
intraoperative monitoring
56
Intraoperative Intraoperative Monitoring Monitoring
-
Upload
anaesthesiology-mgmcri -
Category
Healthcare
-
view
337 -
download
2
Transcript of intraoperative monitoring

Intraoperative Intraoperative MonitoringMonitoring
Intraoperative monitoringIntraoperative monitoring:: IntroductionThe most primitive method of monitoring the The most primitive method of monitoring the
patient 25 years ago was patient 25 years ago was continuous continuous palpationpalpation of the of the radial pulsationsradial pulsations throughout the operation!!throughout the operation!!
What is the value of knowing this?What is the value of knowing this? To understand & appreciate the To understand & appreciate the
value of value of clinicalclinical monitoring. monitoring. RULERULE:: your your clinical clinical
judgement/assessmentjudgement/assessment is much is much BETTERBETTER & much more & much more VALUABLEVALUABLE than the digital monitor.than the digital monitor.
To appreciate that modern monitors To appreciate that modern monitors have made life much easier for us. have made life much easier for us. They are present to make monitoring They are present to make monitoring easier for us NOT to be omitted or easier for us NOT to be omitted or ignored.ignored.

Intraoperative monitoringIntraoperative monitoring:: IntroductionWhy do we need intraoperative monitoring???Why do we need intraoperative monitoring??? To maintain the normal pt physiology & homeostasis To maintain the normal pt physiology & homeostasis
throughout anesthesia and surgery: induction, throughout anesthesia and surgery: induction, maintenance & recovery as much as possible. To maintenance & recovery as much as possible. To ensure the well being of the pt.ensure the well being of the pt.
Surgery is a very stressful condition → severe Surgery is a very stressful condition → severe sympathetic stimulation, HTN, tachycardia, sympathetic stimulation, HTN, tachycardia, arrhythmias.arrhythmias.
Most drugs used for general & regional anesthesia Most drugs used for general & regional anesthesia cause hemodynamic instability, myocardial cause hemodynamic instability, myocardial depression, hypotension & arrhythmias.depression, hypotension & arrhythmias.
Under GA the pt may be Under GA the pt may be hypohypo or or hyperventilatedhyperventilated and may develop and may develop hypothermiahypothermia..
Blood loss → anemia, hypotension. So it is necessary Blood loss → anemia, hypotension. So it is necessary to recognise when the pt is in need of blood to recognise when the pt is in need of blood transfusion transfusion (transfusion point)(transfusion point)..

Intraoperative monitoringIntraoperative monitoring:: IntroductionThe FOUR BASIC MonitorsThe FOUR BASIC Monitors:: We are NOT authorised to start a surgery in We are NOT authorised to start a surgery in
the absence of any of these monitors:the absence of any of these monitors: ECG.ECG. SpO2: arterial O2 saturation.SpO2: arterial O2 saturation. Blood Pressure: NIBP (non-invasive), IBP Blood Pressure: NIBP (non-invasive), IBP
(invasive).(invasive). ± [Capnography].± [Capnography].
The most critical 2 times during anesthesia The most critical 2 times during anesthesia are: are: INDUCTION INDUCTION - - RECOVERYRECOVERY..
Exactly like Exactly like ““flying a planeflying a plane”” induction (= induction (= take off) & recovery (= landing). The aim is to take off) & recovery (= landing). The aim is to achieve a achieve a smoothsmooth induction & a induction & a smoothsmooth recovery & a recovery & a smoothsmooth intraoperative course. intraoperative course.

