
Intravenous Administration of Formul ary Medications ...
74
Intravenous Administration of Formul ary Medications - Pediatric/Neonatal - Inpatient/Ambulatory Clinical Practice Guideline Table of Contents Executive Summary............................................................................................................................................... 3 Scope ...................................................................................................................................................................... 4 Methodology........................................................................................................................................................... 4 Definitions .............................................................................................................................................................. 5 Introduction ............................................................................................................................................................ 5 Recommendations................................................................................................................................................. 6 UW Health Implementation ................................................................................................................................. 72 References............................................................................................................................................................ 72 Appendix A. Evidence Grading Scheme ........................................................................................................... 74 Appendix B. Medications Requiring Central Lines ......................................................................................... 75 Contact for Content and Changes: Philip Trapskin, Manager, Patient Care Services and Drug Policy Program Phone Number: (608) 263-1328 Email: [email protected] Guideline Authors: Joshua Vanderloo, PharmD Emily Zimmerman, PharmD Coordinating Team Members: Joshua Vanderloo, PharmD; Philip Trapskin, PharmD, BCPS Review Individuals/Bodies: AFCH Nursing Leadership: Barbara Byrne, VP AFCH Clinical Operations; Laura Ahola, Nurse Manager PUCU; Angela Baker, Nurse Manager NICU; Devon Christenson, Nurse Manager Diagnostic/Therapy Center; Carrie Cronk, Nurse Manager P4; Kirsten Koffarnus, CNS P5; Laura Konkol, CNS NICU; Kitty Montgomery, CNS P4; Anne Moseley, Director Pediatric Nursing; Sue Quamme, Nurse Manager PI44; Windy Smith, Nurse Manager P5 Deborah Soetenga, CNS PI44; Lori Williams, CNS PUCU Pharmacists; Brian LaRowe, PharmD; Nicole Lubcke, PharmD; Mary Mably, Pharmacy Coordinator Oncology, PharmD, BCOP; Aaron Steffenhagen, Pharmacy Manager Critical Care, PharmD, BCPS; Meghann Voegeli, Pharmacy Manager Pediatrics, PharmD Dan O’Connell, MD, Pediatric Gastroenterology Daniel Sklansky, MD, Hospitalist Benjamin Walker, MD, Pediatric Anesthesiology Effective 7/8/2021. Contact [email protected] for previous versions Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Transcript of Intravenous Administration of Formul ary Medications ...
Intravenous Administration of Formul
ary Medications - Pediatric/Neonatal - Inpatient/Ambulatory
Clinical Practice Guideline
Table of Contents Executive Summary ............................................................................................................................................... 3
Scope ...................................................................................................................................................................... 4
Methodology........................................................................................................................................................... 4 Definitions .............................................................................................................................................................. 5
Introduction ............................................................................................................................................................ 5
Recommendations ................................................................................................................................................. 6
UW Health Implementation ................................................................................................................................. 72
References............................................................................................................................................................ 72 Appendix A. Evidence Grading Scheme ........................................................................................................... 74
Appendix B. Medications Requiring Central Lines ......................................................................................... 75
Contact for Content and Changes: Philip Trapskin, Manager, Patient Care Services and Drug Policy Program Phone Number: (608) 263-1328 Email: [email protected]
Guideline Authors: Joshua Vanderloo, PharmD Emily Zimmerman, PharmD
Coordinating Team Members: Joshua Vanderloo, PharmD; Philip Trapskin, PharmD, BCPS
Review Individuals/Bodies: AFCH Nursing Leadership: Barbara Byrne, VP AFCH Clinical Operations; Laura Ahola, Nurse Manager PUCU; Angela Baker, Nurse Manager NICU; Devon Christenson, Nurse Manager Diagnostic/Therapy Center; Carrie Cronk, Nurse Manager P4; Kirsten Koffarnus, CNS P5; Laura Konkol, CNS NICU; Kitty Montgomery, CNS P4; Anne Moseley, Director Pediatric Nursing; Sue Quamme, Nurse Manager PI44; Windy Smith, Nurse Manager P5 Deborah Soetenga, CNS PI44; Lori Williams, CNS PUCU
Pharmacists; Brian LaRowe, PharmD; Nicole Lubcke, PharmD; Mary Mably, Pharmacy Coordinator Oncology, PharmD, BCOP; Aaron Steffenhagen, Pharmacy Manager Critical Care, PharmD, BCPS; Meghann Voegeli, Pharmacy Manager Pediatrics, PharmD
Dan O’Connell, MD, Pediatric Gastroenterology Daniel Sklansky, MD, Hospitalist Benjamin Walker, MD, Pediatric Anesthesiology
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Committee Approvals/Dates: Pharmacy and Therapeutics Committee (Last Periodic Review: September 2014)
• Interim Revisions: November 2014, January 2015, September 2015, Novemeber 2015, November 2017, December 2017, January 2018
Release Date: October 2016 Next Review Date: October 2018 Executive Summary Guideline Overview This guideline directs the appropriate administration of intravenous medications to pediatric patients across UWHealth throughout inpatient, procedural, and ambulatory settings. Necessary elements include appropriate level of care, monitoring, and physicochemical considerations. There are many medications given intravenously both in inpatient settings, procedural areas, or ambulatory care settings. The purpose of this guideline is to provide guidance for the administration of intravenous medications to pediatric patients across these care settings. The medications in this guideline were chosen based on their inclusion in the UWHC medication formulary and the units were administration is appropriate. These administration guidelines are not absolute; administration of intravenous medications should be tailored to fit the therapeutic needs of a pediatric patient as appropriate. Key Revisions January 2018 Minor Revision
• Addition of siltuximab December 2017 Minor Revision
• Midazolam use in general care areas for prolonged epilepsy monitoring November 2017 Minor Revision
• Addition of guidance for rapid infusion of infliximab 2016 Periodic Review
• Addition of new intravenous medications since previous September 2014 revision: ethacrynic acid, tocilizumab, isavuconazole, eculizumab, C1 esterase inhibitor (CINRYZE®), peramivir, levofloxacin, dinutuximab, doripenem, laronidase, granisetron, sugammadex, vedolizumab, lacosamide, defibrotide, daratumumab, vincristine
• Clarification of magnesium administration rates for repletion, torsades de pointes, and bronchospasm • Addition of appendix detailing medications requiring central line
Key Practice Recommendations The guideline includes recommendations for UWHealth formulary intravenous medications with respect to recommended infusion rates, considereations for administration, and monitoring of medications with administration. See table in Recommendations section for information on specific medications. Companion Documents
• Guideline for the Management of Extravasation of Chemotherapeutic Agents – Adult/Pediatric – Inpatient/Ambulatory Clinical Practice Guideline
• Guideline for Non-chemotherapeutic Agents: Prevention and Treatment of Chemical Phlebitis and Extravasation of Peripherally Administered Non-chemotherapeutic Agents – Adult and Pediatric – Inpatient Clinical Practice Guideline
• Acetylcysteine (N-Acetylcysteine) – Pediatric/Adult – Inpatient Clinical Practice Guideline • Procoagulant Therapy for Treatment of Non-Hemophiliac Bleeding – Adult Clinical Practice Guideline • Granulocyte Colony Stimulating Factor – Adult/Pediatric – Inpatient Clinical Practice Guideline • Fosphenytoin and Phenytoin – Adult and Pediatric – Inpatient Clinical Practice Guideline • Therapeutic Dosing of Unfractionated Heparin – Pediatric/Neonatal – Inpatient Clinical Practice Guideline • Intravenous Immunoglobulin (IVIG) – Adult/Pediatric – Inpatient /Ambulatory Clinical Practice Guideline • High-dose Methotrexate, Leucovorin, and Glucarpidase Dosing, Administration, and Monitoring –
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Adult/Pediatric Intpatient Clinical Practice Guideline • Use of Rasburicase – Adult and Pediatric – Inpatient Clinical Practice Guideline • Intravenous Hypertonic Sodium Chloride – Adult and Pediatric – Inpatient Clinical Practice Guideline
Pertinent UWHC Policies and Procedures
• Policy 8.31 Guidelines for Hospital Location Specific Administration of IV Medications • Policy 8.33 High Alert Medication Administration • Policy 8.56 Pediatric Sedation • Policy 6.1.11 Preventing Non-therapeutic Exposure to Hazardous Drugs • Factor 7a Recombinant Operating Procedure • Factor 9 Complex Concentrate (PCC) Operating Procedure • Policy 10.18 Parenteral Lidocaine for Neuropathic Pain
Scope Disease/Condition: Intravenous medication administration Extravasation of medications is not addressed in this guideline. For this information, refer to:
• UWHC Guidelines for the Management of Extravasation of Chemotherapeutic Agents – Adult/Pediatric – Inpatient/Ambulatory Clinical Practice Guideline
• Guideline for Non-chemotherapeutic Agents: Prevention and Treatment of Chemical Phlebitis and Extravasation of Peripherally Administered Non-chemotherapeutic Agents – Adult and Pediatric – Inpatient Clinical Practice Guideline
Clinical Specialty: This guideline is intended for all personnel authorized to prescribe, to monitor, or to administer intravenous medications in all clinical specialties of pediatric practice. Intended Users: Physicians, advanced practice providers, pharmacists, and nurses Objective: To provide guidelines and monitoring parameters for the intravenous administration of UWHC formulary medications to pediatric patient. Target Population: Pediatric patients requiring intravenous medications. Interventions and Practices Considered:
• Physiochemical properties of intravenous medications • Appropriate administration technique • Safe and effective dosing and administration rates • Key monitoring parameters for intravenous medications
Major Outcomes Considered:
• Safe and standardized administration of intravenous medications to prevent patient harm. Methodology Methods Used to Collect/Select the Evidence Electronic database searches, literature review,manufacturer labeling and tertiary care references were used to collect evidence for review. Methods Used to Formulate the Recommendations Available evidence from the literature, manufacturer labeling and tertiary references was combined to formulate recommendations. Clinical expert consensus was utilized to formulate specific recommendations and levels of care for administration.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Methods Used to Assess the Quality and Strength of the Evidence Internally developed recommendations, or those adopted from external sources without an assigned evidence grade, were evaluated by the guideline workgroup using and algorithm adapted from the Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology (see Figure 1 in Appendix A).1 Cost Analysis: No formal cost analysis was performed. Recognition of Potential Health Care Disparities: No health care disparities were identified. Definitions 1.0 IV administration routes and lines
1.1 Central: intravenous medication to be administered through a central IV line 1.1.1 A central line placed 1.1.2 Some medications cannot be administered through a peripheral IV line due to osmolarity of
the drug or risk of vein irritation. A patient must have a central line available to receive these medications.
1.2 Peripheral: intravenous medication to be administered through a peripheral IV line 1.2.1 Mildline catheters should not be used in pediatric patients based on Policy 1.55A Midline
Intravenous Midline Catheters 1.3 Vesicant: An agent that can produce local irritation, necrosis, and sloughing of tissues when
inadvertently injected into subcutaneous or muscle tissue during intravenous administration 1.3.1 Guideline for the Management of Extravasation of Chemotherapeutic Agents – Adult/Pediatric
– Inpatient/Ambulatory Clinical Practice Guideline 1.3.2 Guideline for Non-chemotherapeutic Agents: Prevention and Treatment of Chemical Phlebitis
and Extravasation of Peripherally Administered Non-chemotherapeutic Agents – Adult and Pediatric – Inpatient Clinical Practice Guideline
Introduction The following table presents guidelines and monitoring parameters for the intravenous administration of UWHC formulary drugs. Although some recommendations may exist to prevent serious toxicities, often the rates of administration or amount of diluent can be different provided appropriate precautions are taken. When using this table, tailor the guidelines to fit the patient’s total therapeutic needs. Use of this guideline is encouraged but is not a substitute for researching drugs with which you are not familiar.
If a specific patient’s fluid or dosing requirements do not fit within the guidelines presented, the following questions should be asked:
• What information exists regarding a faster rate (e.g., can cause hypotension, cardiac arrhythmias, etc.) or more concentrated dilutions (e.g., may cause thrombophlebitis, toxic peak blood concentrations, etc.)?
• What is the incidence of this adverse reaction (i.e., is the reaction rarely induced versus always induced)? • What is the benefit/ risk ratio in this particular patient? • What parameters could be monitored to decrease the risk of serious adverse effects? • What other special precautions could be taken?
In accordance with Administrative Policy 8.31, a level has been assigned to each medication to designate the nursing units on which the drug may be administered. If a patient is in the process of being transferred to an Intermediate Care Unit (IMC) or ICU and requires a level 3 or 4 medication, the medication can be ordered and initiated in the transition process. The levels are defined as follows:
• Level 1 medications: May be administered on all General Care Nursing Units.. • Level 2 medications: May be administered on General Nursing Units with telemetry including the
Pediatric Universal Care Unit, Pediatric Sedation, Hybrid Catheterization Lab, Day Treatment, and Campground.
• Level 3 medications: May be administered on Intermediate Care Units (IMC) and in Interventional Radiology. Each IMC is qualified to administer different Level III drugs based on specialty populations served.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
• Level 4 medications: May be administered on Intensive Care Units, the Emergency Department, Operating Room, Recovery Room, Medflight, Children’s Hospital Emergency Transport Ambulance (CHETA), the Diagnostic Pavilion (excluding Day Treatment). Interventional Radiology may monitor on-going infusions of Level 4 drugs based on appropriate competency assessment.
Administration of medications outside of indicated level on this guideline may occur if the unit nurse manager and pharmacist agree to deviate from this guideline in the interest of patient care. Some medications (e.g. benzodiazepenes) may be used for more than one indication (e.g. benzodiazepenes for anxiolysis or sedation). Areas of administration and monitoring requirements may differ based on what the medication is being used for and the table contained within this guideline should be referenced to guide use. Approved investigational protocols will detail specific administration guidelines and monitoring parameters. Chemotherapeutic agents may only be administered by nurses certified in chemotherapy and only on P4 and Day Treatment. Exceptions may be made where chemotherapy certified nurses go to another unit to administer chemotherapy, but only by prior agreement and when appropriate monitoring can be accomplished following chemotherapy. High-alert medications pose a heightened risk of causing significant patient harm or injury when administered in error and are noted in this guideline for convenience. Specific practices for high alert medications are included in Administrative Policy 8.33 High Alert Medication Administration. Recommendations All recommendations within this guideline have been given a UWHealth Strong Recommendation, Moderat Quality of Evidence recommendation based on information obtained from initial clinical trials of the medications, product package inserts, and drug databases.2 When available, specific recommendations for neonates is called out; this information is derived from Neofax.3 For adolescent patients weighing 40 kg or more, the Adult Intravenous Administration Guidelines may be reasonable to use for guidance of the administration of medications. (UWHealth Weak/conditional Recommendation,Very Low Quality of Evidence).
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
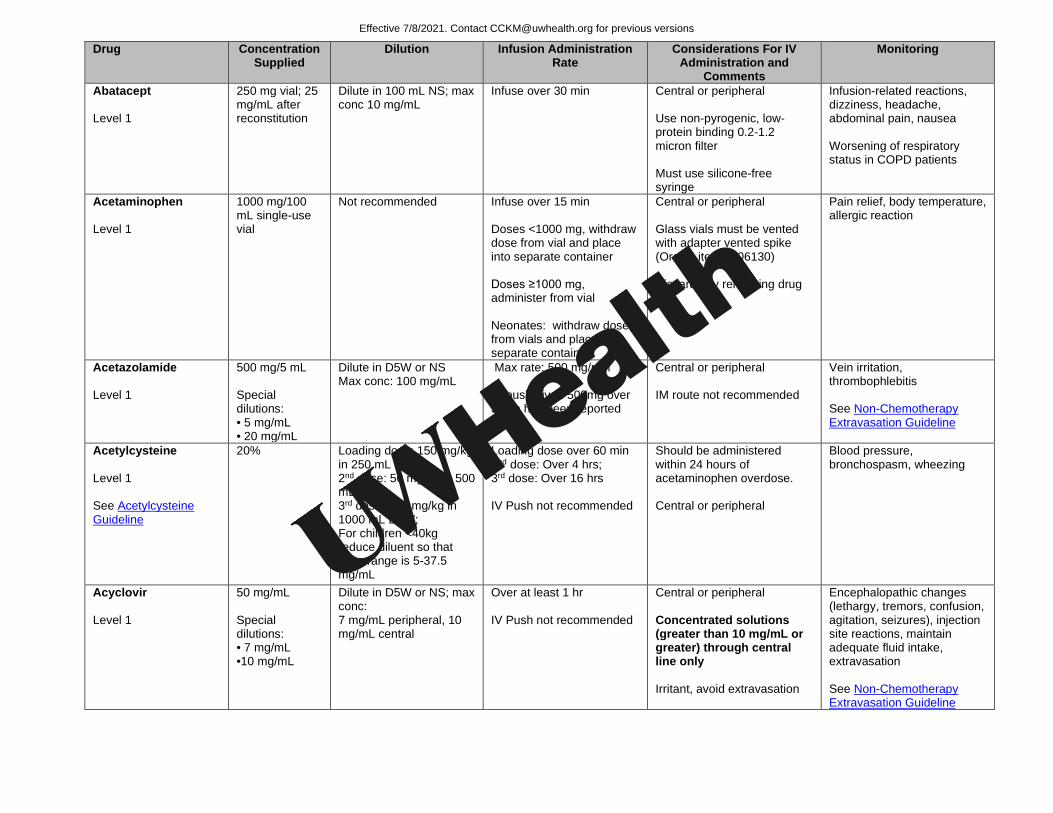
Abatacept Level 1
250 mg vial; 25 mg/mL after reconstitution
Dilute in 100 mL NS; max conc 10 mg/mL
Infuse over 30 min Central or peripheral Use non-pyrogenic, low-protein binding 0.2-1.2 micron filter Must use silicone-free syringe
Infusion-related reactions, dizziness, headache, abdominal pain, nausea Worsening of respiratory status in COPD patients
Acetaminophen Level 1
1000 mg/100 mL single-use vial
Not recommended Infuse over 15 min Doses <1000 mg, withdraw dose from vial and place into separate container Doses ≥1000 mg, administer from vial Neonates: withdraw dose from vials and place into separate container
Central or peripheral Glass vials must be vented with adapter vented spike (Oracle item 1006130) Discard any remaining drug
Pain relief, body temperature, allergic reaction
Acetazolamide Level 1
500 mg/5 mL Special dilutions: • 5 mg/mL • 20 mg/mL
Dilute in D5W or NS Max conc: 100 mg/mL
Max rate: 500 mg/min IV push given 500mg over 3 min has been reported
Central or peripheral IM route not recommended
