
Interpersonal Psychotherapy and Antidepressants in Major Depression in Type 2 Diabetes Patients...
39
Interpersonal Psychotherapy and Interpersonal Psychotherapy and Antidepressants in Major Antidepressants in Major Depression in Type 2 Diabetes Depression in Type 2 Diabetes Patients Patients International Society for Interpersonal Psychotherapy 4th International Conference Amsterdam,2011 Gois C*, Duarte R**, Carmo I***, Barbosa A* Gois C*, Duarte R**, Carmo I***, Barbosa A* *Psychiatry Department, Hospital de Santa Maria, Lisbon *Psychiatry Department, Hospital de Santa Maria, Lisbon **Portuguese Diabetes Association, Lisbon **Portuguese Diabetes Association, Lisbon ***Endocrinology, Diabetes and Metabolism Department, ***Endocrinology, Diabetes and Metabolism Department, Hospital de Santa Maria, Lisbon Hospital de Santa Maria, Lisbon
-
Upload
john-lewis -
Category
Documents
-
view
219 -
download
2
Transcript of Interpersonal Psychotherapy and Antidepressants in Major Depression in Type 2 Diabetes Patients...
Interpersonal Psychotherapy and Interpersonal Psychotherapy and Antidepressants in Major Depression Antidepressants in Major Depression
in Type 2 Diabetes Patientsin Type 2 Diabetes Patients
International Society for Interpersonal Psychotherapy
4th International ConferenceAmsterdam,2011
Gois C*, Duarte R**, Carmo I***, Barbosa A*Gois C*, Duarte R**, Carmo I***, Barbosa A*
*Psychiatry Department, Hospital de Santa Maria, Lisbon*Psychiatry Department, Hospital de Santa Maria, Lisbon
**Portuguese Diabetes Association, Lisbon**Portuguese Diabetes Association, Lisbon
***Endocrinology, Diabetes and Metabolism Department, ***Endocrinology, Diabetes and Metabolism Department, Hospital de Santa Maria, LisbonHospital de Santa Maria, Lisbon
Background
Type 2 diabetes (90%)
adult metabolic disease
lack or dysfunctional insulin (resistance)
life style association (obesity)
treatment: oral hypoglycemic/insulin,
diet, exercise, self management
Type 1 diabetes
young metabolic disease
lack of insulin (B cell pancreatic autoimune failure)
treatment: insulin, diet, exercise, self management
Type 2 Diabetes Mellitus: prevalence 12,9% Cowie et al, 2009

Background
Depression and Diabetes MellitusTwo pandemic morbidities
WHO predictions
2020 depression from 4th to 2nd main cause of disability
2030 diabetes doubles to 366 millions persons worldwide

Depression prevalence in chronic somatic diseases
Somatic Somatic DiseaseDisease
Major Major DepressionDepression
CancerCancer 1,5 – 50%1,5 – 50%
Post strokePost stroke 9 – 31%9 – 31%
ParkinsonParkinson 20 – 30%20 – 30%
Multiple sclerosisMultiple sclerosis 16 – 30%16 – 30%
Coronary DiseaseCoronary Disease 15 – 23%15 – 23%
Diabetes Diabetes MellitusMellitus
11 – 15%11 – 15%
HIVHIV 4 – 23%4 – 23%Raison et al, 2005
Background

Ramalheira, 1996; DSM IV-TR, 2000; Anderson, 2001; Jacobson, 2002; Nichols, 2003; Gusmão, 2005
GeneralGeneralPopulatioPopulatio
nn
Type 1 Type 1 Diabetes Diabetes
Type 2Type 2Diabetes Diabetes
MajorMajorDepressioDepressio
nn
3 – 9%3 – 9% 13 - 29%13 - 29% 11 - 33%11 - 33%
Prevalence
Background
2 – 3 times more Depression with Diabetes

Background
Depression Diabetes
Behavioral: ↓ self-care
Biologic: hormonal, glucose disfunction, neuroinflammation
may affect

Major Depression in DiabetesMajor Depression in Diabetes
↓↓ HHealthier behaviors: treatment adherence, smoking ealthier behaviors: treatment adherence, smoking
↑ ↑ Wasting with health, Wasting with health, ↑↑ Inpatient Inpatient admittancesadmittances
↑↑ Morbidity - chronic complications (severity and Morbidity - chronic complications (severity and
number)number)
↑↑ Mortality - Cardio Vascular DiseasesMortality - Cardio Vascular Diseases
DM + DEP = 2,4 DM + DEP = 2,4 x x Only DEP = 1,3 Only DEP = 1,3 x x Only DM = 2,3 xOnly DM = 2,3 x
Egede et al, 2005
Background

