Interpersonal Approaches to Treating Depression in ... · Interpersonal Approaches to Treating...
34
Interpersonal Approaches to Treating Depression in Adolescents and Adults Presented By: Mary Acri, PhD June 13, 2018
Transcript of Interpersonal Approaches to Treating Depression in ... · Interpersonal Approaches to Treating...
Interpersonal Approaches to Treating Depression in Adolescents and Adults
Presented By: Mary Acri, PhD
June 13, 2018
Outline 1. Depression: An Overview
2. Interpersonal Theories of Depression
3. Assessment & Screening Tools, Strategies and Interventions
4. Case Example
6. Additional Resources
Depression: An Overview

Let’s Chat ‣ Is depression a common diagnosis that you treat or provide
services for?
‣ What are you currently doing for adolescents who suffer with depression?
‣ What are you currently doing for adults who suffer with depression?
Prevalence • Depression is a common mood disorder and the second leading
cause of disability worldwide1
• Epidemiological studies have shown that depression affects between 4-5% of adolescents annually, and 16.6% of adults at some point during their lifetime.2,3
• Certain groups, including women and persons who are impacted
by poverty, are at increased risk of depression.4,5
Prevalence and Burden • Untreated depression is associated with…
• impairments in academic, social, and occupational functioning,
• comorbid health and mental health disorders,
• premature morbidity and mortality.6-8
• The annual economic burden of depression is approximated at 52.9 billion in the United States alone.9
Risk Factors • Risk factors associated with depression include…
• Biological factors • Genetics and hereditary factors10,11
• Psychological factors
• Co-morbid mental health problems, past suicide attempts12,13
• Environmental and social factors
• Stressful life events and early childhood experiences, rejection by peers and social isolation14-16
• Among adolescents, a family history of depression and stress
exposure are the strongest predictors of depression.2
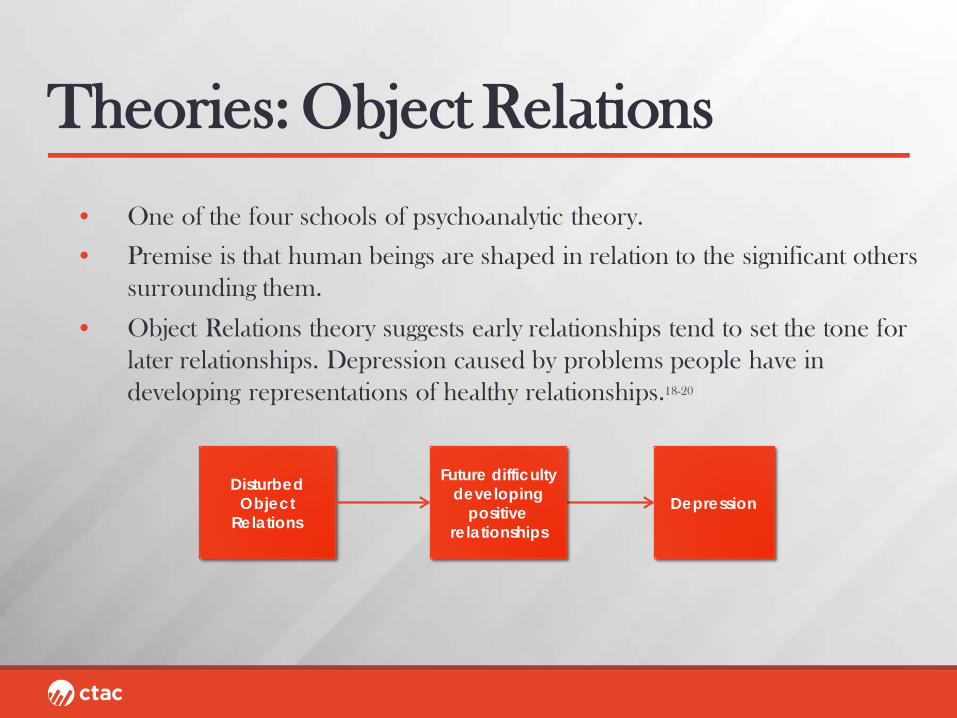
Theories: Object Relations
• One of the four schools of psychoanalytic theory.
• Premise is that human beings are shaped in relation to the significant others surrounding them.
• Object Relations theory suggests early relationships tend to set the tone for later relationships. Depression caused by problems people have in developing representations of healthy relationships.18-20
Disturbed Object
Relations
Future difficulty developing
positive relationships
Depression

Theories: Interactional Theory • Postulated that our interactions with others can influence our
emotional well-being.21
• May be moderated by excessive reassurance and rejection.
Interactions w/Others Depression
Excessive Reassurance,
Rejection

