INTERPROFESSIONAL TRAUMA CONFERENCE · The authors, Maryse Dagenais & Michal Stachura, do not have...
41
INTERPROFESSIONAL TRAUMA CONFERENCE FAMILY-CENTRED CARE IN PEDIATRIC TRAUMA: A REVIEW OF THE BEST PRACTICES IN A PEDIATRIC INTENSIVE CARE UNIT Montréal, September 28, 2018
-
Upload
vuongquynh -
Category
Documents
-
view
214 -
download
0
Transcript of INTERPROFESSIONAL TRAUMA CONFERENCE · The authors, Maryse Dagenais & Michal Stachura, do not have...

INTERPROFESSIONAL TRAUMA CONFERENCE
FAMILY-CENTRED CARE IN PEDIATRIC TRAUMA:
A REVIEW OF THE BEST PRACTICES IN A PEDIATRIC INTENSIVE CARE UNIT
Montréal, September 28, 2018

PEDIATRIC INTENSIVE CARE
UNIT Maryse Dagenais RN, MSc(A), CNCCP(C) Interim Nurse Manager, PICU Clinical Nurse Specialist, PICU Contact: [email protected]
Michal Stachura RN, MSc(A) Nurse Clinician, PICU Interim Nurse-Consultant, Pediatric Infection Prevention & Control Contact: [email protected]
The authors, Maryse Dagenais & Michal Stachura, do not have any conflicts of interest to declare
POTENTIAL CONFLICT OF INTEREST DISCLOSURE

Injuries are the second most common cause of hospitalization in the pediatric population. They are the leading cause of death in children from 1 to 19 years of age. When the injured child is admitted to the pediatric intensive care unit (PICU), the interdisciplinary team focuses on providing care to restore the homeostasis of the patient, as the health outcomes of the child will be influenced by efficient, appropriate, and timely delivery of care. The family witnessing the level of activity surrounding the child may be overwhelmed. Family role disturbances and uncertainty may cause high level of stress and impair the family’s ability to communicate with the team and to become partners in care.
This presentation aims to review how family-centred care guidelines can be implemented in the pediatric intensive care environment. Examples will be used to illustrate how this approach can benefit patients, families, and healthcare providers.
Abstract
Introduction
Review of guidelines, by category:
1. Family presence
2. Support offered to family
3. Communication with family members
4. Use of specific professionals & consultants
5. Operational & environmental considerations
PRESENTATION OUTLINE

๏ PICU admission: major family event, massive disruption of roles & function of family system
๏ Parents of children hospitalized in a PICU at risk for: • anxiety • depression • post-traumatic stress disorder (PTSD)
๏ Working with family on coping skills builds resilience: helps family acquire tools to manage stressful situations in the future
(Slota, 2014)
INTRODUCTION

INTRODUCTION Our definitions:
๏ Family: the individuals who provide support and with whom the patient has a significant relationship
๏ Family-centred care: approach that is respectful and responsive to family’s needs and values

SIMULATION OF A TYPICAL
PICU TRAUMA
ADMISSION

Parental stressors: • trauma of actual or threatened death or serious injury
to child • lack of privacy • unfamiliar people, environment • logistics (lodging, transportation, etc.) • needs of other family members & own needs
(Slota, 2014)
INTRODUCTION

Parental response to stress: • reduced ability to use incoming information • decreased ability to think clearly and solve problems • reduced ability to master tasks • decreased sense of personal effectiveness • reduced ability to make constructive decisions • heightened/decreased sensitivity of self • decreased sensitivity to the environment & staff
(Slota, 2014)
INTRODUCTION

How do parents see their role in a PICU?
1. Being present and participating in the child's care;
2. Forming a partnership of trust with the PICU health care team; and
3. Being informed of the child's progress and treatment plan as the person who “knows” the child best.
(Ames et al, 2011)
INTRODUCTION

What is the role of the care team in a PICU?
1. Maintaining an environment that fosters patient’s and family’s psychosocial adaptation;
2. Addressing needs and anticipating needs; recognizing and addressing distress; and
3. Applying comforting skills, play therapies, and psychotherapeutic interventions.
(Carnevale & Dagenais, 2014)
INTRODUCTION
Why is family-centred care important in a PICU?
1. We expect families to make complex, difficult decisions
2. We anticipate that the families will provide post-ICU care
3. Family health is central to patient recovery
INTRODUCTION

