Intrahepatic Cholestasis of Pregnancy: What is the evidence?§ Mean IUFD rate of 1.74% § Uniform...
14
Intrahepatic Cholestasis of Pregnancy: What is the evidence? Joyce Sung, MD Associate Professor, CU MFM Objectives ➧ Diagnose intrahepatic cholestasis of pregnancy (ICP) ➧ Understand fetal, neonatal, and maternal outcomes with ICP ➧ Manage pregnancies complicated by ICP Outline ➧ Background ➧ Pathophysiology ➧ Maternal and Fetal Outcomes ➧ Delivery considerations ➧ Pharmacotherapy ➧ Fetal Monitoring ➧ Society Guidelines and proposed algorithm 3
Transcript of Intrahepatic Cholestasis of Pregnancy: What is the evidence?§ Mean IUFD rate of 1.74% § Uniform...

Intrahepatic Cholestasis of Pregnancy: What is the evidence?
Joyce Sung, MDAssociate Professor, CU MFM
Objectives
➧ Diagnose intrahepatic cholestasis of pregnancy (ICP)➧ Understand fetal, neonatal, and maternal outcomes with
ICP➧ Manage pregnancies complicated by ICP
Outline
➧ Background➧ Pathophysiology➧ Maternal and Fetal Outcomes➧ Delivery considerations➧ Pharmacotherapy➧ Fetal Monitoring➧ Society Guidelines and proposed algorithm
3

ICP - Background
➧ Incidence: 0.2-2%§ Varies with ethnicity and geography§ Most common: South America, Northern Europe
➧ Risk factors:§ Multiple pregnancy (up to 22% risk in one study!!)§ IVF – mild increase (2.7% vs 2%)§ >35 yo§ Winter months
ICP – Clinical Presentation➧ Classically third trimester (80% > 30 weeks)
§ Can happen earlier, as early as 7 weeks reported➧ Pruritus: palms/soles
§ Often worse at night§ Worsens with advancing gestation§ No specific skin findings
➧ Cholestasis:§ Dark urine§ Pale stools§ Jaundice (rare)
➧ Resolves rapidly after delivery§ Symptoms within days of delivery § LFTs 4-6 weeks
➧ Can recur with future pregnancies or OCPs§ 50-60% recurrence (If family hx, might be up to 92%)
ICP – Laboratory abnormalities
➧ Abnormal liver function: elevated transaminases§ Can occur before or after increased bile acids; doesn’t correlate§ ALT more sensitive than AST (2x-30x)
➧ Elevated bilirubin in up to 10%§ Usually mild conjugated hyperbilirubinemia
➧ Elevated serum bile acids§ Most labs upper limit of normal is 10-14 µmol/L for total serum
bile acids§ Lower if fasting (6-10 µmol/L)

ICP - Diagnosis
➧ Diagnosis of exclusion: other causes of pruritus and/or hepatic impairment➧ Most sensitive and specific marker is elevated bile acids
§ Typical pruritus + elevated bile acids➧ UK RCOG: If bile acids not available, ICP can be
diagnosed if typical pruritus + abnormal LFTs with resolution of both post-delivery
ICP:Pathophysiology
9
8/19/2019 Biochemistry Glossary: Enterohepatic Circulation | Draw It to Know It
https://www.drawittoknowit.com/course/biochemistry/glossary/physiological-process/enterohepatic-circulation 1/1
Cookie Policy
By continuing to use this website, you agree to our use of cookies as described in our Privacy Policy.
BiochemistryIntegration of Chemical & Physiologic Processes
A comprehensive approach to the chemical processes within and related to
living organisms with a special focus on topics covered on the USMLE and
COMLEX Exams. Clinical correlations are presented to integrate biochemistry
with the pathophysiologic basis of disease.
142 tutorials (19 hours)
- Academic Textbook
Organization
- 6-8 Minute Animated, Narrated
Tutorials
- Bulleted Notes & Final
Drawings
Web-based Drawing Pad
- 2800+ Drag/Drop Labels
- Downloadable Starter Images
- Precision Touch Sensitivity
1050+ Quiz Questions
- Rapid Review
250+ Clinical Correlations
- Real-Life Correlations
700+ Scienti�c References
- Sources You TrustView Plans & Start Your 1-Week Free Trial Now!
Courses/PricingInstitutional
Registration
Log
InSearch Flashcards & FAQ �
Previous Term Next Term
Biochemistry FlashcardsBack� L
Related Tutorials
Liver and Gallbladder
Enterohepatic Circulation
� Back to Course
Share this Flash Card:
`be�Let's �rst address bile secretion.
Draw the liver.
Show two hepatic ducts that extend from it that merge to form the common
hepatic duct.
Beneath the liver, draw the gallbladder.
Demarcate its cystic duct.
Show that the cystic and hepatic ducts merge to form the common bile duct.
Now, show yellowish bile in the gallbladder.
Draw a section of the duodenum (of the small intestine) and show that the
common bile duct empties into it.
Next, label the sphincter of Oddi (aka hepatopancreatic sphincter), at the
junction of the common bile duct and small intestine.
Now let's discuss how bile salts are recycled in the enterohepatic circulation system.
Draw the ileum (of the small intestine).
Draw a capillary bed, which transitions into the hepatic portal vein, which then
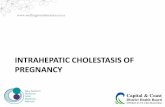
Bile Salt Recycling in Enterohepatic CirculationBile salts pass down the length of the small intestine to the ileum
Reabsorbed into circulation at the ileum (they the enter recycling pathway:
enterohepatic circulation).
Travel through the hepatic portal vein back to the liver where they are
recycled and re-secreted into newly formed bile.
Note: The hepatic portal vein drains nutrient-rich blood from the small intestine to thel f b l
Drawittoknowit.com
From Stenvall et al, Physics in Medicine & Biology, 2014; 59(13).
Overview of hepatobiliary circulation