(1) ECG(1) ECG

Intraoperative monitoringIntraoperative monitoring:: (1) ECG(1) ECGValueValue:: Heart rate.Heart rate. Rhythm (arrhythmias) usually best identified from Rhythm (arrhythmias) usually best identified from
lead II.lead II. Ischemic changes & ST segment analysis.Ischemic changes & ST segment analysis.Timing of ECG monitoringTiming of ECG monitoring:: Throughout the surgery: Throughout the surgery:
before induction until after extubation & recovery.before induction until after extubation & recovery.Types & connections of ECG cablesTypes & connections of ECG cables::
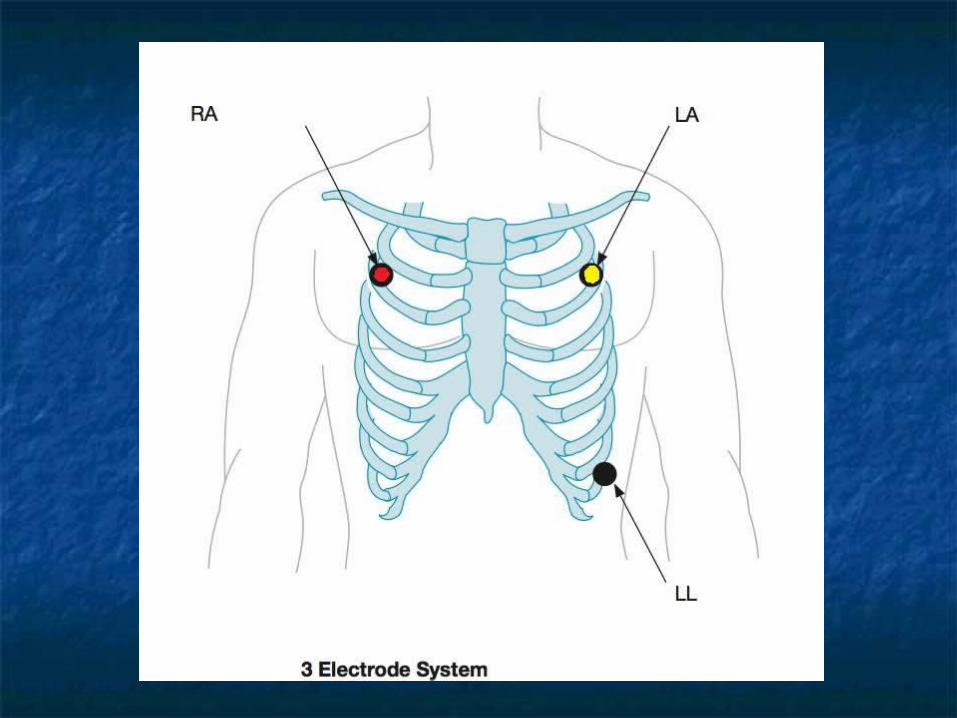
3-leads3-leads: : RRed=ed=RRight Yeight YeLLLLow=ow=LLeft eft BBlack=Alack=Appex (can read leads: I, II, III)ex (can read leads: I, II, III)
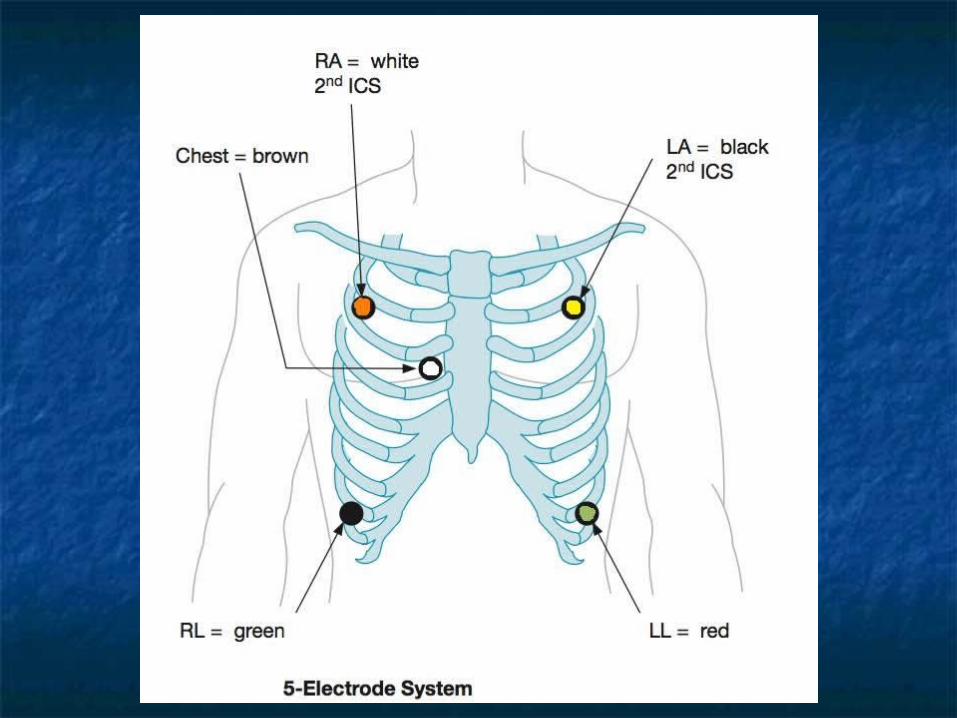
5-leads5-leads: : RRed=ed=RRight Yeight YeLLLLow=ow=LLeft eft Black=under red Green=under yellow Black=under red Green=under yellow White=central (can read any of the 12 White=central (can read any of the 12 leads: I, II, III, avR, avL, avF, V1-V6).leads: I, II, III, avR, avL, avF, V1-V6).
Intraoperative monitoringIntraoperative monitoring:: (1) ECG(1) ECG How to attach ECG electrodes:How to attach ECG electrodes:
Choose a Choose a bony prominencebony prominence. Avoid fatty regions. Avoid fatty regions AVOID hairyAVOID hairy areas (up to shaving if required in areas (up to shaving if required in
very hairy persons).very hairy persons). Position them Position them far awayfar away from each other to give e from each other to give e
higher voltage and better gain.higher voltage and better gain. Ensure Ensure good contactgood contact with the skin: by using KY- with the skin: by using KY-
Gel.Gel. If the electrodes will not be accessible during the If the electrodes will not be accessible during the
surgery (eg. on the back in thyroidectomy or surgery (eg. on the back in thyroidectomy or breast surgery) or will be soaked in betadine (eg. breast surgery) or will be soaked in betadine (eg. in abdominal surgery) after ensuring good ECG in abdominal surgery) after ensuring good ECG trace cover the stickers with adhesive tape.trace cover the stickers with adhesive tape.
Intraoperative monitoringIntraoperative monitoring:: (1) ECG(1) ECGIf the EGC gives no trace (noise If the EGC gives no trace (noise شخبطةشخبطة): follow ): follow
ECG cable from the pt to the monitor:ECG cable from the pt to the monitor: Ensure good contact with the pt: non-hairy Ensure good contact with the pt: non-hairy
areas, apply KY-Gel, search for slipped or areas, apply KY-Gel, search for slipped or loose electrodes.loose electrodes.
Ensure proper fitting of cable connections. Ensure proper fitting of cable connections. (Sometimes we apply alcohol to dissolve (Sometimes we apply alcohol to dissolve betadine).betadine).
Ensure proper fitting of the cable to the Ensure proper fitting of the cable to the monitor.monitor.
Change monitor settings: try different leads (I, Change monitor settings: try different leads (I, II, III, avR, avR, avL, V1-6), filter, size II, III, avR, avR, avL, V1-6), filter, size (amplitude) of ECG.(amplitude) of ECG.
Ensure earthing of the monitor (earth cable Ensure earthing of the monitor (earth cable from behind). from behind). األرضي األرضي سلك سلك
Intraoperative monitoringIntraoperative monitoring:: (1) ECG(1) ECG RULESRULES::
QRS QRS beep ONbeep ON must be heard at all must be heard at all times. NO silent monitors.times. NO silent monitors.
Remember that your Remember that your clinical clinical judgementjudgement is much more superior is much more superior to the monitor. Check peripheral to the monitor. Check peripheral pulsations.pulsations.
Cautery → artefacts & fallacies in Cautery → artefacts & fallacies in ECG (noise/ electrical interference) → ECG (noise/ electrical interference) → check radial (peripheral) pulsations.check radial (peripheral) pulsations.
Arrythmias → check radial Arrythmias → check radial (peripheral) pulsations.(peripheral) pulsations.