Comorbity depression and diabetes: worse decrements in health
Moussavi et al, 2007
Background
Explains 3% of HbA1c variance (more in type 1 diabetes) Explains 3% of HbA1c variance (more in type 1 diabetes) Depression treatment: Depression treatment: ↑↑41 to 58% persons with a good 41 to 58% persons with a good
controlcontrol
< 1% redution in HbA1c < 1% redution in HbA1c →→ 33% decrease of retinophaty 33% decrease of retinophaty (DCCT)(DCCT)
Lustman et al, 2000
Background
Depression and metabolic control in diabetes

Hamem, 2005; Kendler, 1999;Ludman et al, 2004
Background
2 – 3 times more Depression with Diabetes,
WHY?
illness intrusivenness
inflamation↑cortisol
attachmentsocial support

Background
Type 2 Diabetes
Attachment
Dismissing attachment ↓ Self-care
Ciechanowski et al, 2004
↓ depressive symptoms Others more reliable (↓ avoidance)Self more worthy of attention (↓ anxiety)
Ciechanowski et al, 2005

Background
Major Depression
Attachment
Murphy & Bates, 1996
Negative view of self independently of view of other
Self-criticism
Anxiety/preoccupation and fearfull attachment
Positive association with depression
Dismissing attachment
Secure attachment
No association with depression
Negative association with depression

Depression treatment (≈ non diabetes)
11 RCTs, Petrak & Herpetz, 2009
Type 1 & 2 diabetes Depression Metabolic control
Psychological (3, n=140)
yes yes (except 1)
Pharmacological (4, n=289)
yes (except 1) no
Mixed (4, n=954) Yes (except 1) no (excepto 1)
11 RCTs e 3 Collaborative care, Katon & van der Feltz-Cornelis, 2010
Type 1 & 2 diabetes Depression (ef size)
Metabolic control (ef size)
Psychological (5, n=310)
moderate-large moderate-large
Pharmacological (6, n=215)
moderate small
Collaborative care (3) moderate-large no effect

Cognitive – behavior therapy vs control
Solution focused therapy vs usual
DM2, ↓ dep, ↓ HbA1c follow-up
DM2, ↓ dep, HbA1c ns
Background
Psychotherapy for Major Depression in Type 2 Diabetes
Citalopram vs Interpersonal Psychotherapy T vs usual
Katon et al, 2004; Bogner et al, 2007;Lustman et al,1998
Age 60 – 80 yrs, follow-up 5 yrs, ↓ mortality

Lustman et al, 1997,2000,2006,2007; Paile-Hyvarinen et al, 2003; Amsterdam et al, 2006;Goodnick et al, 1997
Acute Dep
Recor Dep
Dep HbA1c
nortriptiline yes no ↓ ↑
fluoxetine yes no ↓ ns; ↓
paroxetine yes no ↓ ns
escitalopram
yes no ↓ ns
sertraline yes yes ↓ ↓
bupropion yes yes ↓ ↓
Antidepressants for Major Depression in Type 2 Diabetes
Background

Background
IPT Theory: attachment communication theory social theory
IPT ObjectivesIPT Objectives:
↑ relationships
IP Communication
Problem solutions
Acute Major
DepressionAdapt Stuart S, 2008

Acute Depression and Interpersonal Psychotherapy
1st RCT: IPT+Amitriptiline > IPT = Amitriptiline Weissman et al, 1979
RCT: NIMH – TDCRP (Efficacy Evidence) IPT=CBT=Imipramine Elkin et al,1989
13 RCTs: Meta analisys Remission: IPT=Antidepressant=IPT+AntidepressantSymptom reduction: IPT > CBT
de Mello et al, 2005
Decrease in Symptoms, IP Problems and Attachment(anxiety and avoidance): IPT = IPT + Antidepressants
Outcome: symptoms
Outcome: symptoms + attachment + IP problems
Ravitz et al, 2008

Acute Depression in Somatic Patients and Interpersonal Psychotherapy
Outcome: symptoms
RCT: HIV patients IPT = Imipramine > CBT Markowitz et al, 1998
RCT: Coronary Artery PatientsCitalopram > IPT = Clinical Management
Lespérance F et al, 2007

