Investigations for chronic pelvic pain.pdf
10
Investigations for chronic pelvic pain Ying Cheong a, * , William Stones b a Princess Anne Hospital, Southampton SO16 6YD, UK b University of Southampton, Southampton, UK Received 22 April 2004; accepted 6 July 2005 Available online 19 September 2005 Abstract Chronic pelvic pain (CPP) is a common problem with a prevalence of about 38/1000 among women aged 20–50 years. The main gynaecological diagnoses include endometriosis, pelvic inflammatory disease and adhesions. The most common gastrointestinal diagnosis is irritable bowel syndrome and genitourinary diagnosis includes pathology such as interstitial cystitis. It is a challenge instigating the right investigations for patients with chronic pelvic pain because there is a considerable symptom overlap. They also have a higher prevalence for symptoms such as dysmenorrhea and dyspareunia. In this review, we aim to discuss the clinical consultation necessary to help us decide upon which investigative tools we need to use to help diagnose the cause(s) of CPP, although one needs to stress that a specific cause may not be found in patients with CPP and symptom focused multidisciplinary management of CPP is at least as important as diagnosis of specific pathology and disease focused treatment. # 2005 Elsevier B.V. All rights reserved. Keywords: Chronic pelvic pain; Investigations; Ultrasound; Magnetic resonance imaging; Venography; Laparoscopy; Pelvic congestion syndrome; Adhesions; Endometriosis; Adenomyosis 1. Introduction Chronic pelvic pain (CPP) may be defined as a non- cyclical pain of greater than 6 months’ duration that is localised to the pelvis, anterior abdominal wall at or below the umbilicus, the lumbosacral area, or buttocks, and is of sufficient severity as to cause functional disability or lead to medical care [1]. Pain is generally defined as an unpleasant sensory and emotional experience associated with actual or potential tissue damage. It is therefore most important for health professions to appreciate the emotional and subjective nature of pain, in particular CPP. Historically, gynaecolo- gists have tended to discount pain symptoms with an undue emphasis on visible pathology as validating the patient’s experience. CPP is a common problem: the prevalence of the condition is about 38/1000 among women aged 20–50 years, not dissimilar to the prevalence of common conditions such as asthma (37/1000), back pain (41/1000) and migraine (21/ 1000) [2,3]. There is also evidence that the prevalence of CPP is probably underestimated in clinical studies, as up to 40% of women in a large questionnaire survey reported not seeking any medical help for their pelvic pain [3]. In a cohort study, approximately 5000 women were followed up over a period of 3–4 years from their first contact with primary care. CPP had median symptom duration of 15 months and a third of women had persistent symptoms after 2 years. The study also showed that a quarter of women had no diagnosis made in that 3–4 years follow-up period, and only 40% were referred to a hospital specialist. CPP has been shown significantly to affect women’s daily activities, and has a significant negative impact on their mental and physical health [3]. The main gynaecological diagnoses include endome- triosis, pelvic inflammatory disease and adhesions. The most common gastrointestinal diagnosis is irritable bowel syndrome and possible genitourinary diagnosis includes pathology such as interstitial cystitis. The laparoscopic findings of women with CPP, in increasing order of www.elsevier.com/locate/rigp Reviews in Gynaecological Practice 5 (2005) 227–236 * Corresponding author. E-mail address: [email protected] (Y. Cheong). 1471-7697/$ – see front matter # 2005 Elsevier B.V. All rights reserved. doi:10.1016/j.rigp.2005.07.001
Transcript of Investigations for chronic pelvic pain.pdf

Investigations for chronic pelvic pain
Ying Cheong a,*, William Stones b
aPrincess Anne Hospital, Southampton SO16 6YD, UKbUniversity of Southampton, Southampton, UK
Received 22 April 2004; accepted 6 July 2005
Available online 19 September 2005
Abstract
Chronic pelvic pain (CPP) is a common problem with a prevalence of about 38/1000 among women aged 20–50 years. The main
gynaecological diagnoses include endometriosis, pelvic inflammatory disease and adhesions. The most common gastrointestinal diagnosis is
irritable bowel syndrome and genitourinary diagnosis includes pathology such as interstitial cystitis. It is a challenge instigating the right
investigations for patients with chronic pelvic pain because there is a considerable symptom overlap. They also have a higher prevalence for
symptoms such as dysmenorrhea and dyspareunia. In this review, we aim to discuss the clinical consultation necessary to help us decide upon
which investigative tools we need to use to help diagnose the cause(s) of CPP, although one needs to stress that a specific cause may not be
found in patients with CPP and symptom focused multidisciplinary management of CPP is at least as important as diagnosis of specific
pathology and disease focused treatment.
# 2005 Elsevier B.V. All rights reserved.
Keywords: Chronic pelvic pain; Investigations; Ultrasound; Magnetic resonance imaging; Venography; Laparoscopy; Pelvic congestion syndrome;
Adhesions; Endometriosis; Adenomyosis
www.elsevier.com/locate/rigp
Reviews in Gynaecological Practice 5 (2005) 227–236
1. Introduction
Chronic pelvic pain (CPP) may be defined as a non-
cyclical pain of greater than 6 months’ duration that is
localised to the pelvis, anterior abdominal wall at or below
the umbilicus, the lumbosacral area, or buttocks, and is of
sufficient severity as to cause functional disability or lead to
medical care [1]. Pain is generally defined as an unpleasant
sensory and emotional experience associated with actual or
potential tissue damage. It is therefore most important for
health professions to appreciate the emotional and subjective
nature of pain, in particular CPP. Historically, gynaecolo-
gists have tended to discount pain symptoms with an undue
emphasis on visible pathology as validating the patient’s
experience.
CPP is a common problem: the prevalence of the
condition is about 38/1000 among women aged 20–50 years,
not dissimilar to the prevalence of common conditions such
* Corresponding author.
E-mail address: [email protected] (Y. Cheong).
