Interventional Innovation I: Coronary Interventions and ......Study Title Sirolimus Eluting...
19
S irolimus A ngioplasty B alloon for In-Stent Re stenosis (SABRE) Trial: 3-Year Clinical Follow-Up Interventional Innovation I : Coronary Interventions and Technologies Stefan Verheye (SABRE PI), Mathias Vrolix , Indulis Kumsars , Andrejs Erglis , Dace Sondore , Pierfrancesco Agostoni , Pieter Stella, Kristoff Cornelis, Luc Janssens, Michael Maeng , Ton Slagboom , Giovanni Amoroso, Lisette Okkels Jensen, Per Thayssen Juan F. Granada, MD On Behalf of SABRE Investigators
Transcript of Interventional Innovation I: Coronary Interventions and ......Study Title Sirolimus Eluting...
Sirolimus Angioplasty Balloon for
In-Stent Restenosis (SABRE) Trial:
3-Year Clinical Follow-Up
Interventional Innovation I: Coronary Interventions and Technologies
Stefan Verheye (SABRE PI), Mathias Vrolix, Indulis Kumsars, Andrejs Erglis, Dace Sondore,
Pierfrancesco Agostoni, Pieter Stella, Kristoff Cornelis, Luc Janssens, Michael Maeng,
Ton Slagboom, Giovanni Amoroso, Lisette Okkels Jensen, Per Thayssen
Juan F. Granada, MDOn Behalf of SABRE Investigators
• I, Juan F. Granada DO NOT have a personal financial
interest/arrangement or affiliation with one or more organizations that
could be perceived as a real or apparent conflict of interest in the context
of the subject of this presentation
• Caliber therapeutics has performed sponsored clinical at the
Cardiovascular Research Foundation within the last 12 months
Disclosure Statement of Financial Interest
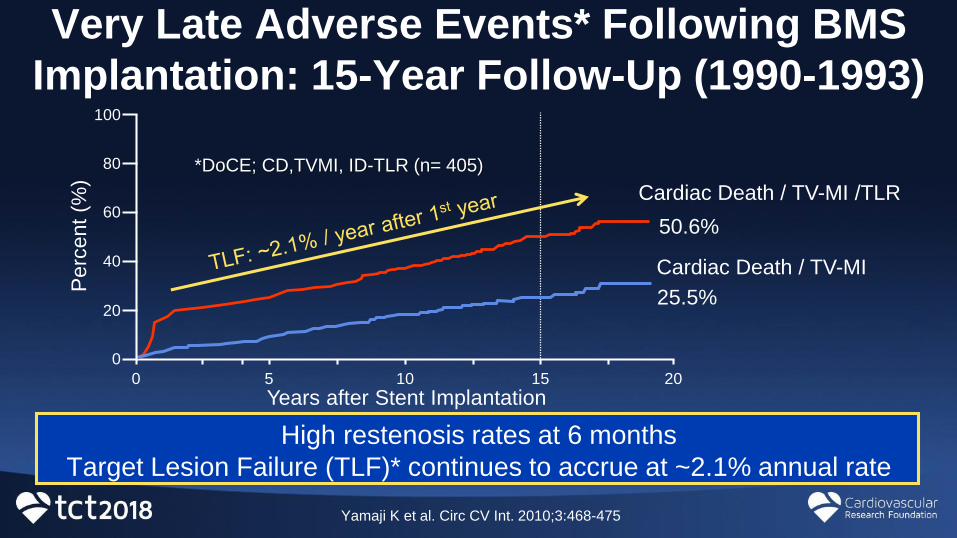
Very Late Adverse Events* Following BMS
Implantation: 15-Year Follow-Up (1990-1993)
High restenosis rates at 6 months
Target Lesion Failure (TLF)* continues to accrue at ~2.1% annual rate
