Intrinsic defects of B cell function in X-linked severe combined immunodeficiency
6
0014-2980/00/0303-732$17.50 + .50/0 © WILEY-VCH Verlag GmbH, D-69451 Weinheim, 2000 Intrinsic defects of B cell function in X-linked severe combined immunodeficiency Harry White 1 , Adrian Thrasher 1 , Paul Veys 2 , Christine Kinnon 1 and Hubert B. Gaspar 1 1 Molecular Immunology Unit, Institute of Child Health, University College London, London, GB 2 Department of Bone Marrow Transplantation, Great Ormond Street Hospital NHS Trust, London, GB The cytokine receptor common gamma chain mutation in X-linked SCID results in a failure of T and NK cell development and an as yet undefined defect of B cells. Using immunoglobulin isotype-specific reverse transcription-PCR we show that although hematopoietic stem cell transplantation restores a diverse repertoire of class-switched B cell clones, on further anal- ysis these are almost all of donor origin. This suggests that host B cells, which predominate after unconditioned transplantation, are still defective even in the presence of normal T cells. These studies imply that effective humoral reconstitution can only be achieved by the engraftment of normal donor B cells. Key words: Class switching / Immunodeficiency / Gamma chain / B cell repertoire Received 27/10/99 Accepted 24/11/99 [I 20226] Abbreviations: X-SCID: X-linked severe combined immu- nodeficiency HSCT: Hematopoietic stem cell transplanta- tion c: Common gamma chain RT: Reverse transcription CDR: Complementarity-determining region 1 Introduction X-linked severe combined immunodeficiency (X-SCID) is caused by mutations in the common gamma chain ( c) subunit which is a component of the high-affinity IL-2, -4, -7, -9 and -15 receptors [1–6]. This defect results in the complete absence of T and NK cell development and an as yet uncharacterized defect of B cells [7, 8]. The out- look for X-SCID is poor in the absence of hematopoietic stem cell transplantation (HSCT). The survival following HSCT for all forms of SCID is now over 90 % when a genotypically matched donor is available [9] and between 50 % and 80 % following non-HLA-identical transplantation from parents or unrelated volunteer donors [9–12]. Despite these encouraging survival fig- ures, a significant number of patients continue to have poor humoral immune function after both HLA-identical and non-HLA-identical bone marrow transplantation [10, 12–14] and require lifelong Ig therapy. The reasons for continued immune dysfunction are poorly understood and may be due to the degree of HLA compatibility of the graft or the extent of donor B cell chimerism. Stem cell transplantation strategies for X-SCID are vari- able. The complete lack of T and NK cell function allows the engraftment of allogeneic donor T cells without prior myeloablative conditioning, a strategy which has signifi- cant benefits in terms of transplant-related mortality. However, under these circumstances, the B cell popula- tion is predominantly of host origin and remains c defi- cient. In a recent report of 34 unconditioned transplanta- tions for X-SCID from both HLA-identical and non-HLA- identical donors, 27 ( 80 %) patients remained on Ig substitution [10]. The suggestion that the continued presence of host c-defective B cells might result in residual humoral defects has been considered by this and a number of previous reports [9, 12, 15]. However, 20 % of the patients in the study by Buckley et al. [10] and significant numbers in other reports [12, 14, 16] had normal B cell function. Thus, although the B cell popula- tion following unconditioned transplantation is of pre- dominantly host origin and therefore c defective, the above data suggest that humoral immune reconstitution is variable. One of the major limitations in studying humoral recon- stitution post HSCT has been the inability of conven- tional assays to analyze the details of B cell diversity in separate lymphocyte populations. To date, assessment has largely been limited to the quantitative analysis of B lymphocytes and total Ig and by humoral responses to mitogenic and specific antigenic stimuli. Molecular details of VDJ recombination in X-SCID have been inves- tigated by analysis of complementarity-determining 732 H. White et al. Eur. J. Immunol. 2000. 30: 732–737
-
Upload
harry-white -
Category
Documents
-
view
213 -
download
0
Transcript of Intrinsic defects of B cell function in X-linked severe combined immunodeficiency

0014-2980/00/0303-732$17.50+.50/0 © WILEY-VCH Verlag GmbH, D-69451 Weinheim, 2000
Intrinsic defects of B cell function in X-linkedsevere combined immunodeficiency
Harry White1, Adrian Thrasher1, Paul Veys2, Christine Kinnon1 and Hubert B. Gaspar1
1 Molecular Immunology Unit, Institute of Child Health, University College London, London, GB2 Department of Bone Marrow Transplantation, Great Ormond Street Hospital NHS Trust,
London, GB
The cytokine receptor common gamma chain mutation in X-linked SCID results in a failure ofT and NK cell development and an as yet undefined defect of B cells. Using immunoglobulinisotype-specific reverse transcription-PCR we show that although hematopoietic stem celltransplantation restores a diverse repertoire of class-switched B cell clones, on further anal-ysis these are almost all of donor origin. This suggests that host B cells, which predominateafter unconditioned transplantation, are still defective even in the presence of normal T cells.These studies imply that effective humoral reconstitution can only be achieved by theengraftment of normal donor B cells.