ICP - Pathophysiology ➧ Estrogen might reduce expression of biliary transport proteins.
➧ Progesterone might act as partial agonist of FXR
➧ Genetics: mutations described in ICP:§ ABCB4 mutations: multidrug
resistance protein 3 (MDR3)§ ATP8Ba: FIC1§ ABCC2§ NR1I2: Pregnane X receptor
(PXR)§ NR1H4: farnesoid X
receptor (FXR)
Williamson and Geenes. Ob Gyn 2014.Dixon and Williamson, Clin Res Hepatology Gastroenter 2016.
ICP:Maternal and Fetal Outcomes
ICP – Maternal Outcomes
➧ Higher rates of GDM and preeclampsia§ Coexisting comorbidities might have worse fetal
prognosis➧ Higher incidence of hepatobiliary disease later in life➧ More common to have Hep C, chronic hepatitis, cirrhosis,
gallstones, cholangitis➧ Offspring at higher risk of high BMI and dyslipidemia
Williamson and Geenes (ICP Review), ObGyn 2014.

ICP – Fetal outcomes➧ Theories for mechanisms
§ sPTB➧ Rodents: dose-dependent effect of BA on myometrial contractility➧ Human myometrium: increased sensitivity and expression of oxytocin receptors
§ Meconium-stained amniotic fluid➧ Sheep: bile acids increase colonic motility (no other signs of fetal distress
§ RDS➧ Rabbits: intra-tracheal BA à atelectasis, eosinophilic infiltration, hyaline
membrane§ Reversed with surfactant
§ Stillbirth➧ ?? Autopsy: evidence acute anoxia; likely sudden acute event➧ Possible fetal arrhythmia (case reports)➧ Rats: decrease contraction rate of cardiomyocytes, develop arrhythmias➧ Vasoconstrictive effect on placental chorionic veins➧ Generally normal birthweight
Williamson and Geenes (ICP Review), ObGyn 2014.
ICP – Fetal outcomes
Studies looking at BA levels with outcomes- Glantz 2004 (Sweden)- Lee 2008 (USA; Hispanics only)- Brouwers 2014 (Netherlands)- Kawakita 2015 (USA)- Cui 2017 (Meta-analysis)- Geenes 2014- Herrera 2018
➧ Increased risks of:§ sPTL§ NRFHT§ Meconium staining of AF (MSAF)§ IUFD§ RDS (independent of PTB)
ICP – Fetal Outcomes
➧ Glantz et al 2004 ➧ Incidence ICP = 1.5% (693/45,485)➧ IUFD (3/690 = 0.4%)
§ 36w (34w), TBA 94§ Twins, 25w (24w), TBA 130§ Twins, 36w (36w), TBA 27, tight knot
None Mild Severe
Fasting TBA (µM) <10 10-39 > 40
N (690 total) 185 409 96
sPTB 2.7% 2.2% 16.7% **
Asphyxia 5.4% 6.3% 13.5% *
MSAF 21% 44% **
Mec Plac 8% 11% 25% **
*p<0.01; ** p<0.001

