Invasive pneumococcal disease (IPD) surveillance in … pneumococcal disease (IPD) surveillance in...
17
1 1 Invasive pneumococcal disease (IPD) surveillance in the South- East Asia Region : Successes and challenges Dr. Pushpa Ranjan Wijesinghe Medical Officer ( Emerging Vaccine Preventable Disease Surveillance) Immunization and Vaccine Development (IVD) WHO - SEARO
-
Upload
phungkhanh -
Category
Documents
-
view
230 -
download
0
Transcript of Invasive pneumococcal disease (IPD) surveillance in … pneumococcal disease (IPD) surveillance in...
11
Invasive pneumococcal disease (IPD) surveillance in the South-
East Asia Region : Successes and challenges
Dr. Pushpa Ranjan Wijesinghe Medical Officer ( Emerging Vaccine Preventable Disease
Surveillance)Immunization and Vaccine Development (IVD)
WHO - SEARO
22
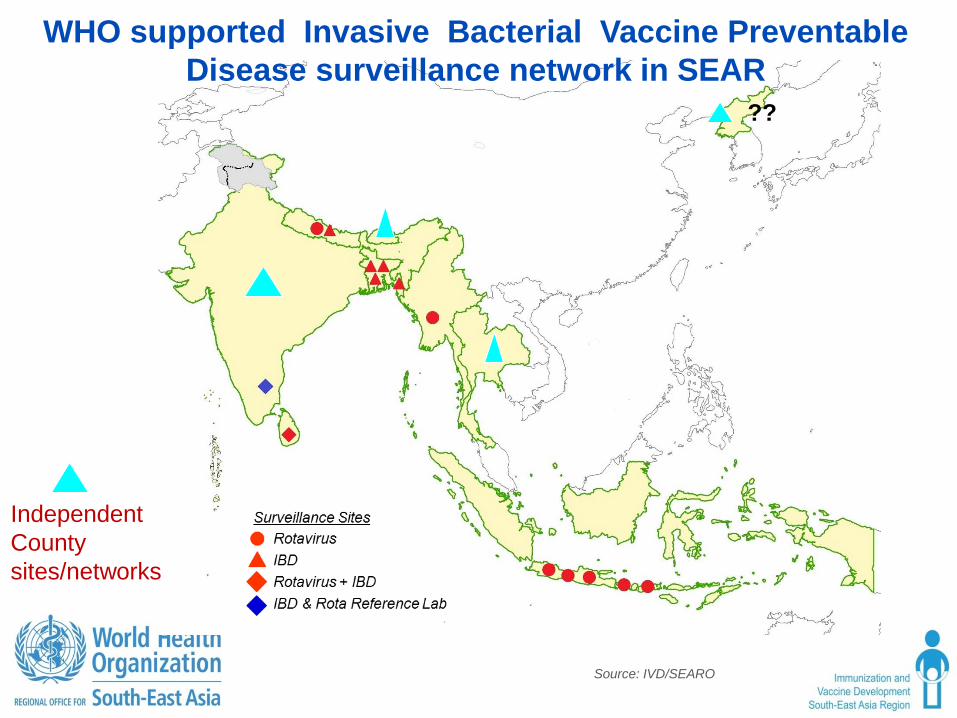
WHO supported Invasive Bacterial Vaccine Preventable Disease surveillance network in SEAR
Source: IVD/SEARO
Independent County sites/networks
??