(2) SpO(2) SpO22

Intraoperative monitoringIntraoperative monitoring:: (2) (2) SpO2SpO2 It is the most important monitor. It gives a LOT of It is the most important monitor. It gives a LOT of
information about the pt.information about the pt. DefinitionDefinition: : % of oxy-Hb% of oxy-Hb / / oxy + deoxy-Hboxy + deoxy-Hb.. TimingTiming of SpO2 monitoring: of SpO2 monitoring: throughout the throughout the
surgery: before induction till after extubation & surgery: before induction till after extubation & recovery. It is the recovery. It is the LASTLAST monitor to be removed off monitor to be removed off the pt before the pt is transferred outside the the pt before the pt is transferred outside the operating room to recovery room. SpO2 operating room to recovery room. SpO2 monitoring should be continued in recovery room.monitoring should be continued in recovery room.
Waveform of pulse oximeter = Waveform of pulse oximeter = plethysmographyplethysmography (arterial waveform). It indicates that the pulse (arterial waveform). It indicates that the pulse oximeter is reading the arterial O2 saturation. oximeter is reading the arterial O2 saturation. Without the waveform pulse oximeter readings are Without the waveform pulse oximeter readings are unreliable & incorrect.unreliable & incorrect.

Intraoperative monitoringIntraoperative monitoring:: (2) (2) SpO2SpO2 ValueValue::
SpO2SpO2: arterial O2 saturation (oxygenation of the : arterial O2 saturation (oxygenation of the pt).pt).
HRHR.. Peripheral perfusion statusPeripheral perfusion status (loss of waveform (loss of waveform
in hypoperfusion states: hypotension & cold in hypoperfusion states: hypotension & cold extremeties).extremeties).
Gives an idea about the Gives an idea about the rhythmrhythm from the from the plethysmography wave (arterial waveform). plethysmography wave (arterial waveform). (Cannot identify the type of arrhythmia but can (Cannot identify the type of arrhythmia but can recognize if irregularity is present).recognize if irregularity is present).
Cardiac arrest.Cardiac arrest. N.B. Pulse oximeter tone changes with N.B. Pulse oximeter tone changes with
desaturation from high pitched to low desaturation from high pitched to low pitched (deep sound). So just by listening to pitched (deep sound). So just by listening to the monitor you can recognize: the monitor you can recognize: (1)(1) HR HR (2) (2) O2 saturationO2 saturation..

Intraoperative monitoringIntraoperative monitoring:: (2) (2) SpO2SpO2 How to attach/apply saturation probe:How to attach/apply saturation probe:
To the To the fingerfinger or or toetoe (if finger is not (if finger is not accessible). The red light is applied to the accessible). The red light is applied to the nail. Nail polish and stains should be nail. Nail polish and stains should be removed → false readings and artefacts.removed → false readings and artefacts.
Can also be applied to the Can also be applied to the ear lobeear lobe.. In infants and children can be applied to In infants and children can be applied to
2 fingers or to the hand.2 fingers or to the hand. Usually attached to the limb with the IV Usually attached to the limb with the IV
line (opposite the limb with the blood line (opposite the limb with the blood pressure cuff).pressure cuff).

Intraoperative monitoringIntraoperative monitoring:: (2) (2) SpO2SpO2ReadingsReadings:: Normal person on room air (O2 = Normal person on room air (O2 =
21%) ˃ 21%) ˃ 96%.96%. Patient under GA (100% O2) =Patient under GA (100% O2) = 98-98-
100%.100%. It is not accepted for O2 saturation to It is not accepted for O2 saturation to
↓ below ↓ below 96%96% with 100% O2 under with 100% O2 under GA. Must search for a cause.GA. Must search for a cause.
< 90%< 90% = hypoxemia. = hypoxemia. < 85%< 85% = severe hypoxemia. = severe hypoxemia.

Intraoperative monitoringIntraoperative monitoring:: (2) (2) SpO2SpO2 Fallacies & Inaccuracies occur when:Fallacies & Inaccuracies occur when:
Misplaced on the pts finger, slipped.Misplaced on the pts finger, slipped. Pt movement, shivering.Pt movement, shivering. Poor tissue perfusion (cold extremities) → Poor tissue perfusion (cold extremities) →
warm the pt, put a glove filled with warm warm the pt, put a glove filled with warm water in the pts hand (always avoid water in the pts hand (always avoid hypothermia).hypothermia).
Poor tissue perfusion (hypotension & Poor tissue perfusion (hypotension & shock).shock).
Cardiac arrest.Cardiac arrest. Sometimes by electrical interference from Sometimes by electrical interference from
cautery in some monitors.cautery in some monitors.