Key words: Class switching / Immunodeficiency / Gamma chain / B cell repertoire
Received 27/10/99Accepted 24/11/99
[I 20226]
Abbreviations: X-SCID: X-linked severe combined immu-nodeficiency HSCT: Hematopoietic stem cell transplanta-tion q c: Common gamma chain RT: Reverse transcriptionCDR: Complementarity-determining region
1 Introduction
X-linked severe combined immunodeficiency (X-SCID) iscaused by mutations in the common gamma chain ( + c)subunit which is a component of the high-affinity IL-2, -4,-7, -9 and -15 receptors [1–6]. This defect results in thecomplete absence of T and NK cell development and anas yet uncharacterized defect of B cells [7, 8]. The out-look for X-SCID is poor in the absence of hematopoieticstem cell transplantation (HSCT). The survival followingHSCT for all forms of SCID is now over 90 % whena genotypically matched donor is available [9] andbetween 50 % and 80 % following non-HLA-identicaltransplantation from parents or unrelated volunteerdonors [9–12]. Despite these encouraging survival fig-ures, a significant number of patients continue to havepoor humoral immune function after both HLA-identicaland non-HLA-identical bone marrow transplantation [10,12–14] and require lifelong Ig therapy. The reasons forcontinued immune dysfunction are poorly understoodand may be due to the degree of HLA compatibility of thegraft or the extent of donor B cell chimerism.
Stem cell transplantation strategies for X-SCID are vari-able. The complete lack of T and NK cell function allowsthe engraftment of allogeneic donor T cells without priormyeloablative conditioning, a strategy which has signifi-cant benefits in terms of transplant-related mortality.However, under these circumstances, the B cell popula-tion is predominantly of host origin and remains + c defi-cient. In a recent report of 34 unconditioned transplanta-tions for X-SCID from both HLA-identical and non-HLA-identical donors, 27 ( ˚ 80 %) patients remained on Igsubstitution [10]. The suggestion that the continuedpresence of host + c-defective B cells might result inresidual humoral defects has been considered by thisand a number of previous reports [9, 12, 15]. However,20 % of the patients in the study by Buckley et al. [10]and significant numbers in other reports [12, 14, 16] hadnormal B cell function. Thus, although the B cell popula-tion following unconditioned transplantation is of pre-dominantly host origin and therefore + c defective, theabove data suggest that humoral immune reconstitutionis variable.
One of the major limitations in studying humoral recon-stitution post HSCT has been the inability of conven-tional assays to analyze the details of B cell diversity inseparate lymphocyte populations. To date, assessmenthas largely been limited to the quantitative analysis ofB lymphocytes and total Ig and by humoral responses tomitogenic and specific antigenic stimuli. Moleculardetails of VDJ recombination in X-SCID have been inves-tigated by analysis of complementarity-determining
732 H. White et al. Eur. J. Immunol. 2000. 30: 732–737

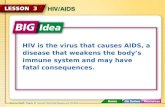
Fig. 1. Ig RT-PCR/CDR3 spectratyping on peripheral bloodB cells. M, IgM; A, IgA, G, IgG2. Samples: n9m, 9-month-oldnormal; n4y, 4-year-old normal; C1pre, X-SCID before trans-plantation; C1post, the same X-SCID 4 years after condi-tioned HSCT; N1, X-SCID 1 year after non-conditionedHSCT; C2e, X-SCID 2 months after conditioned HSCT;C2 the same patient 5 months after HSCT; N2, X-SCID6 months after non-conditioned HSCT.
region (CDR)-3 sequences and demonstrated abnormali-ties in somatic mutation and preferential utilization ofimmature JH segments [17, 18]. However, these studiesdid not analyze isotype switching or the ability of cells toundergo clonal expansion.
