Intracranial+Hemorrhage (1)

of 24
-
Upload
indri-noor-hidayati -
Category
Documents
-
view
233 -
download
0
Transcript of Intracranial+Hemorrhage (1)
-
8/13/2019 Intracranial+Hemorrhage (1)
1/24
Intracranial Hemorrhage
J. Alfredo Caceres, MDa , Joshua N. Goldstein, MD, PhD b ,c ,*
INTRODUCTION
Intracranial hemorrhage refers to any bleeding within the intracranial vault, includingthe brain parenchyma and surrounding meningeal spaces. This article focuses onthe acute diagnosis and management of primary nontraumatic intracerebral hemor-rhage (ICH) and subarachnoid hemorrhage (SAH) in emergency departments (EDs).
INTRACEREBRAL HEMORRHAGE
ICH is a devastating disease. The overall incidence of spontaneous ICH worldwide is24.6 per 100,000 p ers on-years with approximately 40,000 to 67,000 cases per year inthe United States. 13 The 30-day mortality rate ranges from 35% to 52% with only20% of survivors expected to have full functional recovery at 6 months. 3 Approxi-mately half of this mortality occurs within the first 24 hours, 4 highlighting the criticalimportance of early and effective treatment in EDs.
Risk Factors
A recent population-based meta-analysis showed that risk factors for ICH include malegender, older age, and Asian ethnicity. 1,5 ICH is twice as frequent in low-income to
a Department of Neurology, Massachusetts General Hospital, Suite 3B, Zero Emerson Place,
Boston, MA 01940, USA; b
Harvard Medical School, 25 Shattuck Street, Boston, MA 02115,USA; c Department of Emergency Medicine, Massachusetts General Hospital, Suite 3B, ZeroEmersion place, Boston, MA 01940, USA* Corresponding author.E-mail address: [email protected]
KEYWORDS
Intracranial hemorrhage Acute stroke Intracerebral hemorrhage Subarachnoid hemorrhage
KEY POINTS
Intracerebral hemorrhage is the most devastating form of stroke, with high mortality andsevere disability among survivors.
While no single therapy has been demonstrated to improve outcome, there is evidencethat high quality supportive care can provide substantial benefit.
National evidence-based guidelines are available to guide management for both intrace-rebral hemorrhage and subarachnoid hemorrhage.
Ruptured aneurysms are best managed by teams with experience in both surgical and en-dovascular techniques.
Emerg Med Clin N Am 30 (2012) 771794http://dx.doi.org/10.1016/j.emc.2012.06.003 emed.theclinics.com0733-8627/12/$ see front matter 2012 Elsevier Inc. All rights reserved.
mailto:[email protected]://dx.doi.org/10.1016/j.emc.2012.06.003http://emed.theclinics.com/http://emed.theclinics.com/http://dx.doi.org/10.1016/j.emc.2012.06.003mailto:[email protected] -
8/13/2019 Intracranial+Hemorrhage (1)
2/24
middle-income countries compared with high-income countries. 5 In the United States,several studies have shown t hat the incidence of ICH is greater in African Americansand Hispanics than in whites. 68
The most important risk factors for ICH include hypertension (HTN) and cerebra lamyloid angiopathy (CAA). HTN-related ICH is more likely to occur in dee p s tructures, 9
and the risk of ICH increases with increasing blood pressure (BP) values. 10 CAA tendsto occur in a ss ociation with advanced age, and CAA-related ICH tends to occur inlobar regions. 11
Other risk factors for ICH include
1. Alcohol intake: this risk seems dose-dependent, with a higher risk of ICH amongthose with a higher daily alcohol intake. 10 Acute changes in BP during ingestionand withdrawal, effects on platelet function and coagulation, and dysfunction of the vascular endothelium may account for this risk. 12
2. Cholesterol: low levels of total serum cholesterol are risk factors for ICH (in contrastto ischemic stroke, for which high cholesterol levels are a risk). 13
3. Genetics: the gene most strongly associated with ICH is the apolipoprotein E geneand its 2 and 4 alleles. 14 The presence of the 2 allele was recently also linked tohematoma expansion. 15
4. Anticoagulation: oral anticoagulants are widely used as prophylaxis in patients withatrial fibrillation and other cardiovascular and prothrombotic states. The annual riskof ICH in patients taking warfarin ranges from 0.3% to 1.0% per patient-year, witha significantly increased risk when the international normalized ratio (INR) is greaterthan 3.5. 16
5. Drug abuse: sympathomimetic drugs, such as cocaine, are risk factors for ICH, andpatients actively using cocaine at the tim e of their ICH have significantly moresevere presentations and worse outcomes. 17
Pathophysiology
Primary ICH is typically a manifestation of underlying small vessel disease. First, long-standing HTN leads to hypertensive vasculopathy, causing microscopic degenerativechanges in the walls of small-to-medium penetrating vessels, which is known as lip-ohyalinosis. 18 Second, CAA is characterized by the deposition of amyloid- b peptidein the walls of small leptomeningeal and cortical vessels. 19 Although the underlying
mechanism leading to the accumulation of amyloid is still unknown, the final conse-quences are degenerative changes in the vessel wall characterized by the loss of smooth muscle cells, wall thickening, luminal narrowing, microaneurysm formation,and microhemorrhages. 20
After initial vessel rupture, the hematoma causes direct mechanical injury to the brainparenchyma. Perihematomal edema develops within the first 3 hours from symptomonset and peaks between 10 and 20 days. 21 Next, blood and plasma products mediatesecondary injury processes, including an inflammatory response, activation of thecoagulation cascade, and iron deposition from hemoglobin degradation. 21 Finally, t hehematoma can continue to expand in up to 38% of patients during the first 24 hours. 22
Clinical Presentation and Diagnosis
The acute presentation of ICH can be difficult to distinguish from ischemic stroke.Symptoms may include headache, nausea, seizures, and focal or generalized neuro-logic symptoms. Findings, such as coma, headache, vomiting, seizures, neck stiff-ness, and raised diastolic BP, increase the likelihood of ICH compared withischemic stroke, but only neuroimaging can provide a definitive diagnosis. 23
Caceres & Goldstein772
-
8/13/2019 Intracranial+Hemorrhage (1)
3/24
Neuroimaging
Noncontrast CT Noncontrast CT is the most rapid and readily available tool for the diagnosis of ICH 24
and remains the most commonly used technique in the ED. Besides providing the
definitive diagnosis, CT may also show basic characteristics of the hematoma, suchas hematoma location, extension to the ventricular system, presence of surroundingedema, development of mass effect, and midline shift.
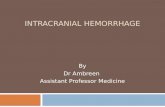
A quick estimation of the hematoma vo lume can be rapidly performed in an ED withthe validated ABC/2 technique ( Fig. 1 ).25 The steps to follow using this technique are
The CT slice with the largest area of hemorrhage is selected. A is the largest hemorrhage diameter on the selected slice (in centimeters [cm]). B is the largest diameter perpendicular to A on the same slice. C is the approximate number of slices in which the hemorrhage is seen multipliedby the slice thickness (often 0.5-cm slices).
A , B , and C are multiplied and the product divided by 2 .
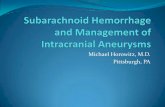
CT angiography CT angiograp hy (CTA) is gaining increasing acceptance as a diagnostic tool in theacute setting. 26 It is the most widely available, noninvasive technique for ruling outvascular abnormali tie s as secondary causes of ICH. The risk of acute nephropathy,if any, is likely low. 27 Up to 15% of patients with ICH sh ow an underlying vascularetiology on CTA, potentially changing acute management. 28 Finally, contrast extrava-sation seen on CTA images, also known as a spot sign ( Fig. 2 ), is thought to representongoing bleeding and seems to mark those patients at highest risk of hematomaexpansion and with poor outcome and mortality. 2932
MRI MRI is equivalent to CT for the detection of acute ICH. 33 The imaging characteristics of ICH vary with time as the hemoglobin passes through different stages during the
Fig. 1. ABC/2 technique. ( From Li N, Wang Y, Wang W, et al. Contrast extravasation oncomputed tomography angiography predicts clinical outcome in primary intracerebralhemorrhage. Stroke 2011;42:34416; with permission.)
