Introduction Bio-products Roche Bio-V2.pdfIntroduction Bio-products 28/01/2013 1 Dr. Mohammed Saleem...
98
Introduction Bio-products 28/01/2013 1 Dr. Mohammed Saleem P. O. Box: 836 Amman 11821 Jordan Tel.: 00962-6-5512561/2 Fax: 00962-6-5512563 [email protected] www.sipsmena.com Science forum for Research Studies & Consultancies (SIPS)
Transcript of Introduction Bio-products Roche Bio-V2.pdfIntroduction Bio-products 28/01/2013 1 Dr. Mohammed Saleem...

Introduction Bio-products
28/01/2013 1
Dr. Mohammed Saleem
P. O. Box: 836 Amman 11821 Jordan
Tel.: 00962-6-5512561/2
Fax: 00962-6-5512563
www.sipsmena.com
Science forum for Research Studies & Consultancies
(SIPS)

2.4 2.6 2.8 3.2 3.5 4.1
34
30
27
24
22
5.3
4.7 4.3
3.3 3.7 5.4
4.7 4.2
3.2 3.6
7.2
4.6 5.1 5.7 6.4 1.5 1.7 2.2 2.2 2.3
2.9 1.5 1.8
2.2 2.5 2.8
3.0
0%
5%
10%
15%
20%
25%
30%
-
5
10
15
20
25
30
35
2006 2007 2008 2009 2010 2011 2012F 2013F 2014F 2015F
Source: IMS Global Market Prognosis, Forecasted updated Mar.2012 *Marked countries pharma market size is estimated, based on trade statistics to represent 23% of MENA total by 2016
2016F
US
$ B
illi
on
s
Bahrain
* Qatar
* Oman
* Yemen
* Syria
* Iraq *
Jordan
Libya *
Lebanon
Tunisia
Morocco
Iran *
United Arab
Emirates Israel *
Egypt
Algeria
Saudi
Arabia
MENA
Growth
Global
Growth
20
18
16 14
12
10
MENA market size has grown by $10 bn in past 5 years, by doubling its size and forecasted to grow another $14bn until 2016…
Prospects for MENA
Saudi, Algeria, Egypt and UAE represent ca.60% of MENA market
MENA Pharma Market Size (US$Bn) & Growth%

Source: IMS MIDAS, 12/2011
(It includes old generation insulins which are unlikely to be targeted by biosimilar players)

0%
2%
4%
6%
8%
10%
12%
14%
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Oncology
Enzyme
Epos
Vaccine
MS
Insulin
Other Biologics
RA/Crohn/Psoraisis
Source: Brogan Inc. Pay Direct Drug Plan Database
Biologics are major growth items within selected therapy areas
Share of Annual
Expenditure

0
Source: Brogan Inc. Pay Direct Drug Plan Database
1
2
3
4
5
6
0M
1M
2M
3M
4M
5M
6M
Patients are starting on biologics earlier in life & staying on them through old age
2001 2011 2021
$/ Claimant Population (M)
Age
Group

Chart notes Biologics include single identified components, whole cells, and include some forms of polymers. They can be purified from human, animal, plant or micro-organism sources. Biologics can be produced by recombinant DNA technology or chemically synthesized. Biosimilar products are biologic products approved in a country which has an abbreviated approval process for biologic products that reference an originator biologic in the regulatory submission.
• Biologics will account for an increased share of spending by 2016, as important clinical advances continue to emerge from research, and patients around the world are treated.
• Spending on biosimilars will increase from $693Mn in 2011 to $4-6Bn by 2016, which represents 2% of biologic spending.
• Adoption is expected to remain modest through 2016, largely because most biologic medicines will stay protected by patents or market exclusivity in many countries.
2016
2011
2006
Source: IMS Consulting Group, May 2012
Global Biologics Spending
Biologics usage will drive many therapeutic areas
$93Bn
$157Bn
$200-210Bn
99.98
%
Total Biologics Market
The Global Use of Medicines: Outlook Through 2016
Report by the IMS Institute for Healthcare Informatics 7
GLOBAL SPENDING ON MEDICINES

Treatment will be transformed by new and existing mechanisms
• Between 32-37 innovative products are expected to be launched per year over the next five years.
• These developments include new mechanisms of action in several disease states such as Alzheimer’s, autoimmune diseases and various types of cancer, which have the potential to transform disease treatment, though not every therapy will become available or achieve its ultimate clinical aims.
• There are also further developments in areas of research where some therapies have already launched including hepatitis C, multiple sclerosis and prostate cancer, which offer the potential to deliver better efficacy, safety or convenient administration.
Selected Product Launches 2012-2016 DISEASE AREA EXISTING MECHANISMS NEW MECHANISMS
Autoimmune • JAK inhibitor (tofacitinib )
Alzheimer’s disease • MAb (bapineuzumab, solanezumab)
The Global Use of Medicines: Outlook Through 2016
Report by the IMS Institute for Healthcare Informatics 9
Breast cancer • MAb (pertuzumab, trastuzumab emtansine)
Diabetes • GLP-1 (albiglutide, dulaglutide, lixisenatide)
• DPP IV (anagliptin, gemigliptin, teneligliptin, trelagliptin)
• SGLT inhibitor (canagliflozin, dapagliflozin, empagliflozin, ipragliflozin, tofogliflozin)
Hepatitis C • NS3/4A proteinase inhibitor (asunaprevir, BI 201335, simeprevir)
• NS5A inhibitor (daclatasvir)
HIV • Reverse transcriptase inhibitor (elvitegravir + emtricitabine + tenofovir disoproxil + cobicistat)
Lupus • Fusion protein (atacicept) • MAb (epratuzumab, tabalumab)
Melanoma • BRAF kinase inhibitor (dabrafenib) • Oncolytic HSV vector (talimogene laherparepvec)*
Multiple sclerosis • Immunomodulator (laquinimod, teriflunomide)
• MAb (daclizumab, ocrelizumab)
Ovarian cancer • Folate-targeted drug conjugate (vintafolide)
• Kinase inhibitor (nintedanib)
Obesity • Appetite suppressants (lorcaserin, phentermine/topiramate)
Thrombosis/ ACS
• Blood clotting factor Xa inhibitor (idraparinux sodium, otamixaban)
Prostate cancer • Antiandrogen (enzalutamide/MDV3100) • Kinase inhibitor (cabozantanib) • Radiotherapeutic (radium-223 chloride)
Chart notes Table includes selected not yet launched New Molecular Entities (NME) expected to be launched by 2016. An NME is the first commercial launch of a novel therapeutic entity. Abbreviations: JAK: janus-like kinase inhibitor; MAb: monocloncal antibody; GLP-1: glucagon-like peptide-1; DPPIV: dipeptidyl peptidase-IV inhibitor; SGLT: sodium-glucose cotransporter inhibitor; HSV: 5-HT2C: immunotherapeutic cancer vaccine, 5-hydroxytryptamine 2C; Xa: Xa coagulation factor inhibitor; NS5A: non-structural protein 5A; HSV: herpes simplex virus; ACS: acute coronary syndrome.
Source: IMS Institute for Healthcare Informatics, May 2012
TRANSFORMATIONS IN DISEASE TREATMENT

