Intravenous Hypertonic Sodium Chloride Adult …...Management of severe sodium chloride depletion...
14
1 Intravenous Hypertonic Sodium Chloride – Adult/Pediatric – Inpatient Clinical Practice Guideline Target Population: Adult and pediatric inpatients using intravenous hypertonic sodium chloride. CPG Contact: Name: Philip Trapskin, Manager, Drug Policy Program Phone Number: 608-263-1328 Email address: [email protected] Guideline Author(s): Jennifer Ng, PharmD Carin Bouchard, PharmD Matt Wolf, PharmD Coordinating Team Members: Sara Shull, PharmD, MBA Review Individuals/Bodies: Josh Medow, MD UW Health Pharmacy and Therapeutics Committee Committee Approvals/Dates: UW P&T Committee/June 2013 UW P&T Committee/June 2006 Release Date: June 2013 June 2015 – Interim Update (administration instructions refer to IV Administration Clinical Practice Guidelines) Next schedule review: June 2015 Copyright © 2013 University of Wisconsin Hospitals and Clinics Authority Contact: Lee Vermeulen, [email protected] Last Revised: 06/2013 [email protected]
Transcript of Intravenous Hypertonic Sodium Chloride Adult …...Management of severe sodium chloride depletion...

1
Intravenous Hypertonic Sodium Chloride – Adult/Pediatric –Inpatient
Clinical Practice Guideline
Target Population: Adult and pediatric inpatients using intravenous hypertonic sodium chloride.
CPG Contact: Name: Philip Trapskin, Manager, Drug Policy Program Phone Number: 608-263-1328 Email address: [email protected]
Guideline Author(s): Jennifer Ng, PharmD Carin Bouchard, PharmD Matt Wolf, PharmD
Coordinating Team Members: Sara Shull, PharmD, MBA
Review Individuals/Bodies: Josh Medow, MD UW Health Pharmacy and Therapeutics Committee
Committee Approvals/Dates: UW P&T Committee/June 2013 UW P&T Committee/June 2006
Release Date: June 2013 June 2015 – Interim Update (administration instructions refer to IV Administration Clinical Practice Guidelines)
Next schedule review: June 2015
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
2
Clinical Practice Guideline (CPG) Executive Summary
Guideline Title: Intravenous Hypertonic Sodium Chloride – Adult and Pediatric – Inpatient – Clinical Practice Guideline
Guideline Overview These clinical practice guidelines are intended to guide clinicians in the use of hypertonic saline in adult and pediatric patients. Graded recommendations for indications, dosing, administration, and precautions for use are included.
Practice Recommendations 1. Hyponatremia
1.1. Indications1.1.1. Management of symptoms of severe hypotonic hyponatremia (Class I, Level of
Evidence A).2,22,23
1.1.2. Management of severe sodium chloride depletion when rapid electrolyte restoration is essential due to ongoing sodium losses (Class I, Level of Evidence A).
2,22
1.1.3. Inappropriate use includes treatment of asymptomatic hyponatremia without ongoing losses (Class III, Level of Evidence A).
23
1.2. Dose 1.2.1. An initial goal serum sodium concentration must be established.
1.2.1.1. Symptoms of severe hyponatremia: goal of 120 mmol/L initially followed by slower correction to approximately 130 mmol/L over the following several days. Initial goal serum sodium level should be lower if the baseline serum sodium is <100 mmol/L.
22
1.2.2. Calculate sodium deficit for patients with hyponatremia (Class I, Level of Evidence A):
2,22,24
1.2.2.1. Calculate Ideal Body Weight 1.2.2.1.1. Males (kg) = 50 kg + [2.3 kg X (each inch over 5 feet)]. 1.2.2.1.2. Females (kg) = 45.5 kg + [2.3 kg X (each inch over 5 feet)].
1.2.2.2. Calculate Total Body Water (TBW) 1.2.2.2.1. Nonelderly (<65 yrs) males TBW (L)= 0.6 X IBW 1.2.2.2.2. Nonelderly (<65 yrs) females and elderly (≥65 yrs) males TBW (L)= 0.5 X
IBW 1.2.2.2.3. Elderly (≥65 yrs) females TBW (L)= 0.45 X IBW
1.2.2.3. Calculate Serum Sodium Deficit 1.2.2.3.1. Target serum sodium concentration (mmol/L) – actual serum sodium
concentration (mmol/L) 1.2.2.4. Calculate Amount of Sodium Chloride Required (mmol)
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
3
1.2.2.4.1. Serum sodium deficit (mmol/L) X TBW (L) 1.2.2.5. See Appendix A for additional useful calculations
1.2.3. Available intravenous sodium chloride solutions for treating hyponatremia:
Table 1. Intravenous Sodium Chloride Solutions
Solution Solution Na+ (mmol/L) Tonicity (mOsm/L)
3% Sodium Chloride 513 1026
1.8% Sodium Chloride 308 616
0.9% Sodium Chloride 154 308
0.45% Sodium Chloride 77 154
1.3. Administration - Refer to UW Health Adult and Pediatric IV Administration Clinical Practice Guidelines for appropriate rate of administration and level of care required
1.3.1. Sodium chloride 3% is a UWHC Level 3 medication which designates the nursing 1.3.2. A central line is preferred for administration of 3% sodium chloride to avoid
thrombophlebitis/extravasation. A central line is not required for 1.8% sodium chloride (Class I, Level of Evidence A).
25
1.3.3. In adult patients: Correction of symptomatic hyponatremia should occur at a rate that reverses the symptoms of hyponatremia, but should not be so rapid as to cause neurologic damage.
22 To help avoid possible myelinolysis and neurologic damage
especially in the chronically hyponatremic individuals,5 the rate of administration of
hypertonic sodium chloride should ideally be strictly controlled so that the serum sodium concentration is raised at the rate at which it fell (Class I, Level of Evidence A).