33
1. Decisions were made and plans are underway for introduction of Pneumococcal conjugated vaccine (PCV) in the SEARa. Bangladesh : 2014b. Nepal: 2014 c. Myanmar : 2016
2. Usefulness of locally/regionally/globally generated evidence at the National Technical Advisory Group of Immunization (NTAGI) for decision makinga. Bangladesh : Introduction and selecting PCV10 over PCV 13b. Nepal: Introduction and selecting PCV10 over PCV 13c. Sri Lanka : based on available evidence, decision to introduce was
deferred in 2010 considering other public health priorities d. Myanmar : No surveillance mechanism; Regional and global
evidence use for decision making
Successes : vaccine introduction
44
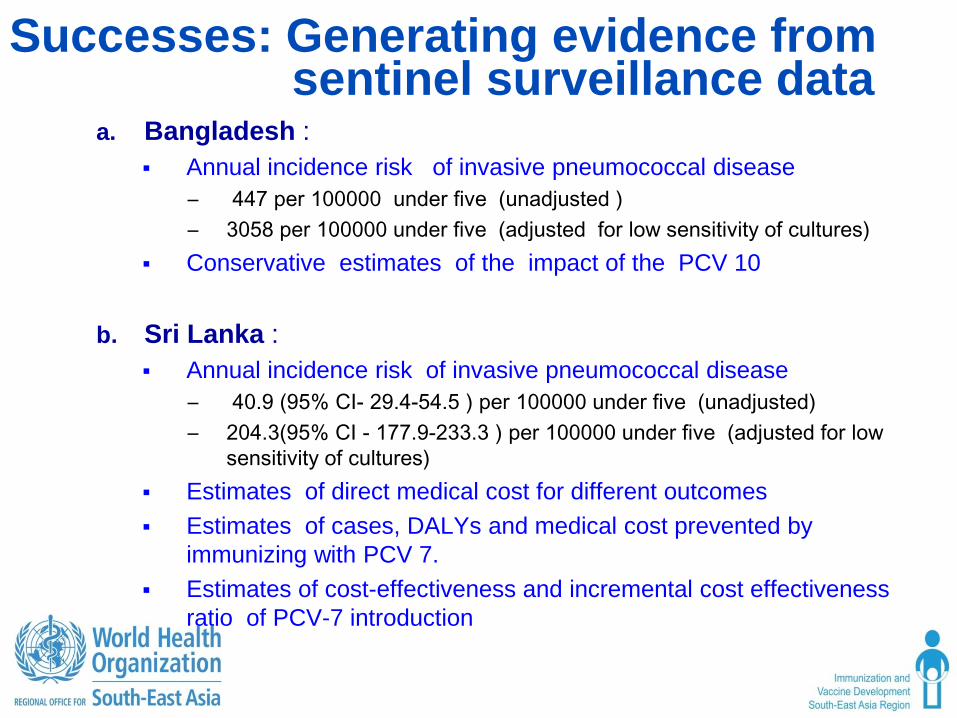
Successes: Generating evidence from sentinel surveillance data
a. Bangladesh : Annual incidence risk of invasive pneumococcal disease
– 447 per 100000 under five (unadjusted )– 3058 per 100000 under five (adjusted for low sensitivity of cultures)
Conservative estimates of the impact of the PCV 10
b. Sri Lanka : Annual incidence risk of invasive pneumococcal disease