PROTEINS!

The Building Blocks of Proteins:
AMINO ACIDS!

R-groups affect Reactivity & Solubility

Amino Acids as Buffers:

How do Amino Acids Link Together to Form Proteins?

DIRECTIONALITY!

Protein Primary Structure
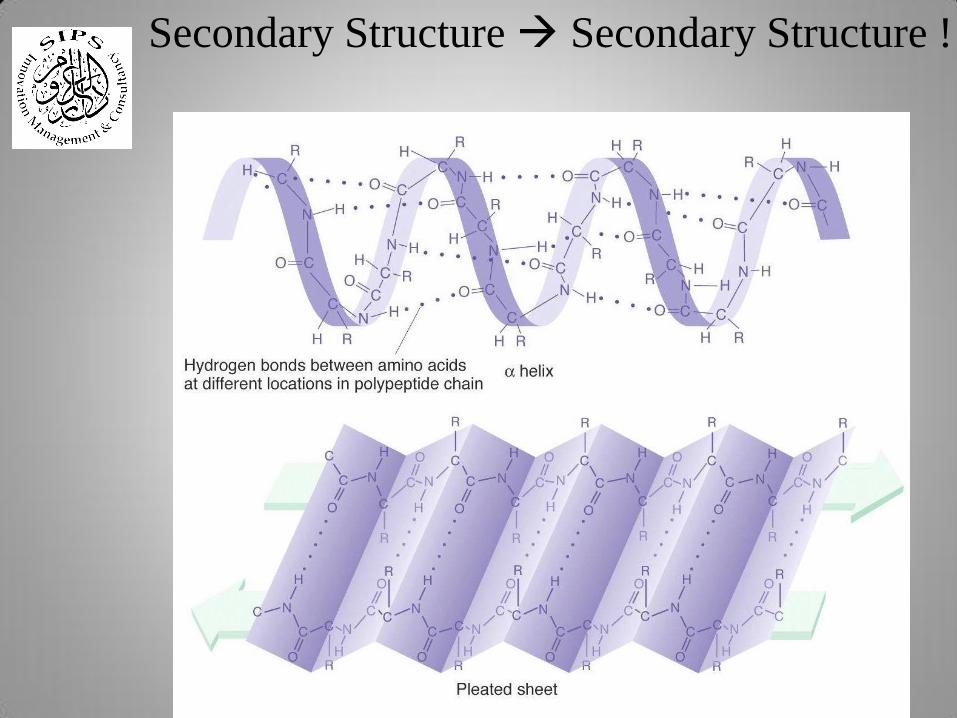
Hydrogen bonding!
Secondary Structure Secondary Structure !

Secondary Structure Tertiary Structure

Tertiary Structure Quaternary Structure (in some proteins)
Hemoglobin’s Chemical Formula: C3032H4816O872N780S8Fe4

Change in primary structure = Change in function!
Mutated Cells

Change in
structure =
Change in
function!

When Protein’s Go Awry = PRIONS!
Normal Misfolded (Prion)
• Scrapie
• Kuru
• Mad Cow

• Insulin (diabetes)
• Interferon b (relapsing MS)
• Interferon g (granulomatous)
• TPA (heart attack)
Protein Pharmaceuticals

• Actimmune (If g)
• Activase (TPA)
• BeneFix (F IX)
• Betaseron (If b)
• Humulin
• Novolin
• Pegademase (AD)
• Epogen
• Regranex (PDGF)
• Novoseven (F VIIa)
• Intron-A
• Neupogen
• Pulmozyme
• Infergen
Protein Pharmaceuticals

Protein Pharmaceuticals
• 77 FDA approved protein drugs
• 66/77 are recombinant proteins
• Protein pharmaceutical sales currently approach $25
billion/yr
• End of 2013 they are expected to exceed $60 billion/yr