INTRODUCTION
What evidence-based interventions assist clinicians in providing family-centred care in a PICU?
Presentation based on the following research findings:
• Davidson et al.’s 2017 Guidelines for Family-Centered Care in the Neonatal, Pediatric, and Adult ICU publication in Critical Care Medicine journal
• evidence-based support strategies
• analysis of over 200 studies yielding 23 recommendations
• recommendations based on moderate to very low quality of evidence, highlighting the “relative nascency of this field of research and the importance of future research to identify the most effective interventions to improve this important aspect of ICU care”
(Davidson et al., 2017)
INTRODUCTION

FAMILY PRESENCE

FAMILY PRESENCE What evidence-based interventions support family presence in an ICU?
(Davidson et al, 2017)
Recommendation Expected Outcome Evidence
1
Offer open or flexible family presence at the bedside that meets their needs while providing support for staff and positive reinforcement for staff to work in partnership with families
Improve family satisfaction 2D
i.e., weak recommendation, very low quality of
evidence
2 Offer the option of participating in interdisciplinary team rounds
Improve satisfaction with communication and increase family engagement
2C
3 Offer the option of being present during resuscitation efforts, with a staff member assigned Support the family 2C

FAMILY PRESENCE
How do we support family presence at the MCH PICU:
1. Culture change: family members are caregivers, not visitors
2. Unrestricted (24/7) presence of parents at bedside
3. Liberal (12 hours per day) presence of other family members on the unit
4. Clinical practice rooted in the McGill Model of Nursing: recognizing & seeking caregiver’s expertise and focus on family strengths
5. Encouragement to family to join in on care team rounds
6. Family presence for invasive procedures and resuscitative efforts, with appropriate accompaniment
7. Respect & accommodation for various family structures: offering family meetings on individual need basis
Teenager in a traumatic motor vehicle accident:
• Parent also injured, hospitalized in adult ICU.
• Extended family providing support and presence.
• Arranged for one member of our team to meet with the injured parent in ICU.
• Collaborated with ICU, Urgences-santé, and PICU to bring the injured parent in to visit injured child.
Trauma story: tragic motor vehicle accident
Teenager in a traumatic arm amputation on farming equipment:
• While child was in OR, PICU team was able to attend to anxious family by providing support and snacks
• Snack packs are a peer-to-peer initiative of a family who went through PICU hospitalization and decided to give back via the MCH Foundation
Trauma story: from farm to OR table