Questions
1st outcome eficiency of treatment of major
depression
in type 2 diabetes patients with
IPT or sertraline or combo
and detect diferences between /within them
2nd outcomes detecting changes in attachment,
diabetes adaptation, diabetes self
efficacy and metabolic control after
treatment by the three treatment groups
and differences between them
Exclusion Criteria
<18>65 years
acute suicidality
antidepressant therapy
other somatic chronic condition
other mental disorder
alcohol or others drugs abuse/dependence
illiteracy, visual handicap

T2Diab
RandomiZaTion
1,5 month 3 month 4 month 5 month 6 month0 month
HADSMADRSMINIInterviiew
MADRSAttachmentDiabetes adjustmentDiabetesSelf EfficacyHbA1c
IPT
USUAL
MADRS MADRS MADRS
MDECOMBO
MADRSAttachmentDiabetes adjustmentDiabetesSelf EfficacyHbA1c
MADRSAttachmentDiabetes adjustmentDiabetesSelf Efficacy
Clinical - Experimental Study
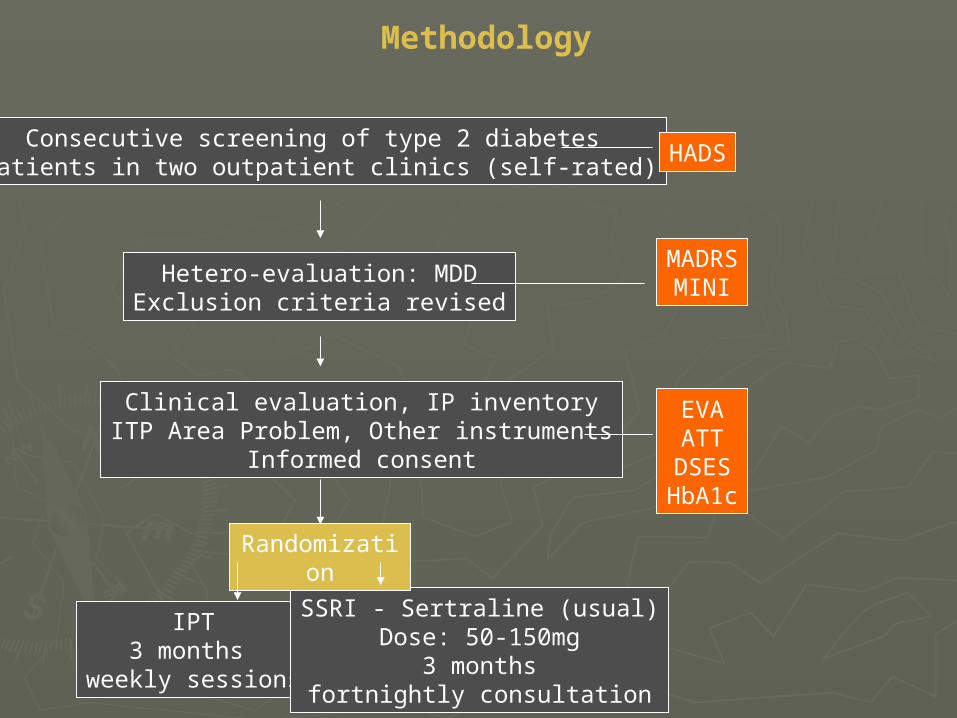
Methodology
