Intraabdominal Abscesses: Image-GuidedDiagnosis and Therapy · 28 MODERN IMAGING TECHNOLOGY...
9
28 MODERN IMAGING TECHNOLOGY Intraabdominal Abscesses: Image-Guided Diagnosis and Therapy Russell S. Montgomery and Samuel E. Wilson From the Department of Surgery, University of California, Irvine, Irvine, California Intraabdominal abscesses may complicate many illnesses including diverticulitis, pancreatitis, and appendicitis, or they may occur during the postoperative period. As new methods of imaging are developed that provide additional information on patients with these abscesses,earlier and more accurate diagnoses can be made, allowing for prompt intervention. With the advent of these new imaging methods, techniques for treatment of abscesses by percutaneous drainage have been devel- oped. In light of these advances, we review the current strategies for the management of intraabdomi- nal abscesses. Techniques for the diagnosis and treatment of intraabdomi- nal abscesses have advanced remarkably as a consequence of the improved capability and availability of diagnostic imaging. CT and ultrasonography provide focused, objective information to expedite diagnosis and define treatment plans. Dramatic changes in the technology of these radiological techniques have expanded their applications, and image-guided therapy now provides additional approaches to drainage of intraabdominal abscesses. The mortality associated with undrained abscesses is high. Several investigators have observed that the mortality rates associated with untreated abscesses approaches 100% [1- 3]. However, as surgical drainage techniques have advanced, the mortality rates associated with this condition have fallen. These improved outcomes can be attributed to several factors includ- ing a better understanding of the pathophysiology of clinical syndromes such as acute peritonitis, sepsis, and multisystem organ failure; appreciation of the importance of early interven- tion and adequate drainage of the abscess cavity; and the advent of the diagnostic imaging techniques ultrasonography and CT. It can be difficult to make the clinical diagnosis of abdominal abscess. An abscess may be suspected on the basis of a subjec- tive history from the patient and/or on the basis of objective findings, which include fever, leukocytosis, rebound tender- ness, or a palpable mass. Despite these physical clues, the diagnosis and underlying etiology of the condition can remain elusive. Physicians can now expeditiously and accurately diag- nose intraabdominal abscesses in most patients with use of ultrasonography and the more sensitive technique of CT. Ear- lier diagnosis can be achieved, leading to immediate interven- Received 12 December 1995; revised 13 February 1996. Reprints or correspondence: Dr. Samuel E. Wilson, Department of Surgery, DCI Medical Center, 101 The City Drive South, Orange, California 92668. Clinical Infectious Diseases 1996;23:28-36 © 1996 by The University of Chicago. All rights reserved. 1058--4838/96/2301-0002$02.00 tion, treatment, and an improved chance for survival. During imaging, guided needle aspiration can be performed to obtain fluid samples. Gram staining and culturing of the fluid can then be performed to document the presence of infection and direct antibiotic therapy. Because of the high concentrations of bacte- ria within the abscess cavity, the use of both drainage and broad-spectrum antimicrobials is essential for the patient's re- covery [4]. The traditional mainstay of treatment for intraabdominal ab- scesses has been operative exploration, mechanical debride- ment, and drainage of the infected cavity. Over the past 15 years, image-guided procedures have been developed that com- plement modem surgical drainage techniques. These proce- dures have proved comparable to surgical techniques in terms of adequate drainage of the cavity and mortality rates [5- 13]. Herein we describe the clinical management options that incorporate surgical techniques and image-guided procedures for the treatment of pancreatic abscesses, diverticular ab- scesses, appendiceal abscesses, and postoperative abscesses. Diagnostic Imaging Plain films of the abdomen, radioisotope scanning, and intra- luminal contrast studies have all played a role in the diagnosis of intraabdominal abscesses. Clinical studies have demon- strated that these techniques have a diagnostic value that ranges from 15% to 50% when they are used for this purpose [14]. However, over the past 15 years, advances in cross-sectional imaging by means of CT and ultrasonography have resulted in greater diagnostic sensitivity and specificity. With the availabil- ity of these techniques, use of the older procedures for diagnos- ing intraabdominal abscesses is generally not considered bene- ficial. Ultrasonography is highly sensitive for detecting fluid within the abdomen and pelvis. The advantages of this diagnostic test include mobility (the equipment can be transported to the bedside of critically ill patients), lack of ionizing radiation, and
Transcript of Intraabdominal Abscesses: Image-GuidedDiagnosis and Therapy · 28 MODERN IMAGING TECHNOLOGY...

28
MODERN IMAGING TECHNOLOGY
Intraabdominal Abscesses: Image-Guided Diagnosis and Therapy
Russell S. Montgomery and Samuel E. Wilson From the Department ofSurgery, University of California, Irvine,Irvine, California
Intraabdominal abscesses may complicate many illnesses including diverticulitis, pancreatitis,and appendicitis, or they may occur during the postoperative period. As new methods of imagingare developed that provide additional information on patients with these abscesses,earlier and moreaccurate diagnoses can be made, allowing for prompt intervention. With the advent of these newimaging methods, techniques for treatment of abscesses by percutaneous drainage have been developed. In light of these advances, we review the current strategies for the management of intraabdominal abscesses.
Techniques for the diagnosis and treatment of intraabdominal abscesses have advanced remarkably as a consequence ofthe improved capability and availability of diagnostic imaging.CT and ultrasonography provide focused, objective informationto expedite diagnosis and define treatment plans. Dramaticchanges in the technology ofthese radiological techniques haveexpanded their applications, and image-guided therapy nowprovides additional approaches to drainage of intraabdominalabscesses.
The mortality associated with undrained abscesses is high.Several investigators have observed that the mortality ratesassociated with untreated abscesses approaches 100% [1-3].However, as surgical drainage techniques have advanced, themortality rates associated with this condition have fallen. Theseimproved outcomes can be attributed to several factors including a better understanding of the pathophysiology of clinicalsyndromes such as acute peritonitis, sepsis, and multisystemorgan failure; appreciation of the importance of early intervention and adequate drainage ofthe abscess cavity; and the adventof the diagnostic imaging techniques ultrasonography and CT.
