
Intracranial lesions mimicking neoplasms
23
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 101 Review Article Intracranial Lesions Mimicking Neoplasms Clare H. Cunliffe, MD; Ingeborg Fischer, MD; David Monoky, MD; Meng Law, MD, MBBS, FRACR; Carolyn Revercomb, MD; Susan Elrich, MD; Michael Jered Kopp, BA; David Zagzag, MD, PhD ● Context.—A broad spectrum of nonneoplastic conditions can mimic a brain tumor, both clinically and radiologically. In this review we consider these, taking into consideration the following etiologic categories: infection, demyelin- ation, vascular diseases, noninfectious inflammatory dis- orders, and iatrogenic conditions. We give an overview of such diseases, which represent a potential pitfall for pa- thologists and other clinicians involved in patient care, and present selected cases from each category. Objective.—To illustrate the radiologic and pathologic features of nontumoral intracranial lesions that can clini- cally and radiologically mimic neoplasia. Data Sources.—Case-derived material and literature re- view. Conclusions.—A variety of nonneoplastic lesions can present clinically and radiologically as primary or meta- static central nervous system tumors and result in surgical biopsy or resection of the lesion. In such situations, the pathologist has an important role to play in correctly de- termining the nature of these lesions. Awareness of the en- tities that can present in this way will assist the pathologist in the correct diagnosis of these lesions. (Arch Pathol Lab Med. 2009;133:101–123) A broad spectrum of nonneoplastic conditions can radio- logically and clinically mimic an intracranial neo- plasm. In this review, we have compiled a unique series of cas- es that presented both clinically and radiologically as in- tracranial mass lesions. Tumor was initially considered in each of the cases. However, pathology revealed a variety of nonneoplastic etiologies, including demyelinating dis- ease, vascular disease, inflammation, and infection, as well as posttreatment effects. Although tumor is often the most likely diagnostic consideration in a patient presenting with a contrast-enhancing mass lesion within the brain paren- chyma with surrounding edema and mass effect, that is not always the case. Not uncommonly, there can be sig- nificant overlap in the radiologic presentation between neoplastic and nonneoplastic diseases. Both neoplastic and nonneoplastic diseases can produce abnormal contrast en- hancement, mass effect, and perilesional edema on both computed tomography (CT) and magnetic resonance im- aging (MRI). Occasionally, some of these nonneoplastic etiologies may produce signs and symptoms mimicking tumoral disease clinically. 1 As such, these situations may Accepted for publication July 25, 2008. From the Department of Pathology, Division of Neuropathology(Drs Cunliffe, Fischer, and Zagzag) and Department of Radiology, Division of Neuroradiology (Dr Monoky), NewYork University Medical Center, New York; the Departments of Radiology and Neurosurgery, Mount Sinai Medical Center, NewYork, NY (Dr Law); the Office of the Chief Medical Examiner, Washington, DC (Dr Revercomb); the Department of Neurology,Yale University Hospital, New Haven, Conn (Dr Elrich); and the Stern School of Business, New York University, NewYork (Mr Kopp). The authors have no relevant financial interest in the products or companies described in this article. Reprints: Clare H. Cunliffe, MD, Department of Pathology, Division of Neuropathology, Mount Sinai School of Medicine, One Gustave L. Levy Place, New York, NY 10029 (e-mail: [email protected]). offer a diagnostic challenge to both the clinician and ra- diologist, and often these patients undergo biopsy. In most cases, the pathologist can readily differentiate between neoplasia and nonneoplastic imitators. However, because the benign nature of some pseudoneoplastic lesions may not be immediately apparent on pathologic examination, it behooves the pathologist to be aware of their existence. The purpose of this case series is to alert pathologists, radiologists, and other clinicians involved in the care of neurooncologic patients to consider nonneoplastic etiolo- gies in the differential diagnosis of both intra-axial and extra-axial mass lesions. Tumor-mimicking conditions from several etiologic cat- egories are presented in tabular form, including infection and inflammation, demyelinating disease, vascular dis- ease, and posttreatment conditions, with accompanying il- lustrations and discussion of the current and pertinent lit- erature. Case examples of each condition discussed are described in the Table. INFECTIONS Case Example 1: Aspergilloma The radiologic finding of erosion of the skull base by this mass lesion may have contributed to its interpretation as a destructive neoplasm, with the differential diagnosis including chondrosarcoma, metastatic lesion, osteosarco- ma, and meningioma. However, the histology in this case ruled out a diagnosis of neoplasm. Based on the hematoxylin-eosin morphology of a granulomatous process, a diagnosis of tuberculosis came to mind. Special stains for microorganisms solved this differential diagnostic dilemma, highlighting fungal hyphae with the characteristic acute angle branching of Aspergillus species. In retrospect, the history of otitis me- dia and mastoidectomy in this patient pointed toward an infectious process, even in the absence of predisposing factors such as immunosuppression or diabetes. Even
-
Upload
mario-fernando-duenas-achicanoy -
Category
Health & Medicine
-
view
81 -
download
1
Transcript of Intracranial lesions mimicking neoplasms
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 101
Review Article
Intracranial Lesions Mimicking NeoplasmsClare H. Cunliffe, MD; Ingeborg Fischer, MD; David Monoky, MD; Meng Law, MD, MBBS, FRACR; Carolyn Revercomb, MD;
Susan Elrich, MD; Michael Jered Kopp, BA; David Zagzag, MD, PhD
● Context.—A broad spectrum of nonneoplastic conditionscan mimic a brain tumor, both clinically and radiologically.In this review we consider these, taking into considerationthe following etiologic categories: infection, demyelin-ation, vascular diseases, noninfectious inflammatory dis-orders, and iatrogenic conditions. We give an overview ofsuch diseases, which represent a potential pitfall for pa-thologists and other clinicians involved in patient care, andpresent selected cases from each category.
Objective.—To illustrate the radiologic and pathologicfeatures of nontumoral intracranial lesions that can clini-cally and radiologically mimic neoplasia.
Data Sources.—Case-derived material and literature re-view.
Conclusions.—A variety of nonneoplastic lesions canpresent clinically and radiologically as primary or meta-static central nervous system tumors and result in surgicalbiopsy or resection of the lesion. In such situations, thepathologist has an important role to play in correctly de-termining the nature of these lesions. Awareness of the en-tities that can present in this way will assist the pathologistin the correct diagnosis of these lesions.
(Arch Pathol Lab Med. 2009;133:101–123)
Abroad spectrum of nonneoplastic conditions can radio-logically and clinically mimic an intracranial neo-
plasm.In this review, we have compiled a unique series of cas-
es that presented both clinically and radiologically as in-tracranial mass lesions. Tumor was initially considered ineach of the cases. However, pathology revealed a varietyof nonneoplastic etiologies, including demyelinating dis-ease, vascular disease, inflammation, and infection, as wellas posttreatment effects. Although tumor is often the mostlikely diagnostic consideration in a patient presenting witha contrast-enhancing mass lesion within the brain paren-chyma with surrounding edema and mass effect, that isnot always the case. Not uncommonly, there can be sig-nificant overlap in the radiologic presentation betweenneoplastic and nonneoplastic diseases. Both neoplastic andnonneoplastic diseases can produce abnormal contrast en-hancement, mass effect, and perilesional edema on bothcomputed tomography (CT) and magnetic resonance im-aging (MRI). Occasionally, some of these nonneoplasticetiologies may produce signs and symptoms mimickingtumoral disease clinically.1 As such, these situations may
Accepted for publication July 25, 2008.From the Department of Pathology, Division of Neuropathology (Drs
Cunliffe, Fischer, and Zagzag) and Department of Radiology, Divisionof Neuroradiology (Dr Monoky), New York University Medical Center,New York; the Departments of Radiology and Neurosurgery, MountSinai Medical Center, New York, NY (Dr Law); the Office of the ChiefMedical Examiner, Washington, DC (Dr Revercomb); the Departmentof Neurology, Yale University Hospital, New Haven, Conn (Dr Elrich);and the Stern School of Business, New York University, New York (MrKopp).
The authors have no relevant financial interest in the products orcompanies described in this article.
Reprints: Clare H. Cunliffe, MD, Department of Pathology, Divisionof Neuropathology, Mount Sinai School of Medicine, One Gustave L.Levy Place, New York, NY 10029 (e-mail: [email protected]).
offer a diagnostic challenge to both the clinician and ra-diologist, and often these patients undergo biopsy. In mostcases, the pathologist can readily differentiate betweenneoplasia and nonneoplastic imitators. However, becausethe benign nature of some pseudoneoplastic lesions maynot be immediately apparent on pathologic examination,it behooves the pathologist to be aware of their existence.
The purpose of this case series is to alert pathologists,radiologists, and other clinicians involved in the care ofneurooncologic patients to consider nonneoplastic etiolo-gies in the differential diagnosis of both intra-axial andextra-axial mass lesions.
Tumor-mimicking conditions from several etiologic cat-egories are presented in tabular form, including infectionand inflammation, demyelinating disease, vascular dis-ease, and posttreatment conditions, with accompanying il-lustrations and discussion of the current and pertinent lit-erature. Case examples of each condition discussed aredescribed in the Table.
INFECTIONSCase Example 1: Aspergilloma
The radiologic finding of erosion of the skull base bythis mass lesion may have contributed to its interpretationas a destructive neoplasm, with the differential diagnosisincluding chondrosarcoma, metastatic lesion, osteosarco-ma, and meningioma.
However, the histology in this case ruled out a diagnosisof neoplasm. Based on the hematoxylin-eosin morphologyof a granulomatous process, a diagnosis of tuberculosiscame to mind. Special stains for microorganisms solvedthis differential diagnostic dilemma, highlighting fungalhyphae with the characteristic acute angle branching ofAspergillus species. In retrospect, the history of otitis me-dia and mastoidectomy in this patient pointed toward aninfectious process, even in the absence of predisposingfactors such as immunosuppression or diabetes. Even