It would be reasonable to hypothesize that the + c signal-ing defect results in intrinsic B cell abnormalities due tothe involvement of + c in IL-4 signaling [19–21]. However,the evidence for this has to date come from in vitro stud-ies and indirectly from the transplantation studies above.We have used a reverse transcription (RT)-PCR-basedtechnique to study the isotype and diversity of theexpressed Ig repertoire [22]. This assay allows us to lookat the ability of host + c-defective and normal donor Bcells to undergo class switching and clonal expansionpre and post HSCT. In this report we offer direct evi-dence that + c-defective B cells retain a variety of intrinsicabnormalities post HSCT even in the presence of normaldonor T cell help.
2 Results
2.1 Analysis of B cell class switching andclonality
To detect the presence of class-switched Ig expressionand clonal expansions in peripheral blood B cells fromX-SCID patients and normal donors, RT-PCR analysisusing Ig VH1 and H chain subclass-specific primers wasperformed. Under such circumstances a ladder of tran-script sizes is detected, representing the in-frame distri-bution of Ig lengths created by VDJ recombination [22].
Samples from two normal donors of appropriate age (9months and 4 years), two X-SCID patients who hadreceived matched unrelated donor HSCT after cytotoxicconditioning (C1post and C2) and two X-SCID patientswho received genotypically matched sibling transplantswithout conditioning (N1 and N2) were analyzed. We alsoanalyzed a pre-transplantation X-SCID samples (C1pre)and a sample 2 months after one of the conditionedmatched transplantations (C2e).
Fig. 1 shows the results obtained after RT-PCR analysisof VH1 gene expression in the IgM, IgA and IgG2 isoty-pes. Normal samples have a complex population of IgM-expressing cells, shown by the smoothness of the tran-script length distribution, and a diverse pool of IgA- andIgG2-expressing cells as evidenced by the number ofdifferent clones in these tracks; large antigen-specificclonal expansions appear as darker bands. The RT-PCRtechnique does not quantitate the number of cells in aclone but does show the number of different clones
above a detection threshold that does not vary betweensamples.
The X-SCID immunophenotype is characterized bynormal or slightly elevated numbers of mostly IgM-expressing B cells and lower or zero serum antibodyconcentrations [8, 23]. This phenotype is consistent withthe results obtained from the X-SCID patient at presenta-tion, shown here as sample C1pre. This shows a neartotal absence of cells expressing class-switched Ig tran-scripts, and all X-SCID patients tested at presentation(n = 4, data not shown) showed this phenotype.
Lanes C1post, C2 and N1, N2 show the results obtainedfrom X-SCID patients who had received HLA-compatibleHSCT with (C) and without (N) conditioning. Transplanta-tion clearly restored diverse class-switched populationsof B cells and produced CDR3 spectratypes comparableto those observed in the normal controls. Sample C2eshows that little reconstitution has occurred in thispatient 2 months after transplantation.
These results are consistent with the clinical status ofthese individuals at the time blood samples wereobtained (Table 1). All patients had discontinued i.v. Igreplacement and showed normal levels of IgG, A and M.Three out of four had shown specific responses to vacci-nations or varicella infection at time of testing. There wasno difference in immune or clinical status between theconditioned and non-conditioned patients.