Intracranial Hemorrhage 773
-
8/13/2019 Intracranial+Hemorrhage (1)
4/24
pathologic process. In the acute phase, gradient-recalled-echo imaging techniqueswith T2* weighting are the best option to detect the presence of ICH. 34 MRI canalso detect underlying secondary causes of ICH, such as tumor and hemorrhagictransformation of ischemic stroke. Finally, for patients with poor kidney function or
contrast allergies, the cerebral vasculature can be analyzed without contrast usingtime-of-flight magnetic resonance angiography. 35
Acute Management
Airway Patients with ICH are often unable to protect the airway. Endotracheal intubation maybe necessary but this decision should be balanced against the risk of losing the
Fig. 2. CT and CTA of acute ICH. ( A) Noncontrast CT shows a right thalamic ICH (24 mL) withassociatedIVH(6mL).( B)CTAdemonstrates3fociofcontrast(spotsigns)withintheICH( arrow-heads ) (C ). Delayed CTA shows increased volume and changed morphology of the spot signs(arrowheads ). (D) Noncontrast CT after 8 hours demonstrates expansion of the ICH (94 mL)and IVH (82 mL). (From Kidwell CS, Chalela JA, Saver JL, et al. Comparison of MRI and CT fordetection of acute intracerebral hemorrhage. JAMA 2004;292[15]:182330; with permission.)
Caceres & Goldstein774
-
8/13/2019 Intracranial+Hemorrhage (1)
5/24
-
8/13/2019 Intracranial+Hemorrhage (1)
6/24
-
8/13/2019 Intracranial+Hemorrhage (1)
7/24
Antiplatelet agents use before an ICH is associated with a small increase in mortality,suggestingan opportunity for intervention. 59 Theutilityandsafetyof platelet transfusionin such patients is unknown, although s ome laboratory data suggest that such transfu-sions may improve platelet activity. 60 Platelet transfusion is, therefore, consideredinvestigational by the AHA and is not recommended by the EUSI. The ongoing P A TCHclinical trial will investigate whether platelet transfusions can improve outcome. 61
Additionally, it is not clear whether low platelets contribute to ongoing bleeding orworse outcome. Pending further data, current AHA recommendations are that patientswith severe thrombocytopenia should receive platelet transfusion. 38 A specific cutoff is not clarified; different groups use thresholds between 10,000 and 50,000 per mL.
Novel antithrombotics Recently, several new agents, such as factor Xa inhibitors,apixaban and rivaroxaban, and the direct thrombin inhibitor, dabigatran, have becomeavailable for stroke prevention. 6264 There is no currently known antidote for reversal of these agents. Specific hemostatic agents, such as recombinant activated factor VIIand PCCs, may be considered, although there are limited data on their use. 65,66 Forthose cases related to dabigatran use, a recently published expert recommendationstates that the drug should be stopped immediately, supportive and symptomatictreatment should be initiated, and, due to its renal excretion, aggressive diuresisand potential dialysis could be considered. 67
Intracranial pressure management An increase in the ICP may arise from the presence of intraventricular hemorrhage(IVH) and subsequent hydrocephalus or from mass effect from a large hematoma orperihematomal edema. Currently, there are limited data regarding indications forICP monitoring. Current guidelines from the AHA/ASA suggest that patients witha Glasgow Coma Scale (GCS) score of less than or equal to 8, those with clinicalevidence of transtentorial herniation, and those with significant IVH or hydrocephalusshould be considered for ICP monitoring and treatment. 38 CPP can then be monitored,and recommendations are to maintain CPP between 50 mm Hg to 70 mm Hg. 28
The initial management of elevated ICP should comprise simple measures, such aselevation of the head of the bed, analgesia, and sedation. Medical options for ICPtreatment include m annito l, hypertonic saline (ranging from 3% to 23.4%), and neuro-musc ular paralysis. 3,68,69 Barbiturates can be considered in refractory intracranialHTN. 36 Although hyperventilation can produce a rapid decrease in the ICP, its effectsare temporary, and its use should be reserved for impending herniation while awaitingsurgical decompression.
Hyperglycemia management Hyperglycemia measured at arrival in the ED is associated with worse outcome in bothnondiabetic and diabetic patients. 70,71 Declining glucose values after ICH are associ-ated with a decreased risk of hematoma expansion and poor outcome, suggestingthat early glucose control may improve outcomes. 46 Early evidence for this interven-tion comes from the Quality in Acute Stroke Care (QASC) trial, in which patients withICH and ischemic stroke were randomized to receive standard care, or a set of inter-ventions aimed at treating fever, hyperglycemia, and performing swallow screens. 72The intervention (including glucose management) lowered mortality, and improvedoutcome, highlighting the need for careful glycemic control in the early phase. 38
TemperatureThe presence of fever is a common finding in patients with ICH, especially in those withIVH. Again, data from the QASC trial suggest lower mortality and improved outcome in
Intracranial Hemorrhage 777
-
8/13/2019 Intracranial+Hemorrhage (1)
8/24
those patients receiving fever control as part of a multidisciplinary approach. 72 Thosewith fever should undergo a thorough investigation to find a fever source if possible. 38
AnemiaThe presence of anemia is common in patients with ICH. It is present in up to 25% of
cases at admission and is associated with larger hematoma volumes. 73 It alsofrequently develops during hospital stay. 74 Although current guidelines do not addressthis issue, a recent study found that packed red bloo d c ell transfusion in these patientswas associated with improved survival at 30 days. 74 Therefore, transfusion can beconsidered in such patients, although the ideal target hemoglobin level has notbeen determined.
AntiepilepticsPatients with ICH are at an increased risk of developing seizures; however, most of these events are subclinical electroencephalographic findings. Seizures are more
common in lobar ICH and during the first 72 hours after admission.7577
The majorityof patients develop a single episode of seizure during hospitalization, suggesting thatthose episodes are related to the pathophysiologic processes that occur early after anICH. 77 The use of prophylactic antiepileptic drugs (AEDs) in patients with ICH isa common practice, although it is not clear that the presence of seizures and/or theuse of prophylactic AEDs affects short-term or long-term outcome. 78,79 Some studieshave reported an association between AEDs and worse outcome, although thesepatients were disproportionately exposed to phenytoin as the AED of choice. 80,81
Currently, the AHA/ASA recommends that AEDs should not be used routinely inpatients with ICH. The only clear indications are the presence of clinical seizures or
electrographic seizures in patients with a change in mental status. They also suggestthat the use of continuous electroencephalography monitoring should be consideredin those patients with depressed mental status out of proportion to the degree of braininjury. 38
Surgical Interventions
External ventricular drain placement As described previously, some patients may benefit from ICP monitoring. Externalventricular drain placement not only provides the ability to monitor ICP but also hasthe advantage of allowing therapeutic drain ag e of the cerebrospinal fluid (CSF), whichis valuable in patients with hydrocephalus. 82 The AHA recommends that ICP moni-toring and treatment be considered in patients with a GCS score less than or equalto 8, those with clinica l evidence of transtentorial herniation, or those with significantIVH or hydrocephalus. 38 The EUSI recommends considering continuous ICP moni-toring in patients who need mechanical ventilation and recommends medical treat-ment of elevated ICP if clinical deterioration is related to increasing edema. 44
Intraventricular thrombolysisIVH occurs when ICH extends into the ventricles. It occurs in approximately 45% of ICH, more frequently in large and deeply located (caudate nucleus and thalamus)hemorrhages. 83 The presence and the volume of IVH are correlated with poor prog-nosis in patients with ICH. 84 Although evacuation of an intraventricular clot is currentlynot routinely recommended, a recent study comparing the use of intraventricularrecombinant tissue plasminogen activator (rtPA) to placebo not only showed thatthe use of rtPA was feasible and safe but also showed a significantly greater rate of blood clot resolution. 85 In addition, a recent meta-analysis found that adding intraven-tricular fibrinolysis to external ventricular drain placement is associated with better
Caceres & Goldstein778
-
8/13/2019 Intracranial+Hemorrhage (1)
9/24
functional outcome, 86 although no prospective randomized trial has evaluated this.The Clot Lysis: Evaluating Accelerated Resolution of Intraventricular Hemorrhage(CLEAR III) study, an ongoing phase III randomized clinical trial, was designed tocompare the effect on clinical outcome of the intraventricular use of rtPA comparedwith placebo ( ClinicalTrials.gov [NCT00784134]).
