Interventions to reduce maternal and infant mortality. A ... · The interventions that have been...
26
Interventions to reduce maternal and infant mortality. A systematic review (Review Protocol) Ministry of Health and Social Protection Group of Sectoral Studies and Public Policy Evaluation July 2016
Transcript of Interventions to reduce maternal and infant mortality. A ... · The interventions that have been...

Interventions to reduce maternal and infant mortality. A systematic review
(Review Protocol)
Ministry of Health and Social Protection Group of Sectoral Studies and Public Policy
Evaluation
July 2016

2
Alejandro Gaviria Uribe Minister of Health and Social Protection Mario Fernando Vargas Cruz Chief of the Office of Planning and Sectoral Studies Technical Team Bibiana Quiroga Forero Mauricio Aguilar Villegas Andrés Acosta Hernández

3
Table of contents
Abstract ...................................................................................................................................................................... 5
Background ............................................................................................................................................................... 5
Description of the condition .......................................................................................................................... 5
Description of the intervention .................................................................................................................... 8
How the intervention might work ............................................................................................................ 10
Why it is important to do this review ..................................................................................................... 11
Objectives ............................................................................................................................................................... 11
Methods ................................................................................................................................................................... 12
Criteria for considering studies for this review ..................................................................................... 13
Types of studies ................................................................................................................................................ 13
Types of Participants ..................................................................................................................................... 13
Types of Interventions .................................................................................................................................. 14
Types of Outcomes of interest ................................................................................................................... 14
Primary outcomes: .................................................................................................................................... 14
Secondary outcomes: ............................................................................................................................... 14
Search methods for identification of studies ....................................................................................... 15
Electronic bibliographic databases .................................................................................................... 15
Other resources .......................................................................................................................................... 15
Data collection and analysis ........................................................................................................................ 16
Selection of studies ................................................................................................................................... 16
Data extraction and management ...................................................................................................... 16
Assessment of risk of bias in included studies .............................................................................. 16
Quality of the evidence ............................................................................................................................ 17
Measures of treatment effect ................................................................................................................ 17
Unit of analysis issues .............................................................................................................................. 17
Dealing with missing data ...................................................................................................................... 17
Assessment of heterogeneity ................................................................................................................ 18
Assessment of reporting biases ........................................................................................................... 18

4
Data synthesis ................................................................................................................................................... 18
Acknowledgements ........................................................................................................................................ 18
Bibliography .......................................................................................................................................................... 19
Appendix 1. Maternal, Neonatal and Under 5 mortality in 2015 by Latin-American Countries. ................................................................................................................................................................ 22
Appendix 2. Search strategies ........................................................................................................................ 22
PubMed search strategy ............................................................................................................................... 22
Embase search strategy ................................................................................................................................ 23
Medline (Ovid) search strategy ................................................................................................................. 23
Cochrane Central Register of Controlled Trials - EBM Reviews (Ovid) search strategy... 24
Appendix 3. Data extraction form ................................................................................................................ 24

5
Interventions to reduce maternal and infant mortality. A systematic review (Review Protocol)
Bibiana Quiroga Forero1; Mauricio Aguilar Villegas1 , Andrés Leonardo Acosta1 Contact address: [email protected]; [email protected]; [email protected] Abstract
This is the protocol for a review and there is no abstract. The objective is as follows:
To synthesise the evidence available to date from rigorous impact evaluations of three types
of interventions: 1) community-based interventions, 2) structural changes to improve
access to maternal and new-born care, and 3) reductions of medical fees.
Background
Description of the condition
This systematic review is focused on two main indicators: maternal and infant mortality. In this case, maternal mortality is understood as fatal pregnancy-related events that occur while pregnant, childbirth, or within 42 days after the birth. On the other hand, the definition of infant mortality integrates three groups, perinatal, late neonatal and post-neonatal mortality. The former is defined as deaths occurring from the 22th week of gestation until the 7 day after birth, the second one refers to deaths between 7 to 28 days after birth and the last one refers to deaths that occur among 29 to 365 days after birth (Ministerio de Salud y Protección Social & Organización Panamericana de la Salud, 2012). One can provide the argument that maternal and child mortality is one of the largest issues of health in the international agenda (Sachs, 2005). This is the case of the Millennium
1 Consultants. Sectoral Studies and Public Policy Evaluation Group. Ministry of Health and Social Protection.