SUPPORT OFFERED TO FAMILY
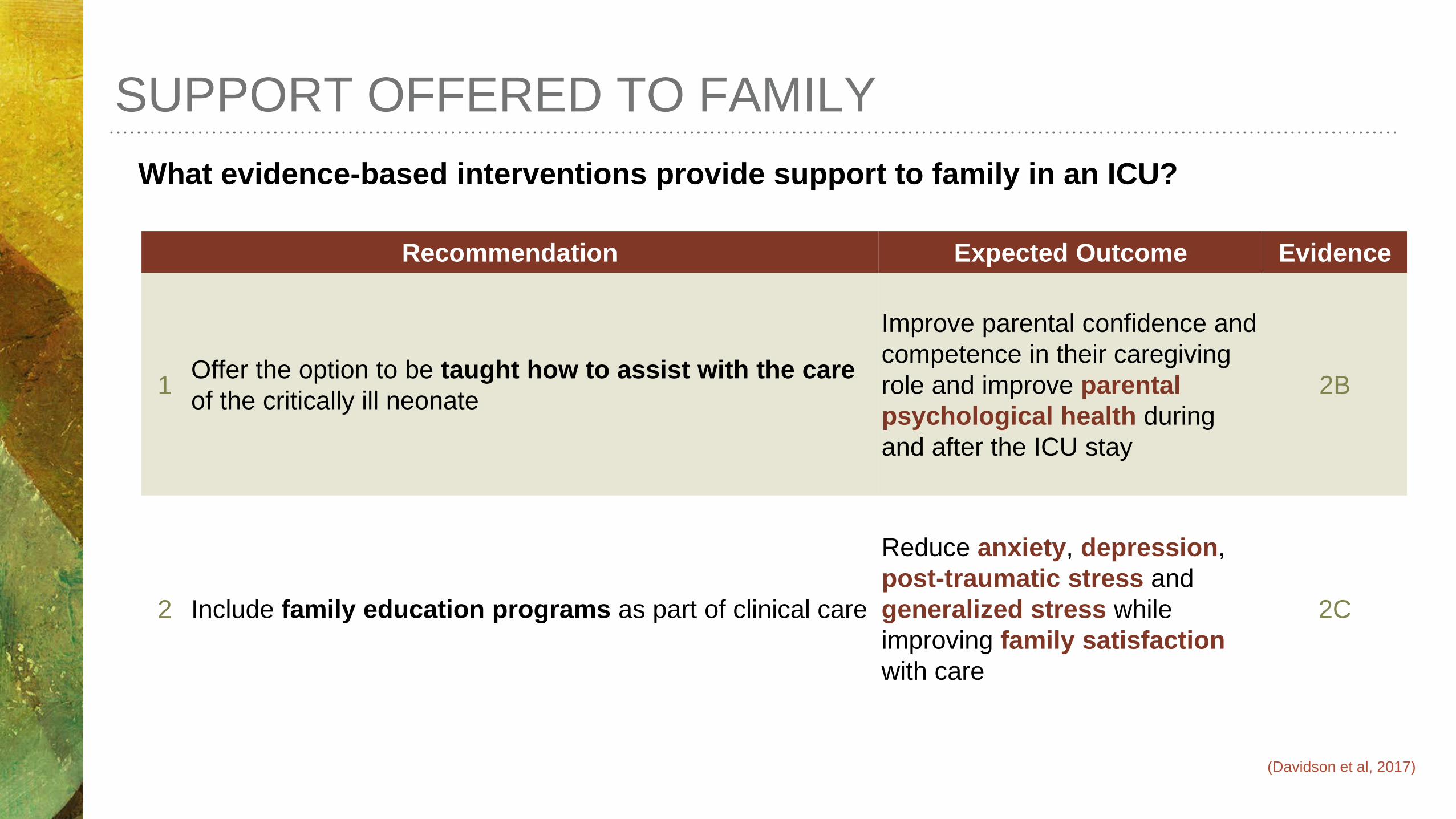
What evidence-based interventions provide support to family in an ICU?
Recommendation Expected Outcome Evidence
1 Offer the option to be taught how to assist with the care of the critically ill neonate
Improve parental confidence and competence in their caregiving role and improve parental psychological health during and after the ICU stay
2B
2 Include family education programs as part of clinical care
Reduce anxiety, depression, post-traumatic stress and generalized stress while improving family satisfaction with care
2C
SUPPORT OFFERED TO FAMILY
(Davidson et al, 2017)

What evidence-based interventions provide support to family in an ICU?
Recommendation Expected Outcome Evidence
3 Implement peer-to-peer support in NICUs Improve family satisfaction, reduce parental stress, and reduce depression
2D
4 Provide family with leaflets that give information about the ICU setting
Reduce family member anxiety and stress 2B
5 Implement ICU diaries Reduce family member anxiety, depression, and post-traumatic stress
2C
SUPPORT OFFERED TO FAMILY
(Davidson et al, 2017)