Hematoma evacuationThe role of surgical evacuation is to decrease mass effect related to the presence of blood as well as to minimize secondary injury. The only clear recommendation forimmediate surgical intervention is in patients with cerebellar hemorrhages with neuro-logic deterioration, brainstem compression, and/or hydrocephalus from ventricularobstruction. 38 For these patients, emergency neurosurgical consultation should beobtained. It is less clear, however, whether patients with supratentorial ICH willbenefit. One large phase III clinical trial, Surgical Treatment for Intracerebral Hemor-rhage (STICH), compared early hematoma evacuation with initial conservative treat-ment of patients with spontaneous supratentorial ICH. 87 This study showed nodifference in outcome, suggesting that surgical evacuation provided no benefit. A subsequent subgroup analysis, however, raised the possibility that those with hema-tomas less than or equal to 1 cm from the cortical surface (which are more easilyaccessible) might receive benefit. 87 This possibility is being evaluated in the ongoingSTICH II trial. 88 The theoretic idea that hyperacute evacuation of the hematoma wouldbe beneficial was not borne out when a study evalua ting the effect of surgery within 4hours was stopped due to a high rate of rebleeding. 89
Minimally invasive surgery
The development of less-invasive surgical techniques may decrease the risk of surgical complications. These techniques are showing promising results, particularlyin deep hemorrhages where conventional surgery showed no benefit in the past. 90
Minimally invasive stereotactic puncture is reported safe and feasible and may leadto better long-term outcome and fewer complications when compared with conven-tional craniotomy 91 and conventional medical treatment. 92,93
Prognosis
Multiple grading scores exist that allow forevidence-based riskstratification in theacutephase. First, the ICH score predicts 30-day mortality using features, such as age, ICHvolume, and the presence of IVH, with higher score associated with worse outcome( Table 2 ).94 Second, the FUNC (functional outcome risk stratification) score predictsfunctional independence rather than mortality at 90 days ( Table 3 ).95 The higher theFUNC score, the greater the chance of the patient recovering functional independence.
There are some data that poor prognosis can lead to self-fulfilling prophecies of early death. Limiting care via early do-not-resuscitate (DNR) orders, withdrawal of care, or deferral of other life-sustaining interventions is independently associatedwith both short-term and long-term mortality after ICH, after controlling for clinicalmar ke rs of disease severity, even in patients who do not specifically require defibrilla-tion. 96 As such, new DNR orders or withdrawal of care is generally not recommendedin the ED. The AHA recommends aggressive full care early after ICH onset with p os t-ponement of new DNR orders until at least the second full day of hospitalization. 38
SUBARACHNOID HEMORRHAGE
SAH is defined by the extravasation of blood into the subarachnoid space. The mostcommon cause of SAH is trauma; among nontraumatic cases, rupture of an
Intracranial Hemorrhage 779
http://clinicaltrials.gov/http://clinicaltrials.gov/ -
8/13/2019 Intracranial+Hemorrhage (1)
10/24
Table 2The ICH Score
Component ICH Score PointsGCS score
34 2512 11315 0
ICH volume (cm3 )30 1
-
8/13/2019 Intracranial+Hemorrhage (1)
11/24
intracranial aneurysm is the leading cause, representing up to 85% of cases. Thisreview focuses on aneurysmal SAH.
Epidemiology
The overall incidence of SAH is between 9 and 20 per 100,000 person-ye ars. SAH ismore frequent in women, and the mean age of presentation i s 55 years. 97,98 In theUnited States, the number of cases of SAH is 30,000 per year. 99
Risk Factors and Prognosis
Major risk factors associated with SAH are current and former history of smoking,HTN, and excessive alcohol intake. 100 Although one-third of cases can be attributedto a current smoking status, this risk seems to rapidly disappear after a few years of smoking cessation. 101 Cocaine use is also associated with SAH, and patients takingcocaine tend to be younger and have a worse outcome. 102,103 First-degree familyhistory as well as some genetic conditions, including autosomal dominant polycystickidney disease, Marfan syndrome, and Ehlers-Danlos syndrome, are also associatedwith an increased risk of SAH. 104
A recent meta-analysis reported that in a population without comorbidities, theprevalence of unruptured intracranial aneurysms is 3.2%. 105 Only a small percentageof these unruptured intracranial aneurysms rupture and cause an SAH. The risk of rupture is increased in cases of previous history of SAH, age older than 60, femalegender, and Japanese or Finnish descent. In addition, the risk is greater for aneurysmsgreater than 10 mm and those located in the posterior circulation. 106108
The introduction of surgical treatment options improved the prognosis of patients
with SAH.109
In a retrospective analysis before the introduction of endovascular treat-ment of SAH, the most important factors predicting poor outcome at 3 months wereincreasing age, worse admission grade on the World Federation of NeurologicalSurgeons (WFNS) grading scale ( Table 4 ), the development of cerebral infarction,and symptomatic vasospasm. Other factors included greater clot thickness on admis-sion CT scan, aneurysm rupture within the posterior circulation, intraven tricular andintracerebral extension of the hematoma, and higher SBP on admission. 110 Analysisfrom the large International Subarachnoid Aneurysm Trial (ISAT ) comparing neurosur-gical clipping with endovascular coiling showed similar results. 111
Pathophysiology
Aneurysms are more common at the bifurcation of the arteries located on the base of the brain, especially the large arteries that form the circle of Willis. 112 Hemodynamicfactors that contribute to the formation and growth of aneurysms are wall shear stress
Table 4World Federation of Neurological Surgeons grading scale
WFNS Grade GCS Motor Deficit1 15 Absent2 13 to 14 Absent3 13 to 14 Present4 7 to 12 Present or absent5 3 to 6 Present or absent
Data from Report of World Federation of Neurological Surgeons committee on a universalsubarachnoid hemorrhage grading scale. J Neurosurg 1988;68(6):9856.
Intracranial Hemorrhage 781
-
8/13/2019 Intracranial+Hemorrhage (1)
12/24
and hydrostatic and transmural pressures. High wall shear stress is encountered at thebranch points of cerebral arteries, and long-term exposure to this could trigger vesselwall remodeling through interaction with the endothelium and the secretion of factors,such as nitric oxide and endothelial growth factors. Hydrostatic and transmural pres-sures produce a mechanical stretch of the wall that induces upregulation of certainmolecules, such as endothelin-1B re ce ptors, that further affect vascular smoothmuscle cells by promoting apoptosis. 113 Although the mechanism of formation andgrowth of aneurysms is partially understood, it is still unclear what leads to aneurysmalrupture.
Clinical Presentation
The characteristic complaint of patients with SAH is a severe headache of acute onset.This headache is commonly described as the worst headache of my life, with thehighest intensity at onset. Although it is frequently accompanied by other symptoms,
headache may be the only complaint in up to 40% of patients.114
Recently, a prospec-tive study found that the following clinical characteristics represent the highest risk of belonging to a case of SAH: age greater than 40 years, associated neck pain or stiff-ness, witnessed loss of consci ous ness, onset with exertion, vomiting, arrival by ambu-lance, and BP above 160/100. 115
A subgroup of patients develops warning signs before the index SAH. The mostcommon warning sign is again headache, which is of moderate intensity and lesssevere than that described in SAH. This is commonly referred to as sentinel headacheor warning leak and may be associated with a small leakage of blood into thesubarachnoid space or a small bleed into the aneurysmal wall. A thorough evaluation
is warranted in these cases, because SAH can develop up to 110 days later.116,117
Physical examination may demonstrate neck stiffness and meningismus. 118
Although not specific, funduscopic evaluation may reveal subhyaloid, vitreous, orintraretinal hemorrhage (known as Terson syndrome), which is associated with highermortality. 119 These eye findings may be found with any intracranial bleeding and arebelieved associated with sudden increase in ICP. Focal neurologic deficits may alsobe found and can be related to nerve compression by the aneurysm, intraparenchymalextension of the bleeding, or vasospasm (which typically occurs later in the course).
Diagnosis
Up to 1 in 20 SAH patients are missed during initial evaluation. 120 A high index of suspicion and a low threshold for performing diagnostic studies are key factors inmaking the diagnosis of SAH.