Poorly characterized
• Traditional vaccines
• Whole blood
• Blood derivatives
• Blood components
• Allergenic extracts
• Stem cells
• Somatic cell and gene therapies
• Toxins
Well-characterized
• Natural proteins
• rDNA-derived proteins
• Monoclonal antibodies
• rDNA-derived vaccines
Types of Biological Drugs
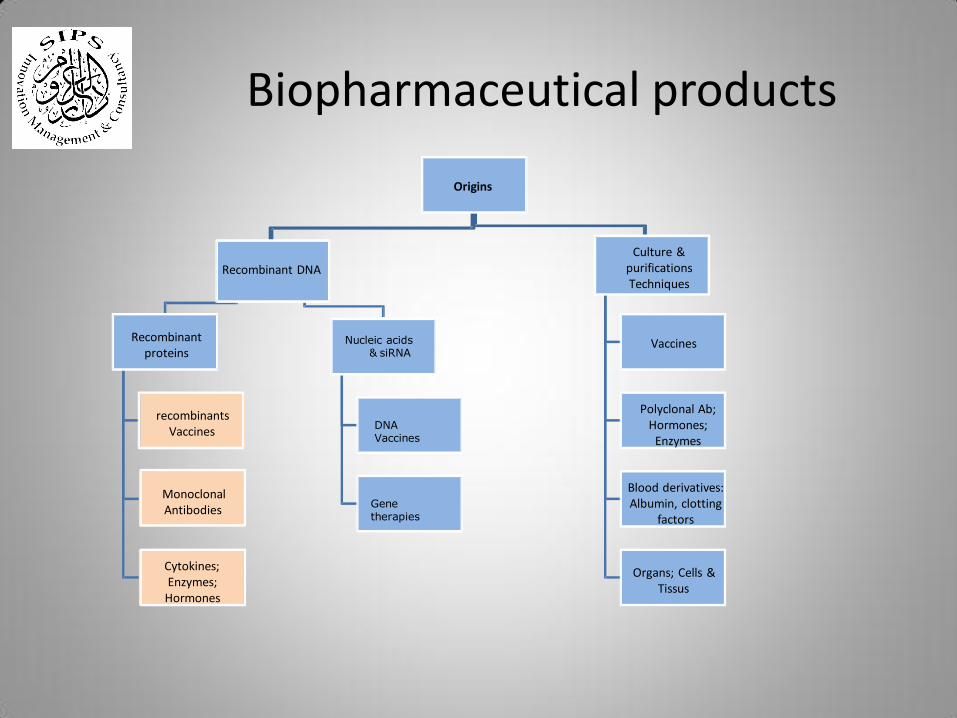
Origins
Recombinant DNA
Recombinant proteins
recombinants Vaccines
Monoclonal Antibodies
Cytokines; Enzymes;
Hormones
Nucleic acids
& siRNA
DNA
Vaccines
Gene
therapies
Culture & purifications Techniques
Vaccines
Polyclonal Ab; Hormones;
Enzymes
Blood derivatives: Albumin, clotting
factors
Organs; Cells & Tissus
Biopharmaceutical products

Proteins have expected:
• Size, charge, hydrophobicity
• Correct folding (S-S bonds)
• Subunits
• Glycosylation
• Bioactivity
& Unexpected:
• Aggregation (side effects)
• Incorrect folding
• Amino acid modifications
– ox, deam, cys • Truncation, proteolysis
Statin
Therapeutic protein ~5,000 - 300,000 Da
~400 Da *
x
Chemical Vs Biological Drugs

Biological
drugs
Size
Structure
Stability
Modification
Manufacturing
Characterization
Large
Complex
Unstable
Many
options
Unique line of living cells
Impossible to make identical copy
Impossible to characterize fully
due to a mixture of related
molecules
Qu
alit
y A
ttri
bu
tes
Chemical drugs
Small
Simple
Stable
Well-defined
Predictable chemical process
Identical copy can be made
Easy to fully
characterize
Chemical Vs Biological Drugs

mAbs Glyco-Protein Polypeptide Chemical
InfliximAb Epoetin Insulin Simvastatin
Immunologicals
Virus Like
~144,190 Da ~34,000 Da ~5,808 Da ~419 Da ~22,000,000 Da
Complexity of Structures
Chemical Vs Biological Drugs

O
H
O
O
HO O
O
H
O
H O
HO O
Simvastatin
Simvastatin Acid
Structural Changes mAbs
Chemical Vs Biological Drugs

O
O
O
HO O
H O
O
O
H
H
O
O
H
Simvastatin-
Closed Lactone Ring
Simvastatin Acid-
Opened Lactone Ring
Identification of Structural Changes
Chemical Vs Biological Drugs

O 2. 1.25
O O
H
2.0 HO O
H
5.97
H
5.50
H
4.11 1.53
1.18.52
9 2.33
2.13
1.53
1.16
1.16
4.25 1.64
1.29
2.01
0.96
3.63
2.5
5
53
5.47
0 1 2 3 4 5 6 PPM
O
O
O
HO O
H
O
O
OH
HO O
H
O 2.53
O
OH
11.0
HO
3.54
O
H
H
5.97
H
5.50
H
4.11 1.53
1.851.29
1.25
2.33
2.13
1.29
1.16
1.16
1.29
1.64
1.29
1.44
0.96
2.38 2.0
5.47 0 2 4 6
PPM 8 10 12
1H-NMR
1 H-NMR
Analytical Identification of Structural Changes
Chemical Vs Biological Drugs

O
O O
HO O
172.
0
H
40.9
145.
3
73.
7
35.
9 22.0
412.29.
0
128.
0
124.
7
24.
5
31.
5
174.0
43.3
25.
1 133.
6
33.
2
18.
0
20.
2
71.
6 31.
0
44.
1
8.4
66.
7
43.
4
0 20 40 60 80 100 PPM
12
0
14
0
16
0
18
0
174.
0
O
O
OH 24.1
HO
66.
7
O
H
40.9
73.7
25.1
145.3
35.9
41.922.
0
128.
0
124.
7
30.5
31.5
133.
6
29.2
18.0
43.3
20.2
31.0
22.0
37.3
8.4
177.
0
43.4
0 20 40 60 80 100 PPM
120 140 160 180
O
O
O
HO O
H
O
O
OH
HO O
H
13C-NMR
13C-NMR
Analytical Identification of Structural Changes
Chemical Vs Biological Drugs

•Monoclonal antibodies are complex molecules
– High level of microheterogeneity, there will always be
differences
– The mode of action is complex and may involve contributions
from multiple mechanisms
– Even small differences may have significant effects.
–Need to combine physicochemical results with functional
assays (e.g. antigen-antibody binding assays and cell-based
assays) and the qualification in preclinical and clinical studies
Increasing complexity of Bioproducts

Theoretical Molecular Mass ~150,000 Da
–>200 AA residues light chain
–>450 AA residues heavy chain
–More than 1 predominant mass
Glycosylated
Complex Structure Biantennary
+/- Core Fucose
Sialylation Disulfide Bonds: – Contain Inter and intra-chain bonds
– C-terminal Lysine Heterogeneity
– Additional Post-translations
Modification
– (deamidation, methionine oxidation,
etc.)
Heterogeneous in both size and
charge
Increasing complexity of Bioproducts