Vein irritation, thrombophlebitis See Non-Chemotherapy Extravasation Guideline
Acetylcysteine Level 1 See Acetylcysteine Guideline
20% Loading dose: 150 mg/kg in 250 mL D5W; 2nd dose: 50 mg/kg in 500 mL D5W; 3rd dose: 100 mg/kg in 1000 mL D5W; For children <40kg reduce diluent so that conc range is 5-37.5 mg/mL
Loading dose over 60 min 2nd dose: Over 4 hrs; 3rd dose: Over 16 hrs IV Push not recommended
Should be administered within 24 hours of acetaminophen overdose. Central or peripheral
Blood pressure, bronchospasm, wheezing
Acyclovir Level 1
50 mg/mL Special dilutions: • 7 mg/mL •10 mg/mL
Dilute in D5W or NS; max conc: 7 mg/mL peripheral, 10 mg/mL central
Over at least 1 hr IV Push not recommended
Central or peripheral Concentrated solutions (greater than 10 mg/mL or greater) through central line only Irritant, avoid extravasation
Encephalopathic changes (lethargy, tremors, confusion, agitation, seizures), injection site reactions, maintain adequate fluid intake, extravasation See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
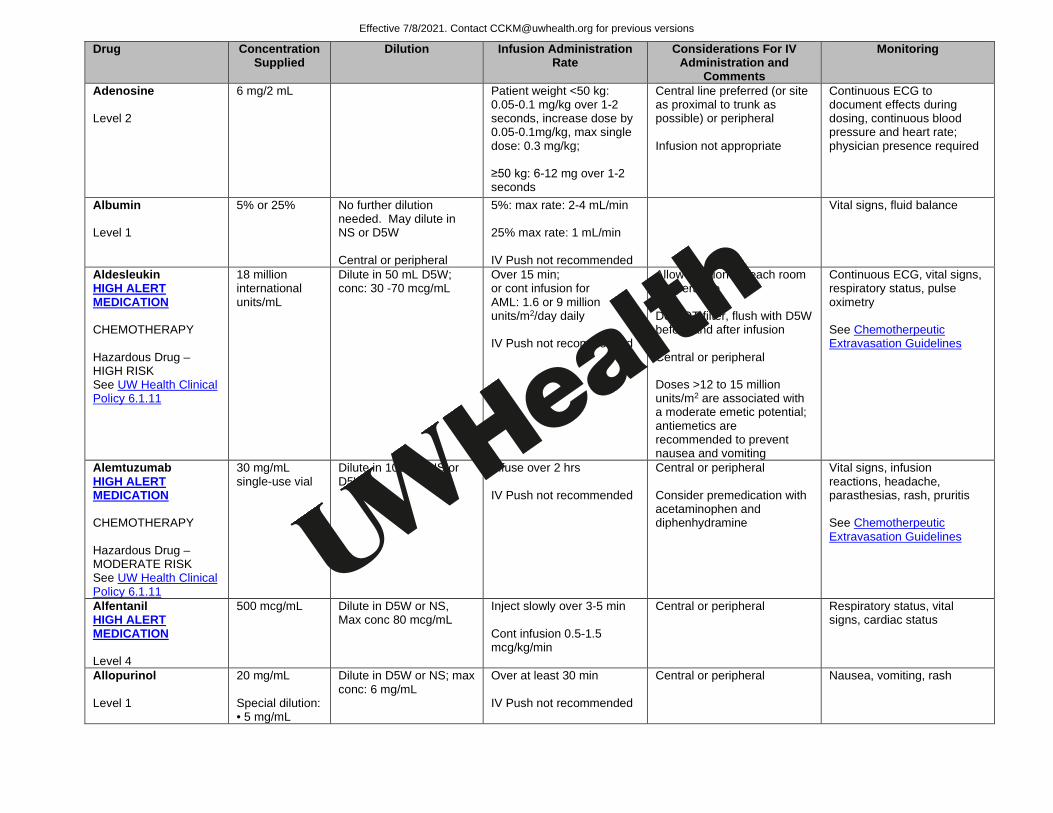
Adenosine Level 2
6 mg/2 mL Patient weight <50 kg: 0.05-0.1 mg/kg over 1-2 seconds, increase dose by 0.05-0.1mg/kg, max single dose: 0.3 mg/kg; ≥50 kg: 6-12 mg over 1-2 seconds
Central line preferred (or site as proximal to trunk as possible) or peripheral Infusion not appropriate
Continuous ECG to document effects during dosing, continuous blood pressure and heart rate; physician presence required
Albumin Level 1
5% or 25% No further dilution needed. May dilute in NS or D5W Central or peripheral
5%: max rate: 2-4 mL/min 25% max rate: 1 mL/min IV Push not recommended
Vital signs, fluid balance
Aldesleukin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
18 million international units/mL
Dilute in 50 mL D5W; conc: 30 -70 mcg/mL
Over 15 min; or cont infusion for AML: 1.6 or 9 million units/m2/day daily IV Push not recommended
Allow solution to reach room temperature Do NOT filter, flush with D5W before and after infusion Central or peripheral Doses >12 to 15 million units/m2 are associated with a moderate emetic potential; antiemetics are recommended to prevent nausea and vomiting
Continuous ECG, vital signs, respiratory status, pulse oximetry See Chemotherpeutic Extravasation Guidelines
Alemtuzumab HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
30 mg/mL single-use vial
Dilute in 100 mL NS or D5W
Infuse over 2 hrs IV Push not recommended
Central or peripheral Consider premedication with acetaminophen and diphenhydramine
Vital signs, infusion reactions, headache, parasthesias, rash, pruritis See Chemotherpeutic Extravasation Guidelines
Alfentanil HIGH ALERT MEDICATION Level 4
500 mcg/mL Dilute in D5W or NS, Max conc 80 mcg/mL
Inject slowly over 3-5 min Cont infusion 0.5-1.5 mcg/kg/min
Central or peripheral Respiratory status, vital signs, cardiac status
Allopurinol Level 1
20 mg/mL Special dilution: • 5 mg/mL
Dilute in D5W or NS; max conc: 6 mg/mL
Over at least 30 min IV Push not recommended
Central or peripheral Nausea, vomiting, rash
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Alpha1-Proteinase Inhibitor Level 1
25 mg/mL after reconstitution
No further dilution Infuse at 0.08 mL/kg/min Central or peripheral Vital signs, infusion reactions
Alprostadil HIGH ALERT MEDICATION– Continuous Infusion Level 4
500 mcg/mL Special dilution: • 5 mcg/mL • 10 mcg/mL • 20 mcg/mL
Pediatric max conc: 20 mcg/mL, use large vein Neonate max conc: 10 mcg/mL, use large vein of umbilical artery catheter placed at the ductus arteriosus
Neonates and infants: 0.05 to 0.1 mcg/kg/min. IV Push not recommended
After a therapeutic response is achieved, the infusion rate should be reduced to the lowest possible dosage that maintains the response; range: 0.01-0.4 mcg/kg/min Must change infusion syringe every 24 hours
Continuous respiratory status and cardiac status, vein irritation/ thrombophlebitis. Neonates: Apnea is seen most often in neonates weighing fewer than 2 kg at birth, and usually appears during the first hour of drug infusion Flushing of arm or face may indicate misplacement of catheter See Non-Chemotherapy Extravasation Guideline Also used perioperatively for liver transplant with different dosing regimen
Alteplase HIGH ALERT MEDICATION (excepting low-dose injections for line clearance) Level 4 Alteplase Flushes—Level 1
500 mcg/mL Special dilution: • 0.1 mg/mL • 0.2 mg/mL
No further dilution; or may dilute to 0.5 mg/mL in NS or 12.5 mg/250 mL for DVT pts with arterial or venous clots
Loading dose over 1 min; give remaining drug as infusion. Systemic thrombosis: 0.1-0.6 mg/kg/hr; titrated to effect, optimum dose unknown
Central or peripheral Catheter clearance – See Central Venous Access Device Occlusion Guideline
Signs/symptoms of bleeding, blood pressure every 15 minutes for 2 hours
Amikacin Sulfate Level 1
250 mg/mL Special dilution: • 5 mg/mL
Dilute in D5W or NS; max conc: 10 mg/mL Neonates Dilute to a final concentration of 2.5-5 mg/mL
Over 30 - 60 min Neonates Infuse over 60-120 min. IV Push not recommended
Central or peripheral Respiratory status, vitals, cardiac status
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
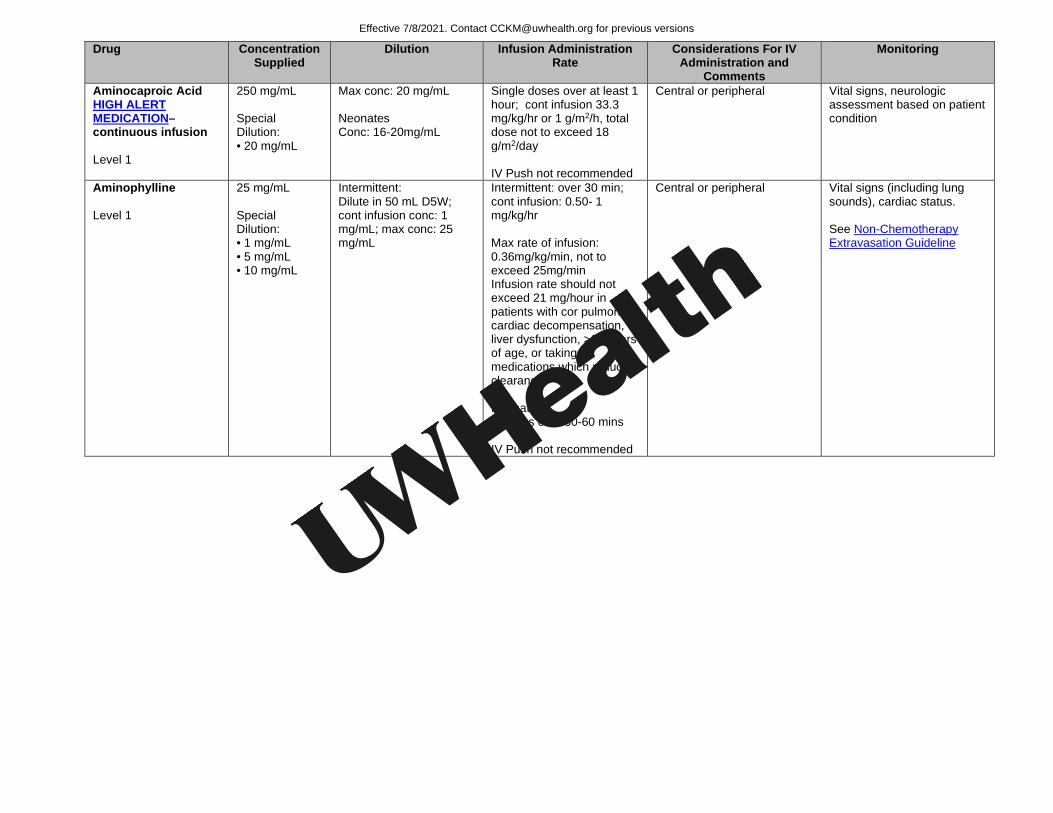
Aminocaproic Acid HIGH ALERT MEDICATION– continuous infusion Level 1
250 mg/mL Special Dilution: • 20 mg/mL
Max conc: 20 mg/mL Neonates Conc: 16-20mg/mL
Single doses over at least 1 hour; cont infusion 33.3 mg/kg/hr or 1 g/m2/h, total dose not to exceed 18 g/m2/day IV Push not recommended
Central or peripheral Vital signs, neurologic assessment based on patient condition
Aminophylline Level 1
25 mg/mL Special Dilution: • 1 mg/mL • 5 mg/mL • 10 mg/mL
Intermittent: Dilute in 50 mL D5W; cont infusion conc: 1 mg/mL; max conc: 25 mg/mL
Intermittent: over 30 min; cont infusion: 0.50- 1 mg/kg/hr Max rate of infusion: 0.36mg/kg/min, not to exceed 25mg/min Infusion rate should not exceed 21 mg/hour in patients with cor pulmonale, cardiac decompensation, liver dysfunction, >60 years of age, or taking medications which reduce clearance. Neonates IV bolus over 30-60 mins IV Push not recommended
Central or peripheral Vital signs (including lung sounds), cardiac status. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
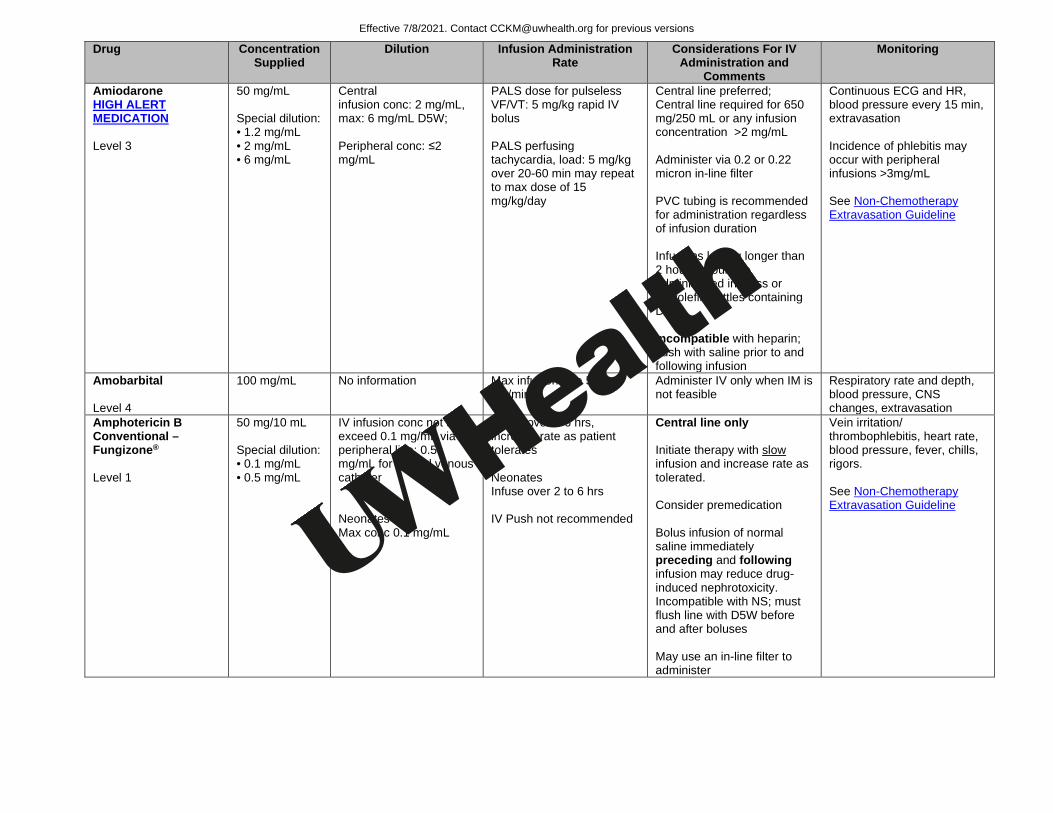
Amiodarone HIGH ALERT MEDICATION Level 3
50 mg/mL Special dilution: • 1.2 mg/mL • 2 mg/mL • 6 mg/mL
Central infusion conc: 2 mg/mL, max: 6 mg/mL D5W; Peripheral conc: ≤2 mg/mL
PALS dose for pulseless VF/VT: 5 mg/kg rapid IV bolus PALS perfusing tachycardia, load: 5 mg/kg over 20-60 min may repeat to max dose of 15 mg/kg/day
Central line preferred; Central line required for 650 mg/250 mL or any infusion concentration >2 mg/mL Administer via 0.2 or 0.22 micron in-line filter PVC tubing is recommended for administration regardless of infusion duration Infusions lasting longer than 2 hours should be administered in glass or polyolefin bottles containing D5W Incompatible with heparin; flush with saline prior to and following infusion
Continuous ECG and HR, blood pressure every 15 min, extravasation Incidence of phlebitis may occur with peripheral infusions >3mg/mL See Non-Chemotherapy Extravasation Guideline
Amobarbital Level 4
100 mg/mL No information Max infusion rate 50 mg/min
Administer IV only when IM is not feasible
Respiratory rate and depth, blood pressure, CNS changes, extravasation
Amphotericin B Conventional –Fungizone® Level 1
50 mg/10 mL Special dilution: • 0.1 mg/mL • 0.5 mg/mL
IV infusion conc not to exceed 0.1 mg/mL via peripheral line; 0.5 mg/mL for central venous catheter Neonates Max conc 0.1 mg/mL
Infuse over 2-6 hrs, increase rate as patient tolerates Neonates Infuse over 2 to 6 hrs IV Push not recommended
Central line only Initiate therapy with slow infusion and increase rate as tolerated. Consider premedication Bolus infusion of normal saline immediately preceding and following infusion may reduce drug-induced nephrotoxicity. Incompatible with NS; must flush line with D5W before and after boluses May use an in-line filter to administer
Vein irritation/ thrombophlebitis, heart rate, blood pressure, fever, chills, rigors. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
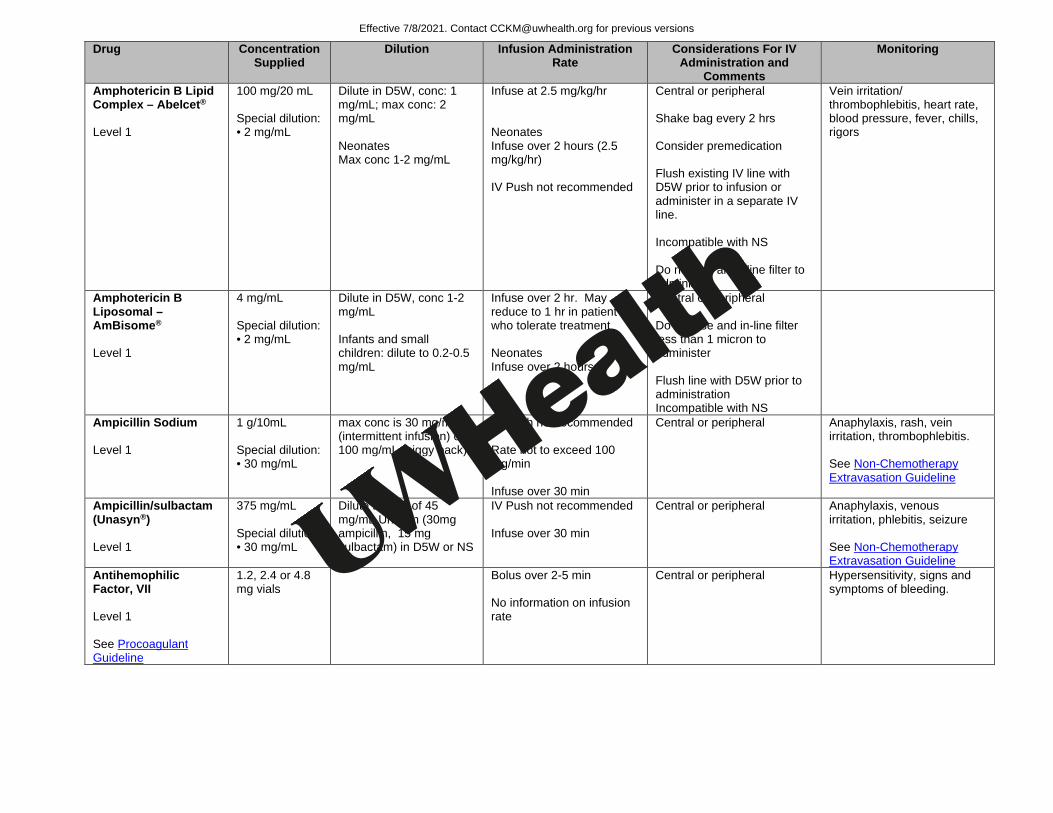
Amphotericin B Lipid Complex – Abelcet® Level 1
100 mg/20 mL Special dilution: • 2 mg/mL
Dilute in D5W, conc: 1 mg/mL; max conc: 2 mg/mL Neonates Max conc 1-2 mg/mL
Infuse at 2.5 mg/kg/hr Neonates Infuse over 2 hours (2.5 mg/kg/hr) IV Push not recommended
Central or peripheral Shake bag every 2 hrs Consider premedication Flush existing IV line with D5W prior to infusion or administer in a separate IV line. Incompatible with NS Do not use an in-line filter to administer
Vein irritation/ thrombophlebitis, heart rate, blood pressure, fever, chills, rigors
Amphotericin B Liposomal – AmBisome®
Level 1
4 mg/mL Special dilution: • 2 mg/mL
Dilute in D5W, conc 1-2 mg/mL Infants and small children: dilute to 0.2-0.5 mg/mL
Infuse over 2 hr. May reduce to 1 hr in patient who tolerate treatment Neonates Infuse over 2 hours
Central or peripheral Do not use and in-line filter less than 1 micron to administer Flush line with D5W prior to administration Incompatible with NS
Ampicillin Sodium Level 1
1 g/10mL Special dilution: • 30 mg/mL
max conc is 30 mg/mL (intermittent infusion) or 100 mg/mL (piggy back)
IV Push not recommended Rate not to exceed 100 mg/min Infuse over 30 min
Central or peripheral Anaphylaxis, rash, vein irritation, thrombophlebitis. See Non-Chemotherapy Extravasation Guideline
Ampicillin/sulbactam (Unasyn®) Level 1
375 mg/mL Special dilution: • 30 mg/mL
Dilute to max of 45 mg/mL Unasyn (30mg ampicillin, 15 mg sulbactam) in D5W or NS
IV Push not recommended Infuse over 30 min
Central or peripheral Anaphylaxis, venous irritation, phlebitis, seizure See Non-Chemotherapy Extravasation Guideline
Antihemophilic Factor, VII Level 1 See Procoagulant Guideline
1.2, 2.4 or 4.8 mg vials
Bolus over 2-5 min No information on infusion rate
Central or peripheral Hypersensitivity, signs and symptoms of bleeding.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
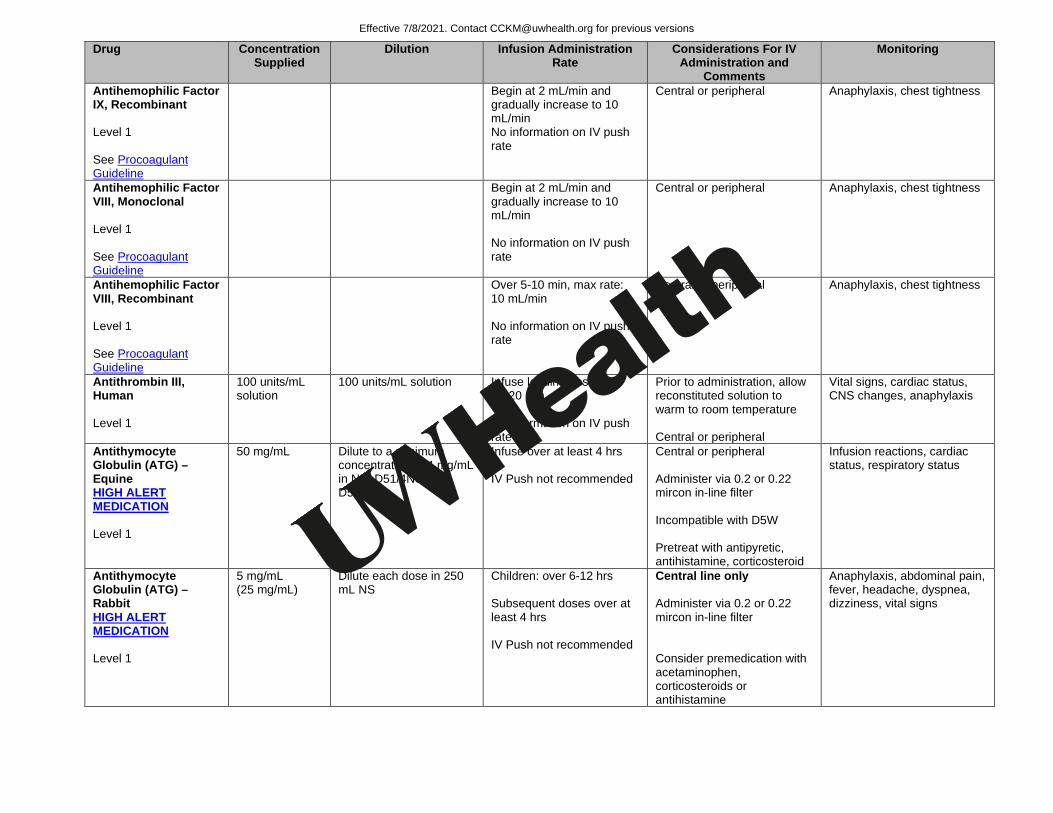
Antihemophilic Factor IX, Recombinant Level 1 See Procoagulant Guideline
Begin at 2 mL/min and gradually increase to 10 mL/min No information on IV push rate
Central or peripheral Anaphylaxis, chest tightness
Antihemophilic Factor VIII, Monoclonal Level 1 See Procoagulant Guideline
Begin at 2 mL/min and gradually increase to 10 mL/min No information on IV push rate
Central or peripheral Anaphylaxis, chest tightness
Antihemophilic Factor VIII, Recombinant Level 1 See Procoagulant Guideline
Over 5-10 min, max rate: 10 mL/min No information on IV push rate
Central or peripheral Anaphylaxis, chest tightness
Antithrombin III, Human Level 1
100 units/mL solution
100 units/mL solution Infuse loading dose over 10-20 min No information on IV push rate
Prior to administration, allow reconstituted solution to warm to room temperature Central or peripheral
Vital signs, cardiac status, CNS changes, anaphylaxis
Antithymocyte Globulin (ATG) – Equine HIGH ALERT MEDICATION Level 1
50 mg/mL Dilute to a minimum concentration of 4 mg/mL in NS, D51/4NS, or D51/2NS
Infuse over at least 4 hrs IV Push not recommended
Central or peripheral Administer via 0.2 or 0.22 mircon in-line filter Incompatible with D5W Pretreat with antipyretic, antihistamine, corticosteroid
Infusion reactions, cardiac status, respiratory status
Antithymocyte Globulin (ATG) – Rabbit HIGH ALERT MEDICATION Level 1
5 mg/mL (25 mg/mL)
Dilute each dose in 250 mL NS
Children: over 6-12 hrs Subsequent doses over at least 4 hrs IV Push not recommended
Central line only Administer via 0.2 or 0.22 mircon in-line filter Consider premedication with acetaminophen, corticosteroids or antihistamine
Anaphylaxis, abdominal pain, fever, headache, dyspnea, dizziness, vital signs
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
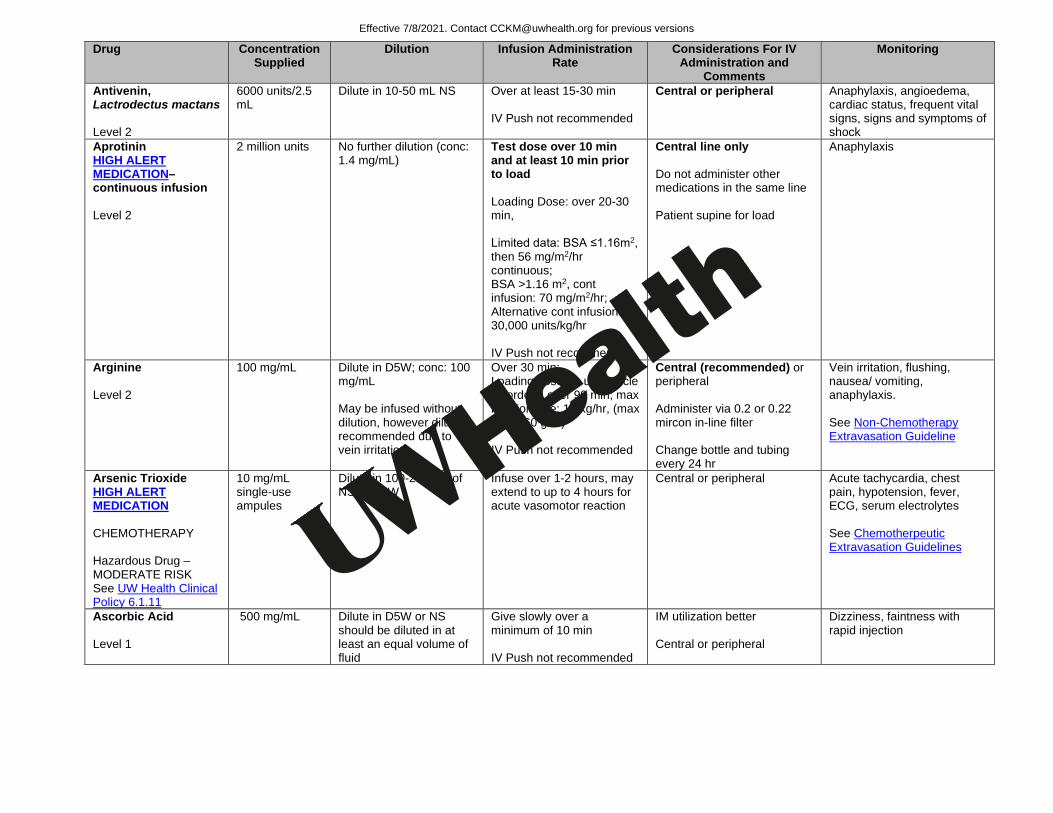
Antivenin, Lactrodectus mactans Level 2
6000 units/2.5 mL
Dilute in 10-50 mL NS Over at least 15-30 min IV Push not recommended
Central or peripheral Anaphylaxis, angioedema, cardiac status, frequent vital signs, signs and symptoms of shock
Aprotinin HIGH ALERT MEDICATION– continuous infusion Level 2
2 million units No further dilution (conc: 1.4 mg/mL)
Test dose over 10 min and at least 10 min prior to load Loading Dose: over 20-30 min, Limited data: BSA ≤1.16m2, then 56 mg/m2/hr continuous; BSA >1.16 m2, cont infusion: 70 mg/m2/hr; Alternative cont infusion: 30,000 units/kg/hr IV Push not recommended
Central line only Do not administer other medications in the same line Patient supine for load
Anaphylaxis
Arginine Level 2
100 mg/mL Dilute in D5W; conc: 100 mg/mL May be infused without dilution, however dilution recommended due to vein irritation
Over 30 min; Loading dose for urea cycle disorders: over 90 min; max infusion rate: 1g/kg/hr, (max dose: 60 g/hr) IV Push not recommended
Central (recommended) or peripheral Administer via 0.2 or 0.22 mircon in-line filter Change bottle and tubing every 24 hr
Vein irritation, flushing, nausea/ vomiting, anaphylaxis. See Non-Chemotherapy Extravasation Guideline
Arsenic Trioxide HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
10 mg/mL single-use ampules
Dilute in 100-250 mL of NS or D5W
Infuse over 1-2 hours, may extend to up to 4 hours for acute vasomotor reaction
Central or peripheral Acute tachycardia, chest pain, hypotension, fever, ECG, serum electrolytes See Chemotherpeutic Extravasation Guidelines
Ascorbic Acid Level 1
500 mg/mL Dilute in D5W or NS should be diluted in at least an equal volume of fluid
Give slowly over a minimum of 10 min IV Push not recommended
IM utilization better Central or peripheral
Dizziness, faintness with rapid injection
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
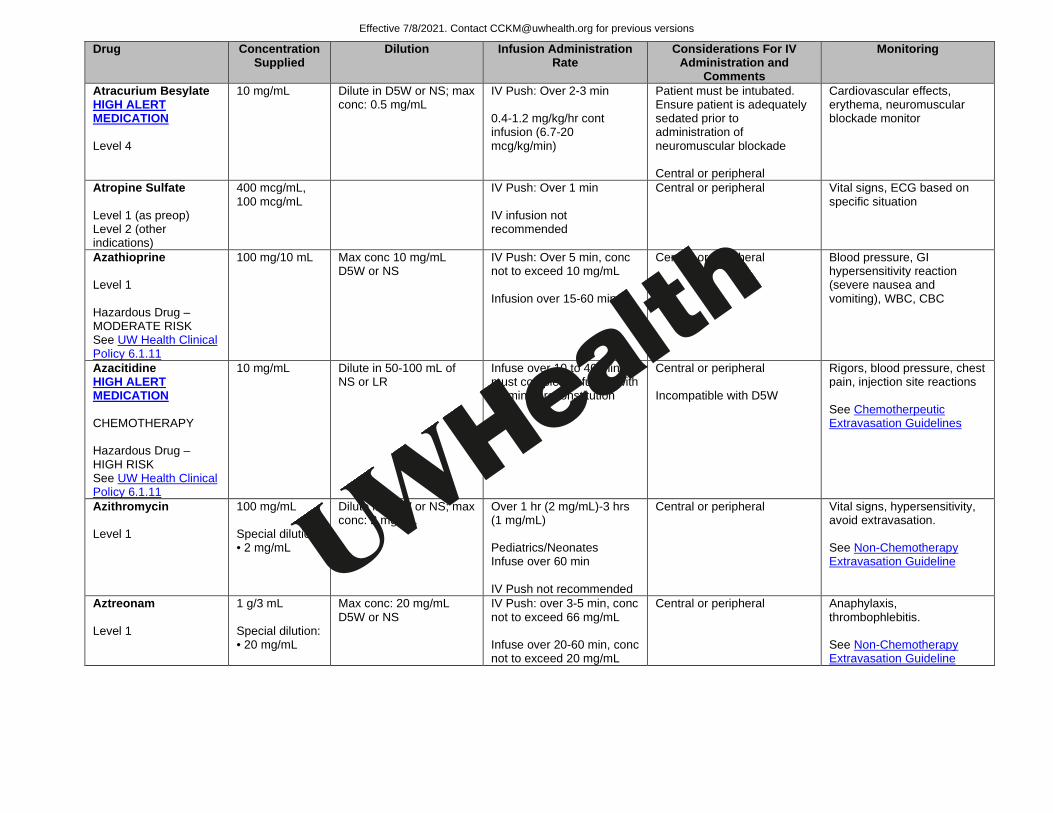
Atracurium Besylate HIGH ALERT MEDICATION Level 4
10 mg/mL Dilute in D5W or NS; max conc: 0.5 mg/mL
IV Push: Over 2-3 min 0.4-1.2 mg/kg/hr cont infusion (6.7-20 mcg/kg/min)
Patient must be intubated. Ensure patient is adequately sedated prior to administration of neuromuscular blockade Central or peripheral
Cardiovascular effects, erythema, neuromuscular blockade monitor
Atropine Sulfate Level 1 (as preop) Level 2 (other indications)
400 mcg/mL, 100 mcg/mL
IV Push: Over 1 min IV infusion not recommended
Central or peripheral Vital signs, ECG based on specific situation
Azathioprine Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
100 mg/10 mL Max conc 10 mg/mL D5W or NS
IV Push: Over 5 min, conc not to exceed 10 mg/mL Infusion over 15-60 min
Central or peripheral Blood pressure, GI hypersensitivity reaction (severe nausea and vomiting), WBC, CBC
Azacitidine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/mL Dilute in 50-100 mL of NS or LR
Infuse over 10 to 40 min; must complete infusion with 60 min of reconstitution
Central or peripheral Incompatible with D5W
Rigors, blood pressure, chest pain, injection site reactions See Chemotherpeutic Extravasation Guidelines
Azithromycin Level 1
100 mg/mL Special dilution: • 2 mg/mL
Dilute in D5W or NS; max conc: 2 mg/mL
Over 1 hr (2 mg/mL)-3 hrs (1 mg/mL) Pediatrics/Neonates Infuse over 60 min IV Push not recommended
Central or peripheral Vital signs, hypersensitivity, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Aztreonam Level 1
1 g/3 mL Special dilution: • 20 mg/mL
Max conc: 20 mg/mL D5W or NS
IV Push: over 3-5 min, conc not to exceed 66 mg/mL Infuse over 20-60 min, conc not to exceed 20 mg/mL
Central or peripheral Anaphylaxis, thrombophlebitis. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
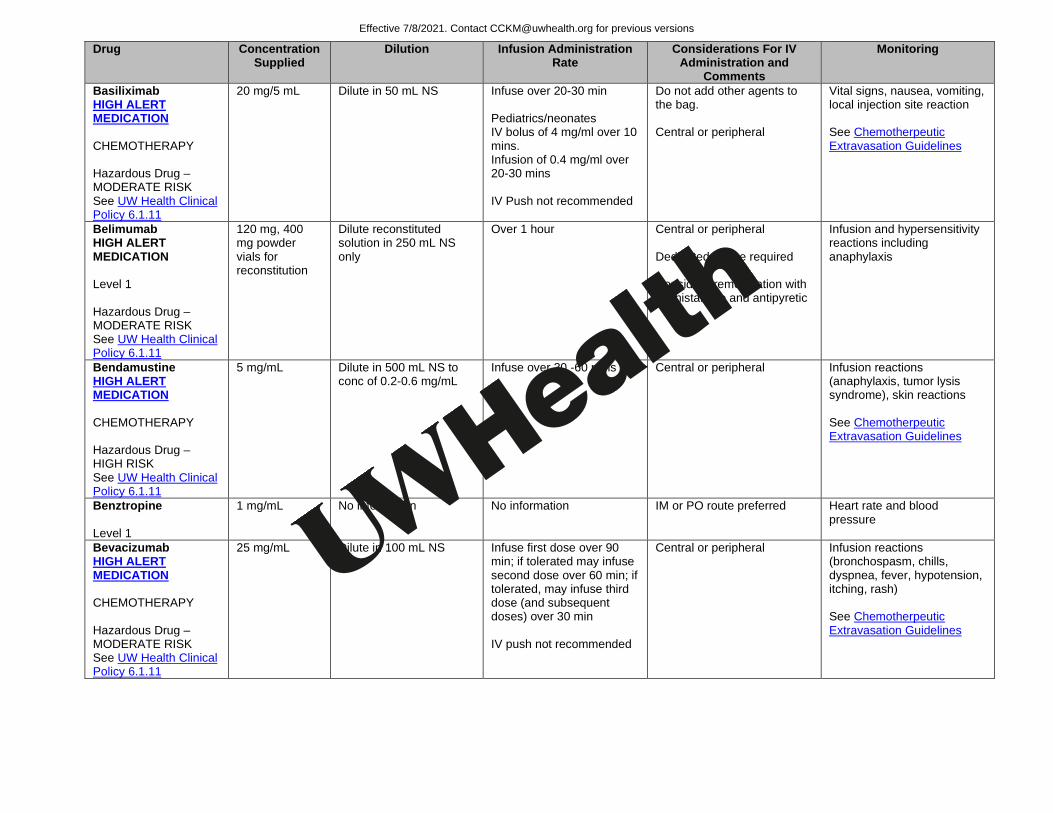
Basiliximab HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
20 mg/5 mL Dilute in 50 mL NS
Infuse over 20-30 min Pediatrics/neonates IV bolus of 4 mg/ml over 10 mins. Infusion of 0.4 mg/ml over 20-30 mins IV Push not recommended
Do not add other agents to the bag. Central or peripheral
Vital signs, nausea, vomiting, local injection site reaction See Chemotherpeutic Extravasation Guidelines
Belimumab HIGH ALERT MEDICATION Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
120 mg, 400 mg powder vials for reconstitution
Dilute reconstituted solution in 250 mL NS only
Over 1 hour Central or peripheral Dedicated IV line required Consider premedication with antihistamine and antipyretic
Infusion and hypersensitivity reactions including anaphylaxis
Bendamustine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
5 mg/mL Dilute in 500 mL NS to conc of 0.2-0.6 mg/mL
Infuse over 30 -60 mins Central or peripheral Infusion reactions (anaphylaxis, tumor lysis syndrome), skin reactions See Chemotherpeutic Extravasation Guidelines
Benztropine Level 1
1 mg/mL No information No information IM or PO route preferred Heart rate and blood pressure
Bevacizumab HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
25 mg/mL Dilute in 100 mL NS Infuse first dose over 90 min; if tolerated may infuse second dose over 60 min; if tolerated, may infuse third dose (and subsequent doses) over 30 min IV push not recommended
Central or peripheral Infusion reactions (bronchospasm, chills, dyspnea, fever, hypotension, itching, rash) See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
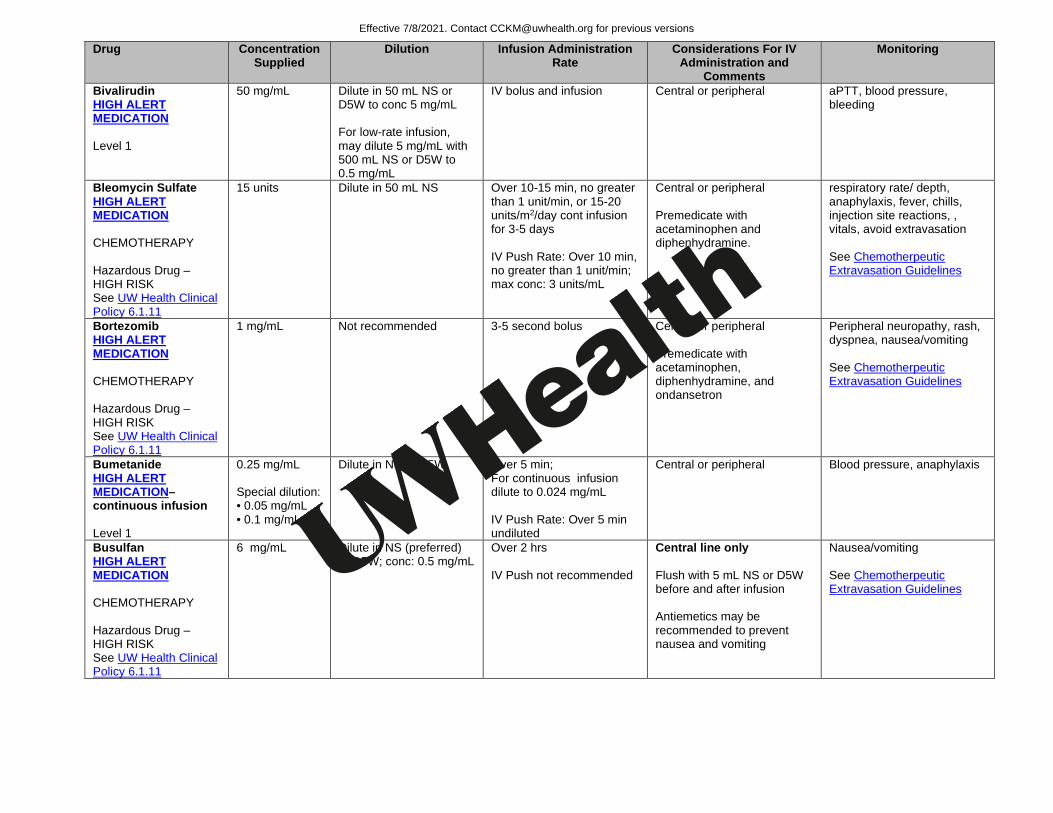
Bivalirudin HIGH ALERT MEDICATION Level 1
50 mg/mL Dilute in 50 mL NS or D5W to conc 5 mg/mL For low-rate infusion, may dilute 5 mg/mL with 500 mL NS or D5W to 0.5 mg/mL
IV bolus and infusion Central or peripheral aPTT, blood pressure, bleeding
Bleomycin Sulfate HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
15 units Dilute in 50 mL NS Over 10-15 min, no greater than 1 unit/min, or 15-20 units/m2/day cont infusion for 3-5 days IV Push Rate: Over 10 min, no greater than 1 unit/min; max conc: 3 units/mL
Central or peripheral Premedicate with acetaminophen and diphenhydramine.
respiratory rate/ depth, anaphylaxis, fever, chills, injection site reactions, , vitals, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Bortezomib HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Not recommended 3-5 second bolus Central or peripheral Premedicate with acetaminophen, diphenhydramine, and ondansetron
Peripheral neuropathy, rash, dyspnea, nausea/vomiting See Chemotherpeutic Extravasation Guidelines
Bumetanide HIGH ALERT MEDICATION– continuous infusion Level 1
0.25 mg/mL Special dilution: • 0.05 mg/mL • 0.1 mg/mL
Dilute in NS or D5W
Over 5 min; For continuous infusion dilute to 0.024 mg/mL IV Push Rate: Over 5 min undiluted
Central or peripheral Blood pressure, anaphylaxis
Busulfan HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
6 mg/mL Dilute in NS (preferred) or D5W; conc: 0.5 mg/mL
Over 2 hrs IV Push not recommended
Central line only Flush with 5 mL NS or D5W before and after infusion Antiemetics may be recommended to prevent nausea and vomiting
Nausea/vomiting See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
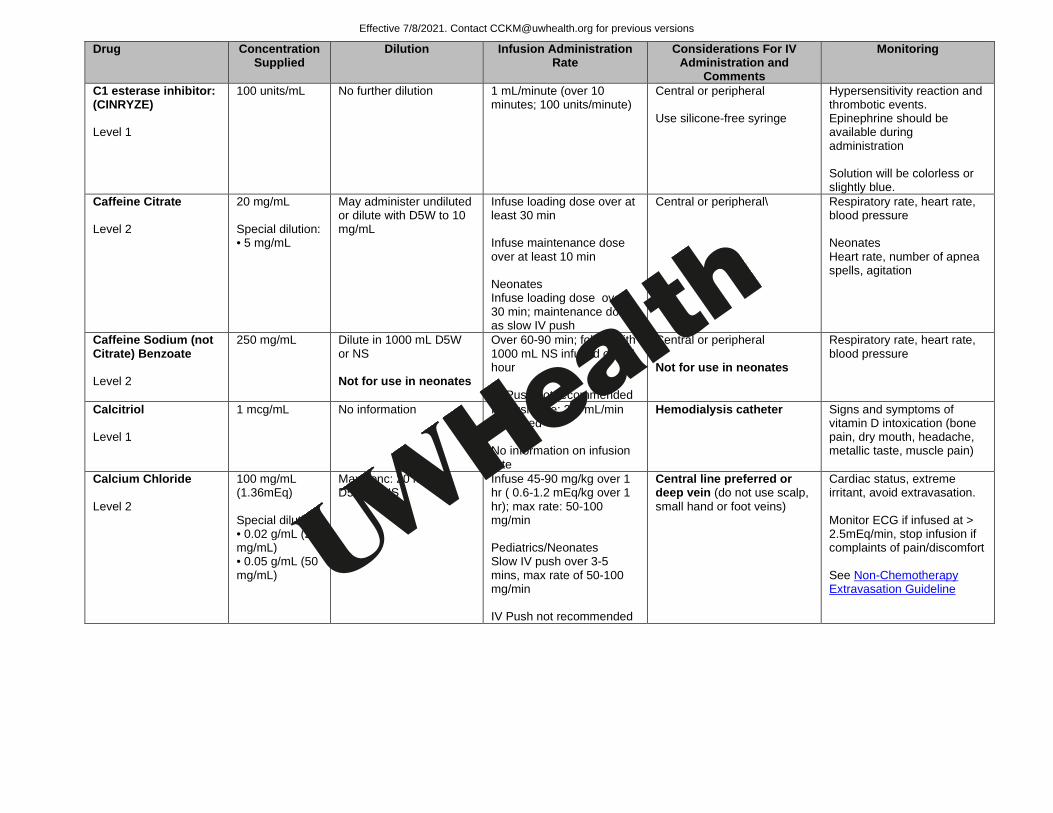
C1 esterase inhibitor: (CINRYZE) Level 1
100 units/mL No further dilution 1 mL/minute (over 10 minutes; 100 units/minute)
Central or peripheral Use silicone-free syringe
Hypersensitivity reaction and thrombotic events. Epinephrine should be available during administration Solution will be colorless or slightly blue.