The gold standard diagnostic approach has been to initially perform a noncontrastCT scan of the brain followed by a lumbar puncture (LP) and analysis of the CSF whenthe CT is negative. Recently, however, some groups have suggested that current-generation multislice CT scanners as well as the availability of CTA in the acute settingmay offer opportunities to selectively defer LP. 121,122
CT When there is clinical suspicion of SAH, the initial test of choice is a noncontrast CTscan. The sensitivity of the CT scan to detect SAH is maximal within the first 24 hoursafter the bleed and then decreases with time. The volume of blood in thesubarachnoid space and the resolution of the scanner also influence the CT detectionrate. 123 A recent multicenter prospective study of 3132 patients found that of thoseundergoing current-generation CT within 6 hours of symptom onset, the sensitivitywas 100% (95% CI, 97%100%) with a negative predictive value of 100% (95% CI,
Caceres & Goldstein782
-
8/13/2019 Intracranial+Hemorrhage (1)
13/24
99.5%100%). 122 Noncontrast CT also provides information regarding the volume of blood, extension to the cerebral parenchyma, the presence of hydrocephalus, and thepotential location of the aneurysm. Blood located in the interhemispheric fissure andthe surrounding sulci has a high probability of coming from an anterior cerebral oranterior communicating artery aneurysm, whereas blood in the posterior aspect of the syl vian fissure is probably related to a middle cerebral artery aneurysm( Fig. 3 ).123125
CT angiography CTA is a fa st, noninvasive, and readily available method to screen for the presence of aneurysm. 126 A recent meta-analysis showed that CTA has a pooled sensitivity of approx imately 98% to detect aneurysm, with sensitivities ranging from 86% to100%. 127 Aneurysm detection rates are related to the experience of the reviewerand aneurysmal size. Po ole d specificity of CTA in this analysis reached 100% with
a range of 50% to 100%.127
Also, 3-D CTA may be as sensitive and s pe cific as digitalsubtraction angiography for the detection of aneurysms ( Fig. 4 ).128 As a result,patients with negative CT/CTA have a less than 1% likelihood of aneurysmalSAH. 121 The Neurocritical Care Society recommends preferential use of CTA as anexploratory approach when it is readily available and of high technical quality overdigital subtraction angiography if an immediate intervention is not planned. 129
Lumbar punctureLP is considered effectively 100% sensitive for detection of blood in the subarachnoidspace, and it is recommended in all patients undergoing a workup for SAH with a nega-
tive CT.130132
CSF characteristics of SAH include an elevated opening pressure,presence of erythrocytes or red blood cells, and xanthochromia. CSF should be visu-ally inspected for the presence of xanthochromia, a term that refers to the yellowaspect of the CSF attributable to the formation of bilirubin from the breakdown of hemoglobin in the CSF. 133
Special consideration should be given to the use of spectrophotometry in CSF anal-ysis for the detection of bilirubin. The use of this technique is strongly advocated in theUnited Kingdom, where the rate of visual assessment of the cerebrospinal fluid fell to
Fig. 3. SAH in the left sylvian fissure, sulci of the left hemisphere and along the left andcentral aspect of the suprasellar cistern, left ambient cistern, and interpenduncular cistern.
Intracranial Hemorrhage 783
-
8/13/2019 Intracranial+Hemorrhage (1)
14/24
6%, whereas the use of spectrophotometry rose to 94% in recent years. 134 Thismethod has been shown to have approximately 100% sensiti vity for the detection
of bilirubin in patients with SAH but with low specificity.135,136
In the United States,however, the majority of centers use visual inspection instead. 137 Some investigatorsrecommend spectrop hoto metry, if available, in those cases where visual inspectionyields doubtful results. 138
Digital subtraction angiography Digital subtraction angiography allows for direct visualization of the cerebral vascula-ture and remains the gold standard for detecting aneurysms. This diagnostic toolrequires a dedicated neurointerventional team and provides an opportunity for thera-peutic interventions as well as diagnosis.
MRI MRI is rarely used to diagnose SAH in the ED because availability is limited, and logis-tical barriers to its use are much higher than with CT. Blood is not easily detectable inT1-weighted and T2-weighted MRI sequences in the acute setting, likely because thegeneration of deoxyhemoglobin with paramagnetic properties is delayed in thesubarachnoid space. 139 The sensitivity of fluid-attenuated inversion recoverysequences, however, is comparable to that of the CT in the acute phase of an SAHand potentially superior in the subacute phase. 140,141
Emergency Management
Airway management The initial management of an SAH does not differ from other medical emergencies,and airway management is similar to that described previously for ICH.
Neurologic examinationDuring the initial evaluation, a neurologic examination should be performed and docu-mented. Clinical grading scales that mark the severity of SAH include the Hunt and
Fig. 4. 3-D reconstruction CTA on the same patient as in Fig. 3. An aneurysmal sac is appre-ciated at the distal M1 segment of the left middle cerebral artery.
Caceres & Goldstein784
-
8/13/2019 Intracranial+Hemorrhage (1)
15/24
Hess scale ( Table 5 ) and the WFNS grading scale (see Table 4 ). The Hunt and Hessscale was originally designed to evaluate the operativ e risk of patients and to aid atdeciding the best timing for neurosurgical intervention, 142 but it is now widely knownand accepted as a predictor of outcome. It is based on the level of severity of clinicalsigns with a correlation with poor outcome with a higher grade. The WFNS gradingscale uses the GCS score and groups them into 5 grades and also takes into accountthe presence of a motor neurologic deficit. 143
Medical Management
Blood pressure management When considering an optimal BP goal, an appropriate balance should be maintained.Hypotension may theoretically increase the risk of ischemia, whereas elevated BP rai-ses the concern for aneurysmal rupture and rebleeding. Current guidelines recom-mend that hypotension should be avoided and that treatment of HTN should beinitiated until the aneurysm is secure only with extreme BP values when the MAP isgreater than 110 mm Hg, aiming at maintaining a good CPP. The recommendedagents to lower BP are nicardipine, labetalol, and esmolol. 129,144
Seizure prophylaxisTo date, no randomized controlled trial has evaluated the benefits of the prophylacticuse of AEDs in patients with SAH. The incidence of seizure varies extensively in theliterature. 145 Risk factors for the development of onset seizures include poor Huntand Hess score, acute hydrocephalus, cerebral ischemia, and large volume of subarachnoid blood. 129,146,147
Nonconvulsive seizures and nonconvulsive status epilepticus may occur after SAH,leading clinicians to recommend continuous electroencephalography monitoring inpatients with poor Hunt and Hess scores. 148 Current guidelines recommend consid-ering the use of routine AEDs, especially in patients at higher risk, and using an alter-native to phenytoin, which has been linked to a poor prognosis. 129 Commonly usedagents include levetiracetam, valproate, and fosphenytoin (it is unclear whether thisshares the same possible negative effects as phenytoin).