Consecutive screening of type 2 diabetes patients in two outpatient clinics (self-rated) HADS
Hetero-evaluation: MDDExclusion criteria revised
MADRSMINI
Clinical evaluation, IP inventoryITP Area Problem, Other instruments
Informed consent
EVAATT
DSESHbA1c
IPT3 months
weekly sessions
SSRI - Sertraline (usual)Dose: 50-150mg
3 monthsfortnightly consultation
Randomization
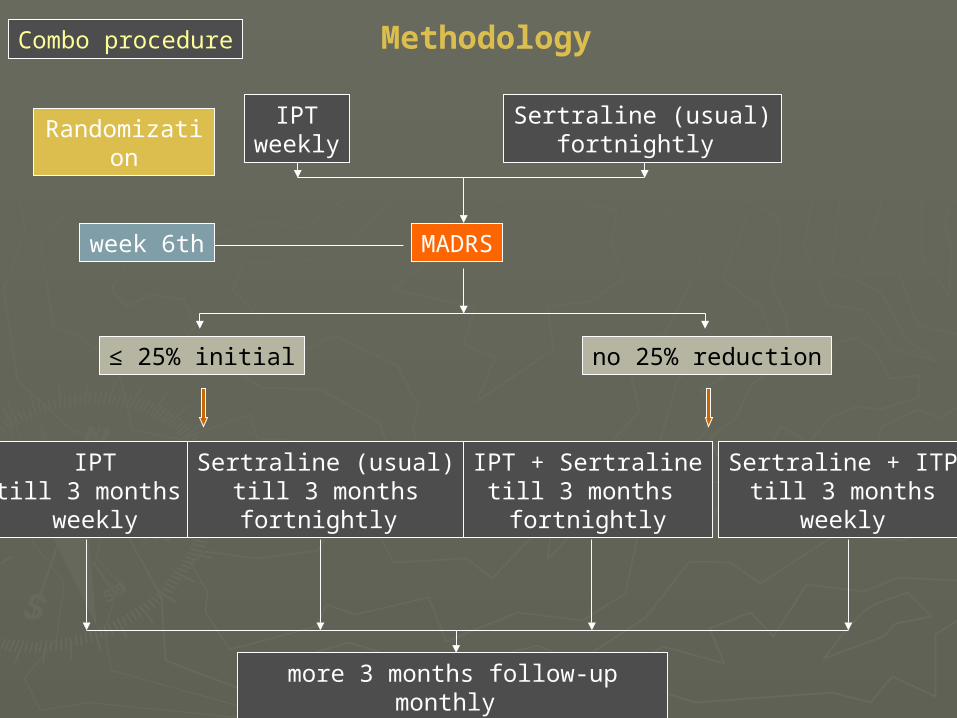
MethodologyCombo procedure
week 6th MADRS
IPTtill 3 months
weekly
Sertraline (usual)till 3 monthsfortnightly
≤ 25% initial no 25% reduction
IPT + Sertralinetill 3 months
fortnightly
Sertraline + ITPtill 3 months
weekly
more 3 months follow-up monthly
IPTweekly
Sertraline (usual)fortnightly
Randomization
raters don´t treat patients, are blind to treatment type and inter-rater attuned
Methodology
MADRS regular evaluations
Data concerning COMBO intervention include baseline data (before COMBO formal beginning ) as a third treatment
group
Same care provider for all patients