It can be difficult to make the clinical diagnosis of abdominalabscess. An abscess may be suspected on the basis of a subjective history from the patient and/or on the basis of objectivefindings, which include fever, leukocytosis, rebound tenderness, or a palpable mass. Despite these physical clues, thediagnosis and underlying etiology of the condition can remainelusive. Physicians can now expeditiously and accurately diagnose intraabdominal abscesses in most patients with use ofultrasonography and the more sensitive technique of CT. Earlier diagnosis can be achieved, leading to immediate interven-
Received 12 December 1995; revised 13 February 1996.Reprints or correspondence: Dr. Samuel E. Wilson, Department of Surgery,
DCI Medical Center, 101 The City Drive South, Orange, California 92668.
Clinical Infectious Diseases 1996;23:28-36© 1996 by The University of Chicago. All rights reserved.1058--4838/96/2301-0002$02.00
tion, treatment, and an improved chance for survival. Duringimaging, guided needle aspiration can be performed to obtainfluid samples. Gram staining and culturing of the fluid can thenbe performed to document the presence of infection and directantibiotic therapy. Because ofthe high concentrations ofbacteria within the abscess cavity, the use of both drainage andbroad-spectrum antimicrobials is essential for the patient's recovery [4].
The traditional mainstay of treatment for intraabdominal abscesses has been operative exploration, mechanical debridement, and drainage of the infected cavity. Over the past 15years, image-guided procedures have been developed that complement modem surgical drainage techniques. These procedures have proved comparable to surgical techniques in termsof adequate drainage of the cavity and mortality rates [513]. Herein we describe the clinical management options thatincorporate surgical techniques and image-guided proceduresfor the treatment of pancreatic abscesses, diverticular abscesses, appendiceal abscesses, and postoperative abscesses.
Diagnostic Imaging
Plain films of the abdomen, radioisotope scanning, and intraluminal contrast studies have all played a role in the diagnosisof intraabdominal abscesses. Clinical studies have demonstrated that these techniques have a diagnostic value that rangesfrom 15% to 50% when they are used for this purpose [14].However, over the past 15 years, advances in cross-sectionalimaging by means of CT and ultrasonography have resulted ingreater diagnostic sensitivity and specificity. With the availability ofthese techniques, use ofthe older procedures for diagnosing intraabdominal abscesses is generally not considered beneficial.
Ultrasonography is highly sensitive for detecting fluid withinthe abdomen and pelvis. The advantages of this diagnostictest include mobility (the equipment can be transported to thebedside of critically ill patients), lack of ionizing radiation, and

em 1996;23 (July) Imaging of Intraabdominal Abscesses 29
greater cost-effectiveness than other methods of diagnosis. Thesensitivity of ultrasonography for localizing fluid collections isrelated to its use in specific regions within the abdomen. If thepatient has not previously undergone surgery, the left and rightupper quadrants and the pelvis can be accurately visualized.Once a fluid collection is discovered, the differences betweenone that is infected and one that is sterile can be subtle. Theshape of the cavity walls, the presence of debris, internal echogenicity, and the presence of gas within fluid collections allmay suggest infection; however, an absolute diagnosis cannotbe made. Technical limitations may also be present: the utilityof ultrasonography can be limited by the presence of bone orsurgical wounds or by the size of the patient, which may prevent imaging of all areas in the abdomen and pelvis. Duringthe postoperative period, when fluid collections and gaseousbowel distention (ileus) are common, the interpretability anddiagnostic capabilities of ultrasonography may be significantlyreduced [5, 15, 16].
CT is currently considered the study ofchoice for the diagnosis of an intraabdominal abscess [15, 17-20]. CT is moreaccurate than ultrasonography, provides high anatomic resolution, and is less operator dependent than is ultrasonography.CT allows visualization of retroperitoneal structures and intraluminal fluid collections, which may not be visualized whenother imaging techniques are used. The presence of a fluidcollection is suspected when areas of low attenuation (0-50Hounsfield units) are detected in an extraluminal space orwithin a parenchymal organ. The shape of the cavity walls andthe presence of debris, loculations, and gas are all suspiciousof infection on both ultrasonograms and computed tomograms.Contrast enhancement may be used to define a cavity wall, butaccurate differentiation between sterile fluid collections andinfected fluid collections is not possible.
Diagnostic fluid aspiration under CT guidance confirms thatfluid is infected and allows for prompt, definitive managementby means of surgical or percutaneous drainage. While superficial, large cavities and intraparenchymal cavities can be easilylocated with ultrasonography, CT-guided procedures have theadvantage of penetrating small, deeper fluid collections. Thehigh anatomic resolution of CT is useful in determining a safepathway for accurate fluid aspiration and possible percutaneousdrainage.
The route selected in performing needle aspiration is important, as passage of the needle through a loop of bowel maylead to infection of a sterile fluid collection, resulting in afalse-positive diagnosis. Performance of fine-needle aspirationprovides important information for the treatment of intraabdominal abscesses. The results of gram staining and culture ofthe aspirate guide selection of appropriate antibiotic agents,and additional information regarding the character, viscosity,and cellularity of the aspirate guides consideration of percutaneous drainage procedures.
A well-defined unilocular cavity, a safe drainage route, absence of excessive cellular debris, low viscosity of the fluid,
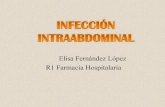
Figure 1. CT image demonstrating successful percutaneous drainage of a posterior intraabdominal abscess. The trocar catheter technique was used to enter the abscess cavity.
and immediate surgical access if failure or a complication occurs are several criteria for successful percutaneous drainage.Percutaneous drainage can be performed by means of severalmethods. The two basic drainage techniques used are the Seldinger tandem catheter system and the trocar catheter (singlepuncture) technique. The Seldinger tandem catheter techniquedeploys a drainage catheter over a guide wire and is preferredwhen abscesses are small, deep, parenchymal, or in proximityto loops of bowel. The trocar catheter technique is generallyused for larger, more accessible lesions (figure I). With bothsystems, syringe suction is initially used to aspirate material.followed by placement of a drainage bag or bulb suction device[16].
