Interpretation of SD-OCT Gella Laxmi 2009PHXF013P.
20
Interpretation of SD- OCT Gella Laxmi 2009PHXF013P
-
Upload
vernon-palmer -
Category
Documents
-
view
221 -
download
3
Transcript of Interpretation of SD-OCT Gella Laxmi 2009PHXF013P.

Interpretation of SD-OCT
Gella Laxmi
2009PHXF013P

How to go about….
• Interpretation should proceed sequentially from vitreous towards choroid
• Evaluate each layers
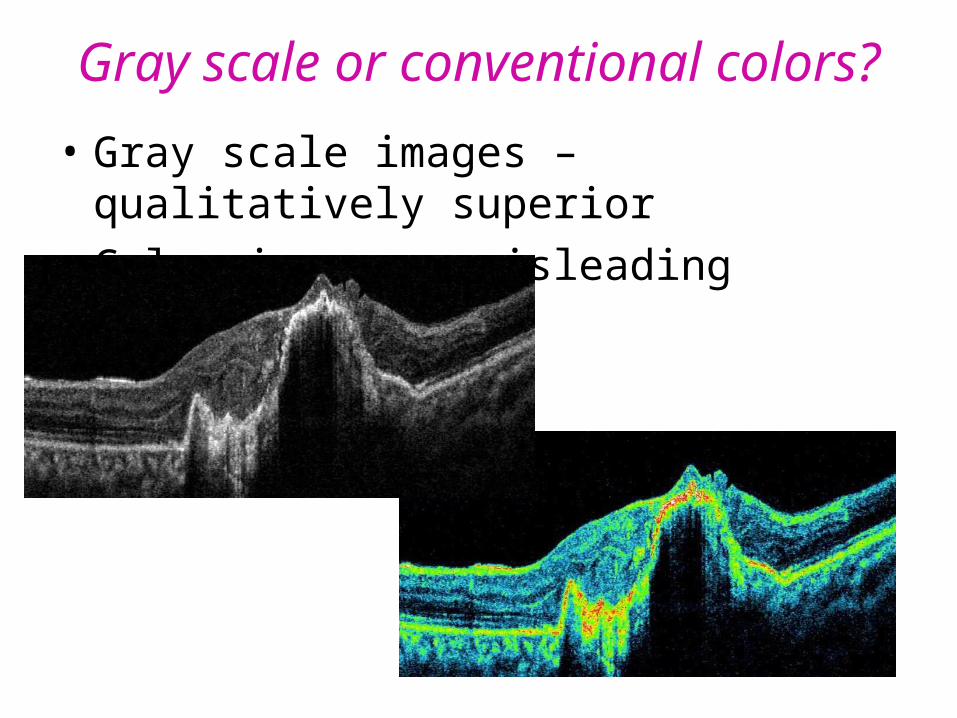
Gray scale or conventional colors?
• Gray scale images – qualitatively superior
• Color images – misleading

ReflectivityHyper reflective Lesions (Red ) Hypo reflective Lesions (Black) (Fluid)
ME
PED
SRF
FovealschisisERM
CNVM
DRUSEN
HE

ThicknessIncreased
(edema, CNVM) Decreased

Morphology
“Missing" retina "Extra" retinal tissue

Before advising OCT ......
Answer 2 questions...
“Why OCT in this case?” “What to look for in OCT?”