2,22,23
1.3.3.1. Acute onset of hyponatremia (<48 hours): raise serum sodium by 1 to 2 mmol/L/hr in the first 2 to 3 hours until symptoms abate (Class I, Level of Evidence A).
2,22,23
1.3.3.2. Chronic onset of hyponatremia (>48 hours or hyponatremia of unknown Duration): raise serum sodium by no more than 0.5 mmol/L/hr in the first 2 to 3 hours until symptoms abate (Class I, Level of Evidence A).
23,26
1.3.3.3. The maximum recommended rate of correction is ≤8 mmol/L/24 hrs (Class I, Level of Evidence A).
2,22
1.3.3.4. A typical initial rate of infusion of 3% sodium chloride is approximately 15 to 80 mL/hr (1mL/kg/hour) for 2 to 3 hours (Class I, Level of Evidence A).
22
1.3.3.5. The concurrent use of a loop diuretic (e.g. furosemide) is usually applied in nonhypovolemic patients to mandate free water excretion and to avoid treatment induced expansion of the extracellular fluid volume (Class I, Level of Evidence A).
2,22,23
1.3.3.6. Vasopressin antagonists are non-formulary at UWHC (e.g. tolvaptan, conivaptan).
1.3.4. In pediatric patients: Correction of symptomatic hyponatremia should occur at a rate that reverses the symptoms of hyponatremia and restores any intravascular fluid deficits but should not be so rapid as to cause neurologic damage.
22 To help avoid
possible myelinolysis and neurologic damage especially in the chronically hyponatremic individuals,
5 the rate of administration of hypertonic sodium chloride
should ideally be strictly controlled so that the serum sodium concentration is raised at the rate at which it fell (Class I, Level of Evidence A).
2
Hyponatremic seizures are a medical emergency and must be treated with HTS solution. In this situation, the serum sodium can be raised by as much as 4-8 mmol/L in the first hour or until the seizure activity ceases. Following this, the rate of 3% HTS
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
4
solution infusion should raise the plasma sodium by about 1 mmol/L per hour until either: 1) the patient is alert and seizure free; 2) the plasma sodium has increased by 20 mmol/L or 3) a serum sodium of about 125-130 mmol/L has been achieved, whichever occurs first (Class I, Level of Evidence A).
27
1.3.4.1. Assuming body water is 50% of weight, 1 mL/kg of 3% sodium chloride will increase the serum sodium concentration by 1 mmol/L.
27
1.3.5. The recommended indications for stopping rapid correction are:22
1.3.5.1. Cessation of life threatening manifestations (Class I, Level of Evidence A).2,22,23
1.3.5.2. Moderation of severe symptoms such as seizure, severe obtundation, coma, or respiratory arrest (Class I, Level of Evidence A).
2,22,23
1.3.5.3. Serum sodium concentration of 120 mmol/L or lower if the baseline serum sodium was <100 mmol/L (Class I, Level of Evidence A).
22
1.3.6. Serum sodium and serum potassium levels should be monitored every 1 to 4 hours during therapy (1 to 2 hours during initial increased rates of therapy). Ongoing gastrointestinal and/or urinary losses associated with diarrheal, cerebral, or nephrogenic sodium wasting syndromes should be monitored closely as well (Class I, Level of Evidence A).
2,22,23
2. Elevated Intracranial pressure (ICP)2.1. Indications
2.1.1. Management of life threatening intracranial hypertension with clinical/radiologic evidence of elevated ICP (>20 – 25 mmHg) secondary to brain edema (Class I, Level of Evidence A).
7,9,14,20,28
2.1.1.1. Patient with elevated ICP values as defined by an ICP monitor. 2.1.1.2. Cerebral edema or mass effect.
2.1.2. Inappropriate use includes treatment of increased ICPs in patients with elevated sodium levels (Class IIb, Level of Evidence B).
7,29
2.1.2.1.1. Serum Na+ >160 mmol/L* and/or serum Osmol >360 mOsm/L (*upon weighing risk and benefits of therapy, practitioners may wish to exceed serum Na+ of 160 mmol/L to control ICP; however, there is an increased risk for renal failure).
2.2. Dose 2.2.1. In adult patients: The goal serum sodium concentration is 150 to 160 mmol/L (Class
I, Level of Evidence B).7,30,31
2.2.1.1. Goal of hyperosmolar therapy for cerebral edema is to maintain serum osmolality levels in the 300 to 320 mOsm/L range, with allowance of the serum osmolality to reach 360 mOsm/L (Class I, Level of Evidence B).
7
2.2.2. In pediatric patients: The goal is to maintain ICP <20 mmHg, with allowance of the serum osmolality to reach 360 mOsm/L (Class I, Level of Evidence A).
32,33
2.2.3. Available sodium chloride solutions for the treatment of elevated ICP:
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]

5
Table 2. Intravenous Sodium Chloride Solutions
Solution Solution Na+ (mmol/L) Tonicity (mOsm/L)
7.5% Sodium Chloride (bolus only) 1274 2548
3% Sodium Chloride 513 1026
1.8% Sodium Chloride 308 616
0.9% Sodium Chloride 154 308
0.45% Sodium Chloride 77 154
2.3. Administration – 2.3.1. Refer to UW Health Adult and Pediatric IV Administration Clinical Practice Guidelines
for appropriate rate of administration and required level of care. 2.3.2. Sodium chloride 7.5% may only be initiated by a Neurosurgery ICU attending/chief or
Pediatric ICU attending/chief who is directly involved in the primary care of the patient or in a consultative manner by another attending.
2.4. Preparation 2.4.1. All doses of sodium chloride 7.5% will be patient specific and prepared and dispensed
from the central pharmacy with a maximum volume of 250mL per dose
2.4.2. In adult patients: 2.4.2.1. Sodium chloride 1.8% or 3% - Initiate infusion at 1 to 2 mL/kg/hr (administration
rate range: 75 to 150 mL/hr). A 250 mL bolus over 30 minutes may be administered if more aggressive therapy is desired (Class I, Level of Evidence B).
