetiology. First and fore-most, inter-implant crestal bone loss will be af-fected by the horizontal distance between thetwo implants which should be minimum 3 mm(Fig. 7). It will also be influenced by the level ofmicro-gap, biologic width, and whether plat-form switching was used or not. A clear tendencyfor increased inter-implant vertical bone lossoccurs as the distance between two implants de-creases below 3 mm.54, 55
Histological data from animal experimentsusing 2—piece, moderately rough surface, sub-merged implants, showed that vertical inter-implant bone loss decreased from 1.98 mm for a2 mm inter-implant distance to 0.23 mm for 5 mm inter-implant distance.56
_Conclusion
Significant differences in marginal bone losshave been identified between implants withplatform switching and implants without plat-form switching only in the first year after load-ing. It may be concluded that the platformswitching concept represents a bone preservingtechnique.
Preservation of crestal bone around dentalimplants cannot be attributed to a single param-eter. That is the result of a number of importantfactors, especially in the challenging aestheticzone.
It is important to understand the mechanismthat permits the implant-abutment connectionto maintain a seal against the bacterial ingressbefore and after loading due to absence of mi-cromovements.
An appropriate understanding of the impor-tance of biologic width and the use of platformswitching concept in the routine treatment is ofreal support in maintaining a more stable mar-ginal bone level around implants.
This stable marginal bone as a support of thesoft tissue is determinant for the long-term aes-thetic stability.
Further neutral clinical studies are required todemonstrate the importance of micro-gap, bio-logic width and platform-switching in crestalbone preservation around dental implants.
For the support I thank:Dr. Mazen Tamimi, Private Practice, Amman,
Jordan, Dr. Rainer Valentin, Private practice,Cologne, Germany, Dr. R. & M. Vollmer, Privatepractices, Wissen, Germany
Editorial note: The literature list can be re-quested from the author.
Dr Virgil Koszegi Stoianov MscOffice: Str.Paciurea No. 5300036 Timisoara, RomaniaTel.: +40 356433733Mobile: +40 723573443E-mail: [email protected]
_contact implants


implants2_2010
_ Introduction
Zygomatic implants, first introduced byBrånemark in 1988, are especially suitable for pa-tients with advanced atrophy of the maxilla andwho refuse or have suffered a complication afterbone grafting procedures. The few studies withlarge samples and adequate follow-ups1-6, showexcellent results. Survival and success rates, aswell as, the incidence of complications are de-tailed below based on a Medline review on zygo-matic implant papers.
Traditionally, these implants had a palatalemergence, crossed the maxillary sinus and wereanchored in the zygomatic bone. Nowadays, thepalatal emergence can be avoided by using the“extramaxillary” implants technique, where thezygomatic implant goes through the lateral wallof the maxillary sinus. The high survival rates(higher than 90 %) and the low incidence of com-plications reported in the reviewed papers, makezygomatic implants a good treatment option forthe rehabilitation of severely resorbed maxillas. Inthis paper, the authors will address the anatomyof the region, the indications of these implants,the several available surgical techniques, the sur-vival rates and complications.
_The zygomatic implant
The classical zygomatic fixture design (Bråne-mark Osseointegration Centre and Exopro,Gothenburg, Sweden) was a self-tapping implantin c.p. (commercially pure) titanium with a well-defined machined surface. It was available in dif-ferent lengths ranging from 30 to 52.5 mm, andwas slightly tapered (coronal diameter of 4.5 mm
and apical diameter of 4.0 mm). This diametervariation was due to the necessity of increasingthe anchorage at the alveolar process while re-ducing the risk of complications (orbital bleeding,infraorbitary nerve affectation, etc.) in the apicalregion. The coronal portion of the implant pre-sented a tilted connection of 45° to facilitate theprosthetic rehabilitation.1
At present, this implant has a rough surfaceand the coronal portion of the implants may pres-ent different angles ranging from 25° to 55°.Boyes-Varley et al. 7 proposed a 55° angle in orderto avoid the palatal emergence of the prostheticconnection, which is one of the most discussedinconveniences of these fixtures.
_Anatomical basis for the zygomatic implant
The zygomatic bone could be compared to apyramid, offering a solid anatomic structure forimplant anchorage.8 A histological analysis of thisarea revealed the presence of a regular and densebone with very high osseous density (up to 98 %).9
Due to these features, the zygomatic bone has al-ready been used to place miniplates as a part ofthe orthodontic treatment. According to ananatomical study, the mean length of useful bonein this region is 14 mm.10
_Indications of the technique
According to Malevez et al.6 and Aparicio et al.11
the zygomatic implants are a valid alternative tobone grafting in patients with advanced maxillaryatrophy. This technique would be suitable whenthe following conditions are present:
Rehabilitation of atrophicmaxillas using zygomaticimplantsA literature review
Authors_Joan Pi-Urgell1, Javier Mir-Mari2, Rui Figueiredo & Cosme Gay-Escoda3, Spain
implants2_2010
1. Light to moderate bone atrophy in the anteriorregion of the maxilla, with a posterior resorp-tion of the alveolar process: This situation al-lows the placement of two to four implants inthe anterior region, but the resorption of theposterior maxilla makes the placement of stan-dard fixtures in this area unfeasible. In this casetwo zygomatic implants will be placed, one foreach side.
2. Advanced atrophy of the maxilla (anterior andposterior): In this case two options are avail-able: the use of bone grafting techniques in theanterior region can be performed and theplacement of two zygomatic implants for theposterior region; or the placement of four zy-gomatic implants, two on each side withoutany anterior standard implants.
_Presurgical evaluation
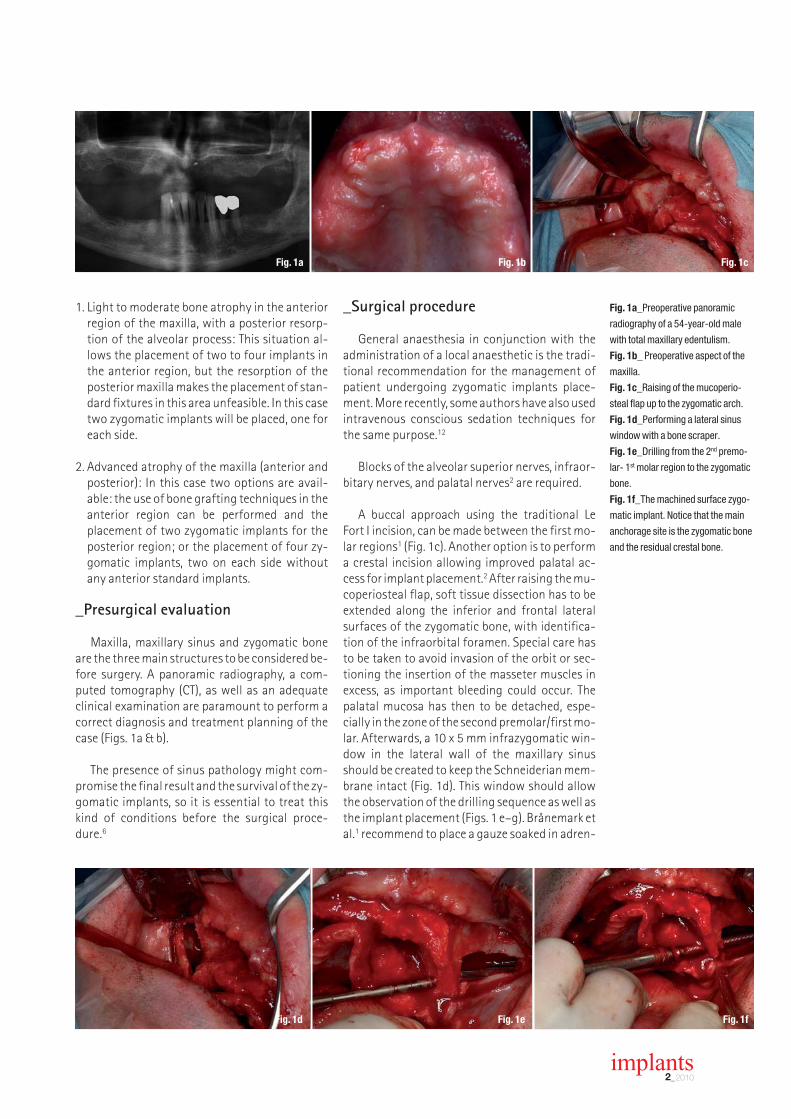
Maxilla, maxillary sinus and zygomatic boneare the three main structures to be considered be-fore surgery. A panoramic radiography, a com-puted tomography (CT), as well as an adequateclinical examination are paramount to perform acorrect diagnosis and treatment planning of thecase (Figs. 1a & b).
The presence of sinus pathology might com-promise the final result and the survival of the zy-gomatic implants, so it is essential to treat thiskind of conditions before the surgical proce-dure.6
_Surgical procedure
General anaesthesia in conjunction with theadministration of a local anaesthetic is the tradi-tional recommendation for the management ofpatient undergoing zygomatic implants place-ment. More recently, some authors have also usedintravenous conscious sedation techniques forthe same purpose.12
Blocks of the alveolar superior nerves, infraor-bitary nerves, and palatal nerves2 are required.
A buccal approach using the traditional Le Fort I incision, can be made between the first mo-lar regions1 (Fig. 1c). Another option is to performa crestal incision allowing improved palatal ac-cess for implant placement.2 After raising the mu-coperiosteal flap, soft tissue dissection has to beextended along the inferior and frontal lateralsurfaces of the zygomatic bone, with identifica-tion of the infraorbital foramen. Special care hasto be taken to avoid invasion of the orbit or sec-tioning the insertion of the masseter muscles inexcess, as important bleeding could occur. Thepalatal mucosa has then to be detached, espe-cially in the zone of the second premolar/first mo-lar. Afterwards, a 10 x 5 mm infrazygomatic win-dow in the lateral wall of the maxillary sinusshould be created to keep the Schneiderian mem-brane intact (Fig. 1d). This window should allowthe observation of the drilling sequence as well asthe implant placement (Figs. 1 e–g). Brånemark etal.1 recommend to place a gauze soaked in adren-
Fig. 1a_Preoperative panoramic
radiography of a 54-year-old male
with total maxillary edentulism.
Fig. 1b_ Preoperative aspect of the
maxilla.
Fig. 1c_Raising of the mucoperio-
steal flap up to the zygomatic arch.
Fig. 1d_Performing a lateral sinus
window with a bone scraper.
Fig. 1e_Drilling from the 2nd premo-
lar- 1st molar region to the zygomatic
bone.
Fig. 1f_The machined surface zygo-
matic implant. Notice that the main
anchorage site is the zygomatic bone
and the residual crestal bone.
Fig. 1a Fig. 1b Fig. 1c
Fig. 1d Fig. 1e Fig. 1f