Caffeine Citrate Level 2
20 mg/mL Special dilution: • 5 mg/mL
May administer undiluted or dilute with D5W to 10 mg/mL
Infuse loading dose over at least 30 min Infuse maintenance dose over at least 10 min Neonates Infuse loading dose over 30 min; maintenance dose as slow IV push
Central or peripheral\ Respiratory rate, heart rate, blood pressure Neonates Heart rate, number of apnea spells, agitation
Caffeine Sodium (not Citrate) Benzoate Level 2
250 mg/mL Dilute in 1000 mL D5W or NS Not for use in neonates
Over 60-90 min; follow with 1000 mL NS infused over 1 hour IV Push not recommended
Central or peripheral Not for use in neonates
Respiratory rate, heart rate, blood pressure
Calcitriol Level 1
1 mcg/mL No information
IV Push rate: 2-3 mL/min Undiluted No information on infusion rate
Hemodialysis catheter Signs and symptoms of vitamin D intoxication (bone pain, dry mouth, headache, metallic taste, muscle pain)
Calcium Chloride Level 2
100 mg/mL (1.36mEq) Special dilution: • 0.02 g/mL (20 mg/mL) • 0.05 g/mL (50 mg/mL)
Max conc: 20 mg/mL D5W or NS
Infuse 45-90 mg/kg over 1 hr ( 0.6-1.2 mEq/kg over 1 hr); max rate: 50-100 mg/min Pediatrics/Neonates Slow IV push over 3-5 mins, max rate of 50-100 mg/min IV Push not recommended
Central line preferred or deep vein (do not use scalp, small hand or foot veins)
Cardiac status, extreme irritant, avoid extravasation. Monitor ECG if infused at > 2.5mEq/min, stop infusion if complaints of pain/discomfort See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
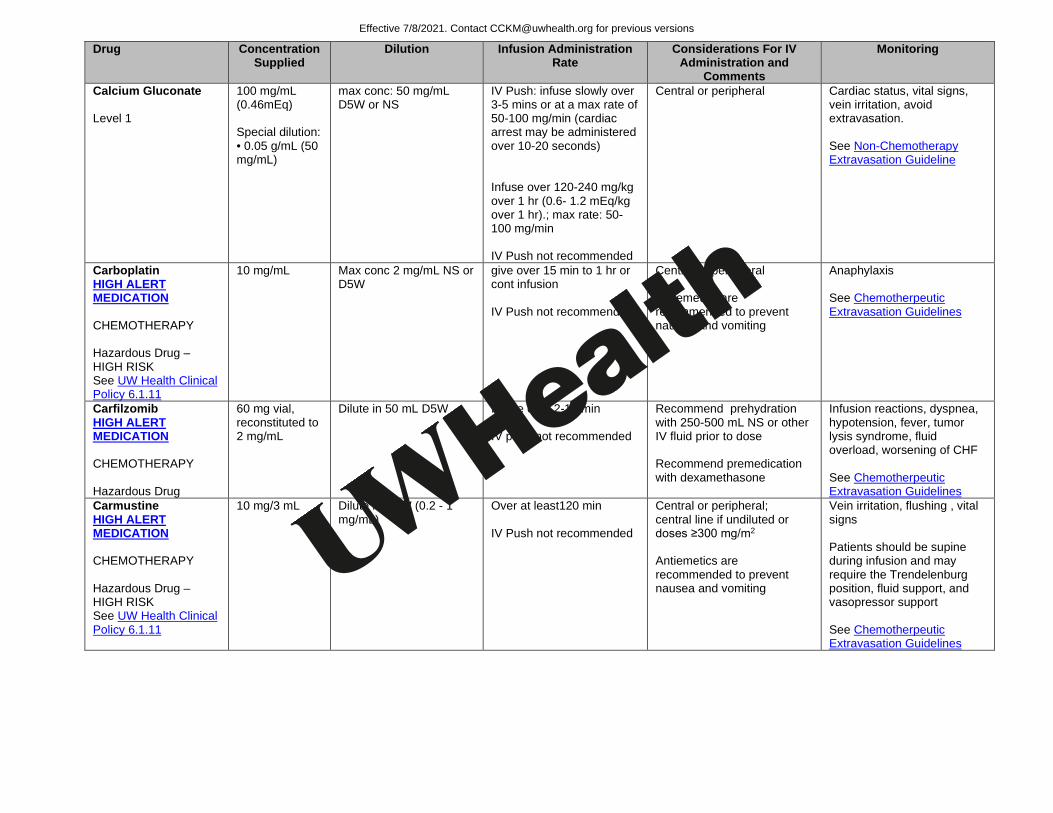
Calcium Gluconate Level 1
100 mg/mL (0.46mEq) Special dilution: • 0.05 g/mL (50 mg/mL)
max conc: 50 mg/mL D5W or NS
IV Push: infuse slowly over 3-5 mins or at a max rate of 50-100 mg/min (cardiac arrest may be administered over 10-20 seconds) Infuse over 120-240 mg/kg over 1 hr (0.6- 1.2 mEq/kg over 1 hr).; max rate: 50-100 mg/min IV Push not recommended
Central or peripheral Cardiac status, vital signs, vein irritation, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Carboplatin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/mL Max conc 2 mg/mL NS or D5W
give over 15 min to 1 hr or cont infusion IV Push not recommended
Central or peripheral Antiemetics are recommended to prevent nausea and vomiting
Anaphylaxis See Chemotherpeutic Extravasation Guidelines
Carfilzomib HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug
60 mg vial, reconstituted to 2 mg/mL
Dilute in 50 mL D5W Infuse over 2-10 min IV push not recommended
Recommend prehydration with 250-500 mL NS or other IV fluid prior to dose Recommend premedication with dexamethasone
Infusion reactions, dyspnea, hypotension, fever, tumor lysis syndrome, fluid overload, worsening of CHF See Chemotherpeutic Extravasation Guidelines
Carmustine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/3 mL Dilute in D5W (0.2 - 1 mg/mL)
Over at least120 min IV Push not recommended
Central or peripheral; central line if undiluted or doses ≥300 mg/m2 Antiemetics are recommended to prevent nausea and vomiting
Vein irritation, flushing , vital signs Patients should be supine during infusion and may require the Trendelenburg position, fluid support, and vasopressor support See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
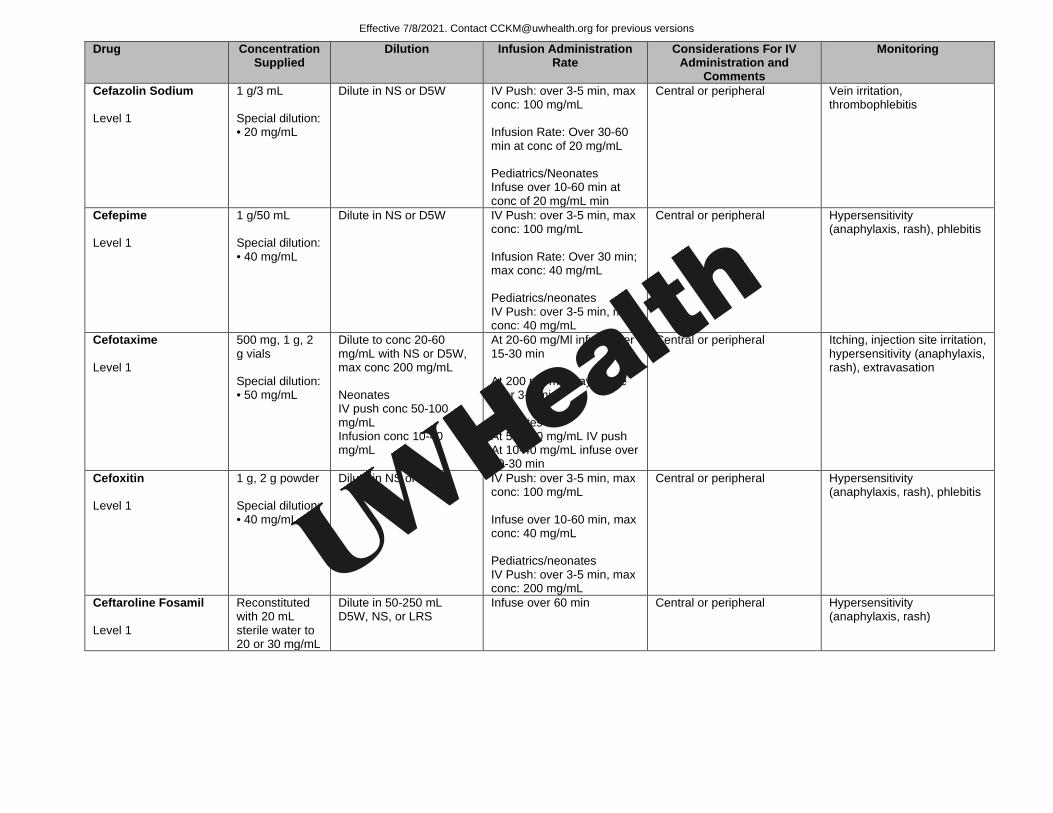
Cefazolin Sodium Level 1
1 g/3 mL Special dilution: • 20 mg/mL
Dilute in NS or D5W IV Push: over 3-5 min, max conc: 100 mg/mL Infusion Rate: Over 30-60 min at conc of 20 mg/mL Pediatrics/Neonates Infuse over 10-60 min at conc of 20 mg/mL min
Central or peripheral Vein irritation, thrombophlebitis
Cefepime Level 1
1 g/50 mL Special dilution: • 40 mg/mL
Dilute in NS or D5W
IV Push: over 3-5 min, max conc: 100 mg/mL Infusion Rate: Over 30 min; max conc: 40 mg/mL Pediatrics/neonates IV Push: over 3-5 min, max conc: 40 mg/mL
Central or peripheral Hypersensitivity (anaphylaxis, rash), phlebitis
Cefotaxime Level 1
500 mg, 1 g, 2 g vials Special dilution: • 50 mg/mL
Dilute to conc 20-60 mg/mL with NS or D5W, max conc 200 mg/mL Neonates IV push conc 50-100 mg/mL Infusion conc 10-40 mg/mL
At 20-60 mg/Ml infuse over 15-30 min At 200 mg/mL may infuse over 3-5 min Neonates At 50-100 mg/mL IV push At 10-40 mg/mL infuse over 10-30 min
Central or peripheral Itching, injection site irritation, hypersensitivity (anaphylaxis, rash), extravasation
Cefoxitin Level 1
1 g, 2 g powder Special dilution: • 40 mg/mL
Dilute in NS or D5W
IV Push: over 3-5 min, max conc: 100 mg/mL Infuse over 10-60 min, max conc: 40 mg/mL Pediatrics/neonates IV Push: over 3-5 min, max conc: 200 mg/mL
Central or peripheral Hypersensitivity (anaphylaxis, rash), phlebitis
Ceftaroline Fosamil Level 1
Reconstituted with 20 mL sterile water to 20 or 30 mg/mL
Dilute in 50-250 mL D5W, NS, or LRS
Infuse over 60 min Central or peripheral Hypersensitivity (anaphylaxis, rash)
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
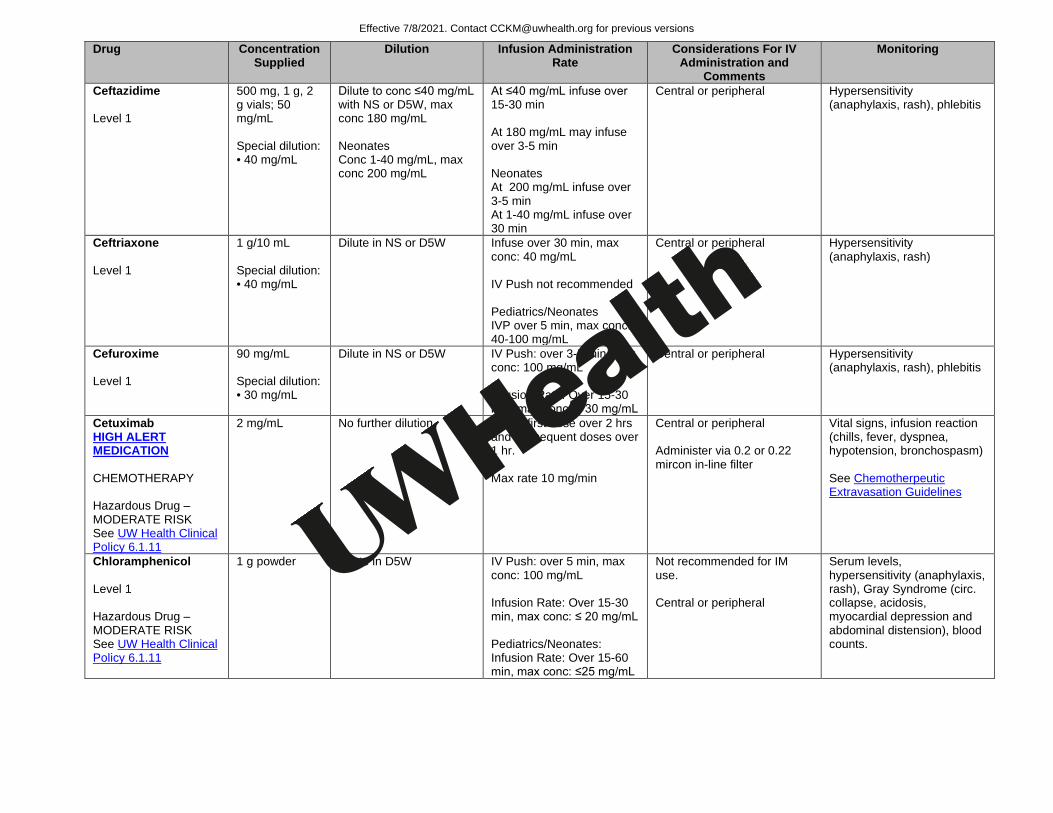
Ceftazidime Level 1
500 mg, 1 g, 2 g vials; 50 mg/mL Special dilution: • 40 mg/mL
Dilute to conc ≤40 mg/mL with NS or D5W, max conc 180 mg/mL Neonates Conc 1-40 mg/mL, max conc 200 mg/mL
At ≤40 mg/mL infuse over 15-30 min At 180 mg/mL may infuse over 3-5 min Neonates At 200 mg/mL infuse over 3-5 min At 1-40 mg/mL infuse over 30 min
Central or peripheral Hypersensitivity (anaphylaxis, rash), phlebitis
Ceftriaxone Level 1
1 g/10 mL Special dilution: • 40 mg/mL
Dilute in NS or D5W Infuse over 30 min, max conc: 40 mg/mL IV Push not recommended Pediatrics/Neonates IVP over 5 min, max conc: 40-100 mg/mL
Central or peripheral Hypersensitivity (anaphylaxis, rash)
Cefuroxime Level 1
90 mg/mL Special dilution: • 30 mg/mL
Dilute in NS or D5W
IV Push: over 3-5 min, max conc: 100 mg/mL Infusion Rate: Over 15-30 min, max conc: ≤ 30 mg/mL
Central or peripheral Hypersensitivity (anaphylaxis, rash), phlebitis
Cetuximab HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
2 mg/mL No further dilution Infuse first dose over 2 hrs and subsequent doses over 1 hr. Max rate 10 mg/min
Central or peripheral Administer via 0.2 or 0.22 mircon in-line filter
Vital signs, infusion reaction (chills, fever, dyspnea, hypotension, bronchospasm) See Chemotherpeutic Extravasation Guidelines
Chloramphenicol Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
1 g powder Dilute in D5W
IV Push: over 5 min, max conc: 100 mg/mL Infusion Rate: Over 15-30 min, max conc: ≤ 20 mg/mL Pediatrics/Neonates: Infusion Rate: Over 15-60 min, max conc: ≤25 mg/mL
Not recommended for IM use. Central or peripheral
Serum levels, hypersensitivity (anaphylaxis, rash), Gray Syndrome (circ. collapse, acidosis, myocardial depression and abdominal distension), blood counts.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
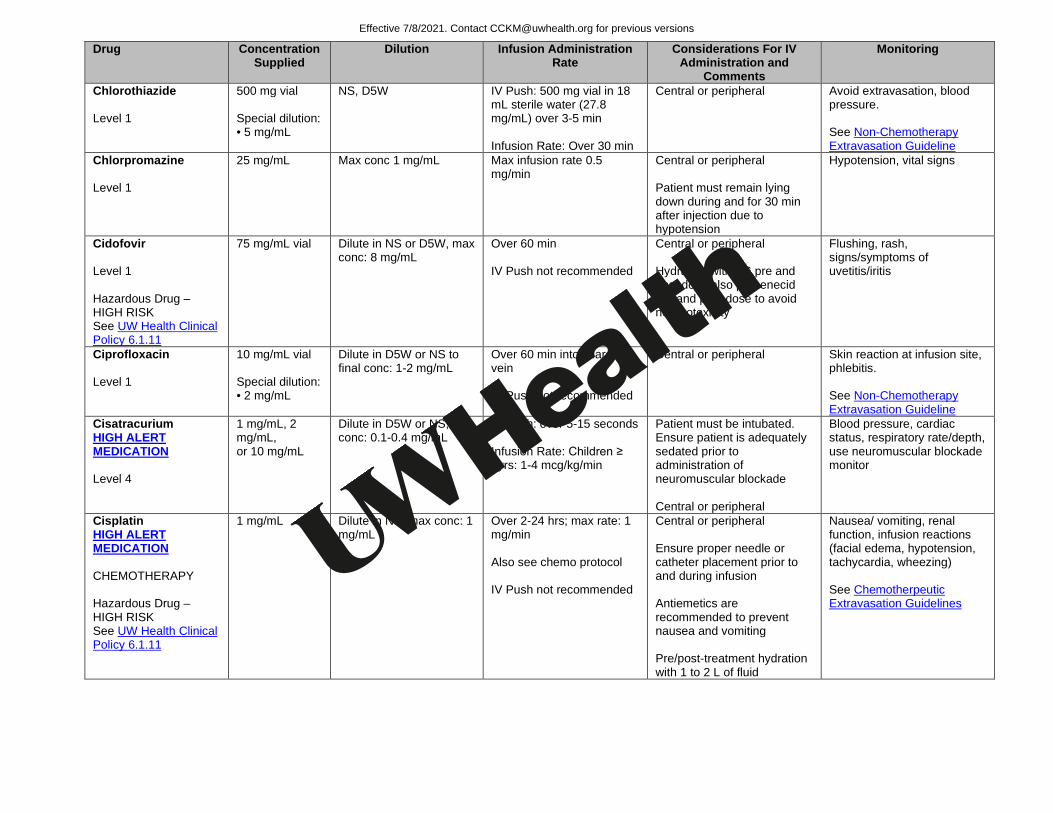
Chlorothiazide Level 1
500 mg vial Special dilution: • 5 mg/mL
NS, D5W
IV Push: 500 mg vial in 18 mL sterile water (27.8 mg/mL) over 3-5 min Infusion Rate: Over 30 min
Central or peripheral Avoid extravasation, blood pressure. See Non-Chemotherapy Extravasation Guideline
Chlorpromazine Level 1
25 mg/mL Max conc 1 mg/mL Max infusion rate 0.5 mg/min
Central or peripheral Patient must remain lying down during and for 30 min after injection due to hypotension
Hypotension, vital signs
Cidofovir Level 1 Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
75 mg/mL vial
Dilute in NS or D5W, max conc: 8 mg/mL
Over 60 min IV Push not recommended
Central or peripheral Hydration with NS pre and post dose also probenecid pre and post dose to avoid nephrotoxicity
Flushing, rash, signs/symptoms of uvetitis/iritis
Ciprofloxacin Level 1
10 mg/mL vial Special dilution: • 2 mg/mL
Dilute in D5W or NS to final conc: 1-2 mg/mL
Over 60 min into a large vein IV Push not recommended
Central or peripheral Skin reaction at infusion site, phlebitis. See Non-Chemotherapy Extravasation Guideline
Cisatracurium HIGH ALERT MEDICATION Level 4
1 mg/mL, 2 mg/mL, or 10 mg/mL
Dilute in D5W or NS; conc: 0.1-0.4 mg/mL
IV Push: over 5-15 seconds Infusion Rate: Children ≥ 2yrs: 1-4 mcg/kg/min
Patient must be intubated. Ensure patient is adequately sedated prior to administration of neuromuscular blockade Central or peripheral
Blood pressure, cardiac status, respiratory rate/depth, use neuromuscular blockade monitor
Cisplatin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute in NS; max conc: 1 mg/mL
Over 2-24 hrs; max rate: 1 mg/min Also see chemo protocol IV Push not recommended
Central or peripheral Ensure proper needle or catheter placement prior to and during infusion Antiemetics are recommended to prevent nausea and vomiting Pre/post-treatment hydration with 1 to 2 L of fluid
Nausea/ vomiting, renal function, infusion reactions (facial edema, hypotension, tachycardia, wheezing) See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
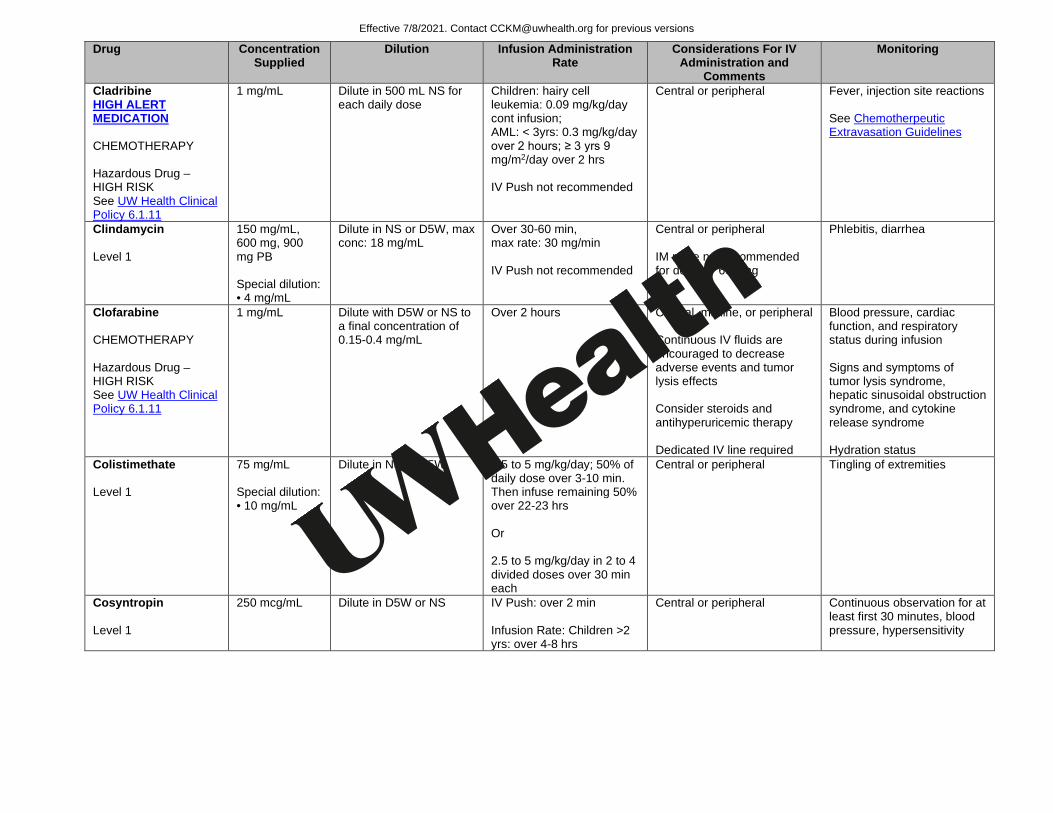
Cladribine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute in 500 mL NS for each daily dose
Children: hairy cell leukemia: 0.09 mg/kg/day cont infusion; AML: < 3yrs: 0.3 mg/kg/day over 2 hours; ≥ 3 yrs 9 mg/m2/day over 2 hrs IV Push not recommended
Central or peripheral Fever, injection site reactions See Chemotherpeutic Extravasation Guidelines
Clindamycin Level 1
150 mg/mL, 600 mg, 900 mg PB Special dilution: • 4 mg/mL
Dilute in NS or D5W, max conc: 18 mg/mL
Over 30-60 min, max rate: 30 mg/min IV Push not recommended
Central or peripheral IM route not recommended for doses > 600 mg
Phlebitis, diarrhea
Clofarabine CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute with D5W or NS to a final concentration of 0.15-0.4 mg/mL
Over 2 hours Central, midline, or peripheral Continuous IV fluids are encouraged to decrease adverse events and tumor lysis effects Consider steroids and antihyperuricemic therapy Dedicated IV line required
Blood pressure, cardiac function, and respiratory status during infusion Signs and symptoms of tumor lysis syndrome, hepatic sinusoidal obstruction syndrome, and cytokine release syndrome Hydration status
Colistimethate Level 1
75 mg/mL Special dilution: • 10 mg/mL
Dilute in NS or D5W
2.5 to 5 mg/kg/day; 50% of daily dose over 3-10 min. Then infuse remaining 50% over 22-23 hrs Or 2.5 to 5 mg/kg/day in 2 to 4 divided doses over 30 min each
Central or peripheral Tingling of extremities
Cosyntropin Level 1
250 mcg/mL Dilute in D5W or NS
IV Push: over 2 min Infusion Rate: Children >2 yrs: over 4-8 hrs
Central or peripheral Continuous observation for at least first 30 minutes, blood pressure, hypersensitivity
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
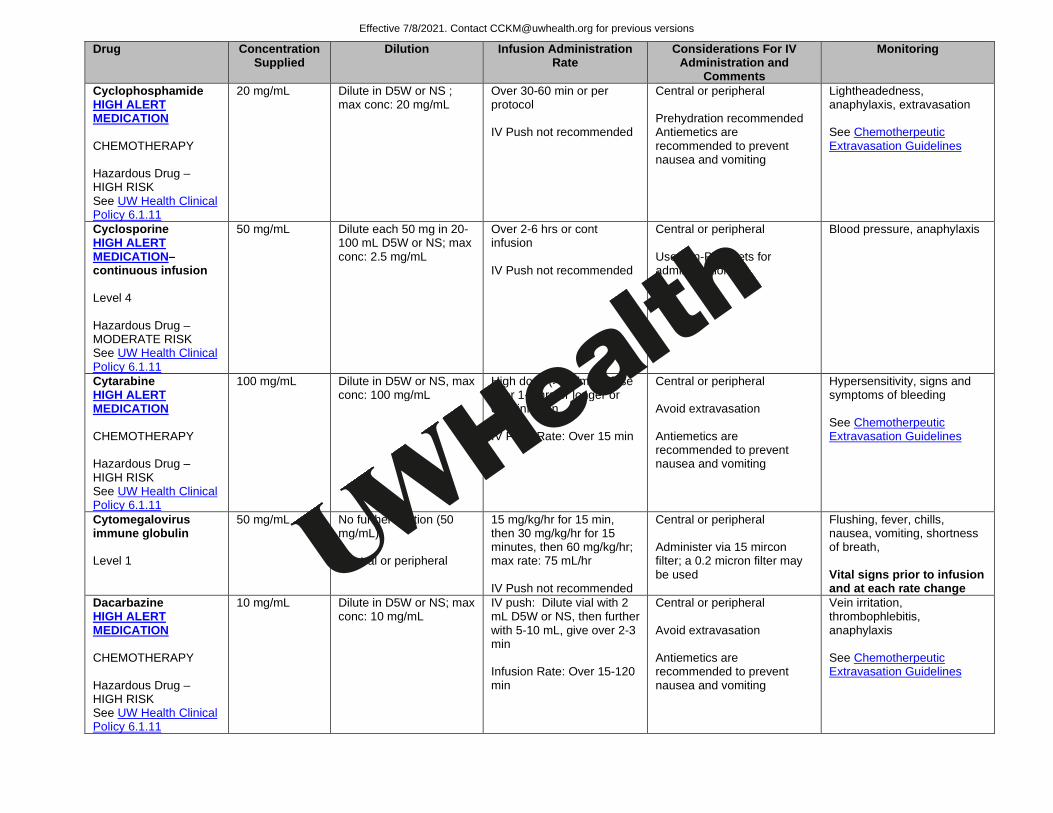
Cyclophosphamide HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
20 mg/mL Dilute in D5W or NS ; max conc: 20 mg/mL
Over 30-60 min or per protocol IV Push not recommended
Central or peripheral Prehydration recommended Antiemetics are recommended to prevent nausea and vomiting
Lightheadedness, anaphylaxis, extravasation See Chemotherpeutic Extravasation Guidelines
Cyclosporine HIGH ALERT MEDICATION– continuous infusion Level 4 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
50 mg/mL Dilute each 50 mg in 20- 100 mL D5W or NS; max conc: 2.5 mg/mL
Over 2-6 hrs or cont infusion IV Push not recommended
Central or peripheral Use non-PVC sets for administration
Blood pressure, anaphylaxis
Cytarabine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
100 mg/mL Dilute in D5W or NS, max conc: 100 mg/mL
High dose (> 1g/m2) infuse over 1-3 hrs or longer or cont infusion IV Push Rate: Over 15 min
Central or peripheral Avoid extravasation Antiemetics are recommended to prevent nausea and vomiting
Hypersensitivity, signs and symptoms of bleeding See Chemotherpeutic Extravasation Guidelines
Cytomegalovirus immune globulin Level 1
50 mg/mL No further dilution (50 mg/mL) Central or peripheral
15 mg/kg/hr for 15 min, then 30 mg/kg/hr for 15 minutes, then 60 mg/kg/hr; max rate: 75 mL/hr IV Push not recommended
Central or peripheral Administer via 15 mircon filter; a 0.2 micron filter may be used
Flushing, fever, chills, nausea, vomiting, shortness of breath, Vital signs prior to infusion and at each rate change
Dacarbazine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/mL Dilute in D5W or NS; max conc: 10 mg/mL
IV push: Dilute vial with 2 mL D5W or NS, then further with 5-10 mL, give over 2-3 min Infusion Rate: Over 15-120 min
Central or peripheral Avoid extravasation Antiemetics are recommended to prevent nausea and vomiting
Vein irritation, thrombophlebitis, anaphylaxis See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
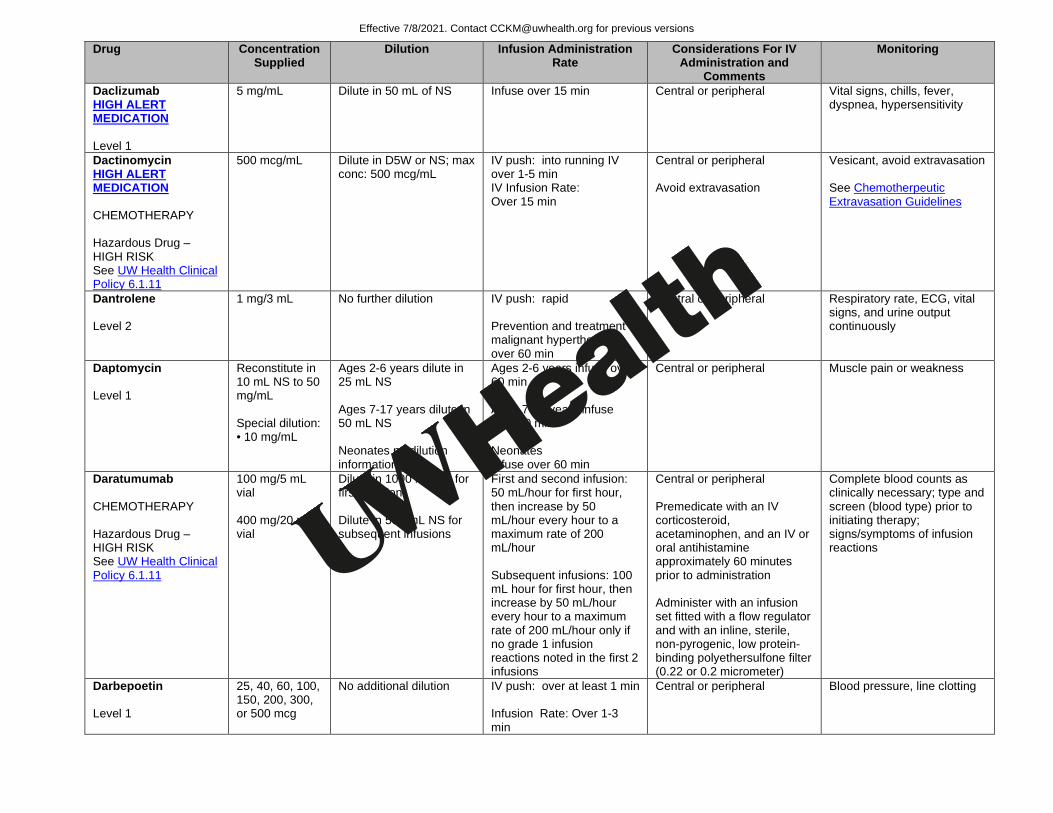
Daclizumab HIGH ALERT MEDICATION Level 1
5 mg/mL Dilute in 50 mL of NS Infuse over 15 min Central or peripheral Vital signs, chills, fever, dyspnea, hypersensitivity
Dactinomycin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
500 mcg/mL Dilute in D5W or NS; max conc: 500 mcg/mL
IV push: into running IV over 1-5 min IV Infusion Rate: Over 15 min
Central or peripheral Avoid extravasation
Vesicant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Dantrolene Level 2
1 mg/3 mL No further dilution IV push: rapid Prevention and treatment of malignant hyperthermia: over 60 min
Central or peripheral Respiratory rate, ECG, vital signs, and urine output continuously
Daptomycin Level 1
Reconstitute in 10 mL NS to 50 mg/mL Special dilution: • 10 mg/mL
Ages 2-6 years dilute in 25 mL NS Ages 7-17 years dilute in 50 mL NS Neonates no dilution information
Ages 2-6 years infuse over 60 min Ages 7-17 years infuse over 30 min Neonates Infuse over 60 min
Central or peripheral Muscle pain or weakness
Daratumumab CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
100 mg/5 mL vial 400 mg/20 mL vial
Dilute in 1000 mL NS for first infusion Dilute in 500 mL NS for subsequent infusions
First and second infusion: 50 mL/hour for first hour, then increase by 50 mL/hour every hour to a maximum rate of 200 mL/hour Subsequent infusions: 100 mL hour for first hour, then increase by 50 mL/hour every hour to a maximum rate of 200 mL/hour only if no grade 1 infusion reactions noted in the first 2 infusions
Central or peripheral Premedicate with an IV corticosteroid, acetaminophen, and an IV or oral antihistamine approximately 60 minutes prior to administration Administer with an infusion set fitted with a flow regulator and with an inline, sterile, non-pyrogenic, low protein-binding polyethersulfone filter (0.22 or 0.2 micrometer)
Complete blood counts as clinically necessary; type and screen (blood type) prior to initiating therapy; signs/symptoms of infusion reactions
Darbepoetin Level 1
25, 40, 60, 100, 150, 200, 300, or 500 mcg
No additional dilution
IV push: over at least 1 min Infusion Rate: Over 1-3 min
Central or peripheral Blood pressure, line clotting
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
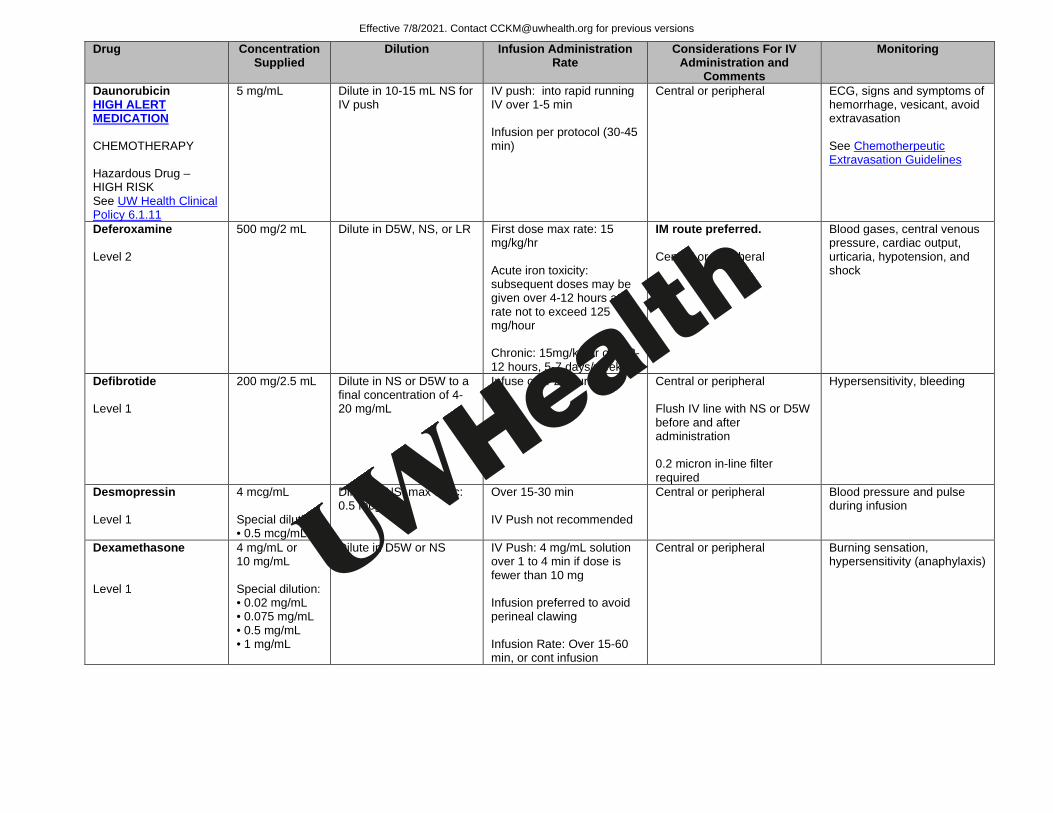
Daunorubicin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
5 mg/mL Dilute in 10-15 mL NS for IV push
IV push: into rapid running IV over 1-5 min Infusion per protocol (30-45 min)
Central or peripheral ECG, signs and symptoms of hemorrhage, vesicant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Deferoxamine Level 2
500 mg/2 mL Dilute in D5W, NS, or LR
First dose max rate: 15 mg/kg/hr Acute iron toxicity: subsequent doses may be given over 4-12 hours at a rate not to exceed 125 mg/hour Chronic: 15mg/kg/hr over 8-12 hours, 5-7 days/week
IM route preferred. Central or peripheral
Blood gases, central venous pressure, cardiac output, urticaria, hypotension, and shock
Defibrotide Level 1
200 mg/2.5 mL Dilute in NS or D5W to a final concentration of 4-20 mg/mL
Infuse over 2 hours Central or peripheral Flush IV line with NS or D5W before and after administration 0.2 micron in-line filter required
Hypersensitivity, bleeding
Desmopressin Level 1
4 mcg/mL Special dilution: • 0.5 mcg/mL
Dilute in NS; max conc: 0.5 mcg/mL
Over 15-30 min IV Push not recommended
Central or peripheral Blood pressure and pulse during infusion
Dexamethasone Level 1
4 mg/mL or 10 mg/mL Special dilution: • 0.02 mg/mL • 0.075 mg/mL • 0.5 mg/mL • 1 mg/mL
Dilute in D5W or NS
IV Push: 4 mg/mL solution over 1 to 4 min if dose is fewer than 10 mg Infusion preferred to avoid perineal clawing Infusion Rate: Over 15-60 min, or cont infusion
Central or peripheral Burning sensation, hypersensitivity (anaphylaxis)
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
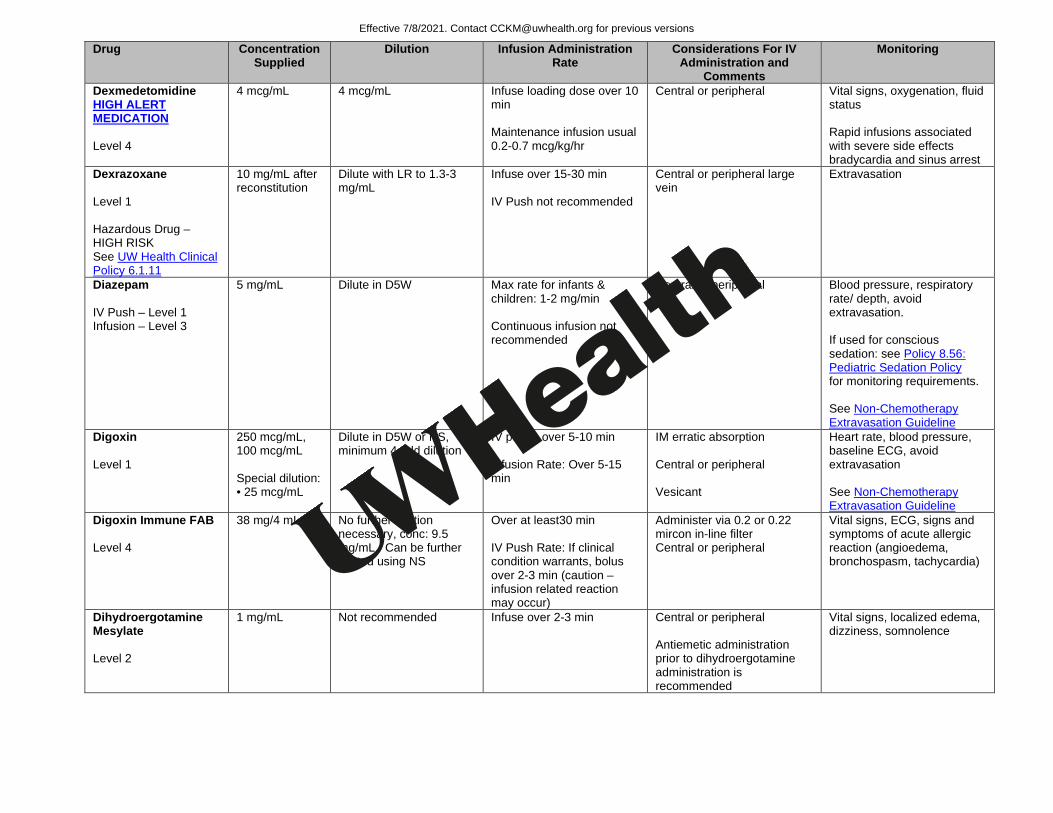
Dexmedetomidine HIGH ALERT MEDICATION Level 4
4 mcg/mL 4 mcg/mL Infuse loading dose over 10 min Maintenance infusion usual 0.2-0.7 mcg/kg/hr
Central or peripheral Vital signs, oxygenation, fluid status Rapid infusions associated with severe side effects bradycardia and sinus arrest
Dexrazoxane Level 1 Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/mL after reconstitution
Dilute with LR to 1.3-3 mg/mL
Infuse over 15-30 min IV Push not recommended
Central or peripheral large vein
Extravasation
Diazepam IV Push – Level 1 Infusion – Level 3
5 mg/mL Dilute in D5W
Max rate for infants & children: 1-2 mg/min Continuous infusion not recommended
Central or peripheral Blood pressure, respiratory rate/ depth, avoid extravasation. If used for conscious sedation: see Policy 8.56: Pediatric Sedation Policy for monitoring requirements. See Non-Chemotherapy Extravasation Guideline
Digoxin Level 1
250 mcg/mL, 100 mcg/mL Special dilution: • 25 mcg/mL
Dilute in D5W or NS, minimum 4-fold dilution
IV push: over 5-10 min Infusion Rate: Over 5-15 min