7,9,11,12
2.4.2.2. Sodium chloride 7.5% - A 2 mL/kg bolus over 30 minutes may be administered if more aggressive therapy is desired (Class IIb, Level of Evidence B).
15-17 Single
bolus doses are limited to a total volume of 250 mL.13,18
2.4.3. In pediatric patients: 2.4.3.1. Sodium chloride 3% - Administer 3% sodium chloride infusion in a range
between 0.1 and 1 mL/kg/hr (Class I, Level of Evidence A).32
A 3 to 5 mL/kgbolus may be given over 30 minutes if more aggressive therapy is desired (Class IIa, Level of Evidence B).
34 Sodium chloride 1.8% may be used in place
of 3% sodium chloride (Class IIa, Level of Evidence C). 2.4.3.2. Sodium chloride 7.5% - Dose has not been established. Use may be approved
by pediatric ICU attending/chief (Class III, Level of Evidence C).
2.4.4. A central line is preferred for administration of 3% sodium chloride and 7.5% sodium chloride boluses to avoid thrombophlebitis/ extravasation (Class I, Level of Evidence A).
25
3. Monitoring3.1. During therapy de-escalation and discontinuation, caution must be taken to avert rebound
hyponatremia and cerebral edema. Consider weaning HTS therapy over 24 to 48 hours (Class I, Level of Evidence B).
7
3.2. Serum sodium every 1 to 8 hours with monitoring occurring every 1 to 4 hours during initial increased rates of therapy (Class I, Level of Evidence A).
2,7,22,23
3.3. Other electrolytes including potassium, bicarbonate, chloride and magnesium, and parameters of renal function including BUN and serum creatinine levels. Measurement of ongoing sodium losses in the urine should be monitored as well if cerebral salt-wasting syndrome is a consideration (Class I, Level of Evidence A).
2,7,22,23
3.4. Fluid balance such as intake and output (Class I, Level of Evidence A).2,7,22,23
3.5. Acid-base balance (Class I, Level of Evidence A).2,7,22,23
3.6. Symptoms of hyponatremia (Class I, Level of Evidence A).2,7,22,23
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]

6
3.7. Neurologic symptoms associated with myelinolysis: mutism, dysarthria, lethargy, affective changes, spastic quadriparesis, pseudobulbar palsy, papillary and oculomotor abnormalities, depressed level of consciousness, ataxia, irregular behavior, and movement disorders (Class I, Level of Evidence A).
2,4,7,22,23
3.8. Intracranial pressure monitor if used for intracranial hypertension (Class I, Level of Evidence B).
7
3.9. With continued therapy for the treatment of elevated ICP, chest radiographs are recommended at least once daily to look for evidence of pulmonary edema. (Class I, Level of Evidence B).
7
4. Cautions/Warnings4.1. Too rapid of serum sodium correction and/or over-correction to hypernatremia can lead to
myelinolysis and permanent neurologic damage (Class III, Level of Evidence A).4
4.1.1. The risk of myelinolysis is higher for patients with chronic hyponatremia (Class III, Level of Evidence A).
5,32
4.2. Use with caution in patients with congestive heart failure, pulmonary edema, cirrhosis of the liver, renal failure, urinary tract obstruction or in any clinical state in which there exists edema and sodium retention (Class I, Level of Evidence A).
2,7,22,23
4.3. The risk of thrombophlebitis/extravasation exists with use of hypertonic solutions. A central line preferred for administration of 3% sodium chloride and 7.5% sodium chloride boluses (Class I, Level of Evidence A).
25,34
5. Drug Interactions5.1. Use caution in patients receiving drugs that can cause sodium retention or increase water
clearance (e.g. corticosteroids and mannitol) (Class IIb, Level of Evidence C). 5.2. Use caution in patients receiving drugs that contain high amounts of sodium (e.g. nafcillin,
ampicillin, sodium polystyrene sulfonate) as well as other potentially hidden sources of sodium (enteral feeds and total parenteral nutrition) (Class IIb, Level of Evidence C).
New Recommendations The May 2013 revision included recommendations to add 7.5% HTS bolus for the treatment of elevated intracranial pressure in adults.
Pertinent UWHC Policies & Procedures 1. UWHC Adult IV Administration Guidelines2. UWHC Pediatric IV Administration Guidelines
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
7
Intravenous Hypertonic Sodium Chloride – Adult and Pediatric – Inpatient – Clinical Practice Guideline
A. Scope1. Guidance for the use of intravenous hypertonic sodium chloride in UWHC adult and pediatric
inpatients.