Fig. 1g_Final aspect of the maxilla.
See the abutments for immediate
loading and the palatal position of the
distal implant in the first quadrant.
Fig. 2a_Metal-ceramic full-arch
rehabilitation with four anterior im-
plants and two zygomatic implants.
Notice the palatal emergence of the
zygomatic implants.
Fig. 2b_Detail of the palatal
emergence.
implants2_2010
aline inside the sinus for a few minutes to preventbleeding and deter mucosal tissue from blockingthe view.
_Technique modifications
The main disadvantage of this technique is re-lated to the palatal emergence (Figs. 2a & b) of theimplants that complicates the design of the pros-thesis, reduces the patient’s ability to speak andcompromises the long-term health of the peri-im-plant tissues due to the difficulty that patients haveto clean this area. Secondly, due to the intrasinusalpath of the implants the risk of sinus pathology de-velopment must be considered.2
Recently, some authors have proposed modifica-tions of the classical technique described before. Wewould like to emphasize the following:
Extramaxillary implantsBasically, it consists of a modification of the im-
plant entrance in the alveolar process and its trajec-tory up to the zygomatic bone.14 In this technique,the implant emergence is located just in the middleof the alveolar process, hence correcting the palatalentrance of the Brånemark technique. In its trajec-tory to the zygomatic bone, the fixture goes throughthe lateral sinus wall keeping the Schneiderianmembrane intact. This technique not only improvesthe design of the prosthesis but also seems to reducethe incidence of sinusitis. Malo et al.14 and Aparicioet al.15 have already published some reports with ex-cellent results (98.5–100 % survival rates). On theother hand, the main complaint would be the factthat the middle part of the implant rests in directcontact with the soft tissue of the cheek.
Zygomatic implants without anterior standardimplants
Frequently, the high degree of maxillary atrophyof these patients forces the surgeon to performbone grafting techniques in the anterior area of themaxilla in order to place four standard implants. Amodification first described by Bothur et al.16 rec-ommended the placement of four to six zygomatic
implants in order to avoid the need of anterior fix-tures and therefore to reduce the necessity of bonegrafting in this area. In a study with 40 edentulousskulls, with atrophic alveolar processes and pre-maxillas, Rossi et al.17 measured the distances be-tween the alveolar process emergence at the canineregion and the premolar/molar region to the zygo-matic bone. The authors stressed the fact that themean length of distance between the canine regionsto the zygomatic bone was 53.42 mm and the max-imum distance was 61.94 mm. Given that thelongest commercially available implant is 52.5 mm,the authors emphasize the importance of a precisepresurgical evaluation of the available distancewhen the placement of four zygomatic implants isplanned.
Sinus-slot technique Stella and Warner18 described this method in
2000. Mainly, the “slot technique” is a reduction ofthe sinus wall perforation doing a slot instead of awindow. Likewise, this modification permits a goodcontrol of the drilling direction and insertion of thezygomatic fixture. Furthermore, according to theauthors a higher amount of bone is preserved andalso the flap size can be reduced, improving the pa-tients’ postoperative recovery. Peñarrocha et al.12
published in 2007 a series of 21 cases with the “Slottechnique” with a 100 % survival rate, but theSchneiderian membrane was perforated in all cases,even though the incidence of sinus pathology waslow (two cases).
Immediate loadingTraditionally, the zygomatic implant loading pro-
tocol has been a two-stage approach. Nowadays,just a few numbers of authors have published resultswith an immediate loading protocol. To our knowl-edge, the first case-series was published in 2006 byBedrossian et al.19 The review included a total of 28zygomatic implants and 55 standard implants thatwere loaded immediately after surgery. The authorsreported very good results with a survival rate of100 % and without any complications. Other recentstudies have also reported similar findings with sur-vival rates ranging from 95.8 % to 100 %.4, 14, 15, 20-22
Fig. 1g Fig. 2a Fig. 2b

_Survival rates
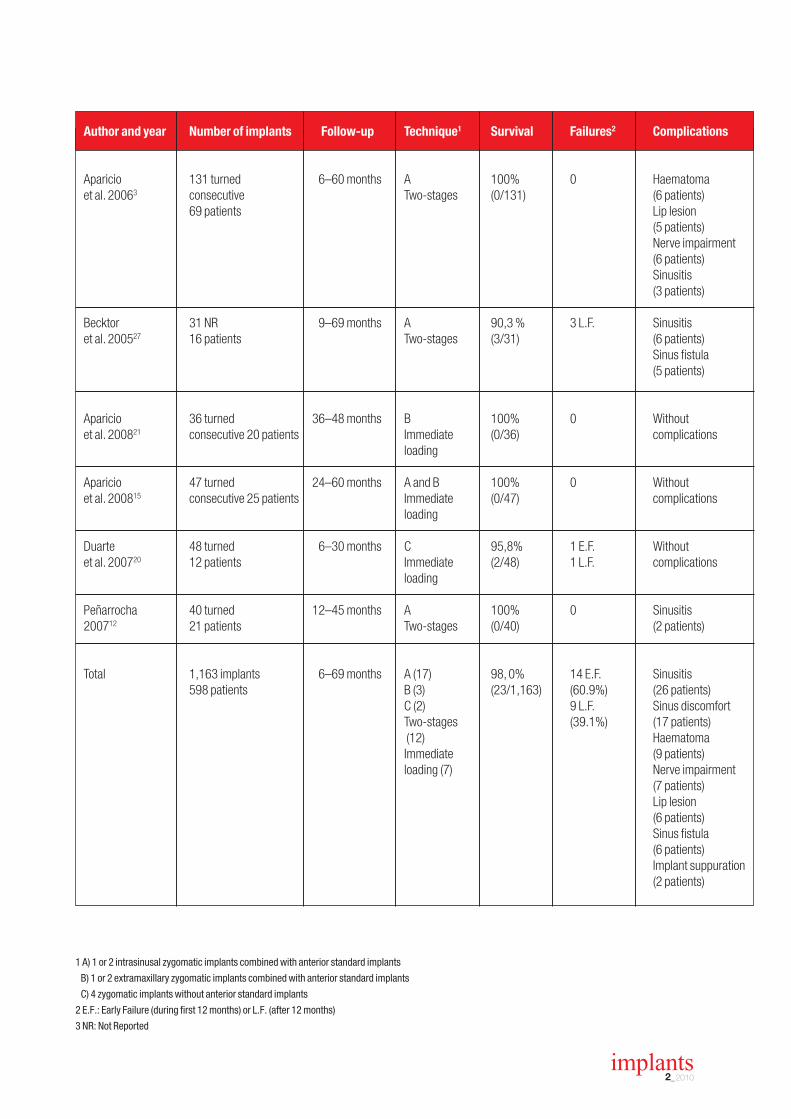
The literature review revealed a mean survival rate for zygomatic implants higherthan 90 %, regardless of the technique used. The most common option is the classi-cal technique, with machined surface implants, in a two-stage loading protocol.Twelve of the 19 papers reviewed with follow-up, met this criteria.1-3, 5-7, 12, 23-27
The other alternatives also present very good results with 95.8–100 % survival rates.4, 14, 15, 19-22 A surprising outcome is that the survival rate of the standard im-plants placed in the anterior region is quite low (73–98 %). This is probably related tothe high degree of resorption that surgeons find in this area, therefore requiring morecomplex grafting procedures.
A total of 1,163 zygomatic implants were found in our review of 19 articles withadequate follow-up. Twenty-three implants (2.0 %) were lost, 14 (60.1 %) during theosseointegration period and nine (39.1 %) after loading. These data can be observedin table 1.
_Complications
Sixteen papers reported complications. Different authors comment as possiblecomplications orbital lesions, maxillary sinus posterior wall and infratemporal fossaperforation, intraoperative bleeding, nerve lesions (infraorbitary nerve), sinuspathology, lip lesion during the drilling, among others. Nevertheless, only some ofthese were actually registered in the reviewed studies (26 cases of sinus patho -logy1-3, 5, 12, 14, 22, 23, 26, 27, seven cases of infraorbitary nerve impairment3, 5, six cases oflip lesion during drilling3, 23 and nine cases of suborbital haematoma3, 23).
It is important to stress that most of the cases with sinus pathology werefavourably solved. Some of them only needed pharmacological therapy, while others were treated with an antrostomy surgery. Only three zygomatic implants, allfrom the same report27, were removed due to their association with recurrent si-nusitis.
_Discussion
First of all, the few number of papers published related with zygomatic implantswas surprisingly low, 59 articles in our Medline review (December, 2009). Amongthem, only 19 presented follow-up results.1-7, 12, 14, 15, 19-27 Moreover, most of the au-thors are broadly experienced oral surgeons, which may difficult the reproducibilityof their results.
Among all published techniques and modifications, the most common treatmentoption published is the classical technique, with machined surface implants, in a two-stage loading protocol (12 studies).1-3, 5-7, 12, 23-27 Another important factor is that themajority of the studies have reduced samples (only five articles had more than 100implants)2, 4-6 and short follow-up times (only Brånemark et al.1 presented a follow-up of five to ten years). These are important limitations that need to be corrected infuture research. Nevertheless, the placement of these implants seems to be a goodtreatment option since the published results so far are excellent, regardless of theused technique (95.8–100 %). On the other hand, the standard implants placed in theanterior region have low survival rates (73–98%). These differences could be relatedwith the grafting techniques used in combination with the cited conventional im-plants. Accordingly, Brånemark et al.1 presented a 73% survival rate of the standardimplants, but in this study, 70% of the patients received bone grafts in the same sur-gical procedure in which the anterior implants were placed.
The failure pattern of zygomatic implant is very similar to that of the standard im-plants. If one takes the studies cited in this review into account, a total of 23 implants
������������������ ���
*Pric
es in
clud
e sh
ippi
ng a
nd V
AT
I hereby agree to receive a free trail subscription of ����������� ��� ��� � ������ ������������� (4 issues per year). I would like to subscribe to cos-metic dentistry for € 44* for German customers, € 46*for customers outside Germany, unless a written can-cellation is sent within 14 days of the receipt of the trialsubscription. The subscription will be renewed auto-matically every year until a written cancellation is sentto OEMUS MEDIA AG, Holbeinstr. 29, 04229 Leipzig,Germany, six weeks prior to the renewal date.
Reply per Fax +49 341 48474-290 to OEMUS MEDIA AG or per E-mail to [email protected]
First Name
Last Name
Company
Street
ZIP/City/County
Signature
Signature
Notice of revocation: I am able to revoke the subscription within14 days after my order by sending a written cancellation toOEMUS MEDIA AG, Holbeinstr. 29, 04229 Leipzig, Germany.
������������ �
OEMUS MEDIA AGHolbeinstraße 29, 04229 Leipzig
Tel.: +49 341 48474-0Fax: +49 341 48474-290
E-Mail: [email protected]� �����
���������� ��� ��� � ������ ������������
AD