Perc
ent
(%)
Cardiac Death / TV-MI
Cardiac Death / TV-MI /TLR
Years after Stent Implantation
50.6%
25.5%
100
80
60
40
20
0
0 5 10 15 20
Yamaji K et al. Circ CV Int. 2010;3:468-475
*DoCE; CD,TVMI, ID-TLR (n= 405)
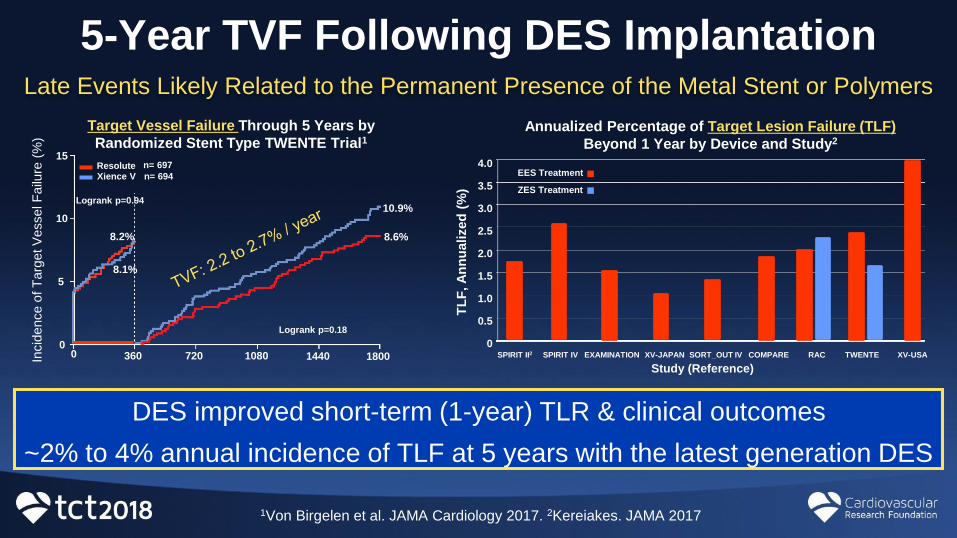
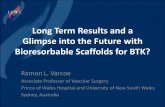
5-Year TVF Following DES ImplantationLate Events Likely Related to the Permanent Presence of the Metal Stent or Polymers
Target Vessel Failure Through 5 Years by
Randomized Stent Type TWENTE Trial115
10
5
00 360 720 1080 1440 1800
Logrank p=0.18
Logrank p=0.94
8.2%
8.1%
8.6%
10.9%
Incid
ence o
f T
arg
et V
esselF
ailu
re(%
)
n= 697
n= 694ResoluteXience V
1Von Birgelen et al. JAMA Cardiology 2017. 2Kereiakes. JAMA 2017
SPIRIT II2 SPIRIT IV EXAMINATION XV-JAPAN SORT_OUT IV COMPARE RAC TWENTE XV-USA
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0
Annualized Percentage of Target Lesion Failure (TLF)
Beyond 1 Year by Device and Study2
EES Treatment
ZES Treatment
Study (Reference)
TL
F, A
nn
ualized
(%
)
DES improved short-term (1-year) TLR & clinical outcomes
~2% to 4% annual incidence of TLF at 5 years with the latest generation DES
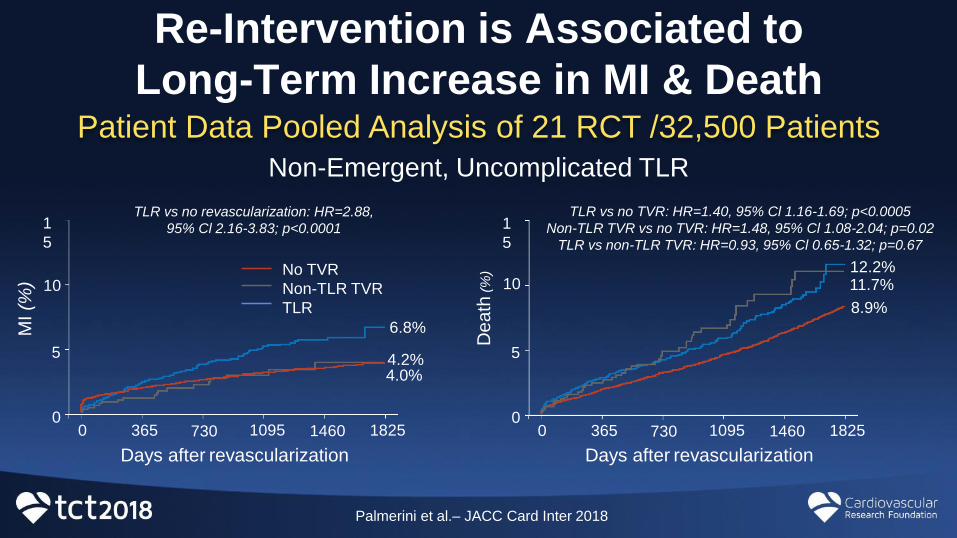
Re-Intervention is Associated to
Long-Term Increase in MI & DeathPatient Data Pooled Analysis of 21 RCT /32,500 Patients
De
ath
(%)
0 365 730 1095 1460 1825
5
10
1
5
0
Days after revascularization
TLR vs no TVR: HR=1.40, 95% Cl 1.16-1.69; p<0.0005
Non-TLR TVR vs no TVR: HR=1.48, 95% Cl 1.08-2.04; p=0.02
TLR vs non-TLR TVR: HR=0.93, 95% Cl 0.65-1.32; p=0.67
12.2%11.7%
8.9%
No TVR
Non-TLR TVR
TLR
0 365 730 1095 1460 1825
5
10
1
5
0
6.8%
4.2%4.0%
MI(%
)
Days after revascularization
TLR vs no revascularization: HR=2.88,
95% Cl 2.16-3.83; p<0.0001
