interstitial lung diseases
66
INTERSTITIAL LUNG DISEASE DR BASITH
-
Upload
drbasith-lateef -
Category
Health & Medicine
-
view
531 -
download
1
Transcript of interstitial lung diseases

INTERSTITIAL LUNG DISEASE
DR BASITH

ILDs represent a large number of conditions that involve the parenchyma of the lung- the alveoli, the alveolar epithelium, the capillary endothelium, and the spaces between those structures as well as the perivascular and lymphatic tissues.
King TE (August 2005). "Clinical advances in the diagnosis and therapy of the interstitial lung diseases". Am. J. Respire. Crit. Care Med. 172 (3): 268–79.

Patients with interstitial lung diseases (ILDs) come to medical attention mainly because of
progressive excertional dyspnea or persistent nonproductive cough. Hemoptysis, wheezing, and chest pain .
Often, the identification of interstitial opacities on chest x-ray focuses the diagnostic approach on one of the ILDs.
* Harrisons principles of internal medicine 19th end

Interstitial lung disease in India was considered to be rare in the past but not now.
ILDs constitute about 10% to 15% of the patients with respiratory diseases.
About 50%of the ILDs are idiopathic in origin while others are associate with identifiable diseases, most commonly connective tissue disorders
UIP, also known as IPF is the most common form of ILD.
* API TEXTBOOK OF MEDICINE 10 EDN
EPIDEMIOLOGY

KNOWN CAUSE Fumes, gases Drugs (antibiotics, amiodarone, gold) and chemotherapy
drugs Asbestos Radiation Aspiration pneumonia Residual of acute respiratory distress syndrome Smoking-related
Desquamative interstitial pneumoniaRespiratory bronchiolitis–associated interstitial lung disease
Pulmonary Langerhans cell granulomatosis
*Harrisons principles of internal medicine 19th edn
MAJOR CATEGORIES OF ILDs (inflammation , alveoloitis, fibrosis)

Idiopathic interstitial pneumonias Idiopathic pulmonary fibrosis Acute interstitial pneumonia (diffuse alveolar
damage) Cryptogenic organizing Pneumonia Nonspecific interstitial Pneumonia Idiopathic lymphocytic interstitial pneumonia
UNKNOWN CAUSE

Pulmonary alveolar proteinosis Lymphocytic infiltrative disorders (lymphocytic
interstitial pneumonitis associated with connective tissue disease)
Eosinophilic pneumonias Lymphangioleiomyomatosis Inherited diseases
Tuberous sclerosis, neurofibromatosis, Niemann-Pick disease, Gaucher disease,
Hermansky pudlak syndrome

Idiopathic pleuro parenchymal fibroelastosis Acute fibrinous and organizing pneumonia Bronchiolo centric patterns of interstitial
pneumonia
RARE AND ILL-DEFINED ENTITIES

Systemic lupus erythematosus, Rheumatoid arthritis, Ankylosing spondylitis, Systemic sclerosis, Sjogren syndrome Polymyositis Dermatomyositis
CONNECTIVE TISSUE DISORDERS

Pulmonary hemorrhage syndromes Goodpasture syndrome, Idiopathic pulmonary hemosiderosis, Isolated pulmonary capillaritis
Amyloidosis
Gastrointestinal or liver diseases (Crohn disease, primary biliary cirrhosis, chronic active hepatitis, ulcerative colitis)
Graft-versus-host disease (bone marrow transplantation; solid organ transplantation)
OTHERS

KNOWN CAUSE Hypersensitivity pneumonitis (organic dusts) UNKOWN CAUSE Sarcoidosis Bronchocentric granulomatosis Granulomatous vasculitides Lymphomatoid granulomatosis Granulomatosis with polyangiitis (Wegener ) Eosinophilic granulomatosis with polyangiitis
(Churg Strauss)
LUNG RESPONSE (granulations)


1. Progressive dyspnea2. Restrictive physiology on pulmonary
function tests3. Diffuse reticular infiltrates or ground-
glass opacities on chest radiographs or thoracic CT imaging
studies*Harrisons principles of internal medicine 19th edn
Hallmarks of ILD

Symptoms◦ Dyspnea on exertion◦ Nonproductive cough◦ Constitutional symptoms - low-grade fever and malaise may
also be present at the onset of disease◦ Fatigue ,weight loss .
Physical exam ◦ Bibasilar inspiratory crackles ◦ Clubbing
Clubbing -indicates advanced fibrotic lung disease and is present in 25 – 50% patients at initial presentation
Not seen in drug induced induced ILD New onset of clubbing may indicate the concomitant
development of lung cancer◦ Cyanosis -severe hypoxemia
Clinical Features