implants2_2010
Table 1_ Results from the reviewed studies with adequate follow-ups.
Bränemark 52 turned consecutive 5–10 years A 94% 2 E.F. Implant suppuration et al. 20041 28 patients Two-stages (3/52) 1 L.F. (2 patients)
Sinusitis(2 patients)
Pi-Urgell 101 turned 1–72 months A 96,0% 2 E.F. Sinusitis (1 patient)et al. 20082 54 patients Two-stages (4/101) 2 L.F.
Ahlgren 25 NR3 11–49 months A 100% 0 Haematoma et al. 200623 13 patients Two-stages (3 patients)
Lip lesion (1 patient)
Al-Nawas 20 NR 12–30 months A 95% 1 E.F. Sinus fistula et al. 200424 4 patients Two-stages (1/20) (1 patient)
Balshi 110 9–60 months A 96,4% 4 E.F. Not reportedet al. 20094 76 turned Immediate (4/110)
34 TiUnite loading56 patients
Bedrossian 44 turned 34 months A 100% 0 Not reportedet al. 200225 22 patients Two-stages (0/44)
Bedrossian 28 TiUnite 12 months A 100% 0 Without et al. 200619 14 patients Immediate (0/28) complications
loading
Boyes-Varley 77 NR 6–30 months A 100% 0 Not reportedet al. 20037 47 45° Two-stages (0/77)
30 55°45 patients
Davo 36 turned consecutive Mean A 100% 0 Sinusitis et al. 200722 18 patients 14 months Immediate (0/36) (1 patient)
loading
Farzard 22 turned 18–46 months A 100% 0 Sinus discomfort et al. 200626 11 patients Two-stages (0/22) (3 patients)
Kahnberg 145 36 months A 96,3% 3 E.F. Sinus discomfortet al. 20075 Turned and TiUnite Two-stages (5/145) 2 L.F. (14 patients)
76 patients Sinusitis (1 patient)Nerve impairment (1 patient)
Malevez 103 turned 6–48 months A 100% 0 Sinusitis et al. 20046 55 patients Two-stages (0/103) (6 patients)
Maló 67 TiUnite 6–18 months A, B, C 98,5% 1 E.F. Sinusitiset al. 200814 29 patients Immediate (1/67) (4 patients)
loading
Author and year Number of implants Follow-up Technique1 Survival Failures2 Complications
implants2_2010
Aparicio 131 turned 6–60 months A 100% 0 Haematoma et al. 20063 consecutive Two-stages (0/131) (6 patients)
69 patients Lip lesion (5 patients)Nerve impairment (6 patients)Sinusitis(3 patients)
Becktor 31 NR 9–69 months A 90,3 % 3 L.F. Sinusitis et al. 200527 16 patients Two-stages (3/31) (6 patients)
Sinus fistula (5 patients)
Aparicio 36 turned 36–48 months B 100% 0 Without et al. 200821 consecutive 20 patients Immediate (0/36) complications
loading
Aparicio 47 turned 24–60 months A and B 100% 0 Without et al. 200815 consecutive 25 patients Immediate (0/47) complications
loading
Duarte 48 turned 6–30 months C 95,8% 1 E.F. Withoutet al. 200720 12 patients Immediate (2/48) 1 L.F. complications
loading
Peñarrocha 40 turned 12–45 months A 100% 0 Sinusitis 200712 21 patients Two-stages (0/40) (2 patients)
Total 1,163 implants 6–69 months A (17) 98, 0% 14 E.F. Sinusitis598 patients B (3) (23/1,163) (60.9%) (26 patients)
C (2) 9 L.F. Sinus discomfortTwo-stages (39.1%) (17 patients)(12) HaematomaImmediate (9 patients)loading (7) Nerve impairment
(7 patients) Lip lesion (6 patients)Sinus fistula (6 patients)Implant suppuration(2 patients)
1 A) 1 or 2 intrasinusal zygomatic implants combined with anterior standard implants
B) 1 or 2 extramaxillary zygomatic implants combined with anterior standard implants
C) 4 zygomatic implants without anterior standard implants
2 E.F.: Early Failure (during first 12 months) or L.F. (after 12 months)
3 NR: Not Reported
Author and year Number of implants Follow-up Technique1 Survival Failures2 Complications

were lost (23/1163; 2.0 %), fourteen (60.1 %) beforeloading and nine (39.1 %) after loading. Only one au-thor (Pi-Urgell et al.)2 presented the fracture of oneof the zygomatic implants, which is probably a rarecomplication. Farzard et al.26 observed that the mar-ginal bone loss in the zygomatic implants would rep-resent a decrease in the stability of the implant overtime, with progressively lower Implant Stability Quo-cient (ISQ) values (<50). This confirms that the mainanchorage site of the zygomatic implants is the zy-gomatic bone, especially in the long term, since andthe resorption of the residual crestal bone can occur.This unfavourable biomechanical situation couldeventually lead to an increase in the incidence of im-plant fractures in future studies with long follow-ups.
Although some authors comment on the level ofsatisfaction or quality of life in their reports6, 19, 28,only Al-Nawas et al.24 introduce success criteria intheir results. These authors analysed the periimplantsoft tissue’s health (gingival bleeding index, probingdepth, microbiological testing, etc.) concluding thatonly eleven of the 20 zygomatic implants (55 %)would be considered successful, while the survivalrate was 95%.
A precise surgical evaluation of the patient ismandatory in this complex technique, since seriouscomplications might occur, especially due to thelength of the implant and to the presence of impor-tant anatomical structures (orbit, infratemporalfossa, etc) in the zygomatic anchorage area. More-over, our literature review showed a low rate of com-plications (9.5 %), all being minor problems. Sinuspathology seems to be the most frequent complica-tion, although other conditions have been reported.According to Maló et al.14 the sinus pathology is re-lated to previous episodes of sinusitis or to the intra-operative perforation of the Schneiderian mem-brane. On the contrary, other authors like Brånemarket al.1 mention in their article that no special effortwas made to keep the sinus membrane intact. As amatter of fact, Peñarrocha et al.12, perforated all thesinus membranes in their study with 40 zygomaticimplants and reported only two cases of sinusitis.This is an interesting aspect to discuss in future re-search, since the available data is clearly insufficient.When sinus pathology is diagnosed long after im-plant placement, it is difficult to identify the cause ofthe sinusitis. In fact, only one of the papers men-tioned the removal of three implants because the pa-tients had frequent episodes of sinus infections. Onthe other hand, all the other authors decided tomaintain the implants and the sinus pathologieswere favourably managed with antibiotics or withantibiotics in combination with antrostomy surgery.The maxillary sinus could also be affected if there is a
substantial marginal bone loss, as described by Al-Nawas et al.24 In these cases, the infection will reachthe maxillary sinus through the periimplant pockets.
The lack of stability, aesthetics and/or function ofthe prosthesis and the deficient hygiene of the abut-ment areas are also important complications. Prob-ably, these are often related to the palatal emergenceof the zygomatic implants. Nowadays, this limitationhas been solved with the extramaxillary implantsprocedure.14, 21 Nevertheless, the long-term exposureof the titanium threads to the cheek’s soft tissue hasto be evaluated carefully.
_Conclusions
Based on the current literature review, zygomaticimplants show excellent survival rates (>90 %) and alow incidence of complications, so this should beconsidered a valid and safe treatment option whendealing with patients with advanced maxillary atro-phy. Nevertheless, the authors would like to expresstheir concern with the scarce amount of publishedstudies (most of them of retrospective nature), withthe low level of scientific evidence available, and withthe lack of studies with long follow-up periods. Theintroduction of success criteria also based on peri-odontal parameters should be considered in futureresearch._
Editorial note: A complete list of references is avail-able from the publisher.
implants2_2010
Dr Rui FigueiredoDDSAssociate professor of the Oral Surgery and Im-plantology Department, Barcelona Institut de Recerca Biomèdica de Bellvitge (IDIBELL)Facultat d’OdontologiaUniversitat de BarcelonaCampus de BellvitgePavelló de Govern 2a planta, Despatx 2.908907 – L’Hospitalet de Llobregat,SpainPhone: +34 93 402 42 74E-mail: [email protected]
1 MD, DDS., Professor of the Master degree pro-gram of Oral Surgery and Implantology, Barcelona
2 DDS. Fellow, Master degree program of Oral Sur-gery and Implantology, Barcelona
3 MD, DDS, PhD. Chairman, Oral Surgery and Im-plantology Department, and Director, Master de-gree Program of Oral Surgery and Implantology,Barcelona.
_contact implants

Anniversary Conference
Please fax this form to: +49-3 41/4 84 74-2 90� More information:
40th International Annual Congress of the DGZI
October 1–2, 2010, Berlin, Germany
office stamp
implants 1/10
�
40th International ANNUALCongress OF THE DGZI
October 1–2, 2010, Berlin, Germany
Essential Oral Implantology
�
Gold Sponsor Silver Sponsor Bronze Sponsor

implants2_2010
2010
1st Croatian-German Implantology Meeting of DGZIWhere: Hvar, CroatiaDate: 10–12 June 2010Website: www.hvarkongres.hr
FDI Annual World Dental CongressWhere: Salvador da Bahia, BrazilDate: 02–05 September 2010Website: www.fdiworldental.org
7th Forum of Innovations in DentistryWhere: Leipzig, GermanyDate: 10–11 September 2010Website: www.event-fiz.de
40th International Congress of DGZIWhere: Berlin, GermanyDate: 01–02 October 2010Website: www.dgzi.de
19th Annual Scientific Meeting of EAOWhere: Glasgow, ScotlandDate: 06–09 October 2010Website: www.eao.org
AAID 59th Annual MeetingWhere: Boston, MA, USADate: 20–23 October 2010Website: www.aaid.com
96th Annual Meeting of AAPWhere: Honolulu, USADate: 30 October–2 November 2010Website: www.perio.org
17th AIDC 2010Where: Alexandria, EgyptDate: 2–5 November 2010Website: ww.aidc-egypt.org
Greater New York Dental MeetingWhere: New York, NY, USADate: 26 November–01 December 2010Website: www.gnydm.org
2011
34th International Dental ShowWhere: Cologne, GermanyDate: 22–26 March 2011E-Mail: [email protected]: www.ids-cologne.de
International Osteology SymposiumWhere: Cannes, FranceDate: 14–17 April 2011Website: www.osteology-cannes.org
International events

implants2_2010
_The large number of participants (40 in total)who attended DGZI’s (German Association of DentalImplantology) weekend course “Anatomy” in earlyOctober 2009 in Dresden has clearly shown that manycolleagues want to be kept up to date about researchin this field, in order to make the right professional de-cisions. This course is now also offered in English.
Thanks to the clearly-structured concept and atheoretical introduction (an impressive demonstra-tion including a live video broadcast from the dissect-ing room and patient-side practices using humanspecimens), the participants obtained the profes-sional skills needed by practicing surgeons and im-plantologists in only two days.
A specially designed DGZI course module foranatomy has already been part of the Implantologycurriculum for one decade. In particular, colleagueswho only want to refresh their anatomical knowledgein a two-day professional training course can registerfor the current weekend course—ideal for colleagueswho may have realized that two years after their stateexamination they are no longer able to recall the enor-mous knowledge required. Consequently there weremany guest participants who took part in the Implan-tology curriculum. The contributions of anatomist Dr med. habil. Wolfgang Schwab of TU Dresden, oralbiologist and anatomist Prof Dr Werner Götz of the University of Bonn, dissection assistant UteNimtschke, implantologists Dr Rainer Valentin and Dr Rolf Vollmer, and oral surgeons Dr Martina Vollmerand Dr Uta Voigt meant that the course was in com-petent hands as well as ensuring that the differentpoints of view of the various disciplines were consid-ered. The first day of the course was dedicated to athorough introduction to the anatomy of the skull, in-cluding an exact demonstration of the supply for
nerves and blood vessels and the anatomy of bones,tongue, throat and larynx. In order to explain the par-ticular surgical basics, the speakers demonstrated theprocedures used for autologous and xenogenousaugmentation and those for bone spreading. Thehighlight of the day was the application by Dr med.habil. Schwab and Prof Dr Götz theoretically obtainedknowledge to an actual anatomical specimen. Cour-tesy of certain modern techniques, including thevideo broadcast from the dissecting room, the partic-ipants could ask questions in real time during thepresentation. The second day of the course startedagain with a theoretical introduction—this time Dr Rolf Vollmer introduced the different implanto-logical techniques. The sponsoring companies(Geistlich, mectron, Schütz, Zepf) explained the fea-tures of all of the instruments and working materialswhich they had provided so that the participantscould practice the acquired techniques with them.Towards the end, Dr Schwab and Dr Valentin demon-strated an autologous bone removal from the iliaccrest. This highly successful professional trainingweekend was completed efficiently and to high stan-dard. All participants agreed that a follow-up of thiscourse should take place in October 2010._
DGZI’s anatomyweekend a full success!Author_Dr Christian Ehrensberger, Germany