Typically after non-conditioned transplantation, the B cellpool is largely host derived [10, 12], although little is
Eur. J. Immunol. 2000. 30: 732–737 B cell defects in X-SCID 733

Table 1. Details of patients mutations and humoral recon-stitution post transplantation at the times of analysis
Patient Surface + cexpression
and mutation
Total Ig(mg/ml)
Vaccine/immuneresponses
C1 + c negative679 delG
G 11.5A 0.53M 0.97
Positive responsesto Hemophilus
influenza b/Tetanus/Measles,Mumps, Rubella
C2 + c negative197
ins40 del3
G 13.8A 0.38M 0.63
Not immunized
N1 + c negative345-8
delTCAG
G 6.69A 0.26M 0.34
Not immunizedbut positiveresponse to
varicellainfection
N2 + c negativeS108P
G 5.36A 0.33M 0.64
Not immunizedbut positiveresponse to
varicellainfection
known about the absolute distribution of class-switchedcells between donor and host populations. Consideringthe data in Fig. 1 this might suggest that reconstitutionof T cell help is enough to restore functional antibodyresponses in + c-negative B cells.
2.2 Analysis of class switching in a donor/hostchimeric B cell population
To address the issue of whether + c mutant B cells con-tribute significantly to the Ig class-switched B cell pool inthe presence of a normal T cell compartment after HSCT,we investigated whether sorted B cells expressing low/zero levels of surface + c which, therefore, are predomi-nantly of host origin, contained any class-switched cells.We therefore used a sample from patient N2 who hadreceived a non-conditioned HSCT and had normal T cellreconstitution.
PBMC were stained for + c (IL-2R + ) and CD19. B cells(CD19+) were FACS sorted according to the scheme indi-cated in Fig. 2. B cells from the normal donor weresorted into two populations containing the “top 50 %”and “bottom 50 %” of + c-expressing cells. The B cellsfrom patient N2, who has a + c mutation known to abro-gate cell surface expression, were sorted into three pop-ulations: the top18 % were selected because these cellsexpressed levels of + c comparable to those seen in the
normal control. The middle 32 % and the bottom 50 %were also collected as indicated in Fig. 2.
The sorted cell samples were analyzed as before by RT-PCR/JH primer run-off, but this time with a forwardprimer specific for the VH3 gene family and reverse prim-ers specific for IgM, A, G1, G2, G3, G4. The VH3 primerwas used because this is the most frequently used genefamily and would give maximal signal from the compara-tively low number of cells obtained after FACS sorting.Fig. 2 shows the results of this analysis.
Both high and low + c-expressing B cell populations fromthe normal sample showed diverse Ig class-switchedcell populations, although it is also clear that the + c low-expressing cell pool shows a significantly increased ratioof class switched cells, particularly those expressingIgG1 and IgG3.
The B cells from patient N2 showing near normal levelsof + c surface expression (top 18 %) also contain adiverse population of class-switched cells. The complex-ity and clonal expansions present in these CDR3 spec-tratypes are comparable to that of the normal samplebottom 50 %, as is the actual level of + c expression(Fig. 2). All of the other B cells from patient N2, both themiddle 32 % and the bottom 50 %, representing the82 % of cells with very low or zero levels of + c expres-sion, show a greatly reduced number of class-switchedB cell clones. Only a few clonal expansions are detect-able, principally in the IgG3 compartment. This impliesthat all or almost all of the class switching and clonalexpansion has occurred in B cells that express detect-able levels of + c.
3 Discussion
The issue of which transplantation strategy to adopt inthe treatment of X-SCID is controversial and has impor-tant implications. Clearly, non-conditioned transplantsfrom HLA-identical or non-HLA-identical donors havesignificant benefits. However, this must be balanced withthe observations of increased defects in humoral recon-stitution following such procedures. The fact that signifi-cant numbers of children do produce Ig and make anti-body responses after unconditioned transplantation indi-cates that there are certain factors that will allow suc-cessful immune reconstitution to occur, but to date it hasnot been clear what those determinants are. The idea ofintrinsic B cell defects persisting after transplantationhas been proposed but not convincingly demonstrated.Previous studies on X inactivation in female carriers of X-SCID show a strong bias towards use of the normal genein IgM-negative peripheral blood B cell lines [24] and this
734 H. White et al. Eur. J. Immunol. 2000. 30: 732–737

Fig. 2. Spectratyping on B cells sorted for surface + c (IL-2RG, as labeled here) expression. M, IgM; A, IgA; G1-4, IgG1-IgG4,IL-2RG, + c. CD19-positive B cells from a normal individual and N2 were FACS sorted on the basis of + c expression. From a nor-mal individual cells were split in half and from patient N2, cells were split into the “top” 18 %, “middle” 32 % and “bottom” 50 %,based on the level of + c expression. Sorted populations were then subjected to Ig RT-PCR/CDR3 spectratyping as shown in thebottom panel.