A thorough medical history with a special focus on ◦ environmental and occupational history ◦ evaluation of all the patient’s current medications
and their duration of use◦ determining the tempo of progression of respiratory
symptoms◦ For example Acute -alveolar hemorrhage syndromes Chronic - Idiopathic Pulmonary Fibrosis
(IPF) or sarcoidosis
MEDICAL HISTORY

Peripheral blood eosinophilia ◦ eosinophilic lung disorder or drug-induced pulmonary
reaction Serological blood testing
◦ for specific connective tissue disorders ◦ anti-neutrophil cystoplasmic antibody (ANCA) Wegener granulomatosis microscopic polyangitis
◦ anti-glomerular basement membrane antibody Goodpasture syndrome
Laboratory Tests

The classic findings of ILD ◦ restrictive ventilatory pattern
a reduction in the FEV1 and FVC with a correspondingly normal or elevated FEV1/FVC ratio
total lung capacity (TLC) finding 80% of predicted values◦ decrease in the DLCO
Chest wall and neuromuscular disorders ◦ Associated with a reduced TLC but a normal DLCO
Arterial blood gases and specifically the PaO2 or SaO2 may be normal at rest in patients with ILD
In patients who have normal gas exchange at rest◦ cardiopulmonary exercise tests (CPET) unmasks the gas exchange
abnormalities
Respiration. 2004 May-Jun;71(3):209-13Pulmonary function testing in interstitial lung diseases.
.
Pulmonary Function Tests

One of the main features of ILD is an abnormal chest radiograph ◦ showing reticular, nodular, or reticulonodular
patterns◦ standard chest radiograph may appear normal in
up to 10% of patients with symptomatic ILD◦ High Resolution CT scan is the imaging modality of
choice in patients with suspected ILD
Radiological Studies

The geographic regional distribution and type of radiographic abnormalities yield useful clues for diagnosis of specific forms of ILD
Predominant abnormal radiographical involvement of the mid-upper lung zones◦ sarcoidosis, pulmonary Langerhans' cell histiocytosis, silicosis, and
hypersensitivity pneumonitis
Pleural-based reticular infiltrates in the lung bases◦ Idiopathic Pulmonary Fibrosis (IPF)
Intrathoracic lymphadenopathy ◦ sarcoidosis, lymphangitic spread of lung cancer, lymphocytic
interstitial pneumonia, berylliosis, and amyloidosis
Spontaneous pneumothorax associated with a cystic ILD ◦ Lymhangioleiomyomatosis (LAM) and Pulmonary Langerhans’ cell
histiocytosisHarrisons principles of internal medicine 19th ednRespiration. 2004 May-Jun;71(3):209-13.Pulmonary function testing in interstitial lung diseases
RADIOLOGICAL STUDIES

Bronchoalveolar lavage is useful -◦ Confirm diffuse alveolar hemorrhage syndromes ◦ eosinophilic pneumonia◦ excluding pulmonary infections associated with diffuse
infiltrates such as Pneumocystis jiroveci pneumonia
Bronchoscopy with transbronchial lung biopsy is useful- in selected patients suspected of having infections for granulomatous disorders such as sarcoidosis and
berylliosis lymphangitic spread of lung cancer
Transbronchial lung biopsy is not useful -◦ different types of idiopathic interstitial pneumonia
Fiberoptic bronchoscopy

The procedure of choice in establishing a diagnosis in patients with ILD secondary to suspected idiopathic interstitial pneumonia (IIP)
The location of the surgical lung biopsy is guided by the distribution of disease on HRCT images
Video-assisted thoracoscopic surgery (VATS) biopsy causes ◦ less morbidity than open thoracotomy ◦ better tolerated
In certain instances of idiopathic interstitial pneumonia suspected of being IPF-◦ a confident clinical diagnosis may be made without
subjecting the patient to surgical lung biopsy, when both clinical findings and the HRCT features are supportive
Surgical lung biopsy

MANAGEMENT(algorithm)

Objectives of management• Provide symptom relief• Slow down disease progression• Prevent complications• Improve quality of life• Prolong survival• Prevent treatment complications• End-of-life care – Palliation

Treatment of primary ILD
Anti-inflammatory drugs Corticosteroids Azathioprine Cyclophosphamide
Anti-fibrotic agents Colchicine Pirfenidone Pentoxyphylline D-Penicillamine TGF-beta antagonist Interferon-gamma
Anti-oxidant agents N-acetylcysteine Nitric oxide synthase
inhibitionSupportive and symptomatic treatments* Oxygen Pulmonary vasodilators Diuretics Antibiotics (if infection)
*Fishmans pulmonary diseases and disorders
Drugs used in the treatment