6
Development Goals (MDGs) that defined two objectives to reduce both maternal and child mortality2 (UN, 2015). This compromise was ratified in the declaration of the Sustainable Development Goals, where two targets have being established by 2030: 1) to reduce the global maternal mortality ratio to less than 70 per 100.000 live births; and 2) to end preventable deaths of new-borns and children under 5 years of age, with all countries aiming to reduce neonatal mortality to at least as low as 12 per 1.000 live births, and under-5 mortality to at least as low as 25 per 1.000 live births. According to the Millennium Development Goals Report 2015, as a result of international efforts, maternal and infant mortality rates have shown important reductions. For instance, the maternal mortality ratio showed a drop of 45% and the mortality rate among children under-5 globally decreased in more than half (UN, 2015). However, the reductions achieved in infant and maternal mortality numbers are only a partial fulfilment of the established goals in that arena so far. It is important to remark that most of maternal and infant deaths occur in Low and Middle Income Countries (LMICs)3 . In this case, the Table 1 shows these indicators across the World Health Organisation (WHO) regions. As can be seen, the global Maternal Mortality Ratio (MMR) in 2015 was 216 per 100.000 live births and the Neonatal (NMR) and Under Five Mortality (U5MR) Rates was 19,2 and 43 per 1.000 live births respectively. The countries in Africa, Eastern Mediterranean and South-East Asia concentrate the highest figures of this problem. In contrast, the regions of Europe and the Americas show the fewest numbers in all the indicators. Nevertheless, analysing only the results for Latin-American countries (see Appendix 1), it is shown that Caribbean countries have similar indicators to those regions with the most problematic scenarios. This is consistent with the argument that high mortality rates are more commonly found within the LMICs, which have shown the less progress in the MGDs’ objectives of reducing
2 See Millennium Development Goals. Target 4: Reduce by two thirds, between 1990 and 2015, the under-five mortality rate, and target 5A: Reduce by 1.000 three quarters, between 1990 and 2015, the maternal mortality ratio.
3 By 2016, low-income economies are defined as those with a GNI per capita, calculated using the World Bank Atlas method, of $1,025 or less in 2015; lower middle-income economies are those with a GNI per capita between $1,026 and $4,035; upper middle-income economies are those with a GNI per capita between $4,036 and $12,475; high-income economies are those with a GNI per capita of $12,476 or more.
7
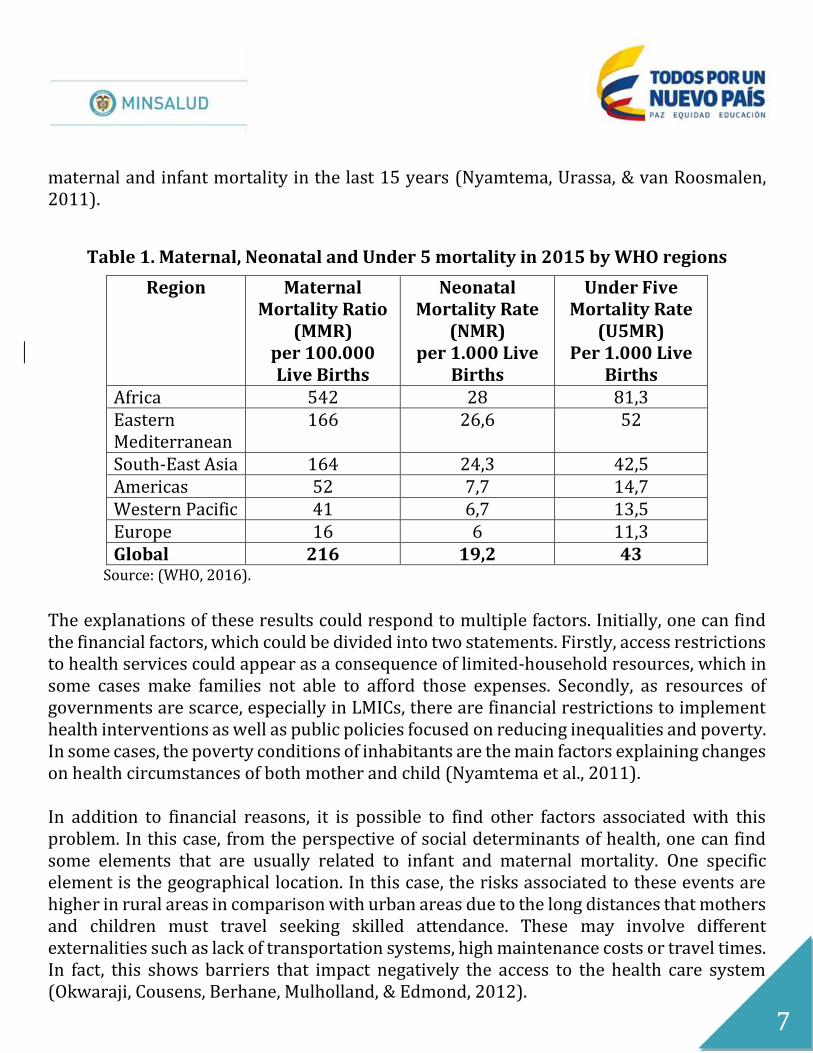
maternal and infant mortality in the last 15 years (Nyamtema, Urassa, & van Roosmalen, 2011).
Table 1. Maternal, Neonatal and Under 5 mortality in 2015 by WHO regions
Region Maternal Mortality Ratio
(MMR) per 100.000 Live Births
Neonatal Mortality Rate
(NMR) per 1.000 Live
Births
Under Five Mortality Rate
(U5MR) Per 1.000 Live
Births Africa 542 28 81,3 Eastern Mediterranean
166 26,6 52
South-East Asia 164 24,3 42,5 Americas 52 7,7 14,7 Western Pacific 41 6,7 13,5 Europe 16 6 11,3 Global 216 19,2 43
Source: (WHO, 2016).
The explanations of these results could respond to multiple factors. Initially, one can find the financial factors, which could be divided into two statements. Firstly, access restrictions to health services could appear as a consequence of limited-household resources, which in some cases make families not able to afford those expenses. Secondly, as resources of governments are scarce, especially in LMICs, there are financial restrictions to implement health interventions as well as public policies focused on reducing inequalities and poverty. In some cases, the poverty conditions of inhabitants are the main factors explaining changes on health circumstances of both mother and child (Nyamtema et al., 2011). In addition to financial reasons, it is possible to find other factors associated with this problem. In this case, from the perspective of social determinants of health, one can find some elements that are usually related to infant and maternal mortality. One specific element is the geographical location. In this case, the risks associated to these events are higher in rural areas in comparison with urban areas due to the long distances that mothers and children must travel seeking skilled attendance. These may involve different externalities such as lack of transportation systems, high maintenance costs or travel times. In fact, this shows barriers that impact negatively the access to the health care system (Okwaraji, Cousens, Berhane, Mulholland, & Edmond, 2012).