Intraoperative monitoringIntraoperative monitoring:: (2) (2) SpO2SpO2RULES:RULES: Keep the Keep the soundsound of the pulse oximeter of the pulse oximeter ONON
at ALL times.at ALL times. Pay attention to the sound of the pulse Pay attention to the sound of the pulse
oximeter. oximeter. NO silentNO silent monitors. monitors. ALWAYS Remember that your ALWAYS Remember that your clinical clinical
judgementjudgement is much more superior to the is much more superior to the monitor. Check pt colour for cyanosis: lips, monitor. Check pt colour for cyanosis: lips, nails.nails.
If hypoxemia occurs immediately check If hypoxemia occurs immediately check the correct the correct position of the probeposition of the probe on the on the pt and check the pts pt and check the pts colourcolour: nails & lips, : nails & lips, then manage accordingly & then manage accordingly & CALL 4 HELPCALL 4 HELP..

(3) Blood Pressure(3) Blood Pressure

Intraoperative monitoringIntraoperative monitoring:: (3) BP(3) BP NIBPNIBP:: (non-invasive ABP monitoring = automated). (non-invasive ABP monitoring = automated).
Gives readings for: systolic BP, diastolic BP & MAP: Gives readings for: systolic BP, diastolic BP & MAP: Systolic/ diastolic (mean).Systolic/ diastolic (mean).
ValueValue:: to avoid and manage extremes of to avoid and manage extremes of hypotension & HTN. hypotension & HTN. SystolicSystolic BP- BP-DiastolicDiastolic BP- BP- MAPMAP..
Avoid ↓ MAP Avoid ↓ MAP < 60 mmHg< 60 mmHg (for (for cerebralcerebral & & renalrenal perfusion) & avoid ↓ perfusion) & avoid ↓ diastolic pressure < 50 diastolic pressure < 50 mmHgmmHg (for (for coronarycoronary perfusion). perfusion).
Risks of HTN episodes: → (CVS): myocardial Risks of HTN episodes: → (CVS): myocardial ischemia, pulmonary edema, (CNS): hemorrhagic ischemia, pulmonary edema, (CNS): hemorrhagic stoke, hypertensive encephalopathy. While stoke, hypertensive encephalopathy. While hypotensive episodes: (CVS): myocardial ischemia, hypotensive episodes: (CVS): myocardial ischemia, (CNS): ischemic stroke, hypoperfusion state (CNS): ischemic stroke, hypoperfusion state metabolic acidosis, delayed recovery, renal metabolic acidosis, delayed recovery, renal shutdown.shutdown.
Intraoperative monitoringIntraoperative monitoring:: (3) BP(3) BP Timing of BP monitoringTiming of BP monitoring: throughout : throughout
the surgery: the surgery: before inductionbefore induction till till after after extubation & recovery. extubation & recovery.
Frequency of measurementFrequency of measurement:: By default every By default every 55 minutes. minutes. Every Every 33 minutes: immediately after spinal minutes: immediately after spinal
anesthesia, in conditions of hemodynamic anesthesia, in conditions of hemodynamic instability, during hypotensive anesthesia.instability, during hypotensive anesthesia.
Every Every 1010 minutes: eg. In awake pts under minutes: eg. In awake pts under local anesthesia: “local anesthesia: “monitored anesthesia monitored anesthesia carecare” (minimal hemodynamic changes).” (minimal hemodynamic changes).

Intraoperative monitoringIntraoperative monitoring:: (3) BP(3) BPHow to attach/applyHow to attach/apply:: Correct cuff sizeCorrect cuff size: width of the cuff should be : width of the cuff should be 1.5 1.5 times times
limblimb diameterdiameter and should occupy at least and should occupy at least 2/32/3 of the arm. of the arm. 2 cuff sizes for adult: 2 cuff sizes for adult: blueblue: for most adult individuals (60-90 : for most adult individuals (60-90
Kg), Kg), redred: for morbid obese.: for morbid obese. Selection of appropriate cuff size is important because a Selection of appropriate cuff size is important because a
titighght cufft cuff leads to leads to false hifalse highgh readings, while a readings, while a LLoose cuffoose cuff gives gives false false LLowow readings. readings.