Idiopathic etiology for usual interstitial pneumonia (UIP)
Generally a chronic and relentlessly progressive disorder
Clinical Features Symptoms
◦ Breathlessness (>90% of patients)◦ Nonproductive Cough (>70%)
Physical Examination◦ Bibasilar Velcro-like Crackles ( >85%)◦ Clubbing (25%)
Respir Crit Care Med : Incidence and Prevalence of Idiopathic Pulmonary Fibrosis:
IDIOPATHIC PULMONARY FIBROSIS

Most common idiopathic interstitial pneumonia (IIP)
Affects at least 200,000 persons in the U.S.
Common age group = 50- 70 years
Median survival = 3 – 5 years from diagnosis
The exact cause = not known
◦ 0.5 - 3.7% of cases of IPF are familial ◦ 60% of patients have a positive history smoking. Harrisons principles of internal medicine 19th edn

1. Exclusion of other known causes of ILD (e.g., domestic and occupational environmental exposures, connective tissue disease, and drug toxicity).
2. The presence of a UIP pattern on HRCT in patients not subjected to surgical lung biopsy
3. Specific combinations of HRCT and surgical lung biopsy pattern in patients subjected to surgical lung biopsy
Am J Respir Crit Care Med Vol 183. pp 788–824, 2011
Diagnostic criteria

HRCT criteria for UIP pattern
1. Subpleural, basal predominance.
2. Reticular abnormality.
3. Honeycombing with or without traction bronchiectasis.
4. Absence of features listed as inconsistent with UIP pattern.

Evidence of marked fibrosis/ architectural distortion, +/- honeycombing in a predominantly subpleural/ paraseptal distribution
Presence of patchy involvement of lung parenchyma by fibrosis
Presence of fibroblast foci Absence of features against a diagnosis of
UIP suggesting an alternate diagnosis
Histopathological criteria for UIP pattern

Restrictive ventilatory limitation◦Normal or increased FEV1/FVC ratio ◦TLC that is < 80% of predicted or the lower limit of normal (LLN)
Single breath DLCO is reduced
Mild to moderate arterial hypoxemia or decreasing SaO2 during exertion
IPF - PFT


Should BAL cellular analysis be performed in the diagnostic evaluation of suspected IPF? NO
Should transbronchial lung biopsy be used in the evaluation of suspected IPF?
NO
Should serologic testing for connective tissues disease be used in the evaluation of suspected IPF?
YES
Should a multi-disciplinary discussion be used in the evaluation of suspected IPF?
YES

Co-existing emphysema Presence of pulmonary hypertension Physiological predictors
◦ Reduced FVC, TLC, and DLCO at the time of diagnosis
◦ Further declines in FVC and DLCO over the succeeding 6 – 12 months
◦ Significantly reduced distance during the six-minute walk test (6-MWT)
◦ Exertional hypoxia
Predictors of reduced survival in IPF
Ley B., Collard HR., King Jr TE. Clinical course and prediction of survival in idiopathic pulmonary fibrosis. Am. J. Respir. Crit. Care Med. 2010 Oct 8.

Coronary artery diseaseLung cancer InfectionPulmonary embolismAcute exacerbation of IPF
Causes of death in IPF

Characterized by ◦ worsening of dyspnea within a few weeks (< 1
month)◦ newly developing diffuse radiographic opacities◦ worsening hypoxemia◦ absence of infectious pneumonia, heart failure,
pulmonary thromoembolism, and sepsis
The rate of these acute exacerbations ranges from 10 to 15%
Acute exacerbation of IPF
Proceedings of the ATS, January 1, 2006; 3(4):330 - 338.

The risk factors for acute exacerbations of IPF are
Infections pulmonary embolism pneumothorax.
Histopathology -Diffuse alveolar damage(DAD) is often found on the
background of UIP
In patients who survive, a recurrence of acute exacerbation is common and usually results in death
Proceedings of the ATS, January 1, 2006; 3(4):330 - 338.