I meetings _ Academy of Osseointegration
implants2_2010
_Various approaches, complications amongmeeting highlights, different approaches to implanttherapy and solutions to unexpected complicationswere among the highlights of the Academy of Os-seointegration’s 25th Anniversary Annual Meeting,March 4–6, at the Walt Disney World Dolphin Resortin Orlando.
It is no surprise that the German Association ofDental Implantology (DGZI) took part in this year’scongress in the United States of America, as the AO isthe DGZI’s largest affiliated association. Members ofthe Board Dr Rainer Valentin and Dr Rolf Vollmer aswell as DGZI’s international representative Dr MazenTamimi attended lectures and exhibitions at the WaltDisney World Dolphin Resort.
To start the conference the current President ofthe AO Vincent J. Jacono presented the congress pro-gram and noted that the Academy’s mission should bethe improvement of oral health. In order to be able todo so, colleagues were brought up to date about thestate of the art in implantology and tissue regenera-tion.
The 25th anniversary annual meeting started onThursday, March 4, with the opening symposium, “AQuarter Century of Experience: The Formula for Pre-dictable Implant Success in the Esthetic Zone.” OtherAO Annual Meeting highlights included Hands-onworkshop: The pre-meeting, daylong series of ses-sions explored how 3-D imaging and navigation tech-nology helps providers fabricate surgical templates,generate final prosthesis and place implants more ef-fectively as part of the “team approach” concept.
AO’s 2010 Corporate Forum featured 36 manufac-turer-hosted educational sessions concerning thelatest research, products and developments. Duringthe congress different options concerning implanttherapies and solutions for unexpected complica-tions were discussed in details in the main podium.Colleagues could also attend hands-on workshopsand listen to the AO corporate panel.
“Treatment Approaches: Controversies in ImplantDentistry,” held on Friday, March 5, and Saturday’s“Unexpected Complications: Complications and So-lutions,” were the key pillars of the meeting’s overall
25th Anniversary of theAcademy of OsseointegrationAuthors_Dr Rolf Vollmer & Dr Rainer Valentin, Germany

meetings _ Academy of Osseointegration I
implants2_2010
theme, “The Formula for Predictable Implant Suc-cess.”
Approaches, controversies Friday’s implant ther-apy program gathered an international roster of ex-perts to review the latest treatments and materialsthrough an evidence- based approach. Saturday’ssession on complications explored why problems oc-cur, how to treat them and what we can do to preventthem.
“Two-Track” scientific program The surgical track explored “Surgical Procedures to
enhance implant success in the Esthetic Zone.” Therestorative track, “Where, When, Why and How,” cov-ered prosthetic considerations for restoring angled ortilted implants; endodontics vs. implants and earlypredictors for biological and technical complications.
Round table clinics Twelve separate sessions offered attendees the
opportunity to discuss diverse topics.
Limited attendance lectures Increased interaction between annual meeting at-
tendees and world-class clinicians on a wide range oftopics.
Allied staff program The annual meeting’s allied staff program offered
concurrent sessions designed for dental lab techni-cians and hygienists.
In addition, colleagues from all over the world ex-hibited more than 250 posters throughout the con-ference. One full day was dedicated to surgical prob-lems in the esthetic zone as well as to the types of es-thetic problems prosthodontists have to deal with.The prosthetic handling of angulated placed im-plants, biological and technical complications, andendodontics, which completes against implants, werediscussed in particular. Altogether this was a very suc-cessful congress with more than 2000 participants.Like every year, DGZI was invited to the International
Affiliates Committee on Saturday afternoon, an eventalso attended by delegations from Canada, Japan,England and Italy. The current President Iacono askedall participants to contribute ideas concerning futurecooperation amongst affiliates.
The participants agreed on the fact that, in thesetimes of globalization, no single country should be se-cluded from the global community. However, the sit-uation in other countries may nonetheless be ex-tremely different. One point for example is the lan-guage barrier of the Japanese colleagues. The socalled Annual Business Meeting took place after themeeting of the international affiliates. The new Pres-ident Dr. Peter Moy delivered his inaugural speech,and he thanked all speakers and representatives of af-filiated associations, especially those who came fromfar away, for their attendance.
“The 2010 meeting served as a celebration ofeverything we have learned in the past 25 years, andhow that knowledge can be applied for the benefit ofour patients today,” Annual Meeting Committee ChairDr Stuart Froum, New York, N.Y., explained.
The next AO congresses will be held in Washington,DC from March 3–5, 2011, in Phoenix, Arizona fromMarch 1–3, 2012, in Tampa, Florida from March 7–9,2013, and in Seattle, Washington from March 6–8,2014. All colleagues interested in attending one ofthose meetings together with us, should contact theDGZI office in Düsseldorf for further details._
DGZI Office DüsseldorfFeldstraße 8040479 Düsseldorf, GermanyTel.: +49 211 16970-77Fax: +49 211 16970-66E-mail: [email protected]
_contact implants
implants2_2010
_March traditionally blesses Egypt with superbweather - warm days and soft evenings, which allowEgyptian hospitality to be showcased perfectly. Cer-tainly the weather conditions were just one of the rea-sons to join the second international dental congressand 6th Arab-German Implantology Meeting held inCairo on 24–26 March 2010.
On behalf of the Faculty of Oral and Dental Medi-cine of Cairo University, Professor Nour Habib, Deanof the Faculty, addressed a warm welcome to all theparticipants of the second international dental con-gress held in Cairo on 24–26 March, 2010.
In the opening ceremony of the Congress he high-lighted the Conference’s aims to promote profes-sional development among dentists by acting as ameans for communication and by encouraging dis-
cussion and research in all areas of dental practice.“We seek also to promote the dental profession in thecommunity at large and to develop a spirit of cooper-ation with other organizations and groups with com-mon interests and concerns,” Professor Nour Habibexplained.
The Congress also hosted the 6th Arab-GermanImplantology Meeting, moderated by well known sci-entific presenters from the Board of the German As-sociation of Dental Implantology (DGZI) who workedas a team of distinguished professionals to resolve atricky dental scenario.
The venue chosen to host the congress was CairoInterContinental City Stars Hotel, where a huge floor-space accommodated the innovative associated Den-tal Trade Industry display. There was ample space for
6th Arab-German Implantology Meetingof DGZIAuthor_xxx

implants2_2010
the profession to experience the new technologiesand materials that were showcased at the event. TheConference was complemented by an exhibitionwhich provided the participants with the valuable op-portunity to engage with vendors and explore the di-versity of dental products and services available tosupport them in their work. Dr Mazen Tamimi , Inter-national Representative of DGZI, Scientific chairmanand Dr. Rolf Vollmer, 1st Vice President of DGZI andCongress Chairman welcomed more than 30 partici-pants from Egypt and Middle East. They promised aninteresting one day scientific program with interna-tional key note speakers and colleagues presentingtheir master thesis as well. “Excellent education is oneof the main focuses of DGZI and is something we con-centrate on for the sake of our patients. In this way, wecan ensure that our professionals benefit from thebest education possible without having to turn tofee-charging companies,” was the statement of Dr Tamimi.
_Scientific Program on Friday 26th ofMarch 2010
AbstractsKey note Speakers
Dr Roland Hille, GermanyThe way to the estheticalsuccess
Implantology in the aes-thetic zone is one of thebiggest challenges in den-tistry. An exact analysis ofthe clinical situation beforewe start with our treatment
gives us confidence in our treatment plan. We mustknow the problems as well as the outcome before westart with our surgery and we also must have a clearconception of the final aesthetic prosthetic situation.The patient contemplates only the crown, not the im-plant in the bone. The patient’s desire is to get a per-fect aesthetic restoration which lasts for a long time.In particular, we need soft tissue support to achieve aperfect aesthetic result. This lecture provides infor-mation about important points to achieve success inthe aesthetic zone, and also shows mistakes oneshould avoid.
Dr Suheil Boutros, USA New Concept in Preparing the Lateral Window in Sinus Lift Surgery
The lateral window sinus lift is a well-documentedtreatment modality used to augment the posteriormaxilla when the remaining alveolar bone is 5 mm orless in height. Several methods of preparing the win-
dow have been proposed anddocumented, including theuse of diamond and end-cut-ting burs and more recentlythe use of piezo surgery. Eachof these techniques has itslimitations; for example, theuse of cutting burs presentshigher incidences of theSchneideri membrane perfo-
ration, where as high as 40% has been documented.More recently the use of piezo surgery has been pre-sented as an effective and safe means in lateral win-dow preparation. The only limitation found with thissurgery is that if the lateral wall is thick, it may becomea time-consuming and less effective technique. Thenew innovation utilizes a large size side cutting bur,which is 5-7mm in diameter, making it very safe, pre-dictable and a fast way to prepare the window.
Dr Mazen Tamimi, Jordan Block Grafts as an option oftreatment of severely atro-phied mandible and maxilla
Several options for treat-ing a severely atrophiedmandible with less than 8 mm of bone remainingabove the inferior alveolar
nerve will be discussed. These include:
_Bone block grafts of autogeneous origin or allograft_Distraction Osteogenesis _Nerve trans-positioning; exact technique & videos _How to perform these advanced surgery solutions _Short implants as an alternative.
There will be a discussion regarding how to choosea suitable treatment option, and how to perform thattechnique.
Dr Robert Laux, Germany Telescopic Attachments,New Modern Concept ofAbutments and Transfers
Telescope or conicalcrowns have been recognizedas successful connection ele-ments for natural abutmentsfor several decades now. They
also offer excellent hygiene. Telescopes require per-fect parallelism or a well-defined slight conicity of theprimary copings. This can only be achieved with cus-tom components or customized prefabricated com-ponents. Conical crowns with a cone angle of 4° allowfor axial divergence between adjacent implants of up
Dr Roland Hille
Dr Suheil Boutros
Dr Mazen Tamimi
Dr Robert Laux