Non-Emergent, Uncomplicated TLR
Palmerini et al.– JACC Card Inter 2018
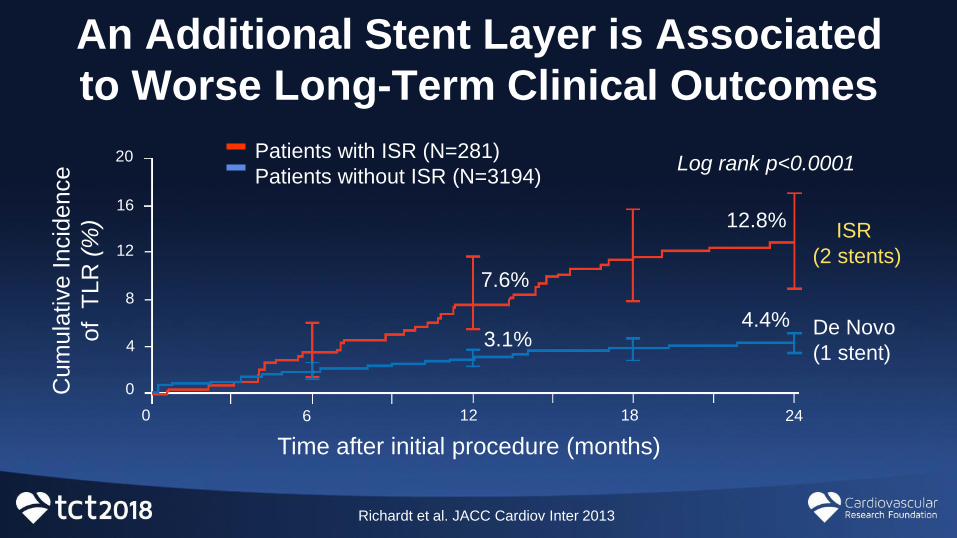
An Additional Stent Layer is Associated
to Worse Long-Term Clinical Outcomes
0
8
16
20
4
12
0 6 12 18 24
ISR
(2 stents)
De Novo
(1 stent)
12.8%
Cum
ula
tive I
ncid
ence
of T
LR
(%)
Time after initial procedure (months)
Log rank p<0.0001
4.4%
7.6%
3.1%
Patients with ISR (N=281)
Patients without ISR (N=3194)
Richardt et al. JACC Cardiov Inter 2013
Balloon-Based Sirolimus DeliveryDesign Requirements
• Dose uniformity and reliability is compromised by inefficient drug
transfer from balloon surface; a dedicated delivery mechanism is
required
• Tissue absorption is limited following acute drug transfer:
Sirolimus degradation / diffusion occurs; “drug protection” (i.e.,
encapsulation) is needed
Sirolimus half life is short (~62-hours) and biological effect depends
on maintaining therapeutic levels (sustained and controlled drug
delivery favored)
• Distal embolization must be minimized or eliminated
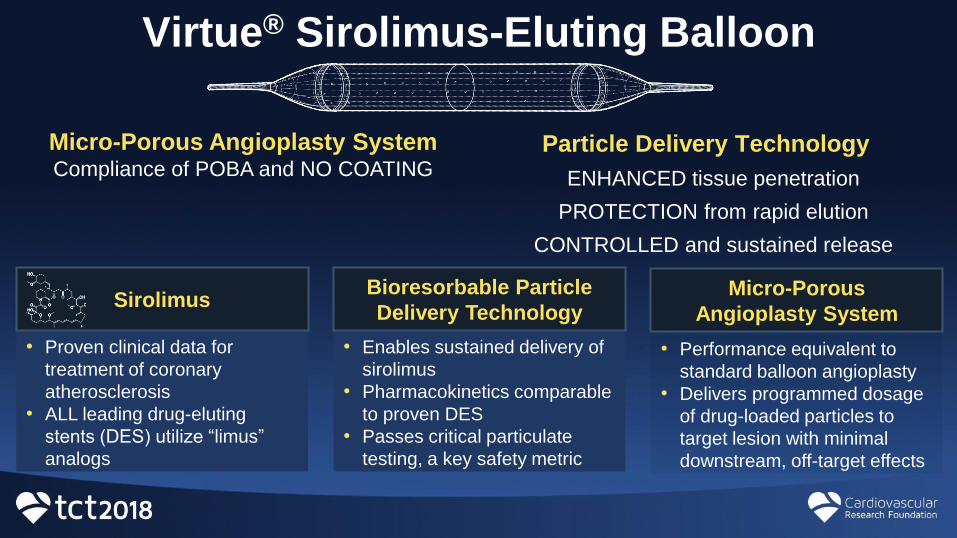
Virtue® Sirolimus-Eluting Balloon
Particle Delivery Technology
ENHANCED tissue penetration
PROTECTION from rapid elution
CONTROLLED and sustained release
Micro-Porous Angioplasty SystemCompliance of POBA and NO COATING
• Proven clinical data for
treatment of coronary
atherosclerosis
• ALL leading drug-eluting
stents (DES) utilize “limus”
analogs
Sirolimus
• Enables sustained delivery of
sirolimus
• Pharmacokinetics comparable
to proven DES
• Passes critical particulate
testing, a key safety metric
Bioresorbable Particle
Delivery Technology
• Performance equivalent to
standard balloon angioplasty
• Delivers programmed dosage
of drug-loaded particles to
target lesion with minimal
