Intra capsular neck of femur fractures
39
Intra-capsular Neck Of Femur Fractures Sheweidin AZIZ – Sep 2015
-
Upload
shewei-aziz -
Category
Health & Medicine
-
view
144 -
download
4
Transcript of Intra capsular neck of femur fractures
Intra-capsular Neck Of Femur Fractures
Sheweidin AZIZ – Sep 2015

Aim1. Background2. Anatomy + Patho-anatomy3. Predisposing factors4. Mechanism of injury5. Clinical presentation/Radiological investigation6. Classification7. Aims of treatment 8. Management9. Complications
Background About 70-75,000 hip fractures per year in UK
(10/1000)
Average age 77 years
Commonest cause of admission to orthopaedic wards
Usually fragility fracture

Background Lifetime risk 15% ♀ and 5% ♂
High mortality rate ~10% in 30 days and up to30% in a year
Annual cost of over £2 billion
About 10-20% admitted from home will move to institutional care

Anatomy
Borders x2 Surfaces x2 Calcar

Anatomy
Described by Crock Extra-capsular ring Retinacular Ligamentun Teres

Anatomy

Predisposing factors1. Loss of bone strength
2. Loss of local shock absorbers
3. Reduction in protective responses
4. Increased risk of falls

Mechanism of injury Low Energy
Direct Indirect
High Energy
Cyclical Loading Stress fracture

Clinical Presentation History
Injury Predisposing factors Inability to weight bear
Clinical examination Shortening and external rotation Inability to SLR Groin tenderness

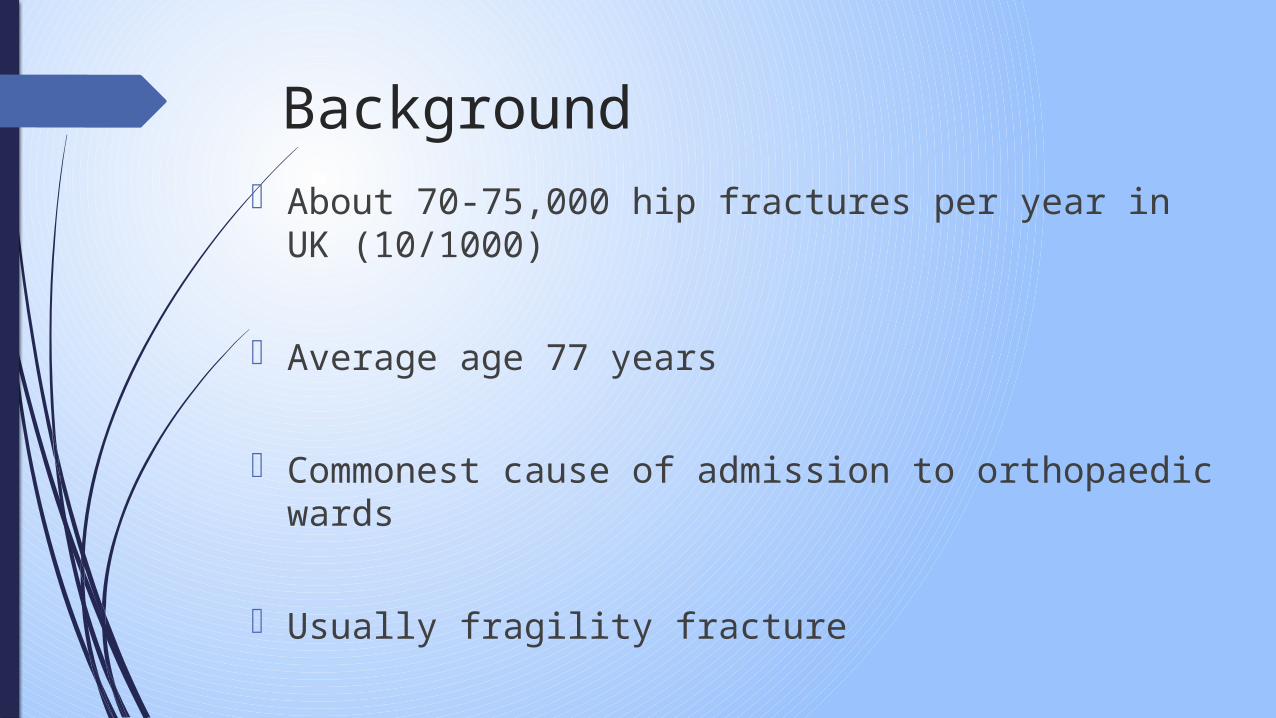
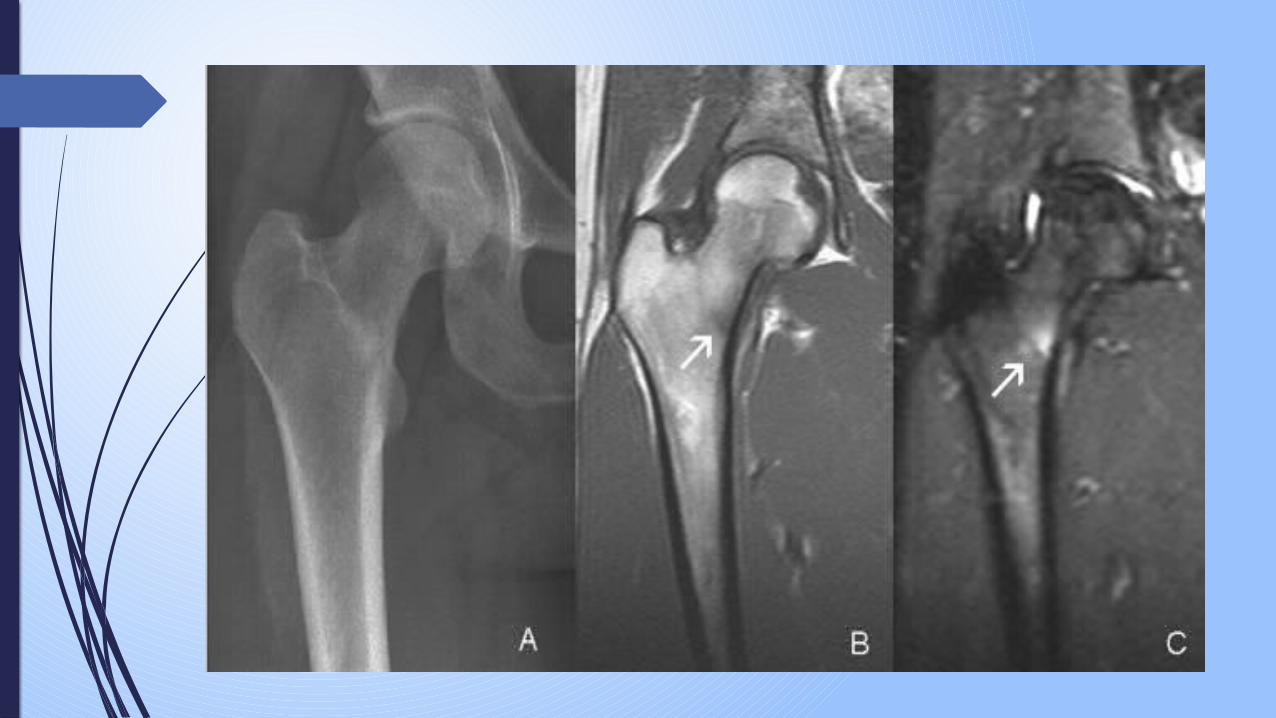
Clinical Presentation