suggests a failure of B cells with the mutant active Xchromosome to develop beyond the IgM+ stage. Assess-ment of humoral reconstitution following stem cell trans-plantation by conventional humoral assays has alsodemonstrated effective humoral reconstitution but inbulk B cell populations, and this overlooks the possibilityof humoral function arising entirely from a small donor Bcell population [10, 14, 16].
We have shown that transplantation restores a diversepopulation of class-switched B cells in the peripheralblood of patients who have received both conditionedand non-conditioned transplants for X-SCID. We show,however, that in patient N2 the surface + c-positive popu-lation – a minority of cells – contains all or almost all theclass-switched antibody-expressing cells. This impliesthat only donor-derived B cells are class switching andthat this population, however, small, is responsible for thebulk of humoral reconstitution seen after transplantation.
A recent study of 14 patients with confirmed + c-deficientSCID after HSCT showed 2/3 HLA-matched and 2/11haploidentical HSCT restored clinically normal B cell
function [16], reaffirming the observations of poorerhumoral function after haploidentical HSCT [10]. Consid-ering all transplantations, 3/14 showed restoration ofclinically normal B cell function in the absence of detect-able donor B cells at the 5 % level of sensitivity althoughone of these patients had no detectable IgE or IgA. Onthe basis of these observation it is possible to concludethat in a minority of cases + c-deficient B cells may func-tion normally although the contribution of an active nor-mal donor B cell population of less than 5 % total B cellscannot be excluded. It was demonstrated, however, thatone of the patients with clinically normal B cell functionwas producing host allotype IgG3. Interestingly, this isthe isotype we observe expressed at a low level in thesurface + c-negative B cell population (Fig. 2).
It would be surprising if the + c defect produced an abso-lute loss of any B cell functional maturation in terms ofclass switching. In mice, class switching to IgG3 is inhib-ited by IL-4 [25]. Considering the observations madeabove, if + c-negative B cells can leak into the class-switched population the absence of IL-4 signaling maybias switching toward IgG3. It has also been suggested
Eur. J. Immunol. 2000. 30: 732–737 B cell defects in X-SCID 735

that in the absence of + c, IL-4 signaling can occurthrough + c-independent pathways, possibly through theIL-13 receptor complex [19, 21, 26]. X-SCID B cells showtyrosine phosphorylation of JAK1, IRS-1 and STAT6 inresponse to IL-4 [19] and in addition are able to prolifer-ate and secrete IgE [21]. However, in contrast to thesereports, our studies using the Ig RT-PCR asssay clearlyshow that this + c-independent pathway is insufficient tosupport effective B cell function in vivo.
Our results suggest that there is a profound intrinsicdefect in + c-negative B cell function and, therefore, thatthe size and quality of the functional B cell repertoire willbe related to the level of normal donor B cell engraftmentin recipients of HSCT for X-SCID. The results establish afirm precedent for a major study to determine the extentof + c-negative B cell contribution to the class-switchedB cell pool in both HLA-matched and mismatched HSCT.These studies also have significant implications fortransplantation strategies for X-SCID. Donor B cellengraftment and therefore stem cell engraftment albeit atlow levels is necessary for successful humoral function.Whether this can be achieved by modifying the stem celldose in unconditioned transplants or by the use of a con-ditioning regime needs to be determined.
4 Materials and methods
4.1 Patients
All patients were treated at Great Ormond Street HospitalNHS Trust. The study was conducted after local ethicalcommittee approval. All patients had a typical T- B+ NK pro-file at presentation and the molecular diagnosis of X-SCIDwas made by the absence of + c surface expression onPBMC and by the identification of a mutation in the IL-2R +gene (summarized in Table 1).