8
Other factor to take into account is the educational level of the mother as determinant of health. For instance, (Lori & Starke, 2012) conducted a study in Liberia where they identified that the majority of women involved in a near-miss event or death presented no education. In the same sense, (Gakidou, Cowling, Lozano, & Murray, 2010), in a study which analysed 175 countries between 1970 and 1990, suggest that increasing the education level of women on reproductive ages is a decisive factor to reduce infant mortality. Furthermore, some aspects related to water supply and sanitation have shown strength relationship with maternal and infant mortality. By way of illustration, (Kidney et al., 2009) in a systematic review found that women in households with poor sanitation had higher probability of maternal mortality. Additionally, (Cheng, Schuster-Wallace, Watt, Newbold, & Mente, 2012) using data for 193 countries, show that MMR, U5MR and Infant Mortality Rate (IMR) decreased as a result of improved access to water and sanitation. Finally, it is recognised that maternal under-nutrition leads to intrauterine growth restriction and consequent low birth weight (Salam, Das, Ali, Lassi, & Bhutta, 2013), complication to which is attributed to 800,000 annual neonatal deaths in the wolrd (Bhutta et al., 2013). This finding is explained as access to micronutrients during pregnancy could be considered as a determining factor in infant mortality. In sum, the problem of child and maternal mortality is not only confined to financial factors, but also it is related to social determinants as educational level of mothers, geographical location, water access, sanitation and nutrition. Description of the intervention The interventions that have been implemented to reduce maternal and infant mortality could vary in different ways and include different actors and roles. Thus, one could classify these interventions according to either demand or supply side. From the demand side it is possible to identify the stage of pregnancy or the populations which are attended. On the one hand, regarding to the stage of pregnancy, it is possible to recognise three phases: prenatal, intra-partum and postnatal stage (Lassi, Haider, & Bhutta, 2011). On the other hand, the target population could be defined, for instance, by the age of mothers, gestational age, comorbidities and others risk factors (Campbell & Graham, 2006). From the supply side it is possible to categorise into four types of interventions, which are not necessarily delivered to the mother: the community based interventions, access to health services, fees changes and pharmacologic interventions.

9
Firstly, the community-based interventions are those in which community members are the main actors. That is to say, mothers, doctors, nurses, traditional birth attendants (TBAs), relatives, etc., are generally part of educational programs where they receive training in prenatal, natal or postnatal care, or they receive information on care promotion and prevention of complications. Examples of these types of interventions could be: training and/or joining TBAs to the health system, training in providing basic prenatal and postnatal care, breastfeeding counselling, design and implementation of strategies to mobilise the community to promote preparation for new-born care or supplementation of vitamin A or beta carotene during pregnancy (Kidney et al., 2009; Lassi & Bhutta, 2015; Lassi et al., 2011; Nyamtema et al., 2011; Sibley, Sipe, & Barry, 2012). Secondly, the interventions to improve access to health services contain actions that involve structural changes in processes or institutions. Examples of these interventions include re-directing care during and after pregnancy4, structural changes in the health system, inclusion of new technologies related to pregnancy in benefit plans, improvements in the provision of drugs and medical devices or creation of specialised centres for obstetric emergencies. Thirdly, it is possible to find interventions to reduce fees. These interventions could represent the decrease or elimination of the costs or payments made by users for any services of maternal and child health (Dzakpasu, Powell-Jackson, & Campbell, 2014). Finally, pharmacologic interventions are those that are applied for treatment of any complication or comorbidity related to pregnancy. For instance, the treatments to attend gestational diabetes, which is one of the major complications in pregnancy, could include strategies with no drugs such as dietary plans and physical activity, or pharmacological attention such as use of metformin or the application of insulin doses (Crowther et al., 2005). As it has been shown, the interventions to reduce maternal or infant mortality include a wide spectrum of possibilities, which could be analysed from either the demand or the supply side. In the particular case of this review, to evaluate from the phases of pregnancy is not considered plausible as it could be complex to clearly differentiate among interventions, which is the focus in this case for policymakers of the Ministry of Health and Social Protection. Thus, the supply approach has been chosen as the interest of this Ministry
4 This intervention consist to redirect attention to specialised centres, if there are obstetric complications.

10
is to develop new interventions or validate the interventions that have been implemented so far. How the intervention might work
Based on the supply classification, it is possible to define the expected effects of these kind of interventions. Firstly, the community-based interventions generally aim to train mothers, family members or community health workers on topics related to promotion and prevention of pre and postnatal care. These interventions could produce changes in the primary knowledge and information of these communities, enhancing capabilities which could produce reductions in maternal and infant mortality (Kidney et al., 2009; Lassi & Bhutta, 2015; Lassi et al., 2011; Nyamtema et al., 2011).
Secondly, when it comes to improve access to health services, the main objective is to remove barriers, changing standards of care and modifying requirements for the provision of care, or enable the referrals to access to health facilities, emergency obstetric centres or medical devices. These changes could result in more utilisation of maternal and new-born services and/or could facilitate early detection of complications. Thus, it is expected that access to health services can reduce complications and in case of the appearance of a complication, it is possible to treat patients adequately and reduce fatal cases(Nyamtema et al., 2011).
Thirdly, it is the group integrated by the interventions that reduce health care fees. With a decrease or elimination of fees, it is expected that households can access to adequate health care services for pregnancy and new-born. Therefore, the pre and postnatal care could be improved, and for this way to reduce the maternal and infant risk of death (Dzakpasu et al., 2014).
Finally, the pharmacological interventions group is in which the specific treatment depends on the condition to be treated. Complications during and after pregnancy, of both mother and child, could vary as well as treatments effects depend on health condition, drugs selected and characteristics like gestational age or the age of mothers. Due to the number of complications that could be presented during pregnancy and the vast variety of likely treatments, this review will not take into account this group of interventions.