102 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Illustrative Case Examples With Corresponding Clinical History, Imaging Findings, Histology, and Final PathologicDiagnosis*
Case No. Age, y/Sex Clinical History Imaging Findings Imaging Differential Diagnoses
1 35/M Chronic otitis media s/p left mastoidec-tomy; headaches, fever, left-sided fa-cial numbness, diplopia, confusion
MRI: Irregularly T1 contrast enhanc-ing, centrally hypointense left skullbase lesion involving the left maxil-lary sinus, cavernous sinus (Figure1, A) with erosion of left temporalbone
Destructive neoplasm; differ-ential diagnoses: chondro-sarcoma, metastasis, osteo-sarcoma, meningioma
2 37/F 10-mo H/O severe headaches, recentonset of double vision, 14-mo H/Oamenorrhea, panhypopituitarism andDI
MRI: 1.5-cm sellar mass extending tosuprasellar cistern adjacent to carot-id arteries (Figure 2, A); low T1 sig-nal intensity with thin enhancingrim and septation (Figure 2, B)
Pituitary adenoma
3 56/F Bizarre behavior; paranoia, Kluver-Bucysyndrome
MRI: Bilateral temporal lobe lesions(Figure 3, A and B)
Infectious process, eg, herpesencephalitis, neoplasm
4 33/M Generalized seizures, s/p resection oflarge anaplastic mixed glioma, in-volving right frontal lobe and basalganglia; 2 y later, experienced 2 epi-sodes of unconsciousness
MRI: New peripherally enhancing le-sion of right frontal lobe (Figure 4,A and B) with cortical extensionand perilesional edema
Recurrent tumor
5 65/F Remote H/O breast cancer s/p right to-tal mastectomy; recent headachesand fever
MRI: Left thalamic ring-enhancing le-sion (Figure 5, A and B)
Favor metastatic neoplasmover abscess
6 60/F s/p large B-cell lymphoma and CHOPTx; new onset seizure
MRI: 1.7-cm ring-enhancing lesion,left parietal white matter; centralhypointensity on T1 (Figure 6, A),hyperintense on DWI (Figure 6, B)
Necrotic lymphoma, abscess
7 35/F Bitemporal headache, left lower extrem-ity weakness and diminished leftplantar sensation; remote PPD posi-tive, CXR negative
MRI: 3-cm right basal ganglia periph-erally enhancing lesion with sur-rounding edema and midline shift(Figure 7, A and B)
Neoplasm: primary or meta-static
8 43/M Disorientation, word-finding difficulty,right hemisensory impairment. HIVpositive, CD4 109, CSF protein 54mg/dL, glucose 53 mg/dL
MRI: Right middle cerebellar pedun-cle/hemisphere T1 hypointense, T2hyperintense lesion (Figure 8, A andB)
Inflammatory, demyelinatingor lymphoproliferative pro-cess
9 62/F Progressive headaches for 1 y; CSF:atypical lymphocytes, histiocytes, andfew eosinophils
MRI: Heterogeneous ring-enhancingsuprasellar lesion separate from pi-tuitary and stalk, near anterior com-municating artery (Figure 9, A andB)
Inflammatory process, cysticneoplasm
10 57/M s/p remote testicular cancer; 3-d H/Obitemporal headache, confusion,memory impairment
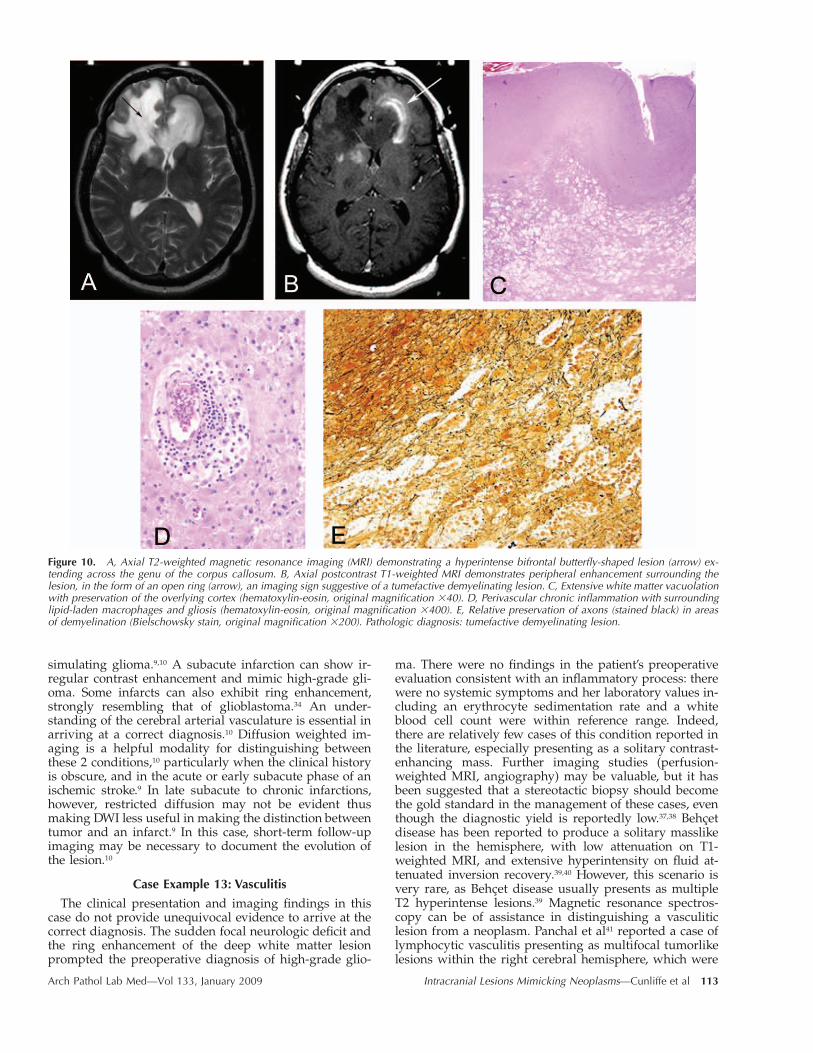
MRI: Bifrontal ‘‘butterfly’’ lesion, T2hyperintense (Figure 10, A) with fo-cal peripheral enhancement onpostcontrast T1 (Figure 10, B)
High-grade glioma
11 77/M H/O seizure disorder, hypertension2004: New onset difficulty driving,
following directions; after biopsy,steroid treatment with symptomimprovement
First MRI 2004: Large right frontalcontrast-enhancing mass and edema(Figure 11, A)
2004: neoplasm
2007: Worsening speech impairment,confusion
Second MRI 2007: Contrast-enhancingsubcortical lesion in left inferior pa-rietal lobe (Figure 11, C)
2007: Demyelination vs neo-plasm
12 64/M Headaches for 7 wk, nausea and vomit-ing, 40-lb weight loss; gait ataxia
MRI: Cerebellar enhancement withmass effect and edema (Figure 12,A); surrounding gyriform enhance-ment of folia on DWI (Figure 12, B)
Lhermitte-Duclos disease
13 43/F Sudden loss of right hand coordinationand difficulty driving
MRI: Left parietal lobe 2-cm whitematter–based lesion with irregularenhancing rim and surroundingedema (Figure 13, A and B)
High-grade glioma, lympho-ma, metastasis, abscess
14i 38/F 18-mo H/O progressive left facialnumbness, first and second divisionstrigeminal nerve
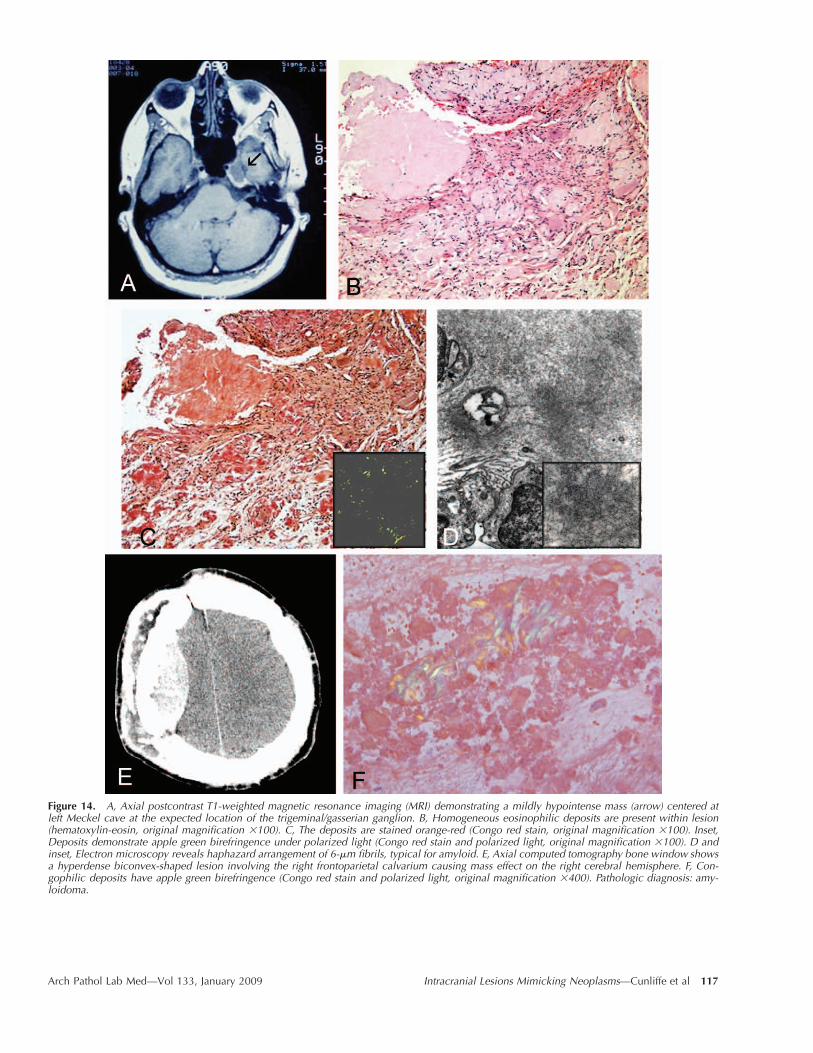
MRI: 1.5-cm hypointense mass at leftMeckel cave, involving left trigemi-nal ganglion (Figure 14, A)
Schwannoma vs meningioma
14ii 44/M 37-y H/O partial seizures, s/p resectionof right frontal and temporal seizurefocus; new onset increased seizurefrequency and left hemiparesis
CT: Hyperdense right frontoparietalvertex extra-axial mass involvingcalvarium (Figure 14, E)
Atypical meningioma, calvari-al/dural metastasis
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 103
Extended
Surgical Procedure Histology Pathologic Diagnosis
Biopsy Granulomatous inflammation with extensive necrosis (Figure 1, B), numerous mul-tinucleated giant cells (Figure 1, B, inset); GMS-positive septate hyphae withacute angle branching (Figure 1, C)
Aspergilloma
Transsphenoidal hy-pophysectomy
Nonadenomatous pituitary gland with fibrinopurulent material containing small-to medium-sized encapsulated yeast forms (Figure 2, C), strongly PAS (Figure 2,D) and GMS positive (Figure 2, E), weakly mucicarmine-positive capsules (Fig-ure 2, D, inset)
Cryptococcoma
Resection of lefttemporal lobe
Lymphohistiocytic perivascular infiltrate (Figure 3, C); macrophages with abundantfoamy cytoplasm (Figure 3, D); strongly PAS-positive bacilliform intracellular or-ganisms (Figure 3, E)
Whipple disease
Resection Bacterial abscess (Figure 4, C and D). No evidence of tumor Bacterial abscess
Biopsy Intense acute inflammation with gram-positive cocci (Figure 5, C and D); Strepto-coccus intermedius on culture
Bacterial abscess
Biopsy Neutrophilic abscess (Figure 6, D), with adjacent gliotic brain (Figure 6, C); fine,filamentous weakly gram-positive organisms (Figure 6, E, arrow); cultures grewNocardia species
Nocardiosis
Stereotactic biopsy Granulomatous inflammation with rare acid-fast bacilli (Figure 7, C through E) Tuberculoma
Biopsy Bizarre, enlarged oligodendrocytes and atypical astrocytes, background histiocyteaccumulation (Figure 8, C and D); MIB1-labeled infected cells (Figure 8, E)
PML
Biopsy Gliosis, thick-walled vessels, chronic inflammation (Figure 9, C) and numerouseosinophils (Figure 9, C, inset); eosinophilic, necrotic cystic structure with ser-rated rim (Figure 9, D)
Cysticercosis
Resection White matter vacuolation (Figure 10, C), perivascular chronic inflammation andgliosis (Figure 10, D); relative preservation of axons (Figure 10, E)
Tumefactive demyelination
2004: First biopsy First biopsy: demyelinating lesion (Figure 11, B) Demyelination
2007: Second biopsy Second biopsy: intense infiltrate of atypical B lymphocytes (Figure 11, D and E) Lymphoma
Resection Sharply demarcated necrosis, cerebellar cortex and white matter (Figure 12, C andD) with ischemic neurons, microglial proliferation, and macrophage accumula-tion (Figure 12, E)
Infarct, subacute
Resection Perivascular mixed inflammatory infiltrate (Figure 13, C and F through H), withfibrinoid necrosis of vessel walls (Figure 13, D) highlighted by azocarmine (Fig-ure 13, E)
Vasculitis
Resection Homogeneous eosinophilic extracellular deposits (Figure 14, B), congophilic (Fig-ure 14, C), apple green birefringence (Figure 14, C, inset); EM: haphazard 6-�mfibrils (Figure 14, D)
Amyloidoma
Resection Amorphous congophilic deposits with apple green birefringence (Figure 14, F) Amyloidoma
104 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Continued
Case No. Age, y/Sex Clinical History Imaging Findings Imaging Differential Diagnoses
15 33/F Recent onset of headaches MRI: Bifrontal lesion on either side offalx, with dural extension (Figure15, A and B)
Neurosarcoidosis, meningio-ma, dural metastases
16 33/M H/O seizure disorder, schizophrenia,IDDM
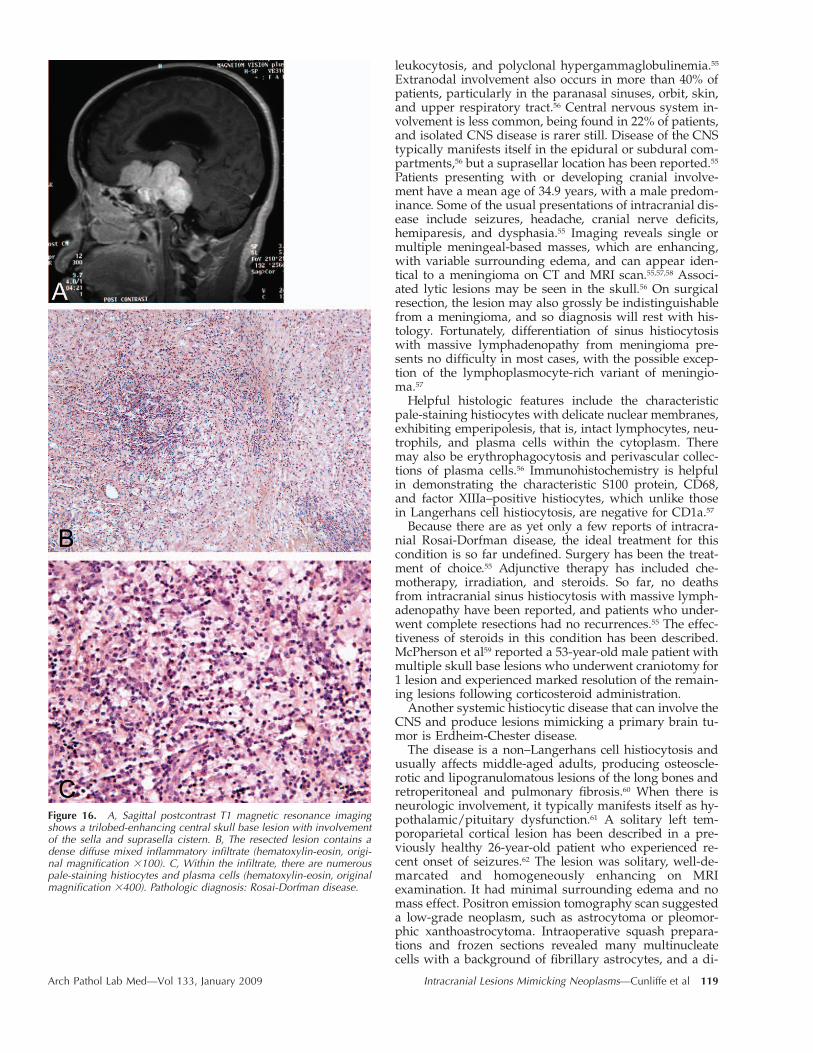
MRI: Multiple skull base lesions (Fig-ure 16, A)
Meningiomas
17 62/M H/O thyroiditis, hypertension; devel-oped vertigo, numbness left corner ofmouth, twitching left hand
MRI: Multiple enhancing lesions inleft cerebellum, corpus callosum,cingulate gyrus, pons, thalamus, su-prasellar region (Figure 17, A and B)with minimal mass effect
Neoplasm: favor metastatic
18 40/M s/p remote glioma resection; 5 y later,enlarging lesion with necrosis at siteof prior resection
MRI: Left parietal lobe lesion with pe-ripheral enhancement on T1 (Figure18, A), hyperintense, partially cysticon T2 (Figure 18, B)
Recurrent tumor with cysticchange vs radiation necrosis
* s/p indicates status post; MRI, magnetic resonance imaging; GMS, Gomori methenamine silver; H/O, history of; DI, diabetes insipidus; PAS,periodic acid–Schiff; CHOP, cyclophosphamide, adriamycin, vincristine, prednisone; Tx, treatment; DWI, diffusion weighted imaging; PPD, purifiedprotein derivative; CXR, chest x-ray; HIV, human immunodeficiency virus; CSF, cerebrospinal fluid; PML, progressive multifocal leukoencephalop-athy; EM, electron microscopy; CT, computed tomography; and IDDM, insulin-dependent diabetes mellitus.
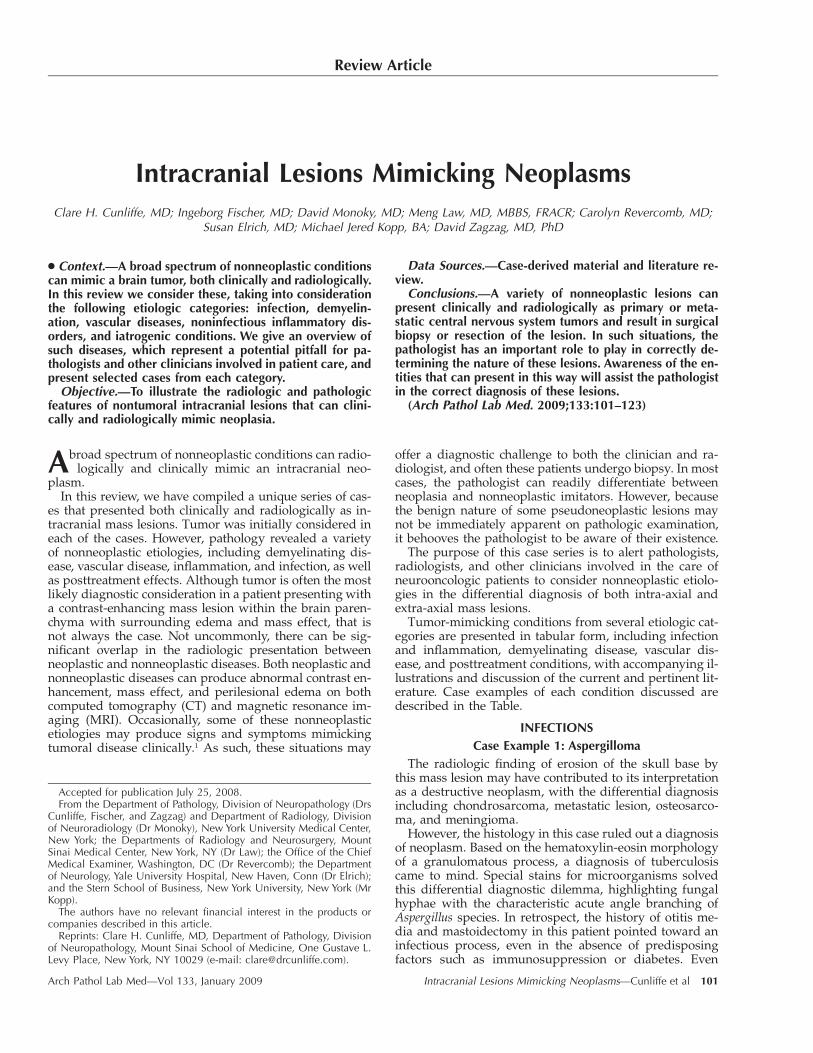
Figure 1. A, Coronal T1-weighted magnetic resonance imaging demonstrating a centrally hypointense lesion (arrow) within the left temporalbone with irregular contrast enhancement. B, Granulomatous inflammation (hematoxylin-eosin, original magnification �200). Inset, Multinucleategiant cells (hematoxylin-eosin, original magnification �400). C, Fungal hyphae with acute angle branching (Gomori methenamine silver stain,original magnification �400). Pathologic diagnosis: aspergilloma.
though most commonly occurring as an opportunistic in-fection, aspergilloma is well described in immunocompe-tent patients, especially in the context of local infection ofthe ear or paranasal sinuses.1,2
The increase in fungal central nervous system (CNS)disease seen by neurosurgeons and neuropathologists canbe attributed to the increasing numbers of immunocom-promised patients, which is due to wide use of immuno-suppressive drugs such as steroids, large elderly and di-abetic populations, and increasing numbers of long-termsurvivors of human immunodeficiency virus infection dueto antiretroviral treatment.3,4 The presentation can be veryvariable, so a high index of suspicion is required in pa-tients with a history of immunosuppression.
Intracranial fungal infection has been described follow-ing a surgical intervention, often with fatal outcome,5 As-pergillus species being the most commonly reported or-ganism in these cases. Typically, cerebral aspergillosis re-sults from hematogenous spread of the organism, or al-ternatively by direct extension from an adjacent focus ofinfection. Central nervous system Aspergillus infectionscan present either as an abscess or as cerebral infarcts but
only rarely as meningitis.6 Aspergilloma may also presentas an extra-axial mass with extension into the brain pa-renchyma. Kim et al7 described a case of extra-axial As-pergillus flavus granuloma involving the left middle andposterior cranial fossa, extending into the skull base andadjacent cerebellar parenchyma. Of note, the patient wasan immunocompetent 34-year-old man with no other sig-nificant history. Radiologically, the mass was hypointenseon T1-weighted MRI and exhibited irregular contrast en-hancement. In the case series by Dubey et al,4 patientswith intracranial fungal granuloma most commonly pre-sented with headache, followed by vomiting, proptosis,and visual disturbances. Other presentations could in-clude cranial nerve palsies and symptoms/signs of ele-vated intracranial pressure and meningismus.8 The gran-ulomas were most frequently seen in the frontal lobe, al-though a classic location of aspergillomas is in a basal cra-nial location, where it is thought to arise from aninfectious focus in the paranasal sinuses.9 In the 40 casesdescribed by Dubey et al,4 aspergilloma was the most fre-quent organism found (25, 63%), followed by mucormy-cosis (7, 18%), cryptococcoma (3), Cladosporium (3), Bipo-
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 105
Extended (Continued)
Surgical Procedure Histology Pathologic Diagnosis
Resection of firm,gray mass
Hyalinized vessels surrounded by dense lymphocytic infiltrate (Figure 15, C) of pre-dominantly B-cell type (Figure 15, D and E)
Castleman disease hyaline-vascular type
Resection Mixed inflammatory infiltrate with admixed pale-staining histiocytes (Figure 16, Band C)
Rosai-Dorfman disease
Biopsy Dense mixed inflammatory infiltrate (Figure 17, C) predominantly histiocytes and Bcells (Figure 17, D and E) with minor T-cell component (Figure 17, F)
Inflammatory pseudotumor
Resection Necrotic parenchyma with hemosiderin deposits and vascular channels (Figure 18,C and D)
Radiation necrosis
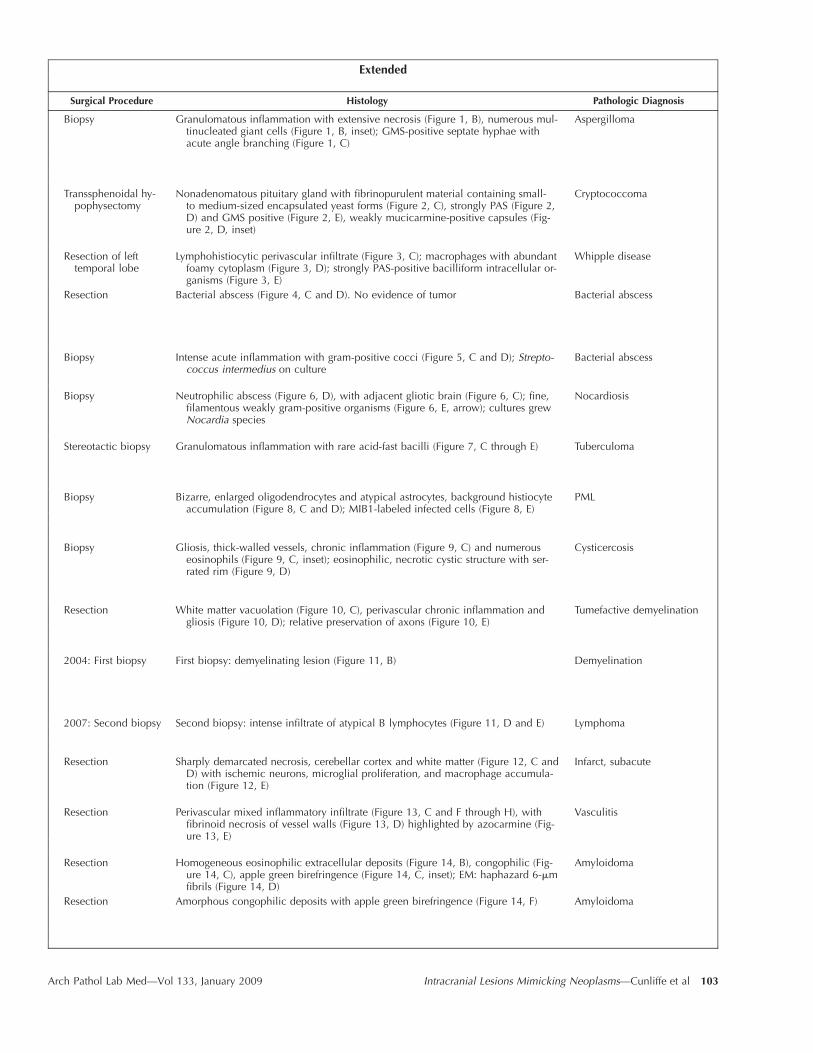
Figure 2. A, Coronal T1-weighted magnetic resonance imaging (MRI) demonstrating a centrally hypointense intrasellar mass (arrow) with a thinrim of peripheral enhancement. B, Axial T1-weighted MRI demonstrating a low signal intensity mass (arrow) within the sella with thin peripheralenhancement and a thin enhancing septation. C, Necrotic basophilic material containing small- to medium-sized oval yeast forms (hematoxylin-eosin, original magnification �200). D, Organisms are strongly periodic acid–Schiff positive (original magnification �400). Inset, Capsule oforganism is weakly mucicarmine positive (original magnification �400). E, Organisms are strongly labeled by Gomori methenamine silver stain(original magnification �400). Pathologic diagnosis: cryptococcoma.
laris hawaiiensis (1), and Candida species (1). There was a63% mortality rate in these patients, mostly due to menin-goencephalitis.
Radiologically, fungal granulomas present as enhancingmasses.9 Adjacent to the dura, they can simulate menin-giomas, even producing a dural tail sign.3 On CT scan,
they may be associated with paranasal sinusitis and smallareas of bony destruction.4 Their MRI appearances canvary somewhat depending on the organism involved. As-pergillomas tend to demonstrate intermediate signal in-tensity surrounded by perilesional edema on T2.4 How-ever, cryptococcomas have low T2-weighted signal inten-