1. Binding to antigen : Inhibition of binding of ligand to receptor
2. Binding to cellular receptors
Fc-gamma-RI Fc-gamma-RII Fc-gamma-RIII FcRn
3. Complement binding
4. Relative contribution of effector functions mostly unknown
Multi-functionality of Monoclonal Antibodies (mAbs)

Subtle changes to the structure can result in profound effects on the activity
The structure of specified molecule is related to the function (biological activity) and susceptible to:
- Genetic Instability of Cell Banks
- Issues within Fermentation and Purification
Post Translational Modifications
Product Degradation or Modification
Purity
Biological activities
Immunogenicity
Multi-functionality of Monoclonal Antibodies (mAbs)
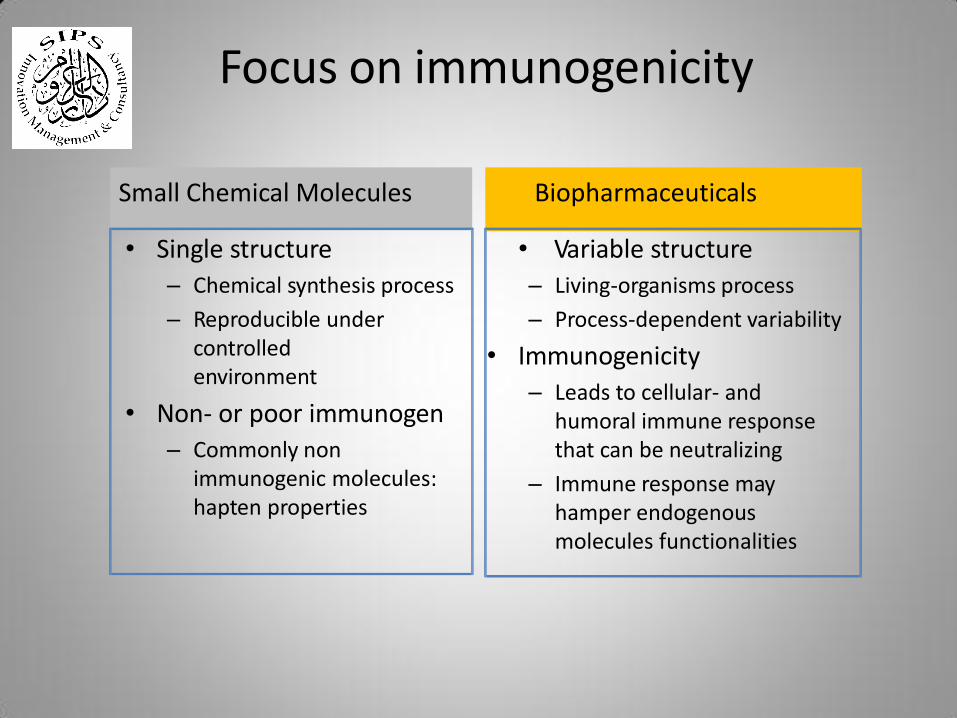
Focus on immunogenicity
Small Chemical Molecules Biopharmaceuticals
• Variable structure
– Living-organisms process
– Process-dependent variability
• Immunogenicity
– Leads to cellular- and
humoral immune response
that can be neutralizing
– Immune response may
hamper endogenous
molecules functionalities
• Single structure
– Chemical synthesis process
– Reproducible under controlled
environment
• Non- or poor immunogen
– Commonly non
immunogenic molecules: hapten properties

Consequences of immunogenicity
- Clinical consequences include loss or reduction of efficacy, local reactions, and systemic reactions - Response can be regained by introduction of an alternative biological
agent of the same or different class (Yanai & Hanauer Am J Gastroenterol. 2011; 106:685-698)
- The risk of immunogenicity needs to be considered individually for each
indication/patient population - Serum antibodies can be used as markers to monitor the safety of
therapeutic biopharmaceuticals
- Acute and delayed consequences - Pathogenic mechanisms of Mabs-related adverse reactions include
hypersensitivity, IgE- and non-IgE-mediated events and cytokine release syndrome (Maggi et al. Expert Rev Clin Immunol. 2011; 7:55-63)
- Autoimmunity (EPO > Pure² Red-Cell Aplasia)…

Immunogenicity assessment
- Important parameters:
- Aggregation
- Protein structure (secondary modifications)
- Excipients and impurities
- Prediction:
- Unwanted immune responses are dependent on the molecule,
manufacturing process, treatment duration and individual patient’s
susceptibility
- In-silico modeling may help to identify T-cell epitopes but does not predict
immunogenicity
- The incidence of immune response is too low to be fully identified during clinical
studies; therefore…
- Systematic post-marketing monitoring may be necessary to capture clinical signs
that could be related to immunogenicity

• Continue benefit risk assessment
• Risk assessment, pharmacovigilance, and post-marketing studies are essential
Immunogenicity

• Immunogenicity can not be fully determine due to limitations of clinical trials
• May not be detected during preapproval
clinical testing – Evaluated through postmarketing surveillance or
studies
Immunogenicity

Immunogenicity
• Immunogenicity is influenced by many factors such as the nature of the active substance and product- and process related impurities
•An immune response to the product may have a
significant impact on its clinical safety and efficacy – Irrelevant for therapy, to serious and life-threatening

What are Biopharmaceuticals
• Biopharmaceuticals are defined as pharmaceuticals manufactured by biotechnology methods, with the products having biological sources, usually involving live organisms or their active components
• Biopharmaceuticals are protein or nucleic acid based pharmaceuticals (substance used for therapeutic or in vivo diagnostic purpose), which are produced by mean other than direct extraction from a native biological source.
43
• The methods and techniques that involve the use of living organisms (such as cells, bacteria, yeast and others) are tools to perform specific industrial or manufacturing process are called biotechnology
• Pharmaceutical Biotechnology will continue to provide new breakthroughs in medical research in the years to come, leading to treatment in field which have previously eluded us (including AIDS, cancer asthma, Parkinson’s disease, Alzheimer disease)
44
Pharmaceutical Biotechnology