11
Why it is important to do this review The main reason to conduct this review is the interest of the Central Government of Colombia through the Ministry of Health and Social Protection to identify the best strategies to reduce maternal and infant mortality. In this case, this interest emerges from an extensive exercise of prioritization in which this problem is in the agenda of public policy evaluations. Notwithstanding Colombia achieved the goal established on the MDGs of reducing child mortality by 2013, it is worthy to remark that Colombia did not achieve the goal of reducing maternal mortality. In this instance, the maternal mortality ratio goal was not reached as by 2015 there were 64 cases of mothers dying for every 100.000 births whereas the goal was of 45 deaths per 100.000 births (PNUD, 2015; WHO, 2016). This means that 400 mothers are dying in Colombia per year. In this case, it is clear that in terms of public policy it is necessary for the Colombian Government to identify the best strategies or interventions to stop infant and mother deaths. These arguments show the importance to conduct this Systematic Review. In this case, with an international overview in which some interventions may reduce this problem, for Colombia, which is classified as a LMIC, is especially important to identify interventions or program packages that could be adaptable to the Colombian context and which have robust evidence of effectiveness. Nevertheless, it is possible to argue that there are interventions that work in high-income countries that could be adapted to a LMIC context. Thus, the evidence from low-income, middle-income and high-income is suitable for this review. Objectives
This review will systemically synthesise the evidence of three sorts of interventions to reduce mortal and infant mortality: 1) community-based interventions, 2) structural changes to improve access to maternal and new-born care, and 3) reductions of medical fees, which comes from the rigorous impact evaluations of low-income, middle-income and high-income countries available to date.
12
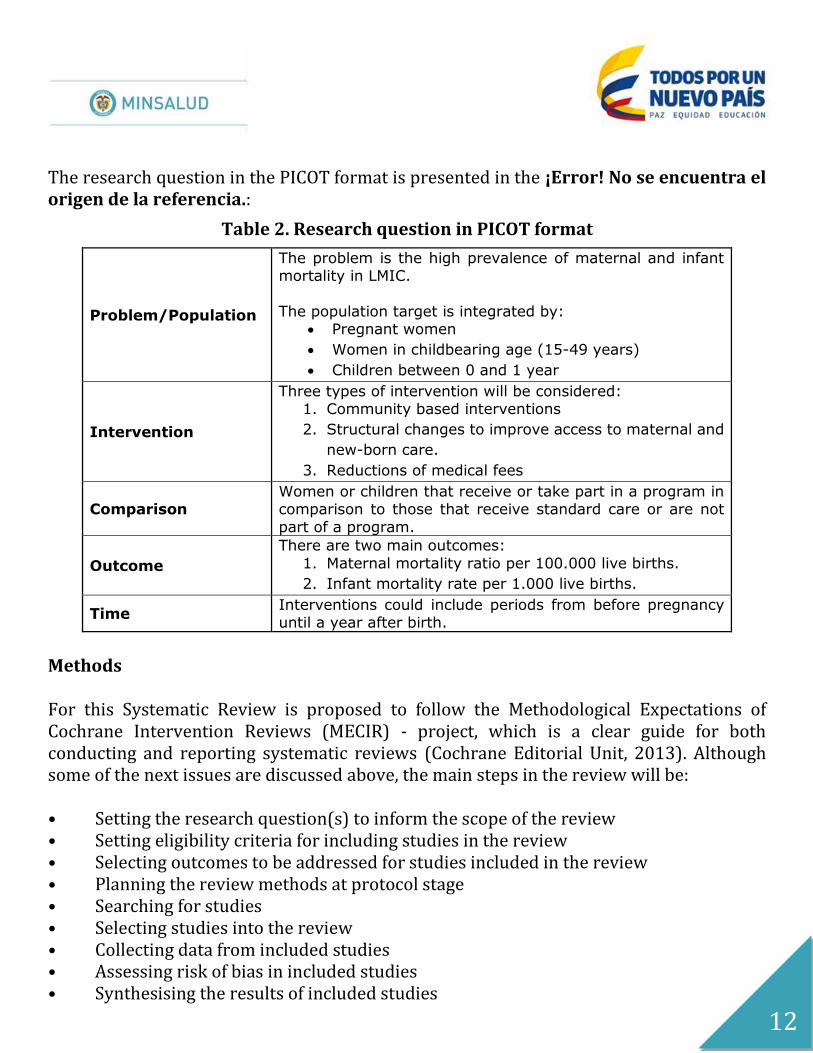
The research question in the PICOT format is presented in the ¡Error! No se encuentra el origen de la referencia.:
Table 2. Research question in PICOT format
Problem/Population
The problem is the high prevalence of maternal and infant mortality in LMIC.
The population target is integrated by:
Pregnant women
Women in childbearing age (15-49 years)
Children between 0 and 1 year
Intervention
Three types of intervention will be considered: 1. Community based interventions
2. Structural changes to improve access to maternal and
new-born care.
3. Reductions of medical fees
Comparison Women or children that receive or take part in a program in comparison to those that receive standard care or are not
part of a program.
Outcome
There are two main outcomes:
1. Maternal mortality ratio per 100.000 live births.
2. Infant mortality rate per 1.000 live births.
Time Interventions could include periods from before pregnancy until a year after birth.
Methods For this Systematic Review is proposed to follow the Methodological Expectations of Cochrane Intervention Reviews (MECIR) - project, which is a clear guide for both conducting and reporting systematic reviews (Cochrane Editorial Unit, 2013). Although some of the next issues are discussed above, the main steps in the review will be: • Setting the research question(s) to inform the scope of the review • Setting eligibility criteria for including studies in the review • Selecting outcomes to be addressed for studies included in the review • Planning the review methods at protocol stage • Searching for studies • Selecting studies into the review • Collecting data from included studies • Assessing risk of bias in included studies • Synthesising the results of included studies
13
• Summarising the findings • Reaching conclusions Criteria for considering studies for this review Types of studies
One of the most important issues in a systematic review is to define the types of studies to be retrieved. For instance, when it comes to evidence it is highly accepted that randomised controlled trials (RCTs) are the gold standard for studies (Concato, Shah, & Horwitz, 2000; Victora, Habicht, & Bryce, 2004; West & Thoemmes, 2010). In fact, RCTs have taken significant strength for the evaluation of public health interventions, since the causal relationship between intervention and outcome is usually largely isolated from sources of bias compared to other study designs (Victora et al., 2004). In contrast, Non-RCTs could be more plausible in regard of costs, timeliness and population enrolled. Nevertheless, the exposure to different sources of bias resulting from flexible methodological designs is greater in Non-RCTs than in RCTs. Furthermore, one can argue that in evaluations of the effectiveness of interventions is desirable to use RCTs and only take into account Non-RCTs when there is a gap of RCT evidence or in cases where it is impossible to conduct an RCT for ethical or practical reasons (De Brún, 2013; Norris et al., 2010). Therefore, the selection criteria will be: • Randomised Controlled Trials (RCTs) • Cluster-randomised Controlled Trials (cRCTs). Types of Participants
Studies will be eligible if they report on the following population: • Pregnant women • Women in childbearing age (15-49 years) • Children between 0 and 1 year