downstream, off-target effects
Micro-Porous
Angioplasty System
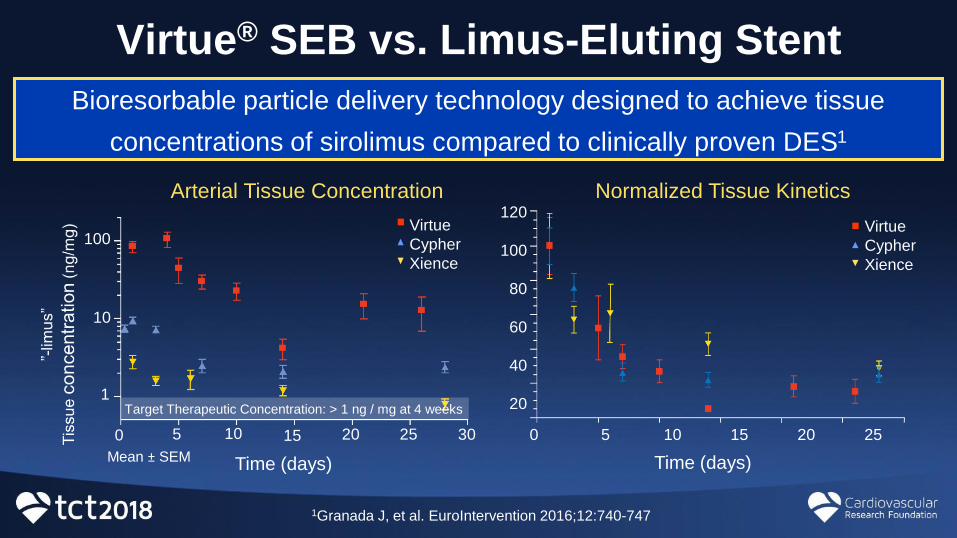
Virtue® SEB vs. Limus-Eluting Stent
Bioresorbable particle delivery technology designed to achieve tissue
concentrations of sirolimus compared to clinically proven DES1
1Granada J, et al. EuroIntervention 2016;12:740-747
Arterial Tissue Concentration
Time (days)Mean ± SEM
100
10
1
0 5 10 15 20 25 30
Virtue
Cypher
Xience
Target Therapeutic Concentration: > 1 ng / mg at 4 weeks
Time (days)
120
100
80
60
40
20
0 5 10 15 20 25
Normalized Tissue Kinetics
Virtue
Cypher
Xience
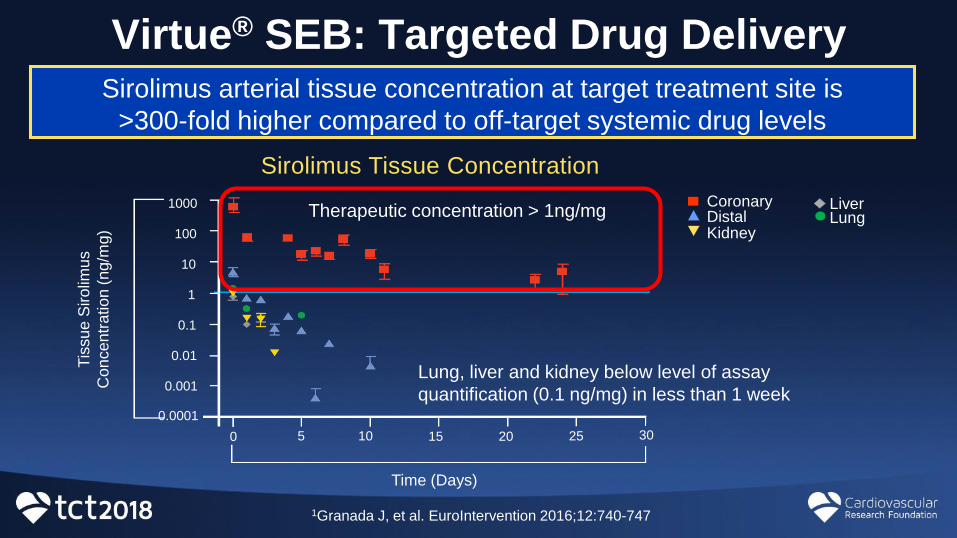
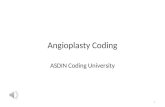
Virtue® SEB: Targeted Drug DeliverySirolimus arterial tissue concentration at target treatment site is
>300-fold higher compared to off-target systemic drug levels
Therapeutic concentration > 1ng/mg
Lung, liver and kidney below level of assay
quantification (0.1 ng/mg) in less than 1 week
Sirolimus Tissue Concentration
CoronaryDistalKidney
LiverLung
1000
100
10
1
0.1
0.01
0.001
0.0001
10 15 20 25 3050
Tis
su
e S
iro
limu
s
Con
ce
ntr
atio
n (
ng/m
g)
Time (Days)
1Granada J, et al. EuroIntervention 2016;12:740-747
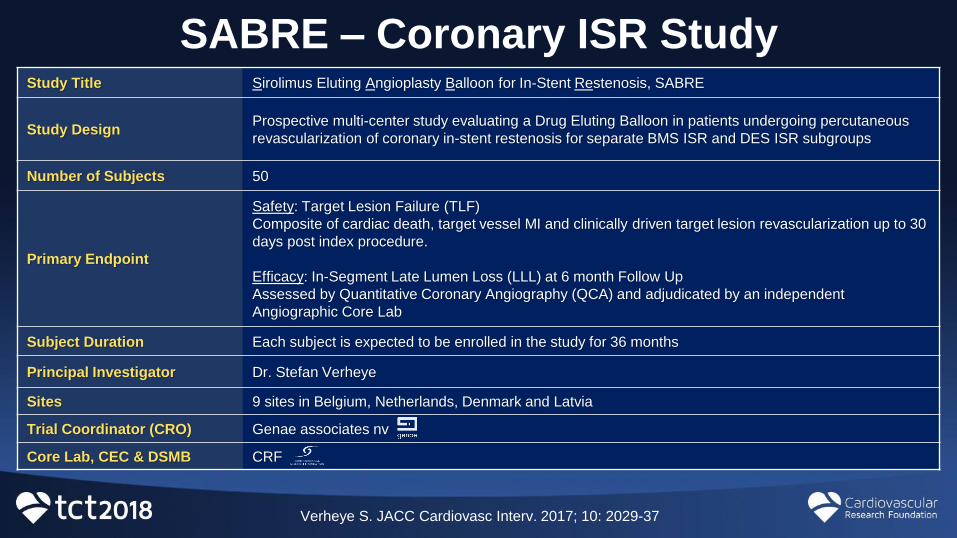
SABRE – Coronary ISR StudyStudy Title Sirolimus Eluting Angioplasty Balloon for In-Stent Restenosis, SABRE
Study DesignProspective multi-center study evaluating a Drug Eluting Balloon in patients undergoing percutaneous
revascularization of coronary in-stent restenosis for separate BMS ISR and DES ISR subgroups
Number of Subjects 50
Primary Endpoint
Safety: Target Lesion Failure (TLF)
Composite of cardiac death, target vessel MI and clinically driven target lesion revascularization up to 30
days post index procedure.