What evidence-based interventions provide support to family in an ICU?
Recommendation Expected Outcome Evidence
6 Implement validated decision support tools for family members (when relevant validated tools exist)
Optimize quality of communication, medical comprehension, and reduce family decisional conflict
2D
7
Among surrogates of ICU patients who are deemed by a clinician to have a poor prognosis, use a communication approach, such as the “VALUE” mnemonic (Value family statements, Acknowledge emotions, Listen, Understand the patient as a person, Elicit questions), during family conferences
Facilitate clinician-family communication 2C
SUPPORT OFFERED TO FAMILY
(Davidson et al, 2017)
SUPPORT OFFERED TO FAMILY
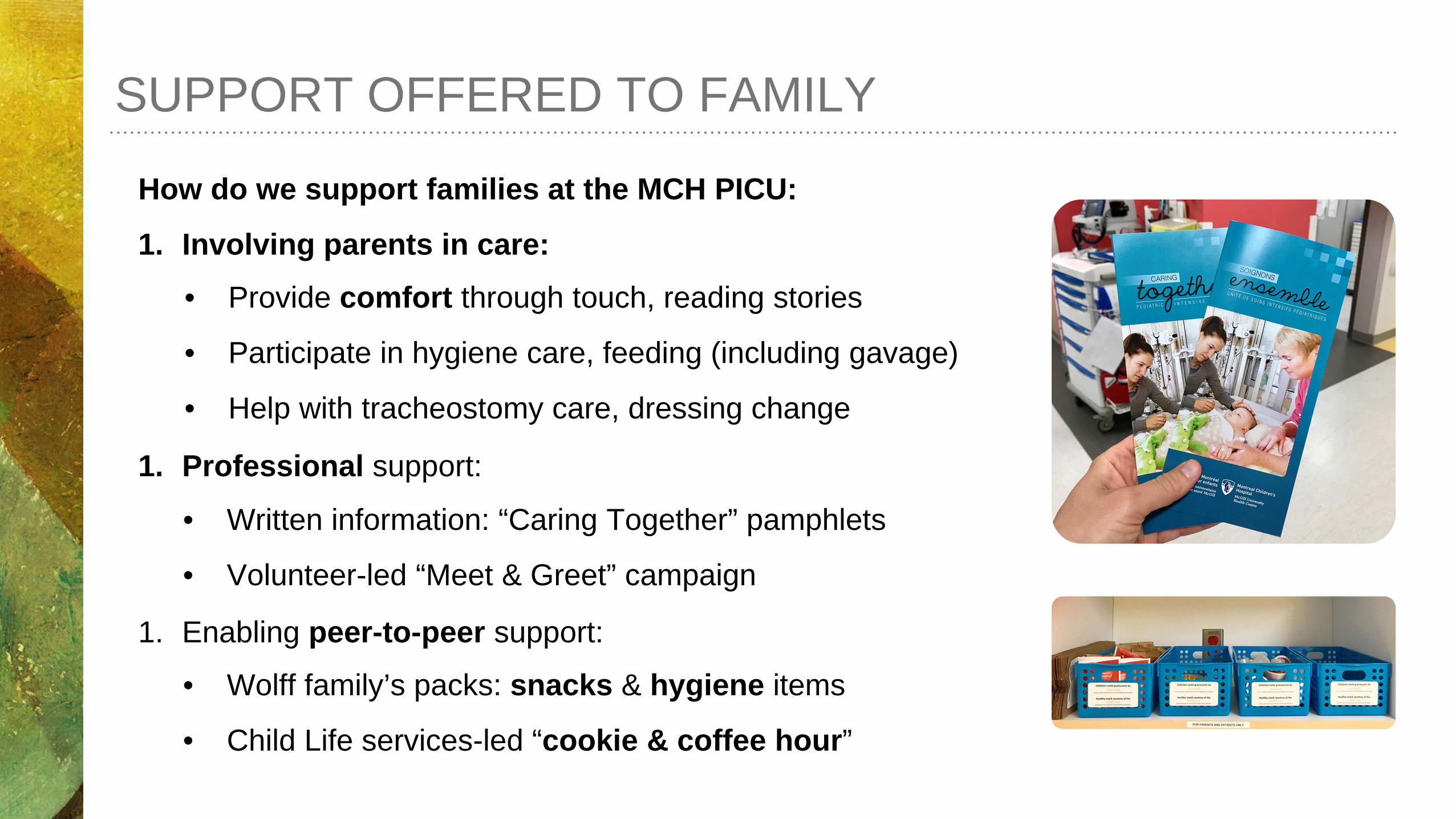
How do we support families at the MCH PICU:
1. Involving parents in care:
1. Professional support:
1. Enabling peer-to-peer support:
• Written information: “Caring Together” pamphlets
• Volunteer-led “Meet & Greet” campaign
• Wolff family’s packs: snacks & hygiene items
• Child Life services-led “cookie & coffee hour”
• Provide comfort through touch, reading stories
• Participate in hygiene care, feeding (including gavage)
• Help with tracheostomy care, dressing change

12-year-old suffering traumatic burns:
• Severe burns to hands, torso, neck, and face while playing with cousin
• Family from a small town more than 100 km away
• Parents are separated, but both present
• Family unable to witness any care initially
• With support, family transitioned from basic care to offering help with burn dressing change
Trauma story: burn victim

COMMUNICATION WITH FAMILY MEMBERS

What evidence-based interventions improve communication in an ICU?
COMMUNICATION WITH FAMILY MEMBERS
Recommendation Expected Outcome Evidence
1 Use interdisciplinary family conferences routinely
Improve family satisfaction with communication and trust in clinicians and to reduce conflict between clinicians and family members
2C
2
Use structured approaches to communication, such as that included in the “VALUE” mnemonic, when engaging in communication with family members, specifically including active listening, expressions of empathy, and making supportive statements around nonabandonment and decision making. In addition, we suggest that family members of critically ill patients who are dying be offered a written bereavement brochure
Reduce family anxiety, depression, and post-traumatic stress and improve family satisfaction with communication
2C
(Davidson et al, 2017)