Diabetic Macular Edema
• Classify (FFA better)
• To R/O Foveolar detachment
• To R/O VMT ( Difficult clinically)
• Post treatment follow up
• Swelling – Focal /Diffuse / Cystoid
• Hard exudates
• Foveolar detachment
• Status of posterior hyaloid
• CWS, Hemorrhage
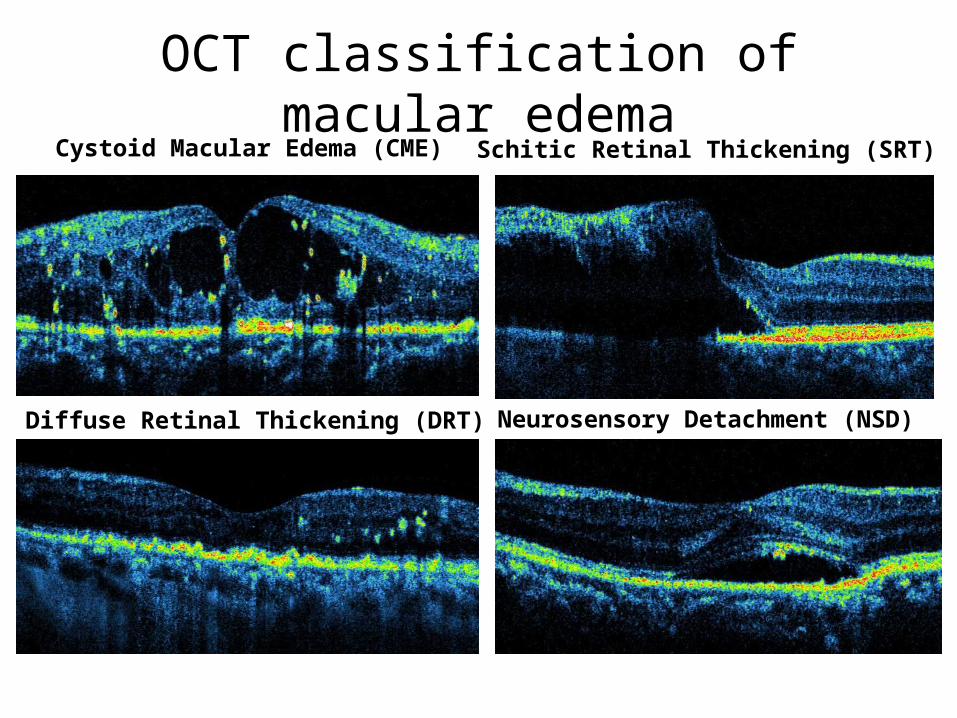
OCT classification of macular edema
Diffuse Retinal Thickening (DRT)
Cystoid Macular Edema (CME)
Neurosensory Detachment (NSD)
Schitic Retinal Thickening (SRT)
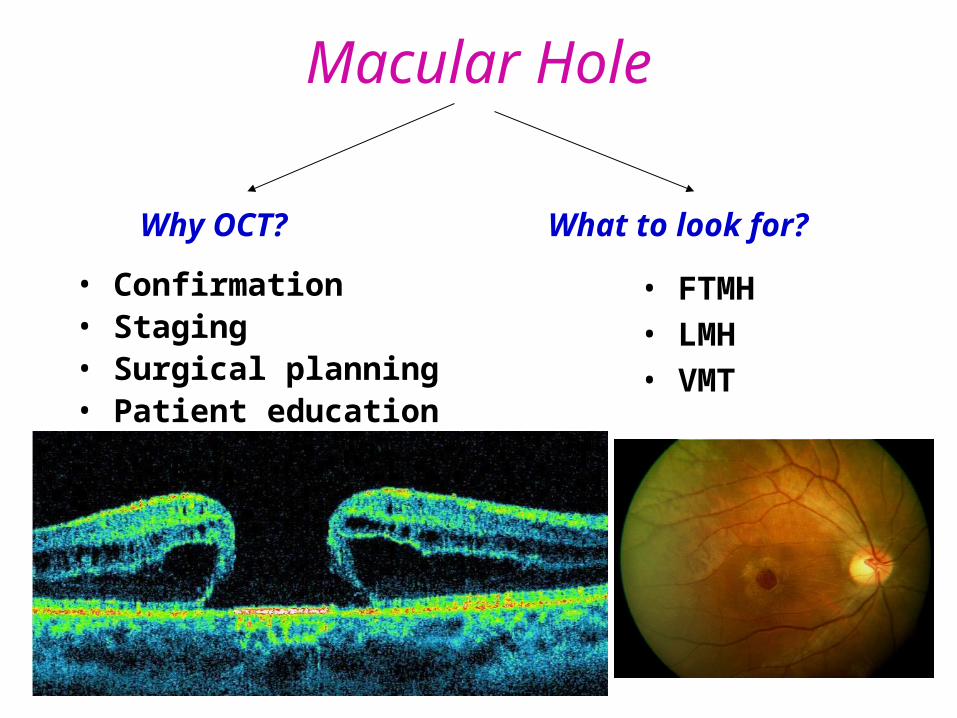
Macular Hole
• Confirmation• Staging• Surgical planning• Patient education
• FTMH • LMH• VMT
What to look for? Why OCT?