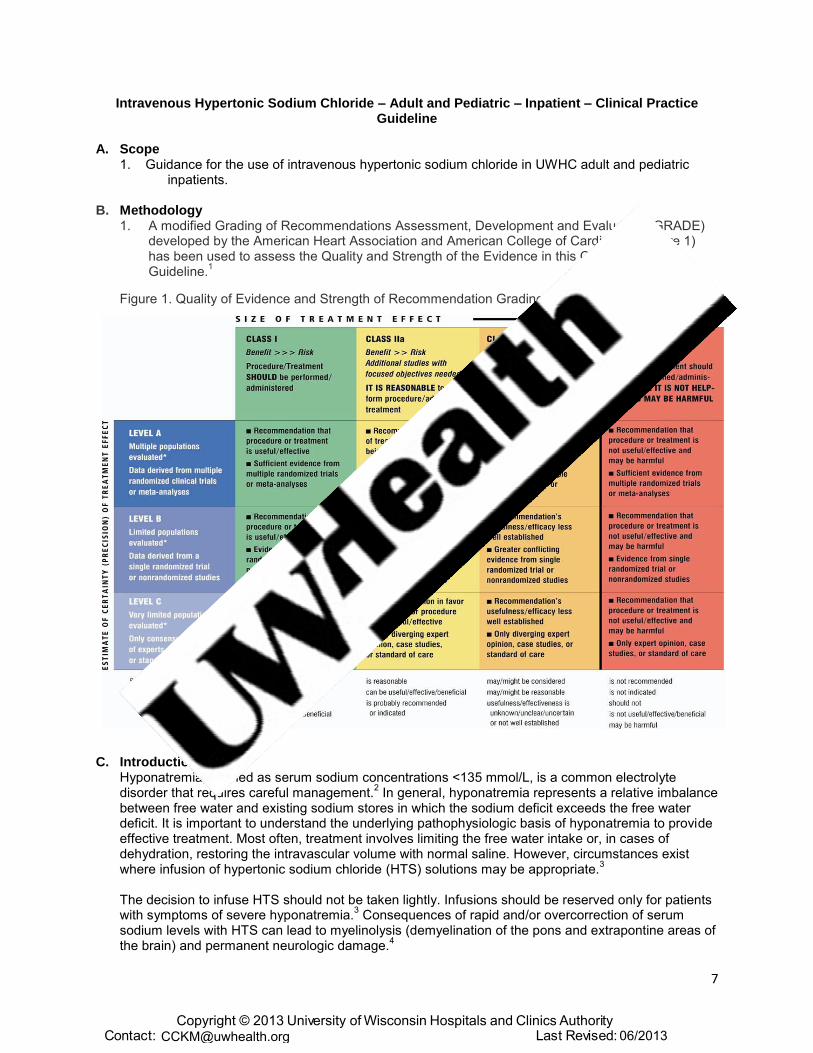
B. Methodology1. A modified Grading of Recommendations Assessment, Development and Evaluation (GRADE)
developed by the American Heart Association and American College of Cardiology (Figure 1)has been used to assess the Quality and Strength of the Evidence in this Clinical PracticeGuideline.
1
Figure 1. Quality of Evidence and Strength of Recommendation Grading Matrix
C. IntroductionHyponatremia, defined as serum sodium concentrations <135 mmol/L, is a common electrolytedisorder that requires careful management.
2 In general, hyponatremia represents a relative imbalance
between free water and existing sodium stores in which the sodium deficit exceeds the free waterdeficit. It is important to understand the underlying pathophysiologic basis of hyponatremia to provideeffective treatment. Most often, treatment involves limiting the free water intake or, in cases ofdehydration, restoring the intravascular volume with normal saline. However, circumstances existwhere infusion of hypertonic sodium chloride (HTS) solutions may be appropriate.
3
The decision to infuse HTS should not be taken lightly. Infusions should be reserved only for patients with symptoms of severe hyponatremia.
3 Consequences of rapid and/or overcorrection of serum
sodium levels with HTS can lead to myelinolysis (demyelination of the pons and extrapontine areas of the brain) and permanent neurologic damage.
4
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
8
Nevertheless, acute, symptomatic, severe hyponatremia is a serious medical condition that may lead to changes in brain cell volume which ultimately may lead to seizures, brain herniation, death, or irreversible brain damage.
5 Symptoms are generally neurologic in nature. Malaise, weakness, and
nausea are commonly the earliest findings when sodium concentrations fall below 125 to 130 mmol/L followed by headache, lethargy, muscle cramps, restlessness, encephalopathy, respiratory failure, arrhythmias and obtundation. Severe symptoms such as seizure, coma, respiratory arrest and death can occur when serum sodium concentrations reach <115 to 120 mmol/L.
6
In addition to management of hyponatremia, HTS has demonstrated efficacy in the management of elevated intracranial pressure (ICP). Elevated ICP is encountered frequently in patients requiring neurologic intensive care.
7 The Brain Trauma Foundation recommends treating elevated ICP above
20 to 25 mmHg. Elevated ICP (>20 mmHg) may reduce cerebral blood flow, thus resulting in significant morbidity.
8 Recently, HTS has been introduced as an option for treating elevated ICP. HTS
exerts its effect primarily through establishing an osmotic gradient between intravascular spaces and the cerebral tissue. This allows water to move from the cerebral intracellular and interstitial spaces into the capillaries, thereby reducing cerebral water content and the ICP.
9
There is no consensus on the most optimal route or concentration of HTS for treatment of elevated ICP, because all concentrations, administered via bolus or continuous infusion, appear to demonstrate favorable effects on ICP.
9-21 In order to minimize the risk associated with use of
concentrated electrolytes, only 3% and 7.5% HTS are available at UWHC.
D. Recommendations1. Hyponatremia
1.1. Indications1.1.1. Management of symptoms of severe hypotonic hyponatremia (Class I, Level of
Evidence A).2,22,23
1.1.2. Management of severe sodium chloride depletion when rapid electrolyte restoration is essential due to ongoing sodium losses (Class I, Level of Evidence A).
2,22
1.1.3. Inappropriate use includes treatment of asymptomatic hyponatremia without ongoing losses (Class III, Level of Evidence A).
23
1.2. Dose 1.2.1. An initial goal serum sodium concentration must be established.
1.2.1.1. Symptoms of severe hyponatremia: goal of 120 mmol/L initially followed by slower correction to approximately 130 mmol/L over the following several days. Initial goal serum sodium level should be lower if the baseline serum sodium is <100 mmol/L.
22
1.2.2. Calculate sodium deficit for patients with hyponatremia (Class I, Level of Evidence A):
2,22,24
1.2.2.1. Calculate Ideal Body Weight 1.2.2.1.1. Males (kg) = 50 kg + [2.3 kg X (each inch over 5 feet)]. 1.2.2.1.2. Females (kg) = 45.5 kg + [2.3 kg X (each inch over 5 feet)].