1471-7697/$ – see front matter # 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.rigp.2005.07.001
as asthma (37/1000), back pain (41/1000) and migraine (21/
1000) [2,3]. There is also evidence that the prevalence of
CPP is probably underestimated in clinical studies, as up to
40% of women in a large questionnaire survey reported not
seeking any medical help for their pelvic pain [3]. In a cohort
study, approximately 5000 women were followed up over a
period of 3–4 years from their first contact with primary
care. CPP had median symptom duration of 15 months and a
third of women had persistent symptoms after 2 years. The
study also showed that a quarter of women had no diagnosis
made in that 3–4 years follow-up period, and only 40% were
referred to a hospital specialist. CPP has been shown
significantly to affect women’s daily activities, and has a
significant negative impact on their mental and physical
health [3].
The main gynaecological diagnoses include endome-
triosis, pelvic inflammatory disease and adhesions. The most
common gastrointestinal diagnosis is irritable bowel
syndrome and possible genitourinary diagnosis includes
pathology such as interstitial cystitis. The laparoscopic
findings of women with CPP, in increasing order of

Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236228
frequency: these were endometriosis (33%), adhesions
(24%) and ‘‘no pathology’’ (35%) [1,3]. This contrasts
with the diagnosis of CPP in the community, where causes
related to urinary (31%) and gastro-intestinal (37%) systems
was more common than gynaecological (20%) diagnoses.
The discrepancies in the diagnosis obtained in these patients
may be due to differences in the population studied, to the
limited diagnostic scope of gynaecology clinics and the
different approaches to the management of the condition in
the community as opposed to tertiary centres.
In this review, we aim to discuss the clinical consultation
necessary to help us decide upon which investigative tools
we will need to use to help diagnose the cause of CPP. We
also aim to discuss how these investigations can best help us
manage CPP. In many cases, a specific cause may not be
found in patients with CPP and symptom focused multi-
disciplinary management of CPP is at least as important as
diagnosis of specific pathology and disease oriented
treatment.
2. The consultation in the gynaecology clinic
Less than half of women with CPP get referred to a
gynaecological specialist [3]. Often, when referred, women
have high expectations of the gynaecologist. Furthermore,
the gynaecologist may be looking for organic pathology,
which may not exist. In our chronic pelvic pain clinic at the
Princess Anne Hospital, Southampton, we try to minimise
this mismatch by identifying the individual needs of each
patient so as to meet their expectations as much as possible.
For some patients, the priority may be to gain an explanation
of the cause(s) of their pain, although most are in search of
more effective symptom control.
In a series of patients referred from general practice, Selfe
et al. showed that the initial gynaecological consultation has
significant impact on the clinical outcome of women with
chronic pelvic pain [4]. The individual doctor undertaking
the consultation was shown to influence the patients’ pain
scores 6 months later. Thus, as clinicians, we need to be
aware of our own consultation styles and attitudes, which
may enter into the dynamics of the management of such
patients. It is obvious that patients with CPP require more
time and effort on the initial consultation, and many will
benefit from a multidisciplinary team assessment and
management setting but there are important practical
limitations to making this universally available.
Table 1
Referred pain from the various somatic nerves are shown
Somatic nerve Dermatome V
Ilioinguinal L1-2 P
Genitofemoral L1-2 P
Lateral femoral cutaneous L2-3 L
Pudendal S2-4 L
Besides enquiring about the routine gynaecological
symptoms, it is also prudent to be aware of psychological
morbidity. Whether a woman with CPP has endometriosis
or not, the likelihood of her having a concomitant mood
disorder is the same [5,6]. Mood disorder is easily missed
in general gynaecology clinic. Simple enquiry about sleep
and mood should be routine in clinic. There is no evidence
that antidepressants per se can ameliorate the symptoms
of CPP, but treatment of depression or anxiety can
improve the patient’s general quality of life. The
awareness of multiple unexplained symptoms in women
with CPP may prompt psychological/psychiatric referral,
thus minimising the risk of inappropriate surgical or
medical intervention. The key feature for somatisation is
the presence of multiple physical symptoms, for example,
referral to many specialists for many complaints. The
latter history would represent a prompt for involving a
liaison psychiatrist. There is a well-defined psychiatric
diagnosis of somatisation disorder but more often women
with CPP seen in a gynaecological setting do not manifest
the full blown syndrome. Specific criteria for mental
health referral include: (1) the presence of significant
mood disorder identified on a questionnaire or in the
history (e.g. suicidal ideation); (2) a history of abuse
(sexual or physical) although it is worth noting that many
patients with a history of abuse have resolved the
psychological consequences, and do not necessarily need
intervention or specific support, although clearly this
needs to be offered; (3) a history of drug or alcohol abuse
and/or addictive behavior; (4) ongoing concomitant
psychiatric illness, for example, an individual with
schizophrenia on multiple medications may still present
with problems needing help from a gynaecologist; in this
situation, it is advantageous to liaise with the mental
health team, although there is no suggestion that that
pelvic pain is due to schizophrenia.
During the clinical examination, it is important to
perform an anterior abdominal wall examination. Trigger
points identified on the anterior abdominal wall may suggest
nerve entrapment. Trigger points are areas of discrete
hyperalgesia. When palpated with fingertip pressure, they
elicit sharp pain that can refer to distant dermatomes.