4.2 RT-PCR
PBMC were isolated using density centrifugation. Total RNAwas extracted using RNAzol B (Biogenesis, GB) accordingto manufacturer’s instructions. cDNA was synthesized usingMoMuLV reverse transcriptase and all reagents from LifeTechnologies, GB, according to manufacturer’s instructions.
4.3 PCR reactions
PCR was performed using the following primers; forward:VH1, CAGGTGCAGCTGGTGCAGTCTGGGGCT; VH3, GAG-GTGCAGCTGGTGGAGTCTGGGGGAG; reverse: IgM, TTT-GTTGCCGTTGGGGTGCTGGAC; IgA, CTGGGCAGGGCA-CAGTCACATCCT; IgG1, ACGGTGGGCATGTGTGAGTTT-TGT; IgG2, GTGCTGGGCACGGTGGGCACTCGA; IgG3,
GGCATGTGTGAGTTGTGTCACCAA; IgG4, GTGCTGGGC-ATGATGGGCATGGGG.
Cycling was as follows: 94 °C, 30 s; 60 °C, 30 s; 72 °C,1 min, for 30 cycles, preceded by an incubation at 94 °C for3 min prior to addition of polymerase. Reactions were per-formed in a 50- ? l volume using standard protocols and 2 ? lcDNA from 50 ? l RT. The common JH primer used for allnested run-off reactions had the following sequence:TGAGGAGACGGTGACCA(GorT)GGT(GorTorC)CC(AorTorC)-TGGCCCC. For each run-off reaction 2 pmol primer wasend-labeled with 3 ? Ci [ + -33P] dATP (Amersham, GB) usingT4 polynucleotide kinase. The reaction was precipitated withethanol, pelleted and washed with 75 % ethanol prior to use.Run-off reactions were performed for 12 cycles with thesame reagents and cycling as for the PCR, and 2 ? l of thefirst-round PCR as target. After cycling, samples weretreated as for standard sequencing gel electrophoresis with5 % denaturing acrylamide gels and autoradiography. ForFig. 2 autoradiography, exposure times were adjusted tonormalize for differences in the starting sample cell count.
4.4 FACS sorting
PBMC were resuspended at 107 cells/ml in DMEM, 10 %FCS and stained with a 1/10 dilution of FITC-conjugatedanti-CD19 (Becton Dickinson), PE-conjugated anti- + c (Phar-mingen, GB) on ice for 1 h. They were washed twice withDMEM, 10 % FCS, resuspended at 106 cells/ml in DMEM,5 % FCS and sorted with a Coulter cell sorter.
Acknowledgements: We should like to acknowledge thehelp of Arnold Pizzey for FACS sorting. H.W. was supportedby Sport Aiding Medical Research for Kids (SPARKS). A.T. isa Senior Wellcome Research Fellow.
References
1 Noguchi, M., Nakamura, Y., Russell, S. M., Ziegler, S. F.,Tsang, M., Cao, X. and Leonard, W. J., Interleukin-2 receptorgamma chain: a functional component of the interleukin-7 recep-tor. Science 1993. 262: 1877–1880.
2 Noguchi, M., Yi, H., Rosenblatt, H. M., Filipovich, A. H., Adel-stein, S., Modi, W. S., McBride, O. W. and Leonard, W. J.,Interleukin-2 receptor gamma chain mutation results in X-linkedsevere combined immunodeficiency in humans. Cell 1993. 73:147–157.
3 Takeshita, T., Asao, H., Ohtani, K., Ishii, N., Kumaki, S.,Tanaka, N., Munakata, H., Nakamura, M. and Sugamura, K.,Cloning of the gamma chain of the human IL-2 receptor. Science1992. 257: 379–382.
4 Russell, S. M., Johnston, J. A., Noguchi, M., Kawamura, M.,Bacon, C. M., Friedmann, M., Berg, M., McVicar, D. W.,Witthuhn, B. A., Silvennoinen, O., Goldman, A. S., Schmal-stieg, F. C., Ihle, J. N., O’Shea, J. J. and Leonard, W. J., Interac-tion of IL-2R beta and gamma c chains with Jak1 and Jak3: impli-cations for XSCID and XCID. Science 1994. 266: 1042–1045.