Pharmaceutical Biotechnology
• Biotechnology offers better product-targeting for specific diseases and patient groups, through the use of innovative technologies, in particular, genetics. Examples include, amongst others, treatment for rare diseases and cancers.
• Some products are not naturally created in sufficient quantities for therapeutics purpose.
• Biotechnology makes large-scale production of existing substances possible, for example, insulin in the field of diabetes treatment
45

Majority of Biotech Products Use Living Cells to Produce a Protein Product
• Insert gene encoding the protein of interest
• Cells require proper conditions for optimal growth (temp, pH, oxygen, feeds, etc.)
• Culture and fermentation can take weeks
• Complex Purification Steps
• Safe product with desired potency
Bar Charts, Inc. 2003

Is our protein of interest glycosylated? needs post-translational modifications
HOST
CELLS
Procaryotic cell
(e.g E. coli) Eucaryotic cell
Yeast cell Mammalian cell
Chinese Hamster Ovary (CHO) Cells)
Better chance to reach the reference API quality by using the same host cells
Technical Development of Biotechnological Drugs

Environmental
Monitoring
Excipients
Environmental
Moniotoring
Media
Components
Environmental
Moniotoring
Media
Components
Cell
Bank
Inprocess
Tests
Production
Cells
InProcess
Tests
Process
Materials
Active
Substance
Container
Closures
InProcess
Tests
Drug Product
Basic Steps of Biological Drugs Manufacturing
Envirnmental Raw Purification InProcess Resins Process
Monitoring Materials Intermediate Tests Materials
Envirnmental Raw Media Fermentation InProcess Process
Monitoring Materials Components Intermediate Tests Materials

Media Prep
Working Cell
Bank
Sub-
Culture
Inoculum
Sub-
Culture
Sub-
Culture
Sub-
Culture
Sub-
Culture
Large Scale Bioreactor
Wave
Bag
Seed Bioreactors
Fermentation
150L
Bioreactor
750L
Bioreactor
5,000L
Bioreactor
26,000L
Bioreactor
Depth
Filtration
Collection
Centrifuge
Harvest/Recovery
Harvest
Collection
Tank
1,500L
Filter
Chromatography
Anion Exchange Chromatography
(QXL)
Column Eluate
Hold
Tank
8,000L
Eluate
Hold
Tank
6,000L
Filter
Chromatography
Protein A
Chromatography
Column
Chromatography
Column
Eluate
Hold
Tank
20,000L
Hydrophobic Interaction Chromatography
(HIC)
Viral
Inactivation
Eluate
Hold
Tank
5,000L
Filter
Chromatography
Anion Exchange Chromatography (QFF - Fast
Flow)
Column
Post-viral
Hold
Vessel
3,000L
Viral Filtering Ultra Filtration
Diafiltration
Bulk
Fill
Purification
24 days 31 days
8 days
1 day
Technical Development of Biotechnological Drugs

Cell Bank System
50

Cell Bank System
51
Starting material
Parental cell line
Master cell bank (MCB)
Manufacturer working cell bank (MWCB)
Production substrate
Late expanded cell bank (LECB)
Genetic transformation
expand
expand
expand

A Cell Bank
• A collection of ampoules of uniform composition
stored under defined conditions, each containing
an aliquot of a single pool of cells
52

The Master Cell Bank (MCB)
• Generally derived from the selected cell clone
containing the expression construct.
• The MCB is used to derive all working cell banks.
53

The Manufacturer Working Cell Bank (MWCB)
• Derived by expansion of one or more ampoules of
the MCB under defined culture conditions
• The working cell bank is used for the production
of the batches.
54

The Late Expanded Cell Bank (LECB)
• Obtained in multiplying the cells used for the
production of the recombinant protein, several
passage after the passage of production.
• It is used to reveal a potential low viral
contamination and to study genetic stability of
the transgene.
55
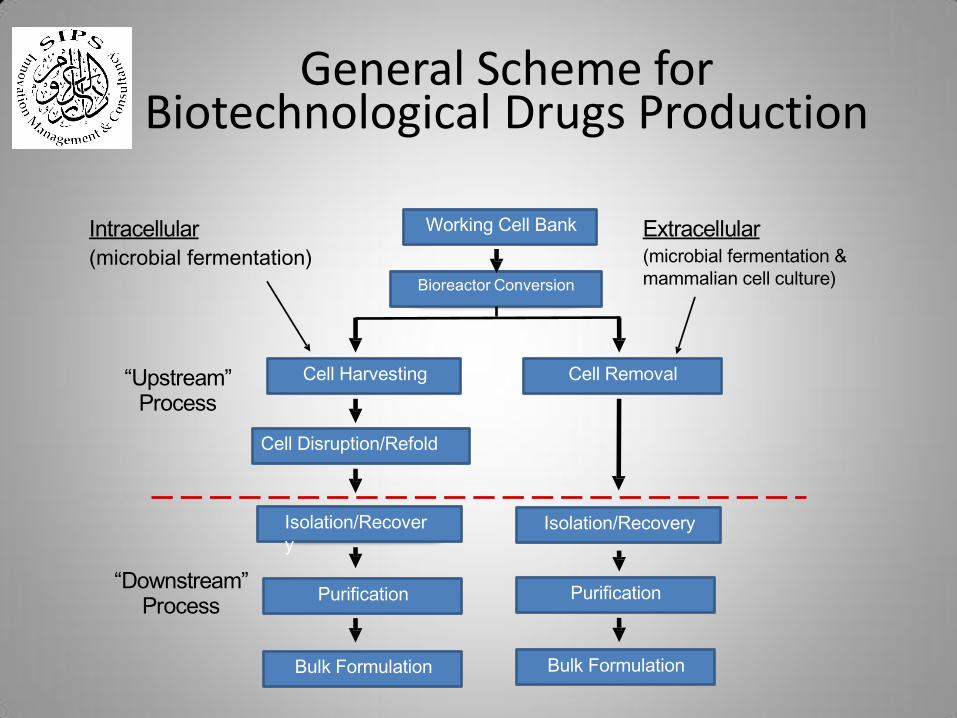
Intracellular
(microbial fermentation)
Bulk Formulation
Purification Purification
Isolation/Recover
y Isolation/Recovery
Cell Disruption/Refold
Cell Harvesting Cell Removal
Bioreactor Conversion
Bulk Formulation
Working Cell Bank Extracellular (microbial fermentation &
mammalian cell culture)
“Downstream” Process
“Upstream” Process
General Scheme for Biotechnological Drugs Production