14
Types of Interventions
Studies will be included if they report at least one of the following types of intervention: • Community-based interventions • Structural changes to improve access to maternal and new-born care. • Changes of medical fees Types of Outcomes of interest
There will be evaluated the outcomes listed below for any period of follow-up:
Primary outcomes:
Maternal mortality ratio: defined as deaths that occur during pregnancy or childbirth or within 42 days after the birth, expressed as number of deaths per 100.000 live births.
Infant Mortality: Including perinatal, neonatal and post-neonatal mortality expressed as child deaths per 1.000 live births.
Secondary outcomes:
Regarding secondary outcomes that are expected to find in the selected studies for the review, there are many interest outcomes that could be derived by the interventions subject to analysis. The following list describe some of the most frequently outcomes that were reported in the studies included in systematic reviews as (Dzakpasu et al., 2014; Lassi & Bhutta, 2015; Lassi et al., 2011; Nyamtema et al., 2011).
Number of visits: studies that report changes in the number of visits of antenatal or
postnatal care. Proportion of births attended: percentage of births attended by skilled health
workers. Breastfeeding: studies that report changes in initiation, duration or frequency of
breastfeeding and postnatal care. Complications of pregnancy: including prolonged or obstructed labour, eclampsia,
postpartum haemorrhage, and postpartum depression.

15
Referral to health facilities: Studies reporting improvements in opportunity referral to an obstetric emergency facility to manage any complication during pregnancy, delivery, or the postpartum period.
Search methods for identification of studies
Electronic bibliographic databases
According to (De Brún, 2013) and other systematics reviews reviewed (Lassi & Bhutta, 2015; Lassi et al., 2011; Nyamtema et al., 2011) the most suitable electronic databases to retrived RCTs and cRTCs are: Cochrane Central, MEDLINE-PubMed, Medline (Ovid) and Embase. No language restriction will be applied. All electronic search strategies will be peer-reviewed. The detailed search strategy for each database is exposed in the Appendix 2.
Other resources
Websites International organizations and evidence-based review institutions will be consulted: • Campbell Collaboration CEBEI (Centre for Evidence Based Early Intervention) • World Bank e-library • 3ie • Clinicaltrials.gov
Grey literature When it comes to retrieve studies for a systematic review, it is possible to say that some of the relevant studies do not appear in journals but may be located in reports, which are not indexed in electronic databases (Petticrew & Roberts, 2006; The Cochrane Public Health Group, 2011). In this case, it will be necessary to invest time capturing the “grey” literature in others sources such as working papers, conference documents, reports from governmental and international entities, and other plausible references.

16
Data collection and analysis
Selection of studies
Search results will be managed with the software Mendeley 1.14 and duplicates will be removed. Two overview authors will independently assess for potential inclusion of studies following a two steps process: Firstly, each author independently will reviewed titles and abstracts and select every study that fits the PICOT question and the inclusion and exclusion criteria. Then, discrepancies will be resolved first by consensus or by a third member of the research team if no agreement is reached. Secondly, two researchers, repeating the process to dissipate discordances, will perform full text screening. The selection process and reasons for exclusion will be documented using the PRISMA flow diagram (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2009).
Data extraction and management
To extract the information of the selected studies, a data-extraction form will be used (Appendix 3) This extraction form is useful to standardise the data collected and it is an adaptation made by the authors based on the checklist of items to consider in (J. Higgins, 2011). Information will be extracted regarding source, eligibility, study design methodology, population and intervention details and comparison groups, outcomes, and effects.
Assessment of risk of bias in included studies
Risk of bias summary assessments for outcomes will follow The Cochrane Collaboration (J. P. Higgins & Altman, 2008) standards which evaluates seven aspects (sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and other sources of bias).