Percutaneous vs. Operative Drainage
During the past 15 years, many studies have been conductedto compare the results ofpercutaneous drainage with the resultsof surgical drainage in patients with intraabdominal abscesses.Most of these studies were neither randomized nor prospectiveand included patients with abscess cavities of different etiologies (i.e., diverticular, appendiceal, and postoperative.) Thefindings suggest that percutaneous drainage of an abscess canbe performed as safely as can surgical drainage, with a similaroutcome.
The most important consideration in choosing a drainagetechnique, independent of the technique itself, is the severityof illness of the patient with an intraabdominal abscess. Recentliterature in which percutaneous and surgical drainage techniques were compared indicates that an objective severity-ofillness scoring system is prognostic in terms of morbidity andmortality [9, 10]. A widely used system for the evaluation ofseverity of illness is APACHE (Acute Physiology and ChronicHealth Evaluation) II, developed by Knaus et al. [21]. In 1991.

30 Montgomery and Wilson em 1996;23 (July)
Table 1. Resultsof intraabdominal abscessdrainage by meansof radiological and surgical procedures.
No. of patients No. of deathsTotal no. of who underwent drainage Success rate (mortality rate
Reference patients (type ofdrainage) (%) in percentage)
[8] 119 119 (Radiological) 76 19 (16)
[9] 83 42 (Radiological) 93 ... (14)41 (Surgical) ... (12)
[13] 89 29 (Radiological) 80 5 (17)60 (Surgical) 81 10(17)
[12] 91 45 (Radiological) 47* 13 (29)46 (Surgical) 54* 13 (28)
[22] 48 18 (Radiological) 67 2 (11)30 (Surgical) 51 8 (27)
[23] 200 200 (Radiological)' 88 10 (5)
* Initial drainage procedure was successful; no further intervention was needed.t Treated byultrasonographically guided drainage.
Hemming et al. [9] described 83 patients with intraabdominalabscesses treated by surgical drainage or percutaneous drainage. The groups were matched for age, abscess location, andetiology of the abscess cavity. No significant difference wasfound in terms of morbidity or mortality between the twogroups; however, APACHE II scores were found to be significantly associated with prognosis.
In 1991, Levison and Zeigler [12] reviewed the cases of 91patients with postoperative abscesses who underwent eitherpercutaneous or surgical drainage. The two groups of patientswere similar with respect to age, sex, abscess location, andseverity of illness as determined by APACHE II. The initialmethod of drainage was selected by the attending physician.
The overall mortality rate was 29% (26 of 91 patients). Whenthe results of percutaneous drainage and operative drainagewere compared, no difference in outcome was demonstratedfor patients with an APACHE II score of < 14 or >25. Theoutcomes for patients with APACHE II scores between 14 and24 were significantly better when they were treated by operativedrainage. In this study, X2 analysis demonstrated independencebetween outcome and drainage technique. Severity of illnesswas a significant factor in patient survival.
Additional studies have demonstrated that percutaneousdrainage can be as effective as traditional surgical managementof intraabdominal abscesses (table 1). In terms of patient survival, early detection and treatment of infection to preventclinical deterioration and sepsis appear to be crucial for moreseverely ill patients.
Drainage of Specific Abscess Cavities
The differences in the underlying causes and sources ofabscesses are important for planning an approach for intervention and treatment. Regardless ofthe technique used for diagnosis, the treating physician must carefully analyze all objectivedata before draining the infected cavity. Contraindications for
percutaneous drainage must be carefully assessed, and therapyshould be immediately instituted to prevent delay and deterioration in the patient's clinical condition. The remainder of thisarticle will focus on specific types of abscess cavities and theirtreatments.
Pancreatic fluid collections. Alcoholism and gallstones account for the majority of cases of acute pancreatitis seen in theUnited States. The diagnosis of acute pancreatitis is traditionally a matter of clinical judgment based on analysis of thepatient's history, physical examination findings, andenzyme levels. Contrast-enhanced CT has become the imagingstudy of choice as a supplement to traditional diagnostic techniques for evaluation of pancreatic morphology and detection
of local complications of pancreatitis [24-27]. Contrastenhanced CT allows quantitation of size, location, and extentof involvement of the pancreas and surrounding retroperitonealtissues. This information can be instrumental in guiding therapeutic decisions in advanced cases and in guiding percutaneousfine-needle aspiration if infection is suspected.
The treatment of acute pancreatitis and its complications remains controversial. One reason for this is that the terminologyused to describe similar clinical conditions is confusing and oftenconflicting. Several classificationsystems exist for staging ofacutepancreatitis. For the purposes of this discussion, we have followedthe clinically based classification system for acute pancreatitis, asproposed at the International Symposium on Acute Pancreatitisin 1992 [28]. Acute pancreatitis can be divided into four maincategories based on clinical findings, laboratory results, ultrasonography findings, and CT findings. These categories are acutepancreatitis (mild and severe), pancreatic necrosis, pancreatic abscess, and pseudocyst due to acute pancreatitis.
Mild acute pancreatitis is not associated with any systemiccomplications and is characterized by prompt resolution ofsymptoms and objective findings. CT or ultrasonography isusually performed within 1 week of the patient's initial presentation and can be helpful in determining the severity, complica-

em 1996; 23 (July) Imaging of Intraabdomina1 Abscesses 31
tions, and possible outcome of the disease [27]. Pancreatitiscan frequently be associated with early acute fluid collections.These fluid collections occur in approximately one-third ofpatients with acute pancreatitis, up to half of which resolvespontaneously [24, 25]. The clinical significance of a fluidcollection can be related to its size, as measured by CT. Fluidcollections >7 em in diameter are more likely to require intervention, especially if they are due to alcoholic pancreatitis [24,29, 30].
