
Introduction It is not too rare 3-5% year of newly diagnosed malignant tumours 4° most common cause...
67
Introduction It is not too rare 3-5% year of newly diagnosed malignant tumours 4° most common cause of cancer- related death in both sex.
-
Upload
hilary-bell -
Category
Documents
-
view
213 -
download
0
Transcript of Introduction It is not too rare 3-5% year of newly diagnosed malignant tumours 4° most common cause...

IntroductionIt is not too rare 3-5% year of newly
diagnosed malignant tumours
4° most common cause of cancer-related death in both sex.

BackgroundThe most important breakthrough in the management
of CUP is the identification of clinicopathologic subgroups to choose specific treatment protocols
20% of patients, the similarity of clinical presentation to those of known primary cancer at a similar stage as resulted in the identification of patients with favourable clinical and pathological future

Background80% of pts have an ufavourable outcome
future
Identification of reliable prognostic factors are currently investigated in many trials

Background Favourable risk (20%)
Unfavourable risk (80%)

Favourable groups
•Poorly differentiated carcinoma with midline nodal distribution
•Women with papillary adenocarcinoma of peritoneal cavity
•Poorly differentiated neuroendocrine carcinomas
•Women with adenocarcinoma involving only axillary lymph nodes

Favourable groups
•Squamous cell carcinoma involving cervical lymph nodes
•Men with blastic bone metastatic lesions from an adenocarcinoma with elevated serum prostate-specific antigen
•Isolated inguinal lymphadenopathy from squamous carcinoma
•Patients with a single small metastasis

Favourable highlights
Tailored treatment as applied in metastatic tumours of known primary
Similar prognosis and clinical course
High response rates to treatments
Observations of the metachronous appearance of the primary tumor

FavourableTreatable Subset of Patients with Cancer of Unknown Primary Site
Subset Histology Special diagnostic Tests Treatment
Women, isolated axillary adenopathy
Adenocarcinoma, PDC
ER/PR/HER2 stains, MR breast
Treat as stage II breast cancer
Women, peritoneal carcinomatosis
Adenocarcinoma, PDC
Serum CA 125 Treat as stage III ovarian cancer
Man, blastic bone metastasis Adenocarcinoma Serum, tumor PSA Treat as metastatic prostate cancer
Single metastasis Adenocarcinoma, PDC
PET scan Definitive local therapy+-chemotherapy
Young man, extragonadal GCT features
PDC Serum HCG, AFP Treat as poor prognosis germ cell tumor
Isolated cervical nodes Squamous ENT exam, PET scan Treat as locally advanced head/neck cancer
Isolated inguinal nodes Squamous Definitive local therapy +-chemotherapy
Neuroendocrine Tumors Well and Poor differentiated
Ocrteoscan,Chromogranine
Octreotide Analogs, Chemotherapy

PENTHEROUDAKIS et Al: Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
Pts with predominantly nodal disease Burden
Female patients had predominantly peritoneal malignant deposits of papillary serous adenocarcinomatous or undifferentiated carcinomatous histology

PENTHEROUDAKIS et Al: Acta Oncologica, 2005
Favourable
Chemotherapy for patients with two favourable subsets of CUP: Active, but how effective?
Pts characteristics
SUBSET

PENTHEROUDAKIS et Al:
Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
Univariate analysis