implants2_2010
to 8°. However, given the anatomical shape of thejaws, especially the maxilla, it is almost impossible toplace anterior implants so that they do not exceed thisaxial divergence. The problem of angle compensationhas to be resolved in the simplest possible manner.Any manipulation at the laboratory constitutes acompromise that defeats the purpose of working withprefabricated components. The Kobold, the Titan andthe complete abutment are systems which lead toeasier success in fixed and removable implant-pros-thetics.
Dr Rolf Vollmer, Germany The posterior atrophiedmaxilla. Patient-centeredchoice of treatment
Sinus lifting techniqueshave been known about formore than 20 years and areaccepted as standard tech-niques, ie beyond the experi-
mental stage. This lecture describes the developmentof sinus lift from its origins and explains the indirectand direct methods as well as giving hints for their dif-ferent indications. However, alternatives to these si-nus lift procedures should also be considered, and wewill therefore discuss minimally invasive procedureswhich may be possible in the future.
Prof Dr Dr Ralf Gutwald,GermanyBioengineering in Implan-tology
For reconstruction priorto dental implantation thegold standard is still autolo-geous bone. Disadvantagesare the limited availability of
bone and the necessity of an additional surgical pro-cedure which always implies the risk of donor sitemorbidity. External Tissue Engineering procedures forhard tissue augmentations of the maxilla offer ad-vantages compared with conventional grafts, asthere is minimal or no donor site morbidity. Addi-tionally, Internal Tissue Engineering with bone-in-ducing factors like BMP-2 look promising for use inbone augmentation procedures.
Current research aims at investigating the influ-ence of stem cells on biomaterials. In animal experi-ments stem cell application (a chair side procedure) incombination with a biomaterial (BioOss) show lamel-lar bone formation. The volume preservation was bet-ter in the test side than in the control side where can-cellous bone was applied only. The new bone forma-tion was comparable.
In a clinical multi centre study 45 sinuses wereaugmented with BioOss and stem cells (test) and 25sinuses were treated with a mixture of BioOss and au-tologeous bone (control). Biopsies were obtainedwhen implants were inserted after three months.There were also no differences in new bone formation.
Master Student presentations
Dr Iyad Ghoneim, MScKrems University, Syria Immediate implantation atthe time of extraction—Clinical study with litera-ture review
Missing teeth is a very oldproblem which has plaguedhumankind for many years.
Various solutions have been attempted, ranging fromre-implanting the teeth extracted, to making artificialprosthesis in the shape of the missing teeth, to im-plantation of a biologically accepted material like ti-tanium, which is the material of choice today. A vastnumber of studies have taken place to assess the rateof success of Titanium implants and much develop-ment has taken place by researchers to develop theseimplants and to improve their mechanical and tech-nical characteristics. At the same time, a variety ofnew surgical techniques have been developed in or-der to provide a larger range of treatments options.
Dr Hussam Bakki, MScKrems University, KuwaitThe Presence of Under-wood’s Septa in the Maxil-lary Sinus Among The Po-pulation of Kuwait
This thesis is intended toexamine the frequency ofUnderwood’s Septa amongst
the population of Kuwait, and consider how to dealwith it while implementing sinus lift surgery by properplanning considering the septa’s morphology and lo-cation, based on a reliable CT scan imaging. For thispurpose radiographs from 8 patients who underwentsinus lift operation were re-evaluated in our special-ist dental centre.
Materials & MethodsIn this study, a relatively small sample population
of 8 patients was considered (2 males and 6 females),with an average age of 35 years, ranging between 26and 44 years. Nine sinuses were operated on (sinuslift). All patients were candidates for dental implant-supported restorations placement - they were in good
Dr Rolf Vollmer
Prof Dr Dr Ralf Gutwald
Dr Iyad Ghoneim (l.)
Dr Hussam Bakki (l.)

implants2_2010
health, all of them were partially edentulous (patientsfor whom we planned to extract teeth during surgerywere considered as partially edentulous in this study)and all surgeries were performed by the same sur-geon.
ResultsIt appears that antral septa are more commonly
found in edentulous atrophic maxillae than in dentateones, in the posterior portion of the maxillae than inthe anterior portion and in the left side rather than theright side of the maxillae. A CT scan is the radiographicmethod of first choice for detecting the presence ofsepta, while panoramic radiography was found to beless sensitive and sometimes misleading in detectingsinus septa. Precise knowledge of patient’s maxillarysinus anatomy allows for exact planning of surgeryand helps to avoid unexpected complications.
Dr Ahmed Fadl, MScKrems University, SudanEvaluation of laser appli-cation to uncover dentalImplant in the second stagesurgery
Lasers have been used inoral surgeries for many yearswith great success. In this re-
search (in which a diode laser 980 nm was used), 10patients participated, each of whom had been treatedwith dental implants more than three months ago,with a conventional first surgical stage.
All the implants were uncovered successfully withlaser aid. For each implant the procedure was com-pleted in less than 10 minutes. All patients reportedvery minimal postoperative discomfort or very slightpain at the one-week recall appointment. A fixturelevel impression was taken at that recall appointment.
According to the results of this research, soft tis-sue laser should be considered as an effective alter-native technique for implant uncovering in the sec-ond surgical stage.
Dr Hisham Abueljebain,MScKrems University, KuwaitStem Cell Derived Bone
Implant therapy has be-come the standard of care foredentulous areas of the oralcavity. Following tooth ex-traction, there is often an in-
adequate amount of bone in which to place dental im-plants. In such cases, a ridge augmentation procedure
is performed prior to implant placement. Ridge aug-mentation techniques to correct these defects in-clude guided bone regeneration (GBR) utilizing a bar-rier membrane, bone graft alone or bone graft with amembrane.
In elderly patients bone grafting may cause an-other injury in the donor site which may take days oreven months to heal. This is often unacceptable tomany patients. We propose here a new techniquewhich is less traumatic and hence more acceptable tothe patients.
Bone marrow contains osteoblast progenitor cellswhich appear to arise from a population of pluripo-tential connective-tissue stem cells, which can be ob-tained with aspiration. When cultured in vitro underconditions that promote an osteoblastic phenotype,osteoblast progenitor cells proliferate to formcolonies of cells that express alkaline phosphataseand, subsequently, a mature osteoblastic phenotype.These cells will produce new bone at the ridge whichmay give an implantologist adequate bone width atthe ridge where an implant should be inserted.
Dr Subea Hijazi MScKrems University, Syria Atrophied posterior man-dible. Where to start?
Implant treatment is be-coming the first choice to re-place missing teeth or fillfree spaces in the jaws.Nowadays, the bone resorp-
tion or bone defects can appear in horizontal or ver-tical direction or both. Bone reconstruction shouldrestore bone volume in both directions. The type ofhandling this defect will allow the maintenance ofimplant and the primary stability, a favourable oc-clusal axis and an environment around implant thatwill facilitate prosthetic reconstruction and hygieneaccess to the implanted area.
Therefore, the posterior mandible region is al-ways a challenge for doctors because of the anterioralveolar nerve, especially if there is advanced boneresorption in the area. Over the last decade many ar-ticles have been written detailing the scientific dis-cussion of this problem and the search for possiblesolutions; we can divide them into:
1. Alternatives to implant treatment (no implant)2. Bone augmentation techniques 3. Alveolar distraction4. Nerve transposition or lateralization 5. Short implant 6. Subperiosteal implant
Dr Ahmed Fadl (l.)
Dr Hisham Abueljebain
Dr Subea Hijazi (r.)

implants2_2010
Dr Salah Daffalah, MScKrems University, Sudan New Implant Abutment
The goal of modern den-tistry is to restore the patientto normal health by restoringthe contour, function and es-thetics. As a result of contin-ued research and improve-
ment in diagnostic tools and treatment techniques,predictable success is now a reality for the rehabilita-tion of many challenging clinical situations. In recentyears, dentistry has become greatly influenced byaesthetic considerations. The primary reason for thisis patients’ demands for natural appearing restora-tions. This has resulted in a massive development inthe field of dental implantology over the past 30years. A new implant abutment made of fiberglasswas introduced recently. This new implant abutmentoption is cost- and time-effective and it meets thepatients’ expectations in relation to function and es-thetics as the implant closely resembles the naturaltooth color. This presentation aims at evaluating theeffectiveness of fiberglass dental implants in relationto function and esthetics.
Dr Nicholas Papadopoulos,MScKrems University, CyprusThe two stage mandibularridge split, an alternativebone expansion technique
IntroductionCases of narrow mandi -
bular ridges (less than 5 mmin mandible) require horizontal augmentation for theplacement of screw-type dental implants. A twostage mandubular ridge splitting to decrease the riskof malfracture during osteotomy and minimize thepossibility of loosing crestal bone is presented.
MethodAfter corticotomy of a rectangular buccal seg-
ment with thin separating disc and a three week heal-ing period, the mandibular ridge was expanded and insome advanced cases split buccally, leaving the buc-cal periosteum attached to the lateralized segment.
ResultsWith buccal segments expanded with no compli-
cations, we can gain on average 2–3 mm of horizon-tal bone width.
DiscussionIn the mandible, greenstick fracture during widen-
ing with osteotomes or expanders has not been con-
trollable to date because of cortical thickness andstrength of the bone; the risk of malfracture in themiddle of the thinnest buccal region is high, with thepossibility of future bone receding being very high.
With this Two Stage Mandibular Ridge Splittechnique the location of the greenstick fracture ispredetermined away from the midfacial crestalarea, and the perfusion of the buccal segment re-mains attached and intact. The buccal cortical seg-ment remains a pediculated graft after ridge split-ting and thus the practical benefit is no bone losscrestally.
Dr Rouven Bönsel, MScKrems University, GermanyPrerequisites for immedi-ate loading of dental im-plants
Modern clinical ap-proaches to loading of dentalimplants promise the pa-tients immediately loaded
implants. Based on this observation, this study will ex-amine whether, considering the processes occurringduring bone healing, immediate functional loading ofdental implants is possible.
This study evaluates the predictability of early andimmediate loading protocols of implants in the upperand lower jaw. In this observational study 450 dentalimplants were loaded early. The implants were in-serted into various regions of the jaw in the maxillaand mandible. The criteria determined was whetherthe osseointegration had been completed after threemonths. The success rate in this observational studyranged from 92 % (upper jaw) to 100 % (lower jaw).The clinical applicability of the treatment concept isvery favourable, due to the shortening of the treat-ment time.
Dr Adel Byadsi, MScKrems University, Palestine Sinus Lift—New Technique
This lecture will show theadvantages of a unique us-age of the Piezo technique infine and precise cutting ofthe bone, without damagingor causing perforation of the
Schneiderian membrane.
This technique enables us to reuse the bone andthus negate the need for additional membrane. Thesuccess rate in such surgery is high and the complica-tions are very low._
Dr Salah Daffalah
Dr Nicholas Papadopoulus
Dr Rouven Bönsel (r.)
Dr Adel Byadsi

I 41
xxx _ xxx I
implants2_2010
_The International Team for Implantology (ITI),a leading academic organization dedicated to the pro-motion of evidence-based education and research inthe field of implant dentistry, welcomed more than4,000 participants from all over the world to the 2010edition of its much anticipated ITI World Symposium.The city of Geneva, Switzerland, provided a pictur-esque backdrop to a full program of topical presenta-tions and debate.
With his keynote address, world-renowned adven-turer and scientist Bertrand Piccard set the tone for thethree-day event that explored new and emerging ter-ritory in implant dentistry. The collective knowledgerepresented by the faculty of 113 experts from 26countries provided a springboard for lively debate anddiscussion that continued beyond the official pro-gram. The scientific program was divided into threemain facets of treatment: New clinical methods for di-agnosis and treatment planning; New and proventreatment procedures; Complications in implant den-tistry or dealing with reality. The smooth delivery andbreadth of information provided over the three daysserved to underline the truth of the ITI's claim of "30 years of leadership and credibility".
For the first time, the main program was comple-mented by a pre-symposium program of two parallelfull-day courses that allowed participants the luxuryof total immersion in two narrowly defined areas oftreatment. The highly popular Limited AttendanceSessions were also expanded from three to four com-pact lectures per session. "The ITI is fortunate that itcan call on such a wide variety of opinion leaders in im-plant dentistry on an international basis to share theirknowledge," said Stephen Chen, Chairman of the Sci-entific Program Committee. "This pool of expertise isthe foundation for the success of the event and rein-
forces its well deserved reputation as the most presti-gious academic event in the implant dentistry calen-dar."
“Every effort was made to ensure the smooth run-ning of the event and give participants the best possi-ble Symposium experience,” commented FriedrichBuck, Executive Director of the ITI. “We also took thedecision to hold an industry exhibition that drew 38 exhibitors from Europe as well as the USA, givingparticipants the opportunity to review some of the lat-est developments in the field and discuss their needsdirectly with manufacturers.”
Rounding off the event was the Research awardwhich attracted a great deal of interest. Competitionfor the nine presentation slots was fierce and the totalof 118 posters testified to the central role played by re-search among the ITI membership as well as theirreadiness to share results.
The success of the ITI World Symposium is undis-puted, it can be measured not only in terms of atten-dance figures, but also the accessibility of the eventwhich provided simultaneous translation in 12 lan-guages for the main program. The next ITI World Sym-posium will take place in 2014._
ITI World Symposium 2010