Approximately 50% of acute fluid collections resolve, anddrainage procedures are not indicated until they mature intopseudocysts, unless they become infected. If the patient develops a fever that is unresponsive to conservative medical management, CT-guided fine-needle aspiration can aid in diagnosisand direction of antibiotic therapy. Severe acute pancreatitiscan be associated with organ failure and, subsequently, localcomplications such as necrosis, abscess, or pseudocyst.
Pancreatic necrosis involves injury to acinar cells, islet cells,and the pancreatic ductal system and results in extensive fatnecrosis and focal areas of nonviable pancreatic parenchyma[28]. Dynamic CT, showing contrast density that does not exceed 50 Hounsfield units in pancreatic parenchyma larger than3 em or in > 30% of the pancreas, can be used to make thisdiagnosis [31]. When pancreatic injury occurs, concomitantinfection may be present. Secondary bacterial infections of thenecrosis can occur in 40%-60% of patients; these infectionsare most frequently due to gram-negative organisms includingEscherichia coli, Klebsiella species, Pseudomonas species, andEnterococcus species. Bacterial translocation and migrationthrough microperforations ofthe transverse colon are suspectedsources of infection. In --"20% of cases, Staphylococcus speciesor Streptococcus species are the offending agents, and in 5%10% of cases, Candida is the cause [32].
It is most important to distinguish between sterile and infected necrotizing pancreatitis. Fluid obtained by CT-guidedfine-needle aspiration should be examined to determine thepresence of bacteria. In 1985, vanSonnenberg et al. [33] wereable to successfully diagnose complicated inflammatory pancreatic disease in 43 of 45 patients by means of CT-guidedfine-needle aspiration. They were able to obtain fluid, including"extremely thick material," with use of 22-gauge needles, 20gauge needles, and 18-gauge needles. No material was aspirated from two of their patients despite the use of the largerneedles.
The treatment of necrotizing pancreatitis remains controversial. In the absence of bacterial contamination and pancreaticnecrosis, image-guided therapy should not be attempted because it may predispose to infection, resulting in the need forsurgical debridement [34]. When bacterial contamination ispresent, the character of the pancreatic inflammation and fluidcollection should be carefully evaluated. Homogeneous or heterogeneous soft-tissue peripancreatic collections, thick necroticpancreatic tissue, and hemorrhagic areas of high attenuationare not amenable to percutaneous drainage, and they should
be considered contraindications to this mode of treatment [35].Patients with these conditions may require surgical "necrosectomy" and debridement or angiographic embolization of ableeding vessel [36]. Completely liquefied areas of pancreaticnecrosis may be amenable to CT-guided drainage in carefullyselected instances. The decision to apply this technique is basedon CT findings, results of needle aspiration, and the clinicalcondition of the patient. Poor drainage from the catheter ordeterioration in the patient's condition should lead to promptreevaluation and, possibly, surgical intervention.
The presence of pus (in association with a culture positivefor bacteria or fungi) in a pancreatic or peripancreatic fluidcollection that contains little or no necrotic material differentiates a pancreatic abscess from acute pancreatitis or necrotizingpancreatitis [28]. It is important to differentiate between abscess and pancreatitis because the risk of death is almost doublewhen pancreatic necrosis is present [33, 37]. Pancreatic abscesses may be amenable to percutaneous drainage. To date,the traditional approach to the treatment of patients with necrotizing pancreatitis has been surgical; however, in selected instances percutaneous drainage may be performed. Followinginitial diagnostic imaging with CT, treatment has been predicated on the clinical stability of the patient and the confirmedpresence of pus in an aspirate.
Several clinical studies have demonstrated successful percutaneous drainage of pancreatic abscesses: success rates in thedefinitive management of this condition have ranged from 32%to 79% [38-42]. Furthermore, vanSonnenberg and colleagues[39] have suggested that percutaneous drainage of complicatedabscess cavities may be used as a temporizing measure incritically ill patients before definitive surgical intervention. Asmore studies and long-term analysis of these patients becomeavailable, a better understanding of the role of image-guidedpercutaneous drainage will be obtained.
Percutaneous drainage guided by ultrasonography, CT, andendoscopic techniques challenge traditional surgical approaches to the treatment of pancreatic pseudocysts due topancreatitis in terms of efficacy. The success of surgical management with internal drainage is well documented. A mortalityrate of 2% and a recurrence rate of 5% has been demonstratedwith internal drainage of mature, uncomplicated pseudocysts[43]. Image-guided therapy is now an adjunct to current therapeutic techniques in the management of pancreatic pseudocysts.Fluid collections with low attenuation and no evidence of thickcellular debris can be considered candidates for a percutaneousprocedure. The location of the fluid collection is important,and selection of patients can influence the choice of drainageprocedure.
Percutaneous drainage can be considered for patients whoare poor candidates for surgery but have symptoms related totheir pseudocysts [44]. Since most of these fluid collectionsresolve, percutaneous drainage should be reserved for largerpseudocysts; those that are larger than 4-6 em usually requireintervention [24, 29, 30]. Prior to planning definitive therapy,

32 Montgomery and Wilson CID 1996;23 (July)
it may be useful to perform endoscopic retrograde cholangiopancreatography to determine ductal anatomy; this procedureallows for accurate prediction of drainage success. Ductal obstruction may indicate a failure of treatment predisposing topancreatic fistula [33].
Studies are also in progress to assess the effectiveness ofconcomitant administration of octreotide acetate in decreasingthe incidence of recurrence of pseudocysts and the incidenceofpancreatic fistulas when percutaneous drainage is performed.[45]. Newer therapeutic techniques, including percutaneousgastrostomy and percutaneous gastroenterostomy, for whichCT is used, are currently being investigated. The disadvantagesof percutaneous drainage include the development of an external pancreatic fistula that is present for a prolonged period anda drain-track infection rate of almost 50% [46].