IM erratic absorption Central or peripheral Vesicant
Heart rate, blood pressure, baseline ECG, avoid extravasation See Non-Chemotherapy Extravasation Guideline
Digoxin Immune FAB Level 4
38 mg/4 mL vial No further dilution necessary, conc: 9.5 mg/mL. Can be further diluted using NS
Over at least30 min IV Push Rate: If clinical condition warrants, bolus over 2-3 min (caution – infusion related reaction may occur)
Administer via 0.2 or 0.22 mircon in-line filter Central or peripheral
Vital signs, ECG, signs and symptoms of acute allergic reaction (angioedema, bronchospasm, tachycardia)
Dihydroergotamine Mesylate Level 2
1 mg/mL Not recommended Infuse over 2-3 min Central or peripheral Antiemetic administration prior to dihydroergotamine administration is recommended
Vital signs, localized edema, dizziness, somnolence
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
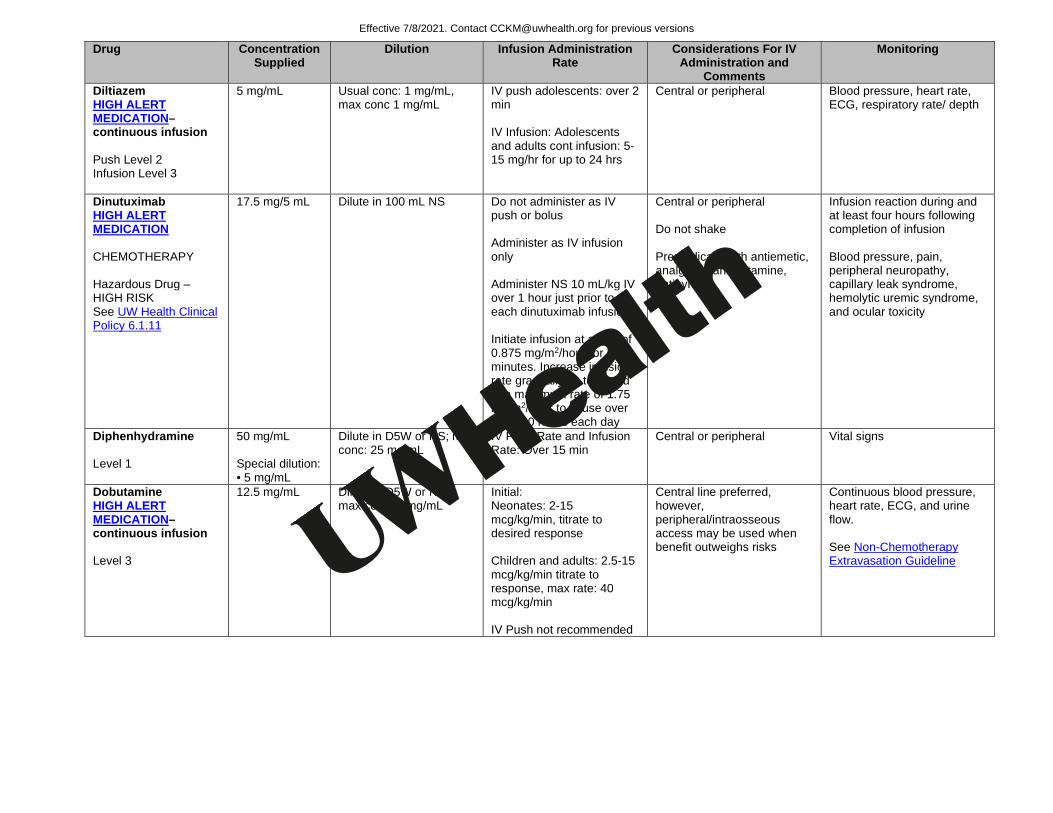
Diltiazem HIGH ALERT MEDICATION–continuous infusion Push Level 2 Infusion Level 3
5 mg/mL Usual conc: 1 mg/mL, max conc 1 mg/mL
IV push adolescents: over 2 min IV Infusion: Adolescents and adults cont infusion: 5-15 mg/hr for up to 24 hrs
Central or peripheral Blood pressure, heart rate, ECG, respiratory rate/ depth
Dinutuximab HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
17.5 mg/5 mL Dilute in 100 mL NS Do not administer as IV push or bolus Administer as IV infusion only Administer NS 10 mL/kg IV over 1 hour just prior to each dinutuximab infusion Initiate infusion at a rate of 0.875 mg/m2/hour for 30 minutes. Increase infusion rate gradually as tolerated to a maximum rate of 1.75 mg/m2/hour to infuse over 10 to 20 hours each day
Central or peripheral Do not shake Premedicate with antiemetic, analgesic, antihistamine, antipyretic
Infusion reaction during and at least four hours following completion of infusion Blood pressure, pain, peripheral neuropathy, capillary leak syndrome, hemolytic uremic syndrome, and ocular toxicity
Diphenhydramine Level 1
50 mg/mL Special dilution: • 5 mg/mL
Dilute in D5W or NS; max conc: 25 mg/mL
IV Push Rate and Infusion Rate: Over 15 min
Central or peripheral Vital signs
Dobutamine HIGH ALERT MEDICATION–continuous infusion Level 3
12.5 mg/mL Dilute in D5W or NS; max conc: 5 mg/mL
Initial: Neonates: 2-15 mcg/kg/min, titrate to desired response Children and adults: 2.5-15 mcg/kg/min titrate to response, max rate: 40 mcg/kg/min IV Push not recommended
Central line preferred, however, peripheral/intraosseous access may be used when benefit outweighs risks
Continuous blood pressure, heart rate, ECG, and urine flow. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
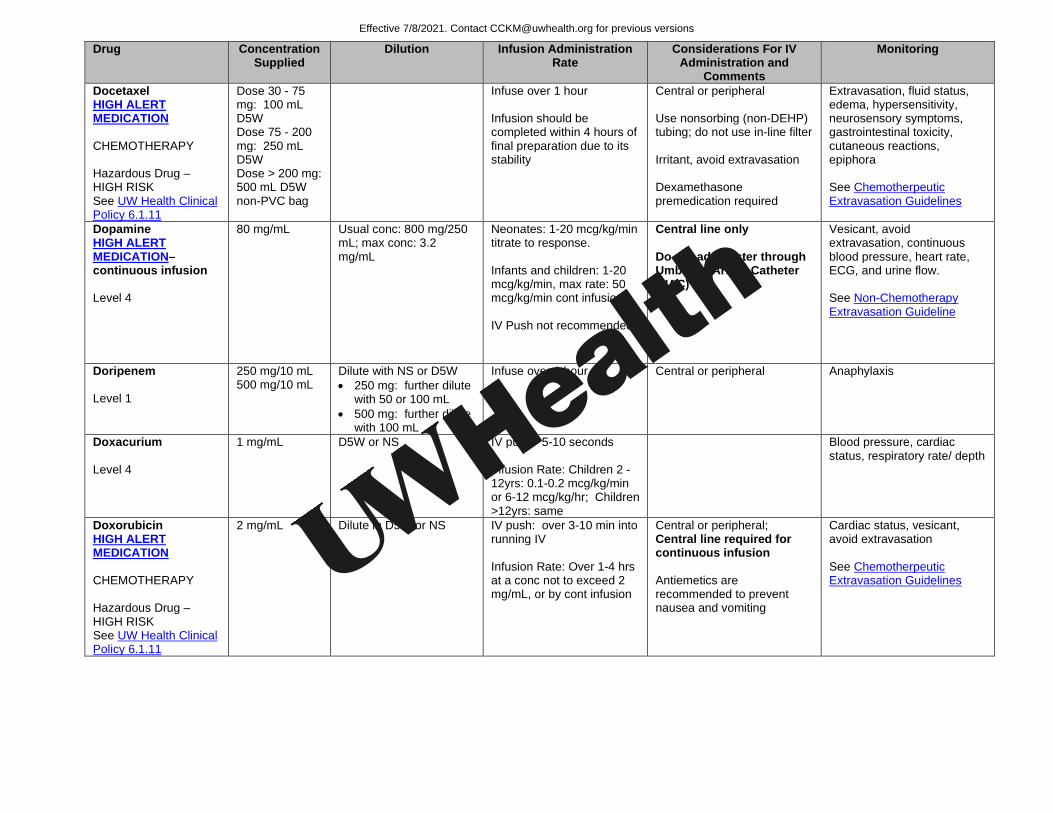
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Docetaxel HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
Dose 30 - 75 mg: 100 mL D5W Dose 75 - 200 mg: 250 mL D5W Dose > 200 mg: 500 mL D5W non-PVC bag
Infuse over 1 hour Infusion should be completed within 4 hours of final preparation due to its stability
Central or peripheral Use nonsorbing (non-DEHP) tubing; do not use in-line filter Irritant, avoid extravasation Dexamethasone premedication required
Extravasation, fluid status, edema, hypersensitivity, neurosensory symptoms, gastrointestinal toxicity, cutaneous reactions, epiphora See Chemotherpeutic Extravasation Guidelines
Dopamine HIGH ALERT MEDICATION–continuous infusion Level 4
80 mg/mL Usual conc: 800 mg/250 mL; max conc: 3.2 mg/mL
Neonates: 1-20 mcg/kg/min titrate to response. Infants and children: 1-20 mcg/kg/min, max rate: 50 mcg/kg/min cont infusion IV Push not recommended
Central line only Do not administer through Umbilical Artery Catheter (UAC)
Vesicant, avoid extravasation, continuous blood pressure, heart rate, ECG, and urine flow. See Non-Chemotherapy Extravasation Guideline
Doripenem Level 1
250 mg/10 mL 500 mg/10 mL
Dilute with NS or D5W • 250 mg: further dilute
with 50 or 100 mL • 500 mg: further dilute
with 100 mL
Infuse over 1 hour Central or peripheral Anaphylaxis
Doxacurium Level 4
1 mg/mL D5W or NS IV push: 5-10 seconds Infusion Rate: Children 2 -12yrs: 0.1-0.2 mcg/kg/min or 6-12 mcg/kg/hr; Children >12yrs: same
Blood pressure, cardiac status, respiratory rate/ depth
Doxorubicin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
2 mg/mL Dilute in D5W or NS
IV push: over 3-10 min into running IV Infusion Rate: Over 1-4 hrs at a conc not to exceed 2 mg/mL, or by cont infusion
Central or peripheral; Central line required for continuous infusion Antiemetics are recommended to prevent nausea and vomiting
Cardiac status, vesicant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Doxycycline Level 1
100 mg/10 mL Special dilution: • 1 mg/mL
Dilute in mL D5W or NS
Over 1hours ; conc not to exceed 1 mg/mL (conc <0.1 mg/mL not recommended) IV Push not recommended
Central or peripheral Vein irritation, thrombophlebitis, avoid extravasation See Non-Chemotherapy Extravasation Guideline
Droperidol Level 1
2.5 mg/mL Special dilution: • 0.25 mg/mL
Dilute in D5W or LR; max conc: 2.5 mg/mL
IV push: over 2-5 min Infusion: No information
Central or peripheral Vital signs, respiratory rate/ depth, palpitations, syncope, ECG prior to use and continued through first 2-3 hrs following administration
Eculizumab Level 1
10 mg/mL Dilute to concentration of 5 mg/mL in D5W, NS, 1/2NS, or LR
Do not administer as IV push or bolus Infuse over 1-4 hours Decrease rate or discontinue for infusion reactions
Central or peripheral Do not shake
Infusion reaction Monitor for infusion reaction for 1 hour after infusion
Edetate calcium disodium Level 2
200 mg/mL Dilute in 250-500 mL D5W or NS
IV infusion: Asymptomatic patients over at least 1 hour, symptomatic patients over at least 2 hours IV Push not recommended
Central or peripheral ECG and vital signs
Edrophonium Chloride Level 2
10 mg/mL Dilute in D5W or NS
IV Push Rate: Children: 0.04 mg/kg over 1 min followed by 0.16mg/kg given within 45 seconds (if no response, max total dose 10 mg) Infusion: No information Infants Initial: 0.1 mg, followed by 0.4 mg (if no response, total dose 0.5mg)
Central or peripheral Blood pressure, cardiac status
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
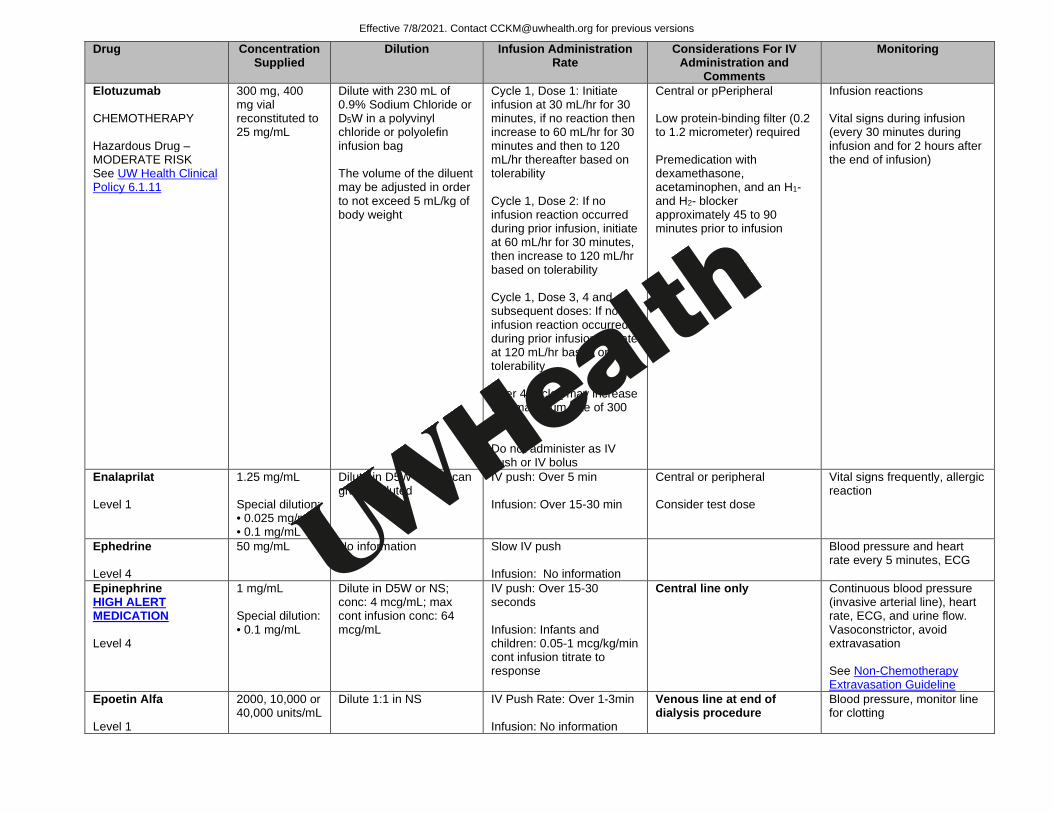
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Elotuzumab CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
300 mg, 400 mg vial reconstituted to 25 mg/mL
Dilute with 230 mL of 0.9% Sodium Chloride or D5W in a polyvinyl chloride or polyolefin infusion bag The volume of the diluent may be adjusted in order to not exceed 5 mL/kg of body weight
Cycle 1, Dose 1: Initiate infusion at 30 mL/hr for 30 minutes, if no reaction then increase to 60 mL/hr for 30 minutes and then to 120 mL/hr thereafter based on tolerability Cycle 1, Dose 2: If no infusion reaction occurred during prior infusion, initiate at 60 mL/hr for 30 minutes, then increase to 120 mL/hr based on tolerability Cycle 1, Dose 3, 4 and all subsequent doses: If no infusion reaction occurred during prior infusion, initiate at 120 mL/hr based on tolerability After 4 cycles may increase to a maximum rate of 300 mL/hr Do not administer as IV push or IV bolus
Central or pPeripheral Low protein-binding filter (0.2 to 1.2 micrometer) required Premedication with dexamethasone, acetaminophen, and an H1- and H2- blocker approximately 45 to 90 minutes prior to infusion
Infusion reactions Vital signs during infusion (every 30 minutes during infusion and for 2 hours after the end of infusion)
Enalaprilat Level 1
1.25 mg/mL Special dilution: • 0.025 mg/mL • 0.1 mg/mL
Dilute in D5W or NS; can give undiluted
IV push: Over 5 min Infusion: Over 15-30 min
Central or peripheral Consider test dose
Vital signs frequently, allergic reaction
Ephedrine Level 4
50 mg/mL No information Slow IV push Infusion: No information
Blood pressure and heart rate every 5 minutes, ECG
Epinephrine HIGH ALERT MEDICATION Level 4
1 mg/mL Special dilution: • 0.1 mg/mL
Dilute in D5W or NS; conc: 4 mcg/mL; max cont infusion conc: 64 mcg/mL
IV push: Over 15-30 seconds Infusion: Infants and children: 0.05-1 mcg/kg/min cont infusion titrate to response
Central line only Continuous blood pressure (invasive arterial line), heart rate, ECG, and urine flow. Vasoconstrictor, avoid extravasation See Non-Chemotherapy Extravasation Guideline
Epoetin Alfa Level 1
2000, 10,000 or 40,000 units/mL
Dilute 1:1 in NS IV Push Rate: Over 1-3min Infusion: No information
Venous line at end of dialysis procedure
Blood pressure, monitor line for clotting
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
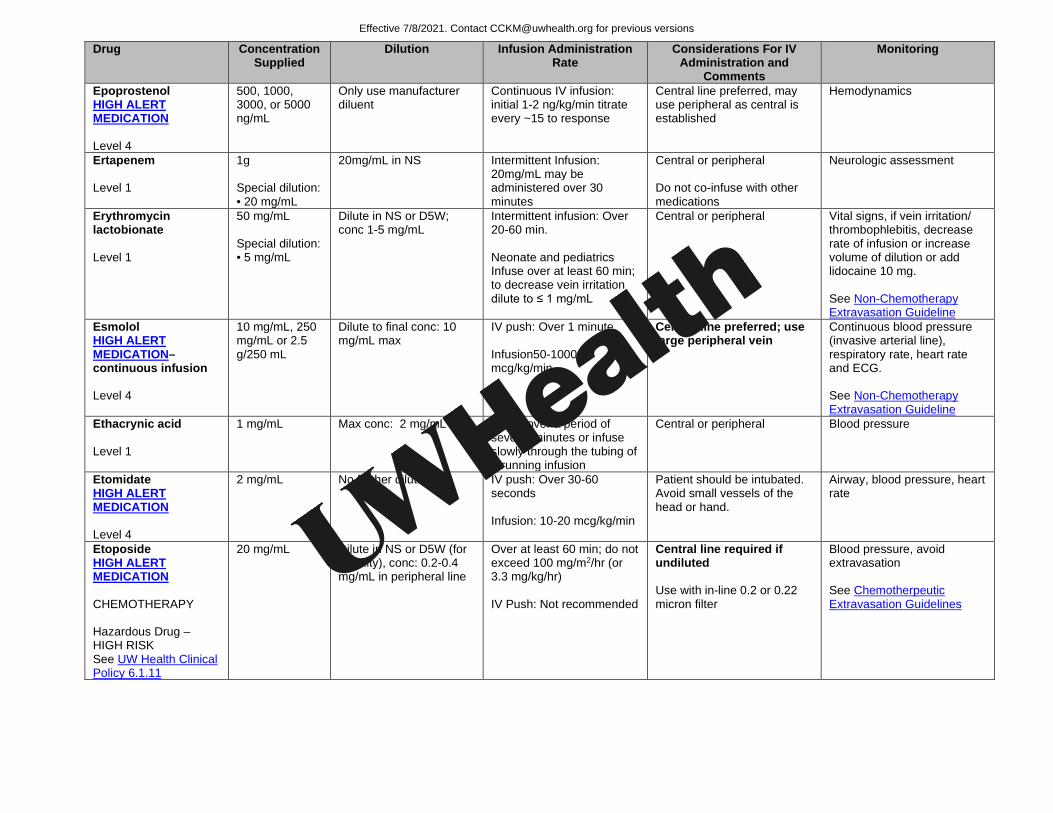
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Epoprostenol HIGH ALERT MEDICATION Level 4
500, 1000, 3000, or 5000 ng/mL
Only use manufacturer diluent
Continuous IV infusion: initial 1-2 ng/kg/min titrate every ~15 to response
Central line preferred, may use peripheral as central is established
Hemodynamics
Ertapenem Level 1
1g Special dilution: • 20 mg/mL
20mg/mL in NS Intermittent Infusion: 20mg/mL may be administered over 30 minutes
Central or peripheral Do not co-infuse with other medications
Neurologic assessment
Erythromycin lactobionate Level 1
50 mg/mL Special dilution: • 5 mg/mL
Dilute in NS or D5W; conc 1-5 mg/mL
Intermittent infusion: Over 20-60 min. Neonate and pediatrics Infuse over at least 60 min; to decrease vein irritation dilute to ≤ 1 mg/mL
Central or peripheral Vital signs, if vein irritation/ thrombophlebitis, decrease rate of infusion or increase volume of dilution or add lidocaine 10 mg. See Non-Chemotherapy Extravasation Guideline
Esmolol HIGH ALERT MEDICATION–continuous infusion Level 4
10 mg/mL, 250 mg/mL or 2.5 g/250 mL
Dilute to final conc: 10 mg/mL max
IV push: Over 1 minute Infusion50-1000 mcg/kg/min
Central line preferred; use large peripheral vein
Continuous blood pressure (invasive arterial line), respiratory rate, heart rate and ECG. See Non-Chemotherapy Extravasation Guideline
Ethacrynic acid Level 1
1 mg/mL Max conc: 2 mg/mL Infuse over a period of several minutes or infuse slowly through the tubing of a running infusion
Central or peripheral Blood pressure
Etomidate HIGH ALERT MEDICATION Level 4
2 mg/mL No further dilution IV push: Over 30-60 seconds Infusion: 10-20 mcg/kg/min
Patient should be intubated. Avoid small vessels of the head or hand.
Airway, blood pressure, heart rate
Etoposide HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
20 mg/mL Dilute in NS or D5W (for stability), conc: 0.2-0.4 mg/mL in peripheral line
Over at least 60 min; do not exceed 100 mg/m2/hr (or 3.3 mg/kg/hr) IV Push: Not recommended
Central line required if undiluted Use with in-line 0.2 or 0.22 micron filter
Blood pressure, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
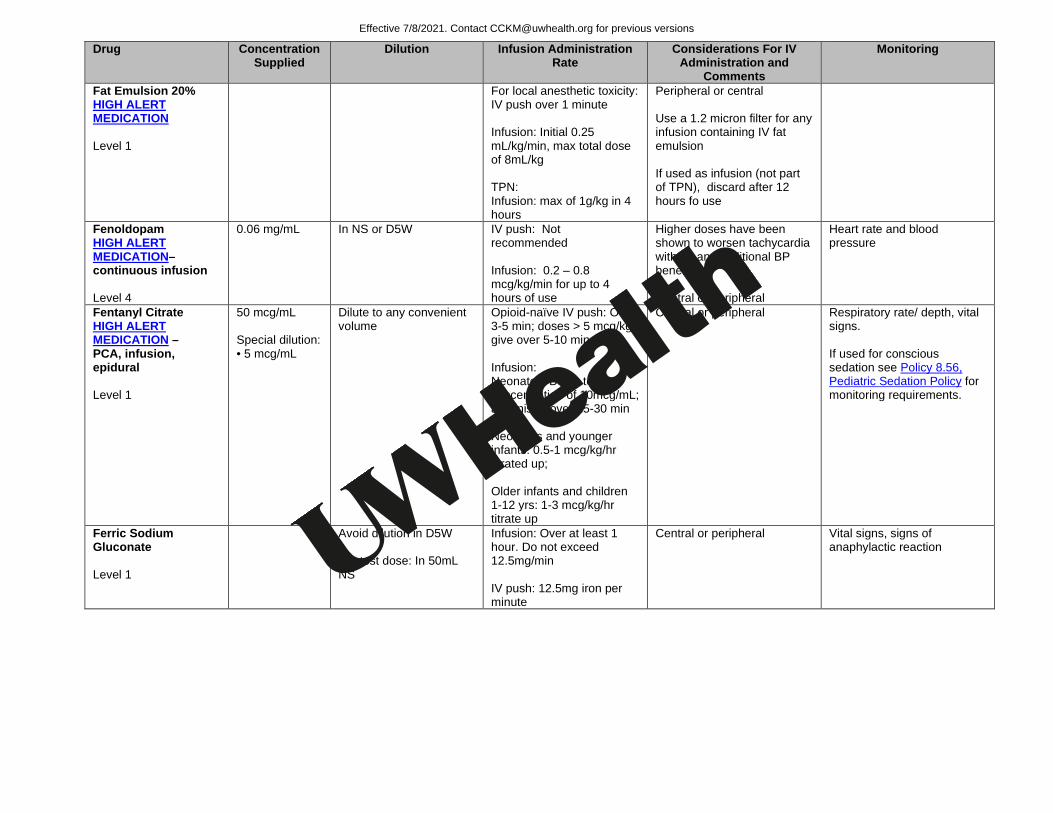
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Fat Emulsion 20% HIGH ALERT MEDICATION Level 1
For local anesthetic toxicity: IV push over 1 minute Infusion: Initial 0.25 mL/kg/min, max total dose of 8mL/kg TPN: Infusion: max of 1g/kg in 4 hours
Peripheral or central Use a 1.2 micron filter for any infusion containing IV fat emulsion If used as infusion (not part of TPN), discard after 12 hours fo use
Fenoldopam HIGH ALERT MEDICATION–continuous infusion Level 4
0.06 mg/mL In NS or D5W IV push: Not recommended Infusion: 0.2 – 0.8 mcg/kg/min for up to 4 hours of use
Higher doses have been shown to worsen tachycardia without any additional BP benefits Central or peripheral
Heart rate and blood pressure
Fentanyl Citrate HIGH ALERT MEDICATION – PCA, infusion, epidural Level 1
50 mcg/mL Special dilution: • 5 mcg/mL
Dilute to any convenient volume
Opioid-naïve IV push: Over 3-5 min; doses > 5 mcg/kg give over 5-10 min Infusion: Neonates: Dilute to a concentration of 10mcg/mL; administer over 15-30 min Neonates and younger infants: 0.5-1 mcg/kg/hr titrated up; Older infants and children 1-12 yrs: 1-3 mcg/kg/hr titrate up
Central or peripheral Respiratory rate/ depth, vital signs. If used for conscious sedation see Policy 8.56, Pediatric Sedation Policy for monitoring requirements.
Ferric Sodium Gluconate Level 1
Avoid dilution in D5W For test dose: In 50mL NS
Infusion: Over at least 1 hour. Do not exceed 12.5mg/min IV push: 12.5mg iron per minute
Central or peripheral Vital signs, signs of anaphylactic reaction
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
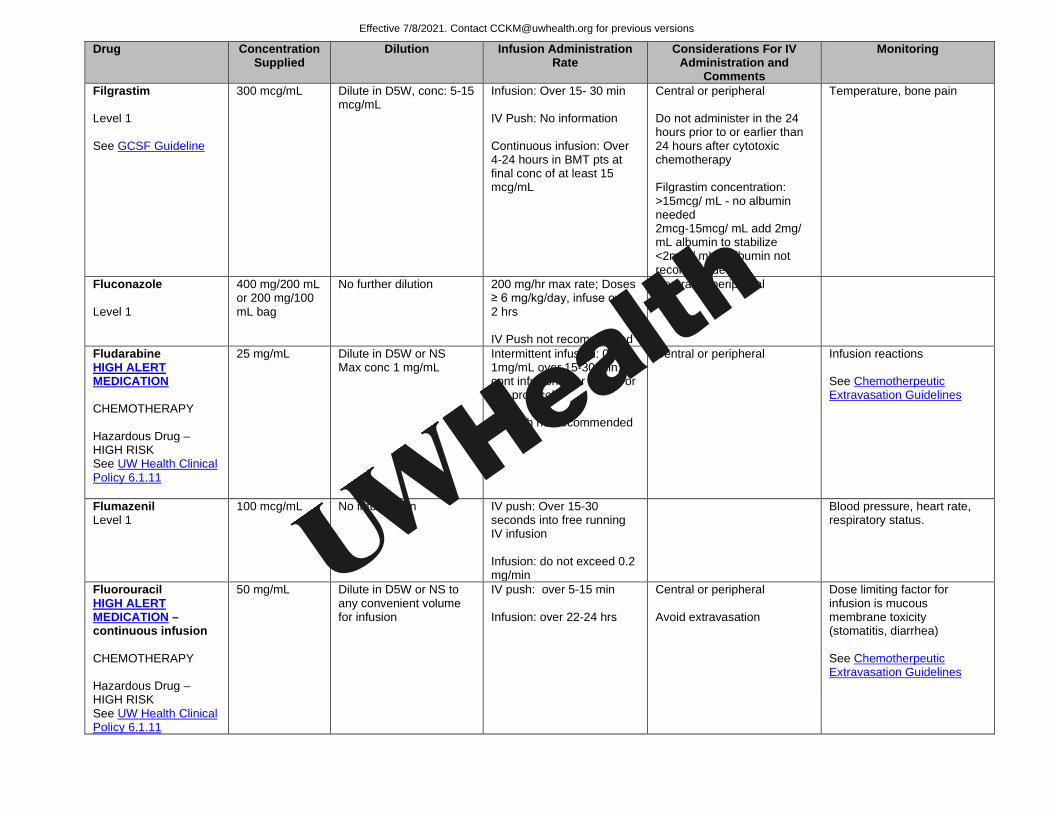
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Filgrastim Level 1 See GCSF Guideline
300 mcg/mL Dilute in D5W, conc: 5-15 mcg/mL
Infusion: Over 15- 30 min IV Push: No information Continuous infusion: Over 4-24 hours in BMT pts at final conc of at least 15 mcg/mL
Central or peripheral Do not administer in the 24 hours prior to or earlier than 24 hours after cytotoxic chemotherapy Filgrastim concentration: >15mcg/ mL - no albumin needed 2mcg-15mcg/ mL add 2mg/ mL albumin to stabilize <2mcg/ mL – albumin not recommended.
Temperature, bone pain
Fluconazole Level 1
400 mg/200 mL or 200 mg/100 mL bag
No further dilution
200 mg/hr max rate; Doses ≥ 6 mg/kg/day, infuse over 2 hrs IV Push not recommended
Central or peripheral
Fludarabine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
25 mg/mL Dilute in D5W or NS Max conc 1 mg/mL
Intermittent infusion: 0.25-1mg/mL over 15-30 min; or cont infusion over 24 hrs or per protocol IV Push not recommended
Central or peripheral Infusion reactions See Chemotherpeutic Extravasation Guidelines
Flumazenil Level 1
100 mcg/mL No information IV push: Over 15-30 seconds into free running IV infusion Infusion: do not exceed 0.2 mg/min
Blood pressure, heart rate, respiratory status.
Fluorouracil HIGH ALERT MEDICATION –continuous infusion CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
50 mg/mL Dilute in D5W or NS to any convenient volume for infusion
IV push: over 5-15 min Infusion: over 22-24 hrs
Central or peripheral Avoid extravasation
Dose limiting factor for infusion is mucous membrane toxicity (stomatitis, diarrhea) See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
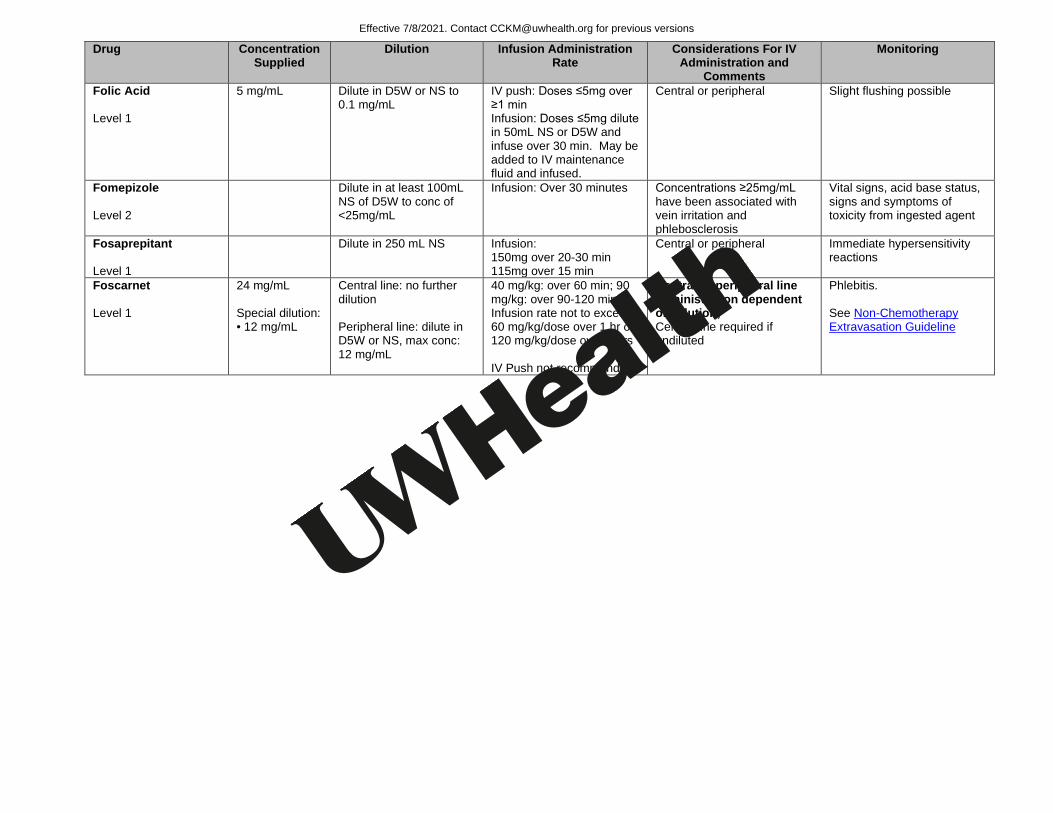
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Folic Acid Level 1
5 mg/mL Dilute in D5W or NS to 0.1 mg/mL
IV push: Doses ≤5mg over ≥1 min Infusion: Doses ≤5mg dilute in 50mL NS or D5W and infuse over 30 min. May be added to IV maintenance fluid and infused.
Central or peripheral Slight flushing possible
Fomepizole Level 2
Dilute in at least 100mL NS of D5W to conc of <25mg/mL
Infusion: Over 30 minutes Concentrations ≥25mg/mL have been associated with vein irritation and phlebosclerosis
Vital signs, acid base status, signs and symptoms of toxicity from ingested agent
Fosaprepitant Level 1
Dilute in 250 mL NS Infusion: 150mg over 20-30 min 115mg over 15 min
Central or peripheral Immediate hypersensitivity reactions
Foscarnet Level 1
24 mg/mL Special dilution: • 12 mg/mL
Central line: no further dilution Peripheral line: dilute in D5W or NS, max conc: 12 mg/mL
40 mg/kg: over 60 min; 90 mg/kg: over 90-120 min Infusion rate not to exceed 60 mg/kg/dose over 1 hr or 120 mg/kg/dose over 2 hrs IV Push not recommended
Central or peripheral line administration dependent on dilution; Central line required if undiluted
Phlebitis. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
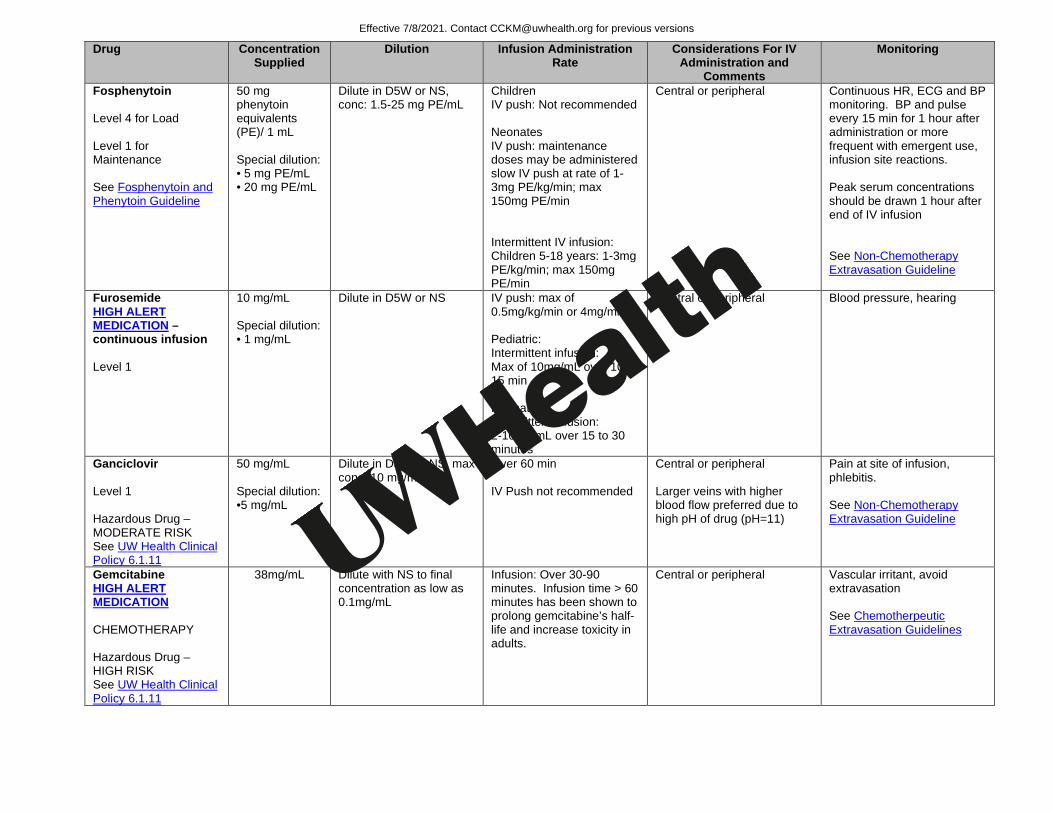
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Fosphenytoin Level 4 for Load Level 1 for Maintenance See Fosphenytoin and Phenytoin Guideline
50 mg phenytoin equivalents (PE)/ 1 mL Special dilution: • 5 mg PE/mL • 20 mg PE/mL
Dilute in D5W or NS, conc: 1.5-25 mg PE/mL
Children IV push: Not recommended Neonates IV push: maintenance doses may be administered slow IV push at rate of 1-3mg PE/kg/min; max 150mg PE/min Intermittent IV infusion: Children 5-18 years: 1-3mg PE/kg/min; max 150mg PE/min
Central or peripheral Continuous HR, ECG and BP monitoring. BP and pulse every 15 min for 1 hour after administration or more frequent with emergent use, infusion site reactions. Peak serum concentrations should be drawn 1 hour after end of IV infusion See Non-Chemotherapy Extravasation Guideline
Furosemide HIGH ALERT MEDICATION –continuous infusion Level 1
10 mg/mL Special dilution: • 1 mg/mL
Dilute in D5W or NS
IV push: max of 0.5mg/kg/min or 4mg/min Pediatric: Intermittent infusion: Max of 10mg/mL over 10-15 min Neonates Intermittent infusion: 2-10mg/mL over 15 to 30 minutes
Central or peripheral Blood pressure, hearing
Ganciclovir Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
50 mg/mL Special dilution: •5 mg/mL
Dilute in D5W or NS, max conc: 10 mg/mL
Over 60 min IV Push not recommended
Central or peripheral Larger veins with higher blood flow preferred due to high pH of drug (pH=11)
Pain at site of infusion, phlebitis. See Non-Chemotherapy Extravasation Guideline
Gemcitabine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
38mg/mL Dilute with NS to final concentration as low as 0.1mg/mL
Infusion: Over 30-90 minutes. Infusion time > 60 minutes has been shown to prolong gemcitabine’s half-life and increase toxicity in adults.
Central or peripheral Vascular irritant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
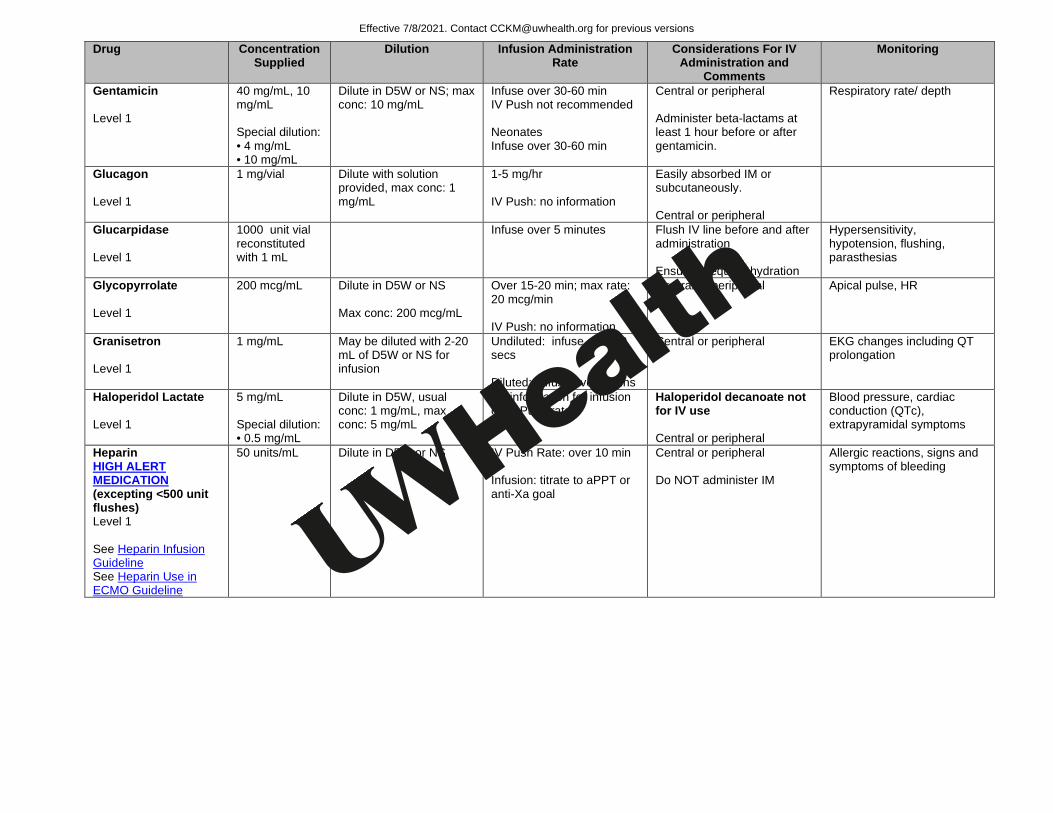
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Gentamicin Level 1
40 mg/mL, 10 mg/mL Special dilution: • 4 mg/mL • 10 mg/mL
Dilute in D5W or NS; max conc: 10 mg/mL
Infuse over 30-60 min IV Push not recommended Neonates Infuse over 30-60 min
Central or peripheral Administer beta-lactams at least 1 hour before or after gentamicin.