42 I
I meetings _ Friadent World Symposium
implants2_2010
_It was a congress of superlatives. 2,500 partic-ipants from more than 60 countries met in Barcelonaon March 19–20, 2010. More than 100 internationallyknown lecturers presented the latest scientific in-sights to an attentive audience and described howthey could be successfully integrated into practice.Professor Lim Kwong Cheung of Hong Kong, Dr HenrySalama from the USA and Professor Heiner Weberfrom Germany were the scientific chairmen of thecongress.
„We offer not only implants but also dental solu-tions from root to crown.“ With these words Dr Werner Groll, managing director of DENTSPLY Friadent, defined the slogan of the congress: „Focuson your Practice Success.“ The company’s partnershipwith users is based on three pillars. The products andprocesses of the DENTSPLY Friadent company for im-plantology and bone augmentation are proven inclinical applications throughout the world. Future-
oriented and innovative technology is aligned to therequirements of the practitioner and the desires ofthe patient. Finally, easy-to-implement marketingconcepts are available for systematic development ofthe dental practice under the stepps brand. DENTSPLY Friadent has based its growth on these three pillars tobecome number three in the world implant market, asdescribed by Dr Groll at the press conference.
The wide and varied range of topics covering all as-pects of modern implant-supported therapy wasclearly structured, allowing attendees to concentrateintensively on topics of interest to them and leave thecongress thoroughly informed. While the lectures inthe “Proven Applications and New Approaches“ fo-rum were primarily practice oriented, the “Today’sProgress for Tomorrow’s Practice“ forum focused onprocedural techniques, study results relevant to den-tal practice and new materials and technologies. Thefocus on interdisciplinary therapy techniques with
Interdisciplinary insightsfrom theory to practice

I 43
meetings _ Friadent World Symposium I
implants2_2010
interfaces to periodontics, endodontics and dentaltechnology played a central role: the congress deliv-ered on the promise of „solutions from root to crown.“
Keynote lectures concentrated on the four successfactors timing, esthetics, treatment protocols and riskmanagement, which are critical for implantology, us-ing practical examples and also with detailed descrip-tions of the essential scientific background.
In the Expert Talk session, which attracted a veryinterested audience on Friday afternoon, Dr DietmarWeng, Dipl.-Ing. Holger Zipprich, Dr Marco Degidi,Professor Tord M. Lundgren, Professor Karl-AndreasSchlegel and Professor Dennis Tarnow discussed theTissueCare Concept and the significance of primarystability. The various discussions concluded that im-portant trends—including immediate loading or es-thetic long-term success rate—should be consideredin more detail with reference to scientific proofs and
there should be a more detailed examination of thecurrent insights.
The final sessions presented by Dr Henry Salamaand Dr Bernhard Saneke described the team approachas a success factor. Interdisciplinary networks and anopen working atmosphere are the foundation stonesof the dental practice of the future. Relaxation was onthe program for Friday evening. Attendees celebratedwith an exciting range of culinary specialties andrhythms on the grounds of the 1929 World Expositionat the Magic Fountain at the foot of Montjuic.
The DENTSPLY Friadent World Symposium hasnow become one of the most important implantol-ogy congresses in the world and still retains a familyatmosphere in spite of its size. Many attendees havealready indicated that they will be attending the nextWorld Symposium on March 16–17, 2012, in Ham-burg._

implants2_2010
Manufacturer news
Materialise DENTAL
New General Managerfor Germany, Austriaand Switzerland
Materialise Dental announced to-day the appointment of DrBerthold Reusch as General Man-ager for Germany, Austria andSwitzerland. Dr Reusch bringsover 17 years of global marketing,sales, clinical and business man-agement experience in the field ofdental materials and digital den-tistry. Most recently, Bertholdworked for the dental division of3M ESPE where he was Director ofOperations for the digital imagingdevice business which he suc-cessfully developed outside the US. From 2007 to2009 Berthold was a member of the executive man-
agement team of Brontes Technologies, a 3M com-pany based in Boston, MA, building the digital im-pressioning business in the US. As General Man-ager at Materialise Dental GmbH, Berthold and histeam will further develop the SimPlant® andSurgiGuide® business within the German, Austrian
and German-speaking Swissmarkets. SimPlant® dental im-plant treatment planning soft-ware allows clinicians to planthe ideal location of implantswhile taking into account vitalanatomical structures and clini-cal and esthetical considera-tions. SurgiGuide®, for which thecompany has partnered up withvarious implant companies andwhich offers solutions for everyimplant case, subsequently pro-vides the link between implant
planning and actual surgery. With SimPlant® andSurgiGuide®, dental professionals have a flexible
treatment planning system at their fingertips toguarantee predictable and safe implant treatmentregardless of the clinical situation. Dr BertholdRausch received his diploma and PhD (Dr rer. nat.)in Physics from the University of Tübingen, Germanyand then went on to receive his MBA, with an em-phasis in marketing and international businessmanagement, from the Business School at theCatholic University of Eichstätt. When asked abouthis new position, Dr Reusch said, “I’m very enthusi-astic to join Materialise Dental, an innovative andtechnologically driven organization. I’m looking for-ward to undertaking the challenging task of headingmy division and—together with my team—offeringour customers the most innovative and advancedproducts to meet their computer-guided implantdentistry needs.”
Materialise DENTAL GmbH
Argelsrieder Feld 10
82234 Oberpfaffenhofen, Germany
Web: www.materialisedental.com
ULTRADENT
Premium Units—made in Germany
With the U 1500, U 5000S and U 5000F treatment units, dental manufacturerULTRADENT from Munich has created an entirely new class of unit that also of-fers exclusive premium standards in the compact treatment unit segment. Thespecial modular ULTRADENT structure makes it possible to equip units in linewith dentists’ individual requirements and specifications. It also sets extremelyhigh standards in terms of design and quality ofworkmanship. The dental equipment for these treatment units hasalso been redesigned, with a view to meeting allpossible requirements in terms of positioning, pro-gramming and information, while also supportingtreatment using numerous exclusive instrumentsand all possible options. The central unit can beused to control everything – from the tartar removerand new micro motors with torque control and anextended speed range to the intraoral camera, theelectrosurgery unit and an integrated saline pump.The simple, symbol-controlled programming cov-ers all instruments and chair positions. It goes with-out saying that this workstation can also be fitted with the ULTRADENT-VISIONmultimedia system.
Details such as the new touch-screen display, an optional wireless foot controland exchangeable control valves facilitate treatment and promote the provisionof service. Comfort is provided by the supersoft chair upholstery, available in 12colors, plus an individual headrest system with magnetic supports. Movablearmrests make it easier to get into the chair. Exclusive comfort upholstery withair conditioning or massage function is an ULTRADENT innovation. This isachieved by six silent ventilators in the backrest and seat that provide pleasantfresh air, or by special electric motors that provide calming relaxation by meansof a gentle massage. This option is especially advantageous for long treatments,
for the dentist and patient alike.The ULTRADENT Premium class realizes manytechnical visions and its overall design generates adegree of fascination and customer satisfactionthat is only possible in the top-of-the-range seg-ment. So, treat yourself to innovation and perfec-tion, and gain inspiration for your practice.Request the latest ULTRADENT Premium brochureand let us surprise you.
ULTRADENT Dental-Medizinische
Geräte GmbH & Co.KG
Eugen-Sänger-Ring 10
85649 Brunnthal, Germany
E-mail: [email protected]
Web: www.ultradent.de

Implants2_2010
Nobel Biocare
The ideal abutment forposterior restorations
Nobel Biocare is pleased to announce the expansionof the popular Snappy abutment product portfoliowith the addition of taller abutment options. Startingimmediately the Snappy Abutment is available in4.0 and 5.5 mm abutment heights. Thanks to its pro-file and design, the Snappy Abutment permits clini-cal use without any modification. In addition, the in-cluded snap-on impression coping ensures simpli-fied impression-taking. The SnappyAbutment is an easy to use pros-thetic solution that is highly suit-able for posterior restora-tions, especially in partiallyedentulous jaws, and forsingle-crown restorationswith an implant.
Easy to use The Snappy Abutment iseasy to use and ensures op-timal precision. In addition,all the prosthetic compo-
nents and individual elements required for restora-tion, e.g. the abutment, abutment screw, impressioncoping, healing cap and temporary coping, are sup-plied in a single package. Thus, the Snappy Abut-ment provides a cost-effective, time-saving andhighly functional prosthetic solution.
Efficient restoration The Snappy Abutment is seated on the implant andthe screw is engaged to a torque of 35 Ncm with theUnigrip Driver and prosthetic torque wranche. Oncethe Snappy Abutment has been secured, the easy-to-use impression coping is snapped in place, an ar-row on the impression coping should be oriented
buccally. The impression material is theninjected around the coping, and a
pick-up impression is taken.This technique allows
very precise impres-sions of the Snappy
Abutment and the fin-ish line without the need
for retraction cord.The dental laboratorycan then use an off-the-shelf abutmentreplica to prepare the
definitive restoration. In addition, a temporary cop-ing for fabricating a provisional restoration is in-cluded, allowing the patient to leave the clinician’spractice with a functional tooth. The final restorationfor the crown is fabricated by the conventional tech-nique. For this purpose NobelProceraTM supplies afull range of restorations for all indications, estheticand cost effective.
Models and sizes The improved Snappy Abutment package containsall the components required including the final abut-ment, the impression coping used to take the im-pression, and the temporary coping for fabricating aprovisional restoration. The available componentsare designated with the code 4 or 5, depending onthe height of the abutment used: the Snappy Abut-ment 4.0 or the Snappy Abutment 5.5. The SnappyAbutment is available for all Nobel Biocare implantsystems, NobelReplace, Brånemark, NobelActive,and for all platform diameters NP, RP, WP, and 6.0.
Nobel Biocare Holding AG
P.O. Box
8058 Zurich Airport, Switzerland
E-mail: [email protected]
Web: www.nobelbiocare.com
The improved Snappy Abutment package contains allthe components required including the final abutment,the impression coping used to take the impression, andthe temporary coping for fabricating a provisionalrestoration.
®
www.omniaspa.eu
OMNIA S.p.A.Via F. Delnevo, 190 - 43036 Fidenza (PR) ItalyTel. +39 0524 527453 - Fax +39 0524 525230
VAT. IT 01711860344 - R.E.A. PR 173685 Company capital € 200.000,00
Since our beginnings, we have always been focused on quality and innovation
toward the battle againstcross - contamination and infections.
In the last 20 years, we have ensured safety and protection to you and your patients, with advanced and reliable products. Tools
that represent the ideal solution for who is operating in dentistry, implantology/oral surgery and general surgery.
With Omnia sure to be safe.
AD
Geistlich Pharma AG
The right cap for the job
The unique Biofunctional properties of GeistlichBio-Oss® have been proven through 24 years of ex-cellent practical experience worldwide. GeistlichBio-Oss® is characterised by volume stabilitythroughout the extensive indication areas of peri-odontology, implantology and cranio-maxillofacialsurgery.Geistlich Bio-Oss® is now available with an opti-mised handling in vials: NEW CAP “EASY+SAFE”.
• SAFE - no sharp edges• EASY - to open
Your opinion is important to us. Answer three ques-tions at http://www.geistlich.com/index.cfm?dom=2&rub=20&id=105702
By participating in this survey, you will be enteredinto a draw to win an unforgettable weekend of re-generation at the Victoria-Jungfrau in Interlaken,(Switzerland) which is a member of the Leading Ho-tels of the World.
Deadline for entry is September 30, 2010. Legal re-course is excluded.
Geistlich Pharma AG
Bahnhofstrasse 40
6110 Wolhusen, Switzerland
Web: www.geistlich-pharma.ch
The new vial cap of Geistlich Bio-Oss® — safe and easy to open.

