Ipertensione Polmonare nelle malattie ematologiche
24
L’Ipertensione Polmonare nelle Malattie Ematologiche Corso di aggiornamento sull’ipertensione polmonare. Pavia 21 maggio 2011 Giovanni Barosi Laboratorio di Epidemiologia Clinica/Centro per lo Studio della Mielofibrosi. IRCCS Policlinico S. Matteo Foundation, Pavia, Italy
-
Upload
pah-ghio -
Category
Health & Medicine
-
view
1.253 -
download
5
description
ipertensione polmonare nelle malattie ematologiche
Transcript of Ipertensione Polmonare nelle malattie ematologiche

L’Ipertensione Polmonare nelle Malattie Ematologiche
Corso di aggiornamento sull’ipertensione polmonare. Pavia 21 maggio 2011
Giovanni Barosi Laboratorio di Epidemiologia Clinica/Centro per lo
Studio della Mielofibrosi. IRCCS Policlinico S. Matteo Foundation, Pavia, Italy

Malattie ematologiche con ipertensione polmonare
Hemolytic anemias• Thalassemia intermedia
• Sickle cell anemia
• Hereditary spherocytosis
• PK deficiency
• Unstable hemoglobin
• Paroxysmal nocturnal hemoglobinuria
• Microangiopathic hemolytic anemia
Myeloproliferative neoplasms• Essential thrombocythemia
• Polycythemia vera
• Primary myelofibrosis
• Eosinophilic leukemia
Lymphoproliferative disorders• Castelman disease
• POEMS

Pathogenesis of PH in hemolytic anemias

Perspectives
• Primary myelofibrosis –associated PH
• PH-associated myelofibrosis
Myelofibrosis and Pulmonary Arterial Hypertension (PH)

WHO Classification of tumours of hematopoietic and lymphoid tissues (2008)
MYELOPROLIFERATIVE NEOPLASMS
• Chronic myelogenous leukemia, BCR-ABL1 positive
• Chronic neutrophilic leukemia
• Polycythemia vera
• Primary myelofibrosis
• Essential thrombocythemia
• Chronic eosinophilic leukemia, NOS
• Mastocytosis
• Myeloproliferative neoplasm, unclassifiable
Classical Ph1-neg MPNsClassical Ph1-neg MPNs

Myeloproliferative Neoplasms (MPNs)
CML CNL/MCD
PV ET
PMF

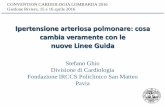
1. Clonal proliferation of hematopoietic stem cell (mutational events like JAK2V617F)
Current Biological Pradigm of MMM

2. Clonal cells (CD34+, megakaryocytes, monocytes) excessively produce hematopoietic, fibrogenic and angiogenic growth factors
Current Biological Pradigm of MMM
MO
fibroblast
endothelium
M-CSF
SCF
IL-6
TGF-
MYELOPROLIFERATION MYELOFIBROSIS NEOANGIOGENESIS
TGF- PDGF
MKCD34+
TGF-VEGF
Castro-Malaspina, 1984; Le Bousse Kardiles et al, 2001; Rameshwar et al, 2000

Primary myelofibrosis

Barosi et al. Blood 2001
Barosi et al, BJH 2003
0
50
100
150
200
250
300
350
MMM PV ET Controls
3. CD34+ hemopoietic stem cells constitutionally migrate from bone marrow to blood and to extramedullary organs
Current Biological Paradigm of MMM
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
4,0
4,5
5,0
MMM Normal
CD34 + in PB CD34 + in Spleen

PERIPHERAL BLOOD
HEMATOPOIESIS FIBROSIS BONE
MARROW
A Biological Model of MMM
CD34+ CELLS
HEMATOPOIESIS
Anemia, thrombocytopenia
SPLEEN
Splenomegaly
Blast transformation
ANGIOGENESIS
ANGIOGENESIS?

•Relief of fatigue and constitutional symptoms•Relief of pruritus•Relief of severe anemia•Relief of transfusion dependent anemia•Treatment of transfusional iron overload•Relief of symptomatic splenomegaly•Relentless of spleen enlargement in progressive splenomegaly•Reversion of accelerated phase or blast transformation of the
disease•Treatment of extramedullary non-hepatosplenic hematopoiesis•Treatment of pulmonary hypertension•Treatment of portal hypertension•Treatment of splanchnic vein thrombosis•Treatment of thrombotic or hemorrhagic complication
Common clinical needs in PMF

PH in PMF (and MPNs)
Author Disorders Diagnosis of PH Incidence
Garypidou et al. (Haematologica 2004)
PV =2ET=14PMF=6CML=2
Transthoracic Echo (TTE)
41.7%
Altintas et al. (Leukemia & Lymphoma, 2007)
ET=46Reactive thrombocytosis=40
TTE ET= 47.8%Reactive thrombocytosis=0%
Gupta et al. (J Natl Med Ass 2006)
ET=9PV=15CML=3
TTE 48%
Cortelezzi et al. (Leukemia, 2008)
PMF or post ET/Post PV MF =36
TTE 36%

Limitations of epidemiological studies in MPNs
• Diagnosis of PH was not established as recommended by guidelines (Overestimation of the incidence)
• No distinction between post-embolic PH and primary PH

Clinical forms of PH in MPNs
• Chronic thromboembolic PH (CTEPH)
• Precapillary PH, mimicking Primary PH

Mechanisms for the development of PAH–like disease in primary myelofibrosis
• Thrombocythosis
• Non-hepatosplenic extramedullary hematopoiesis
• Enhanced angiogenesis
• Portal hypertension

Thrombocytosis
Secretion of vasoactive cytokines
Circulating TPO levels
PDGF secretion
Smooth muscle cells hyperplasia
Pulmonary hypertension

Non-hepatosplenic extramedullary hematopoiesis
Pulmonary myeloid infiltration
Growth factors and cytokine secretion
Pulmonary hypertension


Circulating megakaryocytes
Megakaryocyte embolism
Pulmonary capillary obstruction
Pulmonary hypertension

Enhanced angiogenesisHigh serum VEGF levels, low number of
circulating EPCs
Pulmonary hypertension

The current recommendations for how to manage PH in PMF
Tefferi, Mayo Clinic, 2011
• MF-associated PH is suspected in the presence of dyspnea/hypoxia on exertion and peripheral edema.
• It is important to rule out thromboembolic, infectious or inflammatory lung processes (high resolution CT scanning)
• Increased systolic pulmonary artery pressure on echography and an abnormal pulmonary uptake during technetium 99m sulphur colloid scintigraphy should be documented
• In the absence of an alternative explanation for pulmonary hypertension, treatment with single-fraction (100cGy) whole-lung irradiation is reasonable even if technetium scan was negative

PH-associated myelofibrosis
•Myelofibrosis is present in patients with PH. It is not a primary neoplastic hematopoietic disorder. Its mechanism remains to be elucidated (Popat U et al. Ann Intern Med, 2005
•Increased bone marrow hemangioblast number, alterations in erythroid/myeloid lineages, increased reticulin, and greater mobilization of bone marrow progenitor cells are integral part of PH disease (subclinical myeloproliferative process?) (Farha S et al. Blood 2011)
• Elevation of bone marrow progenitors and reticulin was revealed in non affected family members of patients with familial PH.

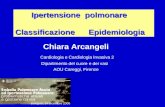
Pulmonary vascular disease and myeloid abnormalities in PAH.
Farha S et al. Blood 2011;117:3485-3493