ICP – Fetal Outcomes – Glantz 2004 (cont’d)
➧ Fetal complications increased ~1-2% per each µM of increasing BA
sPTB
Asphyxia Mec Plac
MSAF
ICP – Fetal Outcomes➧ Lee et al 2008
§ Retrospective review, USC, Latina patients only
§ 2000-2007, Dx code of ICP, standard practice was delivery at 37w
§ TBA as categorical and continuous variable➧ ~20% increase risk of meconium passage
per each 10 µM increase in BA§ IUFD: 1 in severe ICP group
➧ Dx 12w (TBA 113, Tbili 7.9)➧ ursodiol 300 TID x 1 month (self d/c’d)➧ 30w: IUFD, TBA 60
Mild Moderate Severe p
N (122 total)
34 39 49
Bile Acids <20 20-40 >40
sPTB 2.9% 5.1% 4.1% 0.90
Meconium passage
0% 15.4 20.4 0.02
Chorio 14.7%
12.8 8.2 0.62
PPH 5.9% 10.3 4.1 0.50
Asphyxia 2.9% 2.7 2.9 0.7
IUFD 0% 0 2.0 0.47
ICP – Fetal outcomes➧ Brouwers et al, 2015
§ In Mod/Severe groups:➧ Lower GA at delivery➧ Lower BW but not SGA➧ Similar Apgar➧ sPTB➧ Meconium
§ Bile acids as continuous variable:
Mild Mod Severe P
N 108 86 21
BA µM 10-39 40-99 >100
sPTB % 2.8% 3.5 19.0 0.023
MSAF % 13.8 22.1 47.6 0.003
PPH % 2.8 12.8 9.5 0.019
Asphyxia % 2.3 0.345
Perinatal death % 9.5 0.009
NICU admit % 0.9 2.3 9.5 0.062

ICP – Fetal Outcomes➧ Kawakita et al, 2015
§ Group 1 (n=152): TBA 10-39.9 µM§ Group 2 (n=55): 40-99.0§ Group 3 (n=26): > 100
➧ Group 2+3 vs. Group 1:§ Higher PTB (not sPTB);
iatrogenic PTB; meconium; composite neonatal outcome
§ But did not remain after adjusting for iatrogenic PTB and other confounders
GA of IUFD GA of ICP TBA AST/ALT
37w1d 35w 261 à 261 54/91
35w3d 31w 106 à 509 112/124
24w1d 23w 128 37/26
35w5d 32w 57 à 114 à 36 356/424
• IUFD – 4 total
ICP – Fetal outcomes – meta-analysis
➧ Cui et al, 2017: meta-analysis of 9 observational studies that looked at level of maternal TBA (including the 4 already discussed)
➧ Mild 10.0-39.9 µM➧ Severe > 40 µM
➧ Severe ICP vs mild ICP:§ Higher PTB, MSAF,
asphyxia/RDS➧ Stillbirth (3-4 studies)
§ Severe: 10/330 (3%)§ Mild: 3/511 (0.6%)
ICP – Fetal outcomes➧ Geenes et al 2014:➧ Prospective, case-control, UK, 669
singleton severe ICP (BA > 40)§ Compared to controls:
➧ Increased PTB (25% vs 6.5%, aOR 5.39) – most were iatrogenic (~2/3)
➧ Increased NICU admission (12% vs 5.6%, aOR 3.65)
➧ Increased IUFD (1.5% vs 0.5%, aOR 2.58)§ Median GA 35 + 2 weeks; 6/10 occurred at
<37 weeks§ 7/10 had coexisting pregnancy
complications§ Higher peak bile acid levels (median 137
vs median 72)§ Within ICP group, PTB, meconium,
IUFD increased as bile acid levels increased
§ Limitations: only looked at “severe ICP”, did not include 10-39 µmol/L
PTB
MeconiumIUFD
sPTB