Diverticular disease. The prevalence of diverticular disease reportedly ranges from 5% to 50% in populations thatadopt a Western diet [47]. The diagnosis of acute diverticulitiscan be made easily for patients with diverticula of the colon.The use ofultrasonography and CT has made accurate anatomicdefinition of acute diverticulitis possible. Moreover, currentaccepted management of acute diverticulitis depends on accurate diagnosis, staging, and extent ofcolonic involvement. Overthe past 10 years, advances in the use of image-guided drainagehave complemented traditional surgical approaches in the definitive management of this condition.
The treatment of diverticulitis depends on the severity of thedisease. The traditional focus has been on conservative medicalmanagement with low-residue diets, bowel rest, and antibiotictherapy. When operative intervention becomes necessary, resection can occur in one-, two-, or three-stage procedures. Onestage procedures consist ofresection of the diseased segment ofcolon followed by primary anastomosis. Two-stage proceduresconsist of initial resection ofthe diseased segment, with formation of a temporary end colostomy and a second-stage takedown colostomy at a later date. Three-stage procedures initiallyconsist of drainage of the diseased region of bowel and placement of a temporary proximal diverting colostomy, followedby resection of the diseased segment, primary anastomosis, andsubsequent closure of the colostomy. Each of these proceduresis tailored to the intensity of the disease process [48].
The severity of acute diverticulitis varies in relation to theextent of involvement of the colonic wall and the extent of inflammation. CT and ultrasonography are useful techniques forstaging this disease. The extent of involvement must be determined before the best treatment options can be instituted. StageI lesions consist ofmicroabscessesof the colonic wall and peridiverticular inflammation. Stage 2 lesions are small, well-definedmacroabscesses contained within the mesentery or epiploic appendages of the colon. Patients with well-definedmacroabscesses(larger pericolic abscesses and pelvic abscesses) related to diverticular perforation have stage 3 disease, and patients with generalized peritonitis that results from a perforated diverticular abscessor from fecal peritonitis have stage 4 disease.
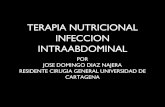
Figure 2. CT images showing the management of a diverticularpelvic abscess by percutaneous drainage. This patient was later treatedwith a one-stage operation, eliminating the need for a colostomy. A:pelvic diverticular abscess with air-fluid levels; B: confirmation ofinfection and drainage route by placement of a percutaneous needle;C: deployment of the catheter into the abscess cavity.

em 1996;23 (July) Imaging of Intraabdominal Abscesses
Table 2. Image-guided management of diverticular abscesses.
No. (%) of patients No. (%) of patientsNo. (%) of patients who underwent who underwent
who underwent percutaneous drainage percutaneous drainageTotal no. percutaneous plus one-stage plus two-stage
Reference of patients drainage alone surgical procedure surgical procedure
[49] 19* None 14 (74) 3 (16)
[50] 24t 2 (8%) 14 (58) 5 (21)
[52] 10 None 8 (80) 2 (20)
[53] 16t 3 (19%) II (69) None
* Two patients refused to undergo a surgical procedure following percutaneous drainage; one patient later died ofpulmonary disease and sepsis.
t Two patients delayed undergoing a surgical procedure following percutaneous drainage. One patient was deemedmedically unsuitable for a surgical procedure and later died.
t One patient required a three-stage surgical procedure after percutaneous drainage. One patient remained toounstable to undergo an operation following percutaneous drainage and later died of respiratory failure.
33
Traditional surgical approaches to stage 3 disease have focused on colostomy for fecal diversion, with resection of thediseased colon and colostomy takedown at a later date. Imageguided therapy has advanced the management of diverticulardisease. Multistage operative procedures and colostomy maynot be necessary for patients who undergo image-guided percutaneous drainage of their abscesses (figure 2), a circumstancethat results in decreased morbidity. The use of CT-guided imaging and ultrasonography in most cases allows differentiationbetween small, well-contained macroabscesses and large pericolic or pelvic collections; thus, appropriate patients are selected to undergo initial percutaneous catheter drainage.
Stabile et al. [49] reviewed the cases of 19 patients followedup for a mean of 17.4 months in order to define the role ofpercutaneous catheter drainage in the initial management ofdiverticular abscess. All of these patients had diverticular disease of the colon, and at least one had had a prior attack ofdiverticulitis. Initial needle aspiration and gram staining wereperformed to confirm that the patients had infected fluid collections. In addition, sinograms were obtained initially throughthe catheter and later at various intervals to determine whether acolonic fistula was present and to assess abscess size. Fourteenpatients (74%) were successfully treated with preoperative percutaneous catheter drainage and subsequent one-stage sigmoidcolectomy. Three patients had fecal fistulas and were treatedby means of colostomy. Two of the patients refused surgery,one of whom died of "uncontrolled sepsis and respiratoryfailure" on day 16 after undergoing the drainage procedure.
This study demonstrates that preoperative catheter drainagetechniques can safely eliminate the need for multistage surgeryin some patients, allowing for the performance of an interimelective one-stage procedure. Similar results have been obtained in additional clinical studies, with success rates of 71%88% for preoperative percutaneous drainage and subsequentprimary anastomosis [50-53] (table 2).
Appendiceal abscesses. Appendicitis remains one of themost commonly encountered causes of acute illness requiring
surgery. The diagnosis remains based primarily on clinical suspicion elicited by the patient's history, the physical examinationfindings, and the results of laboratory studies. In a majority ofcases, the decision to operate is made at the bedside, and thereis no need for further work-up. Thus, undue delays in diagnosisare prevented, and treatment is instituted promptly before thepatient's condition deteriorates. Rates of negative findings onlaparotomy have been recorded to be 10%- 15% for men andas high as 45% for women of childbearing age [54].