What evidence-based interventions improve communication in an ICU?
COMMUNICATION WITH FAMILY MEMBERS
Recommendation Expected Outcome Evidence
3 ICU clinicians to receive family-centred communication training as one element of critical care training
Improve clinician self-efficacy and family satisfaction 2D
(Davidson et al, 2017)

COMMUNICATION WITH FAMILY MEMBERS
How and what do we communicate with families at the MCH PICU:
1. Parents participate in care team rounds
2. ”Glass Door” project
3. Weekly multidisciplinary & psychosocial rounds (improve internal communication)
4. Structured, weekly family meetings
5. Exit satisfaction survey
6. Bereavement support:
• Written information
• Memory box
• Legacy building activities
• Sibling & family support
Drowning & bereavement support:
• Child Life specialist worked with parents & siblings
• Family celebrated the child’s birthday in the PICU and brought her gifts: one of them was a red bicycle, which remained in the room until the patient’s death
• Although not the norm, we accommodated family members’ request to sleep next to their child
Trauma story: the red bicycle
USE OF SPECIFIC PROFESSIONALS &
CONSULTANTS

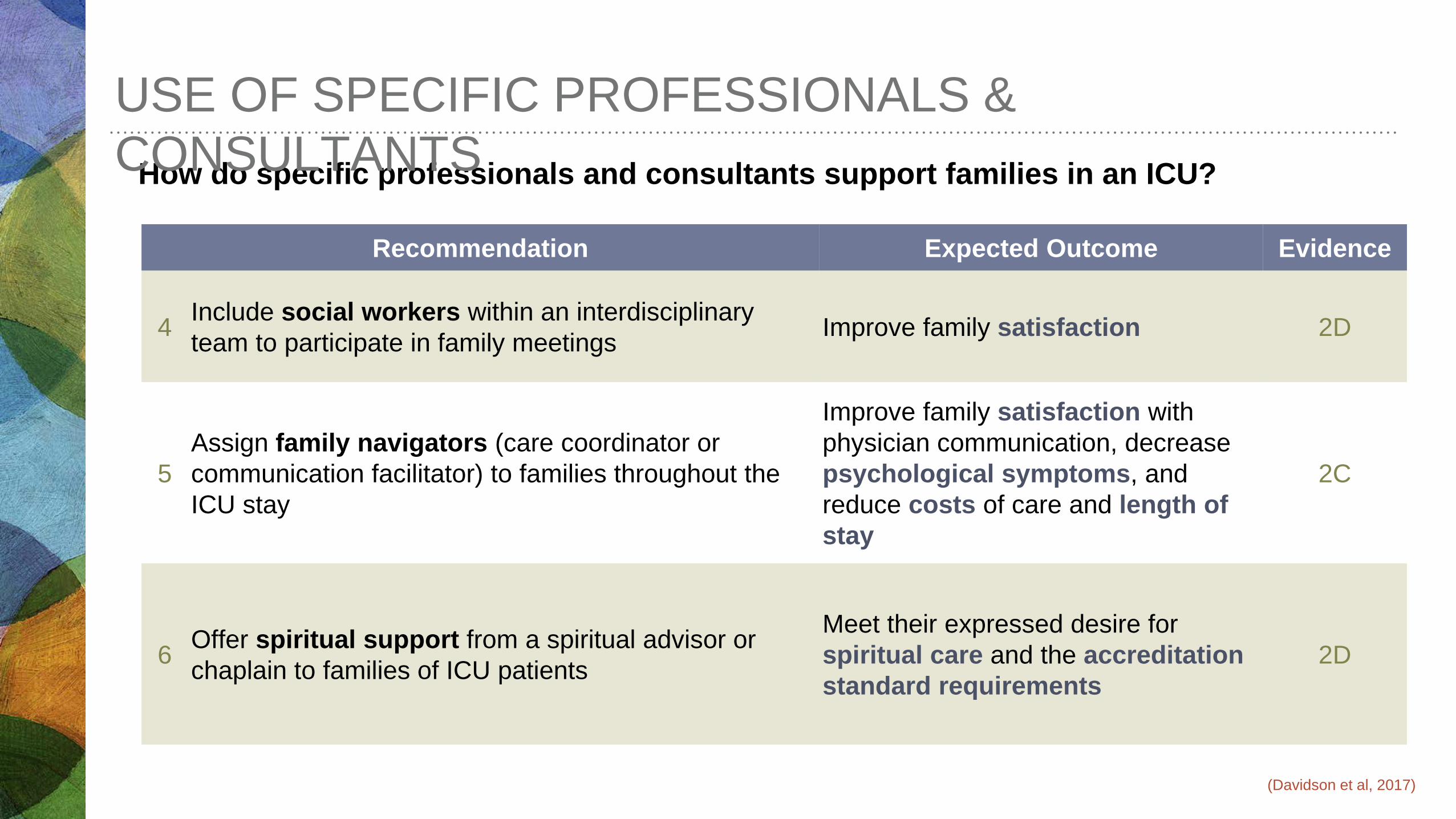
How do specific professionals and consultants support families in an ICU?
USE OF SPECIFIC PROFESSIONALS & CONSULTANTS
Recommendation Expected Outcome Evidence
1 Provide palliative care consultation proactively Decrease ICU and hospital length of stay (LOS) among selected critically ill patients
2C
2 Provide ethics consultation
Decrease ICU and hospital LOS among critically ill patients for whom there is a value-related conflict between clinicians and family
2C
3
Provide a psychologist’s intervention to incorporate a multimodal cognitive behavioural technique (CBT)-based approach; provide targeted video and reading materials
Through psychological support, improve outcomes in mothers of preterm babies admitted to the NICU
2D
(Davidson et al, 2017)
How do specific professionals and consultants support families in an ICU?
USE OF SPECIFIC PROFESSIONALS & CONSULTANTS
Recommendation Expected Outcome Evidence
4 Include social workers within an interdisciplinary team to participate in family meetings Improve family satisfaction 2D
5 Assign family navigators (care coordinator or communication facilitator) to families throughout the ICU stay
Improve family satisfaction with physician communication, decrease psychological symptoms, and reduce costs of care and length of stay
2C
6 Offer spiritual support from a spiritual advisor or chaplain to families of ICU patients
Meet their expressed desire for spiritual care and the accreditation standard requirements
2D
(Davidson et al, 2017)