Ammonium sulfate fractionation
Homogenization Organelle
Size Charge Polarity Affinity
Gel filtration,
SDS-PAGE,
Ultrafiltration
Ion exchange,
Chromatofocusig,
Disc-PAGE,
Isoelectric
focusing
Reverse phase chromatograpy,
HIC,
Salting-out
Affinity
chromatography,
Hydroxyapatite
Small molecule Macromolecule Cell
Debris Amino acid, Sugar,
Nucleotides, etc
Nucleic
acid
Protein
Carbohydrate
(Lipid)
Protein Purification

Peptide
variants
Desired
Product
Post-translational
variants
IMPURITY PROFILE
??? PROFILE
Degradation
Process & Product-related impurities

Challenges with Proteins
• Very large and unstable molecules
• Structure is held together by weak non-covalent forces
• Easily destroyed by relatively mild storage conditions
• Easily destroyed/eliminated by the body
• Hard to obtain in large quantities

Manufacturing processes involved in the production of Biotechnology
Large Molecules compared with Chemical Small Molecules
Technical Development of Biotechnological Drugs

Noncovalent Covalent
- Denaturation - Deamidation
- Aggregation - Oxidation
- Precipitation - Disulfide exchange
- Adsorption - Proteolysis
Problem with Proteins (in vivo – in the body)

Problem with Proteins (in vivo – in the body)
• Elimination by B and T cells
• Proteolysis by endo/exo peptidases
• Small proteins (< 30 kD) filtered out by the kidneys very quickly
• Unwanted allergic reactions may develop (even toxicity)
• Loss due to insolubility/adsorption

General requirements
1. A highly similar protein molecule to reference product
2. Same mechanism of action(s)
3. Same strength, dosage form and route of administration
Biosimilar biological products
• No clinically meaningful differences
• To be considered as a new active ingredients
Not interchangeable
Interchangeable biological products
• Risk of safety or diminishing efficacy of alternation and switching is not greater than the risk of continued use of reference product.
• Substitution with the innovator's products permitted
Innovator Bio-products VS Bio-similar

Upstream
- Cell line development
- Fermentation
Downstream
– Purification
– Fill and Finish
Comprehensive analytical characterization
and comparability study
Clinical study
–Preclinical
–Clinical
Bio-products Development

In-p
rocess c
on
trol finis
hed
-pro
duct
co
ntr
ols
Release
Tests
Extended
Characterization
Manufacturing
Process
Quality data combined with
preclinical and clinical
experience provide the full
picture
Clinical
Assessment
Bioproducts Dvelopment

Physicochemical characterisation
- Mass spectrometry techniques (e.g., MALDI-TOF)
- Nuclear magnetic resonance
- Capillary electrophoresis with laser-induced fluorescence detection (CE-LIF)
Primary structure
- peptide map
Secondary structure detection
- Circular dichroism in near- and far-UV spectra
Comprehensive set of orthogonal analytical methods
“Increasing sensitivity”

Product related variants and impurities
- SEC, CE-SDS, CZE, CEX, etc.
Antigen-antibody interaction
- Surface plasmon resonance
- FACS
Combination of methodologies
- liquid chromatography combined with mass
spectrometry
Comprehensive set of orthogonal analytical methods
“Increasing sensitivity”

Multiple bioassays elucidate structure
function relationships
Analytical Advances have demystified the Complexities

Analytical methods are sensitive to differentiate between:
• Batch to batch variation
• Batches before and after a change of the manufacturing process
• Batches from different sites
Analytical methods can determine whether batches sourced in different
countries are identical or not microheterogeneity of protein structure
• Purity profiles
• Glycan distribution
Analytical method are sensitive enough to even differentiate between individual batches

Complete quality range
for justification of limits
and claiming
biosimilarity
ADCC
basic variants
Variability is significant in Reference Products

Monitoring batches of an
approved mAb revealed a shift in
quality
Shift in glycosylation (structure)
pattern results in different
potency in cell-based assays
(function)
Indication of a change in the
manufacturing process
Such shifts observed in several
original products
A biosimilar mAb can sometimes be more similar to its reference
product than a post-change version to a pre-change version of a
single product
Variability is significant in Reference Products

Expected Heterogeneity- experience with monoclonal antibodies
C terminal lysine variability occurs in most monoclonal antibody products
Manufacturers set acceptable ranges for each species
Can be measured by various techniques, wCEX-HPLC, IEF, others
Doesn’t seem to impact potency or safety profile

Monoclonal antibodies Unacceptable, stress induced heterogeneity
Detectable by various methods
Manufacturers set stability specifications
Can compromise potency if OOS

Heterogeneity- experience with other recombinant products
• Case 1: protein terminus heterogeneity
– Traced to metaloprotease
– Minimal impact on potency
• Case 2: product clipping
– Minimal impact on potency
• Case 3: N-terminal glutamine cyclization
– Cyclized form had increased activity

Carbohydrate Profiles & Comparability
Nature Biotechnology 26, 592 (2008)
FDA balks at Myozyme scale-up by George Mack
“Genzyme ran into a snag in April when the US Food and Drug Administration (FDA) rejected its application to produce Myozyme (alglucosidase alfa, rhGAA) in its 2,000–liter-scale facility under the same approval authorization given for its 160-liter-scale plant. The FDA says the carbohydrate structure of the products manufactured at each scale differs and thus the 2,000-liter product requires a new biologic license application”
* Genzyme has been acquired by Sanofi-Aventis.