– 40.9 (95% CI- 29.4-54.5 ) per 100000 under five (unadjusted)– 204.3(95% CI - 177.9-233.3 ) per 100000 under five (adjusted for low
sensitivity of cultures) Estimates of direct medical cost for different outcomes Estimates of cases, DALYs and medical cost prevented by
immunizing with PCV 7. Estimates of cost-effectiveness and incremental cost effectiveness
ratio of PCV-7 introduction
55
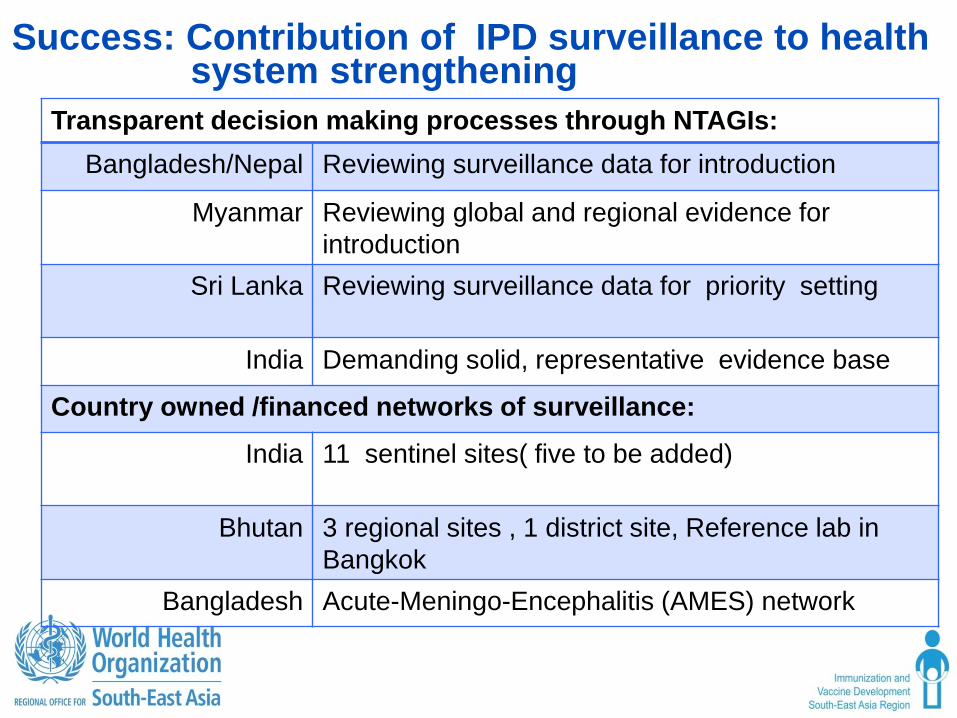
Transparent decision making processes through NTAGIs:Bangladesh/Nepal Reviewing surveillance data for introduction
Myanmar Reviewing global and regional evidence forintroduction
Sri Lanka Reviewing surveillance data for priority setting
India Demanding solid, representative evidence base
Country owned /financed networks of surveillance:
India 11 sentinel sites( five to be added)
Bhutan 3 regional sites , 1 district site, Reference lab in Bangkok
Bangladesh Acute-Meningo-Encephalitis (AMES) network
Success: Contribution of IPD surveillance to health system strengthening
66
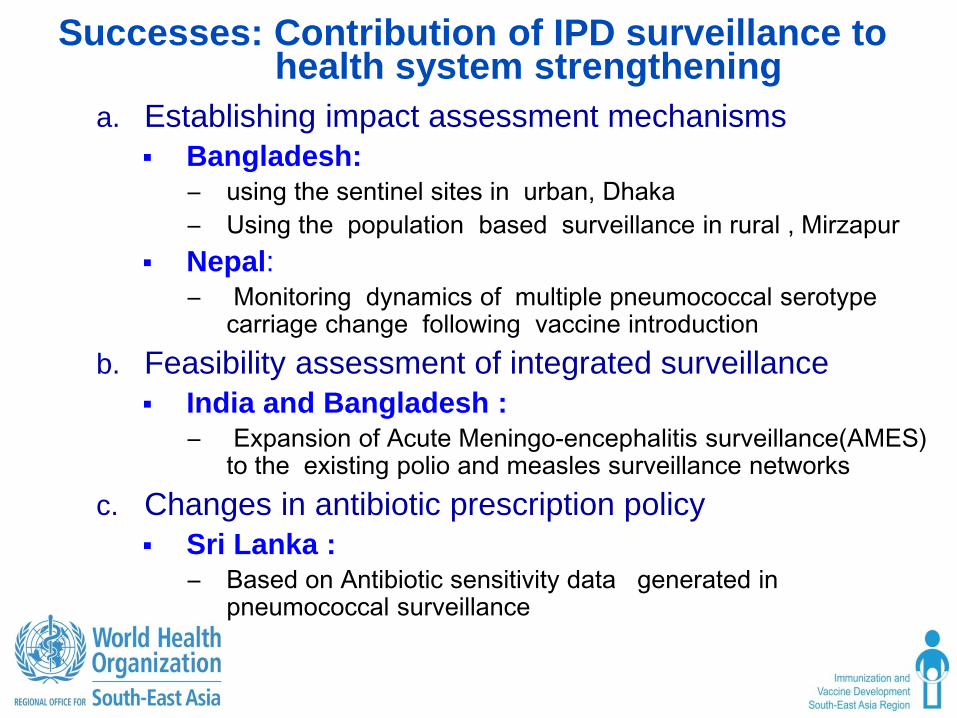
Successes: Contribution of IPD surveillance to health system strengthening