A chronic, progressive disorder
A death rate worse than that of many cancers◦ 3-year survival- 50%.
Lung transplant is the only therapy shown to prolong survival in advanced IPF
Treatment of IPF

Enroll in pulmonary rehabilitation
O2 supplementation at rest or during exercise & sleep
Symptomatic relief for cough with Antitussive agents.◦Thalidomide improves cough.◦GER therapy may be beneficial
Supportive Management IPF

The INPULSIS trials were two randomized, double-blind, placebo-controlled, phase 3 trials that were conducted simultaneously to evaluate the role of nintedanib, as compared with placebo, in patients with IPF◦ Nintedanib (formerly called BIBF-1120)
Antifibrotic properties that are mediated through the inhibition of tyrosine kinase receptors ◦ platelet-derived growth factor◦ fibroblast growth factor◦ Vascular endothelial growth factor
Treatment of IPFNintedanib
N Engl J Med 2014; 370:2142-2143

The ASCEND trial was the fourth in a series of randomized, double-blind, placebo-controlled, phase 3 trials that had been conducted in Japan and at multinational sites in which pirfenidone was compared with placebo in patients with IPF
The results of the first three trials were mixed, leading to approval by many governing bodies worldwide but not by the FDA
Although the precise actions are not clear◦ its primary antifibrotic mechanism is felt to be, at least
in part, mediated through its inhibition of the expression of transforming growth factor β1
Pirfenidone

For patients with ILD exhibiting progressive physiological deterioration who meet established criteria
Current criteria for referral of patients with IPF for single lung transplantation are◦ age < 70 years,◦ histological or radiographic evidence of UIP and any of the following: ◦ DLCO <39% predicted, ◦ 10% or greater decrement in the FVC during 6 months of
follow-up, ◦ a decrease in pulse oximetry to < 88% during a 6-minute
walk test, and◦ honeycombing on HRCT scan
Lung Transplantation

The usual age of onset – Around 50 years (lower than in IPF), Femlaes(who have never smoked)
Most common symptoms : breathlessness and cough
The majority of the patients have a restrictive ventilatory limitation
HRCT ◦ predominant involvement of lower lobes with volume
loss.◦ reticular pattern◦ ground glass appearance.
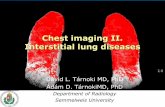
Nonspecific interstitial pneumonia(NSIP)

Histological characteristics ◦ temporal homogeneity and uniform thickening of
alveolar walls◦ with a spectrum of cellular to fibrosing patterns .
PROGNOSIS : Cellular NSIP which has excellent prognosis Fibrotic NSIP which has a less favorable
outcome. The response to steroids is good as opposed to
IPF The five-year survival is above 80%.
Harrisons principles of internal medicine 19th edn

CT image through lower lungs shows predominantly peribronchovascular ground-glass opacity with associated reticular pattern.
Radiology 2005; 236:10–21

The majority of patients with NSIP have a good prognosis (5-year mortality rate estimated at <15%)
With most showing improvement after treatment with glucocorticoids, often used in combination with azathioprine or mycophenolate mofetil.
* Harrisons principles of internal medicine 19th edn
TREATMENT

Acute abrupt onset Age >40 years Prodormal fever, cough, dyspnea preceeds AIP
High mortality rate (>60%)
Hypoxic respiratory failure like in ARDS (acute respiratory distress syndrome)
Histological features –◦diffuse alveolar damage include uniform
temporal appearance, airspace organization and hyaline membranes.
Case Reports in Medicine Volume 2011, Article ID 628743
Acute interstitial Pneumonia (AIP) or Hamman- Rich syndrome

Most patients have moderate to severe hypoxemia and develop respiratory failure.
Mechanical ventilation is often required. Recurrences have been reported The main treatment is supportive. It is not clear that glucocorticoid therapy is
effective.
TREATMENT

Rare disease Unknown eitiology Seen in 5th or 6th decade Presents with cough, fever and dyspnea,weight loss
may be mistaken for the community acquired pneumonia.
The histological features of organizing pneumonia (OP) includes patchy distribution of intraluminal organizing
fibrosis in distal airspaces preservation of the lung architecture uniform temporal appearance and mild chronic inflammation.
Thorax 2000;55:318-328 doi:10.1136/thorax.55.4.318
Cryptogenic organizing pneumonia (COP)

X RAY The radiological studies show consolidation
with the basal predominance.HRCT: Area of air space consolidation Ground glass opacities Broncial wall thickening and,dilation
Cryptogenic organizing pneumonia (COP)

Typical imaging pattern of organising pneumonia with patchy alveolar opacities on chest radiograph.
Copyright © BMJ Publishing Group Ltd & British Thoracic Society. All rights reserved.