1.2.2.2. Calculate Total Body Water (TBW) 1.2.2.2.1. Nonelderly (<65 yrs) males TBW (L)= 0.6 X IBW 1.2.2.2.2. Nonelderly (<65 yrs) females and elderly (≥65 yrs) males TBW (L)= 0.5 X
IBW 1.2.2.2.3. Elderly (≥65 yrs) females TBW (L)= 0.45 X IBW
1.2.2.3. Calculate Serum Sodium Deficit 1.2.2.3.1. Target serum sodium concentration (mmol/L) – actual serum sodium
concentration (mmol/L) 1.2.2.4. Calculate Amount of Sodium Chloride Required (mmol)
1.2.2.4.1. Serum sodium deficit (mmol/L) X TBW (L)
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
9
1.2.2.5. See Appendix A for additional useful calculations
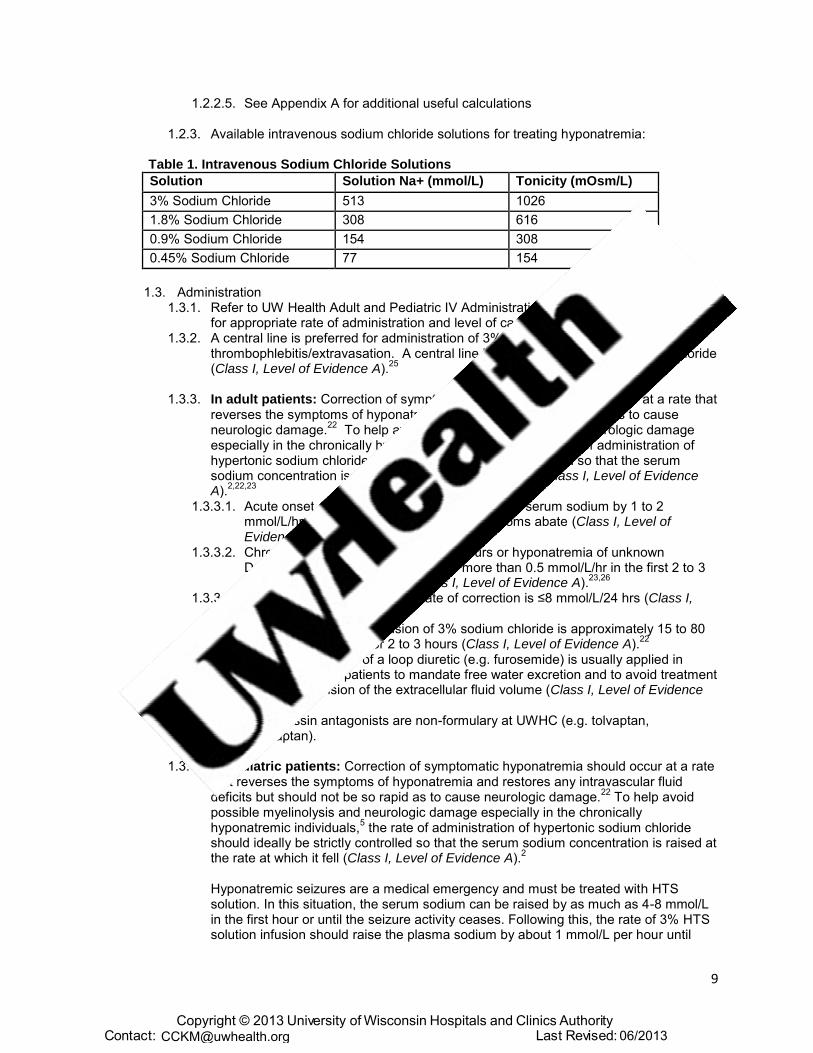
1.2.3. Available intravenous sodium chloride solutions for treating hyponatremia:
Table 1. Intravenous Sodium Chloride Solutions
Solution Solution Na+ (mmol/L) Tonicity (mOsm/L)
3% Sodium Chloride 513 1026
1.8% Sodium Chloride 308 616
0.9% Sodium Chloride 154 308
0.45% Sodium Chloride 77 154
1.3. Administration 1.3.1. Refer to UW Health Adult and Pediatric IV Administration Clinical Practice Guidelines
for appropriate rate of administration and level of care required. 1.3.2. A central line is preferred for administration of 3% sodium chloride to avoid
thrombophlebitis/extravasation. A central line is not required for 1.8% sodium chloride (Class I, Level of Evidence A).
25
1.3.3. In adult patients: Correction of symptomatic hyponatremia should occur at a rate that reverses the symptoms of hyponatremia, but should not be so rapid as to cause neurologic damage.
22 To help avoid possible myelinolysis and neurologic damage
especially in the chronically hyponatremic individuals,5 the rate of administration of
hypertonic sodium chloride should ideally be strictly controlled so that the serum sodium concentration is raised at the rate at which it fell (Class I, Level of Evidence A).
2,22,23
1.3.3.1. Acute onset of hyponatremia (<48 hours): raise serum sodium by 1 to 2 mmol/L/hr in the first 2 to 3 hours until symptoms abate (Class I, Level of Evidence A).
2,22,23
1.3.3.2. Chronic onset of hyponatremia (>48 hours or hyponatremia of unknown Duration): raise serum sodium by no more than 0.5 mmol/L/hr in the first 2 to 3 hours until symptoms abate (Class I, Level of Evidence A).
23,26
1.3.3.3. The maximum recommended rate of correction is ≤8 mmol/L/24 hrs (Class I, Level of Evidence A).
2,22
1.3.3.4. A typical initial rate of infusion of 3% sodium chloride is approximately 15 to 80 mL/hr (1mL/kg/hour) for 2 to 3 hours (Class I, Level of Evidence A).
22
1.3.3.5. The concurrent use of a loop diuretic (e.g. furosemide) is usually applied in nonhypovolemic patients to mandate free water excretion and to avoid treatment induced expansion of the extracellular fluid volume (Class I, Level of Evidence A).