Over the past decade advances in management of appendicitis have focused on prompt perioperative evaluation to avoidunnecessary laparotomies. Imaging studies such as ultrasonography and CT have played a role in preoperative evaluation.These techniques afford the physician additional treatment options if perforation is discovered. In addition, the evolutionof laparoscopic surgery has enabled direct visualization andimmediate directed intervention if pathology is discovered.With these advances in diagnosis and treatment, the morbidity,mortality, and rates of unnecessary laparotomy that are associated with appendiceal disease should gradually decline in thefuture.
The evaluation of acute abdominal pain can occasionally bedifficult, requiring further imaging studies. Ultrasonography ishelpful for evaluating the abdomen when appendicitis is thesuspected cause of pain, and management can be altered basedon the findings. When a large periappendicular phlegmon isdiscovered, patients may benefit from administration of antibiotic therapy, followed by appendectomy. Patients withperiappendicular abscesses can be treated by percutaneousdrainage of the pus, followed by appendectomy 4-6 weekslater. The utility of ultrasonography can be limited by obesity,the presence of distended loops of bowel, the retrocecal anatomy, and the experience of the operator.
CT is also used occasionally in the evaluation of patientswith suspected appendicitis. This technique is associated withhigh positive predictive values (~95%) for the diagnosis of lateappendicitis [55]. The inflamed appendix has a characteristic

34 Montgomery and Wilson ern 1996;23 (July)
"target sign" appearance when seen in transverse CT views.The major disadvantage of these imaging techniques is thedelay in diagnosis if the test is negative, which can possiblyresult in perforation ofan acutely infected appendix and clinicaldeterioration in the patient's condition. Diagnosis ofearly acuteappendicitis is still a clinical determination.
Laparoscopy has become a useful surgical technique in thediagnosis and management of appendiceal disease. Laparoscopy can be useful in the diagnosis of abdominal pain in patients with a normal-appearing appendix. In addition, incidentalappendectomy can be performed with use of a laparoscope,resulting in reduced postoperative morbidity. Patients withacute appendicitis can be treated reasonably promptly withlaparoscopic appendectomy. Some indications for conversionto an open technique include the presence of severe inflammation or perforation at the base of the appendix and adherenceof the bowel to an appendiceal abscess [56].
Postoperative abscesses. Despite advances in surgical careand perioperative antibiotic regimens,postoperative abdominalabscesses continue to be a problem. With the advent of CT andultrasonography, the sensitivity and specificity in diagnosing intraperitoneal infection have increased dramatically. Unfortunately,littleprogresshas been made in loweringthe mortalityratesamongpatients with postoperative abscesses. A study of 47 patients overa 5-year period demonstratedthat the overall mortalityassociatedwith postoperative intraabdominal sepsis was 30% (14 of 47 patients) [57]. This finding is consistentwith those of other clinicalstudies, which demonstrated mortality rates as high as 43% [58].
The timing of imaging studies in the postoperative periodis important. Fluid collections resulting from intraoperativeirrigation, edema, and old blood and inflammatory changesdue to surgical manipulation in the immediate postoperativeperiod can make diagnosis difficult. While ultrasonographyequipment is transportable to the patient's bedside, the diagnostic capabilities of ultrasonography are limited when thepatient is large or when postoperative ileus is present. CTis generally considered the diagnostic study of choice duringthe postoperative period [15, 18-20]. However, its sensitivity may be somewhat decreased during this period, whichshould alert the physician to the possibility of a false-negative result. The eighth postoperative day is generally therecommended time to perform CT imaging [59]. This delayallows for reabsorption of nonsuppurative fluid collectionsand resolution of tissue swelling.
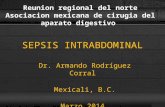
To avoid delay in diagnosis when a postoperative abscessis suspected, it is important to verify the presence of infection by means of percutaneous needle aspiration. When aninfected fluid collection is present, repeated laparotomy canbe performed or percutaneous drainage can be attempted.Percutaneous drainage obviates the need for a general anesthetic and may be definitive treatment in some cases (figure3). In addition, some authors have suggested that percutaneous drainage can be used as a temporizing procedure incritically ill patients [39]. However, limitations to percuta-
Figure 3. Management of postoperative abscesses with CT-guidedpercutaneous drainage. A: Postoperative abscess that resulted from alarge-bowel anastomotic leak following a takedown colostomy procedure. The catheter remained in place for 10 days, and no furthersurgical intervention was required. B: Percutaneous drainage of anabscess and low output fistula following an appendectomy. The catheter was removed 7 days later, after drainage from the cavity stopped.
neous drainage exist: if anastomotic dehiscence is suspected, operative drainage and repair by exteriorization ofthe leak are preferred. The presence of multiple loculations,excessive cellular debris, high fluid viscosity, or an inadequate drainage route also may prevent successful percutaneous drainage.
Premature removal of the drainage catheter may predispose torecurrence of the abscess. The catheter should remain in placeuntil clinical evidence of infection has resolved, drainage from

em 1996;23 (July) Imaging of Intraabdominal Abscesses 35
the catheter ceases, CT imaging indicates absence of fluid, or asinograrn demonstrates collapse of the abscess cavity. [15, 60]
Summary
The diagnosis and treatment of intraabdominal abscesseshave improved with the advent of imaging techniques such asultrasonography and CT. These advances have made minimallyinvasive drainage techniques available; such techniques complement traditional surgical drainage for patients with abdominal abscess cavities.
In most cases, drainage can be performed successfully whena safe route for drainage is available, the fluid collection iswell-localized and unilocular, and evaluation is coordinatedbetween the surgeon and radiologist. However, the recent decrease in mortality associated with intraabdominal abscesses isprobably related to a variety of factors including advances incritical care, the availability of broad-spectrum antibiotics, better nutrition, and earlier diagnosis. Investigators have demonstrated that percutaneous drainage can be as effective as surgical methods for the management of abscesses, and it appearsthat the important determinant of patient survival is severityof illness. Scoring systems such as APACHE II are proving tobe important for determining patient outcome regardless of thedrainage technique employed.
