INTRAOPERATIVE MONITORING DURING CAROTID ENDARTERECTOMY (CEA) Che’Patrick, REEG,EPT,CNIM.
16
INTRAOPERATIVE MONITORING DURING CAROTID ENDARTERECTOMY (CEA) Che’Patrick, REEG,EPT,CNIM
-
Upload
mabel-carroll -
Category
Documents
-
view
221 -
download
1
Transcript of INTRAOPERATIVE MONITORING DURING CAROTID ENDARTERECTOMY (CEA) Che’Patrick, REEG,EPT,CNIM.

INTRAOPERATIVE MONITORING DURING CAROTID
ENDARTERECTOMY (CEA)
Che’Patrick, REEG,EPT,CNIM

Introduction
Electrophysiological monitoring during CEA has proven to be extremely beneficial in preventing permanent neurological deficits. Intraoperative EEG monitoring is the most common choice for CEAEEG provides a quantitative measure for the spontaneous electrical activity of the brain.

CEA Facts
CEA - introduced in 1954 as a surgical procedure designed to remove plaque material from an occluded artery in the neck.Plaque material is made up of cholesterol, calcium and fibrous tissue.If untreated, a blocked artery can cause a stroke. Strokes are the third leading cause of deaths in the United States.NEJM (1991) - concludes that CEA is highly beneficial to patients with recent TIAs and high grade stenosis of greater then 70% of the ICA.

Understanding Our Arterial System
The brain receives blood through four arteries:
a. The right and left common carotid arteries.
b. The right and left vertebral arteries.
The common carotids bifurcate into:
- external carotid artery (supplies face and skull
- internal carotid artery (supplies the brain, no
branches outside cranium)

Carotid Circulation
The circle of Willis is a band of arteries at the base of the brain formed by the internal and the basilar artery.
These arteries form a complete ring which effectively act as anastomoses for each other during cross clampingIn theory, if a communicating artery becomes blocked, blood can flow from another part of the circle to ensure that the brain is not compromised.
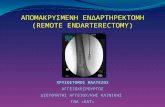
Basilar view of the Circle of Willis

Atherosclerotic plaque tends to develop at the bifurcation of ICA and ECA (just below the level of the jaw)
arrow pointing to bifurcation

Plaque material

Carotid Endarterectomy Surgery
CEA was developed to prevent cerebrovascular accidents or TIAs Clamping of the ICA in the neck to remove the plaque from the blocked artery.To avoid the risk of producing ischemia of the ipsilateral hemisphere and a consequent deficit, techniques employed:
Intraoperative EEG monitoring Somatosensory evoked potentials Transcranial Doppler CBF measurements Internal carotid stump pressure
However, EEG is rapidly becoming the standard of care for inpatients undergoing CEA because it is continuous, non-invasive, inexpensive and most importantly, it provides direct feedback within seconds after carotid clamping that the brain is adequately perfused and oxygenated.

Why are we monitoring?EEG changes can occur 10-15 second after cross clamping of the ipsilateral internal carotid artery occur due to reduced cerebral perfusion as a result of insufficient collateral circulation.Most surgeons resort to shunting once changes are reported, After removal of clamp, slowing may persist for 2-3 minutes until arterial blood flow has been restored to the carotid arteryPrior to surgical monitoring, surgeons would place a bypass shunt around the atherosclerotic plaque, which carried blood to the brain for oxygenation

Technical considerationsUse at least 19 electrodes (international 10-20 system) - covers major vascular territories and allows overlap within the montage should an electrode fail
Electrode application (vary depending on departmental policy): disc electrodes with collodion, disposable sub-dermal needles or electrode
caps.
Patient arrives in laboratory to under go hook-up prior to entering the operating room.
14 or more channels - allows simultaneous display of activity from a variety of cortical areas.
Preoperative EEG baseline obtained during relaxed wakefulness should be performed prior to surgery. Patients with an abnormal EEG are more likely to show changes with cross-clamping of the ICA
Recording parameters:HFF of 70 Hz, LFF 1.0 Hz (60 Hz notch filter may be necessary)
paper speed of at least 15 mm/second

Time To Put The Patient To Sleep

Effects of Anesthesia on EEGPharmacologic agents used for induction and
maintenanceLow doses: rhythmic beta activity (18-25 Hz) over the anterior hemisphere (similar to a normal awake and relaxed patients with eyes closed)This beta increases in amplitude, widespread, anterior maximum and rhythmic, activity (WAR) In addition, intermittent delta waves may be seen over the anterior hemisphere. Other factors that can effect EEG
- lowering of PaC02 < 40 mm Hg - decreased blood pressure - hypothermia - hypoxia

Surgical Procedure
Obtain baselines with patient awake and eyes closed. Anesthetic that provides minimal adverse effects on CNS is preferableCommunicating with the anesthetist to use agents that will not interfere with the EEG recording is very important. medications ready to use. Just remind the anesthesiologist “Not To Bolus”

Induction

Post induction, the EEG can demonstrate generalized slowing, with a decrease in voltage, or a burst suppression pattern.
Should this happen, alert the surgeon immediately since you will not be able be able to tell if a change has occurred from the patient’s baseline when clamping occurs.
The surgeon can choose to proceed with the surgery or wait until the bolus has worn off. Keep in mind cerebral profusion can not be determined with barbiturates on board.

Burst Suppression