Glycemic control Both elevated and low glucose levels are associated with worse outcome after SAH.Hypoglycemia is associated with vasospasm, infarction, and more disability at 3
months. Hyperglycemia on admission and during hospitalization is also associatedwith poor outcome and short-term mortality. 149151 Although a specific target glucoselevel has not been established, it is currently recommended to avoid hypoglycemia(serum glucose
-
8/13/2019 Intracranial+Hemorrhage (1)
16/24
TemperatureFever is common after SAH. Fever at admission and its presence during hospitaliza-tion are associated with poor outcome. 152 A possible infectious etiology should alwaysbe investigated, although this is uncommon during initial presentation. Medical andphysical interventions can be used as therapeutic measures to reduce fever.Currently, it is recommended to initiate therapy with antipyretic agents, such as acet-aminophen, when fever is present. 129 Physical surface or intravascular coolingdevices should be used only when antipyretics fail, and close monitoring and treat-ment of shivering should be started. 129
Vasospasm and Delayed Cerebral Ischemia
Vasospasm and delayed cerebral ischemia are deadly complications of SAH associ-ated with poor outcome. Angiographic vasospasm occurs in up to 70% of cases. 153
Symptomatic vasospasm, associated with new focal neurologic findings and/or dete-
rioration in the level of consciousness, occurs in approximately 30% of cases.154
Delayed cerebral ischemia can occur days after the index SAH and can lead to neuro-logic deterioration and focal neurologic deficits. 155 One preventive measure is the useof oral nimodipine (60 mg by mouth or nasogastric tube every 4 hours for 21 days) andshould be initiated soon after diagnosis of SAH. 156 Once vasospasm occurs, a rangeof medica l and interventional therapies is available to maintain adequate cerebralperfusion. 129 One recognized therapy is the triple-H therapy, characterized by hyper-volemia through volume expansi on, HTN with BP augmentation, and hemodilutionaimed at reducing blood viscosity. 157 Currently, the Neurocritical Care Society recom-mends that euvolemia be pursued and th at the routine use of hemodilution should be
reserved for cases of erythrocythemia. 129 For BP augmentation, a stepwise approachis recommended and an SBP goal of g reater than 160 mm Hg or an MAP greater than120 mm Hg is a reasonable approach. 129,158
Aneurysm Repair
Patients with SAH require emergency neurosurgical and/or endovascular consulta-tion. There are currently at least 2 options for the acute treatment of a ruptured aneu-rysm: endovascular coiling or surgical clipping. Treatment of a recently rupturedaneurysm reduces the rate of rebleeding, and the benefit is related to the time to treat-
ment initiation.159
Current guidelines recommend that surgical clipping or endovascu-lar coiling should be performed to reduce the rate of rebleeding after aneurysmal SAH,and these procedures should be performed early in the disease course. 129,144
The selection of the most appropriate intervention depends on a range of character-istics, including age, clinical status, and medical comorbidities. Aneurysm character-istics, such as location, shape, and size, are taken into consideration as well,highlighting the value of a specialized multidisciplinary group to provide care and deci-sion making. Some expert consensus groups recommend that SAH be preferentiallymanaged at high-volume centers (defined as those centers with greater than 60 casesof SAH per year). 129
REFERENCES
1. van Asch CJ, Luitse MJA, Rinkel GJE, et al. Incidence, case fatality, and func-tional outcome of intracerebral haemorrhage over time, according to age, sex,and ethnic origin: a systematic review and meta-analysis. Lancet Neurol 2010;9(2):16776.
Caceres & Goldstein786
-
8/13/2019 Intracranial+Hemorrhage (1)
17/24
2. Aguilar MI, Freeman WD. Spontaneous intracerebral hemorrhage. Semin Neurol2010;30(5):55564.
3. Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management ofspontaneous intracerebral hemorrhage in adults. Stroke 2007;38(6):200123.
4. Elliott J, Smith M. The acute management of intracerebral hemorrhage: a clinicalreview. Anesth Analg 2010;110(5):141927.
5. Feigin VL, Lawes CMM, Bennett DA, et al. Worldwide stroke incidence and earlycase fatality reported in 56 population-based studies: a systematic review. LancetNeurol 2009;8(4):35569.
6. Labovitz DL, Halim A, Boden-Albala B, et al. The incidence of deep and lobarintracerebral hemorrhage in whites, blacks, and Hispanics. Neurology 2005;65(4):51822.
7. Ayala C, Greenlund KJ, Croft JB, et al. Racial/ethnic disparities in mortality bystroke subtype in the United States, 19951998. Am J Epidemiol 2001;154(11):105763.
8. Qureshi AI, Giles WH, Croft JB. Racial differences in the incidence of intracere-bral hemorrhage. Neurology 1999;52(8):1617.
9. Matsukawa H, Shinoda M, Fujii M, et al. Factors associated with lobar vs. non-lobar intracerebral hemorrhage. Acta Neurol Scand 2011. http://dx.doi.org/ 10.1111/j.1600-0404.2011.01615.x.
10. Ariesen MJ, Claus SP, Rinkel GJE, et al. Risk factors for intracerebral hemor-rhage in the general population. Stroke 2003;34(8):20605.
11. Maia LF, Mackenzie IR, Feldman HH. Clinical phenotypes of cerebral amyloidangiopathy. J Neurol Sci 2007;257(12):2330.
12. Badjatia N, Rosand J. Intracerebral hemorrhage. Neurologist 2005;11(6):31124.13. Wieberdink RG, Poels MMF, Vernooij MW, et al. Serum lipid levels and the risk of
intracerebral hemorrhage: the Rotterdam Study. Arterioscler Thromb Vasc Biol2011;31(12):29829.
14. Biffi A, Sonni A, Anderson CD, et al. Variants at APOE influence risk of deep andlobar intracerebral hemorrhage. Ann Neurol 2010;68(6):93443.
15. Brouwers HB, Biffi A, Ayres AM, et al. Apolipoprotein e genotype predicts hema-toma expansion in lobar intracerebral hemorrhage. Stroke 2012;43(6):14905.
16. Flaherty ML. Anticoagulant-associated intracerebral hemorrhage. Semin Neurol
2010;30(5):56572.17. Martin-Schild S, Albright KC, Hallevi H, et al. Intracerebral hemorrhage in
cocaine users. Stroke 2010;41(4):6804.18. Fisher CM. Pathological observations in hypertensive cerebral hemorrhage.
J Neuropathol Exp Neurol 1971;30(3):53650.19. Vinters H. Cerebral amyloid angiopathy. A critical review. Stroke 1987;18(2):
31124.20. Viswanathan A, Greenberg SM. Cerebral amyloid angiopathy in the elderly. Ann
Neurol 2011;70(6):87180.21. Aronowski J, Zhao X. Molecular pathophysiology of cerebral hemorrhage:
secondary brain injury. Stroke 2011;42(6):17816.22. Brott T, Broderick J, Kothari R, et al. Early hemorrhage growth in patients with
intracerebral hemorrhage. Stroke 1997;28(1):15.23. Runchey S, Mc Gee S. Clinical findings distinguishing hemorrhagic stroke from
ischemic stroke. JAMA 2010;30(22):22806.24. Panagos PD, Jauch EC, Broderick JP. Intracerebral hemorrhage. Emerg Med
Clin North Am 2002;20(3):63155.
Intracranial Hemorrhage 787
-
8/13/2019 Intracranial+Hemorrhage (1)
18/24
25. Kothari RU, Brott T, Broderick JP, et al. The ABCs of measuring intracerebralhemorrhage volumes. Stroke 1996;27(8):13045.
26. Delgado Almandoz JE, Romero JM. Advanced CT imaging in the evaluation ofhemorrhagic stroke. Neuroimaging Clin N Am 2011;21(2):197213.
27. Oleinik A, Romero JM, Schwab K, et al. CT angiography for intracerebral hemor-rhage does not increase risk of acute nephropathy. Stroke 2009;40(7):23937.
28. Delgado Almandoz JE, Schaefer PW, Forero NP, et al. Diagnostic accuracy andyield of multidetector CT angiography in the evaluation of spontaneous intrapar-enchymal cerebral hemorrhage. AJNR Am J Neuroradiol 2009;30(6):121321.
29. Goldstein JN, Fazen LE, Snider R, et al. Contrast extravasation on CT angiog-raphy predicts hematoma expansion in intracerebral hemorrhage. Neurology2007;68(12):88994.
30. Kim J, Smith A, Hemphill JC, et al. Contrast extravasation on CT predictsmortality in primary intracerebral hemorrhage. AJNR Am J Neuroradiol 2008;29(3):5205.
31. Hallevi H, Abraham AT, Barreto AD, et al. The spot sign in intracerebral hemor-rhage: the importance of looking for contrast extravasation. Cerebrovasc Dis2010;29(3):21720.
32. Wada R, Aviv RI, Fox AJ, et al. CT angiography spot sign predicts hematomaexpansion in acute intracerebral hemorrhage. Stroke 2007;38(4):125762.
33. Kidwell CS, Chalela JA, Saver JL, et al. Comparison of MRI and CT for detectionof acute intracerebral hemorrhage. JAMA 2004;292(15):182330.
34. Smith SD, Eskey CJ. Hemorrhagic stroke. Radiol Clin North Am 2011;49(1):2745.35. DeLano MC, DeMarco JK. 3.0 T versus 1.5 T MR angiography of the head and
neck. Neuroimaging Clin N Am 2006;16(2):32141.36. Rincon F, Mayer S. Clinical review: critical care management of spontaneousintracerebral hemorrhage. Crit Care 2008;12(6):237.
37. Goldstein J, Gilson A. Critical care management of acute intracerebral hemor-rhage. Curr Treat Options Neurol 2011;13(2):20416.