PENTHEROUDAKIS et Al: Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
Multivariate analysis
PENTHEROUDAKIS et Al: Acta Oncologica, 2005
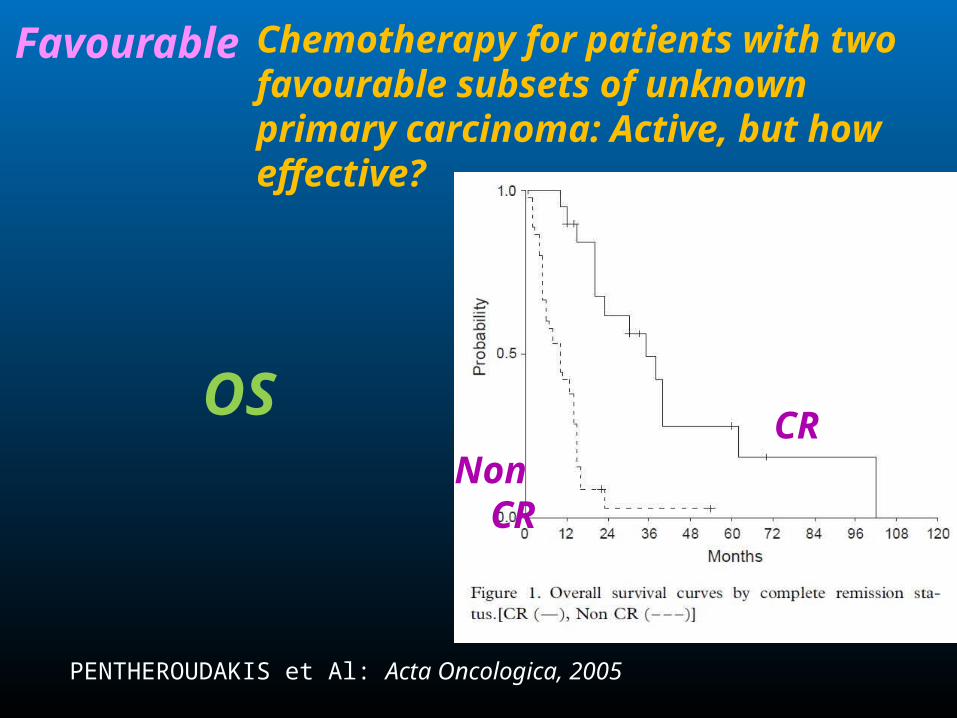
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
OSCR
Non CR

PENTHEROUDAKIS et Al: Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
OS and TTP in months

PENTHEROUDAKIS et Al: Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
Response to chemotherapy

PENTHEROUDAKIS et Al:
Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
ConclusionHighly predictive positive factors:
• N° of metastatic sites (1-3 Vs 4 or more)
• High serum CA125
• Normal serum CA 19-9
Complete response status was not included in the prognostic factor analysis, although its achievement predicted superior outcome

PENTHEROUDAKIS et Al:
Acta Oncologica, 2005
Favourable Chemotherapy for patients with two favourable subsets of unknown primary carcinoma: Active, but how effective?
Conclusion
• No prognostic significance In patient management with platinum-based regimens, sex, performance status,histological grade, and peritoneal or nodal disease group
• Trend for statistical significance for female sex and peritoneal disease

G. R. Varadhachary, et Al:
Lancet Oncol 2008
Favourable Carcinoma of unknown primary with a colon-cancer profile changing paradigm and emerging definitions
• CUP in association with a colon-cancer profile (CCP-CUP) is an example of an emerging, specific CUP subset that seems to benefit from a tailored approach
• CCP-CUP is identified by CK20 and CDX2- positive and CK7-negative immunohistochemistry
• CCP-CUP derive substantial benefit from the use of specific treatments developed for colon cancer
• Larger clinical trials are warranted to more definitely test this finding

G. R. Varadhachary, et Al:
Lancet Oncol 2008
Favourable Carcinoma of unknown primary with a colon-cancer profile changing paradigm and emerging definitions

G. R. Varadhachary, et Al:
JCO 2008
Favourable Molecular Profiling of CUPCorrelation With Clinical Evaluation

G. R. Varadhachary, et Al:
JCO 2008
Favourable Molecular Profiling of CUPCorrelation With Clinical Evaluation

Unfavourable groups
•Adenocarcinoma metastatic to the liver or other organs
•Malignant ascites from a nonpapillary adenocarcinoma
•Multiple cerebral metastases from an adenocarcinoma or squamous carcinoma
•Multiple lung/pleural metastases from an adenocarcinoma
•Multiple metastatic bone disease from an adenocarcinoma

Unfavourable highlights
• Regression or dormancy of the primary
• Development of early
•Aggressive biology
•Systemic metastases
• Resistance to the therapy