106 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 3. A, Axial fluid-attenuated inversion recovery magnetic resonance imaging (MRI) demonstrating bilateral hyperintense temporal lobelesions (arrows), left greater than right, involving cortex and subjacent white matter. B, Axial T1-weighted postcontrast MRI demonstrating bilateralhypointense temporal lobe lesions (arrows) with peripheral enhancement and some prominent surrounding vessels. C, Perivascular lymphohistio-cytic inflammatory infiltrate (hematoxylin-eosin, original magnification �200). D, Macrophages with pale eosinophilic, foamy cytoplasm (hema-toxylin-eosin, original magnification �400). E, Brightly periodic acid-Schiff–positive intracellular organisms within macrophages (original magni-fication �400). Pathologic diagnosis: Whipple disease.
sity in contrast to the surrounding hyperintense cerebraledema. Other fungal infections such as histoplasmosis canalso simulate brain tumors radiologically.9
Case Example 2: Pituitary CryptococcomaIn immunosuppressed individuals, cryptococcal infec-
tions typically produce a diffuse meningitis, and infiltra-tion of the perivascular Virchow-Robin spaces by the or-ganism can result in the formation of small intraparen-chymal gelatinous pseudocysts, with a minimal or absentinflammatory response. In immunocompetent hosts, achronic granulomatous reaction surrounds the organismsand there is neovascular growth around the granulomas,producing contrast enhancement similar to that of pri-mary or secondary brain tumors.10,11 Cryptococcomas maybe seen in individuals with a predisposition to fungal in-fections, which may not be evident on initial inquiry, andmay require more detailed history and workup to identifyconditions such as diabetes or sarcoidosis.12 Cryptococ-comas are most commonly found in the cerebellum, brain-stem, basal ganglia, or temporoparietal lobes. Distinguish-ing them from tumors and abscesses due to other organ-
isms can be challenging because there is no distinctiveradiologic feature that is unique to cryptococcomas. Typ-ically, cryptococcal disease presents on MRI as T2 hyper-intense cystic lesions within the bilateral basal gangliawith variable enhancement and surrounding edema. Theyalso often tend to insinuate in dilated Virchow-Robin peri-vascular spaces. Enhancing cryptococcomas often do notshow restricted diffusion on diffusion-weighted imaging(DWI),9 low signal intensity on T1-weighted imaging, andlow9 or high intensity12 on T2 imaging, with uniform orring enhancement. They may also have mild surroundingedema and focal calcification within them.12 Cryptococ-comas may rarely involve the parasellar or pituitary re-gion. Yu et al13 described a case of parasellar cryptococ-coma occurring in an immunocompetent patient. The ra-diologic features of the lesion were similar to a pituitaryadenoma, showing uniform contrast enhancement, withlow signal on T1-weighted imaging and high signal on T2imaging. The contrast enhancement of the meninges ad-jacent to the cryptococcoma helped in differentiating itfrom an adenoma.

Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 107
Figure 4. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) demonstrating a peripherally enhancing lesion (arrow) withinright frontal lobe, with cortical extension. B, Axial T2-weighted MRI demonstrating marked T2 hyperintense perilesional edema (arrow) typical fora bacterial infection. C, Abscess containing dense collections of neutrophils (hematoxylin-eosin, original magnification �200). D, Edge of abscessis composed of a fibroinflammatory capsule (hematoxylin-eosin, original magnification �200). Pathologic diagnosis: bacterial abscess.
Case Example 3: Whipple Disease
Whipple disease is a chronic inflammatory disorder thatinvolves multiple organ systems, typically the gastrointes-tinal tract and musculoskeletal system.14 The causativeagent is a soil-borne gram-positive bacillus Tropherymawhippelii. The classic presentation includes fever, steator-rhea, weight loss, skin pigmentation, lymphadenopathy,and recurrent arthritis.14,15 The walls of the intestine andlymph nodes are found to contain accumulations of foamymacrophages containing the characteristic periodic acid-Schiff–positive organisms. The CNS is involved in 6% to43% of patients with Whipple disease,15 but isolated CNSdisease is very rare, with only 14 cases described in theliterature.14,15 Radiologically, the lesions are predominantlyhyperintense on T2-weighted magnetic resonance (MR)images and may show homogeneous or ring enhance-ment.15 They can be surrounded by variable perilesionaledema. Generally speaking, patients presenting with pri-mary CNS Whipple disease can be divided into 2 groups.
First, those with multiple lesions may exhibit a plethoraof neurologic symptoms and signs, including seizures,ataxia, supranuclear vertical gaze palsy, headaches, pap-illedema, hemiplegia, syndrome of inappropriate antidi-uretic hormone, and fever. Interestingly, some patientsmay develop oligoclonal bands in the cerebrospinal fluidsimilar to those found in multiple sclerosis, cerebral lupus,human immunodeficiency virus infection, and sarcoido-sis.14 Those with focal mass lesions have symptoms refer-able to the site involved. The patient described by Lohr etal15 had an isolated frontal mass in the white matter,which had MRI features suggestive of a low-grade glioma.It was T2 hyperintense, was slightly hypointense on T1-weighted images, and had subtle ring enhancement with-out perilesional edema. As in our patient, the presentationincluded behavioral changes and aggressiveness. Follow-ing resection of the mass, the characteristic perivascularfoamy macrophages containing periodic acid-Schiff–posi-tive, diastase-resistant rod-shaped organisms were seen.There was marked associated gliosis.