2,22,23
1.3.3.6. Vasopressin antagonists are non-formulary at UWHC (e.g. tolvaptan, conivaptan).
1.3.4. In pediatric patients: Correction of symptomatic hyponatremia should occur at a rate that reverses the symptoms of hyponatremia and restores any intravascular fluid deficits but should not be so rapid as to cause neurologic damage.
22 To help avoid
possible myelinolysis and neurologic damage especially in the chronically hyponatremic individuals,
5 the rate of administration of hypertonic sodium chloride
should ideally be strictly controlled so that the serum sodium concentration is raised at the rate at which it fell (Class I, Level of Evidence A).
2
Hyponatremic seizures are a medical emergency and must be treated with HTS solution. In this situation, the serum sodium can be raised by as much as 4-8 mmol/L in the first hour or until the seizure activity ceases. Following this, the rate of 3% HTS solution infusion should raise the plasma sodium by about 1 mmol/L per hour until
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]

10
either: 1) the patient is alert and seizure free; 2) the plasma sodium has increased by 20 mmol/L or 3) a serum sodium of about 125-130 mmol/L has been achieved, whichever occurs first (Class I, Level of Evidence A).
27
1.3.4.1. Assuming body water is 50% of weight, 1 mL/kg of 3% sodium chloride will increase the serum sodium concentration by 1 mmol/L.
27
1.3.5. The recommended indications for stopping rapid correction are:22
1.3.5.1. Cessation of life threatening manifestations (Class I, Level of Evidence A).2,22,23
1.3.5.2. Moderation of severe symptoms such as seizure, severe obtundation, coma, or respiratory arrest (Class I, Level of Evidence A).
2,22,23
1.3.5.3. Serum sodium concentration of 120 mmol/L or lower if the baseline serum sodium was <100 mmol/L (Class I, Level of Evidence A).
22
1.3.6. Serum sodium and serum potassium levels should be monitored every 1 to 4 hours during therapy (1 to 2 hours during initial increased rates of therapy). Ongoing gastrointestinal and/or urinary losses associated with diarrheal, cerebral, or nephrogenic sodium wasting syndromes should be monitored closely as well (Class I, Level of Evidence A).
2,22,23
2. Elevated Intracranial pressure (ICP)2.1. Indications
2.1.1. Management of life threatening intracranial hypertension with clinical/radiologic evidence of elevated ICP (>20 – 25 mmHg) secondary to brain edema (Class I, Level of Evidence A).
7,9,14,20,28
2.1.1.1. Patient with elevated ICP values as defined by an ICP monitor. 2.1.1.2. Cerebral edema or mass effect.
2.1.2. Inappropriate use includes treatment of increased ICPs in patients with elevated sodium levels (Class IIb, Level of Evidence B).
7,29
2.1.2.1.1. Serum Na+ >160 mmol/L* and/or serum Osmol >360 mOsm/L (*upon weighing risk and benefits of therapy, practitioners may wish to exceed serum Na+ of 160 mmol/L to control ICP; however, there is an increased risk for renal failure).
2.2. Dose 2.2.1. In adult patients: The goal serum sodium concentration is 150 to 160 mmol/L (Class
I, Level of Evidence B).7,30,31
2.2.1.1. Goal of hyperosmolar therapy for cerebral edema is to maintain serum osmolality levels in the 300 to 320 mOsm/L range, with allowance of the serum osmolality to reach 360 mOsm/L (Class I, Level of Evidence B).
7
2.2.2. In pediatric patients: The goal is to maintain ICP <20 mmHg, with allowance of the serum osmolality to reach 360 mOsm/L (Class I, Level of Evidence A).
32,33
2.2.3. Available sodium chloride solutions for the treatment of elevated ICP:
Table 2. Intravenous Sodium Chloride Solutions
Solution Solution Na+ (mmol/L) Tonicity (mOsm/L)
7.5% Sodium Chloride (bolus only) 1274 2548
3% Sodium Chloride 513 1026
1.8% Sodium Chloride 308 616
0.9% Sodium Chloride 154 308
0.45% Sodium Chloride 77 154
2.3. Administration 2.3.1. Refer to UW Health Adult and Pediatric IV Administration Clinical Practice Guidelines
for appropriate rate of administration and level of care required.
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
11
2.3.2. Sodium chloride 7.5% may only be initiated by a Neurosurgery ICU attending/chief or Pediatric ICU attending/chief who is directly involved in the primary care of the patient or in a consultative manner by another attending.
2.4. Preparation 2.4.1. All doses of sodium chloride 7.5% will be patient specific and prepared and dispensed
from the central pharmacy with a maximum volume of 250mL per dose
2.4.2. In adult patients: 2.4.2.1. Sodium chloride 1.8% or 3% - Initiate infusion at 1 to 2 mL/kg/hr (administration
rate range: 75 to 150 mL/hr). A 250 mL bolus over 30 minutes may be administered if more aggressive therapy is desired (Class I, Level of Evidence B).
7,9,11,12
2.4.2.2. Sodium chloride 7.5% - A 2 mL/kg bolus over 30 minutes may be administered if more aggressive therapy is desired (Class IIb, Level of Evidence B).
15-17 Single
bolus doses are limited to a total volume of 250 mL.13,18
2.4.3. In pediatric patients: 2.4.3.1. Sodium chloride 3% - Administer 3% sodium chloride infusion in a range
between 0.1 and 1 mL/kg/hr (Class I, Level of Evidence A).32
A 3 to 5 mL/kgbolus may be given over 30 minutes if more aggressive therapy is desired (Class IIa, Level of Evidence B).
34 Sodium chloride 1.8% may be used in place
of 3% sodium chloride (Class IIa, Level of Evidence C). 2.4.3.2. Sodium chloride 7.5% - Dose has not been established. Use may be approved
by pediatric ICU attending/chief (Class III, Level of Evidence C).