Unfavourable highlights
•Despite of biomolecular knowledge, this remain an eterogeneous group of pathology
•Majority (80%) of pts with CUP had unfavourable outcome features
•Identification of reliable prognostic indicators remain a challenge
•Many studies with multivariate analysis have try to discover prognostic factors, but without an international consensus
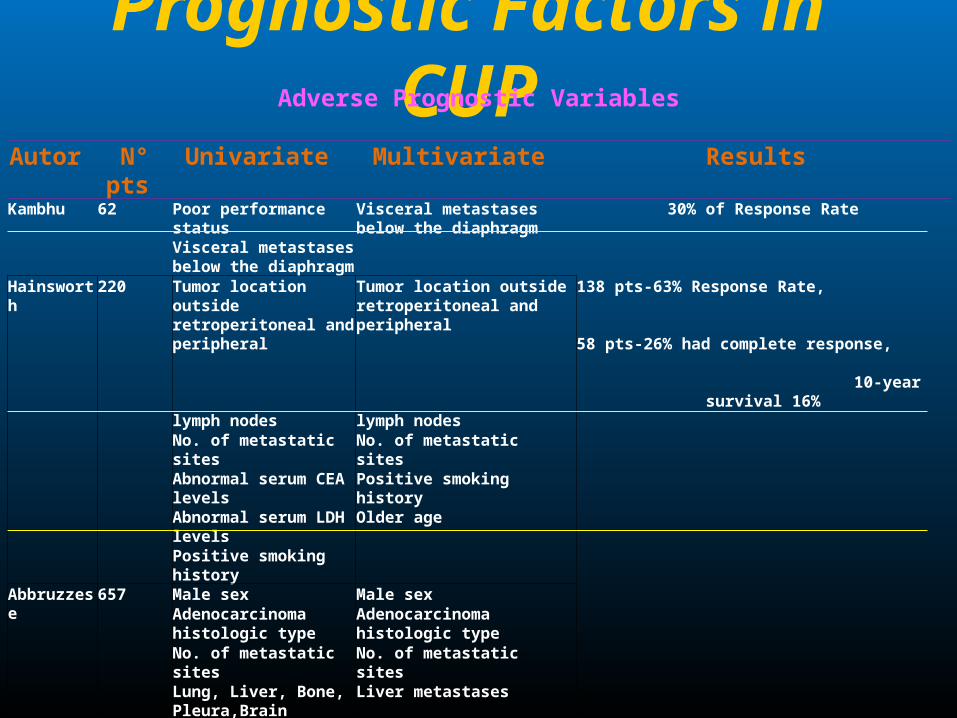
Prognostic Factors in CUP Adverse Prognostic Variables
Autor N° pts Univariate Multivariate Results Kambhu 62 Poor performance status Visceral metastases below the
diaphragm 30% of Response Rate
Visceral metastases below the diaphragm
Hainsworth 220 Tumor location outside retroperitoneal and peripheral
Tumor location outside retroperitoneal and peripheral
138 pts-63% Response Rate, 58 pts-26% had complete
response, 10-year survival 16%
lymph nodes lymph nodes No. of metastatic sites No. of metastatic sites Abnormal serum CEA levels Positive smoking history Abnormal serum LDH levels
Older age
Positive smoking history Abbruzzese 657 Male sex Male sex
Adenocarcinoma histologic type
Adenocarcinoma histologic type
No. of metastatic sites No. of metastatic sites Lung, Liver, Bone, Pleura,Brain metastases
Liver metastases
Van der Gaast
79 Poor performance status Poor performance status Good-prognosis WHO- 0 and alkaline phosphatase < 1.25 times the (N).
median survival >4 years. Intermediate-prognosis WHO 0<=1 or an alkaline
phosphatase level > or = 1.25 N. median survival 10 months
Poor-prognosis WHO>=1 and an alkaline phosphatase level > or = 1.25 N.
median survival 4 months
Adenocarcinoma histologic type
Serum alkaline phosphatase
Bone, Liver metastases Serum alkaline phosphatase
Serum AST