108 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 5. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) demonstrating a left thalamic ring–enhancing lesion (arrow). B,Axial T2-weighted MRI demonstrating a well-circumscribed T2 hyperintense left thalamic lesion (arrow) with peripheral T2 hypointense rim. C,Neutrophilic abscess with collections of basophilic organisms (hematoxylin-eosin, original magnification �400). D, Organisms are gram-positivecocci (Brown-Hopps Gram stain, original magnification �1000). Pathologic diagnosis: bacterial abscess.
Other cases of solitary CNS Whipple disease have alsoinvolved the frontoparietal regions, and in one of these,there was associated destruction of the calvarium adjacentto the lesion.16 In cases of multifocal disease, the lesionshave mostly occurred in the cortical or subcortical greymatter, involving mainly the temporal lobes and thala-mus.15 Although the clinical presentation and radiologicfindings in intracranial Whipple disease can closely mimicthose of a low-grade glioma, the histologic picture of peri-vascular foamy histiocytes should prompt the pathologistto look for the periodic acid-Schiff–positive intracellularorganisms and arrive at the correct diagnosis.
Case Examples 4 and 5: Bacterial AbscessDifferentiating between pyogenic brain abscesses and
centrally necrotic intra-axial tumors can often be challeng-ing radiologically, because both commonly demonstrate
ring enhancement and perilesional edema. A helpful find-ing on MRI examination is the presence of a hypointensecapsule on T2-weighted images, which is not usually seenin tumors.9 Diffusion weighted imaging is a well-knownand valuable radiologic tool in these cases: brain abscessestypically show markedly hyperintense signal changes onDWI, whereas the appearance of high-grade gliomasvaries from slightly hyperintense to hypointense signal.17
The apparent diffusion coefficient reveals reduced valuesin brain abscesses. These findings are, however, not en-tirely specific, because a centrally reduced apparent dif-fusion coefficient has been also reported in neoplastic le-sions.18
Case Example 6: NocardiosisBrain abscess due to Nocardia species is a rare condition,
and although it can occur in patients with an intact im-
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 109
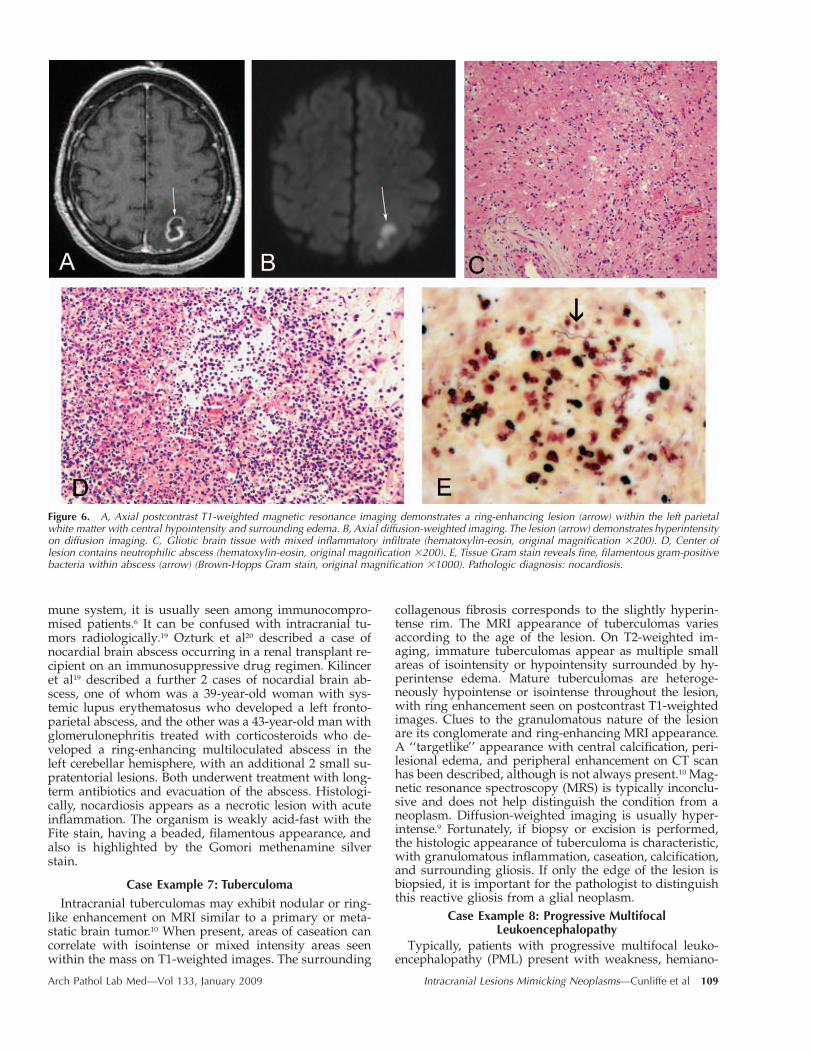
Figure 6. A, Axial postcontrast T1-weighted magnetic resonance imaging demonstrates a ring-enhancing lesion (arrow) within the left parietalwhite matter with central hypointensity and surrounding edema. B, Axial diffusion-weighted imaging. The lesion (arrow) demonstrates hyperintensityon diffusion imaging. C, Gliotic brain tissue with mixed inflammatory infiltrate (hematoxylin-eosin, original magnification �200). D, Center oflesion contains neutrophilic abscess (hematoxylin-eosin, original magnification �200). E, Tissue Gram stain reveals fine, filamentous gram-positivebacteria within abscess (arrow) (Brown-Hopps Gram stain, original magnification �1000). Pathologic diagnosis: nocardiosis.
mune system, it is usually seen among immunocompro-mised patients.6 It can be confused with intracranial tu-mors radiologically.19 Ozturk et al20 described a case ofnocardial brain abscess occurring in a renal transplant re-cipient on an immunosuppressive drug regimen. Kilinceret al19 described a further 2 cases of nocardial brain ab-scess, one of whom was a 39-year-old woman with sys-temic lupus erythematosus who developed a left fronto-parietal abscess, and the other was a 43-year-old man withglomerulonephritis treated with corticosteroids who de-veloped a ring-enhancing multiloculated abscess in theleft cerebellar hemisphere, with an additional 2 small su-pratentorial lesions. Both underwent treatment with long-term antibiotics and evacuation of the abscess. Histologi-cally, nocardiosis appears as a necrotic lesion with acuteinflammation. The organism is weakly acid-fast with theFite stain, having a beaded, filamentous appearance, andalso is highlighted by the Gomori methenamine silverstain.
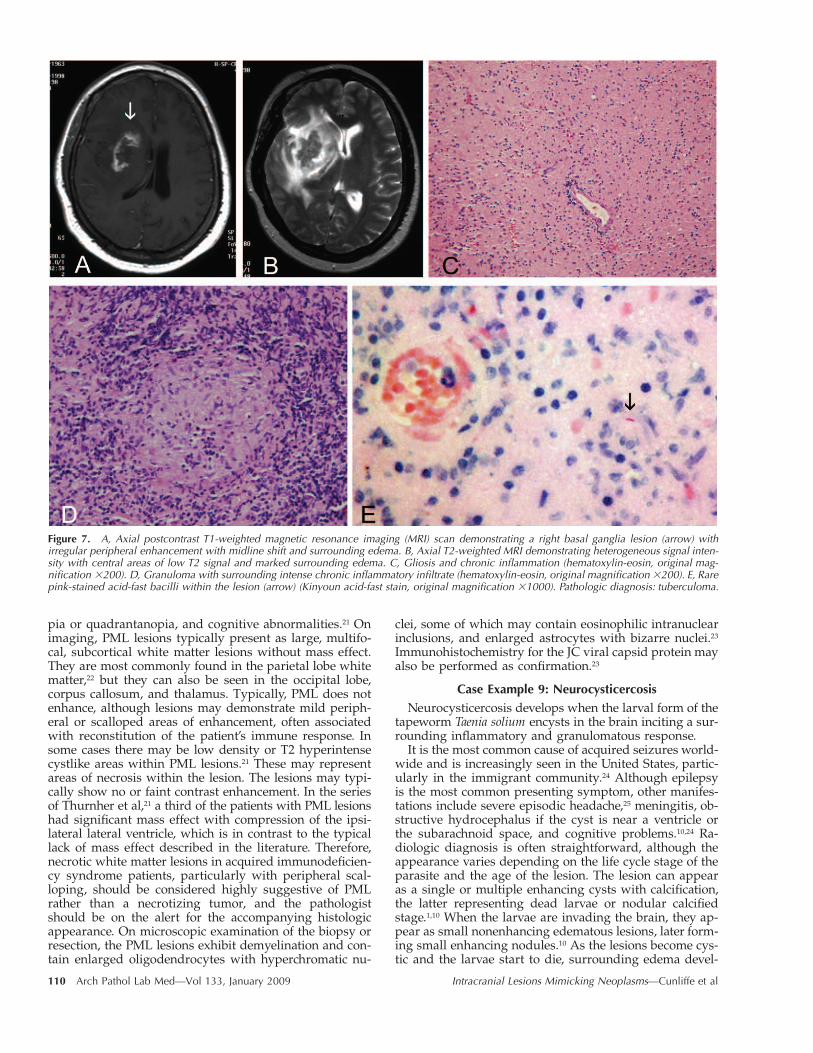
Case Example 7: TuberculomaIntracranial tuberculomas may exhibit nodular or ring-
like enhancement on MRI similar to a primary or meta-static brain tumor.10 When present, areas of caseation cancorrelate with isointense or mixed intensity areas seenwithin the mass on T1-weighted images. The surrounding
collagenous fibrosis corresponds to the slightly hyperin-tense rim. The MRI appearance of tuberculomas variesaccording to the age of the lesion. On T2-weighted im-aging, immature tuberculomas appear as multiple smallareas of isointensity or hypointensity surrounded by hy-perintense edema. Mature tuberculomas are heteroge-neously hypointense or isointense throughout the lesion,with ring enhancement seen on postcontrast T1-weightedimages. Clues to the granulomatous nature of the lesionare its conglomerate and ring-enhancing MRI appearance.A ‘‘targetlike’’ appearance with central calcification, peri-lesional edema, and peripheral enhancement on CT scanhas been described, although is not always present.10 Mag-netic resonance spectroscopy (MRS) is typically inconclu-sive and does not help distinguish the condition from aneoplasm. Diffusion-weighted imaging is usually hyper-intense.9 Fortunately, if biopsy or excision is performed,the histologic appearance of tuberculoma is characteristic,with granulomatous inflammation, caseation, calcification,and surrounding gliosis. If only the edge of the lesion isbiopsied, it is important for the pathologist to distinguishthis reactive gliosis from a glial neoplasm.
Case Example 8: Progressive MultifocalLeukoencephalopathy
Typically, patients with progressive multifocal leuko-encephalopathy (PML) present with weakness, hemiano-
110 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 7. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) scan demonstrating a right basal ganglia lesion (arrow) withirregular peripheral enhancement with midline shift and surrounding edema. B, Axial T2-weighted MRI demonstrating heterogeneous signal inten-sity with central areas of low T2 signal and marked surrounding edema. C, Gliosis and chronic inflammation (hematoxylin-eosin, original mag-nification �200). D, Granuloma with surrounding intense chronic inflammatory infiltrate (hematoxylin-eosin, original magnification �200). E, Rarepink-stained acid-fast bacilli within the lesion (arrow) (Kinyoun acid-fast stain, original magnification �1000). Pathologic diagnosis: tuberculoma.
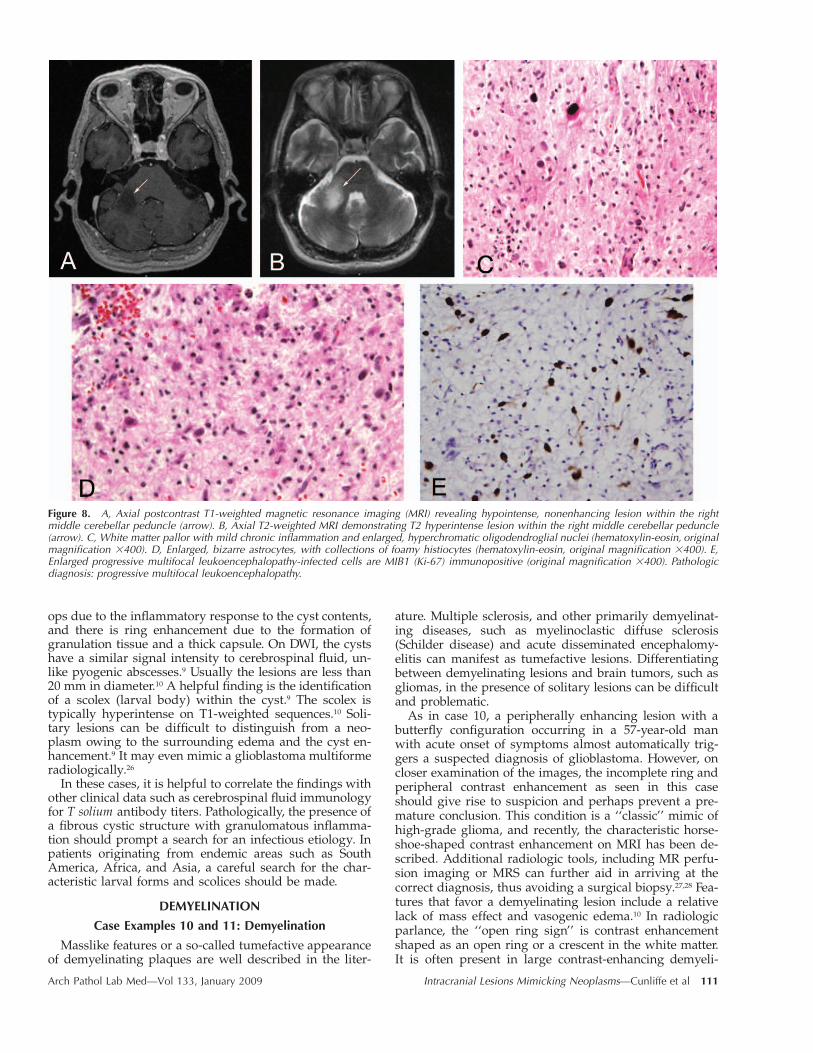
pia or quadrantanopia, and cognitive abnormalities.21 Onimaging, PML lesions typically present as large, multifo-cal, subcortical white matter lesions without mass effect.They are most commonly found in the parietal lobe whitematter,22 but they can also be seen in the occipital lobe,corpus callosum, and thalamus. Typically, PML does notenhance, although lesions may demonstrate mild periph-eral or scalloped areas of enhancement, often associatedwith reconstitution of the patient’s immune response. Insome cases there may be low density or T2 hyperintensecystlike areas within PML lesions.21 These may representareas of necrosis within the lesion. The lesions may typi-cally show no or faint contrast enhancement. In the seriesof Thurnher et al,21 a third of the patients with PML lesionshad significant mass effect with compression of the ipsi-lateral lateral ventricle, which is in contrast to the typicallack of mass effect described in the literature. Therefore,necrotic white matter lesions in acquired immunodeficien-cy syndrome patients, particularly with peripheral scal-loping, should be considered highly suggestive of PMLrather than a necrotizing tumor, and the pathologistshould be on the alert for the accompanying histologicappearance. On microscopic examination of the biopsy orresection, the PML lesions exhibit demyelination and con-tain enlarged oligodendrocytes with hyperchromatic nu-
clei, some of which may contain eosinophilic intranuclearinclusions, and enlarged astrocytes with bizarre nuclei.23
Immunohistochemistry for the JC viral capsid protein mayalso be performed as confirmation.23
Case Example 9: NeurocysticercosisNeurocysticercosis develops when the larval form of the
tapeworm Taenia solium encysts in the brain inciting a sur-rounding inflammatory and granulomatous response.
It is the most common cause of acquired seizures world-wide and is increasingly seen in the United States, partic-ularly in the immigrant community.24 Although epilepsyis the most common presenting symptom, other manifes-tations include severe episodic headache,25 meningitis, ob-structive hydrocephalus if the cyst is near a ventricle orthe subarachnoid space, and cognitive problems.10,24 Ra-diologic diagnosis is often straightforward, although theappearance varies depending on the life cycle stage of theparasite and the age of the lesion. The lesion can appearas a single or multiple enhancing cysts with calcification,the latter representing dead larvae or nodular calcifiedstage.1,10 When the larvae are invading the brain, they ap-pear as small nonenhancing edematous lesions, later form-ing small enhancing nodules.10 As the lesions become cys-tic and the larvae start to die, surrounding edema devel-
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 111
Figure 8. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) revealing hypointense, nonenhancing lesion within the rightmiddle cerebellar peduncle (arrow). B, Axial T2-weighted MRI demonstrating T2 hyperintense lesion within the right middle cerebellar peduncle(arrow). C, White matter pallor with mild chronic inflammation and enlarged, hyperchromatic oligodendroglial nuclei (hematoxylin-eosin, originalmagnification �400). D, Enlarged, bizarre astrocytes, with collections of foamy histiocytes (hematoxylin-eosin, original magnification �400). E,Enlarged progressive multifocal leukoencephalopathy-infected cells are MIB1 (Ki-67) immunopositive (original magnification �400). Pathologicdiagnosis: progressive multifocal leukoencephalopathy.
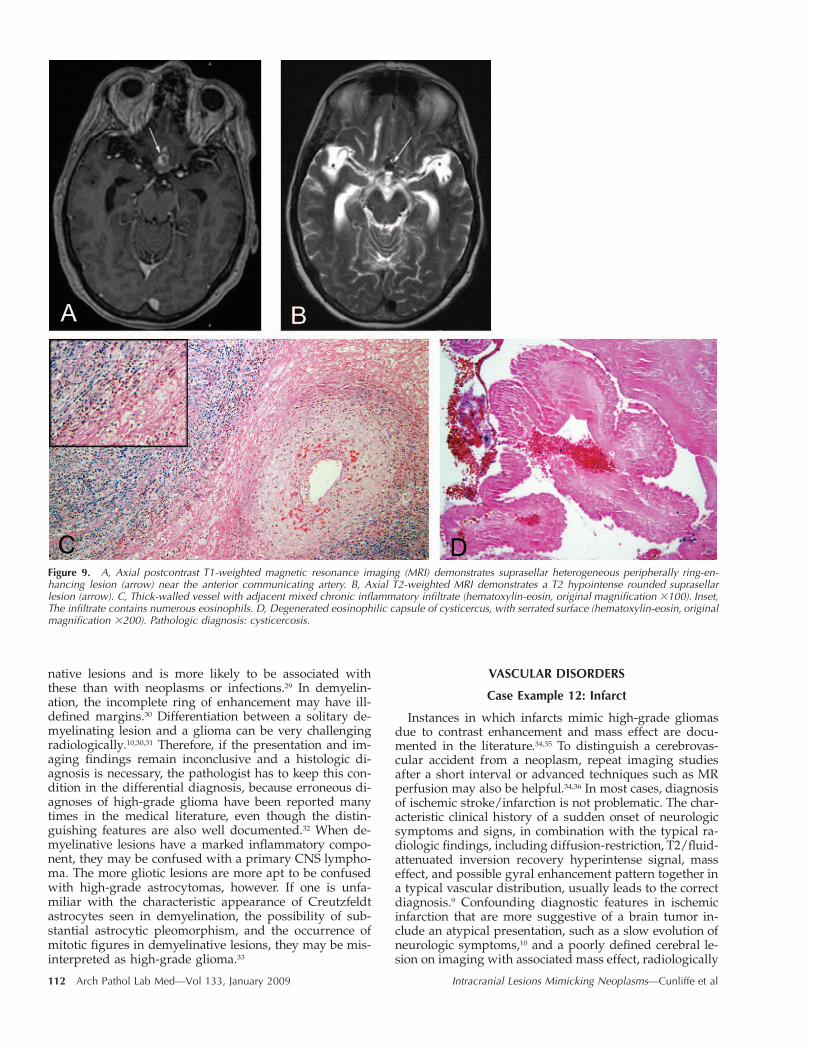
ops due to the inflammatory response to the cyst contents,and there is ring enhancement due to the formation ofgranulation tissue and a thick capsule. On DWI, the cystshave a similar signal intensity to cerebrospinal fluid, un-like pyogenic abscesses.9 Usually the lesions are less than20 mm in diameter.10 A helpful finding is the identificationof a scolex (larval body) within the cyst.9 The scolex istypically hyperintense on T1-weighted sequences.10 Soli-tary lesions can be difficult to distinguish from a neo-plasm owing to the surrounding edema and the cyst en-hancement.9 It may even mimic a glioblastoma multiformeradiologically.26
In these cases, it is helpful to correlate the findings withother clinical data such as cerebrospinal fluid immunologyfor T solium antibody titers. Pathologically, the presence ofa fibrous cystic structure with granulomatous inflamma-tion should prompt a search for an infectious etiology. Inpatients originating from endemic areas such as SouthAmerica, Africa, and Asia, a careful search for the char-acteristic larval forms and scolices should be made.
DEMYELINATION
Case Examples 10 and 11: Demyelination
Masslike features or a so-called tumefactive appearanceof demyelinating plaques are well described in the liter-
ature. Multiple sclerosis, and other primarily demyelinat-ing diseases, such as myelinoclastic diffuse sclerosis(Schilder disease) and acute disseminated encephalomy-elitis can manifest as tumefactive lesions. Differentiatingbetween demyelinating lesions and brain tumors, such asgliomas, in the presence of solitary lesions can be difficultand problematic.
As in case 10, a peripherally enhancing lesion with abutterfly configuration occurring in a 57-year-old manwith acute onset of symptoms almost automatically trig-gers a suspected diagnosis of glioblastoma. However, oncloser examination of the images, the incomplete ring andperipheral contrast enhancement as seen in this caseshould give rise to suspicion and perhaps prevent a pre-mature conclusion. This condition is a ‘‘classic’’ mimic ofhigh-grade glioma, and recently, the characteristic horse-shoe-shaped contrast enhancement on MRI has been de-scribed. Additional radiologic tools, including MR perfu-sion imaging or MRS can further aid in arriving at thecorrect diagnosis, thus avoiding a surgical biopsy.27,28 Fea-tures that favor a demyelinating lesion include a relativelack of mass effect and vasogenic edema.10 In radiologicparlance, the ‘‘open ring sign’’ is contrast enhancementshaped as an open ring or a crescent in the white matter.It is often present in large contrast-enhancing demyeli-
112 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 9. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) demonstrates suprasellar heterogeneous peripherally ring-en-hancing lesion (arrow) near the anterior communicating artery. B, Axial T2-weighted MRI demonstrates a T2 hypointense rounded suprasellarlesion (arrow). C, Thick-walled vessel with adjacent mixed chronic inflammatory infiltrate (hematoxylin-eosin, original magnification �100). Inset,The infiltrate contains numerous eosinophils. D, Degenerated eosinophilic capsule of cysticercus, with serrated surface (hematoxylin-eosin, originalmagnification �200). Pathologic diagnosis: cysticercosis.
native lesions and is more likely to be associated withthese than with neoplasms or infections.29 In demyelin-ation, the incomplete ring of enhancement may have ill-defined margins.30 Differentiation between a solitary de-myelinating lesion and a glioma can be very challengingradiologically.10,30,31 Therefore, if the presentation and im-aging findings remain inconclusive and a histologic di-agnosis is necessary, the pathologist has to keep this con-dition in the differential diagnosis, because erroneous di-agnoses of high-grade glioma have been reported manytimes in the medical literature, even though the distin-guishing features are also well documented.32 When de-myelinative lesions have a marked inflammatory compo-nent, they may be confused with a primary CNS lympho-ma. The more gliotic lesions are more apt to be confusedwith high-grade astrocytomas, however. If one is unfa-miliar with the characteristic appearance of Creutzfeldtastrocytes seen in demyelination, the possibility of sub-stantial astrocytic pleomorphism, and the occurrence ofmitotic figures in demyelinative lesions, they may be mis-interpreted as high-grade glioma.33
VASCULAR DISORDERS
Case Example 12: Infarct
Instances in which infarcts mimic high-grade gliomasdue to contrast enhancement and mass effect are docu-mented in the literature.34,35 To distinguish a cerebrovas-cular accident from a neoplasm, repeat imaging studiesafter a short interval or advanced techniques such as MRperfusion may also be helpful.34,36 In most cases, diagnosisof ischemic stroke/infarction is not problematic. The char-acteristic clinical history of a sudden onset of neurologicsymptoms and signs, in combination with the typical ra-diologic findings, including diffusion-restriction, T2/fluid-attenuated inversion recovery hyperintense signal, masseffect, and possible gyral enhancement pattern together ina typical vascular distribution, usually leads to the correctdiagnosis.9 Confounding diagnostic features in ischemicinfarction that are more suggestive of a brain tumor in-clude an atypical presentation, such as a slow evolution ofneurologic symptoms,10 and a poorly defined cerebral le-sion on imaging with associated mass effect, radiologically
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 113
Figure 10. A, Axial T2-weighted magnetic resonance imaging (MRI) demonstrating a hyperintense bifrontal butterfly-shaped lesion (arrow) ex-tending across the genu of the corpus callosum. B, Axial postcontrast T1-weighted MRI demonstrates peripheral enhancement surrounding thelesion, in the form of an open ring (arrow), an imaging sign suggestive of a tumefactive demyelinating lesion. C, Extensive white matter vacuolationwith preservation of the overlying cortex (hematoxylin-eosin, original magnification �40). D, Perivascular chronic inflammation with surroundinglipid-laden macrophages and gliosis (hematoxylin-eosin, original magnification �400). E, Relative preservation of axons (stained black) in areasof demyelination (Bielschowsky stain, original magnification �200). Pathologic diagnosis: tumefactive demyelinating lesion.
simulating glioma.9,10 A subacute infarction can show ir-regular contrast enhancement and mimic high-grade gli-oma. Some infarcts can also exhibit ring enhancement,strongly resembling that of glioblastoma.34 An under-standing of the cerebral arterial vasculature is essential inarriving at a correct diagnosis.10 Diffusion weighted im-aging is a helpful modality for distinguishing betweenthese 2 conditions,10 particularly when the clinical historyis obscure, and in the acute or early subacute phase of anischemic stroke.9 In late subacute to chronic infarctions,however, restricted diffusion may not be evident thusmaking DWI less useful in making the distinction betweentumor and an infarct.9 In this case, short-term follow-upimaging may be necessary to document the evolution ofthe lesion.10
Case Example 13: Vasculitis
The clinical presentation and imaging findings in thiscase do not provide unequivocal evidence to arrive at thecorrect diagnosis. The sudden focal neurologic deficit andthe ring enhancement of the deep white matter lesionprompted the preoperative diagnosis of high-grade glio-
ma. There were no findings in the patient’s preoperativeevaluation consistent with an inflammatory process: therewere no systemic symptoms and her laboratory values in-cluding an erythrocyte sedimentation rate and a whiteblood cell count were within reference range. Indeed,there are relatively few cases of this condition reported inthe literature, especially presenting as a solitary contrast-enhancing mass. Further imaging studies (perfusion-weighted MRI, angiography) may be valuable, but it hasbeen suggested that a stereotactic biopsy should becomethe gold standard in the management of these cases, eventhough the diagnostic yield is reportedly low.37,38 Behcetdisease has been reported to produce a solitary masslikelesion in the hemisphere, with low attenuation on T1-weighted MRI, and extensive hyperintensity on fluid at-tenuated inversion recovery.39,40 However, this scenario isvery rare, as Behcet disease usually presents as multipleT2 hyperintense lesions.39 Magnetic resonance spectros-copy can be of assistance in distinguishing a vasculiticlesion from a neoplasm. Panchal et al41 reported a case oflymphocytic vasculitis presenting as multifocal tumorlikelesions within the right cerebral hemisphere, which were