ICP – Fetal outcomes➧ Herrera et al 2018
§ None <10§ Mild 10-39§ Moderate 40-99§ Severe > 100
➧ Primary outcome: composite neonatal morbidity
➧ IUFDs:§ 35w, weekly testing, Max BA 47§ 23w, short cord, tight nuchal,
possible cord accident, Max BA 31§ 25w, likely due to TTTS, Max BA
118
ICP – Fetal outcomes: summary of IUFD risk➧ Incidence of ICP 0.09%, 0.35%, 1.5%➧ IUFD risk: 0.6% overall (ICP by Dx code, CA)➧ IUFD risk by BA levels
§ Severe > 100:➧ 9.5% (2/21 in Brouwers 2015, GA not specified)➧ 15% (4/26 in Kawakita 2015): 37w1d, 35w3d, 24w1d, 35w5d➧ 3% (1/32 at in mo/di twins with TTTS, Herrera 2018): 25w
§ Severe > 40: ➧ 3% (Cui et al)➧ 1.5% (Geenes 2014): 35 + 2 weeks➧ 2% (1/49 in Lee 2008): 30w➧ 0.4% (3/690 in Glantz 2004): 36w, 25w twins, 36w twins (TBA 27, tight knot)
§ Moderate (40-100)➧ 0/86 [BA 40-100] in Brouwers 2015➧ 0/55 [BA 40-100] in Kawakita 2015➧ 0.9% [BA 40-100] 1/108, Herrera 2018, 35w – normal NST 1 day prior
§ Mild ➧ 0.6% (Cui Meta-analysis)➧ 0.2% (1/347 but possible cord accident, Herrera 2018): 23w
ICP:Delivery Considerations

ICP – Delivery Timing
➧ Puljic et al, 2015➧ Retrospective cohort ➧ For each week of gestation,
determined:§ Risk of stillbirth (# of stillbirths that
week / number of ongoing pregnancies that week)
§ Risk of delivery (risk of infant death at delivery that week)
§ Composite mortality risk of expectant management for 1 additional week
ICP – Delivery timing, cont’d
ICP – Delivery timing, cont’d

ICP – Delivery Options➧ Lo et al 2015➧ Decision Analysis➧ Assumptions:
§ Mean IUFD rate of 1.74%§ Uniform distribution of IUFD rate from 34-40 weeks§ Reported NND, RDS, NEC, CP, and effect of steroids§ QALY
➧ Compared 4 options for each of 35, 36, 37, and 38 weeks§ Empiric steroids, deliver in 4h§ Amnio for FLM, if FLM neg, steroids and delivery in 48h§ Amnio for FLM, if FLM neg, wait a week and retest§ Deliver immediately
➧ For each GA week, Option 4 (deliver immediately) was always the best strategy
ICP:Pharmacotherapy and Fetal Monitoring
ICP - Pharmacotherapy
women, and some clinicians, find it reassuring to haveregular cardiotocography, fetal growth scans, or both.However, it should be noted that there are severalcase reports of normal cardiotocography in the hoursand days preceding fetal death.
Elective Early DeliveryMany authors have advocated the implementation ofelective early delivery of pregnancies with intrahepaticcholestasis of pregnancy. These policies arise from thedemonstration of a clustering of stillbirths from 37weeks of gestation onward13,75 and are aimed at reduc-ing the risk of late stillbirth. At present, the AmericanCollege of Obstetricians and Gynecologists does nothave a guideline on the management of intrahepaticcholestasis of pregnancy. The current Royal Collegeof Obstetricians and Gynecologists guideline for intra-hepatic cholestasis of pregnancy states that there is noevidence to support or refute this practice, but it nev-ertheless has been widely adopted by many clinicians;a recent population-based study from the United King-dom reported iatrogenic preterm delivery rates of17%.14 The majority of early deliveries are inducedand there is no evidence that this results in higher ratesof emergency cesarean delivery. Indeed, it has beenshown in two retrospective cohorts and one prospec-tive study that rates of operative and instrumentaldelivery are not increased in women with intrahepaticcholestasis of pregnancy after induction of labor.28,76,77
As discussed subsequently, the risk of adverseperinatal outcomes has been related to the degree ofmaternal serum bile acid elevations. Thus, some clini-cians effect delivery at 37 weeks of gestation inpregnancies complicated by intrahepatic cholestasis ofpregnancy in which bile acids reach a certain threshold(eg, 40 micromoles/L) and allow those in which thisthreshold is not met to continue to 39 weeks of gestation.We emphasize, however, that no randomized studieshave established the optimal timing for pregnanciescomplicated by intrahepatic cholestasis of pregnancy.
COMPLICATIONSIntrahepatic cholestasis of pregnancy has consistentlybeen associated with an increased incidence of adverseperinatal outcomes, including spontaneous pretermdelivery, nonreassuring fetal status, meconium stainingof the amniotic fluid, and stillbirth (Fig. 3). More recentstudies have also suggested an association with respira-tory distress syndrome that is independent of the risk ofpremature birth.78 However, there has been muchdebate in the literature regarding the precise natureof the risk to the fetus and the true incidence of theseoutcomes. This is largely the result of a lack of consen-sus on diagnostic criteria for intrahepatic cholestasis ofpregnancy and recent changes in management practi-ces, making it difficult to assess the risk fully.
The fetal complications in intrahepatic cholestasisof pregnancy are believed to relate to high levels ofbile acids in the fetal serum. The fetus can synthesize
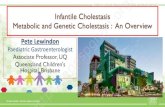
Fig. 2. Schematic showing the com-plementary effects of ursodeox-ycholic acid (orange arrows) andrifampicin (purple arrows) in thetreatment of cholestatic liver disease.Ursodeoxycholic acid enhances thecanalicular excretion of bile acidsand phosphatidylcholine by upregu-lation of BSEP and multidrug resis-tance protein (MDR) 3, respectively. Italso upregulates expression of MRP4at the basolateral membrane, facili-tating further excretion of bile acidsthrough alternative export pathways.Rifampicin enhances excretion ofbilirubin through induction of MRP2and also facilitates the conversion ofhydrophobic bile acids to morehydrophilic species through theinduction of CYP3A4. This then pro-motes bile acid excretion through thebasolateral exporter MRP3. PregnaneX receptor (PXR) is directly upregu-lated by rifampicin.Williamson. Intrahepatic Cholestasis ofPregnancy. Obstet Gynecol 2014.
VOL. 124, NO. 1, JULY 2014 Williamson and Geenes Intrahepatic Cholestasis of Pregnancy 127
➧ Ursodeoxycholic acid (UDCA) (orange)§ Increases canicular excretion of
bile acids (via BSEP and MDR3)§ Increases BA excretion via
alternative export (via MRP4)➧ Rifampicin (purple)
§ Increases BA excretion (MRP2)§ Converts hydrophobic BA to
hydrophilic, more excretion via MRP3
§ Upregulation of PXR
Williamson and Geenes, ObGyn 2014