OCT Staging of macular hole
Stage 1B(Full thickness pseudocyst)
Stage 2 (Partial opening of pseudooperculum focal Vitreous attachment )
Stage 3(Operculated FTMH Vitreous traction released)
Stage 4(With complete PVD)
Post surgery
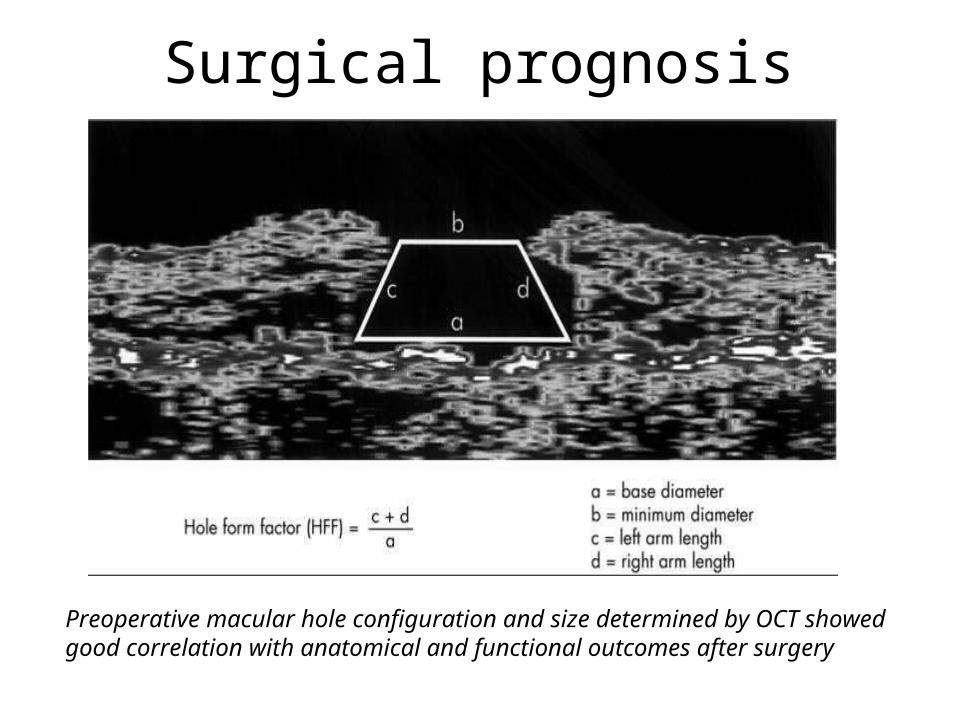
Surgical prognosis
Preoperative macular hole configuration and size determined by OCT showed good correlation with anatomical and functional outcomes after surgery

• HFF > 0.9 - 100 % PRIMARY CLOSURE
HFF = 0.5 - 67 % PRIMARY CLOSURE
HFF < 0.5 - Poor closure rates

ARMD
• Diagnosis - Dry or Wet• Response to treatment
Drusens
• Lipofusin deposits
• Bumpy RPE
• High reflective
• Normal inner retinal layers
• No shadowing

Types of PEDFibrovascular
SerousHemorrhagic
Drusanoid

Types of CNVM• Occult • Classic
Intraretinal fluid is associated with the presence of neovascular membrane
• Disruption of RPE band• Irregular thickening below RPE• CNVM not adequately visualized • Optical shadowing by detached RPE
• Continuous RPE band• Well defined , Hyperreflective fusiform thickening above RPE• Marked , posterior shadowing