736 H. White et al. Eur. J. Immunol. 2000. 30: 732–737

5 Russell, S. M., Keegan, A. D., Harada, N., Nakamura, Y.,Noguchi, M., Leland, P., Friedmann, M. C., Miyajima, A., Puri,R. K., Paul, W. E. and Leonard, W. J., Interleukin-2 receptorgamma chain: a functional component of the interleukin-4 recep-tor. Science 1993. 262: 1880–1883.
6 Giri, J. G., Ahdieh, M., Eisenman, J., Shanebeck, K., Grab-stein, K., Kumaki, S., Namen, A., Park, L. S., Cosman, D. andAnderson, D., Utilization of the beta and gamma chains of theIL-2 receptor by the novel cytokine IL-15. EMBO J. 1994. 13:2822–2830.
7 Stephan, J. L., Vlekova, V., Le Deist, F., Blanche, S., Donadieu,J., De Saint Basile, G., Durandy, A., Griscelli, C. and Fischer,A., Severe combined immunodeficiency: a retrospective single-center study of clinical presentation and outcome in 117 patients.J. Pediatr. 1993. 123: 564–572.
8 Buckley, R. H., Schiff, R. I., Schiff, S. E., Markert, M. L., Willi-ams, L. W., Harville, T. O., Roberts, J. L. and Puck, J. M.,Human severe combined immunodeficiency: genetic, pheno-typic, and functional diversity in one hundred eight infants.J. Pediatr. 1997. 130: 378–387.
9 Fischer, A., Landais, P., Friedrich, W., Morgan, G., Gerritsen,B., Fasth, A., Porta, F., Griscelli, C., Goldman, S. F., Levinsky,R. and Vossen, J., European experience of bone-marrow trans-plantation for severe combined immunodeficiency. Lancet 1990.336: 850–854.
10 Buckley, R. H., Schiff, S. E., Schiff, R. I., Markert, L., Williams,L. W., Roberts, J. L., Myers, L. A. and Ward, F. E., Hematopoi-etic stem-cell transplantation for the treatment of severe com-bined immunodeficiency. N. Engl. J. Med. 1999. 340: 508–516.
11 Veys, P. A., Meral, A., Hassan, A., Goulden, N., Webb, D. andDavies, G., Haploidentical related transplants and unrelateddonor transplants with T cell addback. Bone Marrow Transplant.1998. 21 Suppl 2: S42–S44.
12 van Leeuwen, J. E., van Tol, M. J., Joosten, A. M., Schelle-kens, P. T., van den Berg, R. L., Waaijer, J. L., Oudeman, G. N.,van der Weijden-Ragas, C. P., Roos, M. T., Gerritsen, E. J.,Haraldsson, A., Meera Khan, P. and Vossen, J. M., Relation-ship between patterns of engraftment in peripheral blood andimmune reconstitution after allogeneic bone marrow transplanta-tion for (severe) combined immunodeficiency. Blood 1994. 84:3936–3947.
13 Bertrand, Y., Landais, P., Friedrich, W., Gerritsen, B., Morgan,G., Fasth, A., Cavazzana, C. M., Porta, F., Cant, A., Espanol, T.,Muller, S., Veys, P., Vossen, J., Haddad, E. and Fischer, A.,Influence of severe combined immunodeficiency phenotype onthe outcome of HLA non-identical, T-cell-depleted bone marrowtransplantation: a retrospective European survey from the Euro-pean group for bone marrow transplantation and the europeansociety for immunodeficiency. J. Pediatr. 1999. 134: 740–748.
14 Haddad, E., Landais, P., Friedrich, W., Gerritsen, B., Cavaz-zana, C. M., Morgan, G., Bertrand, Y., Fasth, A., Porta, F.,Cant, A., Espanol, T., Muller, S., Veys, P., Vossen, J. andFischer, A., Long-term immune reconstitution and outcome afterHLA-nonidentical T-cell-depleted bone marrow transplantationfor severe combined immunodeficiency: a European retrospec-tive study of 116 patients. Blood 1998. 91: 3646–3653.
