Intraluminal Wire Retrieval of a Proximally Migrated Pediatric Double-J Ureteral Stent
2
Vol. 164,223424, July 1996 Rid in USA INTRALUMINAL WIRE RETRIEVAL OF A PROXIMALLY MIGRATED PEDIATRIC DOUBLE-J URETERAL STENT ROGER K. Low, BARRY A. KOGAN AND MARSHALL L. STOLLER* From the Department of Urn&, University of California School of Medicine, San Francisco, California W3RD8: ureter, stents, bladder Retrieval of a Proximally figrated Doub1eJ-t ureteral stent can be frustrating and technidy challenging. Numer- ous stent extraction devices and ureteroscopic techniques with or without fluorompic guidance have been described in The small pediatric urethral and ureteral caliber limits endoscopic instrumentation. We describe a minimally invasive technique using stent luminal Wire insertion and misplaced ureteral stent in a 10-year-oldboy. (part B of figure). Subsequent manual caudal renal displace- ment further advanced the distal stent 1 cm. into the bladder (part C of m). me @de wire was removed and a plain film of the kidneys, ureters and bladder verified proper stat length and position. manual caudal renal displacement to retrieve a proximally DISCUSSION Improper proximal placement of Double4 stents is due to excessive stent advancement or, infrequently, proximal stent CASE HISTORY migration. Proximal stent migration is most often due to and pas- badequate Stat length. Once the stent is advanced p rohd sage of gravel per u r e t h m . Diagnostic excretow ~ ~ a p h y to the ureteral orifice stent retraction or removal is required and nuclear renal scanning revealed multiple left renal cal- since it will cause obstruction and renal drain- culi and left ureteropelvic junction obstruction. &r retm We. migration into the bladder is unlibely due grade endo-pyelotomy using the AcuciseS endo-pyelotomy to the acute stent* catheter a 7F 20 cm. Double4 ureteral catheter was fluor+ Endoscopidy scopically positioned into the left renal pelvis. The 4F work- are hue& BucceBBfuI, Obviating the need for ing channel of the 14F pediatric cystoscope prevented sknt open Grasping forceps, biopsy forceps, hooks, placement under direct vision. Subsequently, cystoscopic in- stone baskets and loops have been described to retrieve sue- spection of the bladder identified improper proximal stent cessmy prowJ’ ureteral balloon d& lating devices and Fogarty catheters placed within the stent position (part A of figure). semirigid ureteroscope in the intramural ureter. Attempts at adults.6-8 Placement with retrieval sutures of varying graspers and alligator forceps were unsuccessful. ultimately, Proper placement can be without direct en- visual guidance. The 3.6F working channel of the 8.9F uret- eroscopeadditionally restrids the size of endoscopicgrasping devices. In our me none of the available 3F grasping devices was strong enough to grasp and retract the proximally placed stent. The location of the stent witbin the intramural ureter A 10-year-old boy presented with left renal Of the distal tip Of the fluoroscopidy The distal tip of the stent was visualized with an 8.9F lumen Or a4acent to the Shnt have been reported in grasping the stent with a stone basket, 3-prong fle&le lengths may repsition Proximally stentS*9 a 0.035-inch guide wire was placed though the lumen ofthe dosmpic visualization* channels in d- stent, which straightened, extended and stiffened the stent iber endoeeoPes Prohibit Placement Of mkrd stentS under Accepted for publication December 29,1994. * y s t for reprints: Depampent.of Urology, U-518, University t Medical Engineering Corp., New York, New York. $ Applied Urology, Laguna Hills, California. of Cah oma, San Franasco, Cahfoma 94143-0738. B I C I A, proximally malpositioned Doubled stent with distal end lodged in the intramural ureter. B, after intraluminal guide wire placement. Note straightening and extension of stent through ureteral onfice (arrow). C, advancement of stent into bladder (small arrow) after straightening it with guide wire and subsequent manual caudal renal displacement (large arrow). 223
-
Upload
marshall-l -
Category
Documents
-
view
219 -
download
1
Transcript of Intraluminal Wire Retrieval of a Proximally Migrated Pediatric Double-J Ureteral Stent

Vol. 164,223424, July 1996 R i d in U S A
INTRALUMINAL WIRE RETRIEVAL OF A PROXIMALLY MIGRATED PEDIATRIC DOUBLE-J URETERAL STENT
ROGER K. Low, BARRY A. KOGAN AND MARSHALL L. STOLLER* From the Department of Urn&, University of California School of Medicine, San Francisco, California
W3RD8: ureter, stents, bladder
Retrieval of a Proximally figrated Doub1eJ-t ureteral stent can be frustrating and technidy challenging. Numer- ous stent extraction devices and ureteroscopic techniques with or without fluorompic guidance have been described in
The small pediatric urethral and ureteral caliber limits endoscopic instrumentation. We describe a minimally invasive technique using stent luminal Wire insertion and
misplaced ureteral stent in a 10-year-old boy.