ICP - Therapy➧ Ursodeoxycholic acid (UDCA, ursodiol, Actigall)
§ Reduces pruritus§ May improve labs: LFTs, serum bile acids§ May benefit perinatal outcomes??➧2012 Meta-analysis (limited numbers): reduced PTL, NRFHT, RDS,
NICU admit 1➧2014 Meta-analysis (12 RCTs, 662 patients): reduced pruritus, ALT,
bile acid, PTB, fetal distress, RDS, low Apgar, NICU admits, LBW, GA 2
§ Dosing: typically 200-300 mg BID-TID➧Total daily dose of 500 mg – 2000 mg (2g)/d
§ Side effects: GI upset, n/v/d1. Bacq Y. Gastroenterology 2012.2. Kong X. Medicine 2016.
ICP - Therapy➧ Rifampicin: antibiotic with choleretic properties: enhanced bile acid
detoxification and excretion§ No RCTs; some cases of helping in patients refractory to ursodiol
➧ Cholestyramine: anion exchange resin§ May reduce pruritus, but doesn’t help labs§ Not first-line since reduces intestinal absorption of ursodiol, fat-
soluble vitamins à increased risk of PPH➧ S-adenosyl-L-methionine
§ Effect on hepatic membrane composition§ Inconsistent reports: ?helps symptoms and bioehcm§ Twice daily IV administration – not used much
ICP - Therapy
➧ Antihistamines:§ For pruritus, inducing drowsiness§ No effect on labs
➧ Oral vitamin K: for theoretical risk of malabsorption, no RCTs to support➧ Topical emollients:
§ Aqueous cream with menthol