15 Dror, Y., Gallagher, R., Wara, D. W., Colombe, B. W., Merino,A., Benkerrou, M. and Cowan, M. J., Immune reconstitution insevere combined immunodeficiency disease after lectin-treated,T-cell-depleted haplocompatible bone marrow transplantation.Blood 1993. 81: 2021–2030.
16 Haddad, E., Deist, F. L., Cavazzana, C. M., Blanche, S., Basile,G. D. and Fischer, A., Long-Term Chimerism and B-Cell FunctionAfter Bone Marrow Transplantation in Patients With Severe Com-bined immunodeficiency with B Cells: A Single-Center Study of22 Patients. Blood 1999. 94: 2923–2930.
17 Minegishi, Y., Ishii, N., Tsuchida, M., Okawa, H., Sugamura, K.and Yata, J., T cell reconstitution by haploidentical BMT does notrestore the diversification of the Ig heavy chain gene in patientswith X-linked SCID. Bone Marrow Transplant. 1995. 16: 801–806.
18 Minegishi, Y., Okawa, H., Sugamura, K. and Yata, J., Preferen-tial utilization of the immature JH segment and absence ofsomatic mutation in the CDR3 junction of the Ig H chain gene inthree X-linked severe combined immunodeficiency patiens. Int.Immunol. 1994. 6: 1709–1715.
19 Taylor, N., Candotti, F., Smith, S., Oakes, S. A., Jahn, T., Isa-kov, J., Puck, J. M., O’Shea, J. J., Weinberg, K. and Johnston,J. A., Interleukin-4 signaling in B lymphocytes from patients withX-linked severe combined immunodeficiency. J. Biol. Chem.1997. 272: 7314–7319.
20 Izuhara, K., Heike, T., Otsuka, T., Yamaoka, K., Mayumi, M.,Imamura, T., Niho, Y. and Harada, N., Signal transduction path-way of interleukin-4 and interleukin-13 in human B cells derivedfrom X-linked severe combined immunodeficiency patients.J. Biol. Chem. 1996. 271: 619–622.
21 Matthews, D. J., Clark, P. A., Herbert, J., Morgan, G., Armit-age, R. J., Kinnon, C., Minty, A., Grabstein, K. H., Caput, D.,Ferrara, P. and Callard, R. E., Function of the interleukin-2 (IL-2)receptor gamma-chain in biologic response of X-linked severecombined immunodeficient B cells to IL-2, IL-4, IL-13, and IL-15.Blood 1995. 85: 38–42.
22 White, H. N., Restriction-PCR fingerprinting of the immunoglob-ulin VH repertoire: direct detection of an immune response andglobal analysis of B cell clonality. Eur. J. Immunol. 1998. 28:3268–3279.
23 Stephan, J. L., Vlekova, V., Le Deist, F., De Saint Basile, G.,Donadieu, J., Durandy, A., Blanche, S., Griscelli, C. andFischer, A., A retrospective single-center study of clinical pre-sentation and outcome in 117 patients with severe combinedimmunodeficiency. Immunodeficiency 1993. 4: 87–88.
24 Conley, M. E., Lavoie, A., Briggs, C., Brown, P., Guerra, C. andPuck, J. M., Nonrandom X chromosome inactivation in B cellsfrom carriers of X chromosome-linked severe combined immuno-deficiency. Proc. Natl. Acad. Sci. USA 1988. 85: 3090–3094.
25 Coffman, R. L. and Carty, J., A T cell activity that enhancespolyclonal IgE production and its inhibition by interferon-gamma.J. Immunol. 1986. 136: 949–954.
26 Matthews, D. J., Hibbert, L., Friedrich, K., Minty, A. and Cal-lard, R. E., X-SCID B cell responses to interleukin-4 andinterleukin-13 are mediated by a receptor complex that includesthe interleukin-4 receptor alpha chain (p140) but not the gammac chain. Eur. J. Immunol. 1997. 27: 116–121.
Correspondence: Harry White, Molecular Immunology Unit,Institute of Child Health, 30 Guilford Street, London WC1N1EH, GBFax: +44 171 831 4366e-mail: h.white — ich.ucl.ac.uk
Eur. J. Immunol. 2000. 30: 732–737 B cell defects in X-SCID 737