17
Quality of the evidence
The quality of the evidence will be assessed using the GRADE approach (Guyatt et al., 2011). This methodological approach considers evidence from RCTs as high quality, which will be graded by GRADE pro software to produce the tables of summary of findings.
Measures of treatment effect
Measures of treatment effects will come from primary data in the documents (means, standard deviations and sample size). Estimations for each intervention group will be reported by calculating the Risk Ratio (RR) for dichotomous outcomes, and risk differences (RD) for continuous outcomes with the respective 95% confidence interval. Adjusted measures of outcomes will be preferred, since demographic and baseline differences might exist. To synthesise the information, it will be conducted a meta-analysis following the stated in the Cochrane Handbook for Systematic Reviews of Interventions (J. Higgins, 2011).
Unit of analysis issues
The unit of analysis will be each women in childbearing age, mother or infant randomised. If Cluster RCTs are retrieved, those will be incorporated using the generic inverse variance method.
Dealing with missing data
The authors will be contacted if information or data is missing or incomplete. No data will be imputed for any of the outcomes, thus, if data is missing, for example, from one period of a follow-up, the data will be excluded from both periods of analysis.

18
Assessment of heterogeneity
Following the Cochrane Handbook for Systematic Reviews of Interventions (J. Higgins, 2011). the heterogeneity will be quantified through visual inspection of forest plot and by the I² statistic. The thresholds for interpreting I² will be: 0% to 25%: no heterogeneity; 25% to 49%: low heterogeneity; 40% to 74%: moderate heterogeneity; and 75%: high heterogeneity.
Assessment of reporting biases
Publication bias will be assessed if there are at least 10 trials for meta-analysis. Data synthesis
Meta-analysis will be performed using Review Manager 5.3 software. A fixed effect model will be applied if there are two or more RCTs with comparable interventions and populations. In the case of finding different scales to the same measures, the standardised mean differences (SMDs) will be calculated. For continuous data the mean and standard deviation will be extracted and the analysis will be performed using the weighted mean differences (WMD). Acknowledgements This protocol has been prepared under request of the Ministry of Health and Social Protection. As part of the pre-publication editorial process, four members of the research group have peer-reviewed this protocol.

19
Bibliography
Bhutta, Z. A., Das, J. K., Rizvi, A., Gaffey, M. F., Walker, N., Horton, S., … Black, R. E. (2013). Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? The Lancet, 382(9890), 452–477. http://doi.org/10.1016/S0140-6736(13)60996-4
Campbell, O. M., & Graham, W. J. (2006). Strategies for reducing maternal mortality: getting on with what works. The Lancet, 368(9543), 1284–1299. http://doi.org/10.1016/S0140-6736(06)69381-1
Cheng, J. J., Schuster-Wallace, C. J., Watt, S., Newbold, B. K., & Mente, A. (2012). An ecological quantification of the relationships between water, sanitation and infant, child, and maternal mortality. Environmental Health, 11, 4. http://doi.org/10.1186/1476-069X-11-4
Cochrane Editorial Unit. (2013, December). Methodological Expectations of Cochrane Intervention Reviews (MECIR). Retrieved from http://editorial-unit.cochrane.org/mecir
Concato, J., Shah, N., & Horwitz, R. I. (2000). Randomized, controlled trials, observational studies, and the hierarchy of research designs. The New England Journal of Medicine, 342(25), 1887–1892.
Crowther, C. A., Hiller, J. E., Moss, J. R., McPhee, A. J., Jeffries, W. S., & Robinson, J. S. (2005). Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes. New England Journal of Medicine, 352(24), 2477–2486. http://doi.org/10.1056/NEJMoa042973
De Brún, C. (2013, July 11). Finding the Evidence. A key step in the information production process.
Dzakpasu, S., Powell-Jackson, T., & Campbell, O. M. R. (2014). Impact of user fees on maternal health service utilization and related health outcomes: a systematic review. Health Policy and Planning, 29(2), 137–150. http://doi.org/10.1093/heapol/czs142
Gakidou, E., Cowling, K., Lozano, R., & Murray, C. J. (2010). Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis. The Lancet, 376(9745), 959–974. http://doi.org/10.1016/S0140-6736(10)61257-3
Guyatt, G., Oxman, A. D., Akl, E. A., Kunz, R., Vist, G., Brozek, J., … Schünemann, H. J. (2011). GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings
20
tables. Journal of Clinical Epidemiology, 64(4), 383–394. http://doi.org/10.1016/j.jclinepi.2010.04.026
Higgins, J. (2011). Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration.
Higgins, J. P., & Altman, D. G. (2008). Assessing Risk of Bias in Included Studies. In J. P. H. S. S. V. Fellow & S. G. F. Director (Eds.), Cochrane Handbook for Systematic Reviews of Interventions (pp. 187–241). John Wiley & Sons, Ltd. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/9780470712184.ch8/summary
Kidney, E., Winter, H. R., Khan, K. S., Gülmezoglu, A. M., Meads, C. A., Deeks, J. J., & MacArthur, C. (2009). Systematic review of effect of community-level interventions to reduce maternal mortality. BMC Pregnancy and Childbirth, 9(1), 2. http://doi.org/10.1186/1471-2393-9-2
Lassi, Z. S., & Bhutta, Z. A. (2015). Community-based intervention packages for reducing maternal and neonatal morbidity and mortality and improving neonatal outcomes. In The Cochrane Collaboration (Ed.), Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd. Retrieved from http://doi.wiley.com/10.1002/14651858.CD007754.pub3
Lassi, Z. S., Haider, B. A., & Bhutta, Z. A. (2011). Community-based intervention packages for reducing maternal morbidity and mortality and improving neonatal outcomes (Systematic Review No. 5). International Initiative for impact Evaluation.
Lori, J. R., & Starke, A. E. (2012). A critical analysis of maternal morbidity and mortality in Liberia, West Africa. Midwifery, 28(1), 67–72. http://doi.org/10.1016/j.midw.2010.12.001
Ministerio de Salud y Protección Social, & Organización Panamericana de la Salud. (2012). Estimación de línea basal de mortalidad perinatal y análisis por tasas de periodos de riesgo perinatal (PPR o BABIES) y por PPR ajustado por estratos (MOMS).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine, 6(7), e1000097. http://doi.org/10.1371/journal.pmed.1000097
Norris, S., Atkins, D., Bruening, W., Fox, S., Johnson, E., Kane, R., … Oremus, M. (2010, June). Selecting observational studies for comparing medical interventions. Agency for Healthcare Research and Quality. Methods Guide for Comparative Effectiveness Reviews. Retrieved from http://www.effectivehealthcare.ahrq.gov/ehc/products/196/454/MethodsGuideNorris_06042010.pdf