Epoeitin Alfa
Erstellt von Jamiri
30.4 Kda
2 disulfide linkages
165 amino acids
4 glycosylation sites
Monoclonal Antibodies
K
pyro-E O
D
G
G
D
O D
O
O pyro-E
D
D
D
G
G
150 kda
Pyro-Glu
Methionine oxidation
deamidation
High mannose,
G0, G1, G1, G2
Sialylation S. Kozlowski, OBP, CDER
Erstellt von Jamiri

Glycoform Profiles and Comparability Testing
(Dr. Stephan Fischer, Roche ) Schellekens H., Nephrol Dial Transplant 2005; 20 [Suppl 4]:iv31–iv36 (H. S. has contributed to meetings and publications sponsored by Amgen, Roche, Johnson & Johnson and Shire.)

A Case of MAb Biosimilar or Not?
• Reditux by Dr.Reddy’s approved in India in 2007
• Analysis by Genentech:
Identical amino acid sequence and molecular weight
Glycoforms not comparable
Charge distribution not comparable
Aggregate content not comparable
Effector function not comparable
Higher host cell protein content
Clinical data with Reditux in NHL comprised 17 patients only
Reed Harris, Genentech, Presentations at FABIAN
2008”Biopharma, Biosimilar, Biogenerics? Bioanalysis”,
Groningen, the Netherland, 2008 and “Biogenerics 2008”.

Insulin Case: Marvel Rapid failure
From EMEA Withdrawal Assessment Report EMEA/CHMP/317778/2007
redrawn by Heinemann & Hompesch
J Diabetes Sci Technol 2011;5(3):741-75
Combined Clamp (PD) and PK in 24 healthy subjects
•Early insulin AUCs bioequivalent (95% CI at 1 hour: 103 %-124%), •NOT Early Glucose Infusion Rate AUCs (95% CI at 1 hour: 100%-145%);

- 58 -
Marvel (insulins) 16h January 2008
• Did mot meet PK/PD equivalence margin
• Clinical equivalence margin too broad
• Many CMC deficiencies
Biograstim, Ratiograstim,Tevagrastim: 21st
February
2008
• Many more in the pipeline!
Monoclonal Antibodies
• Next wave of biosimilars
• Data pending
Interpretation of findings Experience in the EU

Alpha interferon case: Alpheon failure
From EMEA Withdrawal Assessment Report Procedure No. EMEA/H/C/000585
”Clinically and statistically significant difference in virological
relapse rates found between the end of therapy and the end of the
observation period.”

- 56 -
Omnitrope (somatropin): 26th January 2006
• Literature reliance not allowed
Valtropin (somatropin): 23rd February 2006
• Different Host Cell Allowed
• Data had to be re-analysed excluding US sourced reference product
Alpheon (alpha interferon) 28th June 2006
• More patients had return of disease after treatment when Alpheon
stopped than for reference medicine and more side effects with
Alpheon
Binocrit, Abseamed, Epo- α Hexal (epoetin α): 28th Aug07
• Slight differences in glycosylation acceptable
• Single comparative study acceptable (guidelines require 2)
• Lack of immunogenicity data in renal patients not acceptable = iv only
Interpretation of findings Experience in the EU

CASE: Silapro EPO Biosimilar Bioassay reflects difference in bioactivity
Found to mirror difference in protein concentration
•Erypo (Eprex) batches were found on average to have 8% higher bioactivity than SB309 (Silapo) batches, although all batches remained within the Ph. Eur. limits, namely 80%-125% (with error limits of 64 to 156%).
•There was a correspondingly higher protein content in the Erypo batches which contained on average 9% over the labelled amount of protein, compared with on average 1% over the labelled amount with SB309.
•The average specific activities for both products were remarkably similar (130.80 for test vs. 130.75 units/μg for reference).

CASE: Silapro EPO Biosimilar
The dosage of the test drug within the last four weeks was approximately 10%
higher than the dosage of the reference product.
Clinical trial does not detect difference during correction
phase - does during maintenance phase
(Silapo EPAR)

Goals of Quality, Non-clinical, and Clinical Studies • Quality
To demonstrate of comparability of the product to a reference product- the most critical step.
• Pre-clinical toxicology
To confirm therapeutic index and safety profile.
To qualify impurities by short-term animal studies .
Full animal toxicity studies are not necessary.
• Non-clinical PK/PD studies
To confirm dosing regimen by PK profiles.
To confirm the mechanism of actions by biomarkers (PD).
• Clinical safety
To compare immunogenicity and/or hypersensitivity with the reference products.
• Efficacy
To conduct confirmatory trials or other clinical trials for interchangeability.
Use of complementary biomarkers,or surrogate endpoints in some cases.
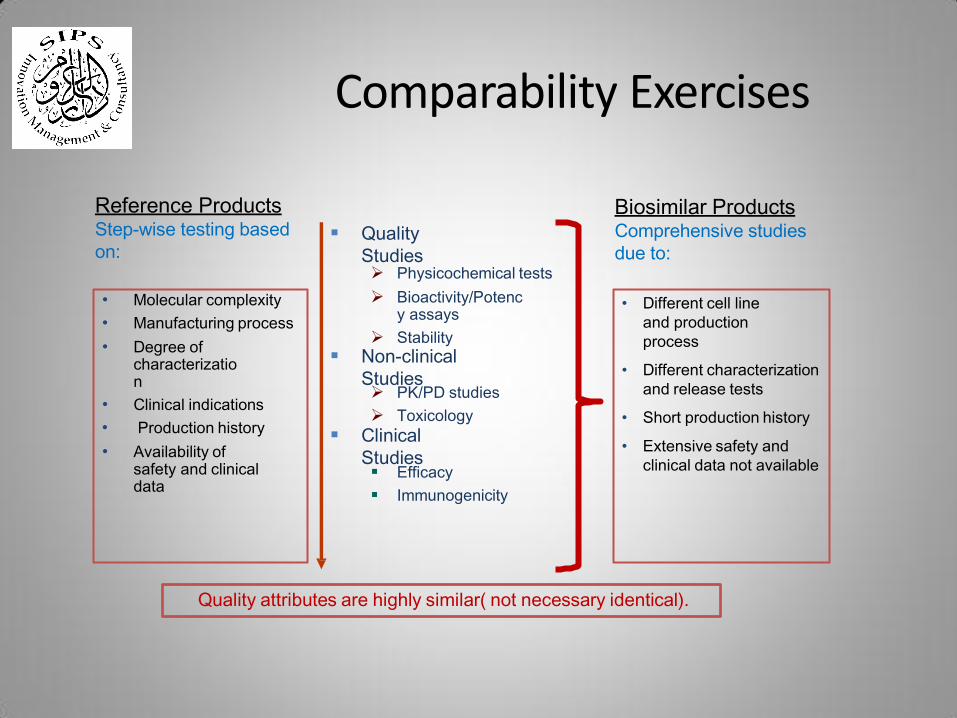
Comparability