a. Establishing impact assessment mechanisms Bangladesh:
– using the sentinel sites in urban, Dhaka – Using the population based surveillance in rural , Mirzapur
Nepal:– Monitoring dynamics of multiple pneumococcal serotype
carriage change following vaccine introduction b. Feasibility assessment of integrated surveillance
India and Bangladesh :– Expansion of Acute Meningo-encephalitis surveillance(AMES)
to the existing polio and measles surveillance networks c. Changes in antibiotic prescription policy
Sri Lanka :– Based on Antibiotic sensitivity data generated in
pneumococcal surveillance

77
Challenges : Sustainability of the WHO supported network
a. Current dependence of surveillance sites on external funding
b. Ensuring full ownership of the national governments
c. Forging new alliances and partnerships for supplementation by countries
88
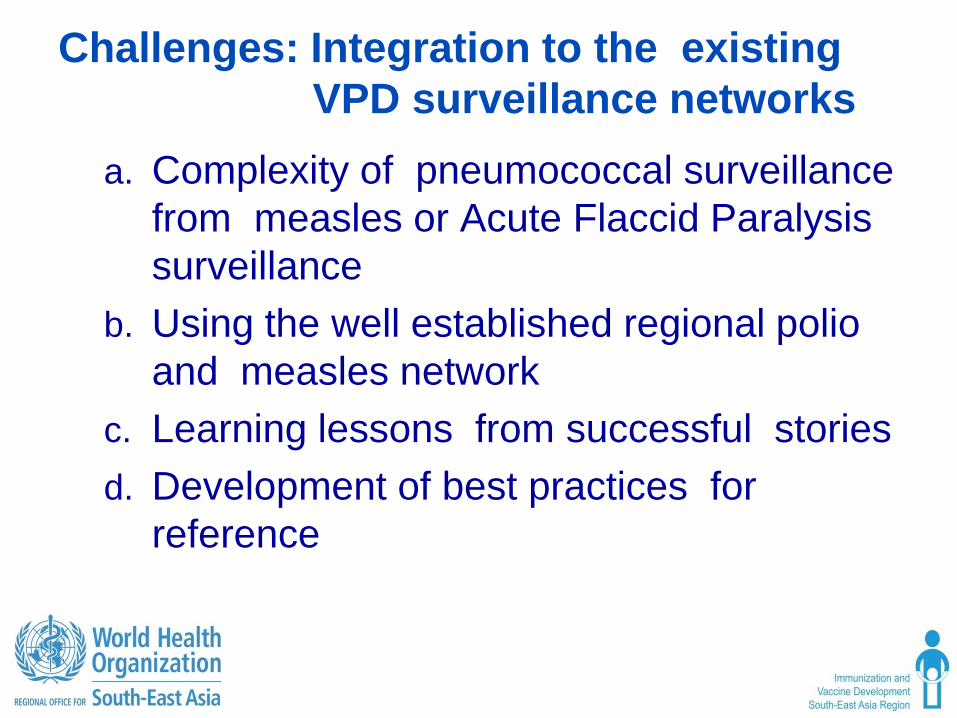
Challenges: Integration to the existing VPD surveillance networks
a. Complexity of pneumococcal surveillance from measles or Acute Flaccid Paralysis surveillance
b. Using the well established regional polio and measles network