USE OF SPECIFIC PROFESSIONALS & CONSULTANTS
Specialized consultation teams and professionals at the MCH PICU:
1. Trauma Team’s presence along the continuum of care (coordination of care)
2. Early involvement of Pediatric Advanced Care Team (PACT)
3. Social worker / Northern module coordinator as integral part of care team
4. Spiritual Care specialist
5. Child Life specialist and school services: for injured children and their siblings
6. Music therapy: role in traumatic brain injury
7. Therapeutic clowns
8. Daycare services for siblings of hospitalized children
OPERATIONAL & ENVIRONMENTAL
CONSIDERATIONS
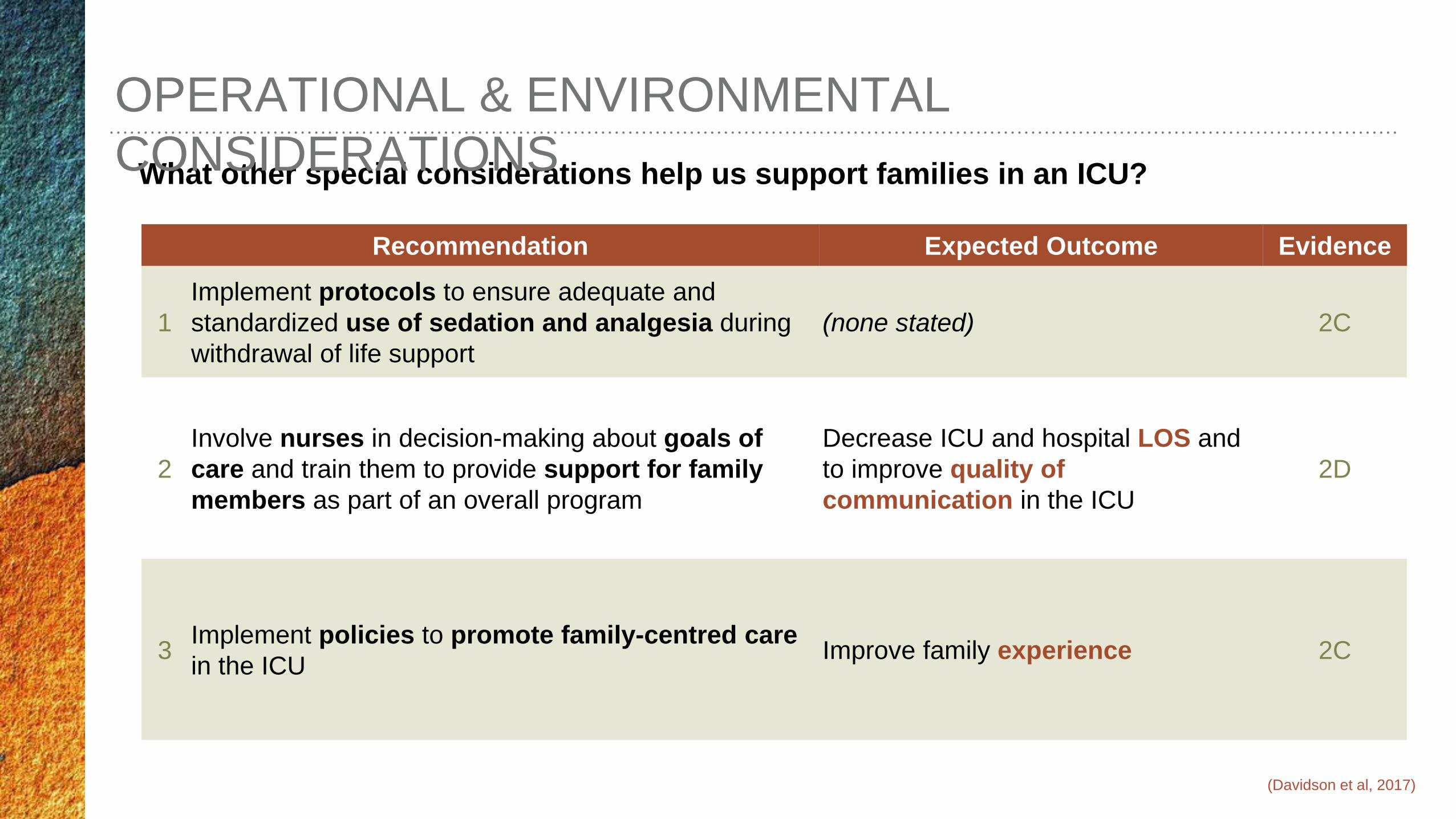
What other special considerations help us support families in an ICU?
OPERATIONAL & ENVIRONMENTAL CONSIDERATIONS
Recommendation Expected Outcome Evidence
1 Implement protocols to ensure adequate and standardized use of sedation and analgesia during withdrawal of life support