implants2_2010
W&H
SOS Children’s Villages visit W&H
As the world’s first manufacturer of dental trans-mission instruments and devices, W&H has longbeen known for its high-quality products and socialawareness. In its official anniversary year, from 6April 2010 to 31 March 2011, W&H will be even moreactive in the social realm by offering support to SOSChildren’s Villages. At the launch of the anniversaryyear, W&H welcomed a children’s group from SOSChildren’s Village Seekirchen on 8 April 2010. Withthe motto “I’m not scared of the dentist”, the chil-dren had the opportunity to examine up-close theproduction of traditionally feared dental instru-ments and also to test them out. During its anniversary year, W&H Dentalwerk Bür-moos will mainly be supporting the Family Strength-
ening Programme in Kakiri, Uganda, initiated bySOS. Thanks to this support, the financing of the en-tire programme will be secure for more than twoyears. The Family Strengthening Programme inKakiri was established in 2006 by SOS Children’sVillages, in order to provide support for children andfamilies who need help as a result of poverty or ill-ness. The goal is to improve their health and their so-
cial situation. This is not a normal SOS children’s vil-lage, but rather a programme for an entire region. Atpresent, the programme assists around 480 chil-dren from 130 families. Its activities include: med-ical assistance for families, securing basic food forfamilies, and educational programmes for childrenof school age. In addition to the Family Strengthen-ing Programme in Kakiri, Uganda, which is sup-ported by W&H Dentalwerk Bürmoos, other SOSChildren’s Villages campaigns are being carried outby W&H subsidiaries and area managers. Celebrate120 years of W&H and help us support SOS Chil-dren’s Villages — staying true to the W&H companyphilosophy: People have Priority.
W&H Deutschland GmbH
Raiffeisenstraße 4
83410 Laufen, Germany
E-mail: [email protected]
Web: www.wh.com
Degradable Solutions
Moldable, in situ hardening bonegraft substitutes
easy-graft® and easy-graft® CRYSTAL are moldable,fully synthetic bone defect fillers for indications in oralsurgery, implantology and periodontology. In contactwith blood, the materials harden within minutes into aporous, inherently stable body. A membrane to containthe materials is not necessary in most cases. The easy-graft® products are frequently used for ridge preserva-tion after tooth extraction. The socket must be free of in-fected and inflamed tissue prior to graft insertion. Thematerials are applied directly from the syringe into the defect where they hardenand seal the extraction wound. For most cases, a membrane or suturing of soft
tissue are unnecessary. easy-graft® and easy-graft® CRYSTAL are designed tohave different resorption characteristics. easy-graft® is composed of phase-pure �-tricalcium phosphate (�-TCP). It degrades completely and is replacedby bone. easy-graft® CRYSTAL contains 40% �-TCP and 60% hydroxyapatite
(HA). It is degraded only partially and remains integrated inthe newly formed bone for long-term volume preservation.In summary, the easy-graft® products combine establishedbiomaterials for bone regeneration with a unique handlingadvantage—moldable from the syringe, hardening in thedefect.
Degradable Solutions AG
Wagistrasse 23
8952 Schlieren, Switzerland
E-mail: [email protected]
Web: www.degradable.ch
Straumann
15th André SchroederResearch Prize goesto Maria Retzepi
One of the most prestigious awards in dentistry, theAndré Schroeder Research Prize, was presented atthe World Symposium of the International Team forImplantology (ITI) in Geneva. Beat Spalinger, Presi-dent and CEO of Straumann, presented the award toDr Maria Retzepi, a specialist periodontist and clin-ical lecturer at the University College London East-man Dental Institute. Dr Retzepi is commended forher work on ‘The Effect of Experimental Diabetes onGuided Bone Regeneration’. It shows that—al-though diabetes compromises the initial stages ofbone healing—guided bone regeneration can pro-
vide an environment that is conducive for signifi-cant, even though delayed, formation of new bone.The use of insulin to control diabetes may enhance
the bone regeneration potential. Understanding thegenetic aspects of the metabolic status may lead tonew approaches for treating oral bone defects in di-abetic patients. The coveted André Schroeder Re-search Prize was first presented in 1992 to promotenew scientific findings in oral implantology and re-lated fields. It is given in honor of the late ProfessorAndré Schroeder (1918–2004), who pioneereddental implantology. The André Schroeder Prize furthers illustratesStraumann’s commitment in the field of researchand development.
Institut Straumann AG
Peter Merian-Weg 12
4052 Basel, Switzerland
E-mail: [email protected]
Web: www.straumann.com

Implants2_2010
EMS
Piezon Master Sur-gery with three newinstrument systems
Since it was introduced, Piezon Master Surgery—based on Piezon technology—has had a remark-able track record in many practices. Today, EMS hasexpanded the clinical scope of application of thePiezon Master Surgery product range. With an en-hanced product offering—and special instrumentssuch as Sinus System and Implant System—prac-titioners have access to technologies allowing themto work even more efficiently. With Piezon MasterSurgery, application-specific instruments are nowavailable: a total of four perio instruments especiallydesigned for resective and regenerative periodontalsurgery, five advanced surgical instruments forgentle and uniform sinus lifts, as well as six specialfully diamond-coated instruments for implant appli-
cations with dual cooling sys-tem and extra-efficient debrisevacuation. Implant instru-ments provide for safe and ef-ficient work with greater preci-sion, says EMS. These instru-ments are seen as particularlysuitable for four clinical applica-tions: implant site preparationfollowing extraction, implant sitepreparation followingsplitting of the alve-olar ridge, implantsite preparationin the posteriortooth area, andimplant sitepreparation in compro-mised areas, such as a narrowalveolar ridge. In principle, in-struments can be used at low
OP temperature of no more than 33 degrees centi-grade. They provide drilling efficiency and precisionin the maxillary area. The entire Piezon Master Sur-gery method is based on piezoceramic ultrasoundwaves producing high-frequency, rectilinear back-and forth oscillations. These vibrations raise thelevel of precision and safety in surgical applica-
tions, notes EMS.
Ultrasound instruments are used selectively tocut hard tissue only. The device delivers re-liable results in periodontal and oral surgeryas well as implantology due in part to a user-friendly ergonomic touch board, says EMS.
EMS Electro Medical Systems
S.A.
Ch. de la Vuarpillière 31
1260 Nyon, Switzerland
E-mail: [email protected]
Web: www.ems-dent.com
Camlog
3rd InternationalCAMLOG Congress, June 10th
through 12th, 2010
Apparently, interest in and expectations for the 3rd InternationalCAMLOG Congress 2010 in Stuttgart are enormously high—analo-gous to the above-average standards that CAMLOG has created andset for itself in the variety and quality of the congress program andthe qualification of top speakers. This again clearly illustrates thecompany's goals: to offer scientifically based, up-to-date continuingeducation, to set new benchmarks in the industry, and to continu-ously increase user benefits. The renowned names of the scientific congress committee speak forthemselves and vouch for quality: Prof Dr Jürgen Becker, Dr SvenMarcus Beschnidt, Prof Dr Dr Rolf Ewers, Prof Dr Dr Dr Robert Sader, PD Dr FrankSchwarz, Prof Dr Dr Wilfried Wagner. Although the majority of the speakers arefrom Germany, internationalization is playing an increasingly prominent role forthe CAMLOG Group. Proof is in the growing number of internationally renownedcongress speakers.CAMLOG is experiencing a significant increase in the number of participants atthe 3rd International Congress in Stuttgart and some workshops are alreadyfully booked.
All information about the Congress and registration options are available atwww.camlogcon gress.com.
CAMLOG Foundation
Margarethenstrasse 38
4053 Basel, Switzerland
E-mail: [email protected]
Web: www.camlogfoundation.org
AD