c. Learning lessons from successful stories d. Development of best practices for
reference
99
Challenges: Sustaining surveillance in the post-introduction period
a. Sustainability for impact assessmentincluding sero-type replacement
b. A paradigm shift to post-introductionsurveillance objective
c. Supporting planned impact assessments inpost-introductory settings Bangladesh Nepal :
d. Establishing sero-type epidemiology inpost-introductory settings
1010
Challenges: Increasing the yield, improving quality and maximum use of data
a. Adopting high sensitive diagnostic methodsb. Using the reference laboratory for better yield
Difficulties with material transfer across borders Budgetary limitations
c. Where feasible establishment of PCR facility and capacity development
d. Standardization of surveillance practice , laboratory diagnosis and data management
e. Maximizing use of existing evidence for decision making
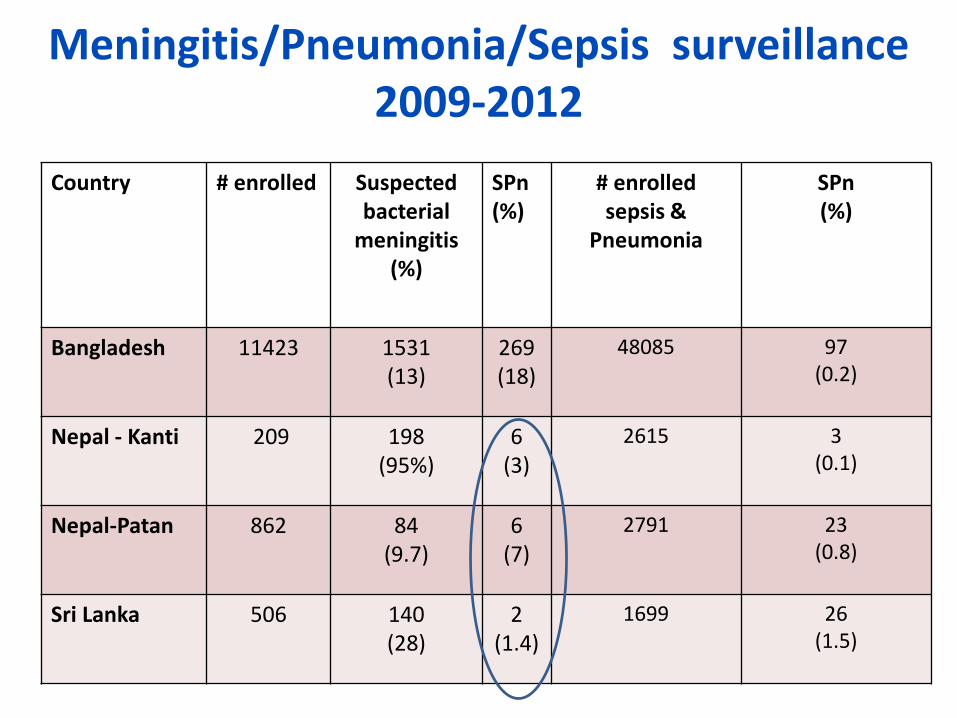
Meningitis/Pneumonia/Sepsis surveillance 2009-2012
Country # enrolled Suspectedbacterial
meningitis (%)
SPn(%)
# enrolled sepsis &
Pneumonia
SPn(%)
Bangladesh 11423 1531(13)
269(18)
48085 97(0.2)