Radiological investigations
Plain radiograph (Antero-posterior and Lateral)
MRI
CT




Classification
Anatomical Location
Garden
Pauwels
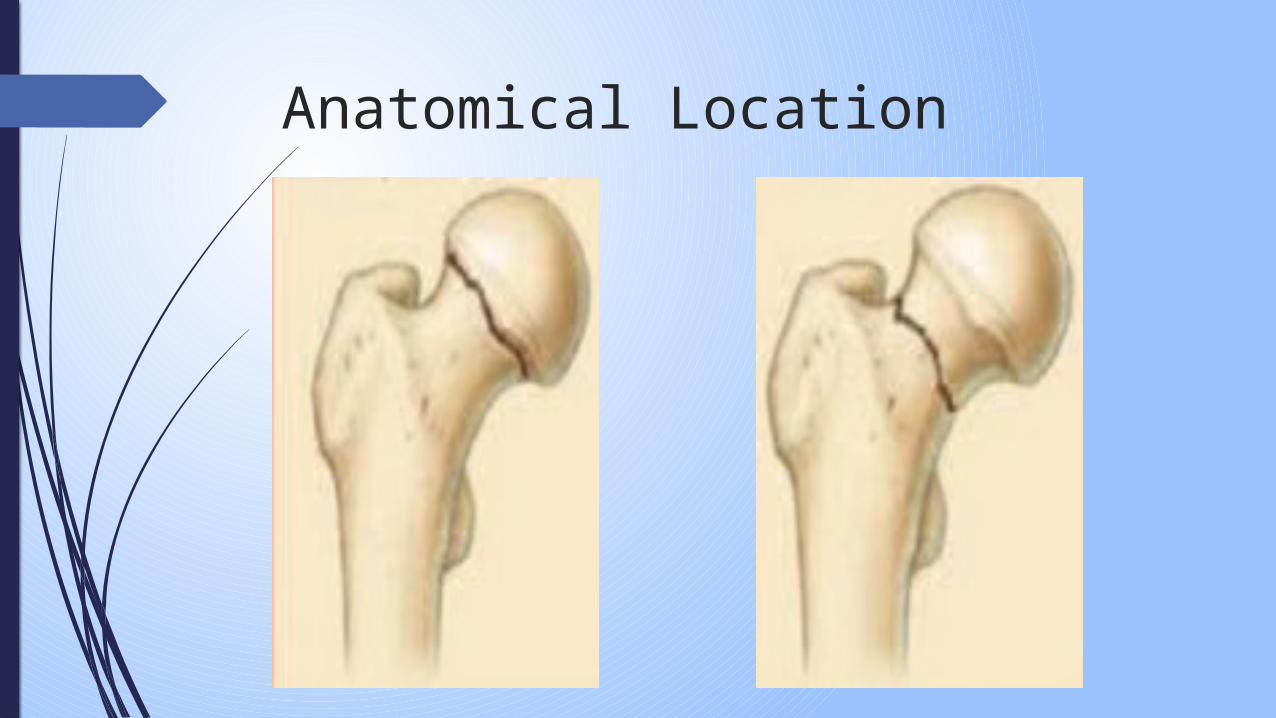
Anatomical Location