114 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 11. A, 2004 postcontrast T1-weighted axial magnetic resonance imaging (MRI) demonstrating a right frontal heterogeneously enhancingmass (arrow) with surrounding edema and mass effect. B, 2004 biopsy, with perivascular chronic inflammation and abundant foamy macrophages(Luxol fast blue and hematoxylin-eosin, original magnification �200). C, 2007 postcontrast T1-weighted axial MRI demonstrating a homogeneouslyenhancing subcortical lesion (arrow) in the left inferior parietal lobe. D, 2007 biopsy, with monotonous lymphocytic infiltrate and numerousapoptotic bodies (hematoxylin-eosin, original magnification �200). E, 2007 biopsy, infiltrate is composed of CD20 (L26) immunopositive B cells(original magnification �200). Pathologic diagnosis: demyelinating disease and central nervous system lymphoma.
enhancing on postgadolinium T1-weighted MR, with as-sociated massive vasogenic edema involving the wholehemisphere. Radiologically, the lesions mimicked a mul-tifocal glioma. However, the MRS pattern was more con-sistent with an inflammatory process (no elevated cholinepeak, marked elevation of glutamate/glutamine metabo-lites) rather than an aggressive neoplasm. The diagnosiswas confirmed by craniotomy and excisional biopsy.
AMYLOIDOSIS
Case Examples 14i and 14ii: Amyloidoma
After the initial clinical and radiologic workup, the le-sion in case 14i was thought to be a schwannoma of thefifth nerve, which would fit the imaging features and pre-sentation. A meningioma was also considered, because thelesion showed a highly suggestive ‘‘dural tail sign’’ onimaging. The absence of any evidence of systemic diseaseassociated with the deposition of amyloid in this casemade this a very difficult diagnosis.
Nonetheless, several such lesions in this location with
similar presentation and imaging findings have been re-ported. Interestingly, the deposits were histochemicallycomposed of � protein, as in the present case.42–44
The most frequent presentation of intracranial amyloidis as cerebral amyloid angiopathy, or as deposits withinthe senile plaques of Alzheimer disease. Amyloidoma isseen much less frequently. Amyloid presenting clinicallyand radiologically as an intracranial tumor is rare. Amy-loid presenting as a tumorlike mass has been reported inthe cerebral hemispheres in patients ranging in age from28 to 60 years, including the temporal45,46 and occipitallobes,46,47 and also the cerebellopontine angle.43 Typically,they appear as supratentorial white matter masses that arehigh density on nonenhanced CT scan, with little to nomass effect.48 They can extend up to the walls of the lateralventricle and have fine, irregular enhancing margins. Cen-tral nervous system amyloid can also present as multiplecontrast-enhancing lesions in the hemispheres.49
Other locations have included the Gasserian ganglion43
manifesting clinically as trigeminal neuropathy, whichhad a signal intensity similar to cortex on T1-weighted

Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 115
Figure 12. A, Axial postcontrast T1-weight-ed magnetic resonance imaging demonstrat-ing abnormal gyriform enhancement involv-ing the bilateral paramedian cerebellar hemi-spheres, left greater than right (arrow), withmass effect and edema. B, Axial diffusion-weighted imaging demonstrates gyriform hy-perintensity of the cerebellar folia (arrow),mimicking the appearance of Lhermitte-Du-clos disease. C, Sharply demarcated area ofcortical necrosis at right of field, extending tounderlying white matter (hematoxylin-eosin,original magnification �12). D, Eosinophilic,demarcated area of cortical necrosis seen atright of field (hematoxylin-eosin, originalmagnification �200). E, Numerous KP-1 im-munopositive macrophages and microgliawithin infarct (original magnification �400).Pathologic diagnosis: subacute infarct.
imaging, heterogeneous signal intensity on T2 imaging,with marked uniform enhancement on postcontrast T1imaging. The mass was thought to be a meningioma orschwannoma preoperatively. The sella50 and choroid plex-us are other known sites. Ragel et al47 described a 59-year-old man with a 6-month history of confusion and head-aches; MRI revealed a left parietooccipital lesion extend-ing to the splenium of the corpus callosum. The mass hadMRI and MRS features of a high-grade glioma, with astellate hyperintense rim on T2-weighted imaging, and el-evated choline peak on MRS. Biopsy findings were thoseof amyloidoma, with amorphous congophilic deposits andapple green birefringence. Findings not consistent withhigh-grade glioma were the lack of peritumoral edemaand minimal mass effect. Another article45 described a
right temporal lobe mass in a 51-year-old woman pre-senting with hearing loss and recurrent right-sided otitismedia. The MRI and CT findings were suspicious for gli-oma, and stereotactic biopsy with intraoperative squashpreparation followed by routine histology and electron mi-croscopy revealed amyloidoma.
Cerebral amyloid angiopathy can also mimic glioma ra-diologically and clinically. Safriel et al46 reported 2 pa-tients with MR findings suggestive of low-grade glioma.The first case was a 49-year-old man with a tumefactivemass in the occipitotemporal lobe without enhancementor restricted diffusion and unremarkable spectra. Biopsyand histopathology revealed cerebral amyloid angiopathywith angiitis. The second case was a 71-year-old womanwith an ill-defined infiltrative nonenhancing mass, with-

116 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 13. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) reveals a centrally hypointense deep left parietal lobe masslesion (arrow) with a thickened, irregular enhancing rim. B, Axial T2-weighted MRI demonstrates a rounded T2 hypointense left parietal lesion(arrow) with marked surrounding edema. C, Prominent perivascular inflammatory infiltrate (hematoxylin-eosin, original magnification �100). D,Fibrinoid necrosis of vessel wall (hematoxylin-eosin, original magnification �400). E, The fibrinoid necrosis is highlighted bright red by an azo-carmine stain (original magnification �400). F, Perivascular histiocytes within the infiltrate are immunopositive for CD68 (KP-1) (original magni-fication �200). G, Perivascular B cells are highlighted by the CD20 immunostain (original magnification �400). H, Perivascular T cells arehighlighted by the CD3 immunostain (original magnification �400). Pathologic diagnosis: vasculitis.
out restricted diffusion, within the right occipital and pa-rietal lobes, and unremarkable MRS findings. Biopsy re-vealed cerebral amyloid angiopathy. Cerebral amyloid an-giopathy may also present as a mass within the brain.Osumi et al51 describe a 59-year-old woman presentingwith a large right temporoparietal lobe mass lesion, whichwas white matter based, and was nonenhancing, nonhem-
orrhagic, and low attenuation on MRI examination. A di-agnosis of low-grade glioma was considered. Biopsy wasnondiagnostic, revealing only gliosis. Subtotal resection ofthe right temporal lobe was then performed, and histologyshowed congophilic vascular mural deposits of amyloid,with diffuse white matter gliosis and edema. There wasno evidence of tumor.
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 117
Figure 14. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) demonstrating a mildly hypointense mass (arrow) centered atleft Meckel cave at the expected location of the trigeminal/gasserian ganglion. B, Homogeneous eosinophilic deposits are present within lesion(hematoxylin-eosin, original magnification �100). C, The deposits are stained orange-red (Congo red stain, original magnification �100). Inset,Deposits demonstrate apple green birefringence under polarized light (Congo red stain and polarized light, original magnification �100). D andinset, Electron microscopy reveals haphazard arrangement of 6-�m fibrils, typical for amyloid. E, Axial computed tomography bone window showsa hyperdense biconvex-shaped lesion involving the right frontoparietal calvarium causing mass effect on the right cerebral hemisphere. F, Con-gophilic deposits have apple green birefringence (Congo red stain and polarized light, original magnification �400). Pathologic diagnosis: amy-loidoma.