Respiratory rate/ depth
Glucagon Level 1
1 mg/vial Dilute with solution provided, max conc: 1 mg/mL
1-5 mg/hr IV Push: no information
Easily absorbed IM or subcutaneously. Central or peripheral
Glucarpidase Level 1
1000 unit vial reconstituted with 1 mL
Infuse over 5 minutes Flush IV line before and after administration Ensure adequate hydration
Hypersensitivity, hypotension, flushing, parasthesias
Glycopyrrolate Level 1
200 mcg/mL Dilute in D5W or NS Max conc: 200 mcg/mL
Over 15-20 min; max rate: 20 mcg/min IV Push: no information
Central or peripheral Apical pulse, HR
Granisetron Level 1
1 mg/mL May be diluted with 2-20 mL of D5W or NS for infusion
Undiluted: infuse over 30 secs Diluted: infuse over 5 mins
Central or peripheral EKG changes including QT prolongation
Haloperidol Lactate Level 1
5 mg/mL Special dilution: • 0.5 mg/mL
Dilute in D5W, usual conc: 1 mg/mL, max conc: 5 mg/mL
No information for infusion or IV Push rate
Haloperidol decanoate not for IV use Central or peripheral
Blood pressure, cardiac conduction (QTc), extrapyramidal symptoms
Heparin HIGH ALERT MEDICATION (excepting <500 unit flushes) Level 1 See Heparin Infusion Guideline See Heparin Use in ECMO Guideline
50 units/mL Dilute in D5W or NS
IV Push Rate: over 10 min Infusion: titrate to aPPT or anti-Xa goal
Central or peripheral Do NOT administer IM
Allergic reactions, signs and symptoms of bleeding
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
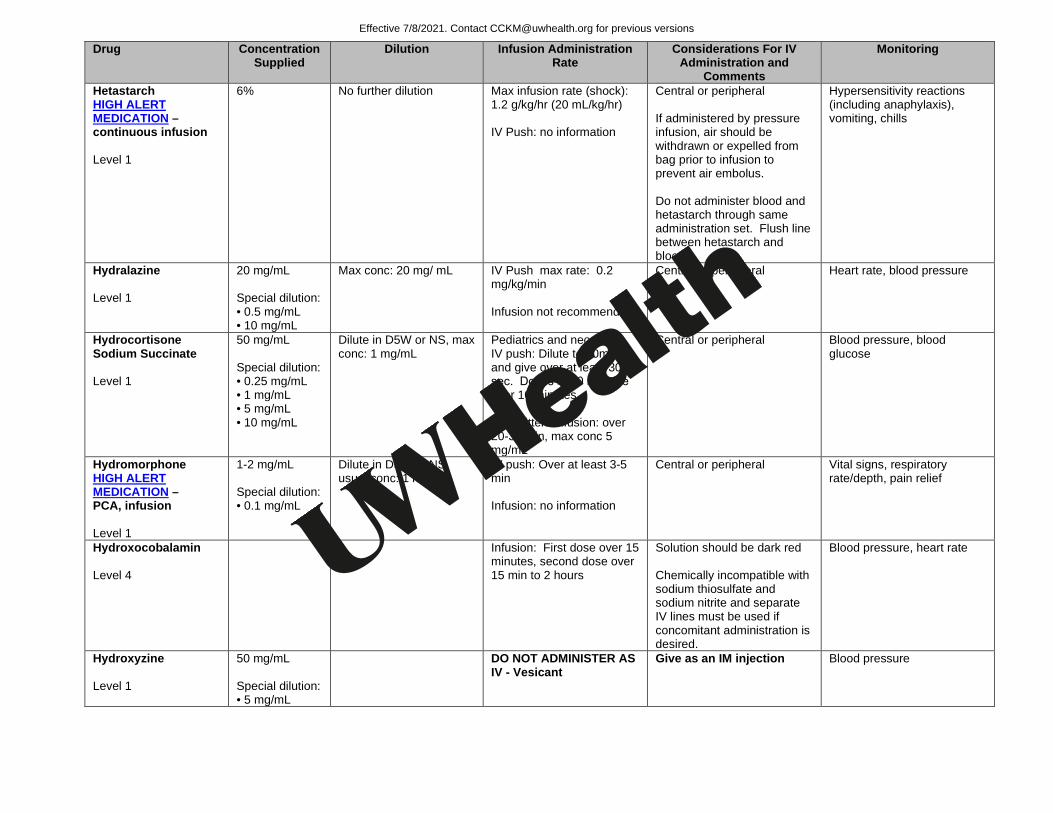
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Hetastarch HIGH ALERT MEDICATION –continuous infusion Level 1
6% No further dilution
Max infusion rate (shock): 1.2 g/kg/hr (20 mL/kg/hr) IV Push: no information
Central or peripheral If administered by pressure infusion, air should be withdrawn or expelled from bag prior to infusion to prevent air embolus. Do not administer blood and hetastarch through same administration set. Flush line between hetastarch and blood.
Hypersensitivity reactions (including anaphylaxis), vomiting, chills
Hydralazine Level 1
20 mg/mL Special dilution: • 0.5 mg/mL • 10 mg/mL
Max conc: 20 mg/ mL
IV Push max rate: 0.2 mg/kg/min Infusion not recommended
Central or peripheral Heart rate, blood pressure
Hydrocortisone Sodium Succinate Level 1
50 mg/mL Special dilution: • 0.25 mg/mL • 1 mg/mL • 5 mg/mL • 10 mg/mL
Dilute in D5W or NS, max conc: 1 mg/mL
Pediatrics and neonates IV push: Dilute to 50mg/mL and give over at least 30 sec. Doses ≥500 mg give over 10 minutes. Intermittent infusion: over 20-30 min, max conc 5 mg/mL
Central or peripheral Blood pressure, blood glucose
Hydromorphone HIGH ALERT MEDICATION – PCA, infusion Level 1
1-2 mg/mL Special dilution: • 0.1 mg/mL
Dilute in D5W or NS, usual conc: 1 mg/mL
IV push: Over at least 3-5 min Infusion: no information
Central or peripheral Vital signs, respiratory rate/depth, pain relief
Hydroxocobalamin Level 4
Infusion: First dose over 15 minutes, second dose over 15 min to 2 hours
Solution should be dark red Chemically incompatible with sodium thiosulfate and sodium nitrite and separate IV lines must be used if concomitant administration is desired.
Blood pressure, heart rate
Hydroxyzine Level 1
50 mg/mL Special dilution: • 5 mg/mL
DO NOT ADMINISTER AS IV - Vesicant
Give as an IM injection Blood pressure
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
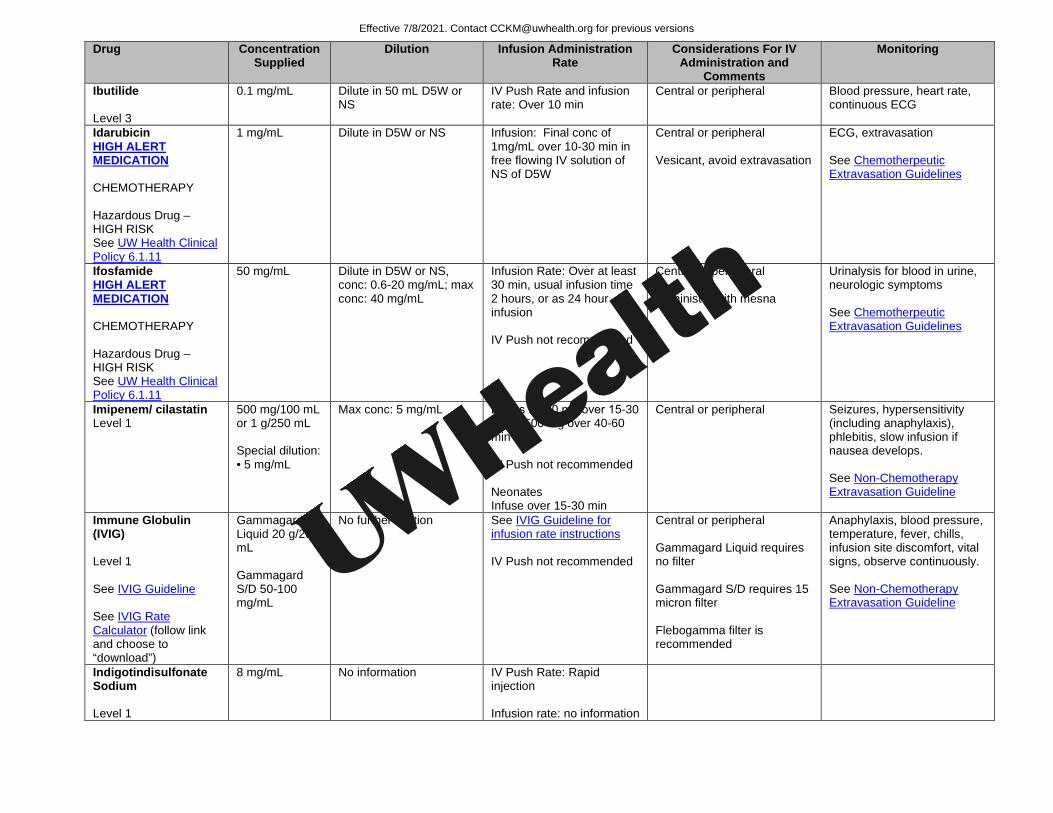
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Ibutilide Level 3
0.1 mg/mL Dilute in 50 mL D5W or NS
IV Push Rate and infusion rate: Over 10 min
Central or peripheral Blood pressure, heart rate, continuous ECG
Idarubicin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute in D5W or NS Infusion: Final conc of 1mg/mL over 10-30 min in free flowing IV solution of NS of D5W
Central or peripheral Vesicant, avoid extravasation
ECG, extravasation See Chemotherpeutic Extravasation Guidelines
Ifosfamide HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
50 mg/mL Dilute in D5W or NS, conc: 0.6-20 mg/mL; max conc: 40 mg/mL
Infusion Rate: Over at least 30 min, usual infusion time 2 hours, or as 24 hour infusion IV Push not recommended
Central or peripheral Administer with mesna
Urinalysis for blood in urine, neurologic symptoms See Chemotherpeutic Extravasation Guidelines
Imipenem/ cilastatin Level 1
500 mg/100 mL or 1 g/250 mL Special dilution: • 5 mg/mL
Max conc: 5 mg/mL
Doses ≤ 500 mg over 15-30 min, >500 mg over 40-60 min IV Push not recommended Neonates Infuse over 15-30 min
Central or peripheral Seizures, hypersensitivity (including anaphylaxis), phlebitis, slow infusion if nausea develops. See Non-Chemotherapy Extravasation Guideline
Immune Globulin (IVIG) Level 1 See IVIG Guideline See IVIG Rate Calculator (follow link and choose to “download”)
Gammagard Liquid 20 g/200 mL Gammagard S/D 50-100 mg/mL
No further dilution See IVIG Guideline for infusion rate instructions IV Push not recommended
Central or peripheral Gammagard Liquid requires no filter Gammagard S/D requires 15 micron filter Flebogamma filter is recommended
Anaphylaxis, blood pressure, temperature, fever, chills, infusion site discomfort, vital signs, observe continuously. See Non-Chemotherapy Extravasation Guideline
Indigotindisulfonate Sodium Level 1
8 mg/mL No information IV Push Rate: Rapid injection Infusion rate: no information
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Indomethacin Level 2
Dilute in preservative free SWI or preservative free NS
Pediatrics: Infusion: Over 20-30 minutes at concentration of 0.5-1mg/mL Neonatal: Infusion: Over at least 30 minutes. IV Push: No recommendation
Central or peripheral If treating PDA: HR, murmur, ECG
Infliximab HIGH ALERT MEDICATION Level 1
10 mg/mL Dilute to final volume of 250 mL NS, conc: 0.4-4 mg/ mL
Standard Infusion Rate (over at least 2 hours): Administer at 10 mL/hr for 15 minutes, then 20 mL/hr for 15 minutes, then 40 mL/hr for 15 minutes, then 80 mL/hr for 15 minutes, then 150 mL/hr for 30 minutes, then 250 mL/hr until completed. Rapid Infusion Rate for use in Day Treatment or Campground for IBD patients who have tolerated at least three previous doses of infliximab with Standard Infusion Rate: Administer at 100 mL/hr for 15 min, then 300 mL/hr until completed IV Push Rate: No information
Do not infuse with other drugs. Administer with 0.2 or 0.22 mircon in-line filter Standard Infusion Rate Adverse Reactions: For adverse reactions, stop infusion. When symptoms resolve, resume infusion at 10 mL/hr and follow same titration schedule Rapid Infusion Rate Adverse Reactions: For adverse reactions, stop infusion. When symptoms resolve, resume infusion at 10 mL/hr and follow the standard titration schedule Central or peripheral
Vitals prior to infusion and every 15-30 minutes during infusion including blood pressure, pulse, and respiratory
Insulin, Regular HIGH ALERT MEDICATION –continuous infusion Level 4
100 units/mL Dilute in NS or D5W; usual conc: 0.5-1 unit/mL
IV push: Over 10-15 seconds Infusion: Give at desired rate
Central or peripheral Frequent blood glucose levels
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
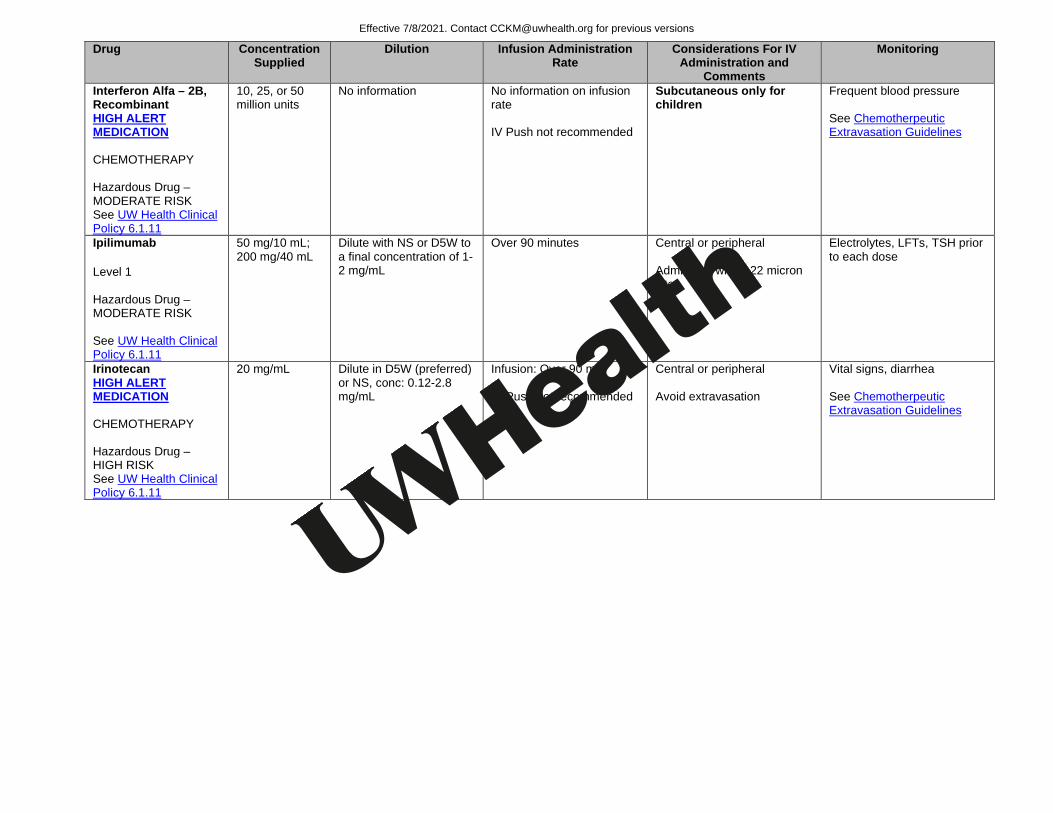
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Interferon Alfa – 2B, Recombinant HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
10, 25, or 50 million units
No information No information on infusion rate IV Push not recommended
Subcutaneous only for children
Frequent blood pressure See Chemotherpeutic Extravasation Guidelines
Ipilimumab Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
50 mg/10 mL; 200 mg/40 mL
Dilute with NS or D5W to a final concentration of 1-2 mg/mL
Over 90 minutes Central or peripheral Administer with 0.22 micron filter
Electrolytes, LFTs, TSH prior to each dose
Irinotecan HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
20 mg/mL Dilute in D5W (preferred) or NS, conc: 0.12-2.8 mg/mL
Infusion: Over 90 min IV Push not recommended
Central or peripheral Avoid extravasation
Vital signs, diarrhea See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
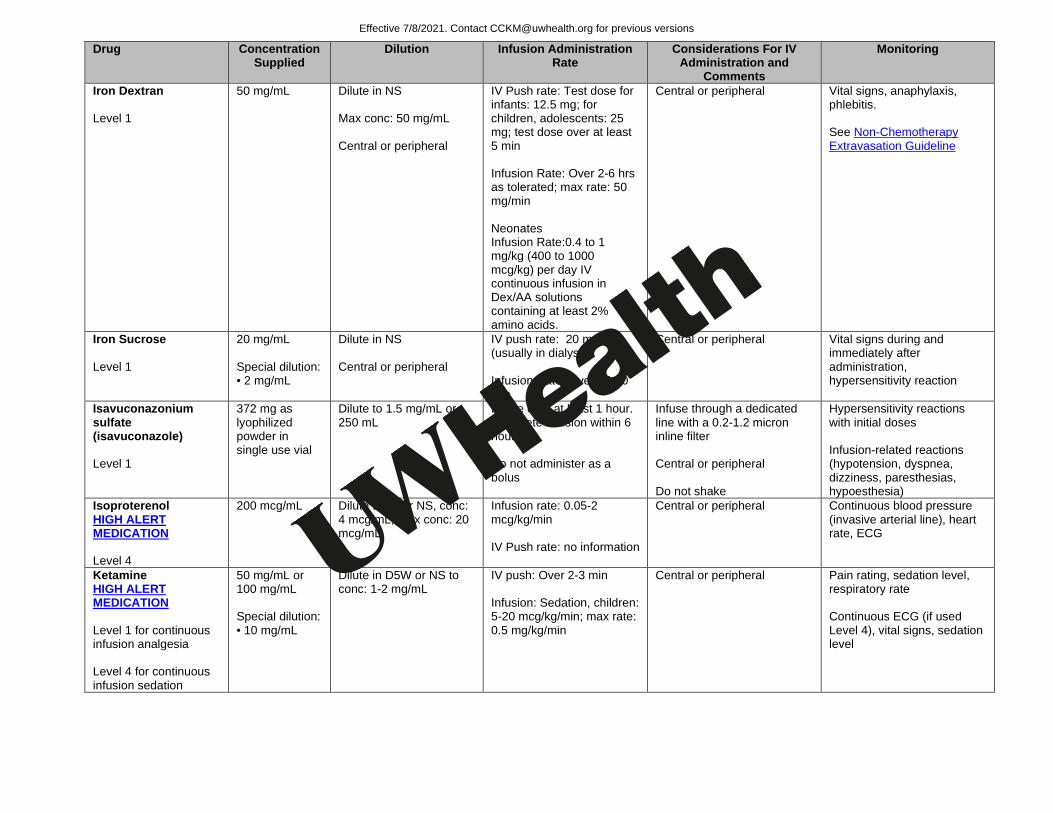
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Iron Dextran Level 1
50 mg/mL Dilute in NS Max conc: 50 mg/mL Central or peripheral
IV Push rate: Test dose for infants: 12.5 mg; for children, adolescents: 25 mg; test dose over at least 5 min Infusion Rate: Over 2-6 hrs as tolerated; max rate: 50 mg/min Neonates Infusion Rate:0.4 to 1 mg/kg (400 to 1000 mcg/kg) per day IV continuous infusion in Dex/AA solutions containing at least 2% amino acids.
Central or peripheral Vital signs, anaphylaxis, phlebitis. See Non-Chemotherapy Extravasation Guideline
Iron Sucrose Level 1
20 mg/mL Special dilution: • 2 mg/mL
Dilute in NS Central or peripheral
IV push rate: 20 mg/min (usually in dialysis) Infusion Rate: Over 15-30 min
Central or peripheral Vital signs during and immediately after administration, hypersensitivity reaction
Isavuconazonium sulfate (isavuconazole) Level 1
372 mg as lyophilized powder in single use vial
Dilute to 1.5 mg/mL or 250 mL
Infuse over at least 1 hour. Complete infusion within 6 hours Do not administer as a bolus
Infuse through a dedicated line with a 0.2-1.2 micron inline filter Central or peripheral Do not shake
Hypersensitivity reactions with initial doses Infusion-related reactions (hypotension, dyspnea, dizziness, paresthesias, hypoesthesia)
Isoproterenol HIGH ALERT MEDICATION Level 4
200 mcg/mL Dilute D5W or NS, conc: 4 mcg/mL; max conc: 20 mcg/mL
Infusion rate: 0.05-2 mcg/kg/min IV Push rate: no information
Central or peripheral Continuous blood pressure (invasive arterial line), heart rate, ECG
Ketamine HIGH ALERT MEDICATION Level 1 for continuous infusion analgesia Level 4 for continuous infusion sedation
50 mg/mL or 100 mg/mL Special dilution: • 10 mg/mL
Dilute in D5W or NS to conc: 1-2 mg/mL
IV push: Over 2-3 min Infusion: Sedation, children: 5-20 mcg/kg/min; max rate: 0.5 mg/kg/min
Central or peripheral Pain rating, sedation level, respiratory rate Continuous ECG (if used Level 4), vital signs, sedation level
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Ketorolac Level 1
30 mg/mL Special dilution: • 2 mg/mL
No information
IV Push rate: Children: dose over 5 min Infusion rate: No information
Central or peripheral Vital signs
Labetalol HIGH ALERT MEDICATION –continuous infusion Level 3 - IV push Level 4 - infusion
5 mg/mL Special dilution: • 1 mg/mL
Dilute in D5W or NS, usual conc: 1 mg/mL
IV push: Over 2-3 min, no faster than 2 mg/min Infusion Rate: Limited information: 0.25-1.5 mg/kg/hr
Central or peripheral Blood pressure before and 5 and 10 minutes after each injection, or every 5 minutes during infusion, respiratory rate/depth
Lacosamide Level 1
20 mg/mL NS, LR, D5W Infusion: Over 30-60 minutes with or w/o further dilution
Central or peripheral ECG prior to initiating therapy and at steady state maintenance dose: bradycardia, AV block
Laronidase Level 2
2.9 mg/5 mL Dilute in 100 – 250 mL NS • ≤ 20 kg: 100 mL • > 20 kg: 250 mL
Over 3 -4 hours depending on weight ≤ 20 kg: 2 mL/hour and double rate every 15 minutes not exceed 32 mL/hour; > 20 kg: 5 mL/hour and double rate every 15 minutes not to exceed 80 mL/hour A total infusion volume of 100 mL NS and slower infusion rate may be considered for patients with cardiac or respiratory compromise who weigh up to 30 kg
Central or peripheral Requires dedicated line and 0.2 micron filter
Hypersensitivity: monitor vital signs every 15 minutes
Leucovorin Calcium finflix Level 1
10 mg/mL or 20 mg/mL
Dilute in 100-500 mL D5W or NS
IV push: Over 3 min, max rate: 160 mg/min Infusion Rate: Over 1- 6 hrs
Central or peripheral
Levetiracetam Level 1
100 mg/mL Special dilution: • 15 mg/mL
Infusion: Pediatrics <16 years: Dilute in NS to conc of 15mg/mL, infuse over 15 min Neonates: Dilute to conc 5-15mg/mL and infuse over 15 min
Central or peripheral Dizziness, somnolence, vital signs
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
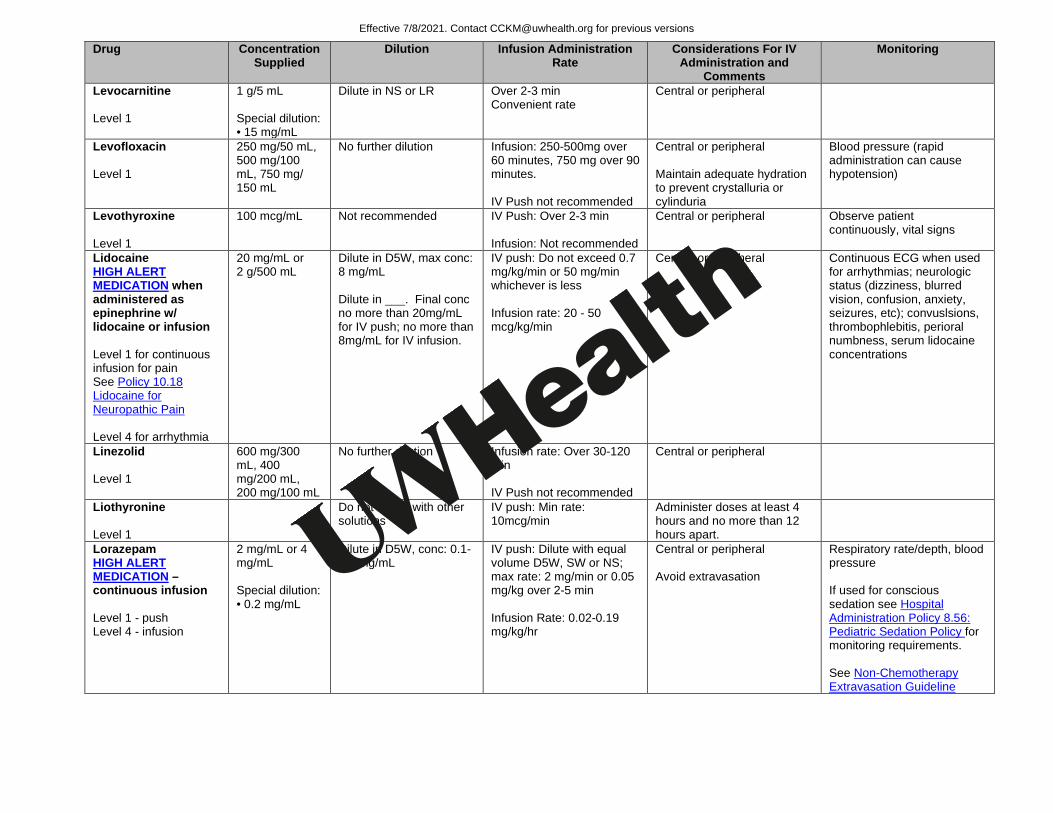
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Levocarnitine Level 1
1 g/5 mL Special dilution: • 15 mg/mL
Dilute in NS or LR
Over 2-3 min Convenient rate
Central or peripheral
Levofloxacin Level 1
250 mg/50 mL, 500 mg/100 mL, 750 mg/ 150 mL
No further dilution Infusion: 250-500mg over 60 minutes, 750 mg over 90 minutes. IV Push not recommended
Central or peripheral Maintain adequate hydration to prevent crystalluria or cylinduria
Blood pressure (rapid administration can cause hypotension)
Levothyroxine Level 1
100 mcg/mL Not recommended
IV Push: Over 2-3 min Infusion: Not recommended
Central or peripheral Observe patient continuously, vital signs
Lidocaine HIGH ALERT MEDICATION when administered as epinephrine w/ lidocaine or infusion Level 1 for continuous infusion for pain See Policy 10.18 Lidocaine for Neuropathic Pain Level 4 for arrhythmia
20 mg/mL or 2 g/500 mL
Dilute in D5W, max conc: 8 mg/mL Dilute in ___. Final conc no more than 20mg/mL for IV push; no more than 8mg/mL for IV infusion.
IV push: Do not exceed 0.7 mg/kg/min or 50 mg/min whichever is less Infusion rate: 20 - 50 mcg/kg/min
Central or peripheral
Continuous ECG when used for arrhythmias; neurologic status (dizziness, blurred vision, confusion, anxiety, seizures, etc); convuslsions, thrombophlebitis, perioral numbness, serum lidocaine concentrations
Linezolid Level 1
600 mg/300 mL, 400 mg/200 mL, 200 mg/100 mL
No further dilution
Infusion rate: Over 30-120 min IV Push not recommended
Central or peripheral
Liothyronine Level 1
Do not admix with other solutions
IV push: Min rate: 10mcg/min
Administer doses at least 4 hours and no more than 12 hours apart.
Lorazepam HIGH ALERT MEDICATION – continuous infusion Level 1 - push Level 4 - infusion
2 mg/mL or 4 mg/mL Special dilution: • 0.2 mg/mL
Dilute in D5W, conc: 0.1-0.2 mg/mL
IV push: Dilute with equal volume D5W, SW or NS; max rate: 2 mg/min or 0.05 mg/kg over 2-5 min Infusion Rate: 0.02-0.19 mg/kg/hr
Central or peripheral Avoid extravasation
Respiratory rate/depth, blood pressure If used for conscious sedation see Hospital Administration Policy 8.56: Pediatric Sedation Policy for monitoring requirements. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
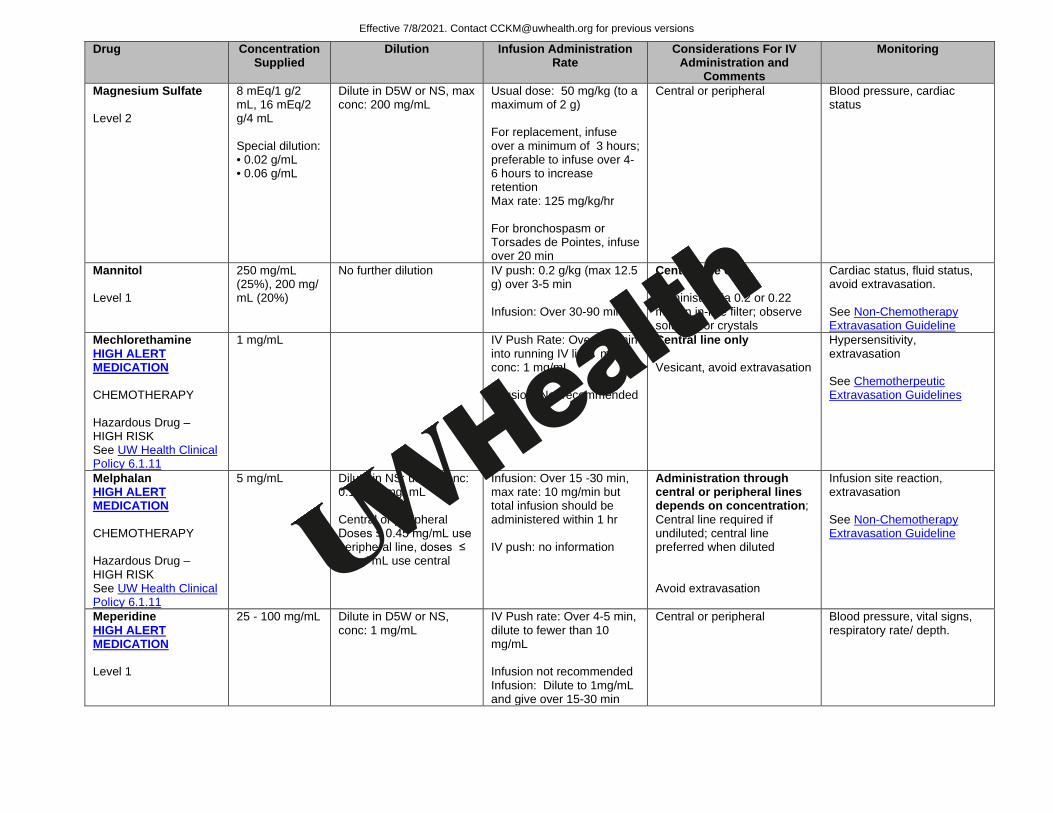
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Magnesium Sulfate Level 2
8 mEq/1 g/2 mL, 16 mEq/2 g/4 mL Special dilution: • 0.02 g/mL • 0.06 g/mL
Dilute in D5W or NS, max conc: 200 mg/mL
Usual dose: 50 mg/kg (to a maximum of 2 g) For replacement, infuse over a minimum of 3 hours; preferable to infuse over 4-6 hours to increase retention Max rate: 125 mg/kg/hr For bronchospasm or Torsades de Pointes, infuse over 20 min
Central or peripheral Blood pressure, cardiac status
Mannitol Level 1
250 mg/mL (25%), 200 mg/ mL (20%)
No further dilution
IV push: 0.2 g/kg (max 12.5 g) over 3-5 min Infusion: Over 30-90 min
Central line only Administer via 0.2 or 0.22 mircon in-line filter; observe solution for crystals
Cardiac status, fluid status, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Mechlorethamine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL IV Push Rate: Over 3-5 min into running IV line; max conc: 1 mg/mL Infusion: Not recommended
Central line only Vesicant, avoid extravasation
Hypersensitivity, extravasation See Chemotherpeutic Extravasation Guidelines
Melphalan HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
5 mg/mL Dilute in NS; usual conc: 0.1-0.45 mg/ mL Central or peripheral Doses ≤ 0.45 mg/mL use peripheral line, doses ≤ 2 mg/ mL use central
Infusion: Over 15 -30 min, max rate: 10 mg/min but total infusion should be administered within 1 hr IV push: no information
Administration through central or peripheral lines depends on concentration; Central line required if undiluted; central line preferred when diluted Avoid extravasation
Infusion site reaction, extravasation See Non-Chemotherapy Extravasation Guideline
Meperidine HIGH ALERT MEDICATION Level 1
25 - 100 mg/mL Dilute in D5W or NS, conc: 1 mg/mL
IV Push rate: Over 4-5 min, dilute to fewer than 10 mg/mL Infusion not recommended Infusion: Dilute to 1mg/mL and give over 15-30 min
Central or peripheral Blood pressure, vital signs, respiratory rate/ depth.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
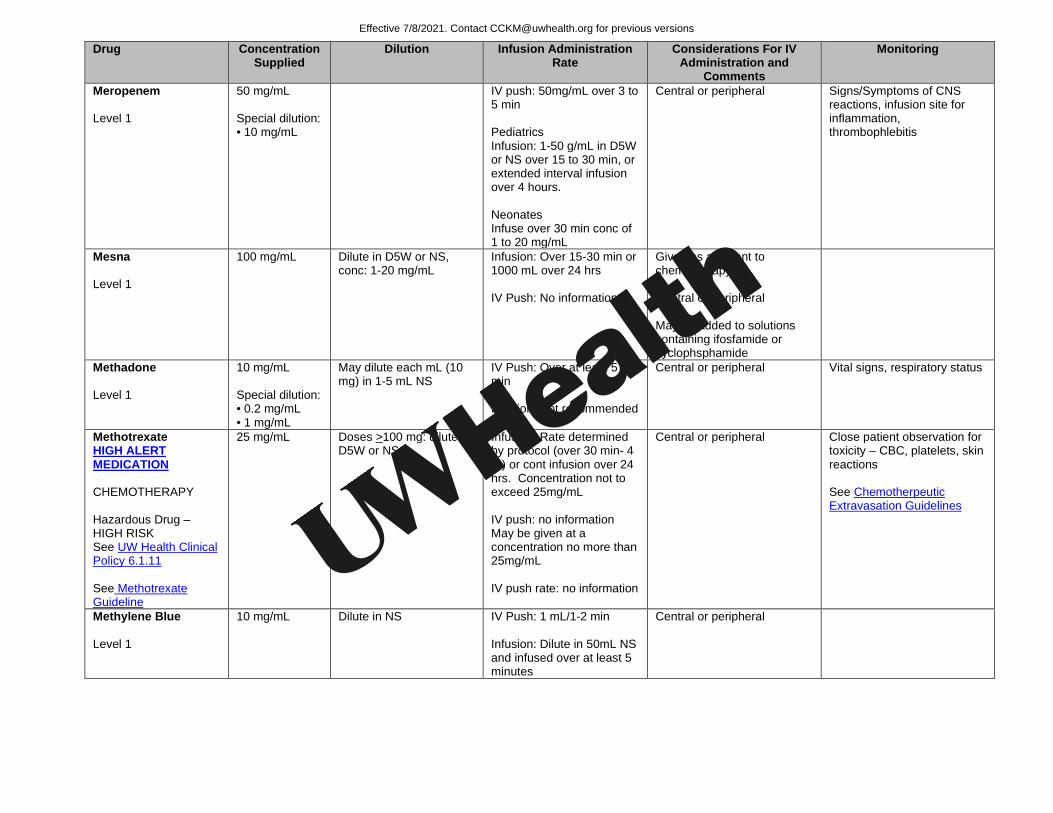
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Meropenem Level 1
50 mg/mL Special dilution: • 10 mg/mL
IV push: 50mg/mL over 3 to 5 min Pediatrics Infusion: 1-50 g/mL in D5W or NS over 15 to 30 min, or extended interval infusion over 4 hours. Neonates Infuse over 30 min conc of 1 to 20 mg/mL
Central or peripheral Signs/Symptoms of CNS reactions, infusion site for inflammation, thrombophlebitis
Mesna Level 1
100 mg/mL Dilute in D5W or NS, conc: 1-20 mg/mL
Infusion: Over 15-30 min or 1000 mL over 24 hrs IV Push: No information
Given as adjuvant to chemotherapy. Central or peripheral May be added to solutions containing ifosfamide or cyclophsphamide
Methadone Level 1
10 mg/mL Special dilution: • 0.2 mg/mL • 1 mg/mL
May dilute each mL (10 mg) in 1-5 mL NS
IV Push: Over at least 5 min Infusion: Not recommended
Central or peripheral Vital signs, respiratory status
Methotrexate HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11 See Methotrexate Guideline
25 mg/mL Doses >100 mg: dilute in D5W or NS
Infusion: Rate determined by protocol (over 30 min- 4 hr) or cont infusion over 24 hrs. Concentration not to exceed 25mg/mL IV push: no information May be given at a concentration no more than 25mg/mL IV push rate: no information
Central or peripheral Close patient observation for toxicity – CBC, platelets, skin reactions See Chemotherpeutic Extravasation Guidelines
Methylene Blue Level 1
10 mg/mL Dilute in NS
IV Push: 1 mL/1-2 min Infusion: Dilute in 50mL NS and infused over at least 5 minutes
Central or peripheral
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
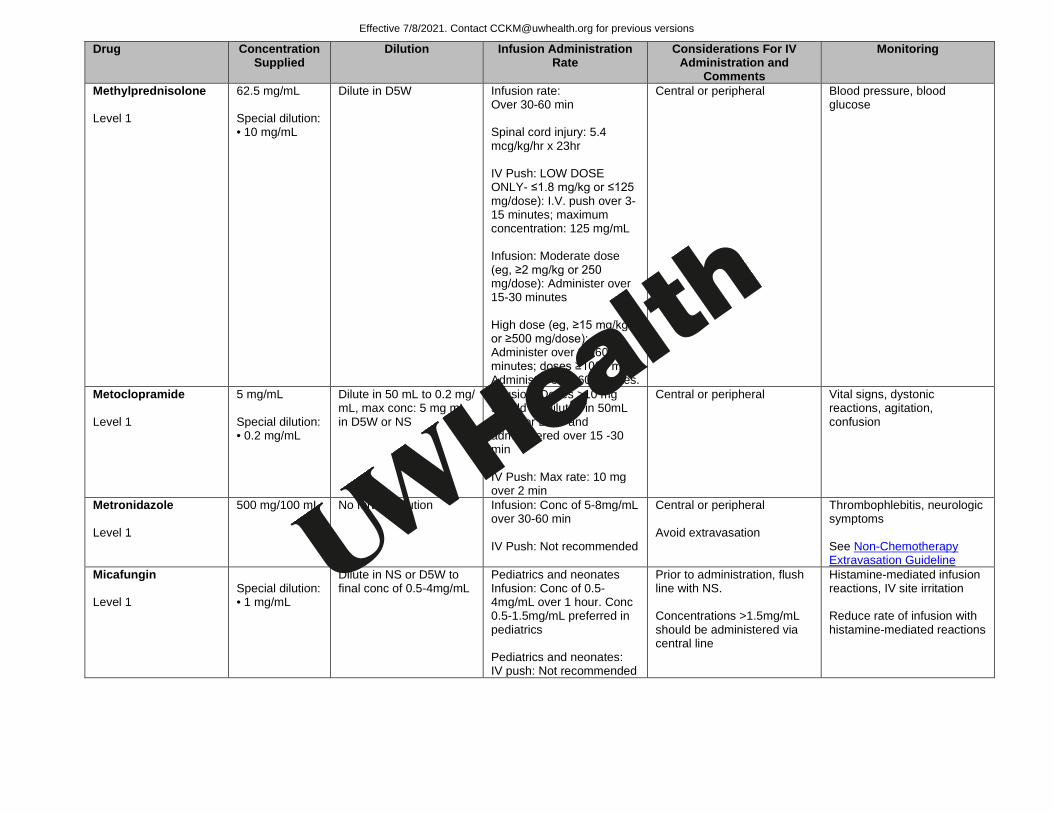
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Methylprednisolone Level 1
62.5 mg/mL Special dilution: • 10 mg/mL
Dilute in D5W
Infusion rate: Over 30-60 min Spinal cord injury: 5.4 mcg/kg/hr x 23hr IV Push: LOW DOSE ONLY- ≤1.8 mg/kg or ≤125 mg/dose): I.V. push over 3-15 minutes; maximum concentration: 125 mg/mL Infusion: Moderate dose (eg, ≥2 mg/kg or 250 mg/dose): Administer over 15-30 minutes High dose (eg, ≥15 mg/kg or ≥500 mg/dose): Administer over 30-60 minutes; doses ≥1000 mg: Administer over 60 minutes.