Is better applied directly to the Is better applied directly to the armarm (remove (remove sleeve). May also be applied to the sleeve). May also be applied to the forearmforearm in in very obese individuals. May be applied to the very obese individuals. May be applied to the calfcalf if the arms are not accessible during surgery.if the arms are not accessible during surgery.
Correct positioningCorrect positioning: cuff is positioned with the : cuff is positioned with the hoses over the hoses over the brachial arterybrachial artery..
Usually attached to the limb opposite the IV line Usually attached to the limb opposite the IV line & pulse oximeter. Unless the pt is performing & pulse oximeter. Unless the pt is performing hand or arm or breast surgery, the BP cuff is hand or arm or breast surgery, the BP cuff is attached with the IV line and saturation probe on attached with the IV line and saturation probe on the same side.the same side.
AVOIDAVOID attaching it to an arm with A-V graft (for attaching it to an arm with A-V graft (for renal dialysis) → damage of AV graft, & renal dialysis) → damage of AV graft, & inaccurate measurements.inaccurate measurements.
Intraoperative monitoringIntraoperative monitoring:: (3) BP(3) BPReading Error/failureReading Error/failure:: Pressure line is disconnected.Pressure line is disconnected. Leakage from damaged cuff.Leakage from damaged cuff. Line is compressed (under Line is compressed (under
someone’s foot or under a weal).someone’s foot or under a weal). Line contains water from washing!Line contains water from washing! Monitor error: cuff cannot inflate due Monitor error: cuff cannot inflate due
to infant or neonate limits.to infant or neonate limits.
Intraoperative monitoringIntraoperative monitoring:: (3) BP(3) BPRULERULE:: YOUR YOUR clinical judgementclinical judgement is always superior to the is always superior to the
monitor. Must check monitor. Must check peripheral pulse volumeperipheral pulse volume from time to time (Radial A, or Dorsalis Pedis A, or from time to time (Radial A, or Dorsalis Pedis A, or Superficial Temporal A) regularly every 10 minutes.Superficial Temporal A) regularly every 10 minutes. Palpation of Palpation of Radial ARadial A → systolic BP → systolic BP ˃ 90˃ 90 mmHg. mmHg. Palpation of Palpation of Dorsalis Pedis ADorsalis Pedis A → systolic BP → systolic BP ˃ 80˃ 80
mmHg.mmHg. Palpation of Palpation of Superficial Temporal ASuperficial Temporal A → systolic BP → systolic BP
˃ ˃ 8080 mmHg. mmHg. i.e If Radial A pulsations are lost = systolic BP is < i.e If Radial A pulsations are lost = systolic BP is <
90 mmHg.90 mmHg. If dorsalis pedis & superficial temporal pulsations If dorsalis pedis & superficial temporal pulsations
are lost = systolic BP is < 80 mmHg.are lost = systolic BP is < 80 mmHg. Check pt colour for Check pt colour for pallorpallor: lips, tongue, nails, : lips, tongue, nails,
conjunctiva.conjunctiva.

Intraoperative monitoringIntraoperative monitoring:: (3) BP(3) BPIBPIBP: (invasive arterial blood pressure monitoring): (invasive arterial blood pressure monitoring) It is It is beat to beatbeat to beat monitoring of ABP via an monitoring of ABP via an arterial arterial
cannula.cannula. Indicated in: major surgeries, during deliberate Indicated in: major surgeries, during deliberate
hypotensive anesthesia, during the use of hypotensive anesthesia, during the use of inotropes, cardiac surgery, in surgeries involving inotropes, cardiac surgery, in surgeries involving extreme hemodynamic changes/instability eg. extreme hemodynamic changes/instability eg. pheochromocytoma, repeated ABG sampling.pheochromocytoma, repeated ABG sampling.

(4) Capnography (CO2)(4) Capnography (CO2)
Intraoperative monitoringIntraoperative monitoring:: (4) CO2(4) CO2 DefinitionDefinition::
What is Capnography?What is Capnography? Continuous CO2 measurement Continuous CO2 measurement
displayed as a displayed as a waveformwaveform sampled sampled from the patient’s airway during from the patient’s airway during ventilation.ventilation. What is EtCO2?What is EtCO2?
A A pointpoint on the capnogram. It is the on the capnogram. It is the final measurement at the endpoint of final measurement at the endpoint of the pts expiration before inspiration the pts expiration before inspiration begins again. It is usually the highest begins again. It is usually the highest CO2 measurement during ventilation.CO2 measurement during ventilation.

Intraoperative monitoringIntraoperative monitoring: : (4) CO2(4) CO2 Phases of the capnogram:Phases of the capnogram:
Balseline: Balseline: A-BA-B Upstroke: Upstroke: B-CB-C Plateau: Plateau: C-DC-D End-tidal: End-tidal: point Dpoint D DownstrokeDownstroke
Intraoperative monitoringIntraoperative monitoring:: (4) CO2(4) CO2 Normal rangeNormal range: : 30-35 mmHg30-35 mmHg. (Usually . (Usually
lower than arterial PaCO2 by lower than arterial PaCO2 by 5-6 mmHg5-6 mmHg due to dilution by dead space ventilation).due to dilution by dead space ventilation).
ValueValue (data gained from capnography & (data gained from capnography & ETCO2):ETCO2):
ETTETT: esophageal intubation.: esophageal intubation. VentilationVentilation: hypo & hyperventilation, curare : hypo & hyperventilation, curare
cleft (spontaneous breathing trials).cleft (spontaneous breathing trials). Pulmonary perfusionPulmonary perfusion: pulmonary embolism.: pulmonary embolism. Breathing circuitBreathing circuit: disconnection, kink, : disconnection, kink,
leakage, obstruction, unidirectional valve leakage, obstruction, unidirectional valve dysfunction, rebreathing, exhausted soda lime.dysfunction, rebreathing, exhausted soda lime.
Cardiac arrestCardiac arrest:: adequacy of resuscitation adequacy of resuscitation during cardiac arrest, and prognostic value during cardiac arrest, and prognostic value (outcome after cardiac arrest).(outcome after cardiac arrest).

Intraoperative monitoringIntraoperative monitoring:: (4) CO2(4) CO2Factors affecting EtCO2: what ↑ what Factors affecting EtCO2: what ↑ what
↓ EtCO2?↓ EtCO2?