Efficacy: In-Segment Late Lumen Loss (LLL) at 6 month Follow Up
Assessed by Quantitative Coronary Angiography (QCA) and adjudicated by an independent
Angiographic Core Lab
Subject Duration Each subject is expected to be enrolled in the study for 36 months
Principal Investigator Dr. Stefan Verheye
Sites 9 sites in Belgium, Netherlands, Denmark and Latvia
Trial Coordinator (CRO) Genae associates nv
Core Lab, CEC & DSMB CRF
Verheye S. JACC Cardiovasc Interv. 2017; 10: 2029-37
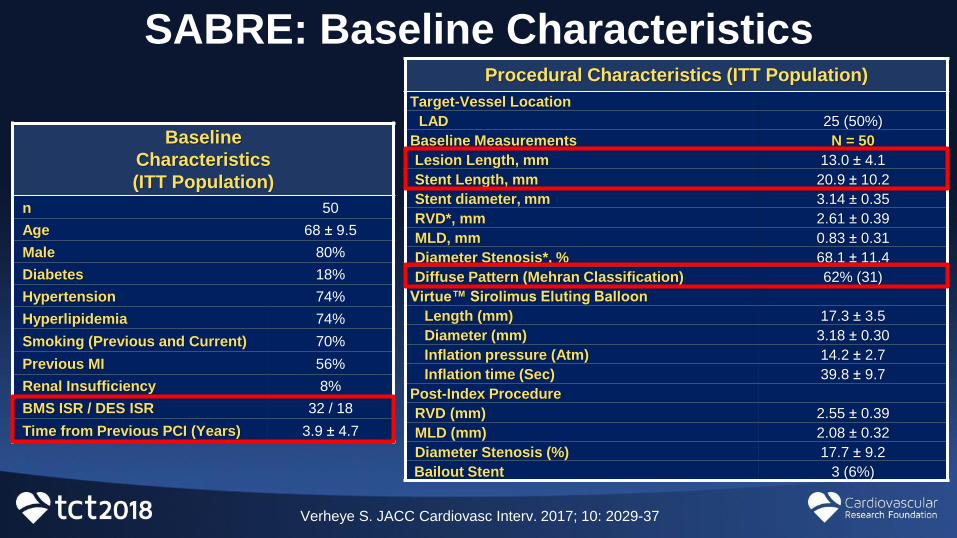
SABRE: Baseline Characteristics
Baseline
Characteristics
(ITT Population)
n 50
Age 68 ± 9.5
Male 80%
Diabetes 18%
Hypertension 74%
Hyperlipidemia 74%
Smoking (Previous and Current) 70%
Previous MI 56%
Renal Insufficiency 8%
BMS ISR / DES ISR 32 / 18
Time from Previous PCI (Years) 3.9 ± 4.7
Procedural Characteristics (ITT Population)
Target-Vessel Location
LAD 25 (50%)
Baseline Measurements N = 50
Lesion Length, mm 13.0 ± 4.1
Stent Length, mm 20.9 ± 10.2
Stent diameter, mm 3.14 ± 0.35
RVD*, mm 2.61 ± 0.39
MLD, mm 0.83 ± 0.31
Diameter Stenosis*, % 68.1 ± 11.4
Diffuse Pattern (Mehran Classification) 62% (31)
Virtue™ Sirolimus Eluting Balloon
Length (mm) 17.3 ± 3.5
Diameter (mm) 3.18 ± 0.30
Inflation pressure (Atm) 14.2 ± 2.7
Inflation time (Sec) 39.8 ± 9.7
Post-Index Procedure
RVD (mm) 2.55 ± 0.39
MLD (mm) 2.08 ± 0.32
Diameter Stenosis (%) 17.7 ± 9.2
Bailout Stent 3 (6%)
Verheye S. JACC Cardiovasc Interv. 2017; 10: 2029-37
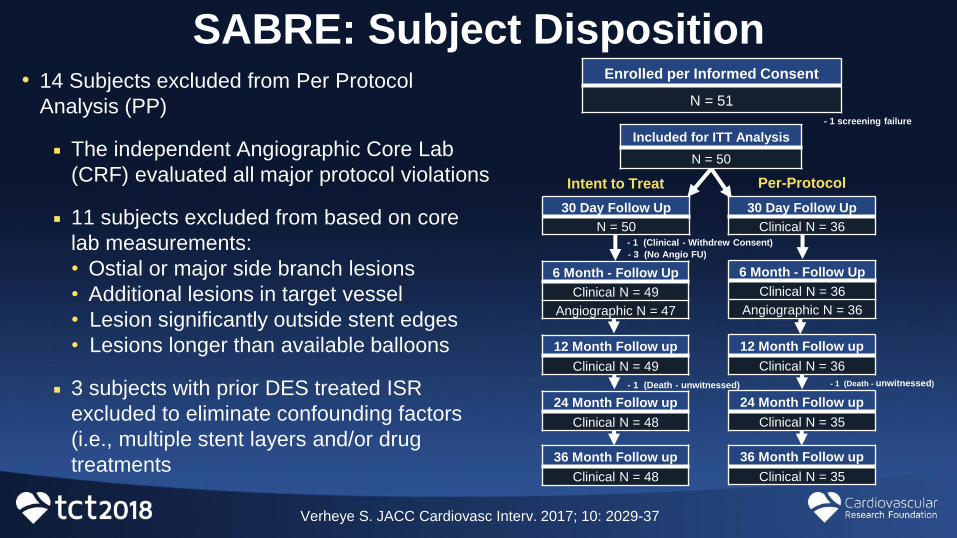
SABRE: Subject Disposition• 14 Subjects excluded from Per Protocol
Analysis (PP)
The independent Angiographic Core Lab
(CRF) evaluated all major protocol violations
11 subjects excluded from based on core
lab measurements:
• Ostial or major side branch lesions
• Additional lesions in target vessel
• Lesion significantly outside stent edges
• Lesions longer than available balloons
3 subjects with prior DES treated ISR
excluded to eliminate confounding factors
(i.e., multiple stent layers and/or drug
treatments
Intent to Treat Per-Protocol
- 1 screening failure
Enrolled per Informed Consent
N = 51
Included for ITT Analysis
N = 50
30 Day Follow Up
N = 50