Central or peripheral Blood pressure, blood glucose
Metoclopramide Level 1
5 mg/mL Special dilution: • 0.2 mg/mL
Dilute in 50 mL to 0.2 mg/ mL, max conc: 5 mg mL in D5W or NS
Infusion: Doses >10 mg should be diluted in 50mL of NS or D5W and administered over 15 -30 min IV Push: Max rate: 10 mg over 2 min
Central or peripheral Vital signs, dystonic reactions, agitation, confusion
Metronidazole Level 1
500 mg/100 mL No further dilution
Infusion: Conc of 5-8mg/mL over 30-60 min IV Push: Not recommended
Central or peripheral Avoid extravasation
Thrombophlebitis, neurologic symptoms See Non-Chemotherapy Extravasation Guideline
Micafungin Level 1
Special dilution: • 1 mg/mL
Dilute in NS or D5W to final conc of 0.5-4mg/mL
Pediatrics and neonates Infusion: Conc of 0.5-4mg/mL over 1 hour. Conc 0.5-1.5mg/mL preferred in pediatrics Pediatrics and neonates: IV push: Not recommended
Prior to administration, flush line with NS. Concentrations >1.5mg/mL should be administered via central line
Histamine-mediated infusion reactions, IV site irritation Reduce rate of infusion with histamine-mediated reactions
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
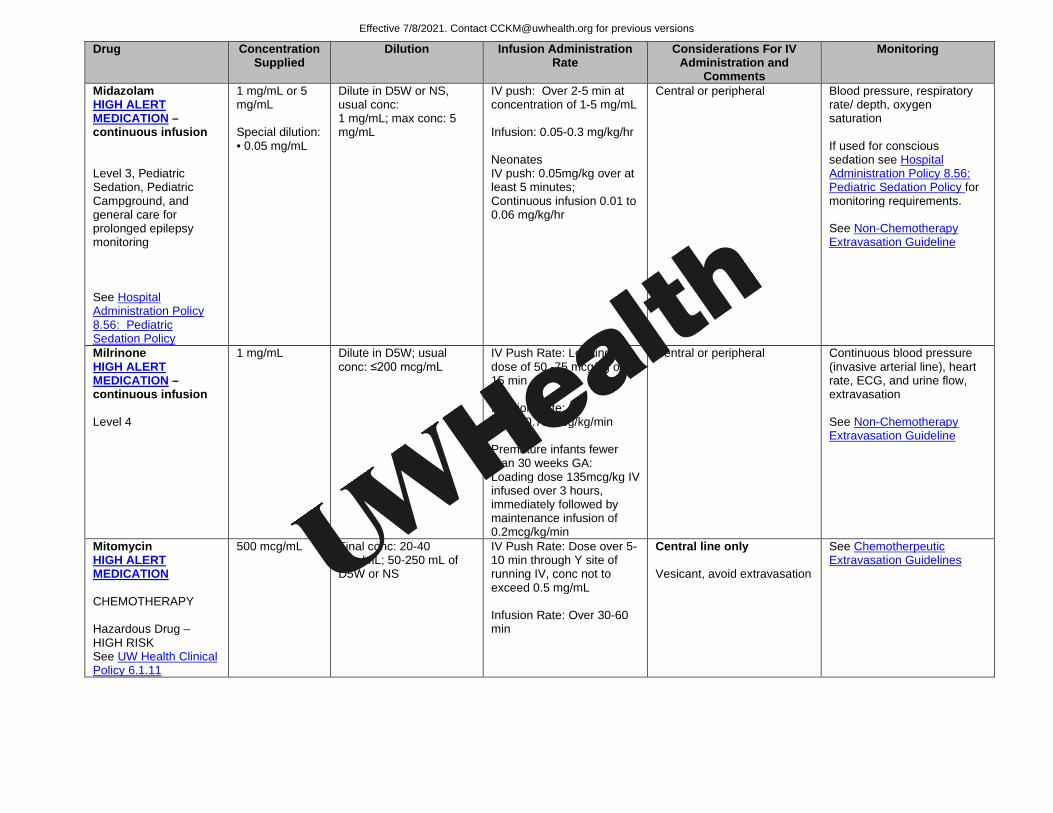
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Midazolam HIGH ALERT MEDICATION –continuous infusion Level 3, Pediatric Sedation, Pediatric Campground, and general care for prolonged epilepsy monitoring See Hospital Administration Policy 8.56: Pediatric Sedation Policy
1 mg/mL or 5 mg/mL Special dilution: • 0.05 mg/mL
Dilute in D5W or NS, usual conc: 1 mg/mL; max conc: 5 mg/mL
IV push: Over 2-5 min at concentration of 1-5 mg/mL Infusion: 0.05-0.3 mg/kg/hr Neonates IV push: 0.05mg/kg over at least 5 minutes; Continuous infusion 0.01 to 0.06 mg/kg/hr
Central or peripheral Blood pressure, respiratory rate/ depth, oxygen saturation If used for conscious sedation see Hospital Administration Policy 8.56: Pediatric Sedation Policy for monitoring requirements. See Non-Chemotherapy Extravasation Guideline
Milrinone HIGH ALERT MEDICATION –continuous infusion Level 4
1 mg/mL Dilute in D5W; usual conc: ≤200 mcg/mL
IV Push Rate: Loading dose of 50 -75 mcg/kg over 15 min Infusion Rate: 0.25 - 0.75 mcg/kg/min Premature infants fewer than 30 weeks GA: Loading dose 135mcg/kg IV infused over 3 hours, immediately followed by maintenance infusion of 0.2mcg/kg/min
Central or peripheral Continuous blood pressure (invasive arterial line), heart rate, ECG, and urine flow, extravasation See Non-Chemotherapy Extravasation Guideline
Mitomycin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
500 mcg/mL Final conc: 20-40 mcg/mL; 50-250 mL of D5W or NS
IV Push Rate: Dose over 5-10 min through Y site of running IV, conc not to exceed 0.5 mg/mL Infusion Rate: Over 30-60 min
Central line only Vesicant, avoid extravasation
See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
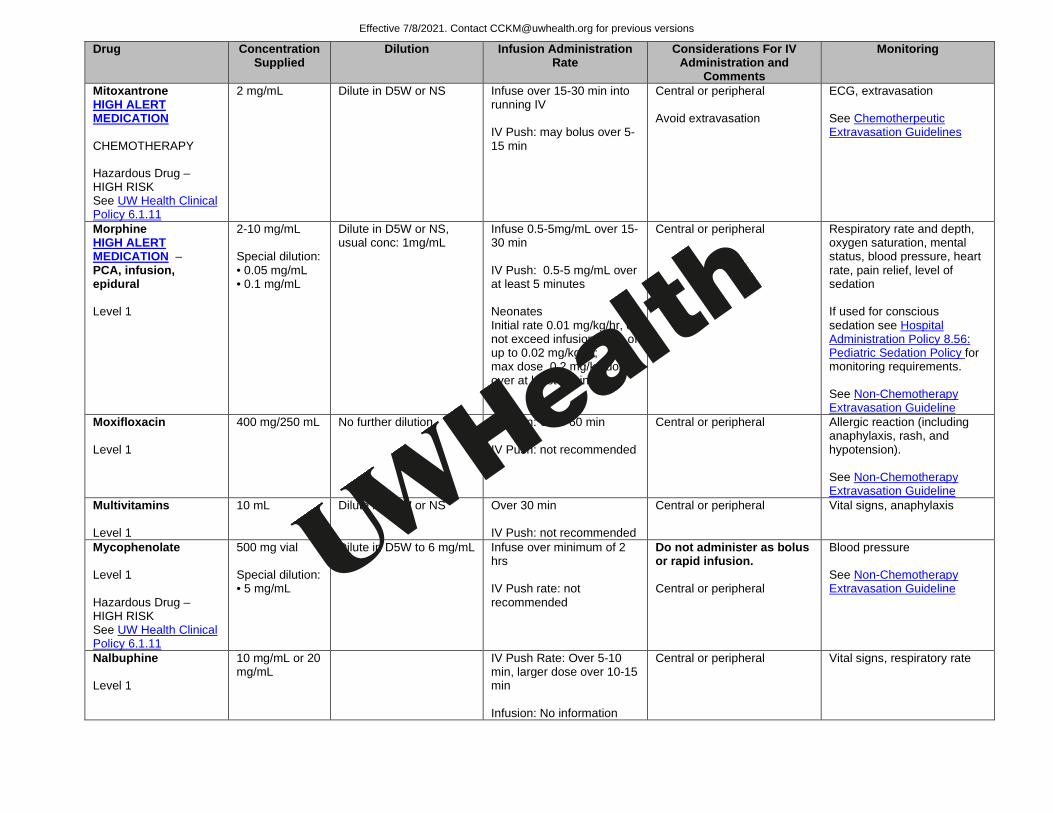
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Mitoxantrone HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
2 mg/mL Dilute in D5W or NS
Infuse over 15-30 min into running IV IV Push: may bolus over 5-15 min
Central or peripheral Avoid extravasation
ECG, extravasation See Chemotherpeutic Extravasation Guidelines
Morphine HIGH ALERT MEDICATION – PCA, infusion, epidural Level 1
2-10 mg/mL Special dilution: • 0.05 mg/mL • 0.1 mg/mL
Dilute in D5W or NS, usual conc: 1mg/mL
Infuse 0.5-5mg/mL over 15-30 min IV Push: 0.5-5 mg/mL over at least 5 minutes Neonates Initial rate 0.01 mg/kg/hr, do not exceed infusion rates of up to 0.02 mg/kg/hr; max dose 0.2 mg/kg/dose over at least 5 minutes
Central or peripheral Respiratory rate and depth, oxygen saturation, mental status, blood pressure, heart rate, pain relief, level of sedation If used for conscious sedation see Hospital Administration Policy 8.56: Pediatric Sedation Policy for monitoring requirements. See Non-Chemotherapy Extravasation Guideline
Moxifloxacin Level 1
400 mg/250 mL No further dilution
Infusion: Over 60 min IV Push: not recommended
Central or peripheral Allergic reaction (including anaphylaxis, rash, and hypotension). See Non-Chemotherapy Extravasation Guideline
Multivitamins Level 1
10 mL Dilute in D5W or NS
Over 30 min IV Push: not recommended
Central or peripheral Vital signs, anaphylaxis
Mycophenolate Level 1 Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
500 mg vial Special dilution: • 5 mg/mL
Dilute in D5W to 6 mg/mL
Infuse over minimum of 2 hrs IV Push rate: not recommended
Do not administer as bolus or rapid infusion. Central or peripheral
Blood pressure See Non-Chemotherapy Extravasation Guideline
Nalbuphine Level 1
10 mg/mL or 20 mg/mL
IV Push Rate: Over 5-10 min, larger dose over 10-15 min Infusion: No information
Central or peripheral Vital signs, respiratory rate
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
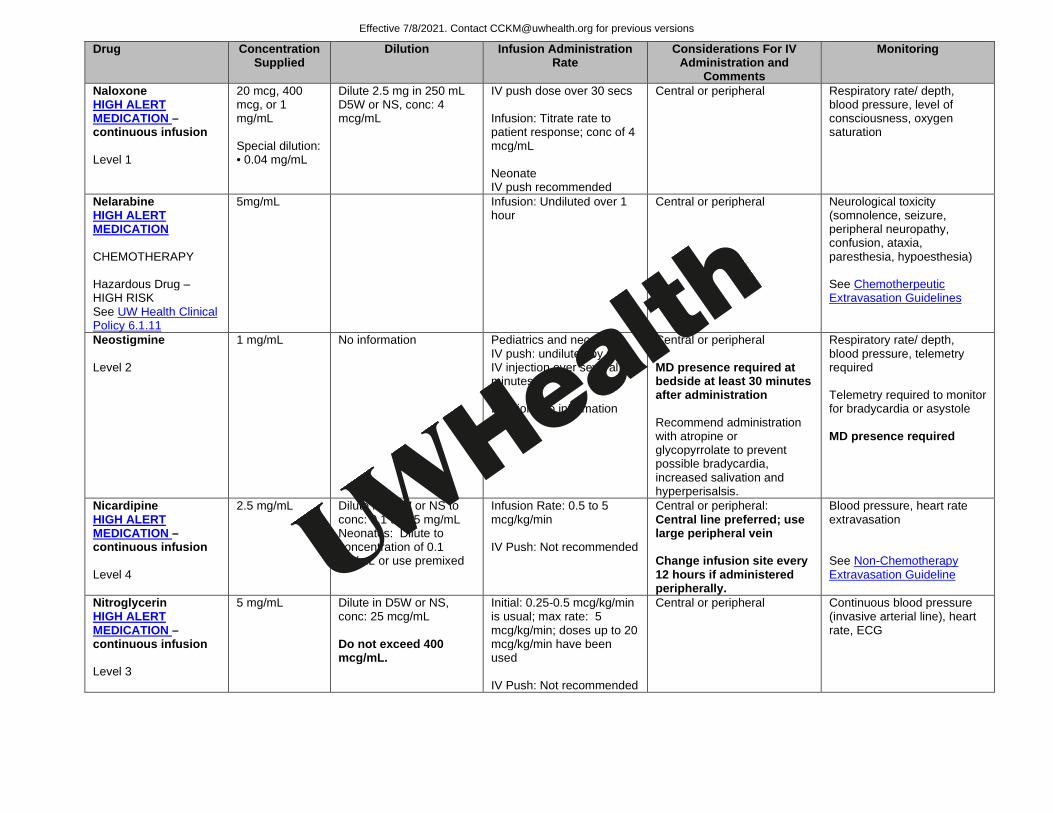
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Naloxone HIGH ALERT MEDICATION –continuous infusion Level 1
20 mcg, 400 mcg, or 1 mg/mL Special dilution: • 0.04 mg/mL
Dilute 2.5 mg in 250 mL D5W or NS, conc: 4 mcg/mL
IV push dose over 30 secs Infusion: Titrate rate to patient response; conc of 4 mcg/mL Neonate IV push recommended
Central or peripheral Respiratory rate/ depth, blood pressure, level of consciousness, oxygen saturation
Nelarabine HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
5mg/mL Infusion: Undiluted over 1 hour
Central or peripheral Neurological toxicity (somnolence, seizure, peripheral neuropathy, confusion, ataxia, paresthesia, hypoesthesia) See Chemotherpeutic Extravasation Guidelines
Neostigmine Level 2
1 mg/mL No information Pediatrics and neonates IV push: undiluted by slow IV injection over several minutes Infusion: No information
Central or peripheral MD presence required at bedside at least 30 minutes after administration Recommend administration with atropine or glycopyrrolate to prevent possible bradycardia, increased salivation and hyperperisalsis.
Respiratory rate/ depth, blood pressure, telemetry required Telemetry required to monitor for bradycardia or asystole MD presence required
Nicardipine HIGH ALERT MEDICATION –continuous infusion Level 4
2.5 mg/mL Dilute in D5W or NS to conc: 0.1 to 0.5 mg/mL Neonates: Dilute to concentration of 0.1 mg/mL or use premixed
Infusion Rate: 0.5 to 5 mcg/kg/min IV Push: Not recommended
Central or peripheral: Central line preferred; use large peripheral vein Change infusion site every 12 hours if administered peripherally.
Blood pressure, heart rate extravasation See Non-Chemotherapy Extravasation Guideline
Nitroglycerin HIGH ALERT MEDICATION –continuous infusion Level 3
5 mg/mL Dilute in D5W or NS, conc: 25 mcg/mL Do not exceed 400 mcg/mL.
Initial: 0.25-0.5 mcg/kg/min is usual; max rate: 5 mcg/kg/min; doses up to 20 mcg/kg/min have been used IV Push: Not recommended
Central or peripheral Continuous blood pressure (invasive arterial line), heart rate, ECG
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
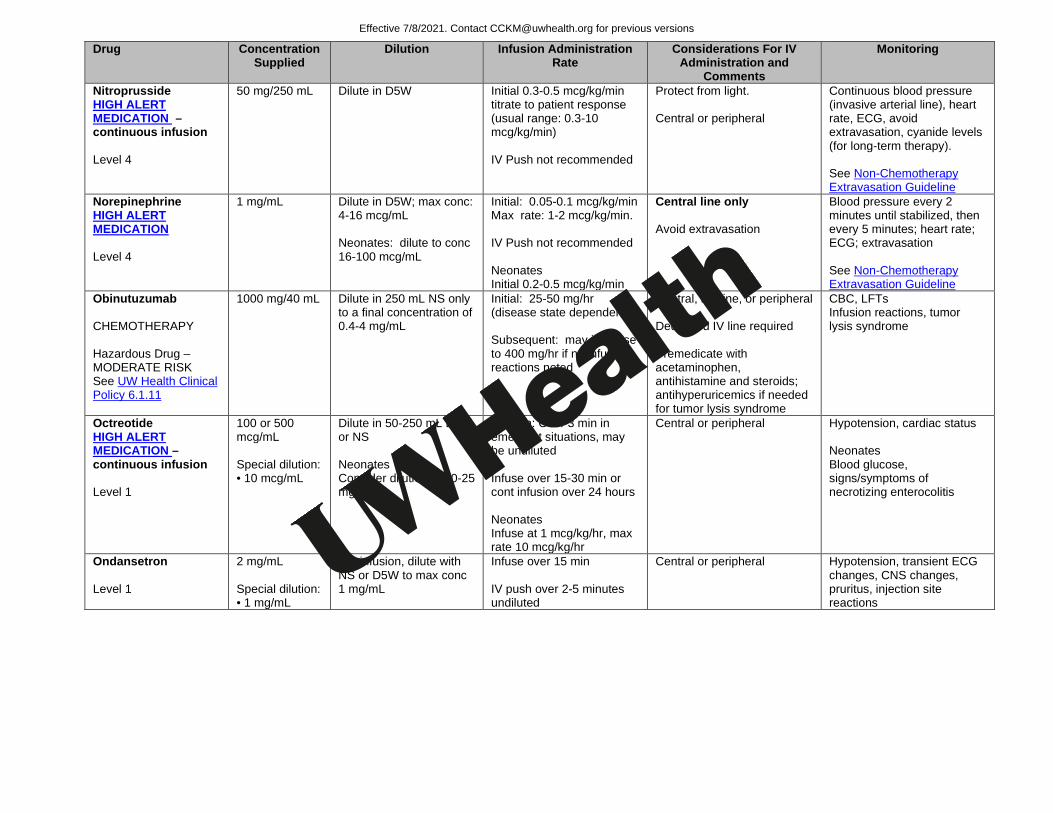
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Nitroprusside HIGH ALERT MEDICATION –continuous infusion Level 4
50 mg/250 mL Dilute in D5W
Initial 0.3-0.5 mcg/kg/min titrate to patient response (usual range: 0.3-10 mcg/kg/min) IV Push not recommended
Protect from light. Central or peripheral
Continuous blood pressure (invasive arterial line), heart rate, ECG, avoid extravasation, cyanide levels (for long-term therapy). See Non-Chemotherapy Extravasation Guideline
Norepinephrine HIGH ALERT MEDICATION Level 4
1 mg/mL Dilute in D5W; max conc: 4-16 mcg/mL Neonates: dilute to conc 16-100 mcg/mL
Initial: 0.05-0.1 mcg/kg/min Max rate: 1-2 mcg/kg/min. IV Push not recommended Neonates Initial 0.2-0.5 mcg/kg/min
Central line only Avoid extravasation
Blood pressure every 2 minutes until stabilized, then every 5 minutes; heart rate; ECG; extravasation See Non-Chemotherapy Extravasation Guideline
Obinutuzumab CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
1000 mg/40 mL Dilute in 250 mL NS only to a final concentration of 0.4-4 mg/mL
Initial: 25-50 mg/hr (disease state dependent) Subsequent: may increase to 400 mg/hr if no infusion reactions noted
Central, midline, or peripheral Dedicated IV line required Premedicate with acetaminophen, antihistamine and steroids; antihyperuricemics if needed for tumor lysis syndrome
CBC, LFTs Infusion reactions, tumor lysis syndrome
Octreotide HIGH ALERT MEDICATION –continuous infusion Level 1
100 or 500 mcg/mL Special dilution: • 10 mcg/mL
Dilute in 50-250 mL D5W or NS Neonates Consider dilution of 10-25 mg/mL
IV push: Over 3 min in emergent situations, may be undiluted Infuse over 15-30 min or cont infusion over 24 hours Neonates Infuse at 1 mcg/kg/hr, max rate 10 mcg/kg/hr
Central or peripheral
Hypotension, cardiac status Neonates Blood glucose, signs/symptoms of necrotizing enterocolitis
Ondansetron Level 1
2 mg/mL Special dilution: • 1 mg/mL
For infusion, dilute with NS or D5W to max conc 1 mg/mL
Infuse over 15 min IV push over 2-5 minutes undiluted
Central or peripheral
Hypotension, transient ECG changes, CNS changes, pruritus, injection site reactions
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
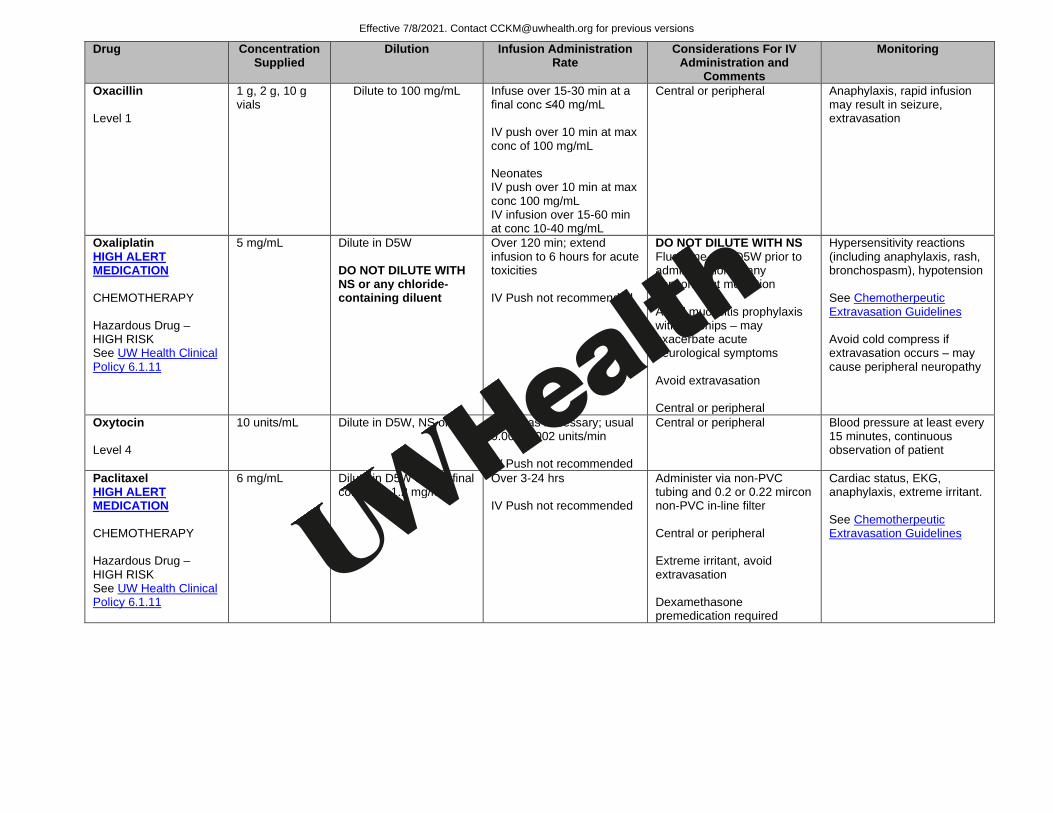
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Oxacillin Level 1
1 g, 2 g, 10 g vials
Dilute to 100 mg/mL Infuse over 15-30 min at a final conc ≤40 mg/mL IV push over 10 min at max conc of 100 mg/mL Neonates IV push over 10 min at max conc 100 mg/mL IV infusion over 15-60 min at conc 10-40 mg/mL
Central or peripheral Anaphylaxis, rapid infusion may result in seizure, extravasation
Oxaliplatin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
5 mg/mL Dilute in D5W DO NOT DILUTE WITH NS or any chloride-containing diluent
Over 120 min; extend infusion to 6 hours for acute toxicities IV Push not recommended
DO NOT DILUTE WITH NS Flush line with D5W prior to administration of any concomitant mediation Avoid mucositis prophylaxis with ice chips – may exacerbate acute neurological symptoms Avoid extravasation Central or peripheral
Hypersensitivity reactions (including anaphylaxis, rash, bronchospasm), hypotension See Chemotherpeutic Extravasation Guidelines Avoid cold compress if extravasation occurs – may cause peripheral neuropathy
Oxytocin Level 4
10 units/mL Dilute in D5W, NS or LR
Adjust as necessary; usual 0.001-0.002 units/min IV Push not recommended
Central or peripheral
Blood pressure at least every 15 minutes, continuous observation of patient
Paclitaxel HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
6 mg/mL Dilute in D5W or NS, final conc: 0.3-1.2 mg/mL
Over 3-24 hrs IV Push not recommended
Administer via non-PVC tubing and 0.2 or 0.22 mircon non-PVC in-line filter Central or peripheral Extreme irritant, avoid extravasation Dexamethasone premedication required
Cardiac status, EKG, anaphylaxis, extreme irritant. See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
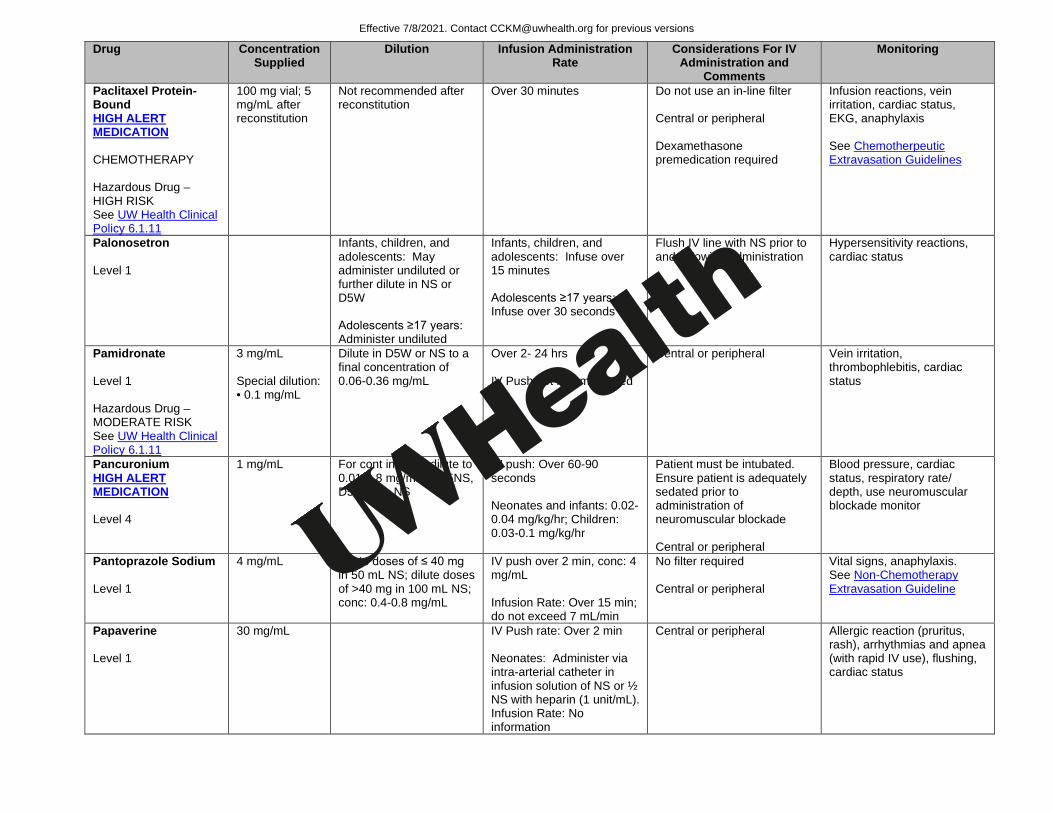
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Paclitaxel Protein-Bound HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
100 mg vial; 5 mg/mL after reconstitution
Not recommended after reconstitution
Over 30 minutes Do not use an in-line filter Central or peripheral Dexamethasone premedication required
Infusion reactions, vein irritation, cardiac status, EKG, anaphylaxis See Chemotherpeutic Extravasation Guidelines
Palonosetron Level 1
Infants, children, and adolescents: May administer undiluted or further dilute in NS or D5W Adolescents ≥17 years: Administer undiluted
Infants, children, and adolescents: Infuse over 15 minutes Adolescents ≥17 years: Infuse over 30 seconds
Flush IV line with NS prior to and following administration
Hypersensitivity reactions, cardiac status
Pamidronate Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
3 mg/mL Special dilution: • 0.1 mg/mL
Dilute in D5W or NS to a final concentration of 0.06-0.36 mg/mL
Over 2- 24 hrs IV Push not recommended
Central or peripheral Vein irritation, thrombophlebitis, cardiac status
Pancuronium HIGH ALERT MEDICATION Level 4
1 mg/mL For cont infusion dilute to 0.01-0.8 mg/mL in D5NS, D5W, LR, NS
IV push: Over 60-90 seconds Neonates and infants: 0.02-0.04 mg/kg/hr; Children: 0.03-0.1 mg/kg/hr
Patient must be intubated. Ensure patient is adequately sedated prior to administration of neuromuscular blockade Central or peripheral
Blood pressure, cardiac status, respiratory rate/ depth, use neuromuscular blockade monitor
Pantoprazole Sodium Level 1
4 mg/mL Dilute doses of ≤ 40 mg in 50 mL NS; dilute doses of >40 mg in 100 mL NS; conc: 0.4-0.8 mg/mL
IV push over 2 min, conc: 4 mg/mL Infusion Rate: Over 15 min; do not exceed 7 mL/min
No filter required Central or peripheral
Vital signs, anaphylaxis. See Non-Chemotherapy Extravasation Guideline
Papaverine Level 1
30 mg/mL IV Push rate: Over 2 min Neonates: Administer via intra-arterial catheter in infusion solution of NS or ½ NS with heparin (1 unit/mL). Infusion Rate: No information
Central or peripheral Allergic reaction (pruritus, rash), arrhythmias and apnea (with rapid IV use), flushing, cardiac status
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
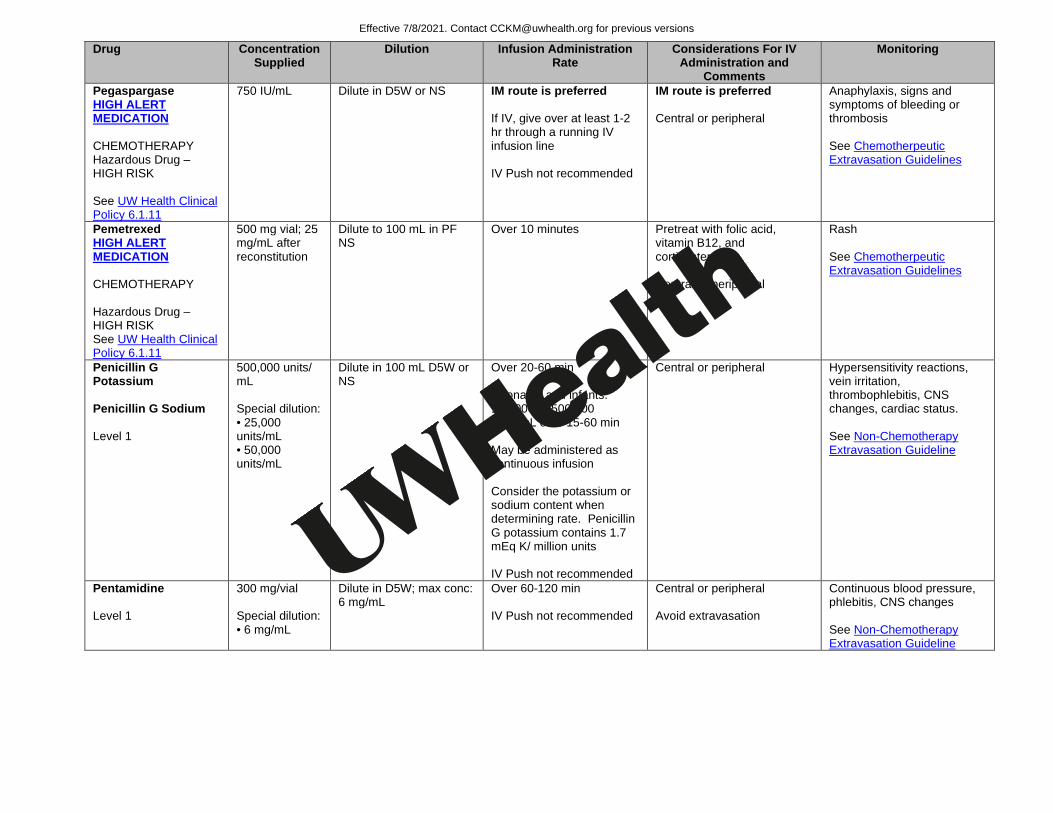
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Pegaspargase HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
750 IU/mL Dilute in D5W or NS
IM route is preferred If IV, give over at least 1-2 hr through a running IV infusion line IV Push not recommended
IM route is preferred Central or peripheral
Anaphylaxis, signs and symptoms of bleeding or thrombosis See Chemotherpeutic Extravasation Guidelines
Pemetrexed HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
500 mg vial; 25 mg/mL after reconstitution
Dilute to 100 mL in PF NS
Over 10 minutes Pretreat with folic acid, vitamin B12, and corticosteroid Central or peripheral
Rash See Chemotherpeutic Extravasation Guidelines
Penicillin G Potassium Penicillin G Sodium Level 1
500,000 units/ mL Special dilution: • 25,000 units/mL • 50,000 units/mL
Dilute in 100 mL D5W or NS
Over 20-60 min Neonates and infants: 100,000 to 500,000 units/mL over 15-60 min May be administered as continuous infusion Consider the potassium or sodium content when determining rate. Penicillin G potassium contains 1.7 mEq K/ million units IV Push not recommended
Central or peripheral Hypersensitivity reactions, vein irritation, thrombophlebitis, CNS changes, cardiac status. See Non-Chemotherapy Extravasation Guideline
Pentamidine Level 1
300 mg/vial Special dilution: • 6 mg/mL
Dilute in D5W; max conc: 6 mg/mL
Over 60-120 min IV Push not recommended
Central or peripheral Avoid extravasation
Continuous blood pressure, phlebitis, CNS changes See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Pentobarbital Level 3
50 mg/mL Max conc: 50 mg/mL for slow IV push; may dilute with D5W, D10W, NS, 1/2NS, LR, D5LR and D/NS combinations
IV push: 50 mg/min max Over 10-30 min
Central or peripheral Avoid extravasation
Blood pressure, pulse, and respirations every 3-5 minutes. If used for conscious sedation see Hospital Administration Policy 8.56: Pediatric Sedation Policy for monitoring requirements. See Non-Chemotherapy Extravasation Guideline
Pentostatin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
2 mg/mL May further dilute in 25-50 mL NS or D5W
Over 20-30 min or IV bolus over 5 min
Hydrate with fluid prior to and after infusion
Cardiac status, CNS changes, phlebitis, allergic reaction See Chemotherpeutic Extravasation Guidelines
Peramivir Level 1
200 mg /20 mL Dilute in NS, D5W, or LR to conc ≤ 6 mg/mL Max total volume 100 mL
Administer over 15-30 mins Central or peripheral Hypersensitivity reactions, dermatologic reactions, neuropsychiatric events and unusual behavior
Phenobarbital Loading - Level 2 Maintenance - Level 1
130 mg/mL Special dilution: • 2 mg/mL • 10 mg/mL
IV Push Rate: No more than 1 mg/kg/min; max rate: 30 mg/min Neonates: Over 10-15 minutes, 2 mg/kg/min; max rate: 30 mg/min Infusion not recommended
Central or peripheral Irritant, avoid extravasation
Vital signs every hour, respiratory rate/ depth, paradoxical stimulatory response, irritant. See Non-Chemotherapy Extravasation Guideline
Phentolamine Level 4
5 mg/mL Dilute in 100 mL NS
No information Central or peripheral Vital signs every 2 minutes initially, cardiac status
Phenylephrine HIGH ALERT MEDICATION Level 4
10 mg/mL Dilute in 250 mL D5W or NS; usual cont infusion conc: 20-60 mcg/mL
IV push: dilute 1 mL in 9 mL SW, conc: 1 mg/mL over 20-30 seconds Infusion: Children: 0.1-0.5 mcg/kg/min, titrated to effect
Central or peripheral; Central line preferred. Infuse into large veins. Vasoconstrictor - avoid extravasation
continuous blood pressure (invasive arterial line), heart rate, ECG, urine flow, and hypersensitivity reaction Potent vasoconstrictor, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
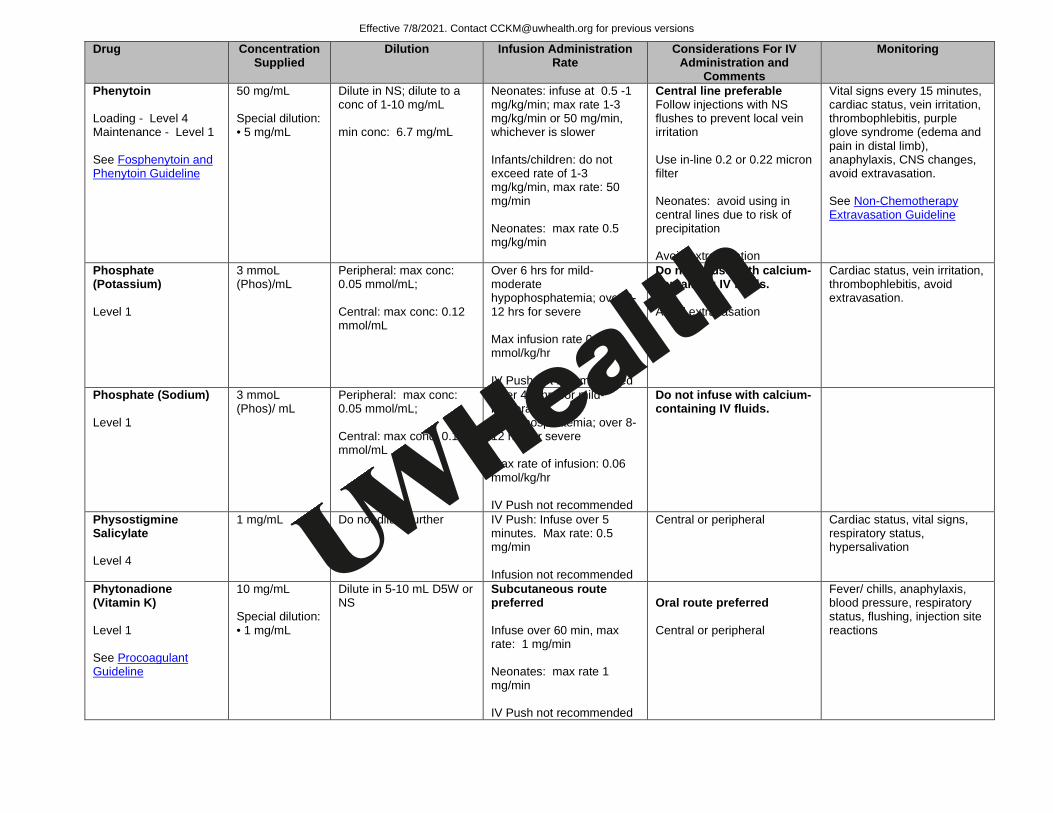
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Phenytoin Loading - Level 4 Maintenance - Level 1 See Fosphenytoin and Phenytoin Guideline
50 mg/mL Special dilution: • 5 mg/mL
Dilute in NS; dilute to a conc of 1-10 mg/mL min conc: 6.7 mg/mL
Neonates: infuse at 0.5 -1 mg/kg/min; max rate 1-3 mg/kg/min or 50 mg/min, whichever is slower Infants/children: do not exceed rate of 1-3 mg/kg/min, max rate: 50 mg/min Neonates: max rate 0.5 mg/kg/min
Central line preferable Follow injections with NS flushes to prevent local vein irritation Use in-line 0.2 or 0.22 micron filter Neonates: avoid using in central lines due to risk of precipitation Avoid extravasation
Vital signs every 15 minutes, cardiac status, vein irritation, thrombophlebitis, purple glove syndrome (edema and pain in distal limb), anaphylaxis, CNS changes, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Phosphate (Potassium) Level 1
3 mmoL (Phos)/mL
Peripheral: max conc: 0.05 mmol/mL; Central: max conc: 0.12 mmol/mL
Over 6 hrs for mild-moderate hypophosphatemia; over 8-12 hrs for severe Max infusion rate 0.06 mmol/kg/hr IV Push not recommended
Do not infuse with calcium-containing IV fluids. Avoid extravasation
Cardiac status, vein irritation, thrombophlebitis, avoid extravasation.