Individual System Individual System MonitoringMonitoring
Position of ETT.Position of ETT. Respiratory System.Respiratory System. CVS & Hemodynamic Monitoring.CVS & Hemodynamic Monitoring. CNS: Awareness.CNS: Awareness. Temperature.Temperature. Monitoring after Extubation & Monitoring after Extubation &
Recovery.Recovery.
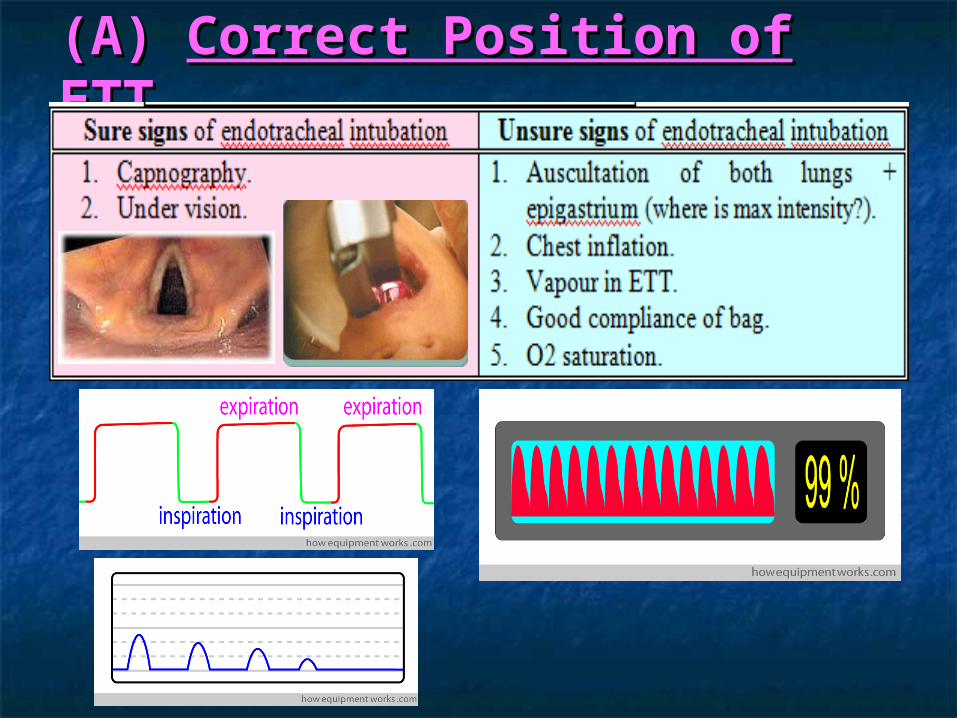
(A) (A) Correct Position of ETTCorrect Position of ETT


(A) (A) Correct Position of ETTCorrect Position of ETT After intubation Auscultation MUST be done in 5 After intubation Auscultation MUST be done in 5
areas:areas:►► Rt & Lt infraclavicular.Rt & Lt infraclavicular.►► Rt & Lt axillary.Rt & Lt axillary.►► EPIGASTRIUMEPIGASTRIUM: to exclude esophageal intubation.: to exclude esophageal intubation.
We MUST ALWAYS auscultate the chest after We MUST ALWAYS auscultate the chest after intubation for:intubation for:(1)(1) Equal air entryEqual air entry: to exclude endobronchial : to exclude endobronchial intubation.intubation.(2)(2) Adventitious soundsAdventitious sounds: wheezes, crepitations, : wheezes, crepitations, pulmonary edema.pulmonary edema.
We MUST ALWAYS auscultate the chest AGAIN We MUST ALWAYS auscultate the chest AGAIN after after repositioningrepositioning to exclude: to exclude: InwardInward displacement → endobronchial intubation. displacement → endobronchial intubation. OutwardOutward displacement → slippage & accidental displacement → slippage & accidental
extubation.extubation.

(B) (B) Respiratory MonitoringRespiratory Monitoring Clinical monitoringClinical monitoring::
Colour: Colour: cyanosiscyanosis: nails, lips, palms, : nails, lips, palms, conjunctiva.conjunctiva.
Chest rise & fall (Chest rise & fall (inflationinflation).). VapourVapour in ETT (absent in ventilators in ETT (absent in ventilators
with humdifiers/if filter is used).with humdifiers/if filter is used). Airway pressureAirway pressure.. Ventilator Ventilator bellowsbellows (return to full inflation (return to full inflation
during expiratory phase).during expiratory phase). Ventilator Ventilator soundsound: during resp cycle. : during resp cycle.
Abnormal sounds eg. leakage, Abnormal sounds eg. leakage, disconnection, high airway pressure, disconnection, high airway pressure, alarms.alarms.