30 Day Follow Up
Clinical N = 36
- 3 (No Angio FU)
- 1 (Clinical - Withdrew Consent)
- 1 (Death - unwitnessed)
6 Month - Follow Up
Clinical N = 49
Angiographic N = 47
6 Month - Follow Up
Clinical N = 36
Angiographic N = 36
12 Month Follow up
Clinical N = 49
12 Month Follow up
Clinical N = 36
24 Month Follow up
Clinical N = 48
24 Month Follow up
Clinical N = 35
36 Month Follow up
Clinical N = 48
36 Month Follow up
Clinical N = 35
- 1 (Death - unwitnessed)
Verheye S. JACC Cardiovasc Interv. 2017; 10: 2029-37
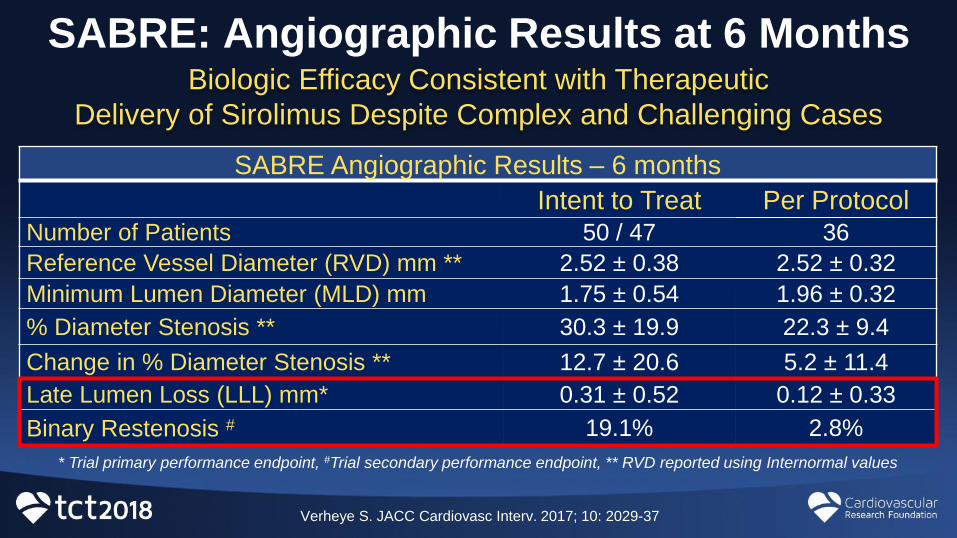
SABRE: Angiographic Results at 6 Months Biologic Efficacy Consistent with Therapeutic
Delivery of Sirolimus Despite Complex and Challenging Cases
SABRE Angiographic Results – 6 months
Intent to Treat Per Protocol Number of Patients 50 / 47 36
Reference Vessel Diameter (RVD) mm ** 2.52 ± 0.38 2.52 ± 0.32
Minimum Lumen Diameter (MLD) mm 1.75 ± 0.54 1.96 ± 0.32
% Diameter Stenosis ** 30.3 ± 19.9 22.3 ± 9.4
Change in % Diameter Stenosis ** 12.7 ± 20.6 5.2 ± 11.4
Late Lumen Loss (LLL) mm* 0.31 ± 0.52 0.12 ± 0.33
Binary Restenosis # 19.1% 2.8%
* Trial primary performance endpoint, #Trial secondary performance endpoint, ** RVD reported using Internormal values
Verheye S. JACC Cardiovasc Interv. 2017; 10: 2029-37
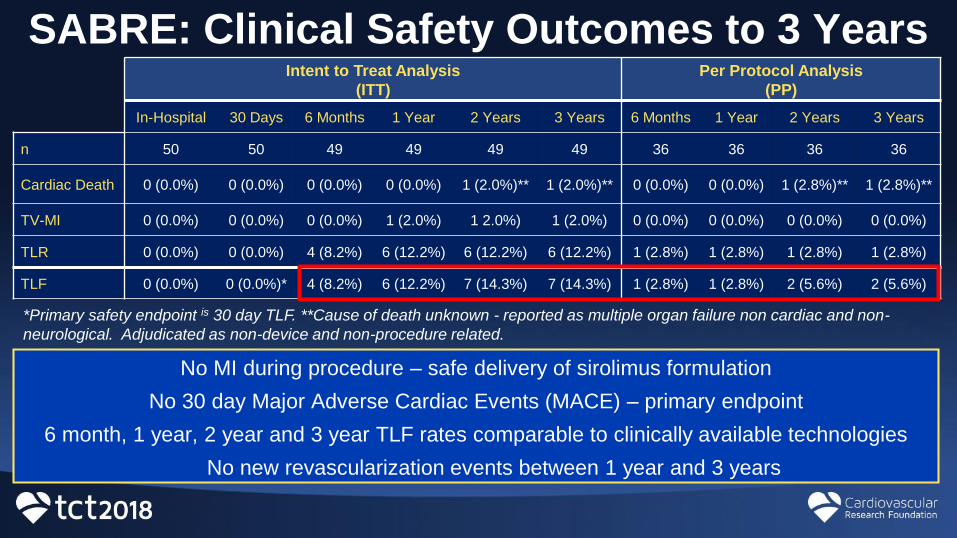
SABRE: Clinical Safety Outcomes to 3 YearsIntent to Treat Analysis
(ITT)
Per Protocol Analysis
(PP)
In-Hospital 30 Days 6 Months 1 Year 2 Years 3 Years 6 Months 1 Year 2 Years 3 Years
n 50 50 49 49 49 49 36 36 36 36
Cardiac Death 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 1 (2.0%)** 1 (2.0%)** 0 (0.0%) 0 (0.0%) 1 (2.8%)** 1 (2.8%)**
TV-MI 0 (0.0%) 0 (0.0%) 0 (0.0%) 1 (2.0%) 1 2.0%) 1 (2.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%)
TLR 0 (0.0%) 0 (0.0%) 4 (8.2%) 6 (12.2%) 6 (12.2%) 6 (12.2%) 1 (2.8%) 1 (2.8%) 1 (2.8%) 1 (2.8%)
TLF 0 (0.0%) 0 (0.0%)* 4 (8.2%) 6 (12.2%) 7 (14.3%) 7 (14.3%) 1 (2.8%) 1 (2.8%) 2 (5.6%) 2 (5.6%)
*Primary safety endpoint is 30 day TLF. **Cause of death unknown - reported as multiple organ failure non cardiac and non-
neurological. Adjudicated as non-device and non-procedure related.