(none stated) 2C
2 Involve nurses in decision-making about goals of care and train them to provide support for family members as part of an overall program
Decrease ICU and hospital LOS and to improve quality of communication in the ICU
2D
3 Implement policies to promote family-centred care in the ICU Improve family experience 2C
(Davidson et al, 2017)
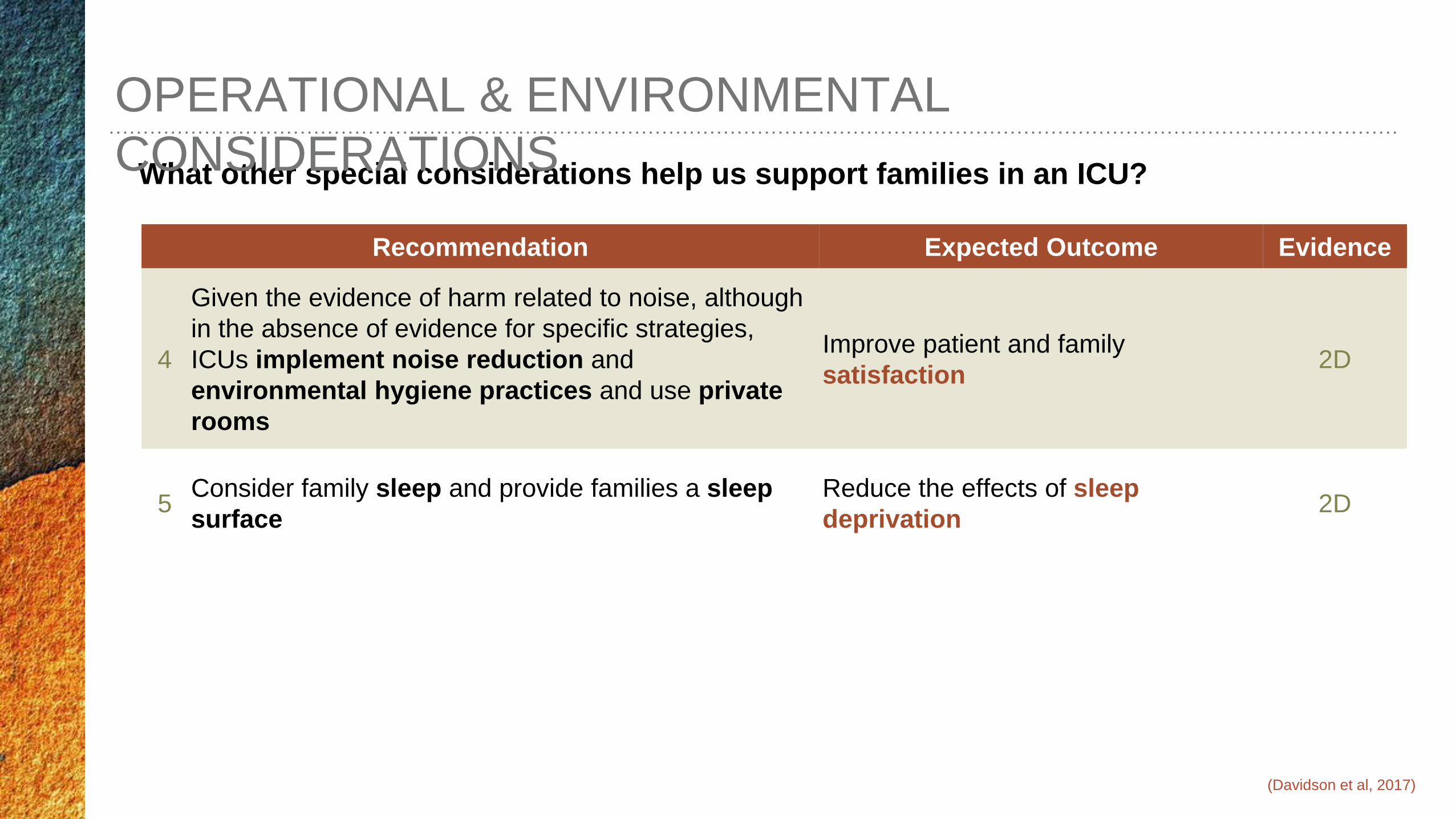
What other special considerations help us support families in an ICU?
OPERATIONAL & ENVIRONMENTAL CONSIDERATIONS
Recommendation Expected Outcome Evidence
4
Given the evidence of harm related to noise, although in the absence of evidence for specific strategies, ICUs implement noise reduction and environmental hygiene practices and use private rooms
Improve patient and family satisfaction 2D
5 Consider family sleep and provide families a sleep surface
Reduce the effects of sleep deprivation 2D
(Davidson et al, 2017)