Some instruments description
ATT 18
EVA
Methodology
Diabetes adaptation, Core Diabetes Integration ConceptPortuguese short version of ATT39 (Dunn et al, 1986)high values – better adaptation, correlates with HbA1c
Portuguese version Adult Attachment Scale – R (Collins & Read, 1990)3 attachment dimensions: Close, Anxiety and DependClose/Secure; Anxiety/Insecure; Depend/↓Avoidant (confidante)
DSESPortuguese version of Diabetes Self-Efficacy Scale (Crabtree 1986)2 dimensions: diet and exercise

Results
Global sample = 34
Age 55.17 ± 5.9 yrs
Education 6.85 ± 3.07 yrs
♀ 30 (88.2%)
≥ 2 chronic complications 14 (41.2%)
Insulin users 18 (52.9%)
Diabetes duration 12.55 ± 5.75 yrs
HADS dep 10.44 ± 2.87
HADS anx 13.14 ± 4.05
MADRS 24.32 ± 5.27
HbA1c 9.05 ± 2.13

Results
TIP=17 USUAL=17
No differences between patients at baseline:
age, gender, diabetes duration, ≥2 chronic complications, insulin users, diabetes adaptation, depression, anxiety,attachment, sub-scales,diabetes ,self-efficacy, HbA1c
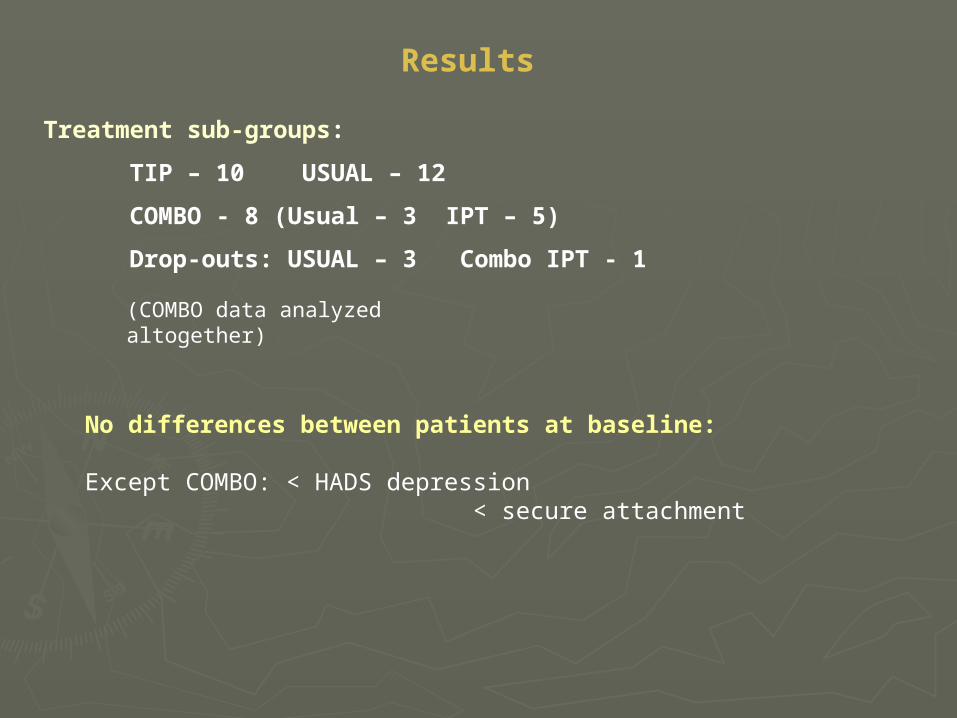
Treatment sub-groups:
TIP – 10 USUAL – 12
COMBO - 8 (Usual – 3 IPT – 5)
Drop-outs: USUAL – 3 Combo IPT - 1
Results
(COMBO data analyzed altogether)
No differences between patients at baseline:
Except COMBO: < HADS depression < secure attachment

Results
TIP - USUAL
Total patients Area Problem
Problem IP Area Number %
Mourning 6 4,3
IP conflicts 18 28,3
Role Transition(3 DM) adaptation
10 10,9

MADRS
**
* ***
**

Adjustment to diabetes
*
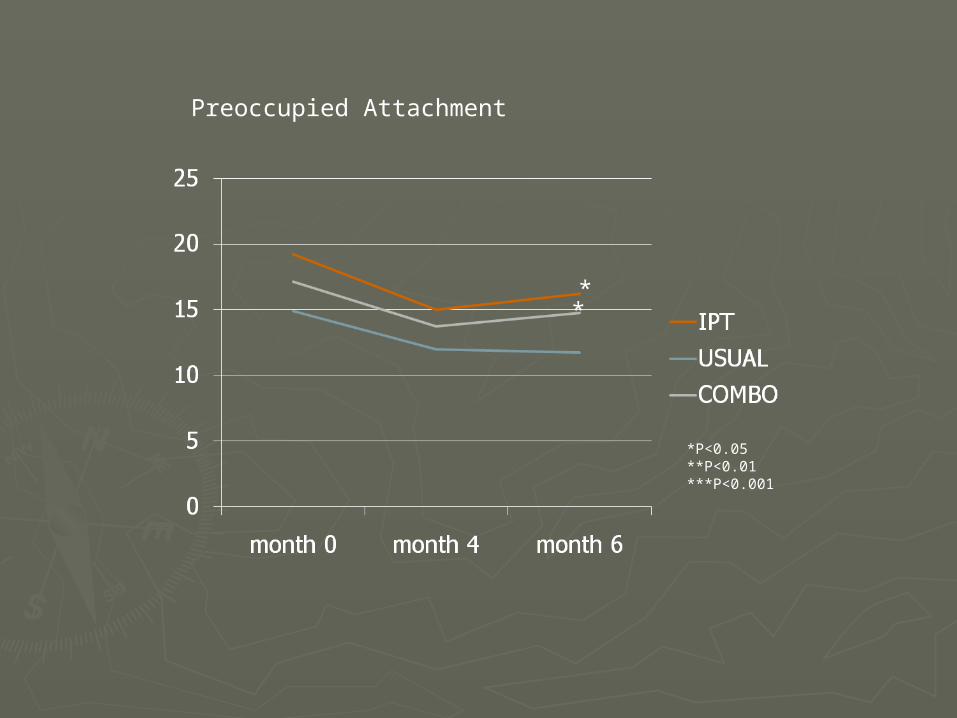
Preoccupied Attachment
*P<0.05**P<0.01***P<0.001
* *