Nepal - Kanti 209 198(95%)
6(3)
2615 3(0.1)
Nepal-Patan 862 84(9.7)
6(7)
2791 23(0.8)
Sri Lanka 506 140(28)
2(1.4)
1699 26(1.5)
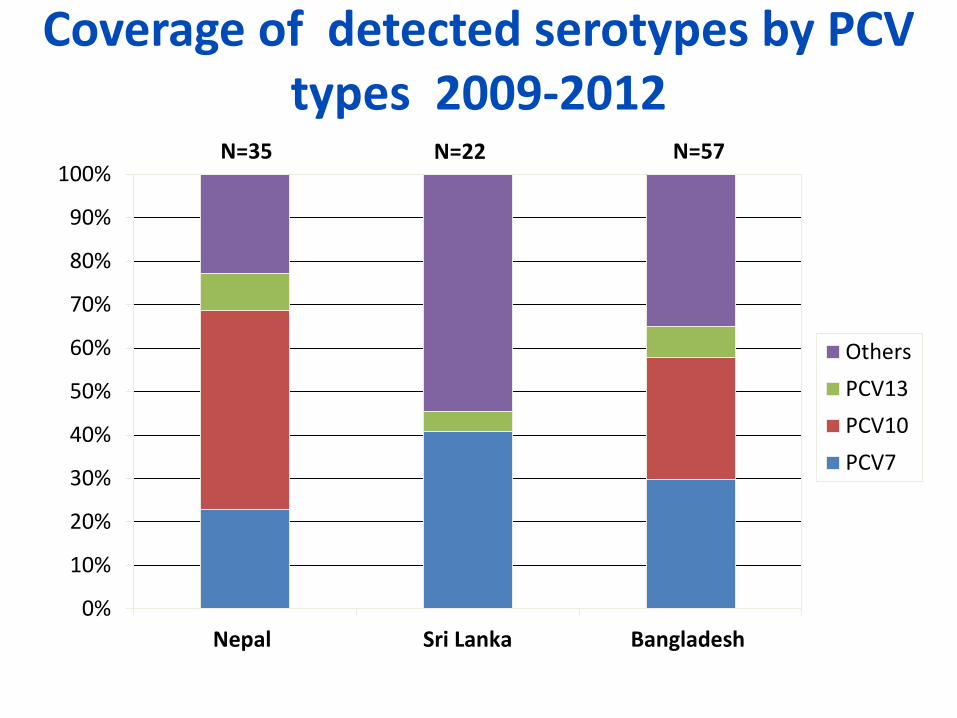
Coverage of detected serotypes by PCV types 2009-2012
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Nepal Sri Lanka Bangladesh
OthersPCV13PCV10PCV7
N=35 N=57N=22
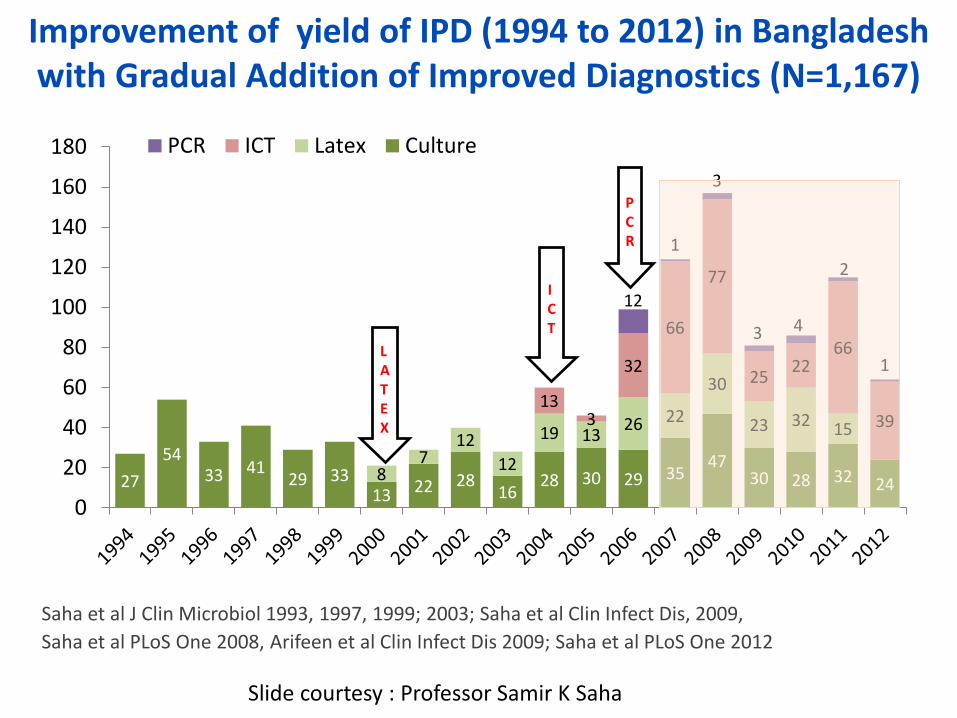
Improvement of yield of IPD (1994 to 2012) in Bangladesh with Gradual Addition of Improved Diagnostics (N=1,167)
2754
33 4129 33
13 22 2816
28 30 29 3547
30 28 32 2487
1212
19 13 26 22
30
23 32 1513
3
32
66
77
25 2266
39
12
1
3
3 4
2
1
0
20
40
60
80
100
120
140
160
180 PCR ICT Latex Culture
LATEX
ICT
PCR
Saha et al J Clin Microbiol 1993, 1997, 1999; 2003; Saha et al Clin Infect Dis, 2009, Saha et al PLoS One 2008, Arifeen et al Clin Infect Dis 2009; Saha et al PLoS One 2012
Slide courtesy : Professor Samir K Saha
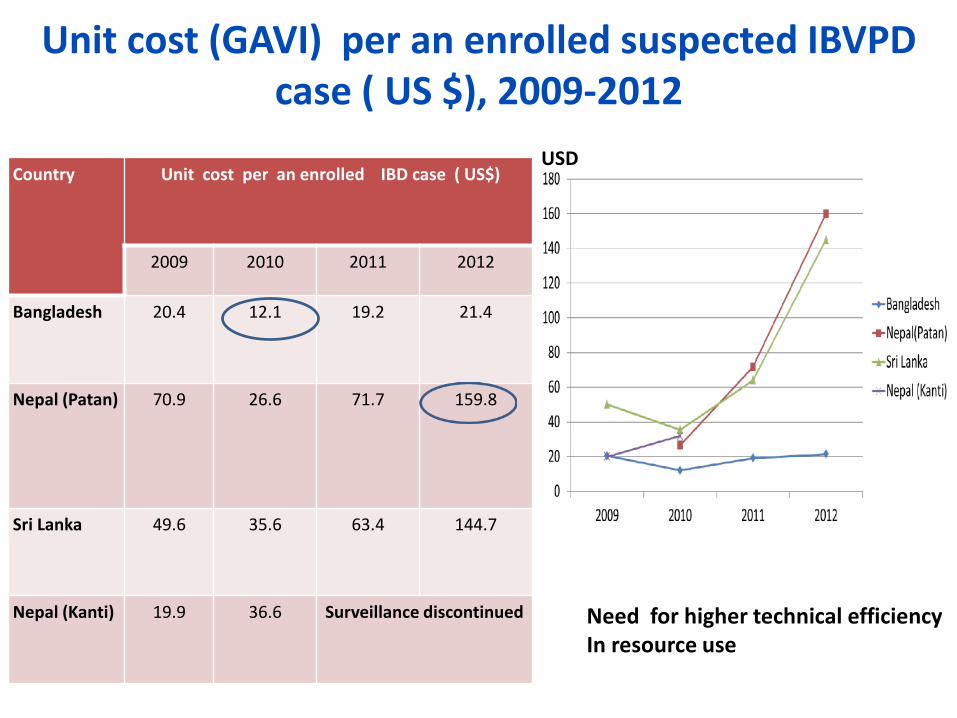
Unit cost (GAVI) per an enrolled suspected IBVPD case ( US $), 2009-2012
Country Unit cost per an enrolled IBD case ( US$)
2009 2010 2011 2012
Bangladesh 20.4 12.1 19.2 21.4
Nepal (Patan) 70.9 26.6 71.7 159.8
Sri Lanka 49.6 35.6 63.4 144.7
Nepal (Kanti) 19.9 36.6 Surveillance discontinued
USD
Need for higher technical efficiencyIn resource use
1515
Challenges : Supporting networks beyond the WHO support
1. Providing technical support to sentinel sites/laboratories beyond the WHO network
2. Standardization of surveillance , laboratory diagnosis and data management in sites beyond the WHO network
3. Reporting data from other networks to the WHO a. for regional and global decision making
1616
Conclusion1. At the beginning, lack of epidemiological and
economic evidence for priority setting and decision making in SEAR
2. Establishment of sentinel surveillance in the SEAR3. Vaccine introduction decision making using local,
regional and global evidence4. Usefulness of generated evidence, despite the
limited scope of sentinel surveillance5. Potential higher performance and usefulness of the
network with more enthusiastic national interests
1717
Thank you
Is the risk of abandoning the network Without being integrated into existing
in-country surveillance networks worth taking
after years of hard work ?