OPERATIONAL & ENVIRONMENTAL CONSIDERATIONS Family focus at the MCH PICU:
1. All projects to improve family and patient experience have a family representative:
2. Family presence policy
3. Private (individual) patient rooms
4. PICU “quiet time” project
5. Parent sleep rooms & sleep accommodations in patient rooms
• Family Care Committee
• Pain, Agitation, Delirium, and Withdrawal (PADW) project

Ames, K.E., Rennick, J.E., & Baillargeon, S. (2011). A qualitative interpretive study exploring parents' perception of the parental role in the paediatric intensive care unit. Intensive and Critical Care Nursing, 27(3), 143-150.
Carnevale, F. A. & Dagenais, M. (2014). Nursing Care in the Pediatric Intensive Care Unit. In D. S. Wheeler, H. R. Wong, T. P. Shanle (Eds.), Pediatric Critical Care Medicine: Care of the critically ill or injured child (41-46). London, UK: Springer-Verlag.
Davidson, J.E., Aslakson, R.A., Long, A.C., Puntillo, K.A., Kross, E.K., Hart, J., Cox, C.E., Wunsch, H., Wickline, M.A., Nunnally, M.E., Netzer, G., Kentish-Barnes, N., Sprung, C.L., Hartog, C.S., Coombs, M., Gerritsen, R.T., Hopkins, R.O., Franck, L.S., Skrobik, Y., Kon, A.A., Scruth, E.A., Harvey, M.A., Lewis-Newby, M., White, D.B., Swoboda, S.M., Cooke, C.R., Levy, M.M., Azoulay, & E., Curtis, J.R. (2017) Guidelines for Family-Centered Care in the Neonatal, Pediatric, and Adult ICU. Critical Care Medicine, 45(1), 103-128.
Slota, M.C. (2014). Psychosocial aspects of pediatric critical care. In M.F. Hazinski (Ed.), Nursing care of the critically ill child (3rd ed., 79-158). St. Louis: Elsevier Mosby.
REFERENCES

QUESTION PERIOD
We invite you to ask your questions in English et en français