Garden

Garden

Pauwels
Goals of treatment
Patient comfort
Restore hip function / independence
Reduce length of immobility

Management - Multidisciplinary team1. General
1. Identify +/- treat cause of injury2. Secondary prevention3. Rehabilitation
2. Specific 1. Management of hip fracture:
Conservative/Operative

Specific management1. Analgesia
2. Hydration
3. Investigations (Bloods, CXR, ECG, Echo .. etc)
4. Identify and treat co-morbidities to avoid delay
Operative management1. Internal Fixation
1. Cannulated screws2. Dynamic Hip screws
2. Arthroplasty1. Cemented Thompson2. Cemented bipolar3. Uncemented Austin Moore4. Total hip Replacement

Cannulated Screws
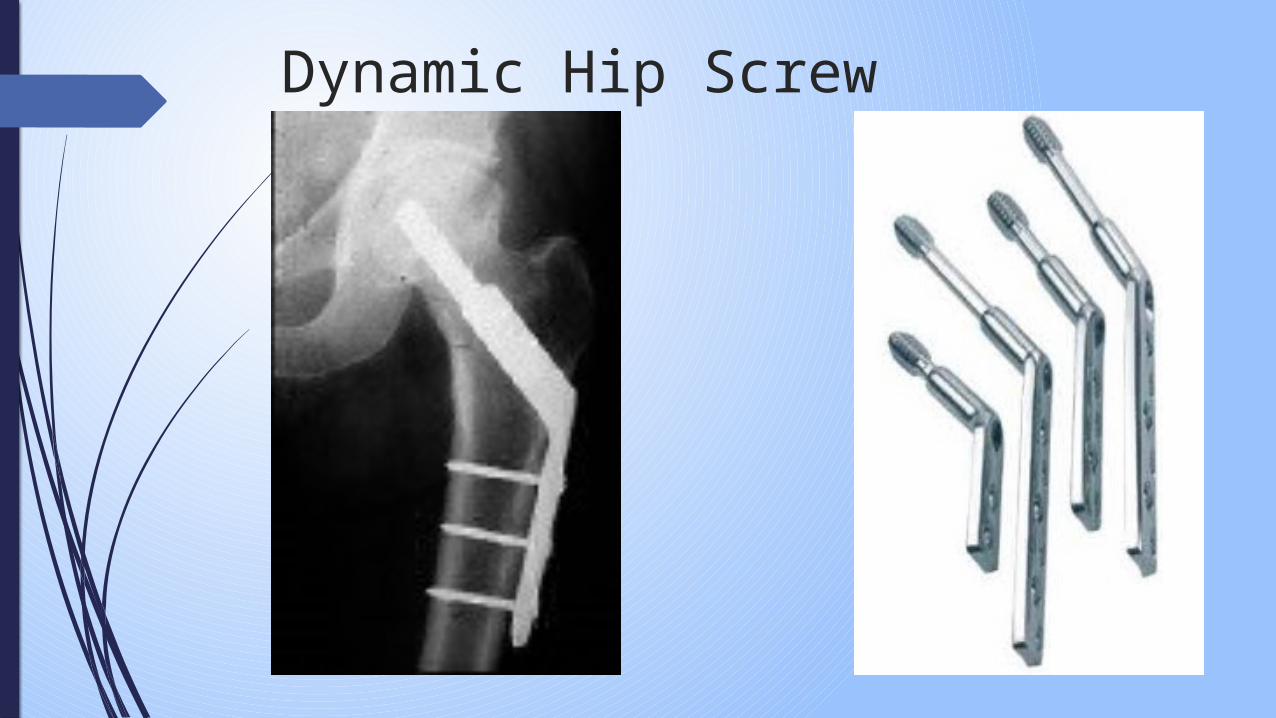
Dynamic Hip Screw

Cemented Thompsons

Cemented bipolar

Austin Moore
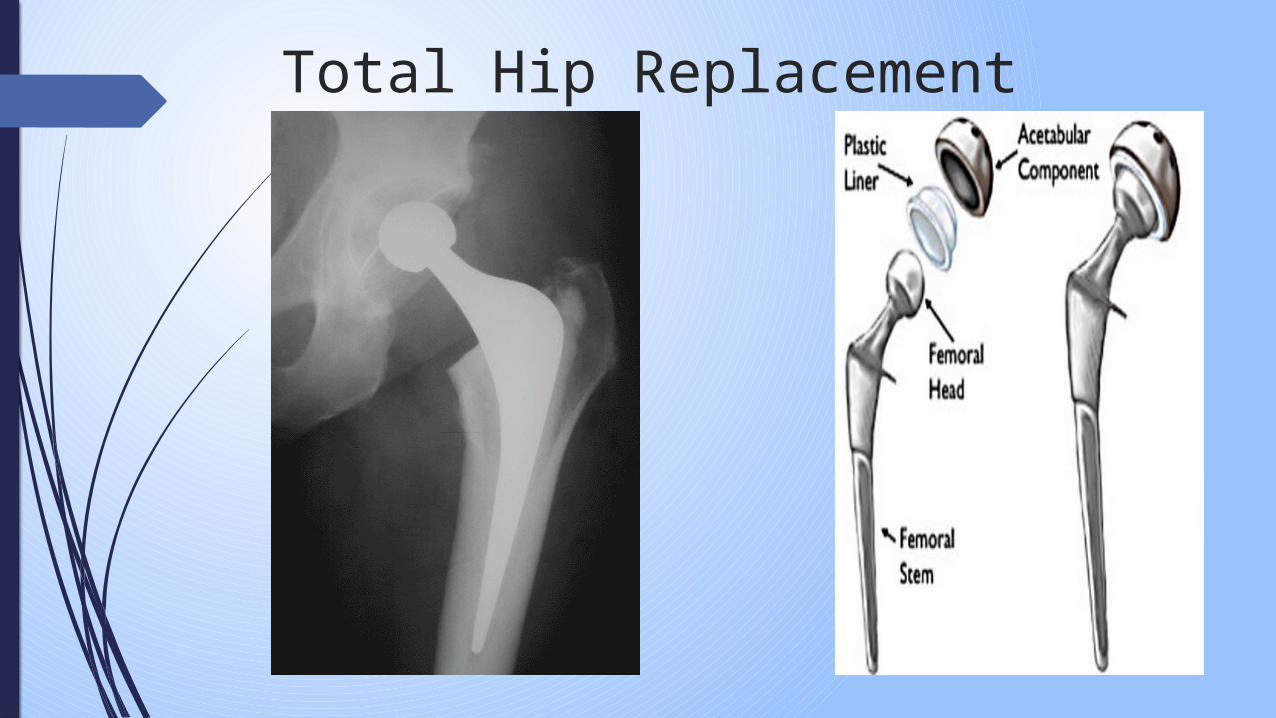
Total Hip Replacement

Complications - General VTE / PE
Infections (UTI / LRTI / Wound)
Bed sores
Osteoarthritis
Avscaulr necrosis
Non union

Complications – Arthroplasty Revision surgery 10%
Higher mortality
Longer hospital stay
Dislocation
Complications – Arthroplasty Leg length discrepancy
Acetabular erosion
Implant infection
Fracture around prosthesis
Expensive

Complications – Internal Fixation
Non union 20-30%
Avascular necrosis 10-20%
Revision surgery 25-30%
Post Operative care1. Check Hb / U&Es
2. VTE prophylaxis
3. Rehabilitation with physio - Mobilise Full weight bearing
4. +/- check X-Rays

Further reading1. Orthopaedic Trauma Association Classification
2. BOAST guidelines on Fragility Hip Fractures
3. National Hip Fracture Database
4. NICE clinical guidance – Management of hip fractures in adults

QUESTIONS