2.4.4. A central line is preferred for administration of 3% sodium chloride and 7.5% sodium chloride boluses to avoid thrombophlebitis/ extravasation (Class I, Level of Evidence A).
25
3. Monitoring3.1. During therapy de-escalation and discontinuation, caution must be taken to avert rebound
hyponatremia and cerebral edema. Consider weaning HTS therapy over 24 to 48 hours (Class I, Level of Evidence B).
7
3.2. Serum sodium every 1 to 8 hours with monitoring occurring every 1 to 4 hours during initial increased rates of therapy (Class I, Level of Evidence A).
2,7,22,23
3.3. Other electrolytes including potassium, bicarbonate, chloride and magnesium, and parameters of renal function including BUN and serum creatinine levels. Measurement of ongoing sodium losses in the urine should be monitored as well if cerebral salt-wasting syndrome is a consideration (Class I, Level of Evidence A).
2,7,22,23
3.4. Fluid balance such as intake and output (Class I, Level of Evidence A).2,7,22,23
3.5. Acid-base balance (Class I, Level of Evidence A).2,7,22,23
3.6. Symptoms of hyponatremia (Class I, Level of Evidence A).2,7,22,23
3.7. Neurologic symptoms associated with myelinolysis: mutism, dysarthria, lethargy, affective changes, spastic quadriparesis, pseudobulbar palsy, papillary and oculomotor abnormalities, depressed level of consciousness, ataxia, irregular behavior, and movement disorders (Class I, Level of Evidence A).
2,4,7,22,23
3.8. Intracranial pressure monitor if used for intracranial hypertension (Class I, Level of Evidence B).
7
3.9. With continued therapy for the treatment of elevated ICP, chest radiographs are recommended at least once daily to look for evidence of pulmonary edema. (Class I, Level of Evidence B).
7
4. Cautions/Warnings4.1. Too rapid of serum sodium correction and/or over-correction to hypernatremia can lead to
myelinolysis and permanent neurologic damage (Class III, Level of Evidence A).4
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
12
4.1.1. The risk of myelinolysis is higher for patients with chronic hyponatremia (Class III, Level of Evidence A).
5,32
4.2. Use with caution in patients with congestive heart failure, pulmonary edema, cirrhosis of the liver, renal failure, urinary tract obstruction or in any clinical state in which there exists edema and sodium retention (Class I, Level of Evidence A).
2,7,22,23
4.3. The risk of thrombophlebitis/extravasation exists with use of hypertonic solutions. A central line preferred for administration of 3% sodium chloride and 7.5% sodium chloride boluses (Class I, Level of Evidence A).
25,34
5. Drug Interactions5.1. Use caution in patients receiving drugs that can cause sodium retention or increase water
clearance (e.g. corticosteroids and mannitol) (Class IIb, Level of Evidence C). 5.2. Use caution in patients receiving drugs that contain high amounts of sodium (e.g. nafcillin,
ampicillin, sodium polystyrene sulfonate) as well as other potentially hidden sources of sodium (enteral feeds and total parenteral nutrition) (Class IIb, Level of Evidence C).
E. Internal References1. UWHC Adult IV Administration Guidelines2. UWHC Pediatric IV Administration Guidelines
F. External References1. Tricoci P, Allen JM, Kramer JM, Califf RM, Smith SC, Jr. Scientific evidence underlying the
ACC/AHA clinical practice guidelines. JAMA. Vol 301. United States2009:831-841.2. Palmer BF, Gates JR, Lader M. Causes and management of hyponatremia. Ann Pharmacother.
Nov 2003;37(11):1694-1702.3. Culpepper RM, Clements BD, Pence SR. Hypertonic saline: patterns of and guidelines for use.
South Med J. Dec 1994;87(12):1203-1207.4. Laureno R, Karp BI. Myelinolysis after correction of hyponatremia. Ann Intern Med. Jan 1
1997;126(1):57-62.5. Oh MS, Kim HJ, Carroll HJ. Recommendations for treatment of symptomatic hyponatremia.
Nephron. 1995;70(2):143-150.6. Al-Salman J, Kemp D, Randall D. Hyponatremia. West J Med. May 2002;176(3):173-176.7. Bhardwaj A, Ulatowski JA. Cerebral Edema: Hypertonic Saline Solutions. Curr Treat Options
Neurol. Jul 1999;1(3):179-188.8. The Brain Trauma Foundation. The American Association of Neurological Surgeons. The Joint
Section on Neurotrauma and Critical Care. Use of mannitol. J Neurotrauma. Jun-Jul 2000;17(6-7):521-525.
9. Qureshi AI, Suarez JI, Bhardwaj A, et al. Use of hypertonic (3%) saline/acetate infusion in thetreatment of cerebral edema: Effect on intracranial pressure and lateral displacement of the brain.Crit Care Med. Mar 1998;26(3):440-446.
10. Mortazavi MM, Romeo AK, Deep A, et al. Hypertonic saline for treating raised intracranialpressure: literature review with meta-analysis. J Neurosurg. Jan 2012;116(1):210-221.
11. De Vivo P, Del Gaudio A, Ciritella P, Puopolo M, Chiarotti F, Mastronardi E. Hypertonic salinesolution: a safe alternative to mannitol 18% in neurosurgery. Minerva Anestesiol. Sep2001;67(9):603-611.
12. Huang SJ, Chang L, Han YY, Lee YC, Tu YK. Efficacy and safety of hypertonic saline solutions inthe treatment of severe head injury. Surg Neurol. Vol 65. United States2006:539-546; discussion546.
13. Oddo M, Levine JM, Frangos S, et al. Effect of mannitol and hypertonic saline on cerebraloxygenation in patients with severe traumatic brain injury and refractory intracranial hypertension.J Neurol Neurosurg Psychiatry. Vol 80. England2009:916-920.
14. Kamel H, Navi BB, Nakagawa K, Hemphill JC, 3rd, Ko NU. Hypertonic saline versus mannitol forthe treatment of elevated intracranial pressure: a meta-analysis of randomized clinical trials. CritCare Med. Mar 2011;39(3):554-559.