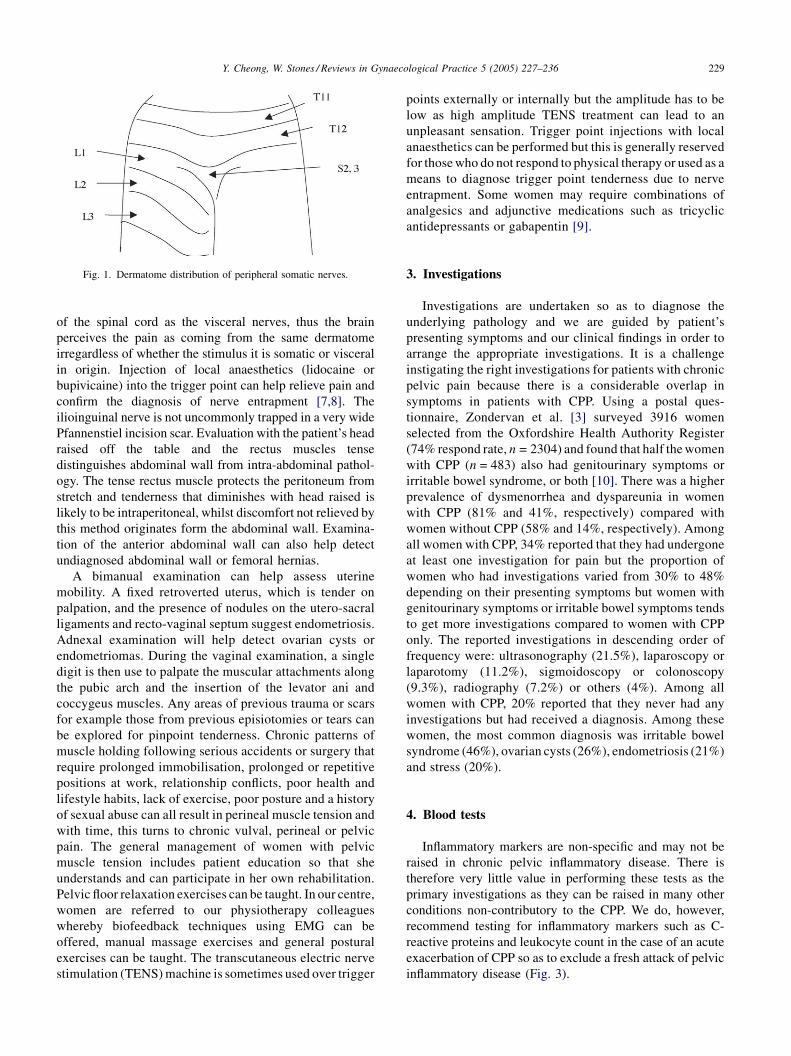
Referred pain from different somatic nerves is illustrated in
Table 1 and Fig. 1. Because of a physiological phenomenon
called ‘viscerosomatic convergence’, subjective discrimina-
tion of somatic and visceral pain can be difficult. This is
because the somatic nerves synapse in the same dorsal horn
isceral field
roximal tube, uterine fundus
roximal tube, uterine fundus
ower uterine segment
ower uterine segment, cervix, bladder, distal ureter, upper vagina, rectum
Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236 229
Fig. 1. Dermatome distribution of peripheral somatic nerves.
of the spinal cord as the visceral nerves, thus the brain
perceives the pain as coming from the same dermatome
irregardless of whether the stimulus it is somatic or visceral
in origin. Injection of local anaesthetics (lidocaine or
bupivicaine) into the trigger point can help relieve pain and
confirm the diagnosis of nerve entrapment [7,8]. The
ilioinguinal nerve is not uncommonly trapped in a very wide
Pfannenstiel incision scar. Evaluation with the patient’s head
raised off the table and the rectus muscles tense
distinguishes abdominal wall from intra-abdominal pathol-
ogy. The tense rectus muscle protects the peritoneum from
stretch and tenderness that diminishes with head raised is
likely to be intraperitoneal, whilst discomfort not relieved by
this method originates form the abdominal wall. Examina-
tion of the anterior abdominal wall can also help detect
undiagnosed abdominal wall or femoral hernias.
A bimanual examination can help assess uterine
mobility. A fixed retroverted uterus, which is tender on
palpation, and the presence of nodules on the utero-sacral
ligaments and recto-vaginal septum suggest endometriosis.
Adnexal examination will help detect ovarian cysts or
endometriomas. During the vaginal examination, a single
digit is then use to palpate the muscular attachments along
the pubic arch and the insertion of the levator ani and
coccygeus muscles. Any areas of previous trauma or scars
for example those from previous episiotomies or tears can
be explored for pinpoint tenderness. Chronic patterns of
muscle holding following serious accidents or surgery that
require prolonged immobilisation, prolonged or repetitive
positions at work, relationship conflicts, poor health and
lifestyle habits, lack of exercise, poor posture and a history
of sexual abuse can all result in perineal muscle tension and
with time, this turns to chronic vulval, perineal or pelvic
pain. The general management of women with pelvic
muscle tension includes patient education so that she
understands and can participate in her own rehabilitation.
Pelvic floor relaxation exercises can be taught. In our centre,
women are referred to our physiotherapy colleagues
whereby biofeedback techniques using EMG can be
offered, manual massage exercises and general postural
exercises can be taught. The transcutaneous electric nerve
stimulation (TENS) machine is sometimes used over trigger
points externally or internally but the amplitude has to be
low as high amplitude TENS treatment can lead to an
unpleasant sensation. Trigger point injections with local
anaesthetics can be performed but this is generally reserved
for those who do not respond to physical therapy or used as a
means to diagnose trigger point tenderness due to nerve
entrapment. Some women may require combinations of
analgesics and adjunctive medications such as tricyclic
antidepressants or gabapentin [9].
3. Investigations
Investigations are undertaken so as to diagnose the
underlying pathology and we are guided by patient’s
presenting symptoms and our clinical findings in order to
arrange the appropriate investigations. It is a challenge
instigating the right investigations for patients with chronic
pelvic pain because there is a considerable overlap in
symptoms in patients with CPP. Using a postal ques-
tionnaire, Zondervan et al. [3] surveyed 3916 women
selected from the Oxfordshire Health Authority Register
(74% respond rate, n = 2304) and found that half the women
with CPP (n = 483) also had genitourinary symptoms or
irritable bowel syndrome, or both [10]. There was a higher
prevalence of dysmenorrhea and dyspareunia in women
with CPP (81% and 41%, respectively) compared with
women without CPP (58% and 14%, respectively). Among
all women with CPP, 34% reported that they had undergone
at least one investigation for pain but the proportion of
women who had investigations varied from 30% to 48%
depending on their presenting symptoms but women with
genitourinary symptoms or irritable bowel symptoms tends
to get more investigations compared to women with CPP
only. The reported investigations in descending order of
frequency were: ultrasonography (21.5%), laparoscopy or
laparotomy (11.2%), sigmoidoscopy or colonoscopy
(9.3%), radiography (7.2%) or others (4%). Among all
women with CPP, 20% reported that they never had any
investigations but had received a diagnosis. Among these
women, the most common diagnosis was irritable bowel
syndrome (46%), ovarian cysts (26%), endometriosis (21%)
and stress (20%).