ICP – Fetal monitoring
➧ Antenatal testing:§ No evidence that this is helpful§ Not listed in ACOG’s Antepartum Fetal Surveillance
(PB#145, 2014)§ Case reports of normal NSTs in hours and days
preceding IUFD➧ Growth scans:
§ No evidence of benefit§ Generally not associated with SGA
ICP:Society GuidelinesProposed Algorithm
ICP – What do societies say?➧ Societies with independent guidelines for ICP:
§ 2016 ACG (American College of Gastroenterology)§ 2011 RCOG (Royal College of Obstetricians and
Gynecologists)§ 2011 SMFM (Society for Maternal Fetal Medicine)§ 2009 EASL (European Association for the Study of the Liver)§ 2016 SAMNCP (South Australian Maternal and Neonatal
Community of Practice)§ 2014 GWADOH (Gov’t of W Australia Dept of Health)
Bicocca 2018

ICP – Society Guidelines
➧ Diagnosis:§ RCOG: ➧Pruritus required➧ If GGT, bile acids, or LFTs elevated, these are diagnostic➧Elevated bile acids not required➧Must have resolution postpartum
§ SMFM and ACG:➧Pruritus required, resolves with delivery➧>10 µM diagnostic
Bicocca 2018
ICP – Society GuidelinesVariable RCOG ACG SMFM
Lab evaluation
Bile acids Y Y Y
LFTs Y Y Maybe
GGT Y -- --
Follow-up? Weekly LFTs.PT/PTT if LFTs rapidly increase.
US to r/u cholelithiasis --
Antenatal testing
-- -- Y (insufficient evidence)
Delivery Timing
37 weeks (offer) 37 37-38; sooner with documented pulmonary maturity
Medical management
UDCA: no dosing info.Vit K if prolonged PT
UDCA 10-15 mg/kg/dConsider dexa for risk of PTB
UDCA start at 300 mg BID.Max 600 mg BID
Postpartum Care
No hormonal contraception.Repeat LFTs in 6 weeks
Work-up if symptoms persist Hormonal contraception OK. BF ok.Workup if symptoms persist.
Bicocca 2018
ICP – CU MFM (Proposed) Algorithm

References➧ Dixon P and Williamson C. The pathophysiology of ICP. Clinics and Research in Hepatology
and Gastroenterology, 2016; 40:141-153.➧ Williamson C and Geenes V. Clinical Expert Series: ICP. Ob Gyn 2014; 124(1):120-133.➧ Glantz A et al. ICP: Relationships between bile acid levels and fetal complication rates.
Hepatology 2004; 40(2):467-474.➧ Lee R et al. Pregnancy outcomes during an era of aggressive management for ICP. Am J
Perinatol 2008; 25:341-345.➧ Brouwers L et al. ICP: maternal and fetal outcomes associated with elevated bile acid levels.
AJOG 2015; 212:100.e1-7.➧ Kawakita T et al. Predictors of adverse neonatal outcomes in ICP. AJOG 2015; 213:570.e1-8.➧ Cui D et al. Bile acid levels and risk of adverse perinatal outcomes in ICP: A meta-analysis.
J Obstet Gynaecol Res, 2017; 43(9): 1411-1420.➧ Geenes V et al. Association of severe ICP with adverse pregnancy outcomes: A prospective
population-based case-control study. Hepatology 2014; 59:1482-1491.
References (cont’d)➧ Herrera C et al. Perinatal outcomes associated with ICP. J Maternal Fetal Neonatal Medicine
2018; 31(14):1913-1920.➧ Puljic A et al. The risk of infant and fetal death by each additional week of expectant
management in ICP by gestational age. AJOG 2015; 212:667.e1-5.➧ Lo J et al. ICP and timing of delivery. J Matern Fetal Neonatal Med, 2015; 28(18):2254-
2258. ➧ Bacq Y et al. Efficacy of UDCA in treating ICP: A meta-analysis. Gastroenterology 2012;
143:1492-1501.➧ Kong X et al. Evaluating the effectiveness and afety of UDCA in treatment of ICP: A meta-
analysis (a prisma-compliant study). Medicine 2016; 95:40(34949).➧ Bicocca M et al. ICP: Review of six national and regional guidelines. Eur J Ob Gyn Repro Bio
2018; 231:180-187.➧ Tram T et al. ACG Clinical Guideline: Liver disease and pregnancy. Amer J
Gastroenterology 2016; 111(2):176-194.➧ RCOG Green-top Guideline No. 43: Obstetric Cholestasis, April 2011.➧ SMFM Publications Committee: ICP Explained. April 2011.
Discussion/thanks