21
Nyamtema, A. S., Urassa, D. P., & van Roosmalen, J. (2011). Maternal health interventions in resource limited countries: a systematic review of packages, impacts and factors for change. BMC Pregnancy and Childbirth, 11(1), 30. http://doi.org/10.1186/1471-2393-11-30
Okwaraji, Y. B., Cousens, S., Berhane, Y., Mulholland, K., & Edmond, K. (2012). Effect of Geographical Access to Health Facilities on Child Mortality in Rural Ethiopia: A Community Based Cross Sectional Study. PLOS ONE, 7(3), e33564. http://doi.org/10.1371/journal.pone.0033564
Petticrew, M., & Roberts, H. (2006). Systematic reviews in the social sciences: a practical guide. Malden, MA ; Oxford: Blackwell Pub.
PNUD. (2015). Objetivos de Desarrollo del Milenio. Informe 2015.
Sachs, J. (2005). The Millennium Project: a plan for meeting the Millenium Development. Lancet, 365: 347–53.
Salam, R. A., Das, J. K., Ali, A., Lassi, Z. S., & Bhutta, Z. A. (2013). Maternal undernutrition and intrauterine growth restriction. Expert Review of Obstetrics & Gynecology, 8(6), 559–567. http://doi.org/10.1586/17474108.2013.850857
Sibley, L. M., Sipe, T. A., & Barry, D. (2012). Traditional birth attendant training for improving health behaviours and pregnancy outcomes. In The Cochrane Collaboration (Ed.), Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd. Retrieved from http://doi.wiley.com/10.1002/14651858.CD005460.pub3
The Cochrane Public Health Group. (2011). Guide for developing a Cochrane protocol.
UN. (2015). Millennium Development Goals. Retrieved 25 May 2016, from http://www.un.org/millenniumgoals/childhealth.shtml
Victora, C. G., Habicht, J.-P., & Bryce, J. (2004). Evidence-based public health: moving beyond randomized trials. American Journal of Public Health, 94(3), 400–405.
West, S. G., & Thoemmes, F. (2010). Campbell’s and Rubin’s perspectives on causal inference. Psychological Methods, 15(1), 18–37. http://doi.org/10.1037/a0015917
WHO. (2016). World health statistics 2016: monitoring health for the SDGs, sustainable development goals. World Health Organization.

22
Appendix 1. Maternal, Neonatal and Under 5 mortality in 2015 by Latin-American Countries.
Country MMR per 100.000
Live Births NMR per 1.000
Live Births U5MR per 1.000
Live Births
Argentina 52 6,3 12,5 Bolivia 206 19,6 38,4 Brazil 44 8,9 16,4 Chile 22 4,9 8,1 Colombia 64 8,5 15,9 Costa Rica 25 6,2 9,7 Cuba 39 5,5 2,3 Ecuador 64 10,8 21,0 El Salvador 54 8,3 16,8 Guatemala 88 13,4 29,1 Haití 359 25,4 69,0 Honduras 129 11,0 20,4 Mexico 38 7,0 13,2 Nicaragua 150 9,8 22,1 Panama 94 9,6 17,0 Paraguay 132 10,9 20,5 Peru 68 8,2 16,9 Dominican R. 92 21,7 30,9
Uruguay 15 5,1 10,1 Venezuela 95 8,9 14,9
Fuente:WHO (2016)
MMR: Maternal Mortality Ratio; NMR: Neonatal Mortality Rate; U5MR: Under Five Mortality Rate.
Appendix 2. Search strategies
PubMed search strategy
1 Search "Randomized Controlled Trial" [Publication Type]
2 Search random*[Title/Abstract]
3 Search (#1 OR #2 )