38. Morgenstern LB, Hemphill JC, Anderson C, et al. Guidelines for the manage-ment of spontaneous intracerebral hemorrhage: a guideline for healthcareprofessionals from the American Heart Association/American Stroke Associa-tion. Stroke 2010;41(9):210829.
39. Anderson CS, Huang Y, Wang JG, et al. Intensive blood pressure reduction in
acute cerebral haemorrhage trial (INTERACT): a randomised pilot trial. LancetNeurol 2008;7(5):3919.
40. Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH) investiga-tors. Antihypertensive treatment of acute cerebral hemorrhage. Crit Care Med2010;38(2):63748.
41. Qureshi A, Palesch Y. Antihypertensive Treatment of Acute Cerebral Hemorrhage(ATACH) II: design, methods, and rationale. Neurocrit Care 2011;15(3):55976.
42. Delcourt C, Huang Y, Wang J, et al. The second (main) phase of an open, rand-omised, multicentre study to investigate the effectiveness of an intensive bloodpressure reduction in acute cerebral haemorrhage trial (INTERACT2). Int J
Stroke 2010;5(2):1106.43. Butcher K, Jeerakathil T, Emery D, et al. The intracerebral haemorrhage acutely
decreasing arterial pressure trial: ICH ADAPT. Int J Stroke 2010;5(3):22733.44. Steiner T, Kaste M, Forsting M, et al. Recommendations for the management of
intracranial haemorrhagepart I: spontaneous intracerebral haemorrhage. TheEuropean Stroke Initiative Writing Committee and the Writing Committee for theEUSI Executive Committee. Cerebrovasc Dis 2006;22(4):294316.
Caceres & Goldstein788
-
8/13/2019 Intracranial+Hemorrhage (1)
19/24
45. Mayer SA, Brun NC, Begtrup K, et al. Efficacy and safety of recombinant acti-vated factor VII for acute intracerebral hemorrhage. N Engl J Med 2008;358(20):212737.
46. Aguilar MI, Hart RG, Kase CS, et al. Treatment of warfarin-associated intracere-bral hemorrhage: literature review and expert opinion. Mayo Clin Proc 2007;82(1):8292.
47. Watson HG, Baglin T, Laidlaw SL, et al. A comparison of the efficacy and rate ofresponse to oral and intravenous Vitamin K in reversal of over-anticoagulationwith warfarin. Br J Haematol 2001;115(1):1459.
48. Goodnough LT, Shander A. How I treat warfarin-associated coagulopathy inpatients with intracerebral hemorrhage. Blood 2011;117(23):60919.
49. Recommendations for the management of intracranial haemorrhagepart I:spontaneous intracerebral haemorrhage. Cerebrovasc Dis 2006;22(4):294316.
50. Goldstein J, RosandJ, Schwamm L. Warfarin reversal in anticoagulant-associatedintracerebral hemorrhage. Neurocrit Care 2008;9(2):27783.
51. OShaughnessy DF, Atterbury C, Bolton Maggs P, et al. Guidelines for the use offresh-frozen plasma, cryoprecipitate and cryosupernatant. Br J Haematol 2004;126(1):1128.
52. Steiner T, Rosand J, Diringer M. Intracerebral hemorrhage associated with oralanticoagulant therapy. Stroke 2006;37(1):25662.
53. Goldstein JN, Thomas SH, Frontiero V, et al. Timing of fresh frozen plasmaadministration and rapid correction of coagulopathy in warfarin-related intrace-rebral hemorrhage. Stroke 2006;37(1):1515.
54. Bershad E, Suarez J. Prothrombin complex concentrates for oral anticoagulanttherapy-related intracranial hemorrhage: a review of the literature. NeurocritCare 2010;12(3):40313.
55. Holland L, Warkentin TE, Refaai M, et al. Suboptimal effect of a three-factorprothrombin complex concentrate (Profilnine-SD) in correcting supratherapeuticinternational normalized ratio due to warfarin overdose. Transfusion 2009;49(6):11717.
56. Dentali F, Marchesi C, Pierfranceschi MG, et al. Safety of prothrombin complexconcentrates for rapid anticoagulation reversal of vitamin K antagonists. A meta-analysis. Thromb Haemost 2011;106(3):42938.
57. Goldstein JN, Fazen LE, Wendell L, et al. Risk of thromboembolism followingacute intracerebral hemorrhage. Neurocrit Care 2009;10(1):2834.
58. Gurol M, Greenberg S. Management of intracerebral hemorrhage. Curr Atheros-cler Rep 2008;10(4):32431.
59. Thompson BB, Bejot Y, Caso V, et al. Prior antiplatelet therapy and outcomefollowing intracerebral hemorrhage: a systematic review. Neurology 2010;75(15):133342.
60. Naidech AM, Liebling SM, Rosenberg NF, et al. Early platelet transfusion improvesplatelet activity and may improve outcomes after intracerebral hemorrhage. Neuro-crit Care 2012;16(1):827.
61. de Gans K, de Haan R, Majoie C, et al. Patch: platelet transfusion in cerebralhaemorrhage: study protocol for a multicentre, randomised, controlled trial.BMC Neurol 2010;10(1):19.
62. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin inpatients with atrial fibrillation. N Engl J Med 2011;365(11):98192.
63. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalv-ular atrial fibrillation. N Engl J Med 2011;365(10):88391.
Intracranial Hemorrhage 789
-
8/13/2019 Intracranial+Hemorrhage (1)
20/24
64. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin inpatients with atrial fibrillation. N Engl J Med 2009;361(12):113951.
65. van Ryn J, Stangier J, Haertter S, et al. Dabigatran etexilatea novel, revers-ible, oral direct thrombin inhibitor: interpretation of coagulation assays andreversal of anticoagulant activity. Thromb Haemost 2010;103(6):111627.
66. Eerenberg ES, Kamphuisen PW, Sijpkens MK, et al. Reversal of rivaroxaban anddabigatran by prothrombin complex concentrate: a randomized, placebo-controlled, crossover study in healthy subjects. Circulation 2011;124(14):15739.
67. Watanabe M, Siddiqui FM, Qureshi AI. Incidence and management of ischemicstroke and intracerebral hemorrhage in patients on dabigatran etexilate treat-ment. Neurocrit Care 2012;16(1):2039.
68. Rangel-Castillo L, Gopinath S, Robertson CS. Management of intracranialhypertension. Neurol Clin 2008;26(2):52141.
69. Helbok R, Kurtz P, Schmidt JM, et al. Effect of mannitol on brain metabolism andtissue oxygenation in severe haemorrhagic stroke. J Neurol Neurosurg Psychi-atry 2011;82(4):37883.
70. Stead L, Jain A, Bellolio M, et al. Emergency department hyperglycemia asa predictor of early mortality and worse functional outcome after intracerebralhemorrhage. Neurocrit Care 2010;13(1):6774.
71. Kimura K, Iguchi Y, Inoue T, et al. Hyperglycemia independently increases the riskof early death in acute spontaneous intracerebral hemorrhage. J Neurol Sci 2007;255(12):904.
72. Middleton S, McElduff P, Ward J, et al. Implementation of evidence-based treat-ment protocols to manage fever, hyperglycaemia, and swallowing dysfunction
in acute stroke (QASC): a cluster randomised controlled trial. Lancet 2011;378(9804):1699706.73. Kumar MA, Rost NS, Snider RW, et al. Anemia and hematoma volume in acute
intracerebral hemorrhage. Crit Care Med 2009;37(4):14427.74. Sheth KN, et al. Packed red blood cell transfusion and decreased mortality in
intracerebral hemorrhage. Neurosurgery 2011;68(5):128692.75. Claassen J, Jette N, Chum F, et al. Electrographic seizures and periodic
discharges after intracerebral hemorrhage. Neurology 2007;69(13):135665.76. Vespa PM, OPhelan K, Shah M, et al. Acute seizures after intracerebral hemor-
rhage. Neurology 2003;60(9):14416.
77. De Herdt V, Dumont F, He non H, et al. Early seizures in intracerebral hemor-rhage. Neurology 2011;77(20):1794800.
78. Passero S, Rocchi R, Rossi S, et al. Seizures after spontaneous supratentorialintracerebral hemorrhage. Epilepsia 2002;43(10):117580.
79. Reddig RT, Nixdorf KE, Jensen MB. The prophylactic use of an antiepilepticdrug in intracerebral hemorrhage. Clin Neurol Neurosurg 2011;113(10):8957.