Phosphate (Sodium) Level 1
3 mmoL (Phos)/ mL
Peripheral: max conc: 0.05 mmol/mL; Central: max conc: 0.12 mmol/mL
Over 4-6 hrs for mild-moderate hypophosphatemia; over 8-12 hrs for severe Max rate of infusion: 0.06 mmol/kg/hr IV Push not recommended
Do not infuse with calcium-containing IV fluids.
Physostigmine Salicylate Level 4
1 mg/mL Do not dilute further IV Push: Infuse over 5 minutes. Max rate: 0.5 mg/min Infusion not recommended
Central or peripheral Cardiac status, vital signs, respiratory status, hypersalivation
Phytonadione (Vitamin K) Level 1 See Procoagulant Guideline
10 mg/mL Special dilution: • 1 mg/mL
Dilute in 5-10 mL D5W or NS
Subcutaneous route preferred Infuse over 60 min, max rate: 1 mg/min Neonates: max rate 1 mg/min IV Push not recommended
Oral route preferred Central or peripheral
Fever/ chills, anaphylaxis, blood pressure, respiratory status, flushing, injection site reactions
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
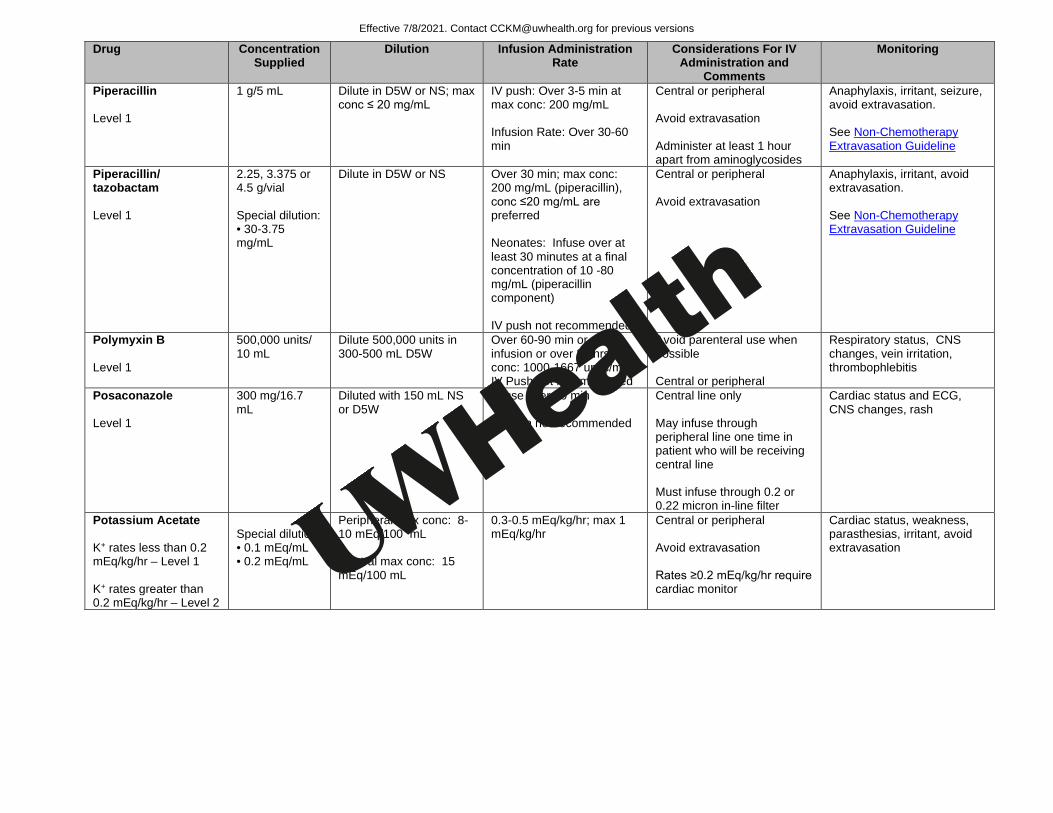
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Piperacillin Level 1
1 g/5 mL Dilute in D5W or NS; max conc ≤ 20 mg/mL
IV push: Over 3-5 min at max conc: 200 mg/mL Infusion Rate: Over 30-60 min
Central or peripheral Avoid extravasation Administer at least 1 hour apart from aminoglycosides
Anaphylaxis, irritant, seizure, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Piperacillin/ tazobactam Level 1
2.25, 3.375 or 4.5 g/vial Special dilution: • 30-3.75 mg/mL
Dilute in D5W or NS
Over 30 min; max conc: 200 mg/mL (piperacillin), conc ≤20 mg/mL are preferred Neonates: Infuse over at least 30 minutes at a final concentration of 10 -80 mg/mL (piperacillin component) IV push not recommended
Central or peripheral Avoid extravasation
Anaphylaxis, irritant, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Polymyxin B Level 1
500,000 units/ 10 mL
Dilute 500,000 units in 300-500 mL D5W
Over 60-90 min or cont infusion or over 24 hrs at a conc: 1000-1667 units/mL IV Push not recommended
Avoid parenteral use when possible Central or peripheral
Respiratory status, CNS changes, vein irritation, thrombophlebitis
Posaconazole Level 1
300 mg/16.7 mL
Diluted with 150 mL NS or D5W
Infuse over 90 min IV push not recommended
Central line only May infuse through peripheral line one time in patient who will be receiving central line Must infuse through 0.2 or 0.22 micron in-line filter
Cardiac status and ECG, CNS changes, rash
Potassium Acetate K+ rates less than 0.2 mEq/kg/hr – Level 1 K+ rates greater than 0.2 mEq/kg/hr – Level 2
Special dilution: • 0.1 mEq/mL • 0.2 mEq/mL
Peripheral max conc: 8-10 mEq/100 mL Central max conc: 15 mEq/100 mL
0.3-0.5 mEq/kg/hr; max 1 mEq/kg/hr
Central or peripheral Avoid extravasation Rates ≥0.2 mEq/kg/hr require cardiac monitor
Cardiac status, weakness, parasthesias, irritant, avoid extravasation
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Potassium Chloride K+ rates less than 0.2 mEq/kg/hr – Level 1 K+ rates greater than 0.2 mEq/kg/hr – Level 2
2 mEq/mL Special dilution: • 0.1 mEq/mL
Peripheral: 8 mEq/100 mL Central: 15 mEq/100 mL Neonates Peripheral: 4 mEq/100 mL Central: 8 mEq/100 mL
Infusion: 0.3-0.5 mEq/kg/hr, max 1 mEq/kg/hr up to 40 mEq/hr Neonates: 0.5-1 mEq/kg over 1 hour IV Push not recommended
Central or peripheral Rates ≥0.2 mEq/kg/hr require cardiac monitor Neonates: Continuous EKG monitoring recommended, especially with central IV administration
Cardiac status, vein irritation, thrombophlebitis, vesicant, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Potassium Phosphate K+ rates less than 0.2 mEq/kg/hr – Level 1 K+ rates greater than 0.2 mEq/kg/hr – Level 2
7.5 or 15 mmol/100 mL bag Special dilution: • 0.12 mmol/mL
Peripheral: 0.05 mmol/mL Central: 0.12 mmol/mL
Max 0.06 mmol/kg/hr Central or peripheral Do not infuse with calcium-containing IV fluids Recommend using 0.2 or 0.22 micron in-line filter
Cardiac status, weakness, parasthesias
Pralatrexate HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
20 mg/mL 40 mg/2 mL
Do not dilute Over 3-5 minutes into free-flowing line of NS
Central or peripheral Patients must be receiving folic acid and cyanocobalamin while receiving pralatrexate
Dyspnea, mucositis, tumor lysis syndrome, tachycardia See Chemotherpeutic Extravasation Guidelines
Pralidoxime Level 4
50 mg/mL Dilute in NS to 10-20 mg/mL, max conc 50 mg/mL
Infusion: Over 15-30 min IV Push Rate: Max: 200 mg/ min
Central or peripheral Continuous vital signs and blood pressure, muscle fasiculations and strength
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
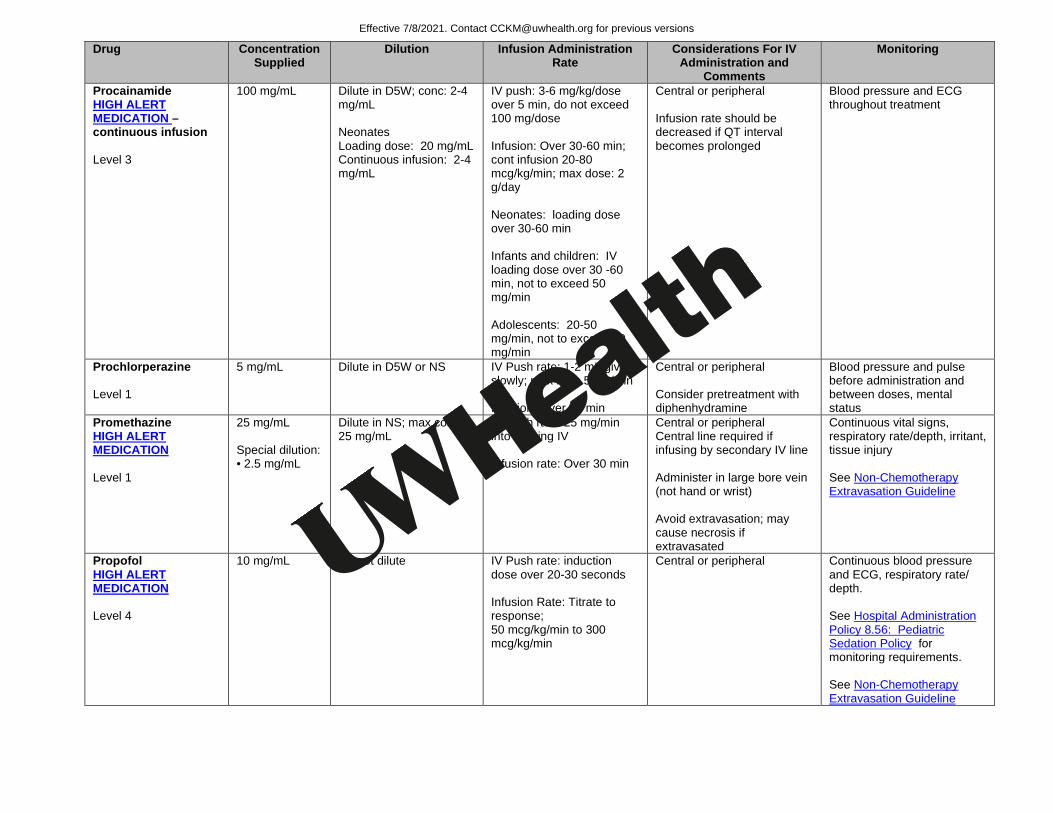
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Procainamide HIGH ALERT MEDICATION –continuous infusion Level 3
100 mg/mL Dilute in D5W; conc: 2-4 mg/mL Neonates Loading dose: 20 mg/mL Continuous infusion: 2-4 mg/mL
IV push: 3-6 mg/kg/dose over 5 min, do not exceed 100 mg/dose Infusion: Over 30-60 min; cont infusion 20-80 mcg/kg/min; max dose: 2 g/day Neonates: loading dose over 30-60 min Infants and children: IV loading dose over 30 -60 min, not to exceed 50 mg/min Adolescents: 20-50 mg/min, not to exceed 50 mg/min
Central or peripheral Infusion rate should be decreased if QT interval becomes prolonged
Blood pressure and ECG throughout treatment
Prochlorperazine Level 1
5 mg/mL Dilute in D5W or NS
IV Push rate: 1-2 mL given slowly; max rate: 5 mg/min Infusion: Over 30 min
Central or peripheral Consider pretreatment with diphenhydramine
Blood pressure and pulse before administration and between doses, mental status
Promethazine HIGH ALERT MEDICATION Level 1
25 mg/mL Special dilution: • 2.5 mg/mL
Dilute in NS; max conc: 25 mg/mL
IV Push rate: 25 mg/min into running IV Infusion rate: Over 30 min
Central or peripheral Central line required if infusing by secondary IV line Administer in large bore vein (not hand or wrist) Avoid extravasation; may cause necrosis if extravasated
Continuous vital signs, respiratory rate/depth, irritant, tissue injury See Non-Chemotherapy Extravasation Guideline
Propofol HIGH ALERT MEDICATION Level 4
10 mg/mL Do not dilute
IV Push rate: induction dose over 20-30 seconds Infusion Rate: Titrate to response; 50 mcg/kg/min to 300 mcg/kg/min
Central or peripheral Continuous blood pressure and ECG, respiratory rate/ depth. See Hospital Administration Policy 8.56: Pediatric Sedation Policy for monitoring requirements. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Propranolol Level 4
1 mg/mL Special dilution: • 0.1 mg/mL
IV Push rate: Over 10 min; max rate: 1 mg/min Infusion not recommended
Central or peripheral Alternative IV agents recommended due to risk of severe arrhythmias with IV propranolol use in pediatric patients
Continuous blood pressure and ECG, respiratory rate/ depth
Protamine Sulfate Level 2 See Procoagulant Guideline
10 mg/mL Do not further dilute
Inject over 10 min, not to exceed 5 mg/min Neonates: rate of undiluted solution not to exceed 5 mg/min
Central or peripheral Observe patient continuously, flushing, blood pressure, coagulation tests
Pyridostigmine Bromide Level 4
5 mg/mL IV Push rate: Over 2-4 min Infusion rate: no information
Central or peripheral Cardiac status, muscle strength, cholinergic reactions
Pyridoxine Level 1
100 mg/mL Dilute in D5W or NS IV Push rate: 100 mg over 2-3 min Infusion Rate: Give at any convenient rate
Central or peripheral Respiratory rate, heart rate, blood pressure, seizure (with large doses), flushing possible
Quinidine Gluconate Level 2
80 mg/mL Dilute 800 mg in 50 mL D5W; conc: 16 mg/mL
Infusion rate: Max rate: 0.25 mg/kg/min or 10 mg/min whichever is lowest
Central or peripheral Use non-PVC tubing
Continuous blood pressure and ECG, hypoglycemia
Ranitidine Level 1
25 mg/mL Special dilution: • 2.5 mg/mL
Dilute in D5W or NS; cont infusion: 150 mg/250 mL
IV Push: over at least 5 min; not to exceed 10 mg/min at max conc: 2.5 mg/mL Intermittent infusion: over at least 5 min, not to exceed 10 mg/min; max conc 2.5 mg/mL Infusion: Single dose of 1 mg/kg, then 0.08 – 0.17 mg/kg/hr; max conc: 0.6 mg/mL Neonates Slow IV push or cont infusion 0.04-0.1 mg/kg/hr
Central or peripheral Intermittent infusion preferred to IV Push
Vital signs, burning/itching at injection site
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
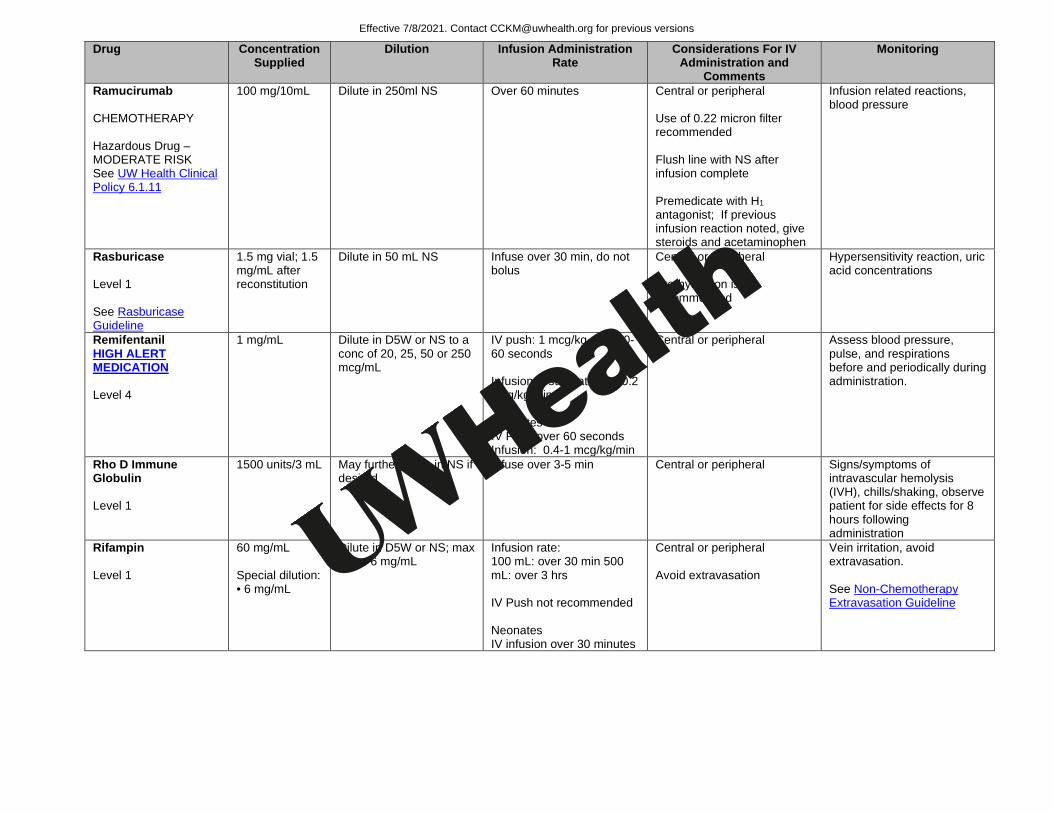
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Ramucirumab CHEMOTHERAPY Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
100 mg/10mL Dilute in 250ml NS Over 60 minutes Central or peripheral Use of 0.22 micron filter recommended Flush line with NS after infusion complete Premedicate with H1 antagonist; If previous infusion reaction noted, give steroids and acetaminophen
Infusion related reactions, blood pressure
Rasburicase Level 1 See Rasburicase Guideline
1.5 mg vial; 1.5 mg/mL after reconstitution
Dilute in 50 mL NS Infuse over 30 min, do not bolus
Central or peripheral Pre-hydration is recommended
Hypersensitivity reaction, uric acid concentrations
Remifentanil HIGH ALERT MEDICATION Level 4
1 mg/mL Dilute in D5W or NS to a conc of 20, 25, 50 or 250 mcg/mL
IV push: 1 mcg/kg over 30-60 seconds Infusion: Usual rate: 0.1-0.2 mcg/kg/min Neonates IV Push over 60 seconds Infusion: 0.4-1 mcg/kg/min
Central or peripheral Assess blood pressure, pulse, and respirations before and periodically during administration.
Rho D Immune Globulin Level 1
1500 units/3 mL May further dilute in NS if desired
Infuse over 3-5 min Central or peripheral Signs/symptoms of intravascular hemolysis (IVH), chills/shaking, observe patient for side effects for 8 hours following administration
Rifampin Level 1
60 mg/mL Special dilution: • 6 mg/mL
Dilute in D5W or NS; max conc: 6 mg/mL
Infusion rate: 100 mL: over 30 min 500 mL: over 3 hrs IV Push not recommended Neonates IV infusion over 30 minutes
Central or peripheral Avoid extravasation
Vein irritation, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
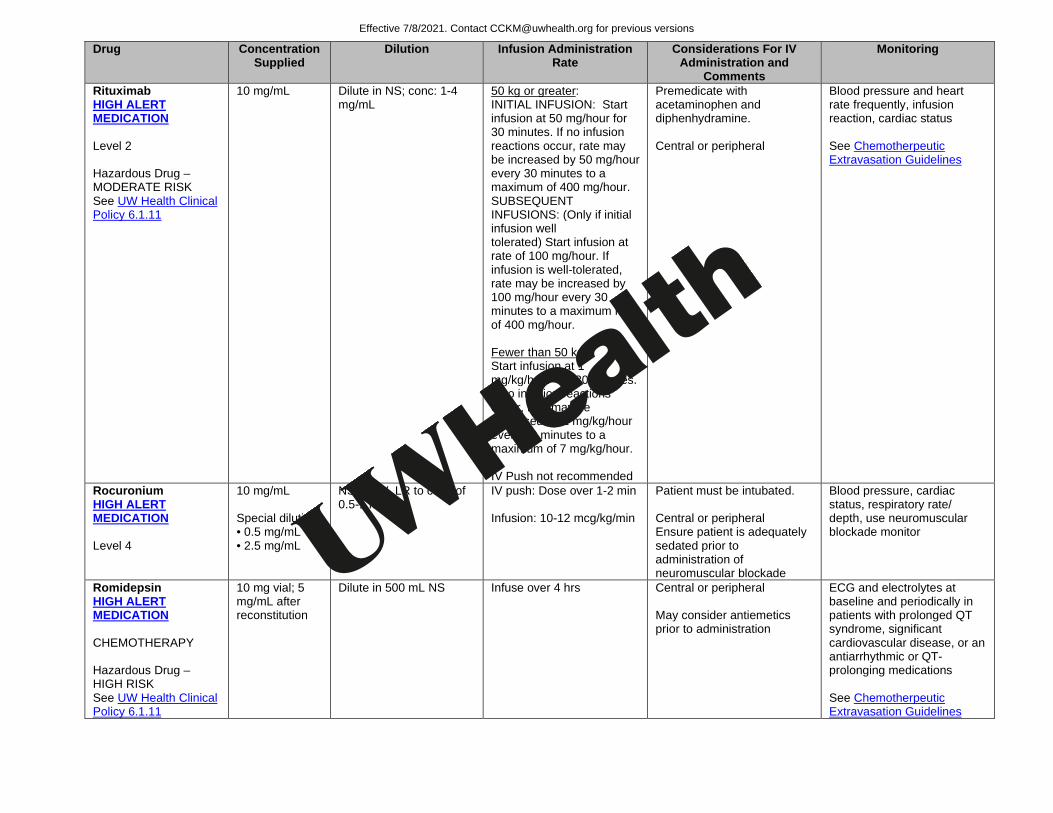
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Rituximab HIGH ALERT MEDICATION Level 2 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
10 mg/mL Dilute in NS; conc: 1-4 mg/mL
50 kg or greater: INITIAL INFUSION: Start infusion at 50 mg/hour for 30 minutes. If no infusion reactions occur, rate may be increased by 50 mg/hour every 30 minutes to a maximum of 400 mg/hour. SUBSEQUENT INFUSIONS: (Only if initial infusion well tolerated) Start infusion at rate of 100 mg/hour. If infusion is well-tolerated, rate may be increased by 100 mg/hour every 30 minutes to a maximum rate of 400 mg/hour. Fewer than 50 kg: Start infusion at 1 mg/kg/hour for 30 minutes. If no infusion reactions occur, rate may be increased by 1 mg/kg/hour every 30 minutes to a maximum of 7 mg/kg/hour. IV Push not recommended
Premedicate with acetaminophen and diphenhydramine. Central or peripheral
Blood pressure and heart rate frequently, infusion reaction, cardiac status See Chemotherpeutic Extravasation Guidelines
Rocuronium HIGH ALERT MEDICATION Level 4
10 mg/mL Special dilution: • 0.5 mg/mL • 2.5 mg/mL
NS, D5W, LR to conc of 0.5-1 mg/mL
IV push: Dose over 1-2 min Infusion: 10-12 mcg/kg/min
Patient must be intubated. Central or peripheral Ensure patient is adequately sedated prior to administration of neuromuscular blockade
Blood pressure, cardiac status, respiratory rate/ depth, use neuromuscular blockade monitor
Romidepsin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg vial; 5 mg/mL after reconstitution
Dilute in 500 mL NS Infuse over 4 hrs Central or peripheral May consider antiemetics prior to administration
ECG and electrolytes at baseline and periodically in patients with prolonged QT syndrome, significant cardiovascular disease, or an antiarrhythmic or QT-prolonging medications See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
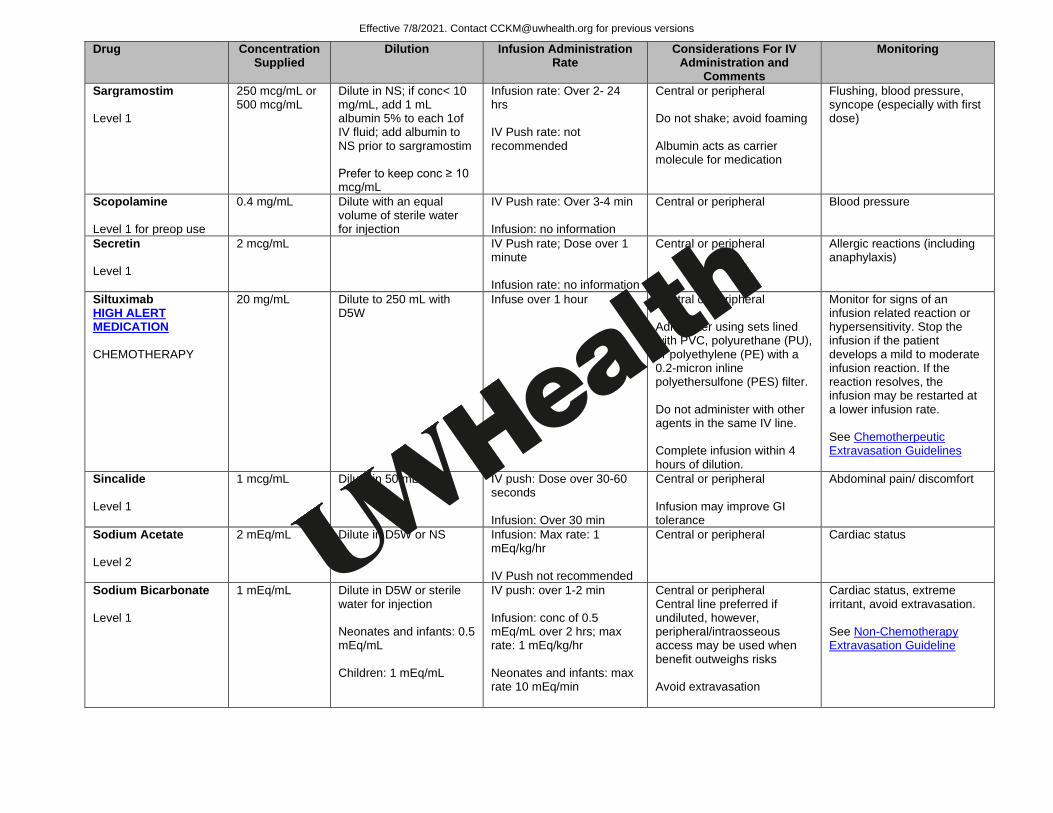
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Sargramostim Level 1
250 mcg/mL or 500 mcg/mL
Dilute in NS; if conc< 10 mg/mL, add 1 mL albumin 5% to each 1of IV fluid; add albumin to NS prior to sargramostim Prefer to keep conc ≥ 10 mcg/mL
Infusion rate: Over 2- 24 hrs IV Push rate: not recommended
Central or peripheral Do not shake; avoid foaming Albumin acts as carrier molecule for medication
Flushing, blood pressure, syncope (especially with first dose)
Scopolamine Level 1 for preop use
0.4 mg/mL Dilute with an equal volume of sterile water for injection
IV Push rate: Over 3-4 min Infusion: no information
Central or peripheral Blood pressure
Secretin Level 1
2 mcg/mL IV Push rate; Dose over 1 minute Infusion rate: no information
Central or peripheral Allergic reactions (including anaphylaxis)
Siltuximab HIGH ALERT MEDICATION CHEMOTHERAPY
20 mg/mL Dilute to 250 mL with D5W
Infuse over 1 hour Central or peripheral Administer using sets lined with PVC, polyurethane (PU), or polyethylene (PE) with a 0.2-micron inline polyethersulfone (PES) filter. Do not administer with other agents in the same IV line. Complete infusion within 4 hours of dilution.