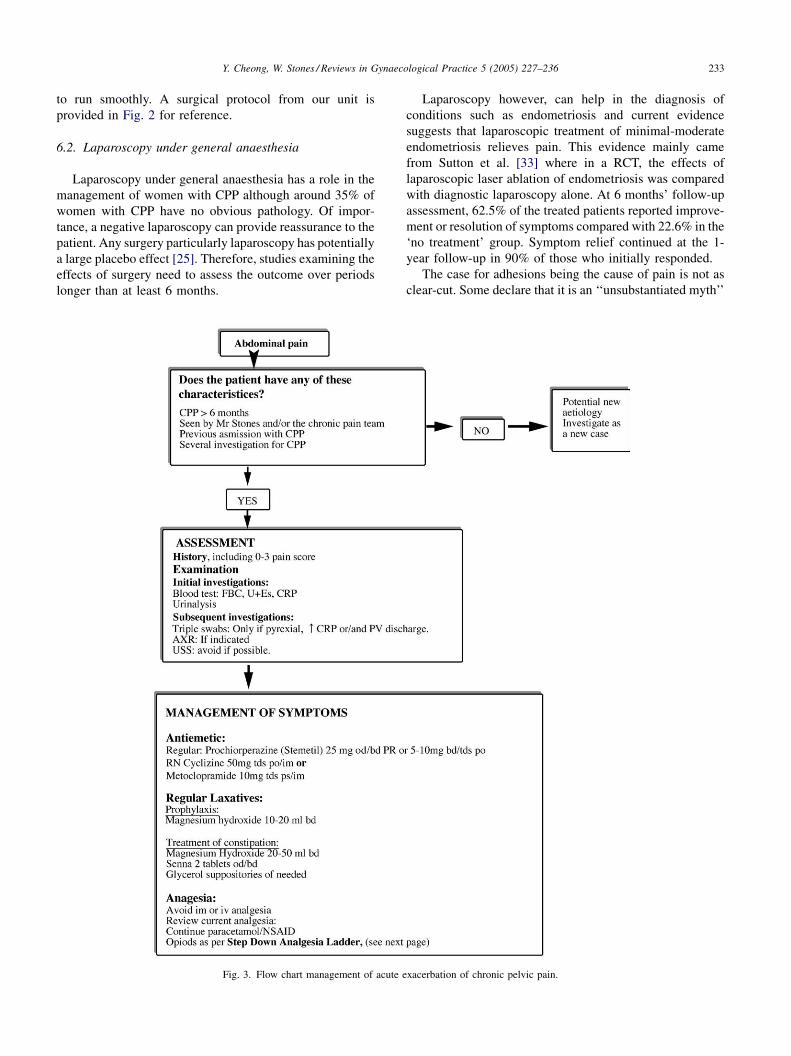
4. Blood tests
Inflammatory markers are non-specific and may not be
raised in chronic pelvic inflammatory disease. There is
therefore very little value in performing these tests as the
primary investigations as they can be raised in many other
conditions non-contributory to the CPP. We do, however,
recommend testing for inflammatory markers such as C-
reactive proteins and leukocyte count in the case of an acute
exacerbation of CPP so as to exclude a fresh attack of pelvic
inflammatory disease (Fig. 3).

Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236230
5. Radiological
5.1. Endometriosis
Transvaginal ultrasonography (TVS) is helpful in
assessing endometriotic ovarian cysts. On TVS, endome-
triomas appear as ovarian cysts with low level internal
echoes, multilocularity or hyperechoic wall foci. TVS,
however, has little value in assessing the presence of
adhesions and mild peritoneal deposits. In deep infiltrating
disease, where endometriosis involves the Pouch of
Douglas, often hypoechoic linear thickening, or nodules/
masses with or without regular contours can be seen on TVS,
occasionally infiltrating into organs or on the uterosacral
ligaments. The Pouch of Douglas can also be obliterated
with or without free fluid. Bazot et al. [34] examined 142
women with clinical signs of endometriosis with transva-
ginal scanning (TVS) in a prospective cohort study where
ultrasound findings were compared to surgical and
histological findings. They found that the sensitivity,
specificity, positive and negative predictive values of TVS
for predicting deep infiltrating pelvic endometriosis were
79%, 95%, 95% and 78%.
More recently, the role of endoanal ultrasound has been
evaluated for the diagnosis of deep infiltrating endome-
triosis. Delpy et al. [6] studied the use of anorectal
endoscopic ultrasonographic examination (EUS) in the
diagnosis of severe rectovaginal septum endoemtriosis in
30 patients. EUS showed the presence of rectovaginal
septum endometriosis in 26 patients (88%), in the
uterosacral ligaments in 10 patients (33%) and in the
ovaries in 2 patients (6%). Subsequent surgical explora-
tion demonstrated RV septum endometriosis in 26 patients
(88%) and the uterosacral ligament in 22 (73%) cases, and
the ovaries in 6 (20%) cases. They concluded that EUS
has a sensitivity of 96%, specificity of 100%, positive
predictive value of 100% and negative predictive value of
83% in diagnosing endometriosis in the rectovaginal
septum [6].
It therefore appears that TVS and endoanal ultrasono-
graphy, in the right hands within an appropriate referral
population is reasonably accurate in diagnosing deeply
infiltrating posterior endometriosis although this degree of
accuracy may not be achievable in all units. More
importantly, although laparoscopy is the ‘gold standard’
for diagnosis of endometriosis, the correlation between
visible endometriosis and histological diagnosis can vary
[11,12]. As not all patients in these studies who have visible
endometriosis during laparoscopy have histologically con-
firmed endometriosis, the results may be confounded.
Further studies with larger sample sizes are needed to
confirm or refute the reliability and accuracy of routine use
of such radiological investigations for the diagnosis of deep
infiltrating pelvic endometriosis.
Adenomyosis is characterized by the presence of
heterotrophic endometrial glands and stroma in the
myometrium with adjacent smooth muscle hyperplasia.
Women with adenomyosis often present with pelvic pain,
dysmenorrhea and menorrhagia. Pre-operative diagnosis of
adenomyosis is poor, ranging from 2.6% to 26%.
