KUB IVP: intravenous pyelography Ultrasonography CT scan & MRI studies Renal scan Topics.
Upload
hisham-khatibCategory
view
93download
0
9/10/1438
1
Introduction to Renal CT Scan Protocol
Hisham AlKhatib, M.D.Consultant Radiologist
Common Clinical Problems in the Kidney • suspected renal calculus
• suspected renal infection
• r/o renal mass
• evaluate renal mass (cyst vs. tumor)
• stage renal cancer
• evaluate hematuria
• trauma
• ? renal artery stenosis
• ? renal vein thrombosis

9/10/1438
2
Patient preparation and technique
Before study
• Fasting 4 hours
• Creatinine level
• Pertinent history to decide the protocol needed
• Protocol design

9/10/1438
3
What are the risk factors for contrast induced acute
renal failure?
• preexisting renal failure
• diabetes mellitus
• dehydration
• cardiovascular disease and diuretics
• age over 75 years
• multiple myeloma (in dehydrated person)
• hypertension
• uricosuria
Scanning phases
• precontrast phase
• arterial
• corticomedullary phase
• nephrographic phase
• excretory phase

9/10/1438
4
Noncontrast scan
• baseline density measurements for evaluating renal masses or renal cysts
• urolithiasis, nephrolithiasis, renal calcifications
• in patients unable to receive intravenous contrast (i.e., contrast allergy, poor renal function, etc.).
Unenhanced CT of the Kidney
• Optimal Phase For Detection of-- Calculus- Cyst versus mass (HDRC versus solid tumor)- High density renal cyst- Identify location of the kidneys to define coverage

9/10/1438
5

9/10/1438
6
arterial phase
• is a short phase that occurs about 15–25 seconds after the start of intravenous contrast medium injection and is marked by maximum opacification of the renal arteries.
• The renal veins also usually opacify in the late arterial phase.

9/10/1438
7
corticomedullary (angionephrographic) phase
• The starts at about 30–40 seconds after the start of contrast medium injection.
• There is intense enhancement of the renal cortex due to preferential arterial flow to the cortex and glomerular filtration of the contrast material, while the medulla remains relatively less enhanced.
• This is also the best phase for maximum opacification of the renal veins.

9/10/1438
8
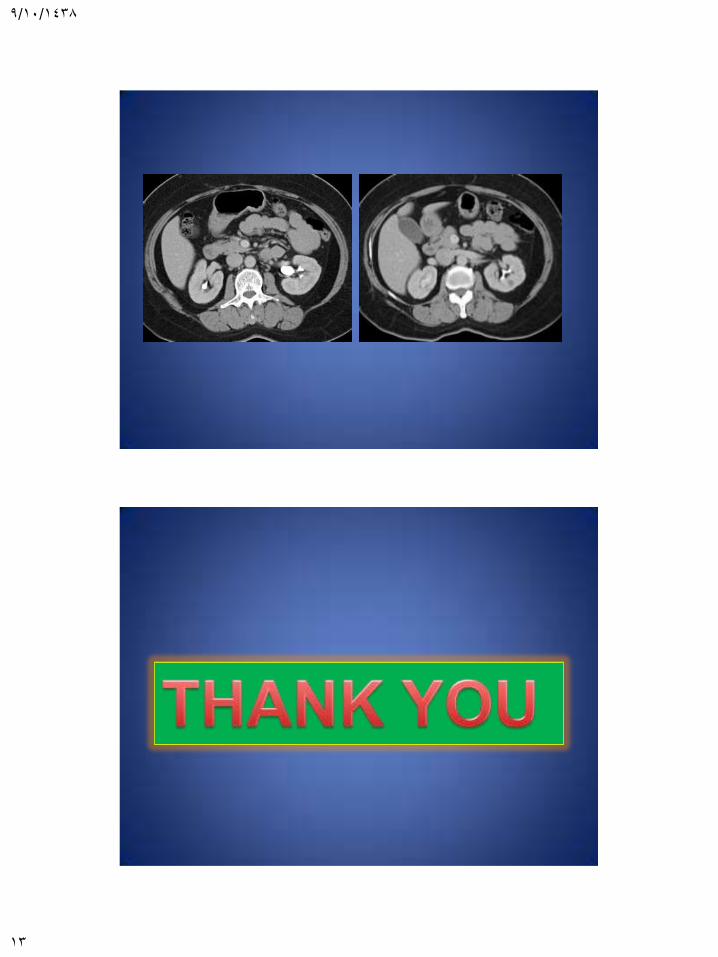
nephrographic phase
• begins at 80–120 seconds after the start of contrast medium injection.
• Tubular filtration of contrast material produces homogeneous enhancement of the renal parenchyma.
• the best phase for detection of subtle parenchymal lesions.
Nephrographic Phase
• (60-140 sec):
• Optimal Phase For Detection of-- Renal lesion detection- Pyelonephritis- Tumor invasion (renal vein/IVC)- Characterize lesion density- Perfusion changes- Renal vein or IVC thrombus

9/10/1438
9

9/10/1438
10
excretory or urographic phase
• starts at 180 seconds (3 minutes) after the start of contrast medium injection.
• Excretion of the contrast material allows opacification of the calyces, renal pelvises, and ureters, while the intensity of the nephrogram progressively declines.
• routinely acquire excretory phase images at 4–5 minutes to ensure opacification of the ureters.

9/10/1438
11
Excretory (pyelogram)Phase
• delayed scans ( 3-5 minutes)
• Contrast in calyces ,pelvis and ureters
• Excretory Phase Imaging is optimal for detecting;
– pathology in the renal pelvis or collecting system
– visualization of the renal parenchyma
– pathology in the ureter
CT Urography: Indications per Society of Uroradiology
•
- Painless gross and microscopic hematuria- Suspected transitional cell carcinoma- Follow up of transitional cell carcinoma- Recurrent UTI’s- Congenital anomalies- Renal trauma

9/10/1438
12
Ct urogram
Split Bolus Technique for CT Urography
- Scan without contrast from top of kidneys thru the base of the bladder- Inject 50 ml of iodixanol at 3 cc/sec- Wait 5 minutes- Inject 80 ml of iodixanol at 3 cc/sec- Wait 100 seconds and then scan the patient from the top of the kidneys thru the pelvis (combined nephrographic and excretory phase)
9/10/1438
13