Quality
Studies Physicochemical tests
Bioactivity/Potency assays
Stability
Non-clinical
Studies PK/PD studies
Toxicology
Clinical
Studies Efficacy
Immunogenicity
Quality attributes are highly similar( not necessary identical).
Reference Products Step-wise testing based
on:
Biosimilar Products Comprehensive studies
due to:
• Molecular complexity
• Manufacturing process
• Degree of
characterization
• Clinical indications
• Production history
• Availability of
safety and clinical
data
• Complex structure
• Different cell line
and production
process
• Different characterization
and release tests
• Extensive safety and
clinical data not available
Comparability Exercises
• Molecular complexity
• Manufacturing process
• Degree of characterization
• Clinical indications
• Production history
• Availability of safety and clinical data
Quality
Studies Physicochemical tests
Bioactivity/Potency assays
Stability
Non-clinical
Studies PK/PD studies
Toxicology
Clinical
Studies Efficacy
Immunogenicity
Quality attributes are highly similar( not necessary identical).
Reference Products Step-wise testing based
on:
Biosimilar Products Comprehensive studies
due to:
• Different cell line
and production
process
• Different characterization
and release tests
• Short production history
• Extensive safety and
clinical data not available
Comparability Exercises

LMH
W Heparin-induced
thrombocytopenia type II, anaphylactoid and anaphylactic reactions
Safety data should be collected from a cohort of patients representing all approved therapeutic indications
Post-marketing studies
Specific requirement for specific product
G-C
SF
Antibodies to the currently marketed rG-CSF occur infrequently
Attention should be paid to immunogenicity and potential rare serious adverse events, especially in patients undergoing chronic administration
Lack of efficacy should also be monitored, especially in individuals undergoing hematopoietic progenitor cell mobilization
Specific requirement for specific product

Specific requirement for specific product
Eryt
hro
po
ieti
n Rare serious adverse events such
as immune mediated Pure red cell aplasia “PRCA” and immune- related adverse events
Hypertension/aggravation of hypertension and thromboembolic events
Safety data should be collected from a cohort of patients representing all approved therapeutic indications

Regulatory trends
• Equivalence trials
– EU to consider non-inferiority for phase III
• Reference Product
– EU to change requirements on EU sourcing
• Risk-based approach
– FDA Totality-of-the-Evidence
• Step-wise approach from CMC via N-C to Clinical parts

EU Specific requirements – Clinical
(*) = Low end total subjects in studies where known from EPARs
Product PK PD Efficacy Safety
Somatropin HV (25*) HV (PK) Juvenile def. (90) 12 m Efficacy pop (90)
Insulin T1D Clamp No need 6 m appr., 12 m follow-up
G-CSF HV (2X28) NC (4X36) Chemo prot (140)
Not spec (160; 6 cycles)
IFNα 2a/2b HV (2x25) Markers (2x25)
Viral elim w12 (200/arm)
48 wk Efficacy pop (400)
LMw heparin By PD HV marker Thrombosis prev
“Sufficient number”
EPO HV (24) HV (PK) 1 route (200/arm)
(bridge w PK/PD)
12 m Efficacy pop (600)
mAb HV/pat ? HV/pat (PK) ? Risk based Risk-based – SciAdv!

Scientific advice
EU product specific Clinical Requirements
Directive 2001/83/EC
General guideline CHMP/437/04
Quality Issues CHMP/BWP/49348/200
5
Non-Clinical & Clinical Issues CHMP/BMWP/42835/2005
Revision concepts 2011
Revision draft2012
Changes planned? Legal level
Overarching
guidance
Level(s)
Detailed
guidance
level
Som
Ins
G-CSF
LMW Hepar
EPO IFN α 2a/b
mAb
IFN β FSH

Safety data
Risk Management Program
– Within the authorisation procedure the applicant should present an updated of the risk management plan in accordance with current EU legislation and pharmacovigilance guidelines. This should take into account risks identified during product development and potential risks.

Safety data
Immunogenicity
– If high levels of neutralising antibodies associated with comparator, then similar immunogenicity easier to investigate
– If serious immunogenic events rare than may need very large trial e.g. 30 000 patients to detect PRCA with Eprex
– Impact of neutralising antibodies – critical for epoetin, acceptable for interferon.
– Impact of non-neutralising antibodies - complex, may even enhance efficacy
– Need testing plan
– Need validated assay

Safety data
Extent of Data Base
• Not the detection of adverse events per se, but the evaluation of differences in occurrence.
• Study duration and sample size calculation should consider both frequency and magnitude of reasonably expectable adverse events
• Look for possible differences in clinical presentation (duration, magnitude, reversibility, response to treatment etc.).
• Acute/chronic use
• See also ICH guideline ICH E1
– 300 – 600 patients for 6 months
– 1500 patients

Do we need all the pieces to fully understand the picture?

Do we need all the pieces to fully understand the picture? to know it is a women – NO to know if she is smiling? – we need more information and a smile can make the difference!