Transabdominal ultrasound does not have as good a
resolution as the transvaginal ultrasound. Criteria used for
diagnosing adenomyosis on transvaginal ultrasound include
uterine enlargement not explained by the presence of
fibroids, asymmetric thickening of the anterior or posterior
myometrial walls, heterogeneous, poorly circumscribed area
in the myometrium, anechoic lacunae cysts of caring size
and increased echo texture of the myometrium [13]. The
most accurate modality for the diagnosis of adenomyosis is
probably MR imaging. It has a sensitivity and specificity
ranging from 86% to 100%. This high accuracy is attributed
by the excellent soft tissue differentiation of MR imaging
compared to other imaging modalities. It is important to note
that many of these studies are measured against histopatho-
logical findings after hysterectomy. MR is less operator-
dependent compared to ultrasound but is however limited by
the high cost and availability of this imaging modality,
especially when the symptoms of adenomyosis can be rather
non-specific.
5.2. Adhesions
No method currently is in use for rapid, inexpensive and
noninvasive identification of infra-umbilical bowel adhe-
sions before laparoscopy. Existing entry methods, such as
entering the left upper quadrant or performing a small
laparotomy, do not directly address the issue of adequately
identifying those with adhesions, and require tissue
dissection. Ultrasound is easily available to gynaecologists
and surgeons. Transabdominal ultrasound when used
together with the ‘‘visceral slide test’’ can help diagnose
the presence of anterior abdominal wall adhesions [14,15].
The visceral slide test refers to a phenomenon whereby
respiratory movement or manual ballottement induces the
viscera, as visualised on ultrasound, to slide just beneath
the anterior abdominal wall. In the presence of adhesions,
this sliding motion is limited and thus indicative of the
presence of anterior abdominal wall adhesions. This
technique may be particularly useful to aid in the initial
safe placement of instruments at laparoscopy in patients
with an increased risk of complications secondary to
anterior abdominal wall adhesions. A more recent study by
Tu et al. evaluated 60 women at risk for intra-abdominal
adhesions who underwent laparoscopy or laparotomy [15].
All participants underwent the visceral slide test with peri-
umbilical sonographic measurements. With a prevalence
of infra-umbilical bowel adhesions of 12%, they found that
the visceral slide test has sensitivity = 86%, specifi-
city = 91%, positive predictive value = 55% and negative
predictive value = 98%. Visceral slide testing can therefore
inform a decision on trocar site, and with a high negative
predictive value, can serve to expand on the number of

Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236 231
patients who might benefit from laparoscopy and avoid
laparotomy. It is however important to note that the above
study was not blinded and this could have confounded the
results. Further trials are required to evaluate the role of
ultrasound and the visceral slide test in determining the
best port site as well as decreasing port-related complica-
tions.
As for adhesions in the pelvis, Ubaldi et al. performed
TVS on 133 women who attended their fertility clinic in
Belgium [16]. They suspected pelvic adhesions when
there was poor definition of pelvic structures. Pelvic
adhesions were diagnosed by TVS in 13 patients and this
finding was confirmed at laparoscopy in 11 patients. Of
the 120 TVS findings that showed no adhesions, 113 were
confirmed by laparoscopy. In seven patients with filmy
adhesions, TVS failed to detect these. The sensitivity,
specificity, positive and negative predictive values of TVS
for diagnosing adhesions were 61%, 98%, 84% and 94%,
respectively. The authors also calculated the efficiency to
be 93%. Thus, it appears that TVS is poor in picking up
the presence of adhesions, but TVS is fairly accurate in
predicting the absence of adhesions except when the
adhesions are filmy [16]. Laparoscopy however, remains
the investigation of choice if one suspects clinically
significant adhesions.
5.3. Pelvic congestion syndrome
Pelvic congestion is a condition associated with
dilatation and reduced venous clearance in the pelvis.
The exact patho-physiology is still a puzzle although it is
thought to be associated with psychological as well as
biological predisposition. The common symptoms are
shifting location of pain, deep dyspareunia and post-coital
pain and exacerbation of pain after prolonged standing
[17]. Venography is still considered the definitive
radiological investigation for women with pelvic conges-
tion syndrome. The radiological features are dilated
uterine and ovarian veins with reduced venous clearance
of contrast medium [18]. The absence of reflux on the
ovarian vein does not preclude the diagnosis of pelvic
congestion syndrome because other diagnostic features
include the diameter of the ovarian veins, the distribution
of vessels, and the delay in contrast medium. Ultrasound
does not appear to be as good as venography in the
diagnosis of the condition and the correlation between
ultrasound and venography is poor [19]. Diagnosis via
laparoscopy is also possible although there is no objective
measure of the diameter of the pelvic veins. Small
anecdotal studies have suggested retroperitoneal ovarian
vein ligation via laparotomy or laparoscopically, or
radiological embolisation of the ovarian veins has been
described. These surgical modalities of treatment are still
under research [20–22]. Treatment of the condition
primarily involves of ovarian suppression and physiolo-
gical intervention such as stress reduction.
6. Endoscopic
6.1. Laparoscopy under local anaesthesia
Conscious laparoscopic pain mapping (CLPM) is a
diagnostic laparoscopy performed under local anaesthesia in
women with chronic pelvic pain (CPP); the objective is to
localise the sources of tenderness with the aid of the patient
when mechanical stimulus is applied to areas in the pelvis
and the pelvic organs. During CLPM, the advantage is that
the patient can be conscious and can therefore alert the
clinician to the site of tenderness, the assumption is made
that pain stimulus in CPP must be mechanical. This, in fact,
has not been fully supported by the literature. The patho-
physiology of pain in CPP is often not mechanical. There is
little research on the actual effect of laparoscopy and
gaseous insufflations on pain perception. Furthermore, even
when pathology such as endometriosis is diagnosed, the pain
correlation with mechanical stimulus to the affected areas is
inconsistent [23].
However, the findings of CLPM can help to guide the
clinician as to the subsequent steps of management of CPP.