Secure Attachment
*P<0.05**P<0.01***P<0.001
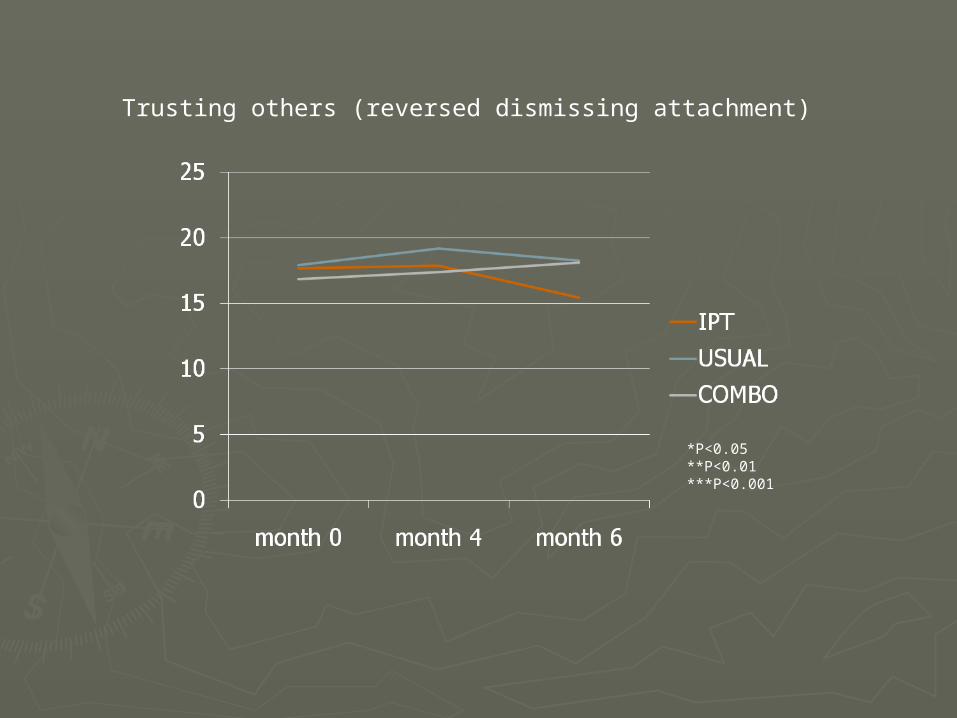
Trusting others (reversed dismissing attachment)
*P<0.05**P<0.01***P<0.001

Diabetes Self-efficacy DIET
*P<0.05**P<0.01***P<0.001
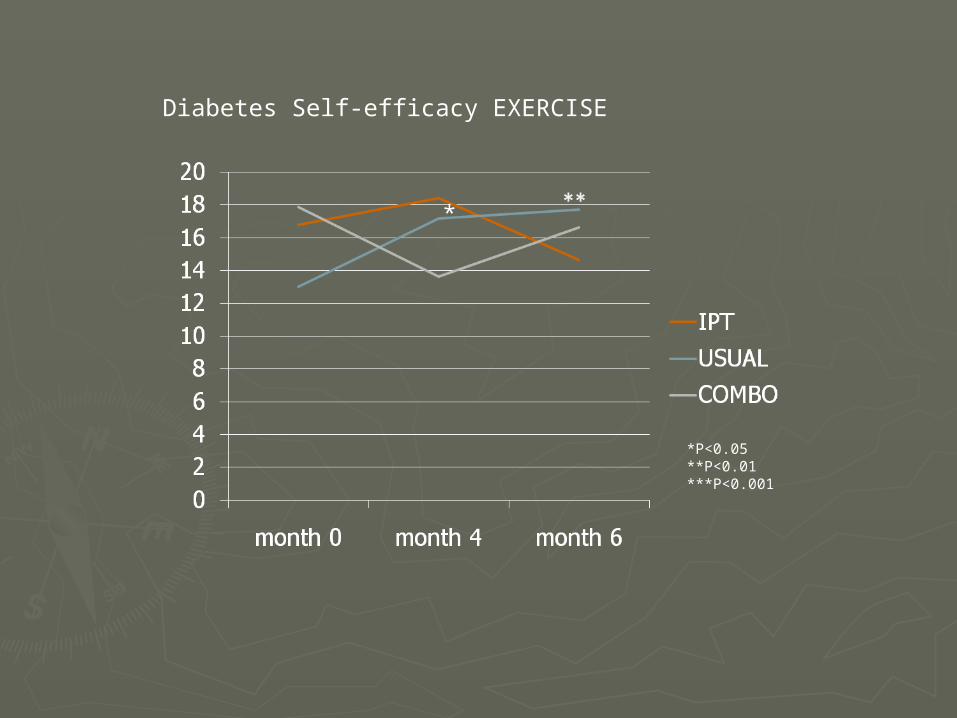
Diabetes Self-efficacy EXERCISE
*P<0.05**P<0.01***P<0.001
*