80. Naidech AM, Garg RK, Liebling S, et al. Anticonvulsant use and outcomes afterintracerebral hemorrhage. Stroke 2009;40(12):38105.
81. Messe S, Sansing L, Cucchiara B, et al. Prophylactic antiepileptic drug use isassociated with poor outcome following ICH. Neurocrit Care 2009;11(1):3844.
82. Smith M. Monitoring intracranial pressure in traumatic brain injury. Anesth Analg2008;106(1):2408.
83. Hallevi H, Albright KC, Aronowski J, et al. Intraventricular hemorrhage.Neurology 2008;70(11):84852.
84. Tuhrim S, Horowitz DR, Sacher M, et al. Volume of ventricular blood is an impor-tant determinant of outcome in supratentorial intracerebral hemorrhage. CritCare Med 1999;27(3):61721.
Caceres & Goldstein790
-
8/13/2019 Intracranial+Hemorrhage (1)
21/24
85. Naff N, Williams MA, Keyl PM, et al. Low-dose recombinant tissue-type plasmin-ogen activator enhances clot resolution in brain hemorrhage. Stroke 2011;42(11):300916.
86. Gaberel T, Magheru C, Parienti J-J, et al. Intraventricular fibrinolysis versusexternal ventricular drainage alone in intraventricular hemorrhage. Stroke2011;42(10):277681.
87. Mendelow AD, Gregson BA, Fernandes HM, et al. Early surgery versus initialconservative treatment in patients with spontaneous supratentorial intracerebralhaematomas in the International Surgical Trial in Intracerebral Haemorrhage(STICH): a randomised trial. Lancet 2005;365(9457):38797.
88. Mendelow AD, Gregson B, Mitchell P, et al. Surgical trial in lobar intracerebralhaemorrhage (STICH II) protocol. Trials 2011;12(1):124.
89. Morgenstern LB, Demchuk AM, Kim DH, et al. Rebleeding leads to pooroutcome in ultra-early craniotomy for intracerebral hemorrhage. Neurology2001;56(10):12949.
90. Tan SH, Ng PY, Yeo TT, et al. Hypertensive basal ganglia hemorrhage:a prospective study comparing surgical and nonsurgical management. SurgNeurol 2001;56(5):28792.
91. Zhou H, Zhang Y, Liu L, et al. A prospective controlled study: minimally invasivestereotactic puncture therapy versus conventional craniotomy in the treatmentof acute intracerebral hemorrhage. BMC Neurol 2011;11(1):76.
92. Wang WZ, Jiang B, Liu H-M, et al. Minimally invasive craniopuncture therapy vs.conservative treatment for spontaneous intracerebral hemorrhage: results froma randomized clinical trial in China. Int J Stroke 2009;4(1):116.
93. Marquardt G, Wolff R, Janzen RWC, et al. Basal ganglia haematomas in non-comatose patients: subacute stereotactic aspiration improves long-term outcomein comparison to purely medical treatment. Neurosurg Rev 2005;28(1):649.
94. Hemphill JC 3rd, Bonovich DC, Besmertis L, et al. The ICH score: a simple, reli-able grading scale for intracerebral hemorrhage. Stroke 2001;32(4):8917.
95. Rost NS, Smith EE, Chang Y, et al. Prediction of functional outcome in patientswith primary intracerebral hemorrhage: the FUNC score. Stroke 2008;39(8):23049.
96. Zahuranec DB, Brown DL, Lisabeth LD, et al. Early care limitations indepen-dently predict mortality after intracerebral hemorrhage. Neurology 2007;
68(20):16517.97. van Gijn J, Rinkel GJ. Subarachnoid haemorrhage: diagnosis, causes and
management. Brain 2001;124(2):24978.98. de Rooij NK, Linn FHH, van der Plas JA, et al. Incidence of subarachnoid hae-
morrhage: a systematic review with emphasis on region, age, gender and timetrends. J Neurol Neurosurg Psychiatry 2007;78(12):136572.
99. Zacharia BE, Hickman ZL, Grobelny BT, et al. Epidemiology of aneurysmalsubarachnoid hemorrhage. Neurosurg Clin N Am 2010;21(2):22133.
100. Feigin VL, Rinkel GJE, Lawes CMM, et al. Risk factors for subarachnoid hemor-rhage. Stroke 2005;36(12):277380.
101. Anderson CS, Feigin V, Bennett D, et al. Active and passive smoking and therisk of subarachnoid hemorrhage. Stroke 2004;35(3):6337.
102. Broderick JP, Viscoli CM, Brott T, et al. Major risk factors for aneurysmal subarach-noid hemorrhage in the young are modifiable. Stroke 2003;34(6):137581.
103. Vannemreddy P, Caldito G, Willis B, et al. Influence of cocaine on ruptured intra-cranial aneurysms: a case control study of poor prognostic indicators. J Neurol2008;108(3):4706.
Intracranial Hemorrhage 791
-
8/13/2019 Intracranial+Hemorrhage (1)
22/24
104. Ferro J, Canha o P, Peralta R. Update on subarachnoid haemorrhage. J Neurol2008;255(4):46579.
105. Vlak MH, Algra A, Brandenburg R, et al. Prevalence of unruptured intracranialaneurysms, with emphasis on sex, age, comorbidity, country, and time period:a systematic review and meta-analysis. Lancet Neurol 2011;10(7):62636.
106. Wermer MJ, van der Schaaf IC, Algra A, et al. Risk of rupture of unruptured intra-cranial aneurysms in relation to patient and aneurysm characteristics. Stroke2007;38(4):140410.
107. Wiebers DO. Unruptured intracranial aneurysms: natural history, clinicaloutcome, and risks of surgical and endovascular treatment. Lancet 2003;362(9378):10310.
108. Ishibashi T, Murayama Y, Urashima M, et al. Unruptured intracranial aneurysms.Stroke 2009;40(1):3136.
109. Lerch C, Yonekawa Y, Muroi C, et al. Specialized neurocritical care, severitygrade, and outcome of patients with aneurysmal subarachnoid hemorrhage.Neurocrit Care 2006;5(2):8592.
110. Rosengart AJ, Schultheiss KE, Tolentino J, et al. Prognostic factors for outcome inpatients with aneurysmal subarachnoid hemorrhage.Stroke2007;38(8):231521.
111. Risselada R, Lingsma HF, Bauer-Mehren A, et al. Prediction of 60 day case-fatality after aneurysmal subarachnoid haemorrhage: results from the Interna-tional Subarachnoid Aneurysm Trial (ISAT). Eur J Epidemiol 2010;25(4):2616.
112. Kelly ME,Dodd R,SteinbergGK. Chapter 39subarachnoid hemorrhage. In: MarcF,editor. Handbook of clinical neurology. Amsterdam: Elsevier; 2008. p. 791808.
113. Penn DL, Komotar RJ, Sander Connolly E. Hemodynamic mechanisms under-
lying cerebral aneurysm pathogenesis. J Clin Neurosci 2011;18(11):14358.114. Polmear A. Sentinel headaches in aneurysmal subarachnoid haemorrhage: whatis the true incidence? A systematic review. Cephalalgia 2003;23(10):93541.
115. Perry JJ, Stiell IG, Sivilotti ML, et al. High risk clinical characteristics forsubarachnoid haemorrhage in patients with acute headache: prospectivecohort study. BMJ 2010;341:c5204.
116. Shinohara Y. Hemorrhagic stroke syndromes: clinical manifestations of intrace-rebral and subarachnoid hemorrhage. In: Marc F, editor. Handbook of clinicalneurology. Amsterdam: Elsevier; 2008. p. 57794.
117. Suarez JI, Tarr RW, Selman WR. Aneurysmal subarachnoid hemorrhage. N Engl
J Med 2006;354(4):38796.118. van Gijn J, Kerr RS, Rinkel GJ. Subarachnoid haemorrhage. Lancet 2007;
369(9558):30618.119. Hassan A, Lanzino G, Wijdicks E, et al. Tersons syndrome. Neurocrit Care 2011;
15(3):5548.120. Vermeulen MJ, Schull MJ. Missed diagnosis of subarachnoid hemorrhage in the
emergency department. Stroke 2007;38(4):121621.121. McCormack RF, Hutson A. Can computed tomography angiography of the brain
replace lumbar puncture in the evaluation of acute-onset headache after a nega-tive noncontrast cranial computed tomography scan? Acad Emerg Med 2010;
17(4):44451.122. Perry JJ, Stiell IG, Sivilotti ML, et al. Sensitivity of computed tomography per-
formed within six hours of onset of headache for diagnosis of subarachnoid hae-morrhage: prospective cohort study. BMJ 2011;343:d4277.