(B) (B) Respiratory MonitoringRespiratory Monitoring N.B. Various alarms by the ventilator:N.B. Various alarms by the ventilator:NEVER ignore an alarm by the ventilator!NEVER ignore an alarm by the ventilator!
Low airway pressureLow airway pressure: leakage, : leakage, disconnection.disconnection.
High airway pressureHigh airway pressure: kink, biting of the : kink, biting of the tube, bronchospasm, slipped → tube, bronchospasm, slipped → esophagus.esophagus.
Low expired tidal volumeLow expired tidal volume: leakage.: leakage. Apnea alarmApnea alarm: disconnection.: disconnection. O2 sensor failureO2 sensor failure: (unfortunately common : (unfortunately common
in many of our ventilators).in many of our ventilators). Flow sensor failureFlow sensor failure: (unfortunately : (unfortunately
common in many of our ventilators).common in many of our ventilators).
(B) (B) Respiratory MonitoringRespiratory MonitoringRespiratory MonitorsRespiratory Monitors:: O2 Saturation.O2 Saturation. Capnography EtCO2.Capnography EtCO2. Airway pressure.Airway pressure. ABG samples.ABG samples.
(C) (C) CVS Hemodynamic MonitoringCVS Hemodynamic Monitoring Clinical monitoringClinical monitoring:: ColourColour:: pallorpallor (lips, tongue, nails) = anemia, (lips, tongue, nails) = anemia,
shock.shock. Palpate Palpate peripheral pulsationsperipheral pulsations every 10 minutes every 10 minutes
(Radial A, Dorsalis pedis A, Superficial temporal (Radial A, Dorsalis pedis A, Superficial temporal A).A).
Capillary refilling timeCapillary refilling time: compress nail bed until : compress nail bed until it is blanched. After release of pressure refilling it is blanched. After release of pressure refilling should occur within 2 seconds. should occur within 2 seconds. If ˃ 5 seconds = If ˃ 5 seconds = poor peripheral perfusion/circulation.poor peripheral perfusion/circulation.
UOPUOP:: Values: it is an indicator of: Values: it is an indicator of: 1)1) good hydration good hydration 2)2) good tissue good tissue
(renal) perfusion (renal) perfusion 3)3) good renal function. [Urine is the good renal function. [Urine is the champagne of anesthetists and urologists!!].champagne of anesthetists and urologists!!].
Indications: Indications: 1)1) lengthy surgery ˃ 4 hrs lengthy surgery ˃ 4 hrs 2)2) major surgery with major surgery with major blood loss major blood loss 3)3) C-section: to monitor injury to the C-section: to monitor injury to the bladder or ureter.bladder or ureter.
Normal: 0.5-1 ml/kg/hr.Normal: 0.5-1 ml/kg/hr. When the catheter is inserted u must always note the When the catheter is inserted u must always note the
baseline urine volumebaseline urine volume at the start of operation. at the start of operation.
(C) (C) CVS Hemodynamic MonitoringCVS Hemodynamic MonitoringManagement of oliguria or anuriaManagement of oliguria or anuria:: Check that the line is not Check that the line is not kinkedkinked or or
disconnecteddisconnected.. PalpatePalpate the urinary bladder (suprapubic the urinary bladder (suprapubic
fullness), or ask the surgeon to palpate it.fullness), or ask the surgeon to palpate it. Raise BP (MAP ˃ 80 mmHg): renal perfusion.Raise BP (MAP ˃ 80 mmHg): renal perfusion. IV IV fluid challengefluid challenge.. DiureticsDiuretics.. N.B. Sometimes trendlenberg position (head N.B. Sometimes trendlenberg position (head
down) causes ↓ UOP. Reversal of this down) causes ↓ UOP. Reversal of this position results in immediate flow of urine.position results in immediate flow of urine.
(C) (C) CVS Hemodynamic MonitoringCVS Hemodynamic Monitoring
CVS MonitorsCVS Monitors:: ECG.ECG. Blood pressure (NIBP, IBP).Blood pressure (NIBP, IBP). Central Venous Pressure: value: Central Venous Pressure: value:
indicator of:indicator of:1)1) IV volume.IV volume.2)2) RV function.RV function.

(D) (D) CNSCNS: Awareness: AwarenessClinical monitoringClinical monitoring::Signs of pt awareness:Signs of pt awareness: Movement, grimacing (facial expression).Movement, grimacing (facial expression). Pupils dilated.Pupils dilated. Lacrimation.Lacrimation. Tachycardia.Tachycardia. HTN.HTN. SweatingSweating:: is always an is always an alarming/warning signalarming/warning sign. .
Causes:Causes: Awareness.Awareness. Hypoglycemia.Hypoglycemia. Hypercapnia.Hypercapnia. Thyroid storm (thyrotoxic crisis).Thyroid storm (thyrotoxic crisis). Fever.Fever.
Always check the Always check the concentration of ur vaporizerconcentration of ur vaporizer & & make sure that ur make sure that ur vaporizer is not emptyvaporizer is not empty (below (below minimum = gives a concentration lower than minimum = gives a concentration lower than adjusted).adjusted).

(E) (E) Temperature MonitoringTemperature Monitoring Clinical monitoringClinical monitoring: ur hands.: ur hands. MonitorsMonitors: temperature probe: : temperature probe:
nasopharyngeal, esophageal.nasopharyngeal, esophageal. AVOID hypothermiaAVOID hypothermia < 36< 36ooCC. Why? & How?. Why? & How? Especially in Especially in pediatricspediatrics & & geriatricsgeriatrics
(extremes of age).(extremes of age). WhyWhy is it necessary to avoid hypothermia? is it necessary to avoid hypothermia?
(complications of hypothermia):(complications of hypothermia): Cardiac arrhythmias: VT & cardiac arrest.Cardiac arrhythmias: VT & cardiac arrest. Myocardial depression.Myocardial depression. Delayed recovery (delays drug metabolism).Delayed recovery (delays drug metabolism). Delayed enzymatic drug metabolism.Delayed enzymatic drug metabolism. Metabolic acidosis (tissue hypoperfusion → anerobic Metabolic acidosis (tissue hypoperfusion → anerobic
glycolysis → lactic acidosis) & hyperkalemia.glycolysis → lactic acidosis) & hyperkalemia. Coagulopathy.Coagulopathy.

(E) (E) Temperature MonitoringTemperature MonitoringHow to avoid hypothermiaHow to avoid hypothermia:: Warm IV fluids.Warm IV fluids. Intermittently switching off air-Intermittently switching off air-
conditioning esp. towards the conditioning esp. towards the end of surgery (end of surgery (↑ ambient room ↑ ambient room temptemp).).
Pediatrics: warming blanket.Pediatrics: warming blanket.