Prognostic Factors in CUPPrognostic Variables
Autor N° pts Prognostic Variables Results Lortholary 311 Male sex
PS 1Adenocarcinoma
No. of metastatic sites 1
adenocarcinoma: 164 cases; squamous cell carcinoma: 90 cases; neuro-endocrine tumor: 10 cases; and others: 20 cases primary carcinoma was found in only 6% of the cases
Median survival 9 monthsCuline 150 PS 1
Elevated LDH levels3 subgroups of patients with median survivals of 10.8, 6.0, and 2.4 months; Good-risk and poor-risk patients were identified, with median survivals of 11.7 months and 3.9 months, 1-year survival rates were 53% and 23%, respectively
Seve 317 PS 1Liver metastases
High comorbidity scoreLymphopenia
Elevated LDH serum levelsLow serum albumin levels
good-risk patients median survivals of 371 days poor-risk patients median survivals 103 days
Lenzi 337 Male sexAge 64 years
No. of metastatic sites 2
977 pts with CUP; PDC patients enjoyed better survival than PDA; The long median survival and chemotherapy
responsiveness of UPC patients with PDC and PDA could not be confirmed
Hess 1000 1 or 2 metastatic organ sites, nonadenocarcinoma , histology,
NO liver, bone, adrenal, or pleural metastases
Mediansurvival of the 10 subgroups ranged from 40 months
(95% confidence interval, 22–66 months), High risk group median survival 5 months

Kenneth R. Hess et Al: Clinical Cancer Research 1999
Classification and Regression Tree Analysis of 1000 Consecutive Patients with Unknown Primary Carcinoma
1000 pts
segregated into 10 groups with similar clinical features and survival
Unfavourable

Kenneth R. Hess et Al: Clinical Cancer Research 1999
Classification and Regression Tree Analysis of 1000 Consecutive Patients with Unknown Primary Carcinoma

Kenneth R. Hess et Al: Clinical Cancer Research 1999
Classification and Regression Tree Analysis of 1000 Consecutive Patients with Unknown Primary Carcinoma
OS

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With Carcinomas of an Unknown Primary Site
• Identification of subsets of patients with clinical and pathologic features requiring specific guidelines that may translate into prolonged survival
•Unfortunately, the majority of CUP (85%) do not fall into one of these favorable subsets
•The benefit of chemotherapy over best supportive care is still unknown
• The optimal chemotherapy remains to be determined

S Culine et Al: JCO, 2002
Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With CUP
• 150 pts
•CUP excluding favourable subset
•Results were validated in an independent
set of pts
Unfavourable

S Culine et Al: JCO, 2002
Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With CUP
Unfavourable
Pts characteristics

S Culine et Al: JCO, 2002
Unfavourable
Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With CUP
Univariate analysis for survival

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With CUP

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With CUP

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With Carcinomas of an Unknown Primary Site
Univariate analysis for survival

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With Carcinomas of an Unknown Primary Site

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With Carcinomas of an Unknown Primary Site
Prognostic Model

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With Carcinomas of an Unknown Primary Site
OS in Reference Population

S Culine et Al: JCO, 2002
Unfavourable Development and Validation of a Prognostic Model to Predict the Length of Survival in Patients With Carcinomas of an Unknown Primary Site
OS in Validation Population

P. Seve et Al: Cancer, march 2006
The Influence of Comorbidities, Age, and Performance Status on the Prognosis and Treatment of Patients with Metastatic Carcinomas of Unknown Primary Site
OS
evaluated at cancer center
NOT evaluated at cancer center

P. Seve et Al: Cancer, march 2006
The Influence of Comorbidities, Age, and Performance Status on the Prognosis and Treatment of Patients with Metastatic Carcinomas of Unknown Primary Site

P. Seve et Al: Cancer, September 2006
Unfavourable
Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site

P. Seve et Al: Cancer, September 2006
Unfavourable
Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site

P. Seve et Al: Cancer, September 2006
Unfavourable Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site

P. Seve et Al: Cancer,
September 2006
Unfavourable Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site
Multivariate AnalisysOf OS

P. Seve et Al: Cancer, September 2006
Unfavourable Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site
Prognostic Model
Good No liver Metastases
Poor Liver Metastases
and Low albumin
or Low albumin
61 39 371
122 12 108
Prognostic Group
Prognosticvariable
Survival,% Survival (months)
N° pts 1yr Median

P. Seve et Al: Cancer, September 2006
Favourable Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site
OSIn Reference pts
Good risk
Poor risk

P. Seve et Al: Cancer, September 2006
Favourable Low Serum Albumin Levels and Liver Metastasis Are Powerful Prognostic Markers for Survival in Patients With Carcinomas of Unknown Primary Site
Good risk
Poor risk
OSIn Independent pts

M. Kodaira, et Al:
Annals of Oncology 2009
Bone metastasis and poor performance status are prognostic factors for survival of CUP in patients treated with systematic chemotherapy
Pts characteristics