Monitor for signs of an infusion related reaction or hypersensitivity. Stop the infusion if the patient develops a mild to moderate infusion reaction. If the reaction resolves, the infusion may be restarted at a lower infusion rate. See Chemotherpeutic Extravasation Guidelines
Sincalide Level 1
1 mcg/mL Dilute in 50 mL NS IV push: Dose over 30-60 seconds Infusion: Over 30 min
Central or peripheral Infusion may improve GI tolerance
Abdominal pain/ discomfort
Sodium Acetate Level 2
2 mEq/mL Dilute in D5W or NS Infusion: Max rate: 1 mEq/kg/hr IV Push not recommended
Central or peripheral Cardiac status
Sodium Bicarbonate Level 1
1 mEq/mL Dilute in D5W or sterile water for injection Neonates and infants: 0.5 mEq/mL Children: 1 mEq/mL
IV push: over 1-2 min Infusion: conc of 0.5 mEq/mL over 2 hrs; max rate: 1 mEq/kg/hr Neonates and infants: max rate 10 mEq/min
Central or peripheral Central line preferred if undiluted, however, peripheral/intraosseous access may be used when benefit outweighs risks Avoid extravasation
Cardiac status, extreme irritant, avoid extravasation. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
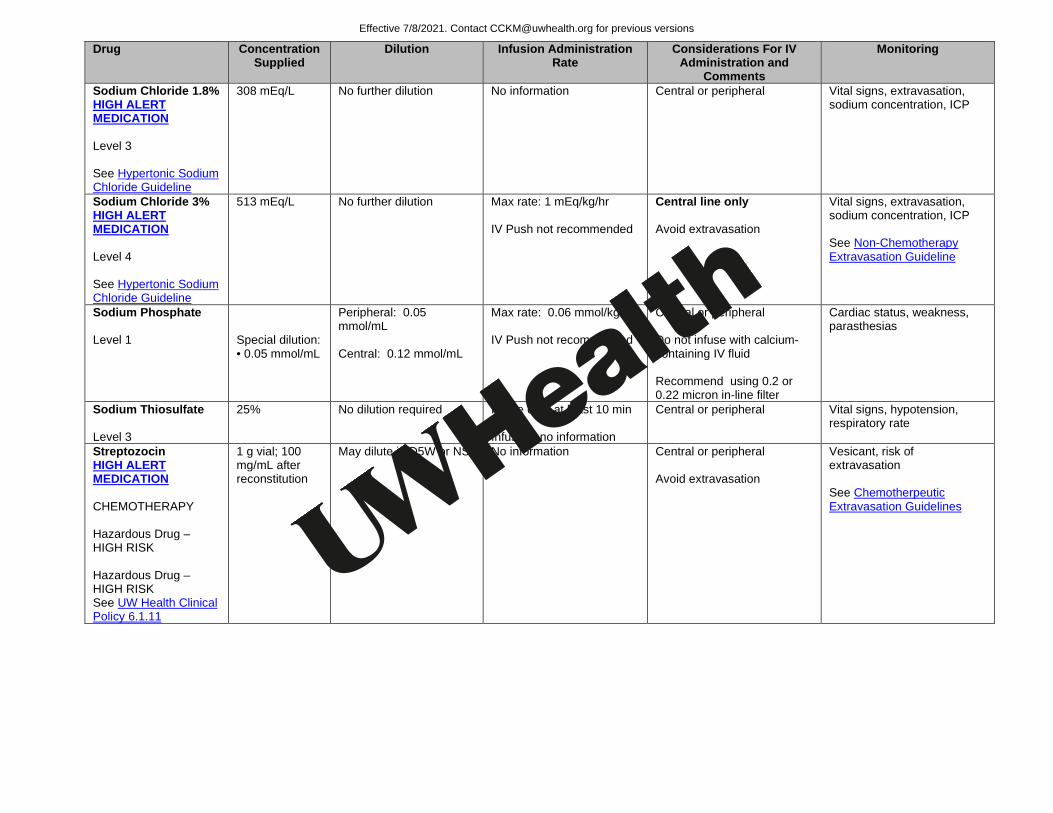
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Sodium Chloride 1.8% HIGH ALERT MEDICATION Level 3 See Hypertonic Sodium Chloride Guideline
308 mEq/L No further dilution No information Central or peripheral Vital signs, extravasation, sodium concentration, ICP
Sodium Chloride 3% HIGH ALERT MEDICATION Level 4 See Hypertonic Sodium Chloride Guideline
513 mEq/L No further dilution
Max rate: 1 mEq/kg/hr IV Push not recommended
Central line only Avoid extravasation
Vital signs, extravasation, sodium concentration, ICP See Non-Chemotherapy Extravasation Guideline
Sodium Phosphate Level 1
Special dilution: • 0.05 mmol/mL
Peripheral: 0.05 mmol/mL Central: 0.12 mmol/mL
Max rate: 0.06 mmol/kg/hr IV Push not recommended
Central or peripheral Do not infuse with calcium-containing IV fluid Recommend using 0.2 or 0.22 micron in-line filter
Cardiac status, weakness, parasthesias
Sodium Thiosulfate Level 3
25% No dilution required Infuse over at least 10 min Infusion: no information
Central or peripheral Vital signs, hypotension, respiratory rate
Streptozocin HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 g vial; 100 mg/mL after reconstitution
May dilute in D5W or NS No information Central or peripheral Avoid extravasation
Vesicant, risk of extravasation See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Succinylcholine HIGH ALERT MEDICATION Level 4
20 mg/mL Neonates: may dilute in compatible solution to conc 1-2 mg/mL
Dose over 30 seconds undiluted Cont infusions not recommended
Patient must be intubated. Central or peripheral Use with caution in patient with severe trauma, severe/extensive burns, skeletal muscle denervation, degenerative/dystrophic neuromuscular disease due to hyperkalemia risk Use with caution in patients with fractures or muscle spasms as initial fasiculations may cause additional trauma
Blood pressure, cardiac status, respiratory rate/ depth, serum potassium, use neuromuscular blockade monitor
Sufentanil HIGH ALERT MEDICATION Level 4
50 mcg/mL IV Push rate: Over 30 seconds Infusion: no information
Central or peripheral Assess blood pressure, pulse, and respirations before and periodically during administration, neurologic status
Sugammedex Level 4
500 mg/5 mL Two years and older: No dilution required Younger than two years: Dilute in NS to 25 mg/mL
Over 10 seconds Central, midline, or peripheral Flush lV line with NS before and after administration of sugammadex
Hypersensitivity and anaphylaxis, bradycardia, recurrence of neuromuscular blockade, respiratory function, skeletal muscle tone Drug interaction with hormonal contraceptive agents
Tacrolimus Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
5 mg/mL Dilute in D5W or NS; conc: 0.004-0.02 mg/mL
IV Push not recommended Avoid PVC-containing containers and tubing Central or peripheral
Blood pressure, anaphylaxis, tacrolimus concentrations
TBO-filgrastim Level 1
300 mcg, 480 mcg
Final conc 15 mcg/mL If final conc 5 to <15 mcg/mL, add albumin to a final conc of 2 mg/mL Avoid conc <5 mcg/mL
Infusion over 15-30 min or continuous infusion or 4- or 24-hr infusion
Do not shake; avoid foaming Temperature, CBC, cardiac status, hypersensitivity reaction
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
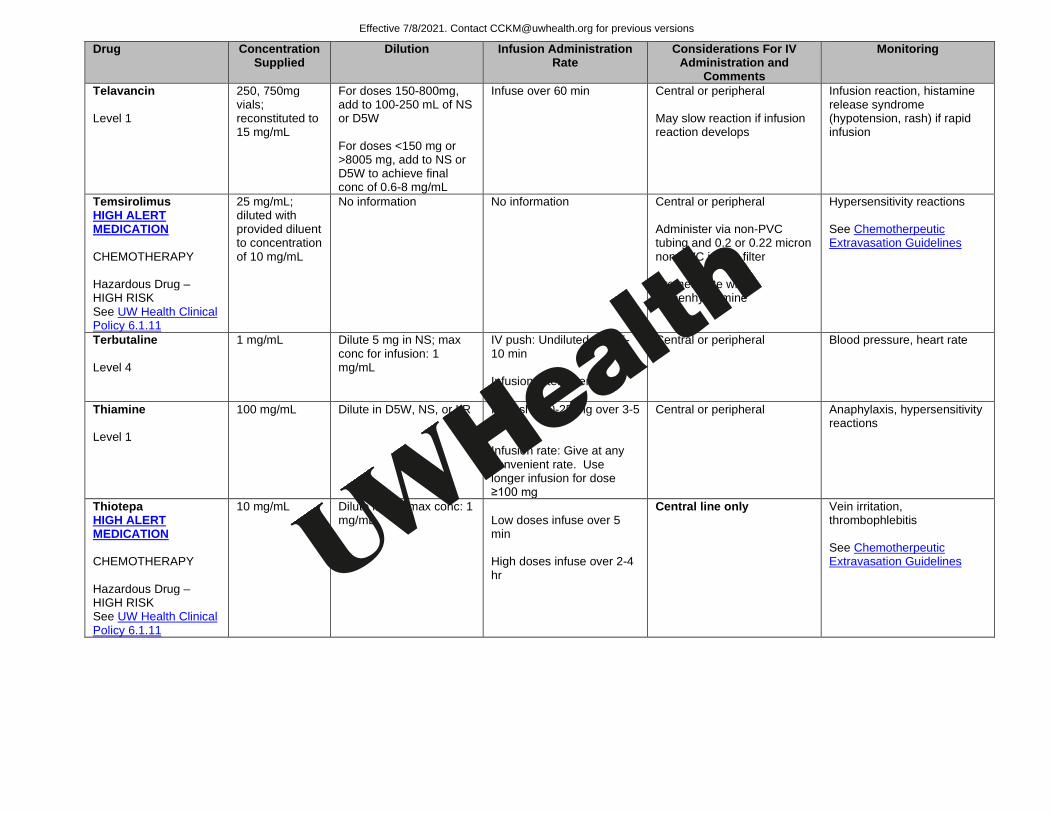
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Telavancin Level 1
250, 750mg vials; reconstituted to 15 mg/mL
For doses 150-800mg, add to 100-250 mL of NS or D5W For doses <150 mg or >8005 mg, add to NS or D5W to achieve final conc of 0.6-8 mg/mL
Infuse over 60 min Central or peripheral May slow reaction if infusion reaction develops
Infusion reaction, histamine release syndrome (hypotension, rash) if rapid infusion
Temsirolimus HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
25 mg/mL; diluted with provided diluent to concentration of 10 mg/mL
No information No information Central or peripheral Administer via non-PVC tubing and 0.2 or 0.22 micron non-PVC in-line filter Premedicate with diphenhydramine
Hypersensitivity reactions See Chemotherpeutic Extravasation Guidelines
Terbutaline Level 4
1 mg/mL Dilute 5 mg in NS; max conc for infusion: 1 mg/mL
IV push: Undiluted over 5-10 min Infusion rate: Over 12-24 hrs
Central or peripheral Blood pressure, heart rate
Thiamine Level 1
100 mg/mL Dilute in D5W, NS, or LR
IV push: 10-25 mg over 3-5 min Infusion rate: Give at any convenient rate. Use longer infusion for dose ≥100 mg
Central or peripheral Anaphylaxis, hypersensitivity reactions
Thiotepa HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/mL Dilute in NS; max conc: 1 mg/mL
Low doses infuse over 5 min High doses infuse over 2-4 hr
Central line only Vein irritation, thrombophlebitis See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
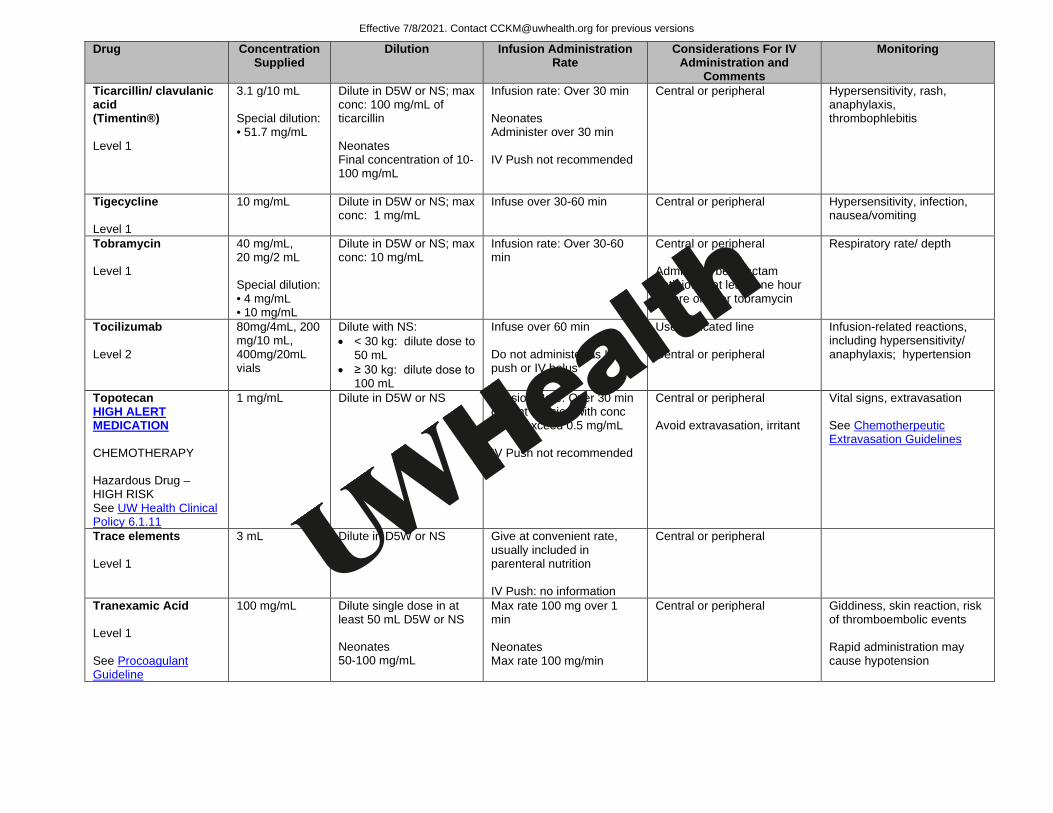
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Ticarcillin/ clavulanic acid (Timentin®) Level 1
3.1 g/10 mL Special dilution: • 51.7 mg/mL
Dilute in D5W or NS; max conc: 100 mg/mL of ticarcillin Neonates Final concentration of 10-100 mg/mL
Infusion rate: Over 30 min Neonates Administer over 30 min IV Push not recommended
Central or peripheral Hypersensitivity, rash, anaphylaxis, thrombophlebitis
Tigecycline Level 1
10 mg/mL Dilute in D5W or NS; max conc: 1 mg/mL
Infuse over 30-60 min Central or peripheral Hypersensitivity, infection, nausea/vomiting
Tobramycin Level 1
40 mg/mL, 20 mg/2 mL Special dilution: • 4 mg/mL • 10 mg/mL
Dilute in D5W or NS; max conc: 10 mg/mL
Infusion rate: Over 30-60 min
Central or peripheral Administer beta-lactam antibiotics at least one hour before or after tobramycin
Respiratory rate/ depth
Tocilizumab Level 2
80mg/4mL, 200 mg/10 mL, 400mg/20mL vials
Dilute with NS: • < 30 kg: dilute dose to
50 mL • ≥ 30 kg: dilute dose to
100 mL
Infuse over 60 min Do not administer as IV push or IV bolus
Use dedicated line Central or peripheral
Infusion-related reactions, including hypersensitivity/ anaphylaxis; hypertension
Topotecan HIGH ALERT MEDICATION CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute in D5W or NS
Infusion Rate: Over 30 min or cont infusion with conc not to exceed 0.5 mg/mL IV Push not recommended
Central or peripheral Avoid extravasation, irritant
Vital signs, extravasation See Chemotherpeutic Extravasation Guidelines
Trace elements Level 1
3 mL Dilute in D5W or NS
Give at convenient rate, usually included in parenteral nutrition IV Push: no information
Central or peripheral
Tranexamic Acid Level 1 See Procoagulant Guideline
100 mg/mL Dilute single dose in at least 50 mL D5W or NS Neonates 50-100 mg/mL
Max rate 100 mg over 1 min Neonates Max rate 100 mg/min
Central or peripheral Giddiness, skin reaction, risk of thromboembolic events Rapid administration may cause hypotension
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
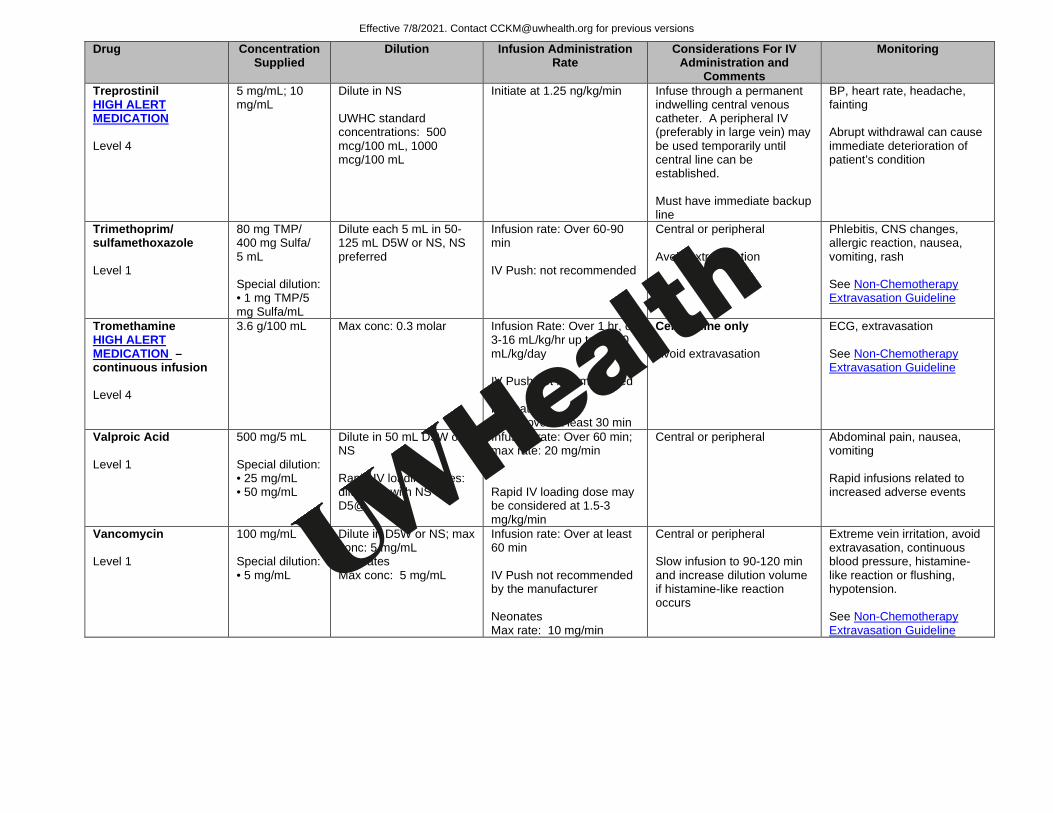
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Treprostinil HIGH ALERT MEDICATION Level 4
5 mg/mL; 10 mg/mL
Dilute in NS UWHC standard concentrations: 500 mcg/100 mL, 1000 mcg/100 mL
Initiate at 1.25 ng/kg/min Infuse through a permanent indwelling central venous catheter. A peripheral IV (preferably in large vein) may be used temporarily until central line can be established. Must have immediate backup line
BP, heart rate, headache, fainting Abrupt withdrawal can cause immediate deterioration of patient’s condition
Trimethoprim/ sulfamethoxazole Level 1
80 mg TMP/ 400 mg Sulfa/ 5 mL Special dilution: • 1 mg TMP/5 mg Sulfa/mL
Dilute each 5 mL in 50-125 mL D5W or NS, NS preferred
Infusion rate: Over 60-90 min IV Push: not recommended
Central or peripheral Avoid extravasation
Phlebitis, CNS changes, allergic reaction, nausea, vomiting, rash See Non-Chemotherapy Extravasation Guideline
Tromethamine HIGH ALERT MEDICATION – continuous infusion Level 4
3.6 g/100 mL Max conc: 0.3 molar
Infusion Rate: Over 1 hr, or 3-16 mL/kg/hr up to 33-40 mL/kg/day IV Push not recommended Neonates Infuse over at least 30 min
Central line only Avoid extravasation
ECG, extravasation See Non-Chemotherapy Extravasation Guideline
Valproic Acid Level 1
500 mg/5 mL Special dilution: • 25 mg/mL • 50 mg/mL
Dilute in 50 mL D5W or NS Rapid IV loading doses: dilute 1:1 with NS or D5@
Infusion rate: Over 60 min; max rate: 20 mg/min Rapid IV loading dose may be considered at 1.5-3 mg/kg/min
Central or peripheral Abdominal pain, nausea, vomiting Rapid infusions related to increased adverse events
Vancomycin Level 1
100 mg/mL Special dilution: • 5 mg/mL
Dilute in D5W or NS; max conc: 5 mg/mL Neonates Max conc: 5 mg/mL
Infusion rate: Over at least 60 min IV Push not recommended by the manufacturer Neonates Max rate: 10 mg/min
Central or peripheral Slow infusion to 90-120 min and increase dilution volume if histamine-like reaction occurs
Extreme vein irritation, avoid extravasation, continuous blood pressure, histamine-like reaction or flushing, hypotension. See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
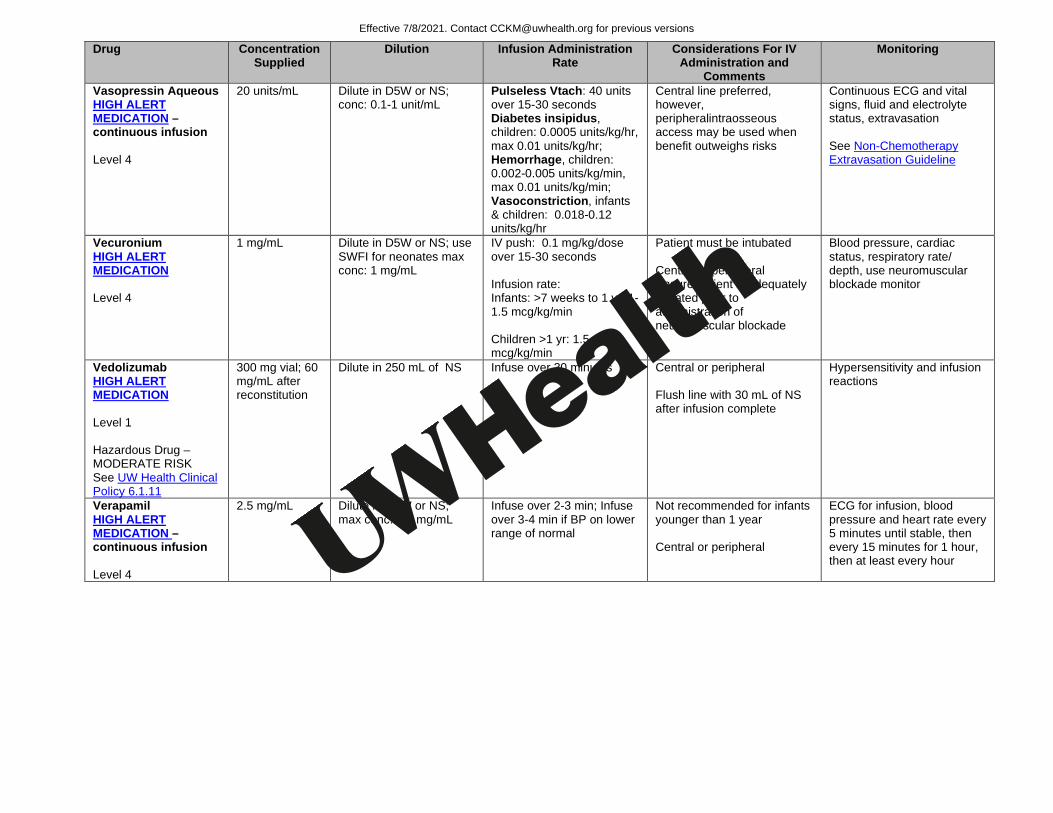
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Vasopressin Aqueous HIGH ALERT MEDICATION – continuous infusion Level 4
20 units/mL Dilute in D5W or NS; conc: 0.1-1 unit/mL
Pulseless Vtach: 40 units over 15-30 seconds Diabetes insipidus, children: 0.0005 units/kg/hr, max 0.01 units/kg/hr; Hemorrhage, children: 0.002-0.005 units/kg/min, max 0.01 units/kg/min; Vasoconstriction, infants & children: 0.018-0.12 units/kg/hr
Central line preferred, however, peripheralintraosseous access may be used when benefit outweighs risks
Continuous ECG and vital signs, fluid and electrolyte status, extravasation See Non-Chemotherapy Extravasation Guideline
Vecuronium HIGH ALERT MEDICATION Level 4
1 mg/mL Dilute in D5W or NS; use SWFI for neonates max conc: 1 mg/mL
IV push: 0.1 mg/kg/dose over 15-30 seconds Infusion rate: Infants: >7 weeks to 1 yr: 1-1.5 mcg/kg/min Children >1 yr: 1.5-2.5 mcg/kg/min
Patient must be intubated Central or peripheral Ensure patient is adequately sedated prior to administration of neuromuscular blockade
Blood pressure, cardiac status, respiratory rate/ depth, use neuromuscular blockade monitor
Vedolizumab HIGH ALERT MEDICATION Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
300 mg vial; 60 mg/mL after reconstitution
Dilute in 250 mL of NS Infuse over 30 minutes Central or peripheral Flush line with 30 mL of NS after infusion complete
Hypersensitivity and infusion reactions
Verapamil HIGH ALERT MEDICATION – continuous infusion Level 4
2.5 mg/mL Dilute in D5W or NS; max conc: 2.5 mg/mL
Infuse over 2-3 min; Infuse over 3-4 min if BP on lower range of normal
Not recommended for infants younger than 1 year Central or peripheral
ECG for infusion, blood pressure and heart rate every 5 minutes until stable, then every 15 minutes for 1 hour, then at least every hour
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
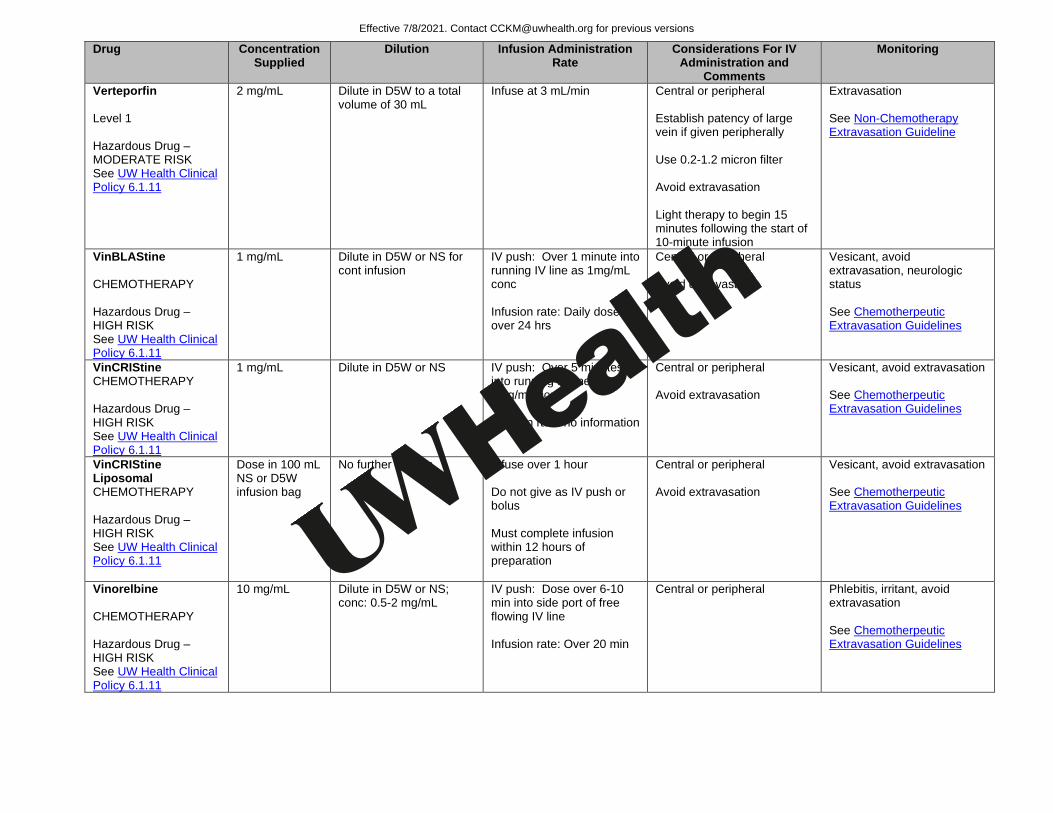
Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Verteporfin Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
2 mg/mL Dilute in D5W to a total volume of 30 mL
Infuse at 3 mL/min Central or peripheral Establish patency of large vein if given peripherally Use 0.2-1.2 micron filter Avoid extravasation Light therapy to begin 15 minutes following the start of 10-minute infusion
Extravasation See Non-Chemotherapy Extravasation Guideline
VinBLAStine CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute in D5W or NS for cont infusion
IV push: Over 1 minute into running IV line as 1mg/mL conc Infusion rate: Daily dose over 24 hrs
Central or peripheral Avoid extravasation
Vesicant, avoid extravasation, neurologic status See Chemotherpeutic Extravasation Guidelines
VinCRIStine CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
1 mg/mL Dilute in D5W or NS
IV push: Over 5 minutes into running IV line as 1mg/mL conc Infusion rate: no information
Central or peripheral Avoid extravasation
Vesicant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
VinCRIStine Liposomal CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
Dose in 100 mL NS or D5W infusion bag
No further dilution Infuse over 1 hour Do not give as IV push or bolus Must complete infusion within 12 hours of preparation
Central or peripheral Avoid extravasation
Vesicant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Vinorelbine CHEMOTHERAPY Hazardous Drug – HIGH RISK See UW Health Clinical Policy 6.1.11
10 mg/mL Dilute in D5W or NS; conc: 0.5-2 mg/mL
IV push: Dose over 6-10 min into side port of free flowing IV line Infusion rate: Over 20 min
Central or peripheral Phlebitis, irritant, avoid extravasation See Chemotherpeutic Extravasation Guidelines
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/clinical/cckm-tools/content/?path=/content/cpg/oncology/name-97715-en.cckm
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy

Drug Concentration Supplied
Dilution Infusion Administration Rate
Considerations For IV Administration and
Comments
Monitoring
Von Willebrand Factor Level 1
No further dilution
IV Push rate: Slowly, max 4 mL/min Infusion rate: no information
Use infusion kit Central or peripheral
Voriconazole Level 1
10 mg/mL Special dilution: • 4 mg/mL
Dilute in D5W or NS; conc: 0.5-5 mg/mL
Over 1-2 hrs; max rate: 3 mg/kg/hr IV Push not recommended
Central or peripheral Hypersensitivity reactions, anaphylaxis, tachycardia
Warfarin Sodium Level 1
2 mg/mL Not recommended IV push: over 1-2 min Infusion not recommended
INR, bleeding
Zinc trace metal Level 1
1 mg/mL, and 5mg/mL as sulfate
Dilute in D5W or NS
Infusion rate: Give at convenient rate IV Push not recommended
Central or peripheral
Zidovudine Level 2
10 mg/mL Special dilution: • 1 mg/mL • 4 mg/mL
Dilute with D5W, max conc: 4 mg/mL
Infuse over 60 min Neonates Infuse over 60 min
Cardiac status (ECG), chills, fever, CNS changes, rash, allergic reactions
Zoledronic Acid Level 1 Hazardous Drug – MODERATE RISK See UW Health Clinical Policy 6.1.11
4 mg/5 mL Dilute in NS or D5W
Infusion rate: Over at least 15 min IV Push not recommended
Avoid extravasation See Non-Chemotherapy Extravasation Guideline
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
https://uconnect.wisc.edu/policies/clinical/uw-health-clinical/medications-and-pharmacy/-6111.policy
UW Health Implementation Potential Benefits:
• Safety and efficacy through standardizaton of intravenous administration of medications • Direction on important monitoring areas
Potentail Harms:
• Standardized intravenous administration may not optimize medication therapy for all patients Qualifying Statements Recommendations in this guideline are based on available evidence. Administration of medications should be evaluated in a patient-specific manner and should take into account the urgency of a given situation when determining administration rate and route. Pertinent UWHC Policies and Procedures
• Policy 8.31 Guidelines for Hospital Location Specific Administration of IV Medications • Policy 8.33 High Alert Medication Administration • Policy 8.56 Pediatric Sedation • Policy 8.89 Preventing Non-therapeutic Exposure to Hazardous Drugs • Factor 7a Recombinant Operating Procedure • Factor 9 Complex Concentrate (PCC) Operating Procedure • Policy 10.18 Parenteral Lidocaine for Neuropathic Pain
Patient Resources None Guideline Metrics Patient Safety Net reports can be monitored for errors or adverse events associated with IV medication administration. Implementation Plan/Clinical Tools 1. Guideline will be posted on uConnect in a dedicated location for Clinical Practice Guidelines. 2. Release of the guideline will be advertised in the Physician/APP Briefing newsletter. 3. Content and hyperlinks within clinical tools, documents, or Health Link related to the guideline
recommendations will be reviewed for consistency and modified as appropriate. Disclaimer Clinical practice guidelines assist clinicians by providing a framework for the evaluation and treatment of patients. This guideline outlines the preferred approach for most patients. It is not intended to replace a clinician’s judgment or to establish a protocol for all patients. It is understood that some patients will not fit the clinical condition contemplated by a guideline and that a guideline will rarely establish the only appropriate approach to a problem.
References 1. Jacobs AK, Kushner FG, Ettinger SM, et al. ACCF/AHA clinical practice guideline methodology summit
report: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2013;61(2):213-265.
2. Lexi-Comp Online™, Lexi-Drugs Online™ Hudson, OH: Lexi-Comp,Inc; Accessed July 2016. 3. Neofax Online®. Micromedex® Ann Arbor, MI: Truven Health Analytics™: Accessed July 2016.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021

Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
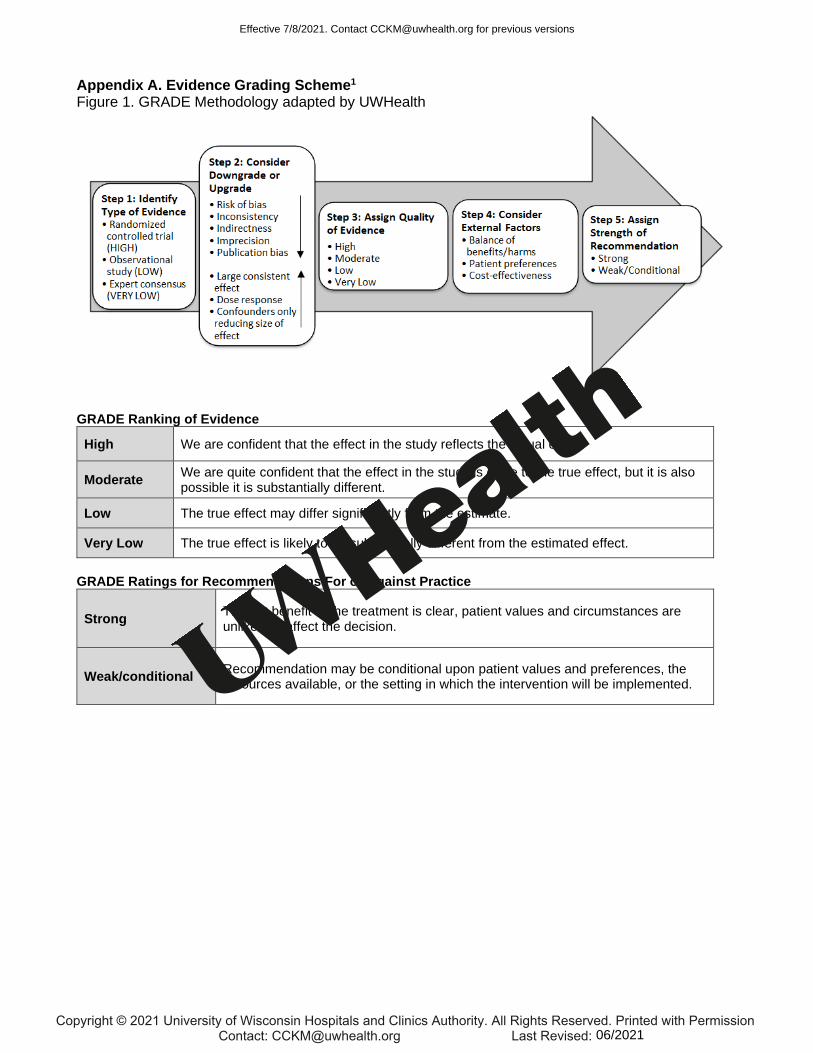
Appendix A. Evidence Grading Scheme1
Figure 1. GRADE Methodology adapted by UWHealth
GRADE Ranking of Evidence
High We are confident that the effect in the study reflects the actual effect.
Moderate We are quite confident that the effect in the study is close to the true effect, but it is also possible it is substantially different.
Low The true effect may differ significantly from the estimate.
Very Low The true effect is likely to be substantially different from the estimated effect.
GRADE Ratings for Recommendations For or Against Practice
Strong The net benefit of the treatment is clear, patient values and circumstances are unlikely to affect the decision.
Weak/conditional Recommendation may be conditional upon patient values and preferences, the resources available, or the setting in which the intervention will be implemented.
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021
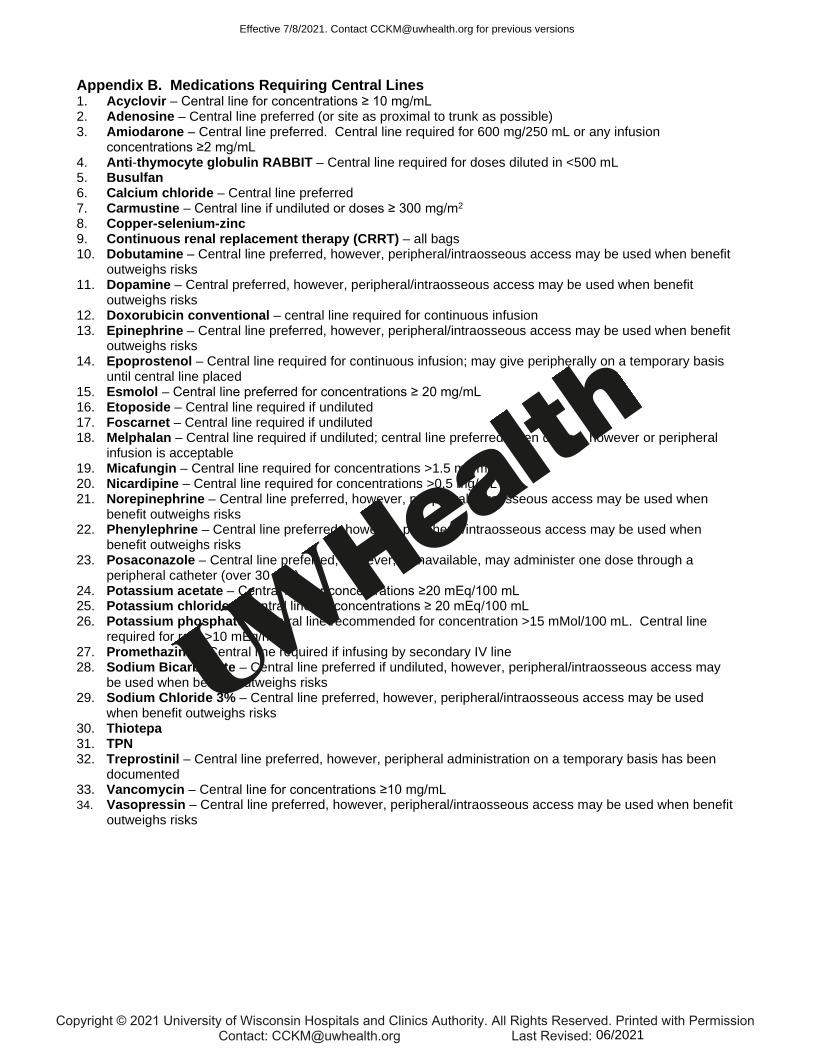
Appendix B. Medications Requiring Central Lines 1. Acyclovir – Central line for concentrations ≥ 10 mg/mL 2. Adenosine – Central line preferred (or site as proximal to trunk as possible) 3. Amiodarone – Central line preferred. Central line required for 600 mg/250 mL or any infusion
concentrations ≥2 mg/mL 4. Anti-thymocyte globulin RABBIT – Central line required for doses diluted in <500 mL 5. Busulfan 6. Calcium chloride – Central line preferred 7. Carmustine – Central line if undiluted or doses ≥ 300 mg/m2 8. Copper-selenium-zinc 9. Continuous renal replacement therapy (CRRT) – all bags 10. Dobutamine – Central line preferred, however, peripheral/intraosseous access may be used when benefit
outweighs risks 11. Dopamine – Central preferred, however, peripheral/intraosseous access may be used when benefit
outweighs risks 12. Doxorubicin conventional – central line required for continuous infusion 13. Epinephrine – Central line preferred, however, peripheral/intraosseous access may be used when benefit
outweighs risks 14. Epoprostenol – Central line required for continuous infusion; may give peripherally on a temporary basis
until central line placed 15. Esmolol – Central line preferred for concentrations ≥ 20 mg/mL 16. Etoposide – Central line required if undiluted 17. Foscarnet – Central line required if undiluted 18. Melphalan – Central line required if undiluted; central line preferred when diluted, however or peripheral
infusion is acceptable 19. Micafungin – Central line required for concentrations >1.5 mg/mL 20. Nicardipine – Central line required for concentrations >0.5 mg/mL 21. Norepinephrine – Central line preferred, however, peripheral/intraosseous access may be used when
benefit outweighs risks 22. Phenylephrine – Central line preferred, however, peripheral/intraosseous access may be used when
benefit outweighs risks 23. Posaconazole – Central line preferred, however, if unavailable, may administer one dose through a
peripheral catheter (over 30 min) 24. Potassium acetate – Central line for concentrations ≥20 mEq/100 mL 25. Potassium chloride – Central line for concentrations ≥ 20 mEq/100 mL 26. Potassium phosphate – Central line recommended for concentration >15 mMol/100 mL. Central line
required for rate >10 mEq/hr 27. Promethazine – Central line required if infusing by secondary IV line 28. Sodium Bicarbonate – Central line preferred if undiluted, however, peripheral/intraosseous access may
be used when benefit outweighs risks 29. Sodium Chloride 3% – Central line preferred, however, peripheral/intraosseous access may be used
when benefit outweighs risks 30. Thiotepa 31. TPN 32. Treprostinil – Central line preferred, however, peripheral administration on a temporary basis has been
documented 33. Vancomycin – Central line for concentrations ≥10 mg/mL 34. Vasopressin – Central line preferred, however, peripheral/intraosseous access may be used when benefit
outweighs risks
Effective 7/8/2021. Contact [email protected] for previous versions
Copyright © 2021 University of Wisconsin Hospitals and Clinics Authority. All Rights Reserved. Printed with Permission Contact: [email protected] Last Revised: 06/2021


