References
1. Ochsner A, Graves AM. Subphrenic abscess: an analysis of3,372 collectedand personal cases. Ann Surg 1933;98:961-90.
2. Altemeier WA, Culbertson WR, Fullen WD, Shook CD. Intra-abdominal
abscesses. Am J Surg 1973; 125:70-9.3. Levison MA. Percutaneous versus open operative drainage of intra-abdom
inal abscesses. Infect Dis Clin North Am 1992;6:525-44.
4. Fry DE, Garrison RN, Trachtenberg L, et al. Bacterial inoculum and theactivity of antimicrobial agents. Surg Gynecol Obstet 1985; 160:
105-8.5. Gerzof SG, Robbins AH, Johnson WC, Birkett DH, Nabseth DC. Percuta
neous catheter drainage of abdominal abscesses: a five-year experience.N Engl J Med 1981; 305:653 - 7.
6. vanSonnenberg E, Ferrucci JT Jr, Mueller PR, Wittenberg J, Simeone JF.Percutaneous drainage of abscesses and fluid collections: technique,results, and applications. Radiology 1982; 142:1-10.
7. Clark RA, Towbin R. Abscess drainage with CT and ultrasound guidance.Radiol Clin North Am 1983;21:445-59.
8. Brolin RE, Nosher JL, Leiman S, Lee WS, Greco RS. Percutaneous catheter versus open surgical drainage in the treatment of abdominal abscesses. Am Surg 1984;50:102-8.
9. Hemming A, Davis NL, Robins RE. Surgical versus percutaneous drainage
of intra-abdominal abscesses. Am J Surg 1991; 161:593-5.
10. Lent WM, Goldman MJ, Bizer LS. An objective appraisal of the role of
computed tomographic (CT) guided drainage of intra-abdominal abscesses. Am Surg 1990; 56:688-90.
11. McLean TR, Simmons K, Svensson LG. Management of postoperative
intra-abdominal abscesses by routine percutaneous drainage. Surg Gynecol Obstet 1993; 176:167- 71.
12. Levison MA, Zeigler D. Correlation of APACHE II score, drainage technique and outcome in postoperative intra-abdominal abscess. Surg Gynecol Obstet 1991; 172:89-94.
13. Lurie K, Plzak L, Deveney CWo Intra-abdominal abscess in the 1980s.
Surg Clin North Am 1987;67:621-32.
14. Halber MD, Daffner RH, Morgan CL, et al. Intraabdominal abscesses:
current concepts in radiologic evaluation. AJR Am J Roentgenol 1979;133:9-13.
15. Fry DE. Noninvasive imaging tests in the diagnosis and treatment of intraabdominal abscesses in the postoperative patient. Surg Clin North Am1994; 74(3):693-709.
16. Gazelle GS, Mueller PRo Abdominal abscess: imaging and intervention.
Radiol Clin North Am 1994;32:913-32.
17. Roche 1. Effectiveness of computed tomography in the diagnosis of intraabdominal abscess: a review of III patients. Med J Aust 1981;25:85-8.
18. Korobkin M, Callen PW, Filly RA, Hoffer PB, Shimshak RR, Kressel HY.
Comparison of computed tomography, ultrasonography, and gallium-67
scanning in the evaluation of suspected abdominal abscess. Radiology
1978; 129:89-93.
19. Robison JG, Pollack TW. Computed tomography in the diagnosis and
localization of intraabdominal abscesses. Am J Surg 1980; 140:783-6.20. Dobrin PB, Gully PH, Greenlee HB, et al. Radiologic diagnosis of an
intra-abdominal abscess: do multiple tests help? Arch Surg 1986; 121:41-6.
21. Knaus WA, Draper EA, Wagner DP, Zimmerman lE. APACHE II: aseverity of disease classification system. Crit Care Med 1985; 13:818-29.
22. Malangoni MA, Shumate CR, Thomas HA, Richardson JD. Factors influ
encing the treatment of intra-abdominal abscesses. Am 1 Surg 1990;
159:167-71.
23. Goletti 0, Lippolis PV, Chiarugi M, et al. Percutaneous ultrasound-guideddrainage of intra-abdominal abscesses. Br 1 Surg 1993;80:336-9.
24. Kourtesis G, Wilson SE, Williams RA. The clinical significance of fluid
collections in acute pancreatitis. Am Surg 1990; 56:796-9.25. Silverstein W, IsikoffMB, Hill MC, Barkin 1. Diagnostic imaging of acute
pancreatitis: prospective study using CT and sonography. AJR Am 1Roentgenol 1981; 137:497-502.
26. Crass RA, Meyer AA, Jeffrey RB, et al. Pancreatic abscess: impact ofcomputerized tomography on early diagnosis and surgery. Am 1 Surg1985; 150:127-31.
27. Nordestgaard AG, Wilson SE, Williams RA. Early computed tomography
as a predictor of outcome in acute pancreatitis. Am 1 Surg 1986; 152:127-32.
28. Bradley EL III. A clinically based classification system for acute pancreati
tis. Arch Surg 1993; 128:586-90.29. Bradley EL, Clements JL Jr, Gonzalez AC. The natural history of pancre
atic pseudocysts: a unified concept of management. Am 1 Surg 1979;137:135-41.
30. Yeo CJ, Bastidas JA, Lynch-Nyhan A, Fishman EK, Zinner MJ, Cameron11. The natural history of pancreatic pseudocysts documented by computed tomography. Surg Gynecol Obstet 1990; 170:411-7.
31. Bradley EL III, Murphy F, Ferguson C. Prediction of pancreatic necrosisby dynamic pancreatography. Ann Surg 1989;210:495-503.