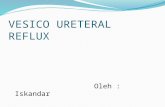
(part B of figure). Subsequent manual caudal renal displace- ment further advanced the distal stent 1 cm. into the bladder (part C of m). m e @de wire was removed and a plain film of the kidneys, ureters and bladder verified proper s t a t length and position.
manual caudal renal displacement to retrieve a proximally DISCUSSION
Improper proximal placement of Double4 stents is due to excessive stent advancement or, infrequently, proximal stent
CASE HISTORY migration. Proximal stent migration is most often due to and pas- badequate S t a t length. Once the stent is advanced p r o h d
sage of gravel per u r e t h m . Diagnostic excretow ~ ~ a p h y to the ureteral orifice stent retraction or removal is required and nuclear renal scanning revealed multiple left renal cal- since it will cause obstruction and renal drain- culi and left ureteropelvic junction obstruction. &r re tm We. migration into the bladder is unlibely due grade endo-pyelotomy using the AcuciseS endo-pyelotomy to the acute stent* catheter a 7F 20 cm. Double4 ureteral catheter was fluor+ Endoscopidy scopically positioned into the left renal pelvis. The 4F work- are hue& BucceBBfuI, Obviating the need for ing channel of the 14F pediatric cystoscope prevented sknt open Grasping forceps, biopsy forceps, hooks, placement under direct vision. Subsequently, cystoscopic in- stone baskets and loops have been described to retrieve sue- spection of the bladder identified improper proximal stent cessmy prowJ’ ureteral balloon d&
lating devices and Fogarty catheters placed within the stent position (part A of figure).
semirigid ureteroscope in the intramural ureter. Attempts at adults.6-8 Placement with retrieval sutures of varying
graspers and alligator forceps were unsuccessful. ultimately, Proper placement can be without direct en-
visual guidance. The 3.6F working channel of the 8.9F uret- eroscope additionally restrids the size of endoscopic grasping devices. In our m e none of the available 3F grasping devices was strong enough to grasp and retract the proximally placed stent. The location of the stent witbin the intramural ureter
A 10-year-old boy presented with left renal
Of the distal tip Of the fluoroscopidy
The dista l tip of the stent was visualized with an 8.9F lumen Or a4acent to the Shnt have been reported in
grasping the stent with a stone basket, 3-prong fle&le lengths may repsition Proximally stentS*9
a 0.035-inch guide wire was placed though the lumen ofthe dosmpic visualization* channels in d- stent, which straightened, extended and stiffened the stent iber endoeeoPes Prohibit Placement Of mkrd stentS under
Accepted for publication December 29,1994. * y s t for reprints: Depampent.of Urology, U-518, University
t Medical Engineering Corp., New York, New York. $ Applied Urology, Laguna Hills, California.
of Cah oma, San Franasco, Cahfoma 94143-0738.
B I C I
A, proximally malpositioned Doubled stent with distal end lodged in the intramural ureter. B , after intraluminal guide wire placement. Note straightening and extension of stent through ureteral onfice (arrow). C, advancement of stent into bladder (small arrow) after straightening it with guide wire and subsequent manual caudal renal displacement (large arrow).
223

224
prevented the proper opening of a stone basket and grasping forceps. Advancement of grasping endoscopic accessories be- yond the tip of the endoscope is required to open the working elements completely. Alternatively, the ureteroscope may be retracted to allow full dedovment of the maspina accessory.
RETRIEVAL OF MIGRATED URETERAL STENT
pediatric population. We describe a new technique using a guide wire and manual caudal renal displacement to reposi- tion successfully proximally placed stents. This technique also has proved beneficial in an adult and should be consid- ered as a minimally invasive technique in the pediatric ure-
In our case retraction placed the ureteroscope back into the bladder and we were unable to visualize the stent.
Our technique for removing a proximally placed stent proved ideal for our pediatric patient. Placement of the guide wire within the visualized lumen of the stent was minimally traumatic to the ureter. Manual caudal displacement of the kidney was facilitated by the thinness of the child. Manual displacement helped to advance the ureteral stent into the bladder after it was stiffened, straightened and lengthened with the guide wire. The stent was advanced over the guide wire or alternatively advanced with the guide wire into the bladder. This technique obviated the need for incising or dilating the ureteral orifice to allow for ureteroscopic access beyond the intramural ureter.
We also have used this technique to reposition a proximally placed ureteral stent in an adult. During placement over a guide wire a stent was inadvertently advanced proximal to the ureteral orifice. Manual caudal renal displacement while keeping the guide wire in place successfully repositioned the stent into the bladder.
CONCLUSIONS
Proximal placement or migration of ureteral stents is an uncommon occurrence in adults and is even rarer in the
ter.
REFERENCES
1. Hezmell, H. P., Flechner, S. M. and Sandler, C. M.: Controlled endoscopic retrieval of ectopic ureteral catheters using fluoro- scopic guidance. Urology, 25 613, 1985.
2. Bagley, D. H. and Huffman, J. L.: Ureteroscopic retrieval of proximally located ureteral stents. Urology, 37: 446, 1991.
3. Killeen, K. P. and Bihrle, W., 111: Ureteroscopic removal of re- tained ureteral Double4 stents. Urology, 35: 354, 1990.
4. Berman, D., Donovan, J., Assimos, D. and OConor, V. J., Jr.: Transurethral removal of migrated indwelling ureteral stents: a new technique. J . Urol., 130 765, 1983.
5. Smith, A. D.: Retrieval ofureteral stents. Urol. Clin. N. h e r . , g: 109, 1982.
6. Chin, J. L. and Denstedt, J. D.: Retrieval of proximally migrated ureteral stents. J. Urol., 148 1205, 1992.
7. Katske, F. A. and Celis, P.: Technique for removal of migrated Double-J ureteral stent. Urology, 31: 579, 1991.
8. Niendorf, D. C. and Kamhi, B.: Retrieval of indwelling ureteral stent utilizing Fogarty catheter. Urology, 6 622, 1975.
9. Collier, M. D., Jerkins, G. R., Noe, H. N. and Soloway, M. S.: Proximal stent displacement as complication of pigtail ure- teral stent. Urology, 13 372, 1979.