No MI during procedure – safe delivery of sirolimus formulation
No 30 day Major Adverse Cardiac Events (MACE) – primary endpoint
6 month, 1 year, 2 year and 3 year TLF rates comparable to clinically available technologies
No new revascularization events between 1 year and 3 years
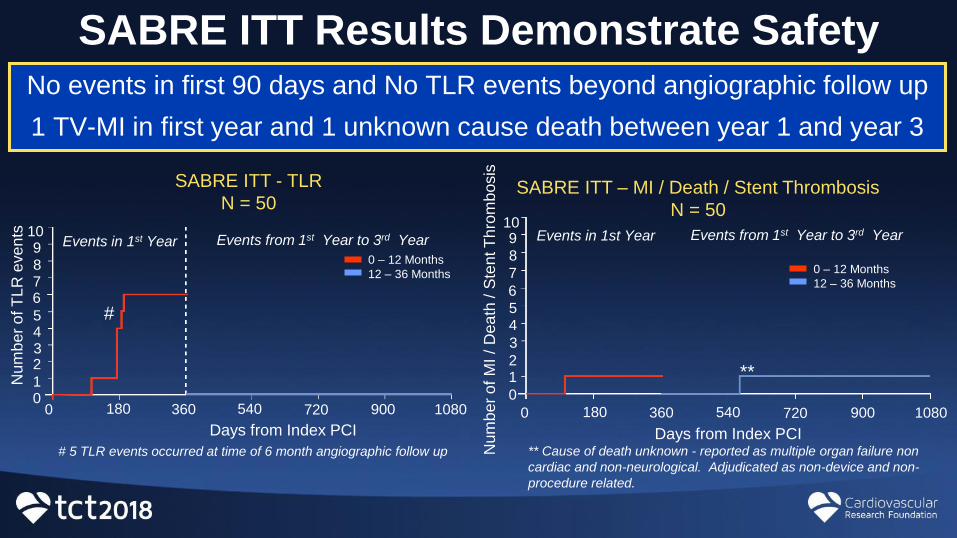
SABRE ITT Results Demonstrate SafetyNo events in first 90 days and No TLR events beyond angiographic follow up
1 TV-MI in first year and 1 unknown cause death between year 1 and year 3
#
Events from 1st Year to 3rd YearEvents in 1st Year
180 360 540 720 900 1080
1098
6
4
7
5
32
10
0
0 – 12 Months
12 – 36 Months
Nu
mb
er
of T
LR
eve
nts
SABRE ITT - TLR
N = 50
# 5 TLR events occurred at time of 6 month angiographic follow up
Days from Index PCI
** Cause of death unknown - reported as multiple organ failure non
cardiac and non-neurological. Adjudicated as non-device and non-
procedure related.