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
13
15. Vialet R, Albanese J, Thomachot L, et al. Isovolume hypertonic solutes (sodium chloride ormannitol) in the treatment of refractory posttraumatic intracranial hypertension: 2 mL/kg 7.5%saline is more effective than 2 mL/kg 20% mannitol. Crit Care Med. Jun 2003;31(6):1683-1687.
16. Cottenceau V, Masson F, Mahamid E, et al. Comparison of effects of equiosmolar doses ofmannitol and hypertonic saline on cerebral blood flow and metabolism in traumatic brain injury. JNeurotrauma. Oct 2011;28(10):2003-2012.
17. Alsharkasy M, Altouny A, Elshatoury H, Ewila H. Comparison between Mannitol 20% andhypertonic saline 7.5% for cerebral resuscitation in severely head injured patients with intra-cranial hypertension. Int J Health Sci (Qassim). Jul 2011;5(2 Suppl 1):36-37.
18. Bulger EM, May S, Brasel KJ, et al. Out-of-hospital hypertonic resuscitation following severetraumatic brain injury: a randomized controlled trial. JAMA. Vol 304. United States2010:1455-1464.
19. Suarez JI, Qureshi AI, Bhardwaj A, et al. Treatment of refractory intracranial hypertension with23.4% saline. Crit Care Med. Jun 1998;26(6):1118-1122.
20. Rockswold GL, Solid CA, Paredes-Andrade E, Rockswold SB, Jancik JT, Quickel RR. Hypertonicsaline and its effect on intracranial pressure, cerebral perfusion pressure, and brain tissueoxygen. Neurosurgery. Vol 65. United States2009:1035-1041; discussion 1041-1032.
21. Ware ML, Nemani VM, Meeker M, Lee C, Morabito DJ, Manley GT. Effects of 23.4% sodiumchloride solution in reducing intracranial pressure in patients with traumatic brain injury: apreliminary study. Neurosurgery. Vol 57. United States2005:727-736; discussion 727-736.
22. Adrogue HJ, Madias NE. Hyponatremia. N Engl J Med. May 25 2000;342(21):1581-1589.23. Vaidya C, Ho W, Freda BJ. Management of hyponatremia: providing treatment and avoiding
harm. Cleve Clin J Med. Vol 77. United States2010:715-726.24. Adrogue HJ, Madias NE. Aiding fluid prescription for the dysnatremias. Intensive Care Med. Mar
1997;23(3):309-316.25. Zimmet SE. The prevention of cutaneous necrosis following extravasation of hypertonic saline
and sodium tetradecyl sulfate. J Dermatol Surg Oncol. Jul 1993;19(7):641-646.26. Ellis SJ. Severe hyponatraemia: complications and treatment. QJM. Dec 1995;88(12):905-909.27. Moritz ML, Ayus JC. Preventing neurological complications from dysnatremias in children. Pediatr
Nephrol. Dec 2005;20(12):1687-1700.28. Forsyth LL, Liu-DeRyke X, Parker D, Jr., Rhoney DH. Role of hypertonic saline for the
management of intracranial hypertension after stroke and traumatic brain injury.Pharmacotherapy. Apr 2008;28(4):469-484.
29. Paredes-Andrade E, Solid CA, Rockswold SB, Odland RM, Rockswold GL. Hypertonic salinereduces intracranial hypertension in the presence of high serum and cerebrospinal fluidosmolalities. Neurocrit Care. Oct 2012;17(2):204-210.
30. Martin RJ. Central pontine and extrapontine myelinolysis: the osmotic demyelination syndromes.J Neurol Neurosurg Psychiatry. Vol 75 Suppl 3. England2004:iii22-28.
31. Thongrong C, Kong N, Govindarajan B, Allen D, Mendel E, Bergese SD. Current Purpose andPractice of Hypertonic Saline in Neurosurgery: A Review of the Literature. World Neurosurg. Feb9 2013.
32. Adelson PD, Bratton SL, Carney NA, et al. Guidelines for the acute medical management ofsevere traumatic brain injury in infants, children, and adolescents. Chapter 11. Use ofhyperosmolar therapy in the management of severe pediatric traumatic brain injury. Pediatr CritCare Med. Jul 2003;4(3 Suppl):S40-44.
33. Dominguez TE, Priestley MA, Huh JW. Caution should be exercised when maintaining a serumsodium level >160 meq/L. Crit Care Med. Vol 32. United States2004:1438-1439; author reply1439-1440.
34. Brenkert TE, Estrada CM, McMorrow SP, Abramo TJ. Intravenous hypertonic saline use in thepediatric emergency department. Pediatr Emerg Care. Vol 29. United States2013:71-73.
G. Benefits/Harms of ImplementationImplementation of this guideline calls for the creation of a 7.5% HTS ERx in Health Link. Due to thehigh-alert status of the medication, 7.5% HTS requires special storage, handling, and check systemsto prevent potentially fatal errors. All doses of 7.5% HTS will be patient specific and prepared anddispensed from the central pharmacy utilizing 2.5mEq/mL NaCl.
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]
14
H. Implementation StrategyThe guideline was reviewed by pharmacy staff and then sent to adult and pediatric physicians forreview. After pharmacy and physician review, the guideline will be presented to the P & T committeefor approval.
I. Implementation Tools/Plan –1. A request will be sent to the Drug Product Supply and Selection Committee for approval2. Health link will have to be updated to include ERx for 7.5% HTS.
J. DisclaimerThis Clinical Practice Guideline provides an evidence-based approach for treatment of . It is understood that occasionally patients will not match the conditions considered in the guideline.
Copyright © 2013 University of Wisconsin Hospitals and Clinics AuthorityContact: Lee Vermeulen, [email protected] Last Revised: 06/[email protected]