M. Kodaira, et Al:
Annals of Oncology 2009
Treatments Results
Bone metastasis and poor performance status are prognostic factors for survival of CUP in patients treated with systematic chemotherapy

M. Kodaira, et Al:
Annals of Oncology 2009
Bone metastasis and poor performance status are prognostic factors for survival of CUP in patients treated with systematic chemotherapy
Univariate e
Multivariate analisys

M. Kodaira, et Al:
Annals of Oncology 2009
Bone metastasis and poor performance status are prognostic factors for survival of CUP in patients treated with systematic chemotherapy
Prognostic Model

But the chemotherapy regimens influences the
outcome of CUP?

D. E. Saad, et Al:
Oncology/Hematology 2000
Prognostic stratification in UPC: a role for assessing the value of conventional-dose and high-dose chemotherapy for CUP

D. E. Saad, et Al:
Oncology/Hematology 2000
Prognostic stratification in UPC: a role for assessing the value of conventional-dose and high-dose chemotherapy for CUP

D. E. Saad, et Al:
Oncology/Hematology 2000
Prognostic stratification in UPC: a role for assessing the value of conventional-dose and high-dose chemotherapy for CUP
• No chemotherapy regimen can be considered standard in the treatment of CUP without features of the extragonadal germ cell syndrome or of the other favorable subgroups
• Trials performed to date had only active treatments in their arms, and therefore no definitive conclusions can be drawn regarding the superiority of active therapy versus best supportive care

V. Golfinopoulos, et Al:
Cancer Treatment Reviews 2009
Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis
• Data sources: PubMed and the Cochrane Library Central Registry of Controlled Trials
• Randomized controlled trials comparing
• No favourable subset
• Regimens are divided in : platinum, taxane, both, or neither; non-platinum/non-taxane.
• No type of chemotherapy has been solidly proven to prolong survival in patients with CUP

V. Golfinopoulos, et Al:
Cancer Treatment Reviews 2009
Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis

V. Golfinopoulos, et Al:
Cancer Treatment Reviews 2009
Comparative survival with diverse chemotherapy regimens for cancer of unknown primary site: Multiple-treatments meta-analysis
CONCLUSION• No trials compared systemic treatment to best supportive
care
• All arms referred to chemotherapy
• Multiple-treatments meta-analysis showed no significant benefit
• Point estimates of hazard ratios favored platinum, taxane,or both (hazard ratios 0.69, 0.66, and 0.81, respectively, as
compared with monotherapy with an agent other than platinum or taxane)

Molecular assignment of tissue of origin in cancer of unknown primary may not predict response to therapy or outcome: A systematic literature review
Pentheroudakis, et Al:
Cancer Treatment Reviews 2009

Molecular assignment of tissue of origin in cancer of unknown primary may not predict response to therapy or outcome: A systematic literature review
Pentheroudakis, et Al:
Cancer Treatment Reviews 2009

Molecular assignment of tissue of origin in cancer of unknown primary may not predict response to therapy or outcome: A systematic literature review
Pentheroudakis, et Al:
Cancer Treatment Reviews 2009

Molecular assignment of tissue of origin in cancer of unknown primary may not predict response to therapy or outcome: A systematic literature review
Pentheroudakis, et Al:
Cancer Treatment Reviews 2009
Chemotherapy activity and pts Outcome in CUP and Metastatic tumors
of KNOWN primary

CONCLUSION• Despite advances in molecular
immunohistochemistry and imaging technology, the diagnosis and therapy of CUP remains a challenge
• Major advance in the field over the last decade was made by identifying the clinicopathological subsets of CUP patients with a more favourable prognosis.

CONCLUSION• This allowed for tailoring of the therapeutic strategy
towards more intensive modalities for good risk groups
• Patients with midline nodal metastases as well as women with non-mucinous peritoneal carcinomatosis are thought to have entities equivalent to extragonadal germ cell cancer and ovarian cancer may respond to systemic platinum-based chemotherapy and occasionally enjoy long-term survival

CONCLUSION• Most patients received platinum based
chemotherapy, commonly coupled with a taxane. Response rate 50%, among the highest reported to date, reproduced by a few authors using platinum-taxane regimens
• No prospective studies or meta-analysis of prognostic factors for CUP have been published


