32. Beger HG, Bittner R, Block S, Buchler M. Bacterial contamination ofpancreatic necrosis: a prospective clinical study. Gastroenterology 1986;91:433-8.
33. vanSonnenberg E, Wittich GR, Casola G, et al. Complicated pancreatic
inflammatory disease: diagnostic and therapeutic role of interventional
radiology. Radiology 1985; 155:335-40.
34. Hariri M, Slivka A, Carr-Locke DL, Banks PA. Pseudocyst drainage pre
disposes to infection when pancreatic necrosis is unrecognized. Am 1Gastroenterol 1994; 89:1781-4.
35. Balthazar El, Freeny PC, van Sonnenberg E. Imaging and intervention inacute pancreatitis. Radiology 1994; 193:297- 306.
36. Rattner DW, Legermate DA, Lee Ml, Mueller PR, Warshaw AL. Earlysurgical debridement of symptomatic pancreatic necrosis is beneficialirrespective of infection. Am 1 Surg 1992; 163:I05- 9.

36 Montgomery and Wilson em 1996;23 (July)
37. Bittner R, Block S, Buchler M, Beger HG. Pancreatic abscess and infected
pancreatic necrosis: different local septic complications in acute pancre
atitis. Dig Dis Sci 1987;32:1082-7.
38. Lang EK, Paolini RM, Pottmeyer A. The efficacy of palliative and defini
tive percutaneous versus surgical drainage of pancreatic abscesses and
pseudocysts: a prospective study of 85 patients. South Med J 1991; 84:
55-64.
39. vanSonnenberg E, Wing VW, Casola G, et al. Temporizing effect of
percutaneous drainage of complicated abscesses in critically ill patients.
AJR Am J Roentgenol1984; 142:821-6.
40. Karlson KB, Martin EC, Fankuchen EI, Mattern RF, Schultz RW, Casarella
WJ. Percutaneous drainage of pancreatic pseudocysts and abscesses.
Radiology 1982; 142:619-24.
41. van Waes PF, Feldberg MA, Mali WP, et al. Management of loculated
abscesses that are difficult to drain: a new approach. Radiology 1983;
147:57-63.
42. vanSonnenberg E, Mueller PR, Ferrucci JT Jr. Percutaneous drainage of
250 abdominal abscesses and fluid collections. Part I: Results, failures,
and complications. Radiology 1984; 151:337-41.43. Bradley EL III. Cysts and pseudocysts of the pancreas. surgical aspects.
In: Berk JE, ed. Gastroenterology. Vol 6. London: W.B. Saunders, 1985:
4151-7.
44. vanSonnenberg E, Wittich GR, Casola G, et al. Percutaneous drainage of
infected and noninfected pancreatic pseudocysts: experience in 101
cases. Radiology 1989; 170:757-61.
45. D'Agostino HB, van Sonnenberg E, Sanchez RB, Goodacre BW, Vil
laveiran RG, Lyche K. Treatment of pancreatic pseudocysts with percu
taneous drainage and octreotide: work in progress. Radiology 1993;
187:685-8.
46. Szentes MJ, Traverso LW, Kozarek RA, Freeny PC. Invasive treatment
of pancreatic fluid collections with surgical and nonsurgical methods.Am J Surg 1991; 161:600-5.
47. Hackford AW, Veidenheimer MC. Diverticular disease of the colon: cur
rent concepts and management. Surg Clin North Am 1985;65:347-63.
48. Gordon PH. Diverticular disease of the colon. In: Gordon PH, Nivatvongs
S. Principles and practice of surgery for the colon, rectum and anus.St. Louis: Quality Medical Publishing, 1992:739-98.
49. Stabile BE, Puccio E, vanSonnenberg E, NeffCC. Preoperative percutane
ous drainage of diverticular abscesses. Am J Surg 1990; 159:99-104.
50. Mueller PR, Saini S, Wittenburg J, et al. Sigmoid diverticular abscesses:
percutaneous drainage as an adjunct to surgical resection in 24 cases.
Radiology 1987; 164:321-5.
51. Saini S, Mueller PR, Wittenberg J, et al. Percutaneous drainage ofdivertic
ular abscess: an adjunct to surgical therapy. Arch Surg 1986; 121:
475-8.
52. Schechter S, Eisenstat TE, Oliver GC, Rubin RJ, Salvati EP. Computerized
tomographic scan-guided drainage of intra-abdominal abscesses: preop
erative and postoperative modalities in colon and rectal surgery. DisColon Rectum 1994;37:984-8.
53. NeffCC, vanSonnenberg E, Casola G, et al. Diverticular abscesses: percu
taneous drainage. Radiology 1987; 163:15-8.
54. Berry J Jr, Malt RA. Appendicitis near its centenary. Ann Surg 1984; 200:567-75.
55. Borushok KF, Jeffrey RB Jr, Laing FC, Townsend RR. Sonographic diag
nosis of perforation in patients with acute appendicitis. AJR Am J
Roentgenol 1990; 154:275-8.
56. Connor TJ, Garcha IS, Ramshaw BJ, et al. Diagnostic laparoscopy for
suspected appendicitis. Am Surg 1995; 61:187- 9.
57. Butler JA, Huang J, Wilson SE. Repeated laparotomy for postoperative
intra-abdominal sepsis: an analysis of outcome predictors. Arch Surg
1987; 122:702-6.
58. Hinsdale JG, Jaffe BM. Re-operation for intra-abdominal sepsis: indica
tions and results in modem critical care. Ann Surg 1984; 199:31-6.
59. Norwood SH, Civetta JM. Abdominal CT scanning in critically ill surgical
patients. Ann Surg 1985; 202:166-75.60. Pruett TL, Rotstein OD, Crass J, Frick MP, Flohr A, Simmons RL. Percuta
neous aspiration and drainage for suspected abdominal infection. Sur
gery 1984;96:731-7.