118 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 15. A, Axial fluid-attentuated inversion recovery magnetic resonance imaging (MRI) demonstrates increased signal intensity bifrontally oneither side of the falx (arrow). B, Axial postcontrast T1-weighted MRI shows contrast-enhancing lesion (arrow) along the falx and frontal durabilaterally. C, A dense lymphocytic infiltrate surrounds hyalinized central vessel (hematoxylin-eosin, original magnification �400). D, The lym-phocytic infiltrate is predominantly B cells (CD20 immunostain, original magnification �400). E, There is a minor population of T cells (CD3immunostain, original magnification �400). Pathologic diagnosis: Castleman disease, hyaline-vascular type.
NONINFECTIOUS INFLAMMATORY CONDITIONS
Case Example 15: Castleman Disease
Castleman disease, also known as angiofollicular lymphnode hyperplasia, occurs in 2 forms. Most cases are thehyaline-vascular type, as in our case, with the typical his-tologic finding of hyalinized follicular centers with a ra-dial penetrating vessels and prominent interfollicular cap-illary proliferation. The plasma cell type represents only5% to 10% of cases, and is characterized by large lym-phoid follicles separated by sheets of mature plasma cellsand less stromal vascularization.52,53 Localized forms of thedisease are generally asymptomatic, while the generalizedform may present with fever, weight loss, anemia, poly-neuropathy, organomegaly, and monoclonal proteinemia,thus resembling a paraneoplastic syndrome. IntracranialCastleman disease is very rare, with 13 cases described inthe literature, and in this locality it may mimic a neo-plasm, in particular a meningioma. Previously describedlocations include the hemisphere convexities and adjacentto the falx. As expected with the predominantly corticallocation of the lesion, patients presented most commonlywith seizures, and focal signs such as right hand clumsi-ness,53 left hemiparesis, and incoherent speech.52 By CTimaging, the lesions were homogeneously enhancing with
perilesional edema.52 Some demonstrated dural enhance-ment by MRI, mimicking a meningioma.53 Angiographyof these intracranial cases revealed no vascular blush, incontrast to other sites where there is typically a homoge-neous capillary blush from neovascularization.52 Althoughmost cases occur in adults, there is a single report in an8-year-old girl.54 The child presented with sudden onsetof partial motor seizures and a left posterior parietal, par-tially mineralized, contrast-enhancing meningeal mass.
The treatment of choice for localized Castleman diseaseis gross total resection of the lesion, after which total andcomplete recovery is the rule52,54 including resolution ofthe systemic manifestations of the disorder. In summary,although it is a rare entity in the CNS, Castleman diseaseshould be considered in the differential diagnosis of in-tracranial meningeal tumors.
Case Example 16: Rosai-Dorfman Disease
Sinus histiocytosis with massive lymphadenopathy, orRosai-Dorfman disease, was first described in 1969.55 Ittypically presents in children and young adults, and hasa mean age of onset of 20.6 years, with bilateral, painlesscervical lymphadenopathy. Some patients also have sys-temic symptoms such as elevated sedimentation rate, fever,
Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 119
Figure 16. A, Sagittal postcontrast T1 magnetic resonance imagingshows a trilobed-enhancing central skull base lesion with involvementof the sella and suprasella cistern. B, The resected lesion contains adense diffuse mixed inflammatory infiltrate (hematoxylin-eosin, origi-nal magnification �100). C, Within the infiltrate, there are numerouspale-staining histiocytes and plasma cells (hematoxylin-eosin, originalmagnification �400). Pathologic diagnosis: Rosai-Dorfman disease.
leukocytosis, and polyclonal hypergammaglobulinemia.55
Extranodal involvement also occurs in more than 40% ofpatients, particularly in the paranasal sinuses, orbit, skin,and upper respiratory tract.56 Central nervous system in-volvement is less common, being found in 22% of patients,and isolated CNS disease is rarer still. Disease of the CNStypically manifests itself in the epidural or subdural com-partments,56 but a suprasellar location has been reported.55
Patients presenting with or developing cranial involve-ment have a mean age of 34.9 years, with a male predom-inance. Some of the usual presentations of intracranial dis-ease include seizures, headache, cranial nerve deficits,hemiparesis, and dysphasia.55 Imaging reveals single ormultiple meningeal-based masses, which are enhancing,with variable surrounding edema, and can appear iden-tical to a meningioma on CT and MRI scan.55,57,58 Associ-ated lytic lesions may be seen in the skull.56 On surgicalresection, the lesion may also grossly be indistinguishablefrom a meningioma, and so diagnosis will rest with his-tology. Fortunately, differentiation of sinus histiocytosiswith massive lymphadenopathy from meningioma pre-sents no difficulty in most cases, with the possible excep-tion of the lymphoplasmocyte-rich variant of meningio-ma.57
Helpful histologic features include the characteristicpale-staining histiocytes with delicate nuclear membranes,exhibiting emperipolesis, that is, intact lymphocytes, neu-trophils, and plasma cells within the cytoplasm. Theremay also be erythrophagocytosis and perivascular collec-tions of plasma cells.56 Immunohistochemistry is helpfulin demonstrating the characteristic S100 protein, CD68,and factor XIIIa–positive histiocytes, which unlike thosein Langerhans cell histiocytosis, are negative for CD1a.57
Because there are as yet only a few reports of intracra-nial Rosai-Dorfman disease, the ideal treatment for thiscondition is so far undefined. Surgery has been the treat-ment of choice.55 Adjunctive therapy has included che-motherapy, irradiation, and steroids. So far, no deathsfrom intracranial sinus histiocytosis with massive lymph-adenopathy have been reported, and patients who under-went complete resections had no recurrences.55 The effec-tiveness of steroids in this condition has been described.McPherson et al59 reported a 53-year-old male patient withmultiple skull base lesions who underwent craniotomy for1 lesion and experienced marked resolution of the remain-ing lesions following corticosteroid administration.
Another systemic histiocytic disease that can involve theCNS and produce lesions mimicking a primary brain tu-mor is Erdheim-Chester disease.
The disease is a non–Langerhans cell histiocytosis andusually affects middle-aged adults, producing osteoscle-rotic and lipogranulomatous lesions of the long bones andretroperitoneal and pulmonary fibrosis.60 When there isneurologic involvement, it typically manifests itself as hy-pothalamic/pituitary dysfunction.61 A solitary left tem-poroparietal cortical lesion has been described in a pre-viously healthy 26-year-old patient who experienced re-cent onset of seizures.62 The lesion was solitary, well-de-marcated and homogeneously enhancing on MRIexamination. It had minimal surrounding edema and nomass effect. Positron emission tomography scan suggesteda low-grade neoplasm, such as astrocytoma or pleomor-phic xanthoastrocytoma. Intraoperative squash prepara-tions and frozen sections revealed many multinucleatecells with a background of fibrillary astrocytes, and a di-

120 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
Figure 17. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) demonstrating a homogeneously enhancing left cerebellar mass(lower arrow) with perilesional edema and a second right pontine–enhancing nodule (upper arrow). B, Sagittal postcontrast T1-weighted MRI againreveals the cerebellar lesion (lower arrow) with additional enhancing lesions (upper arrows) within the corpus callosum, posterior cingulate gyrus,anterior thalamus, and suprasellar region. C, The lesion consists of a dense mixed inflammatory infiltrate (hematoxylin-eosin, original magnification�400). D, Histiocytes are present within the infiltrate (CD68 immunostain, original magnification �400). E, The B-cell component of the infiltrateis highlighted by the CD20 immunostain (original magnification �400). F, Scattered rare T cells are present within the infiltrate (CD3 immunostain,original magnification �400). Pathologic diagnosis: inflammatory pseudotumor.

Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 121
Figure 18. A, Axial postcontrast T1-weighted magnetic resonance imaging (MRI) demonstrates a well-circumscribed mass (arrow) within the leftposterior parietooccipital region with thin peripheral enhancement. B, Axial T2-weighted MRI reveals a hyperintense partially cystic lesion (arrow)with an internal fluid-fluid level. C, There is parenchymal necrosis with hemosiderin deposits and dilated vascular channels (hematoxylin-eosin,original magnification �200). D, Necrosis and hemosiderin deposits (hematoxylin-eosin, original magnification �400). Pathologic diagnosis:radiation necrosis.
agnosis of glial neoplasm was made. On permanent his-tology, clusters of xanthomatous histiocytic cells were ev-ident, many of which were multinucleate with a wreath-like nuclear arrangement, surrounded by dense gliosis.The histiocytic cells were KP-1 (CD68) immunopositiveand negative for CD1a and S100 (in contrast to those seenin Rosai-Dorfman disease or Langerhans cell histiocyto-sis).
Case Example 17: Inflammatory Pseudotumor
Inflammatory pseudotumors, also known as inflam-matory myofibroblastic tumors, may involve any organsystem.63 In the CNS, it most commonly produces a dural-based/meningeal mass, although it may be intraparen-chymal or may occasionally arise from the choroid plexus,producing a hyperdense intraventricular mass on CT im-aging.3 Shah and McClain64 described a form of inflam-matory pseudotumor (plasma cell granuloma) involvingthe cavernous sinus and middle cranial fossa in a 14-year-old girl. On MRI, it was seen to extend into the pterygo-palatine and infratemporal fossae producing thickening ofthe right lateral tentorium and edema of the right tem-poral lobe. Typically, inflammatory pseudotumor is hy-
pointense on T1-weighted images and markedly hypoin-tense on T2. Because of its polymorphous histologic ap-pearance, ranging from hypocellular connective tissuecontaining scattered mixed mononuclear inflammatorycells to a proliferation of plump fibroblastic cells with aprominent inflammatory component, it may potentially beconfused with a lymphoplasmacyte-rich meningioma oreven a fibroblastic meningioma. The radiologic appear-ance of a dural-based mass may further mislead the pa-thologist. The demographics of patients with the 2 lesionsare different, however, with most inflammatory pseudo-tumors (73%) occurring in those younger than 40 years.10
There is a distinct male predominance,10 and most casesin the CNS are solitary (82%). Intraparenchymal hetero-geneously enhancing inflammatory pseudotumors maymimic a malignant brain neoplasm.63
IATROGENIC CONDITIONSCase Example 18: Radiation Necrosis
Distinguishing between radiation necrosis and gliomarecurrence can be difficult.65 In cases of high-grade glio-ma, both are likely to be present at the same time, but inthese cases the challenge is to determine whether one or