A clinical audit of all the women who underwent pain
mapping over the last 4 years in Southampton showed that
the number of women with tenderness over the following
areas in decreasing order of frequency were: ovaries and/or
uterus (38%, n = 15); generalised hyperalgesia, therefore
suggesting neuropathic pain (21%, n = 8); adhesions and
sterilisation clip (13%, n = 5); abdominal wall (8%, n = 3);
occult inguinal hernia (8%, n = 3); vaginal vault (5%, n = 2)
and others (5%, n = 2) [24]. As a result of the findings, we
are able to triage women who had CLPM in our study for
further surgery (41%, n = 16) further hormonal treatment
(28%, n = 11), further pain management via the multi-
disciplinary pain team 26% (n = 10) and 5% (n = 2) were
discharged back to the GP. Defining ‘‘success’’ as the
outcomes of benefit to the patient (Table 2), we concluded on
the basis of the case note review that 82% of the procedures
were successful. It should be noted that these audit findings
cannot be generalized to other settings and CLPM cannot be
recommended a routine investigation. In our clinical
practice, patients who are elect to undergo CLPM are a
specific sub-group where following a clinical history and
examination the assessment is that CLPM could (1) identify
a problem that can be resolvable by further surgery and/or
(2) demonstrate the presence of generalised non-localised
tenderness, a finding that may enable the patient to reorient
her goals towards pain management rather than a search for
specific focal pathology. No black and white rules exist in
the selection of these women for CLPM; rather the process is
seen as very much dependent on the consultation and the
goals and expectations of the individual patient. In
particular, given the unpleasantness of the procedure, it is
only to be considered when positively desired by the patient
after full counseling. The right theatre set-up with
appropriate anaesthetic support is required for the procedure
Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236232
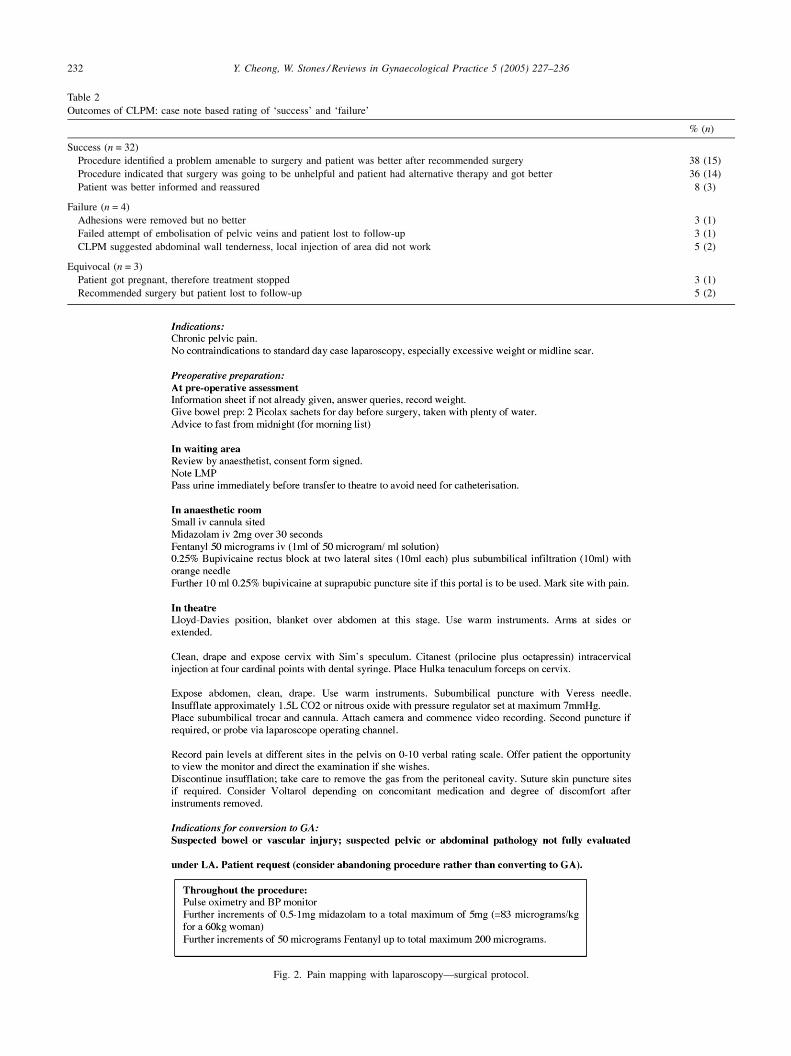
Fig. 2. Pain mapping with laparoscopy—surgical protocol.
Table 2
Outcomes of CLPM: case note based rating of ‘success’ and ‘failure’
% (n)
Success (n = 32)
Procedure identified a problem amenable to surgery and patient was better after recommended surgery 38 (15)
Procedure indicated that surgery was going to be unhelpful and patient had alternative therapy and got better 36 (14)
Patient was better informed and reassured 8 (3)
Failure (n = 4)
Adhesions were removed but no better 3 (1)
Failed attempt of embolisation of pelvic veins and patient lost to follow-up 3 (1)
CLPM suggested abdominal wall tenderness, local injection of area did not work 5 (2)
Equivocal (n = 3)
Patient got pregnant, therefore treatment stopped 3 (1)
Recommended surgery but patient lost to follow-up 5 (2)
Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236 233
to run smoothly. A surgical protocol from our unit is
provided in Fig. 2 for reference.
6.2. Laparoscopy under general anaesthesia
Laparoscopy under general anaesthesia has a role in the
management of women with CPP although around 35% of
women with CPP have no obvious pathology. Of impor-
tance, a negative laparoscopy can provide reassurance to the
patient. Any surgery particularly laparoscopy has potentially
a large placebo effect [25]. Therefore, studies examining the
effects of surgery need to assess the outcome over periods
longer than at least 6 months.
Fig. 3. Flow chart management of acute e
Laparoscopy however, can help in the diagnosis of
conditions such as endometriosis and current evidence
suggests that laparoscopic treatment of minimal-moderate
endometriosis relieves pain. This evidence mainly came
from Sutton et al. [33] where in a RCT, the effects of
laparoscopic laser ablation of endometriosis was compared
with diagnostic laparoscopy alone. At 6 months’ follow-up
assessment, 62.5% of the treated patients reported improve-
ment or resolution of symptoms compared with 22.6% in the
‘no treatment’ group. Symptom relief continued at the 1-
year follow-up in 90% of those who initially responded.
The case for adhesions being the cause of pain is not as
clear-cut. Some declare that it is an ‘‘unsubstantiated myth’’
xacerbation of chronic pelvic pain.

Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236234
that adhesions cause pain [26] while others think that
‘‘adhesions can cause pelvic pain and adhesiolysis relieves it
in 60–90% of the cases’’ [27]. It therefore appears that some
adhesions are associated with pain and some not. The
Cochrane review [28] concluded that although adhesiolysis
in general does not resolve CPP, there is some benefit if the
adhesions are vascular and dense, based on the results of a
single study by Peters et al. [29].
In terms of patho-physiology, it is hypothesised that the
peritoneum, when under traction and tension, produces pain
as a result of activation of nerves in the adhesion tissue and
the viscera. To date, the best evidence for the latter comes
Fig. 4. Illustration of a step down analgesia pain ladde
from Kresch et al. [30]. In this study, the investigators
compared the findings in 100 women with pelvic pain for a
minimum period of 6 months with a control group of 50
asymptomatic women who were undergoing laparoscopic
sterilisation. In the 100 women with chronic pelvic pain,
48% had adhesions involving their uterus, ovaries and
bowel and 32% had endometriosis, while in the control
group 14% had adhesions and 15% had endometriosis. The
investigators also observed that the adhesions in the
control group were loose and did not restrict bowel
mobility whilst adhesions in the group of women with
chronic pelvic pain were more restrictive of the mobility of
r used in Princess Anne Hospital, Southampton.

Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236 235
the viscera. In this study, the one important patient
inclusion criterion was that the pain needed to be in a
consistent location, regardless of its character. This
criterion is not always used in many other studies.
Furthermore, some organs such as the ovaries are richly
innervated, and during processes such as ovulation,
produces the long recognised phenomenon of Mittelsch-
mertz (ovulation pain). Similarly, when the ovary is been
trapped or stretched by adhesions, pain can result.
More interestingly, adhesion tissue contains nerve fibres.
Kligman et al. obtained adhesion tissue from 17 patients, ten
with chronic pain and seven without, and examined the
tissue by immunohistochemistry for nerve tissues [31]. Ten
of the 17 specimens contained nerve fibres. The nerve fibres
were evenly distributed between patients with and without
pain. Tulandi et al. performed a similar but larger study on
50 patients and found no difference in the amount and
quantity of nerve fibres in adhesions from women with
pelvic pain and from those without pelvic pain [32].
However, Tulandi et al. [32] remarked on the limitations of
the study: based on a 77% proportion of nerve fibres in
women without pelvic pain, to detect a 10% difference in the
proportion of nerve fibres in the two groups of women with a
5% level of significance and a power of 80%, a total of 502
women (251 women in each group) is needed. Therefore, the
two studies to date that have examined nerve fibres and
adhesion tissue did not have enough power to answer the
question. Nevertheless, the findings that adhesion tissues
contain nerves may help explain why only some adhesions
cause pain. Adhesions that are stretched during movement of
the viscera can result in stimulation of the pain fibres, thus
initiating the release of chemical mediators and pain
response. More fundamentally, it is unlikely that the
difference between adhesions associated with pain or not
is simply the number of fibres: there may be differences in
the pattern of new innervation following tissue injury, with
differential involvement of sensory afferents expressing sub-
classes of neurotransmitter such as substance P and CGRP,
and varying in sensitivity to capsaicin. At present the normal
innervation of the peritoneum, let alone changes in sensory
nerve distribution and thresholds for activation of sensory
nerves following injury are poorly understood even in
animal experimental models of nociception, let alone in the
human context.
7. Multidisciplinary team approach
The core elements of a multidisciplinary team include a
gynaecologist with special interest in pain management, a
psychologist, a pain clinic nurse and a physiotherapist. The
multidisciplinary ‘package’ in the United Kingdom even
when available is quite varied but may include cognitive
behavioral psychotherapy, nursing support (such as in
between clinic times where medications need readjusting),
and the use of complimentary therapy including acupunc-
ture. In our unit, the team includes a gynaecologist, a pain
physician who is able to offer pain management advice and
nerve blocks where appropriate, a clinical psychologist
focusing on cognitive behavioral aspects and a pain clinic
nurse. A pain ladder protocol (Figs. 3 and 4) is used for acute
on chronic pelvic pain ward admissions. The main evidence
to show that a multidisciplinary team approach works come
from Leiden, The Netherlands [12]. The randomised
controlled trial showed that multidisciplinary approach is
beneficial compared to a conventional approach in terms of
improvement of quality of life scores although the McGill
pain score were not different in the two approaches. There
are important questions about the optimal use of this
approach as it is time consuming and expensive. Realisti-
cally, many cases will continue to be seen by a single
specialist, emphasizing the need for skills relevant to CPP
being embedded in gynaecological specialist training.
8. Conclusion
There are at present a multitude of investigational tools
for women with chronic pelvic pain. The choice of
investigations will depend on the patient’s clinical history,
symptoms. Although many of the investigations may not
reveal a diagnosis but the simple reassurance of the normal
results may be enough for some women. Perhaps we can say
that in the absence of a specific identifiable cause, CPP can
be considered a diagnostic category in its own right, as with
other types of chronic pain (i.e. pain is the disease). Many
clinicians suffer ‘heart sink’ when they see women with
chronic pelvic pain. However, much can be done to improve
care for these women by taking a broad based approach.
Much lies in the clinicians’ insight into the condition,
individual attitudes towards women with CPP, and appro-
priate management and referrals. Time spend on the initial
consultation to delineate the problems and understand the
issues underlying the condition is time well spent.
References
[1] Howard F. The role of laparoscopy in the chronic pelvic pain patient.
Clin Obstet Gynaecol 1998;46(4):749–66.
[2] Mathias SD, Kuppermann M, Liberman RF, Lipschutz RC, Steege JF.
Chronic pelvic pain: prevalence, health related quality of life, and
economic correlates. Obstet Gynecol 1996;87:321–7.
[3] Zondervan KT, Yudkin PL, Vessey MP, Jenkinson CP, Dawes MG,
Barlow DH, et al. The community prevalence of chronic pelvic pain in
women with associated illness behaviour. Br J Gen Pract
2001;51:541–7.
[4] Selfe SA, Van Vugt M, Stones RW. Chronic gynaecological pain: an
exploration of medical attitudes. Pain 1998;77(2):215–25.