implants1_2010
Congratulations and Happy Birthday to all DGZI-members around the world
70th BirthdayDr Hans-Jürgen Friemert (10.04.)Dr Hartmut Steinkrüger (26.04.)Dr Jürgen Huhmann (27.04.)
65th BirthdayDr Osman Sahovic (07.04.)Dr Elizabeth Siswanto-Hartmann (08.04.)
60th BirthdayDr Johannes Schüssler (21.04.)
55th BirthdayDr Rüdiger Hobohm (14.04.)Dr Bernd Thomaschewski (16.04.)Josef Pechl (21.04.)ZTM Ulrich Gonsberg (25.04.)Dr Veselko Jovanovic (29.04.)Dr Thomas Gross (30.04.)
50th BirthdayInes Ayoub (05.04.)Dr Helmuth Althoff (06.04.)Dr Dr Stephan Wolf (08.04.)ZTM Claus Fiderer (13.04.)
ZA Rolf Hoppenrath (16.04.)Dr Rene Kleinlugtenbelt (17.04.)Dr Kamal Tizieni (18.04.)Günter Somberg (23.04.)Drs Marcel A. Kruitbosch (26.04.)Dr Masud Sayed (28.04.)
45th BirthdayDr Robert Suetter (02.04.)Dr Jan van den Daele (02.04.)Dr Stefan Eckardt (05.04.)Dr Bernd Ronneburg (06.04.)Dr Susanne Martin (17.04.)
Dr Stephan Arnold (20.04.)Dr Mario Heupel (26.04.)Dr Knut Langer (28.04.)
40th BirthdayDr Jan Kielhorn (03.04.)Dr Sven Schultze (13.04.)Dr Marc Hausamen (17.04.)ZA Anka Fritzsch (19.04.)Dr Ammar Hamdah (19.04.)Dr Timo Weihing (21.04.)Dr Jörg Umfermann, MSc, (24.04.)
75th BirthdayDr Hany Moharm (25.05.)
70th BirthdayDr Goizot Indra (05.05.)
65th BirthdayDr Johannes Wolf (16.05.)
60th BirthdayDr Dr. Hans-Joachim Schütz (01.05.)Dr Harald Rahmann (07.05.)Gustav Stecher (11.05.)Dr Hermann Klumpen (12.05.)
Dr Nenad Bogdanovic (13.05.)Dr Herbert Sirch (19.05.)Dr Volkmar Karnstedt (25.05.)Dr Klaus Engstler (27.05.)Dr Gerhard Treuel (28.05.)
55th BirthdayDr Klaus-Peter Ullmann (07.05.)Dr Robert Kempter (09.05.)Dr Barbara Melchior (09.05.)
50th BirthdayDr Martin Angermeier (01.05.)Dr Bert Eger (02.05.)
Christian Lelonek (08.05.)Dr Hansjörg Schmidt (09.05.)Dr Rolf Olbertz (12.05.)Armin Göring (25.05.)Dr Michael Stumpf (25.05.)Wolfgang Balmes (28.05.)Dr Matthias Wolf (30.05.)
45th BirthdayDr Hans-Joachim Nickenig (03.05.)ZÄ Catrin Westermann-Lammers (10.05.)ZA Mattgias Erich Mergner (12.05.)Dr Khaldoun Khourdaji (17.05.)
Dr Sigmar Schnutenhaus (19.05.)Dr Christian Jänichen (20.05.)Dr Monika Sausen-Bootsch (23.05.)Dr Frank Scott (25.05.)Dr Thomas Ducke (28.05.)
40th BirthdayZA Stavros Avgerinos (01.05.)Emanuel Adrian Brauti (15.05.)Nicolaos Tsacmacidis (24.05.)Dr Matthias Baierl (25.05.)
APRIL 2010
65th BirthdayDr Franz Konczwald (03.06.)Dr Jan Erik Rosenbaum (10.06.)Ortwin Hüsken (22.06.)
60th BirthdayDr Dr. Peter Barth (12.06.)Dr Enver Yazicioglu (22.06.)
55th BirthdayZA Andreas Wiegand (11.06.)Dr Elvira Perder-Seipold (13.06.)Dr Alexander Györffy (19.06.)
Dr Abdul Rahman AlTayeh (21.06.)Dr Arisaka Ryuichi (25.06.)Dr Robert Böttcher (28.06.)
50th BirthdayZA Frank Dehnert (06.06.)ZA Haris Apostolidis (08.06.)ZA Michael Röhner (08.06.)Dr Arleta Stefaniak-Brzuchalski (10.06.)Dr Fritz Bergmann (11.06.)Dr Mohammad Jamal Mourtada (11.06.)Dr Johan de Jonge (19.06.)ZA Bernfried Hauf (19.06.)
Dr Jamil Al Sabuba (21.06.)Dr Reiner Tegeler (24.06.)Dr Kirsten von Helldorff (29.06.)
45th BirthdayDr Mohammad Al Harkan (01.06.)Dr Hermann Steffens (02.06.)ZA Jens Tartsch (02.06.)Dr Thomas Maier (03.06.)Dr Norbert Wellens (04.06.)Dr Jan von der Brelie (05.06.)Dr Frank-Lothar Kirchberg (09.06.)Dr Mahmoud Al Hariri (10.06.)
Kachoum Farouk (12.06.)Ahmad Kalach (12.06.)Dr Claus Schüttler-Janikulla (14.06.)Dr Tamrouk Khaled (16.06.)ZA Adolf Thürmann (18.06.)Dr Gregor Dohmen (28.06.)Dr Jan Scheuer (29.06.)
40th BirthdayDr Michel Dibb (01.06.)ZA Navid Zomorrodi (20.06.)ZA Gernbot Bartl (25.06.)Mhd Firas Kharboutly (26.06.)
JUNE 2010
MAY 2010

KONGRESHVARME UNARODNI STOMATOLOŠKI KONGRES
Lecturers:
DT Lecturers:
Dr. David L.Hoexter - USAProf.Dr. Bilal Al-Nawas - GERDr. Istvan Urban - HUNDr. Suheil Michael Boutros - USADr. Francesco Mintrone - ITADr. Darko Slovsa - CROProf. Dr. Claus Udo Fritzemeier - GERDr. Mazen Tamimi - JORDr. Nadim Abou Jaoude - LBNProf.Dr. Nabil Jean Barakat - LBNMUDr. Jiri Holahovski - CZEDr. Rainer Valentin - GERDr. Rolf Vollmer - GERDr. Ulf Krueger Janson - GERDr. Wolfgang Richter - AUTDr. Luca Lorenzo Dalloca
Dr. Stefano Ardu - CHEDr. Dusko Gedosev - GERDr. Gregory Brambilla - ITAProf. Dr. Ivica Anic - CROProf. Dr. Ivana Miletic - CRO
Dr. Mark P. Collona - USADr. Zelimir Bozic - CRODr. Douglas Ness - USADr. Oscar Von Stetten - GERProf. Dr. Davor Katanec - CRO
Dr. Thomas Schindler – AUTDr.Vanja Coric - CRODr. Fay Goldstep - CANDr. Ross W. Nash - USADr. Elliot Mechanic - CANDr. George Freedman - CANProf. Dr. Edward Lynch - GBRDr. Orsolya Rigo - HUN
MDT. Harald Hoer - AUTMDT. Roberto Iafrate - ITCDT. Przemek Seweryniak - SWEDT. Jorn Trocha - GERMDT. Jerko Marsic - CRODT. Senad Bajramagic - CRODT. Leon Cebovski - CROProf. Dr. Hrvoje Juric - CRO
Prof. Dr. Bozidar Pavelic - CRODr. Zeljka Cabunac - SRB
2010CONGRESSHVAR
INTERNATIONALDENTALCONGRESSCROATIA10.06.2010. - 12.06.2010.
www.hvarkongres.hr
Dear Colleagues,
we take great pleasure in inviting you to participate in the 1st Hvar InternationalDental Congress.
From 10. to 12. of June 2010., HSK - Croatian Dental Chamber in cooperation withOral Dent company, supported by three international associations DGZI - DeutscheGesellschaft für Zahnärztliche Implantologie e.V., IADFE - International Academy forDental Facial Esthetics and ESCD - European Society of Cosmetic Dentistry organizes an extraordinary assembly of experts from all over the world on the island ofHvar, Croatia.
More than 40 lecturers from Europe, the United States of America and Middle East willgive lectures on the island of Hvar. We organize programs for dentists, dental tech-nictians, world Ozon Symposium,Laser Symposium, many workshops and biginternational exhibition. Along with the educational program, we organize luxuriousentertaining social programs with numerous surprises during all three congress days.
The whole event will be held in Grand Hotel Amfora, in the town of Hvar, in the periodof 10. to 12. of June 2010. It is important to mention that the Croatian Dental Chamberrated this Congress with the maximal 12 points, which ranks this Congressamong the best events in Croatia in 2010.
The island of Hvar is the queen of the Croatian Dalmatian islands. It has been famous since the antique because of its important strategic and nautical position, the rich of the various historical periods, the culture and natural monuments and the literature.Thanks to the mild climate, the warm winters and pleasant summers Hvar receives many guests, scientists and travellers, who are attracted by the dense mediterranean nature, rich tradition and arhitecture, and nightlife.
All dental companies which are interested in participation and renting exhibitionbooths on this congress can find all the information on our web sitewww.hvarkongres.hr or can contact us directly via e-mail [email protected] Wewill be happy to provide you with detailed information.
Looking forward to welcoming you on the island of Hvar.
Sincerely Yours,
the Organizing committee
GRAD HVAR
– ITA

50 I
I about the publisher _ imprint
implants2_2010
Copyright Regulations _implants international magazine of oral implantology is published by Oemus Media AG and will appear in 2010 with one issue every quarter. The
magazine and all articles and illustrations therein are protected by copyright. Any utilization without the prior consent of editor and publisher is inad-mi ssible and liable to prosecution. This applies in particular to duplicate copies, translations, microfilms, and storage and processing in electronic systems.
Reproductions, including extracts, may only be made with the permission of the publisher. Given no statement to the contrary, any submissions to theeditorial department are understood to be in agreement with a full or partial publishing of said submission. The editorial department reserves the right tocheck all submitted articles for formal errors and factual authority, and to make amendments if necessary. No responsibility shall be taken for unsolicitedbooks and manuscripts. Articles bearing symbols other than that of the editorial department, or which are distinguished by the name of the author, representthe opinion of the afore-mentioned, and do not have to comply with the views of Oemus Media AG. Responsibility for such articles shall be borne by the author.Responsibility for advertisements and other specially labeled items shall not be borne by the editorial department. Likewise, no responsibility shall be assumedfor information published about associations, companies and commercial markets. All cases of consequential liability arising from inaccurate or faulty representation are excluded. General terms and conditions apply, legal venue is Leipzig, Germany.
PublisherTorsten R. Oemus [email protected]
CEOIngolf Dö[email protected]
Members of the BoardJürgen [email protected]
Lutz V. [email protected]
Chief Editorial ManagerDr Torsten Hartmann (V. i. S. d. P.)[email protected]
Editorial CouncilDr Friedhelm [email protected]
Dr Roland [email protected]
Prof Dr Dr Kurt [email protected]
Dr Torsten [email protected]
Dr Suheil [email protected]
Editorial OfficeKristin [email protected]
Executive ProducerGernot [email protected]
DesignerSarah [email protected]
Customer ServiceMarius [email protected]
Published byOemus Media AGHolbeinstraße 2904229 Leipzig, GermanyTel.: +49 341 48474-0Fax: +49 341 [email protected]
Printed byMessedruck Leipzig GmbHAn der Hebemärchte 604316 Leipzig, Germany
implantsinternational magazine of oral implantologyis published in cooperation with the GermanAssociation of Dental Implantology (DGZI).
DGZI PresidentDr Friedhelm HeinemannDGZI Central Office Feldstraße 80, 40479 Düsseldorf, GermanyTel.: +49 211 16970-77Fax: +49 211 [email protected]
www.dgzi.dewww.oemus.com
implantsinternational magazine of oral implantology

implantsinternational magazine of oral implantology
One issue free of charge!I hereby agree to receive a free trial subscription of implantsinternational magazine of oral implantology (4 issuesper year).
I would like to subscribe to implants for € 44* for Germancustomers, € 46* for customers outside of Germany, unless awritten cancellation is sent within 14 days of the receipt of thetrial subscription. The subscription will be renewed automati-cally every year until a written cancellation is sent to OEMUSMEDIA AG, Holbeinstr. 29, 04229 Leipzig, Germany, six weeksprior to the renewal date.
*Pric
es in
clud
e sh
ippi
ng a
nd V
AT
Last Name, First Name
Company
Street
ZIP/City/County
E-mail Signature
Signature
OEMUS MEDIA AGHolbeinstraße 29, 04229 Leipzig, Germany, Tel.: +49 341 48474-0, Fax: +49 341 48474-290, E-Mail: [email protected]
Reply via Fax +49 341 48474-290 to OEMUS MEDIA AG or per E-mail to [email protected]
Notice of revocation: I am able to revoke the subscription within 14 days after my order by sending a writtencancellation to OEMUS MEDIA AG, Holbeinstr. 29, 04229 Leipzig, Germany.
IM 2
/10
Subscribe now!
ww
w.a
dwor
k.de
BIONIC ENGINEERING DESIGNED IMPLANTS
BEGO Semados® patented Implants embody:
Indication-optimised contour design
Function-optimised implant-abutment-connection
High purity and ultra-homogenous-surface
Polished rim for an infl ammation-free gingiva-attachment
100 % German design – 100 % German manufacturing
Value for money
www.bego-implantology.com
GO FOR GOLD.
BEGO Semados®
Mini-Implant
Bionic Engineering Design transfer of optimal living nature solutions
to technical productsBEGO Semados®
S-ImplantBEGO Semados®
RI-Implant
Official care provider to the German Olympic teams since 2002
Are YouInterested?








![Manual Energia Solar 4a Ed Salvador Escoda[1]](https://static.fdocuments.net/doc/165x107/577ce5491a28abf103904a84/manual-energia-solar-4a-ed-salvador-escoda1.jpg)