Glucocorticoid therapy induces clinical recovery in two thirds of patients.
A few patients have rapidly progressive courses with fatal outcomes despite glucocorticoids
TREATMENT

1. Desquamative interstitial pneumonia2. Respiratory bronchiolitis associated ILD.3. Pulmonary Langerhans cell histiocytosis.
Thorax.bmj.com/ on September 20, 2015
ILD ASSOCIATED WITH SMOKING

Clinical manifestations DIP is Rare Exclusively seen in smokers peak in 4 th or 5 th decade Presents as cough and dyspnea
Histologic findings A diffuse and uniform accumulation of macrophages in the alveolar spaces is the hallmark of DIP.
Treatment: Clinical recognition of DIP is important because the process is associated with a better prognosis (10-year survival rate is ~70%) in response to smoking cessation.
There are no clear data showing that systemic glucocorticoids are effective in DIP.
Desquamative interstitial pneumonia (DIP)

Its considered to be a subset of DIP. The clinical presentation is similar to that of
DIP. Crackles are often heard on chest
examination and occur throughout inspiration sometimes they continue into expiration.
Respiratory bronchiolitis associated ILD

Histology : include alveolar macrophage accumulation
in respiratory bronchioles, with a variable chronic inflammatory cell infiltrate in bronchiolar and surrounding alveolar walls and occasional per bronchial alveolar septal fibrosis.
The pulmonary parenchyma may show presence of smoking-related emphysema.
Treatment RB-ILD appears to resolve in most patients after smoking cessation alone.
Thorax.bmj.com/ on September 20, 2015Harrisons priciples of inernal medicine 19th edn

It is a rare, smoking-related, diffuse lung disease that primarily affects Men between the ages of 20 and 40 years. Varies from an asymptomatic state to a
rapidly progressive condition Dyspnea, chest pain, weight loss, and fever. Pneumothorax occurs in ~25% of patients. Hemoptysis and diabetes insipidus are rare
manifestations.
Pulmonary langerhans cell histiocytosis

HRCT : A combination of nodules and thin-walled cysts is virtually diagnostic of PLCH.
The most common pulmonary function abnormality is a markedly reduced DLCO
Histopathology : presence of nodular sclerosing lesions that contain Langerhans cells accompanied by mixed cellular infiltrates
TREATMENT Discontinuance of smoking is the key
treatment(1/3 improve) Most patients with PLCH experience persistent
or progressive disease

INTERSTITIAL LUNG DISEASES IN CONNECTIVE TISSUE DISORDERS Clinical findings suggestive of a CTD
(musculoskeletal pain, weakness, fatigue, fever, joint pain or swelling, photosensitivity, Raynaud’s phenomenon, pleuritis, dry eyes, dry mouth) should be sought in any patient with ILD.
The most common form of pulmonary involvement is the nonspecific interstitial pneumonia
For the majority of CTDs, recommended initial treatment for ILD includes oral glucocorticoids often in association with
oral or intravenous cyclophosphamide or alazathioprine


Toxic fumes and vapours Oxygen Chlorine, fluorine and other gases Nitrogen dioxide LipidsDrugs Cytotoxics Nitrofurantoin Sulfasalazine, salicylates Gold Penicillamine AmiodaronePoisons Paraquat Toxic oil syndrome Radiation
* Fishmans pulmonary diseases and disorders
DRUG INDUCED ILDs

The drug may have been taken for several years before a reaction develops (eg: amiodarone)
The lung disease may occur weeks to years after the drug has been discontinued (e.g., carmustine).
Histology : The patterns of lung injury vary widely and depend on the agent.
Treatment : discontinuation of any possible offending drug and supportive care.

Clinical Manifestations cough fever, dyspnea. Severe respiratory distress requiring ventilatory
support.
Although hemoptysis is expected, it can be absent at the time of presentation.
An elevated white blood cell count and falling hematocrit are common.
Focal segmental necrotizing glomerulonephritis may be present
*Fishmans pulmonary diseases and disorders
SYNDROMES OF ILD WITH DIFFUSE ALVEOLAR HEMORRHAGE


Histology :Injury to arterioles, venules, and the alveolar
septal (alveolar wall or interstitial) capillaries secondary to disruption of the alveolar-capillary basement membrane.
This results in bleeding into the alveolar spaces.
Treatment IV methylprednisolone, 0.5–2 g daily in
divided doses for up to 5 days, followed by a gradual tapering, and then maintenance on an oral preparation.

2014-07-11 65
Inherited Disorders AD tuberous sclerosis indistinguishable from LAM
both radiographically & histopatho-logically
neurofibromatosis bilateral lower lobe fibrosis & bullae or cystic changes
AR Gaucher’s disease interstitial infiltration w/ fibrosis, alveolar consolidation, & filling of alveolar spaces
Niemann-Pick dis-ease
infiltration of the characteristic "foam cell" throughout the pulmonary lymphatics, the pulmonary arteries, & the pulmonary alveoli
Hermansky-Pudlak syndrome
Pulmonary fibrosis; onset in the 30th~ 40th slowly progressive



