[5] Walker KG, Shaw RW. Endometriosis, pelvic pain and psychological
functioning. Fertil Steril 1995;63:796–800.
[6] Delpy R, Barthet M, Gasmi M, Berdah S, Shojai R, Desjeux A, et al.
Value of endorectal ultrasonography for diagnosing rectovaginal

Y. Cheong, W. Stones / Reviews in Gynaecological Practice 5 (2005) 227–236236
septal endometriosis infiltrating the rectum. Endoscopy 2005;37(4):
357–61.
[7] Alvarez D, Rockwell P. Trigger points: diagnosis and management.
Am Fam Phys 2002;65(4):653–60.
[8] Ling F, Slocumb J. Use of trigger point injections in chronic pelvic
pain. Obstet Gynaecol Clin N Am 1993;20(4):809–15.
[9] Costello K. Myofascial syndromes, 1st ed, USA: WB Saunders, 1998.
[10] Zondervan KT, Yudkin PL, Vessey MP, Jenkinson CP, Dawes MG,
Barlow DH, et al. Chronic pelvic pain in the community—symptoms,
investigations, and diagnoses. Am J Obstet Gynecol 2001;184(6):
1149–55.
[11] Schollmeyer T, Pandit K, Schmutzler A, Mettler L. Correlation of
endoscopic interpretation of endometriosis with histological verifica-
tion. Clin Exp Obstet Gynecol 2004;31(2):107–9.
[12] Walter A, Hentz J, Magtibay P, Cornella J, Magrina J. Endometriosis:
correlation between histological and visual findings at laparoscopy.
Am J Obstet Gynecol 2001;184(7):1411–3.
[13] Reinhold C, Tafazoli F, Mehio A, Wang L, Atri M, Siegelman ES, et al.
Uterine adenomyosis: endovaginal US and MR imaging features with
histopathologic correlation. Radiographics 1999;19:S147–60.
[14] Caprini J, Arcelus J, Swanson J. The ultrasonic localisation of
abdominal wall adhesions. Surg Endosc 1995;16:283–5.
[15] Tu F, Lamvu G, Hartmann K, Steege J. Preoperative ultrasound to
predict infraumbilical adhesions: a study of diagnostic accuracy. Am J
Obstet Gynecol 2005;192:74–9.
[16] Ubaldi F, Wisanto A, Camus M, Tournaye H, Clasen K, Devroey P.
The role of transvaginal ultrasonography in the detection of pelvic
pathologies in the infertility workup. Hum Reprod 1998;13(2):
330–3.
[17] Beard RW, Reginald P, Wadsworth J. Clinical features of women with
chronic lower abdominal pain and pelvic congestion. Br J Obstet
Gynaecol 1988;95:153–61.
[18] Beard RW, Highman J, Pearce S, Reginald P. Diagnosis of pelvic
varicosities in women with chronic pelvic pain. Lancet 1984;2
(8409):946–9.
[19] Campbell D, Halligan S, Bartram C, Rogers V, Hollings N, Kingston
K, et al. Transvaginal power doppler ultrasound in pelvic congestion.
Acta Radiol 2003;44:269–74.
[20] Gargiulo T, Mais V, Brokaj L, Cossu E, Melis GB. Bilateral laparo-
scopic transperitoneal ligation of ovarian veins for treatment of pelvic
congestion syndrome. J Am Assoc Gynecol Laparosc 2003;10(4):
501–4.
[21] Tarazov PF, Verdiev ND, Prozorovskie KV. Transcatheter emboliza-
tion of ovarian vein varicosities. Vestn Khir Im I I Grek 2002;161(1):
90–4.
[22] Stones RW. Pelvic vascular congestion-half a century later. Clin Obstet
Gynecol 2003;46(4):831–6.
[23] Almeida OD, Val-Gallas JM. Concious pain mapping. J Am Assoc
Gynecol Laparosc 1997;4:587–90.
[24] Cheong YC, Al-Talib R, Stones RW. Role of conscious laparoscopic
pain mapping in the management of women with chronic pelvic pain.
In: Li, T., Ledger, W., editors. Pelvic pain. Sheffield: Taylor and
Francis Medical Books, in press.
[25] Swank DJ, Swank-Bordewijk SC, Hop WC, van Erp WF, Jenssen IM,
Bonjier HJ, et al. Laparoscopic adhesiolysis in patients with chronic
abdominal pain: a blinded randomised controlled multi-centre trial.
Lancet 2003;361(9365):1247–51.
[26] Alexander-Williams J. Do adhesions cause pain? Br Med J Clin Res
Ed 1987;294(6573):659–60.
[27] Duffy D, diZerega G. Adhesion controversies: pelvic pain as a cause of
adhesions, crystalloids in preventing them. J Reprod Med 1996;41(1):
19–26.
[28] Stones RW, Cheong YC, Horward F. Interventions for treating chronic
pelvic pain. The Cochrane Library in press;(3).
[29] Peters A, van Dorst E, Jellis B, van Zuuren E, Hermans J, Trimbos J. A
randomized clinical trial to compare two different approaches in
women with chronic pelvic pain. Obstet Gynecol 1991;77(5):740–4.
[30] Kresch A, Seifer D, Sachs L, Barrese I. Laparoscopy in 100 women
with chronic pelvic pain. Obstet Gynecol 1984;64:672–4.
[31] Kligman I, Drachenberg C, Papadimitriou J, Katz E. Immunohisto-
chemical demonstration of nerve fibres in pelvic adhesions. Obstet
Gynecol 1993;82:566–8.
[32] Tulandi T, Chen M, Al-Took S, Watkin K. A study of nerve fibers and
histopathology of postsurgical, postinfectious, and endometriosis-
related adhesions. Obstet Gynaecol 1998;92(5):766–8.
[33] Sutton CJ, Pooley AS, Ewen SP, Haines P. Follow-up report on a
randomized controlled trial of laser laparoscopy in the treatment of
pelvic pain associated with minimal to moderate endometriosis. Fertil
Steril 1997;68:1070–4.
[34] Bazot M, Thomassin I, Hourani R, Cortez A, Darai E. Diagnostic
accuracy of transvaginal sonography for deep pelvic endometriosis.
Ultrasound Obstet Gynecol 2004;24:180–5.