Glicohemoglobin A1c
*P<0.05**P<0.01***P<0.001
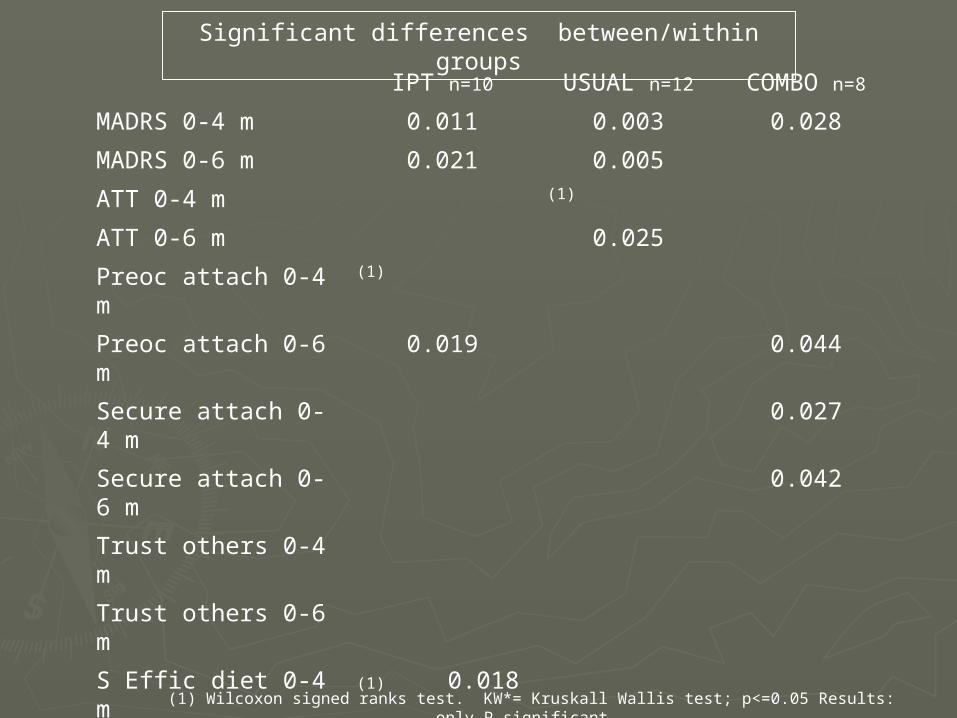
IPT n=10 USUAL n=12 COMBO n=8
MADRS 0-4 m 0.011 0.003 0.028
MADRS 0-6 m 0.021 0.005
ATT 0-4 m (1)
ATT 0-6 m 0.025
Preoc attach 0-4 m (1)
Preoc attach 0-6 m 0.019 0.044
Secure attach 0-4 m
0.027
Secure attach 0-6 m
0.042
Trust others 0-4 m
Trust others 0-6 m
S Effic diet 0-4 m (1) 0.018
S Effic diet 0-6 m (1) 0.018
S Effic exercise 0-4 m
(1) (1) 0.012 (KW*)
S Effic exercise 0-6 m
0.005
HbA1c 0-6 m (1) 0.045
(1) Wilcoxon signed ranks test. KW*= Kruskall Wallis test; p<=0.05 Results: only P significant.
Significant differences between/within groups
Conclusions
Preliminary results, small sample
Both IPT and USUAL reduce MADRS score
Both COMBO and IPT better decrease insecure attachment
COMBO better increase secure attachment
COMBO was not related to depression and metabolic outcome
IPT was not related with metabolic control
USUAL better with diabetes adaptation, self-efficacy and metabolic control


