(F) (F) Monitoring After Extubation & Monitoring After Extubation & RecoveryRecovery After extubationAfter extubation: immediately : immediately fitfit the the face maskface mask
on the pt (with a slight chin lift) and observe the on the pt (with a slight chin lift) and observe the breathing bag:breathing bag: Good regular breathing with adequate tidal volume Good regular breathing with adequate tidal volume
transmitted to the bag.transmitted to the bag. No transmission to the bag → No transmission to the bag → respiratory obstructionrespiratory obstruction
(improve ur support), or (improve ur support), or apneaapnea (attempt to awaken ur pt (attempt to awaken ur pt by painful stimulus or jaw thrust).by painful stimulus or jaw thrust).
BPBP:: within 20% of baseline. within 20% of baseline. SpO2SpO2: ˃ 92%: ˃ 92% BreathingBreathing: regular, adequate tidal volume.: regular, adequate tidal volume. Muscle powerMuscle power: sustained head elevation for 5 : sustained head elevation for 5
seconds, good hand grip, tongue protrusion.seconds, good hand grip, tongue protrusion. Level of consciousnessLevel of consciousness: fully conscious = 1) : fully conscious = 1)
obeying orders, 2) eye opening, 3) purposeful obeying orders, 2) eye opening, 3) purposeful movement.movement.
MOST IMP: Pt MUST be able to MOST IMP: Pt MUST be able to protect his own protect his own airwayairway..

To SummarizeTo Summarize::““How do I monitor the patient in OR?”How do I monitor the patient in OR?”The 4 basic monitors displayed on the The 4 basic monitors displayed on the
screen:screen:1)1) ECG.ECG.2)2) BP.BP.3)3) SpO2.SpO2.4)4) ± Capnogram ± Capnogram (EtCO2).(EtCO2).

Normal target values for an adult under Normal target values for an adult under GAGA::
HRHR:: 60-90 (˃ 90 = tachycardia. < 60 60-90 (˃ 90 = tachycardia. < 60 = bradycardia).= bradycardia).
BPBP:: 90/60 – 140/90. MAP ˃ 60 90/60 – 140/90. MAP ˃ 60 mmHg (cerebral & renal mmHg (cerebral & renal autoregulation). Diastolic BP ˃ 50 autoregulation). Diastolic BP ˃ 50 mmHg (coronary perfusion mmHg (coronary perfusion pressure).pressure).
SpO2SpO2 ˃ 96% on 100% O2. ˃ 96% on 100% O2. EtCO2EtCO2 = 30-35 mmHg. = 30-35 mmHg.
LISTENLISTEN ListenListen to the monitor to the monitor the whole timethe whole time::
To the To the pulse oximeterpulse oximeter tone to identify: tone to identify: 1-1-Heart rateHeart rate 2- 2- O2 saturationO2 saturation from the from the tone (pitch) of pulse oximeter.tone (pitch) of pulse oximeter.
To the sound of the To the sound of the ventilatorventilator, to any , to any abnormal sounds, any alarms.abnormal sounds, any alarms.
RULERULE:: NO silentNO silent monitors. monitors. ALWAYSALWAYS keep the keep the HR sound onHR sound on. If ur monitor is . If ur monitor is silent (sound is not working) u have to silent (sound is not working) u have to look at your monitor the WHOLE time.look at your monitor the WHOLE time.

XX NEVER XXXX NEVER XX
LLööööKK Every Every 55 minutes minutes to note the new to note the new
BP reading.BP reading. If there is any If there is any change in the tonechange in the tone
of the pulse oximeter.of the pulse oximeter. If there is any If there is any irregularity in irregularity in
heart rateheart rate & during the use of & during the use of diathermy.diathermy.
Clinical CheckClinical Check / / 1010 minutesminutes 1)1) Chest inflationChest inflation..
2)2) Ventilator bellowsVentilator bellows: descend and return to : descend and return to become fully inflated.become fully inflated.
3)3) Airway pressureAirway pressure..4)4) Palpate Palpate peripheral pulsationsperipheral pulsations (radial A, or (radial A, or
dorsalis pedis A, or superficial temporal A):dorsalis pedis A, or superficial temporal A): For pulse volume.For pulse volume. During the use of cautery.During the use of cautery. In doubt of ECG rhythm (arrythmias).In doubt of ECG rhythm (arrythmias). In case monitor or ECG disconnected.In case monitor or ECG disconnected.
5)5) Pt Pt colourcolour (nails): cyanosis, pallor. (nails): cyanosis, pallor.6)6) VaporizerVaporizer::
a)a) Check Check concentrationconcentration opened.opened.b)b) LevelLevel of the volatile agent (if needs to be filled). of the volatile agent (if needs to be filled).

RULESRULES NEVER to FORGET: NEVER to FORGET: NeverNever start induction with a missing monitor: start induction with a missing monitor:
ECG, BP, SpO2.ECG, BP, SpO2. NeverNever remove any monitors before extubation & remove any monitors before extubation &
recovery.recovery. NEVERNEVER ignore an alarm by the ventilator. ignore an alarm by the ventilator. ALWAYSALWAYS remember than ur remember than ur clinical senseclinical sense & &
judgement is better than & superior to any judgement is better than & superior to any monitor. U are a doctor u are not a robot. The monitor. U are a doctor u are not a robot. The monitor is present to help u not to be ignored and monitor is present to help u not to be ignored and not to cancel ur brain.not to cancel ur brain.
Last but by no means least:Last but by no means least: ALWAYSALWAYS remember that there is NO such thing remember that there is NO such thing
as as ““all monitors disconnected”all monitors disconnected” →→ check that ur check that ur pt is pt is ALIVEALIVE!! Immediately check !! Immediately check peripheralperipheral & & carotid pulsationscarotid pulsations to make sure that ur pt is not to make sure that ur pt is not ARRESTEDARRESTED!! Once u have ensured pt safety !! Once u have ensured pt safety reattach ur monitors once again.reattach ur monitors once again.



