Central Serous Retinopathy
• RPE defect
• SRF
• Cystoid spaces
• Foveal atrophy/thinning
• Subretinal fibrin
• CNVM
• Compare the reflectivity with
vitreous
• Granular outer segment in
chronic cases

Parafoveal Telangiectasia
• Cystic spaces• Minimum/ moderate thickening• Defect at the level of photoreceptor layer• Intraretinal high reflective areas causing
shadow (migrated pigments)
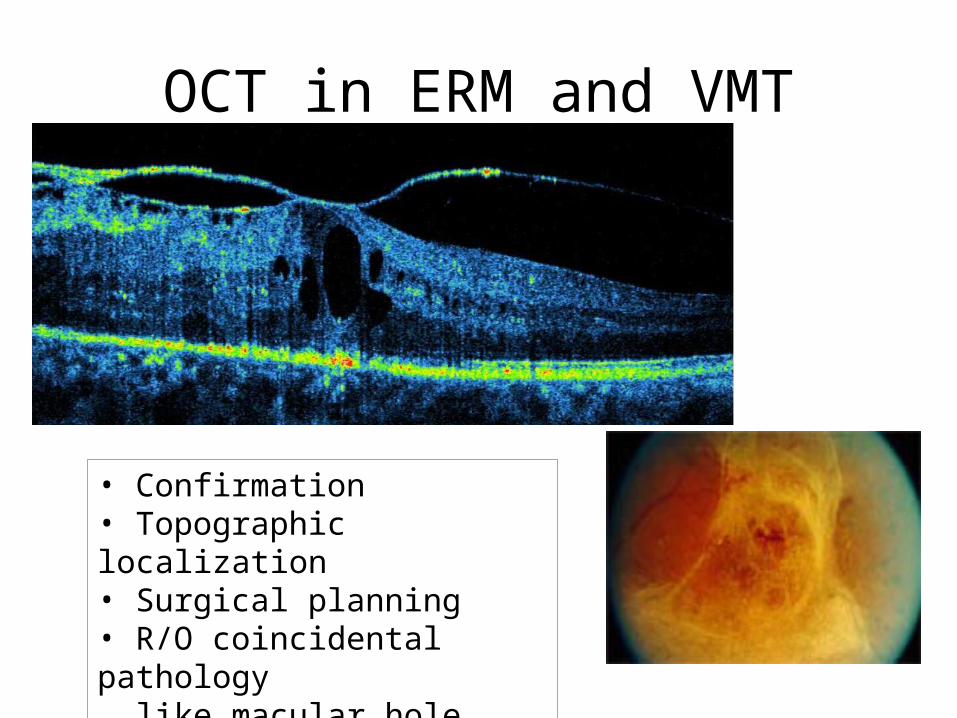
OCT in ERM and VMT
• Confirmation• Topographic localization• Surgical planning • R/O coincidental pathology like macular hole /pseudohole

References
• M Brar, D-U G Bartsch. Colour versus grey-scale display of images on high-resolution spectral OCT. Br J Ophthalmol. 2009; 93: 597-602.
• Brian Y. Kim, Scott D. Smith, et al. Optical Coherence Tomographic patterns of Diabetic Macular Edema. Am J Ophthalmol. 2006; 142;405-412.
• S Ullrich, C Haritoglou, C Gass, M Schaumberger, M W Ulbig. Macular hole size as a prognostic factor in macular hole surgery. Br J Ophthalmol. 2002 April; 86(4): 390–393.
• Kusuhara S, Teraoka Escano MF, Fujii S et al. Prediction of postoperative visual outcome based on hole configuration by optical coherence tomography in eyes with idiopathic macular holes. Am J Ophthalmol 2004; 138: 709–16.
• Lisandro M Sakata, Julio DeLeon-Ortega et al. Optical coherence tomography of the retina and optic nerve – a review. Clinical and Experimental Ophthalmology 2009; 37: 90–99.