122 Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al
the other is predominant because this may affect treat-ment planning. Increased contrast enhancement second-ary to irradiation may be seen within a variable timeframe after administration of radiotherapy. These changesmay be seen as soon as 2 to 4 months after the treatmentand may improve over time.9 Additionally, delayed radi-ation necrosis should be considered when patients presentwith a new enhancing lesion, particularly in the irradia-tion field, months or years after the end of treatment.9 Ob-viously, obtaining an accurate clinical history is importantin these cases. Diffusion weighted imaging, which showsa spotty hypointense lesion in the irradiation field, is sug-gestive of radiation necrosis.66 Radiation necrosis sharessome major MRI features with recurrent glioma, includingcontrast enhancement, vasogenic edema, and mass effect.67
However, some additional features that may favor radia-tion necrosis include conversion from no enhancement toenhancement and remote new enhancement, new periven-tricular enhancement, and ‘‘Swiss cheese’’ enhancement.68
In 1 study, MRI findings which favored recurrent tumorincluded involvement of the corpus callosum with sub-ependymal spread, corpus callosal involvement withcrossing of the midline and multifocal lesions, and thecombination of corpus callosal involvement with subep-endymal spread and multiple lesions.65 Of note, the au-thors found that these combinations of MRI findings rath-er than individual features were statistically significant.However, in many cases, the definitive diagnosis of radi-ation necrosis versus recurrent tumor rests with surgeryand biopsy.
References1. Alapatt JP, Kutty RK, Gopi PP, Challissery J. Middle and posterior fossa as-
pergilloma. Surg Neurol. 2006;66:75–78; discussion 78–79.2. Siddiqui AA, Bashir SH, Ali Shah A, et al. Diagnostic MR imaging features
of craniocerebral aspergillosis of sino-nasal origin in immunocompetent patients.Acta Neurochir (Wien). 2006;148:155–166; discussion 166.
3. Okamoto K, Furusawa T, Ishikawa K, Quadery FA, Sasai K, Tokiguchi S.Mimics of brain tumor on neuroimaging: part II. Radiat Med. 2004;22:135–142.
4. Dubey A, Patwardhan RV, Sampth S, Santosh V, Kolluri S, Nanda A. Intra-cranial fungal granuloma: analysis of 40 patients and review of the literature.Surg Neurol. 2005;63:254–260; discussion 260.
5. Dickerman RD, Stevens QE, Schneider SJ. Sudden death secondary to ful-minant intracranial aspergillosis in a healthy teenager after posterior fossa surgery:the role of corticosteroids and prophylactic recommendations. J Neurosurg Sci.2004;48:87–89; discussion 90.
6. Cunha BA. Central nervous system infections in the compromised host: adiagnostic approach. Infect Dis Clin North Am. 2001;15:567–590.
7. Kim TK, Chang KH, Kim CJ, Goo JM, Kook MC, Han MH. Intracranial tu-berculoma: comparison of MR with pathologic findings. AJNR Am J Neuroradiol.1995;16:1903–1908.
8. Murthy JM, Sundaram C, Prasad VS, Purohit AK, Rammurti S, Laxmi V. As-pergillosis of central nervous system: a study of 21 patients seen in a universityhospital in south India. J Assoc Physicians India. 2000;48:677–681.
9. Omuro AM, Leite CC, Mokhtari K, Delattre JY. Pitfalls in the diagnosis ofbrain tumours. Lancet Neurol. 2006;5:937–948.
10. Okamoto K, Furusawa T, Ishikawa K, Quadery FA, Sasai K, Tokiguchi S.Mimics of brain tumor on neuroimaging: part I. Radiat Med. 2004;22:63–76.
11. Tien RD, Chu PK, Hesselink JR, Duberg A, Wiley C. Intracranial crypto-coccosis in immunocompromised patients: CT and MR findings in 29 cases. AJNRAm J Neuroradiol. 1991;12:283–289.
12. Kanaly CW, Selznick LA, Cummings TJ, Adamson DC. Cerebellar crypto-coccoma in a patient with undiagnosed sarcoidosis: case report. Neurosurgery.2007;60:E571; discussion E571.
13. Yu YQ, Jiang XX, Gao YJ. MRI of a pituitary cryptococcoma simulating anadenoma. Neuroradiology. 1995;37:449–450.
14. Panegyres PK, Edis R, Beaman M, Fallon M. Primary Whipple’s disease ofthe brain: characterization of the clinical syndrome and molecular diagnosis. QJ Med. 2006;99:609–623.
15. Lohr M, Stenzel W, Plum G, Gross WP, Deckert M, Klug N. Whippledisease confined to the central nervous system presenting as a solitary frontaltumor: case report. J Neurosurg. 2004;101:336–339.
16. Akar Z, Tanriover N, Tuzgen S, et al. Intracerebral Whipple disease: un-usual location and bone destruction: case report. J Neurosurg. 2002;97:988–991.
17. Bink A, Gaa J, Franz K, et al. Importance of diffusion-weighted imaging in
the diagnosis of cystic brain tumors and intracerebral abscesses. Zentralbl Neu-rochir. 2005;66:119–125.
18. Tung GA, Evangelista P, Rogg JM, Duncan JA III. Diffusion-weighted MRimaging of rim-enhancing brain masses: is markedly decreased water diffusionspecific for brain abscess? AJR Am J Roentgenol. 2001;177:709–712.
19. Kilincer C, Hamamcioglu MK, Simsek O, et al. Nocardial brain abscess:review of clinical management. J Clin Neurosci. 2006;13:481–485.
20. Ozturk S, Tufan F, Alisir S, et al. A case of isolated Nocardia asteroidesbrain abscess in a kidney transplant recipient. Transplant Proc. 2006;38:3121–3124.
21. Thurnher MM, Thurnher SA, Muhlbauer B, et al. Progressive multifocalleukoencephalopathy in AIDS: initial and follow-up CT and MRI. Neuroradiology.1997;39:611–618.
22. Whiteman ML, Post MJ, Berger JR, Tate LG, Bell MD, Limonte LP. Pro-gressive multifocal leukoencephalopathy in 47 HIV-seropositive patients: neuro-imaging with clinical and pathologic correlation. Radiology. 1993;187:233–240.
23. Gallia GL, DelValle L, Laine C, Curtis M, Khalili K. Concomitant progres-sive multifocal leucoencephalopathy and primary central nervous system lym-phoma expressing JC virus oncogenic protein, large T antigen. Mol Pathol. 2001;54:354–359.
24. Shandera WX, Kass JS. Neurocysticercosis: current knowledge and ad-vances. Curr Neurol Neurosci Rep. 2006;6:453–459.
25. Rajshekhar V. Severe episodic headache as the sole presenting ictal eventin patients with a solitary cysticercus granuloma. Acta Neurol Scand. 2000;102:44–46.
26. Sabel M, Neuen-Jacob E, Vogt C, Weber F. Intracerebral neurocysticercosismimicking glioblastoma multiforme: a rare differential diagnosis in Central Eu-rope. Neuroradiology. 2001;43:227–230.
27. Cha S, Pierce S, Knopp EA, et al. Dynamic contrast-enhanced T2*-weight-ed MR imaging of tumefactive demyelinating lesions. AJNR Am J Neuroradiol.2001;22:1109–1116.
28. Saindane AM, Cha S, Law M, Xue X, Knopp EA, Zagzag D. Proton MRspectroscopy of tumefactive demyelinating lesions. AJNR Am J Neuroradiol.2002;23:1378–1386.
29. Masdeu JC, Moreira J, Trasi S, Visintainer P, Cavaliere R, Grundman M.The open ring: a new imaging sign in demyelinating disease. J Neuroimaging.1996;6:104–107.
30. Heyman D, Delhaye M, Fournier D, Mercier P, Rousselet MC, Menei P.Pseudotumoral demyelination: a diagnosis pitfall (report of three cases). J Neu-rooncol. 2001;54:71–76.
31. Pakos EE, Tsekeris PG, Chatzidimou K, et al. Astrocytoma-like multiplesclerosis. Clin Neurol Neurosurg. 2005;107:152–157.
32. Zagzag D, Miller DC, Kleinman GM, Abati A, Donnenfeld H, BudzilovichGN. Demyelinating disease versus tumor in surgical neuropathology: clues to acorrect pathological diagnosis. Am J Surg Pathol. 1993;17:537–545.
33. Kleinman GM, Miller DC. Pseudoneoplastic lesions of the central nervoussystem. In: Wick MR, Humphrey PA, Ritter JH, eds. Pathology of PseudoneoplasticLesions. Philadelphia, Pa: Lippincott-Raven; 1997:25–67.
34. Yaldizli O, Kastrup O, Wanke I, Maschke M. Basal ganglia infarction mim-icking glioblastoma. Eur J Med Res. 2005;10:400–401.
35. Wurm G, Parsaei B, Silye R, Fellner FA. Distinct supratentorial lesions mim-icking cerebral gliomas. Acta Neurochir (Wien). 2004;146:19–26; discussion 26.
36. Law M, Hamburger M, Johnson G, et al. Differentiating surgical from non-surgical lesions using perfusion MR imaging and proton MR spectroscopic im-aging. Technol Cancer Res Treat. 2004;3:557–565.
37. Lie JT. Primary (granulomatous) angiitis of the central nervous system: aclinicopathologic analysis of 15 new cases and a review of the literature. HumPathol. 1992;23:164–171.
38. Alrawi A, Trobe JD, Blaivas M, Musch DC. Brain biopsy in primary angiitisof the central nervous system. Neurology. 1999;53:858–860.
39. Bennett DL, McCabe DJ, Stevens JM, Mifsud V, Kitchen ND, GiovannoniG. Tumefactive neuro-Behcet disease. Neurology. 2004;63:709.
40. Geny C, Cesaro P, Heran F, Nguyen JP, Poirier J, Degos JD. Pseudotumoralneuro-Behcet’s disease. Surg Neurol. 1993;39:374–376.
41. Panchal NJ, Niku S, Imbesi SG. Lymphocytic vasculitis mimicking aggres-sive multifocal cerebral neoplasm: MR imaging and MR spectroscopic appear-ance. AJNR Am J Neuroradiol. 2005;26:642–645.
42. Bornemann A, Bohl J, Hey O, et al. Amyloidoma of the gasserian ganglionas a cause of symptomatic neuralgia of the trigeminal nerve: report of three cases.J Neurol. 1993;241:10–14.
43. Matsumoto T, Tani E, Fukami M, Kaba K, Yokota M, Hoshii Y. Amyloidomain the gasserian ganglion: case report. Surg Neurol. 1999;52:600–603.
44. Vorster SJ, Lee JH, Ruggieri P. Amyloidoma of the gasserian ganglion. AJNRAm J Neuroradiol. 1998;19:1853–1855.
45. Meir K, Maly B, Shoshan Y, Maly A, Soffer D. Cerebral amyloidoma di-agnosed intraoperatively with squash preparations: a case report. Acta Cytol.2005;49:195–198.
46. Safriel Y, Sze G, Westmark K, Baehring J. MR spectroscopy in the diagnosisof cerebral amyloid angiopathy presenting as a brain tumor. AJNR Am J Neuro-radiol. 2004;25:1705–1708.
47. Ragel BT, Blumenthal DT, Browd SR, Salzman KL, Jensen RL. Intracerebralamyloidoma can mimic high-grade glioma on magnetic resonance imaging andspectroscopy. Arch Neurol. 2006;63:906–907.
48. Gandhi D, Wee R, Goyal M. CT and MR imaging of intracerebral amy-

Arch Pathol Lab Med—Vol 133, January 2009 Intracranial Lesions Mimicking Neoplasms—Cunliffe et al 123
loidoma: case report and review of the literature. AJNR Am J Neuroradiol. 2003;24:519–522.
49. Blattler T, Siegel AM, Jochum W, Aguzzi A, Hess K. Primary cerebral amy-loidoma. Neurology. 2001;56:777.
50. Mori H, Mori S, Saitoh Y, Moriwaki K, Iida S, Matsumoto K. Growth hor-mone-producing pituitary adenoma with crystal-like amyloid immunohistochem-ically positive for growth hormone. Cancer. 1985;55:96–102.
51. Osumi AK, Tien RD, Felsberg GJ, Rosenbloom M. Cerebral amyloid angi-opathy presenting as a brain mass. AJNR Am J Neuroradiol. 1995;16:911–915.
52. Matsumura K, Nakasu S, Tanaka T, Nioka H, Matsuda M. Intracranial lo-calized Castleman’s disease: case report. Neurol Med Chir (Tokyo). 2005;45:59–65.
53. Hashimoto H, Iida J, Hironaka Y, Sakaki T. Intracranial Castleman’s diseaseof solitary form: case report. J Neurosurg. 1999;90:563–566.
54. Sotrel A, Castellano-Sanchez AA, Prusmack C, Birchansky S, BrathwaiteC, Ragheb J. Castleman’s disease in a child presenting with a partly mineralizedsolitary meningeal mass. Pediatr Neurosurg. 2003;38:232–237.
55. Kattner KA, Stroink AR, Roth TC, Lee JM. Rosai-Dorfman disease mimick-ing parasagittal meningioma: case presentation and review of literature. SurgNeurol. 2000;53:452–457; discussion 457.
56. McClain KL, Natkunam Y, Swerdlow SH. Atypical cellular disorders. He-matology Am Soc Hematol Educ Program. 2004:283–296.
57. Gies U, Gruia D, Lassmann H, Bergmann M. A case of rapidly progressiveRosai-Dorfman disease restricted to the central nervous system. Zentralbl Neu-rochir. 2005;66:142–146.
58. Wu M, Anderson AE, Kahn LB. A report of intracranial Rosai-Dorfmandisease with literature review. Ann Diagn Pathol. 2001;5:96–102.
59. McPherson CM, Brown J, Kim AW, DeMonte F. Regression of intracranial
Rosai-Dorfman disease following corticosteroid therapy: case report. J Neurosurg.2006;104:840–844.
60. Adle-Biassette H, Chetritt J, Bergemer-Fouquet AM, Wechsler J, MussiniJM, Gray F. Pathology of the central nervous system in Chester-Erdheim disease:report of three cases. J Neuropathol Exp Neurol. 1997;56:1207–1216.
61. Oweity T, Scheithauer BW, Ching HS, Lei C, Wong KP. Multiple systemErdheim-Chester disease with massive hypothalamic-sellar involvement and hy-popituitarism. J Neurosurg. 2002;96:344–351.
62. Rushing EJ, Bouffard JP, Neal CJ, et al. Erdheim-Chester disease mimickinga primary brain tumor: case report. J Neurosurg. 2004;100:1115–1118.
63. Hausler M, Schaade L, Ramaekers VT, Doenges M, Heimann G, SellhausB. Inflammatory pseudotumors of the central nervous system: report of 3 casesand a literature review. Hum Pathol. 2003;34:253–262.
64. Shah MD, McClain KL. Intracranial plasma cell granuloma: case reportand treatment of recurrence with methotrexate and 6-mercaptopurine. J PediatrHematol Oncol. 2005;27:599–603.
65. Mullins ME, Barest GD, Schaefer PW, Hochberg FH, Gonzalez RG, LevMH. Radiation necrosis versus glioma recurrence: conventional MR imagingclues to diagnosis. AJNR Am J Neuroradiol. 2005;26:1967–1972.
66. Sugahara T, Korogi Y, Tomiguchi S, et al. Posttherapeutic intraaxial braintumor: the value of perfusion-sensitive contrast-enhanced MR imaging for differ-entiating tumor recurrence from nonneoplastic contrast-enhancing tissue. AJNRAm J Neuroradiol. 2000;21:901–909.
67. Castel JC, Caille JM. Imaging of irradiated brain tumours: value of magneticresonance imaging. J Neuroradiol. 1989;16:81–132.
68. Kumar AJ, Leeds NE, Fuller GN, et al. Malignant gliomas: MR imagingspectrum of radiation therapy- and chemotherapy-induced necrosis of the brainafter treatment. Radiology. 2000;217:377–384.

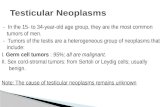
![Thrombosed Large Middle Cerebral Artery Aneurysm Mimicking … · 2015-05-05 · Intracranial aneurysms are common and affecting approxi-mately 5% of the population [4]. And MCA aneurysms](https://static.fdocuments.net/doc/165x107/5ed573adc0b3156ac4174ccc/thrombosed-large-middle-cerebral-artery-aneurysm-mimicking-2015-05-05-intracranial.jpg)


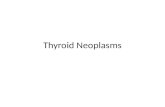



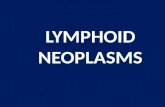


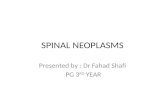



![Case Report Anaplastic meningioma: a case report and ... · Meningioma is the most common intracranial brain tumor, accounting for over one-third of primary brain neoplasms [3]. Meningioma](https://static.fdocuments.net/doc/165x107/5f0d4eca7e708231d439b3ab/case-report-anaplastic-meningioma-a-case-report-and-meningioma-is-the-most.jpg)