23
4 Search "Maternal Mortality"[Mesh]
5 Search "Maternal Death"[Mesh]
6 Search "Infant Death"[Mesh]
7 Search "Infant Mortality"[Mesh]
8 Search (#4 OR #5 OR #6 OR #7)
9 Search (#3 AND #8)
Embase search strategy 1 randomized controlled trial'/exp
2 random*'/exp
3 #1 OR #2
4 maternal mortality'/exp
5 infant mortality'/exp
6 #4 OR #5
7 #3 AND #6
Medline (Ovid) search strategy
1 Randomized Controlled Trial.pt.
2 "random* ".ab,ti.
3 1 or 2
4 Maternal Mortality.sh.
5 Maternal Death.sh.
6 Infant Death.sh.
7 Infant Mortality.sh.
8 4 or 5 or 6 or 7
9 3 and 8

24
Cochrane Central Register of Controlled Trials - EBM Reviews (Ovid) search strategy
1 Maternal Mortality.sh.
2 Infant Death.sh.
3 Infant Mortality.sh.
4 1 or 2 or 3
Appendix 3. Data extraction form
Data to be extracted Notes to reviewer Title of study Author Year of publication Where was published? Screening questions Does this study focus on interventions to redece maternal or infant mortality? Is the study design as an RCT? Intervention Description of the intervention Duration of programme Trial design and execution How were participants or units randomised? Description of the Control Group N - Treatment N - Control Who performed the randomisation? Trial registration What method was used for randomisation? Was randomisation the same across all sites/cohorts? How many intervention groups were reported? When was recruitment undertaken? What was the response rate for recruitment? When was the intervention implemented and data collected?

25
Are there conflicts of interest or evidence of allegiance bias? What were the inclusion and exclusion criteria for study participants? What was the overall attrition? What was the definition of a treatment completer? Implementation Did the study report any planned or unplanned deviation from protocol? Where was the intervention implemented? What was the service context? Is the trial led by the treatment developer? What quality control mechanisms were in place? Were any quality control problems? Baseline characteristics Was a baseline collected?
What were demographics relating to race and ethnicity by arm?
White: % Black: % Latino: % Asian: %
Where there any significant observed baseline difference? Moderators At what level were participants or units randomised? Does the study focus on a sub-group? Outcomes and analysis What were the outcomes for this study? Form of Outcome Assessment Which population/grades are represented in the analyses? How are the outcomes calculated and tested? (mean/OR/ES, within-subjects/between-subjects) Are analyses intention-to-treat? Are analyses treatment on the treat? How were missing data handled? Which follow-up periods are specified?
26
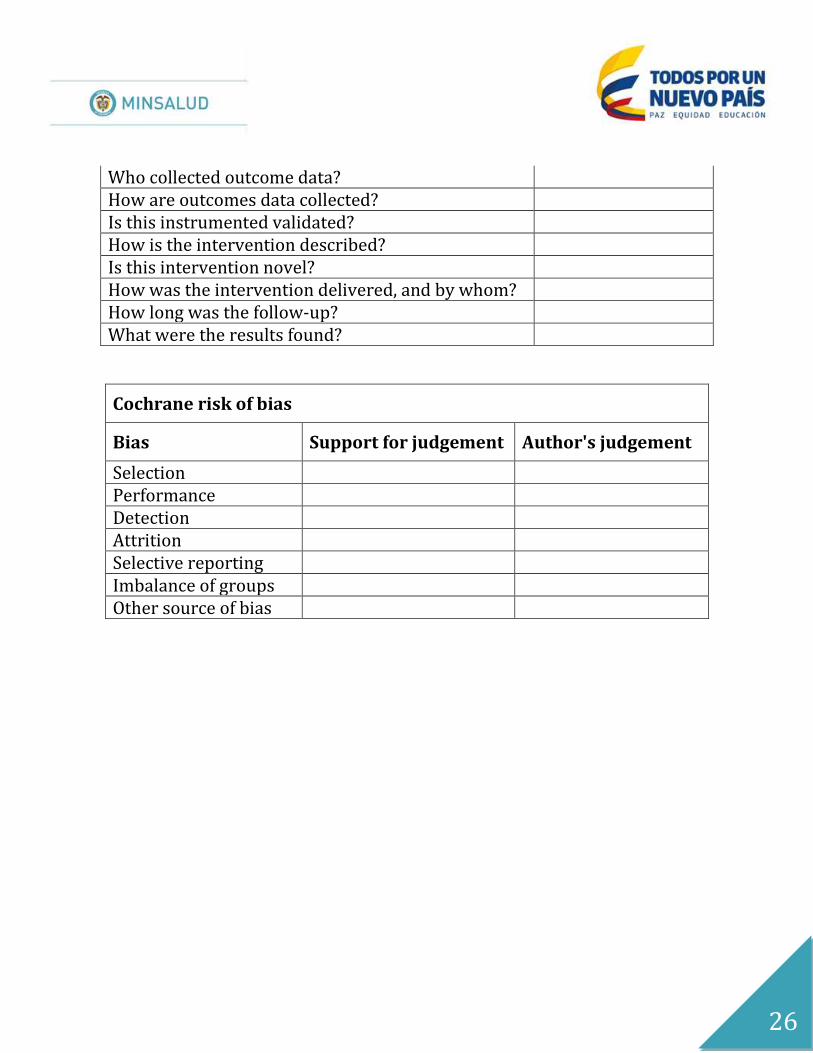
Who collected outcome data? How are outcomes data collected? Is this instrumented validated? How is the intervention described? Is this intervention novel? How was the intervention delivered, and by whom? How long was the follow-up? What were the results found?
Cochrane risk of bias
Bias Support for judgement Author's judgement
Selection Performance Detection Attrition Selective reporting Imbalance of groups Other source of bias