123. Provenzale J, Hacein-Bey L. CT evaluation of subarachnoid hemorrhage: a prac-tical review for the radiologist interpreting emergency room studies. Emerg Ra-diol 2009;16(6):44151.
Caceres & Goldstein792
-
8/13/2019 Intracranial+Hemorrhage (1)
23/24
124. Karttunen AI, Jartti PH, Ukkola VA, et al. Value of the quantity and distribution ofsubarachnoid haemorrhage on CT in the localization of a ruptured cerebralaneurysm. Acta Neurochir 2003;145(8):65561.
125. Tryfonidis M, Evans AL, Coley SC, et al. The value of radio-anatomical featureson non-contrast CT scans in localizing the source in aneurysmal subarachnoidhaemorrhage. Clin Anat 2007;20(6):61823.
126. Hoh BL, Cheung AC, Rabinov JD, et al. Results of a prospective protocol ofcomputed tomographic angiography in place of catheter angiography as theonly diagnostic and pretreatment planning study for cerebral aneurysms bya combined neurovascular team. Neurosurgery 2004;54(6):132940 [discus-sion: 13402].
127. Westerlaan HE, van Dijk JMC, Jansen-van der Weide MC, et al. Intracranialaneurysms in patients with subarachnoid hemorrhage: CT angiography asa primary examination tool for diagnosissystematic review and meta-analysis.Radiology 2011;258(1):13445.
128. Prestigiacomo CJ, Sabit A, He W, et al. Three dimensional CT angiographyversus digital subtraction angiography in the detection of intracranial aneu-rysms in subarachnoid hemorrhage. J Neurointerv Surg 2010;2(4):3859.
129. Diringer M, Bleck T, Claude Hemphill J, et al. Critical care management of patientsfollowing aneurysmal subarachnoid hemorrhage: recommendations from theNeurocritical Care Societys Multidisciplinary Consensus Conference. NeurocritCare 2011;15(2):21140.
130. Vermeulen M, van Gijn J. The diagnosis of subarachnoid haemorrhage. J NeurolNeurosurg Psychiatry 1990;53(5):36572.
131. Edlow JA, Panagos PD, Godwin SA, et al. Clinical policy: critical issues in theevaluation and management of adult patients presenting to the emergencydepartment with acute headache. Ann Emerg Med 2008;52(4):40736.
132. Edlow JA. What are the unintended consequences of changing the diagnosticparadigm for subarachnoid hemorrhage after brain computed tomography tocomputed tomographic angiography in place of lumbar puncture? Acad EmergMed 2010;17(9):9915 [discussion: 9967].
133. Roost KT, Pimstone NR, Diamond I, et al. The formation of cerebrospinal fluidxanthochromia after subarachnoid hemorrhage. Neurology 1972;22(9):973.
134. Petzold A, Keir G, Sharpe LT. Spectrophotometry for xanthochromia. N Engl J
Med 2004;351(16):16956.135. Wood MJ, Dimeski G, Nowitzke AM. CSF spectrophotometry in the diagnosis
and exclusion of spontaneous subarachnoid haemorrhage. J Clin Neurosci2005;12(2):1426.
136. Perry JJ, Sivilotti MLA, Stiell IG, et al. Should spectrophotometry be used toidentify xanthochromia in the cerebrospinal fluid of alert patients suspected ofhaving subarachnoid hemorrhage? Stroke 2006;37(10):246772.
137. Edlow JA, Bruner KS, Horowitz GL. Xanthochromia. Arch Pathol Lab Med 2002;126(4):4135.
138. Linn FHH, Voorbij HAM, Rinkel GJE, et al. Visual inspection versus spectropho-
tometry in detecting bilirubin in cerebrospinal fluid. J Neurol Neurosurg Psychi-atry 2005;76(10):14524.
139. Kidwell CS, Wintermark M. Imaging of intracranial haemorrhage. Lancet Neurol2008;7(3):25667.
140. Mitchell P, Wilkinson ID, Hoggard N, et al. Detection of subarachnoid haemor-rhage with magnetic resonance imaging. J Neurol Neurosurg Psychiatry 2001;70(2):20511.
Intracranial Hemorrhage 793
-
8/13/2019 Intracranial+Hemorrhage (1)
24/24
141. U-King-Im JM, Koo B, Trivedi RA, et al. Current diagnostic approaches tosubarachnoid haemorrhage. Eur Radiol 2005;15(6):113547.
142. Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair ofintracranial aneurysms. J Neurosurg 1968;28(1):1420.
143. Rosen D, MacDonald R. Subarachnoid hemorrhage grading scales. NeurocritCare 2005;2(2):1108.
144. Bederson JB, Connolly ES Jr, Batjer HH, et al. Guidelines for the management ofaneurysmal subarachnoid hemorrhage. Stroke 2009;40(3):9941025.
145. Bederson JB, Connolly ES Jr, Batjer HH, et al. Guidelines for the management ofaneurysmal subarachnoid hemorrhage: a statement for healthcare profes-sionals from a special writing group of the Stroke Council, American Heart Asso-ciation. Stroke 2009;40(3):9941025.
146. Choi K-S, Chun H-J, Yi H-J, et al. Seizures and epilepsy following aneurysmalsubarachnoid hemorrhage: incidence and risk factors. J Korean Neurosurg Soc2009;46(2):938.
147. Pinto A, Canha o P, Ferro J. Seizures at the onset of subarachnoid haemorrhage.J Neurol 1996;243(2):1614.
148. Claassen J, Hirsch L, Frontera J, et al. Prognostic significance of continuousEEG monitoring in patients with poor-grade subarachnoid hemorrhage. Neuro-crit Care 2006;4(2):10312.
149. Naidech A, Levasseur K, Liebling S, et al. Moderate hypoglycemia is associatedwith vasospasm, cerebral infarction, and 3-month disability after subarachnoidhemorrhage. Neurocrit Care 2010;12(2):1817.
150. Lee S-H, Lim J-S, Kim N, et al. Effects of admission glucose level on mortality
after subarachnoid hemorrhage: a comparison between short-term and long-term mortality. J Neurol Sci 2008;275(12):1821.151. Kruyt ND, Biessels GJ, de Haan RJ, et al. Hyperglycemia and clinical outcome
in aneurysmal subarachnoid hemorrhage. Stroke 2009;40(6):e42430.152. Fernandez A, Schmidt JM, Claassen J, et al. Fever after subarachnoid hemor-
rhage. Neurology 2007;68(13):10139.153. Schmidt JM, Wartenberg KE, Fernandez A, et al. Frequency and clinical impact
of asymptomatic cerebral infarction due to vasospasm after subarachnoidhemorrhage. J Neurosurg 2008;109(6):10529.
154. Frontera JA, Fernandez A, Schmidt JM, et al. Defining vasospasm after
subarachnoid hemorrhage. Stroke 2009;40(6):19638.155. Washington C, Zipfel G, Participants in the International Multi-disciplinary
Consensus Conference on the Critical Care Management of SubarachnoidHemorrhage. Hemorrhage, detection and monitoring of vasospasm and de-layed cerebral ischemia: a review and assessment of the literature. NeurocritCare 2011;15(2):3127.
156. Rabinstein AA, Lanzino G, Wijdicks EFM. Multidisciplinary management andemerging therapeutic strategies in aneurysmal subarachnoid haemorrhage.Lancet Neurol 2010;9(5):50419.
157. Treggiari M, Participants in the International Multi-disciplinary Consensus
Conference on the Critical Care Management of Subarachnoid Hemorrhage.Hemorrhage, hemodynamic management of subarachnoid hemorrhage. Neuro-crit Care 2011;15(2):32935.
158. Lee K, Lukovits T, Friedman J. Triple-H therapy for cerebral vasospasmfollowing subarachnoid hemorrhage. Neurocrit Care 2006;4(1):6876.
159. CARAT Investigators. Rates of delayed rebleeding from intracranial aneurysms
Caceres & Goldstein794