**
Events in 1st Year Events from 1st Year to 3rd Year
Num
be
r o
f M
I /
Dea
th / S
ten
t T
hro
mb
osis
SABRE ITT – MI / Death / Stent Thrombosis
N = 50109
8
6
4
7
5
3
21
0
180 360 540 720 900 10800
0 – 12 Months
12 – 36 Months
Days from Index PCI
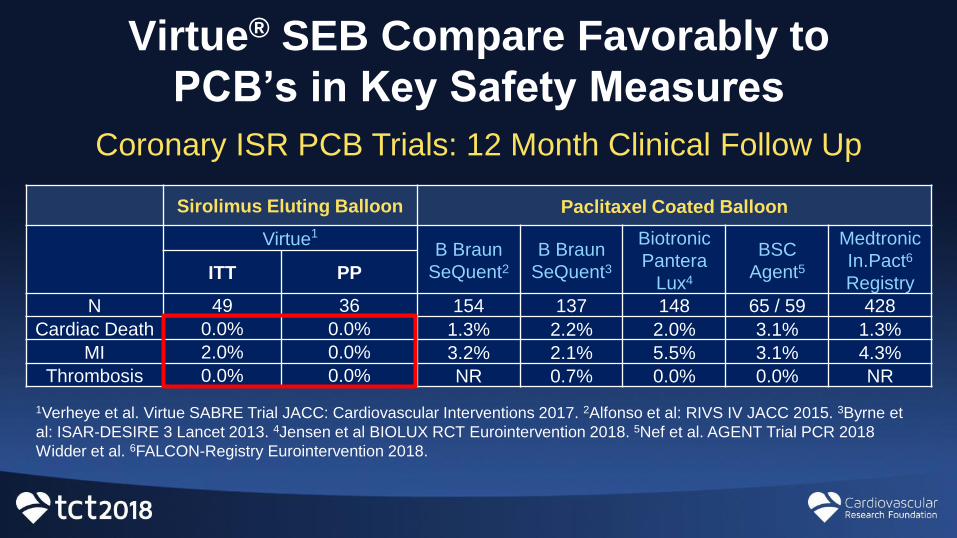
Virtue® SEB Compare Favorably to
PCB’s in Key Safety Measures
Sirolimus Eluting Balloon Paclitaxel Coated Balloon
Virtue1
B Braun
SeQuent2B Braun
SeQuent3
Biotronic
Pantera
Lux4
BSC
Agent5
Medtronic
In.Pact6
RegistryITT PP
N 49 36 154 137 148 65 / 59 428
Cardiac Death 0.0% 0.0% 1.3% 2.2% 2.0% 3.1% 1.3%
MI 2.0% 0.0% 3.2% 2.1% 5.5% 3.1% 4.3%
Thrombosis 0.0% 0.0% NR 0.7% 0.0% 0.0% NR
Coronary ISR PCB Trials: 12 Month Clinical Follow Up
1Verheye et al. Virtue SABRE Trial JACC: Cardiovascular Interventions 2017. 2Alfonso et al: RIVS IV JACC 2015. 3Byrne et
al: ISAR-DESIRE 3 Lancet 2013. 4Jensen et al BIOLUX RCT Eurointervention 2018. 5Nef et al. AGENT Trial PCR 2018
Widder et al. 6FALCON-Registry Eurointervention 2018.
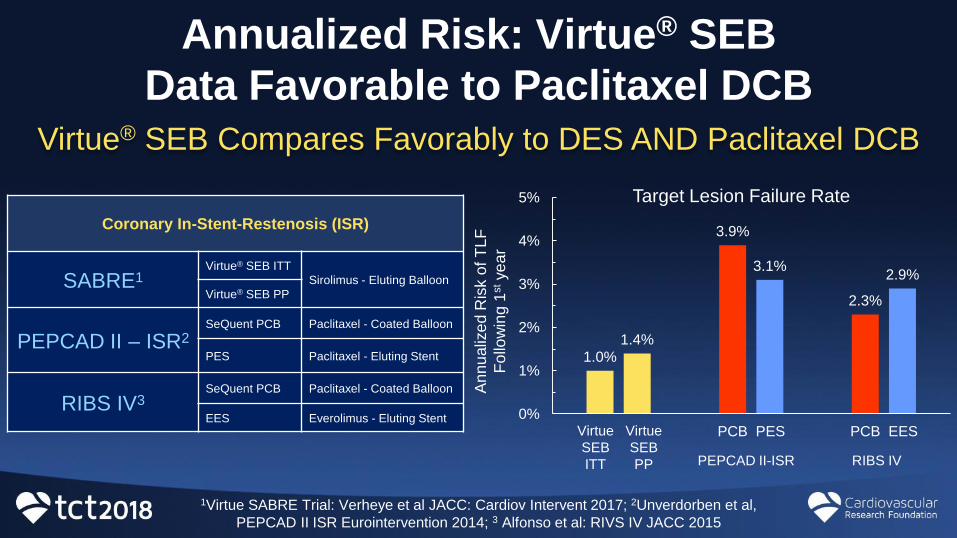
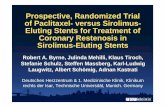
Annualized Risk: Virtue® SEB
Data Favorable to Paclitaxel DCBVirtue® SEB Compares Favorably to DES AND Paclitaxel DCB
1.0%
3.9%
2.3%
1.4%
3.1%2.9%
0%
1%
2%
3%
4%
5%
PCB PES PCB EESVirtue
SEB
ITT
Virtue
SEB
PPA
nn
ualiz
ed
Ris
k o
f T
LF
Fo
llow
ing 1
stye
ar
1Virtue SABRE Trial: Verheye et al JACC: Cardiov Intervent 2017; 2Unverdorben et al,
PEPCAD II ISR Eurointervention 2014; 3 Alfonso et al: RIVS IV JACC 2015
Target Lesion Failure Rate
PEPCAD II-ISR RIBS IV
Coronary In-Stent-Restenosis (ISR)
SABRE1Virtue® SEB ITT
Sirolimus - Eluting Balloon
Virtue® SEB PP
PEPCAD II – ISR2SeQuent PCB Paclitaxel - Coated Balloon
PES Paclitaxel - Eluting Stent
RIBS IV3SeQuent PCB Paclitaxel - Coated Balloon
EES Everolimus - Eluting Stent
• The Virtue® SEB has demonstrated:
A sirolimus elution and safety profile similar to metallic DES
A clinical SAFETY and EFFICACY despite a challenging DES-ISR population
• The SABRE Trial showed:
Angiographic Late Loss: ITT 0.31-mm and PP: 0.12-mm
Clinical Outcomes:
• ITT: 0.0% MACE in hospital and 14.3% TLF at 3 years
• PP: 0.0% MACE in hospital and 5.6% TLF at 3 years
• No TLR events (ITT) following 6 month angiographic assessment
• 1 MACE between year 1 and year 3 (unwitnessed death)
• An IDE study in coronary ISR (SABRE PP population) is under development
SABRE Feasibility Study Summary