Theories: Interpersonal Stress • Those who excessively seek reassurance unintentionally generate
negative life events, some of which are interpersonal in nature, that increase their risk for depression.22,23
Excessive reassurance
Generate negative life
events Depression
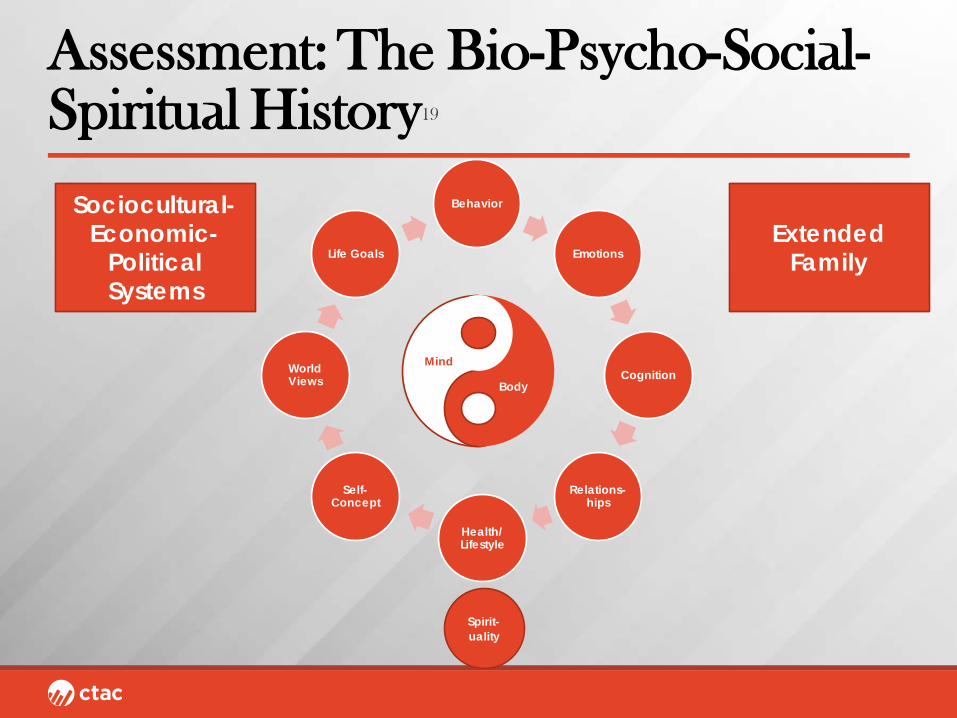
Assessment: The Bio-Psycho-Social-Spiritual History19
Behavior
Emotions
Cognition
Relations-hips
Health/ Lifestyle
Self-Concept
World Views
Life Goals
Sociocultural-Economic-
Political Systems
Extended Family
Spirit-uality
Mind
Body

Assessment: Genogram19
38 31 26
61 60
22 21
10
s 96 d 97
95 m 02
Liv Bo Lea Pat
Eve
Hal
Kendrick
m 71 m 97
32
Rico
5
Ed
24
99
6
Harley
Hank
91 90 89 86 Sal Harriet Iona Ira
Betty
71
m 71
Jo Al
56
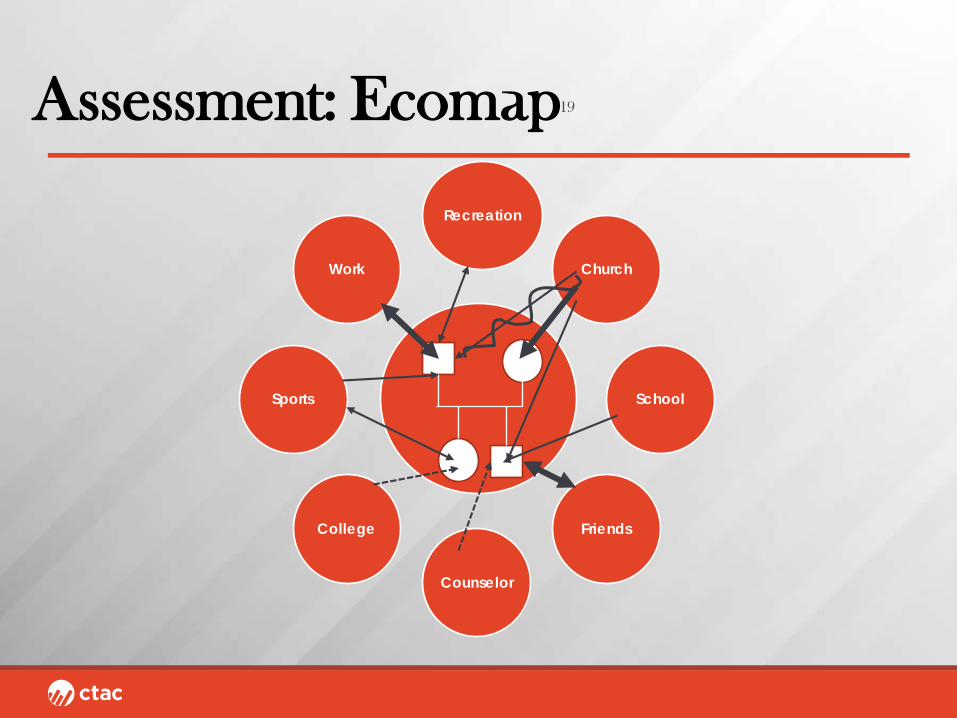
Assessment: Ecomap19
Recreation
Church
School
Friends
Counselor
College
Sports
Work
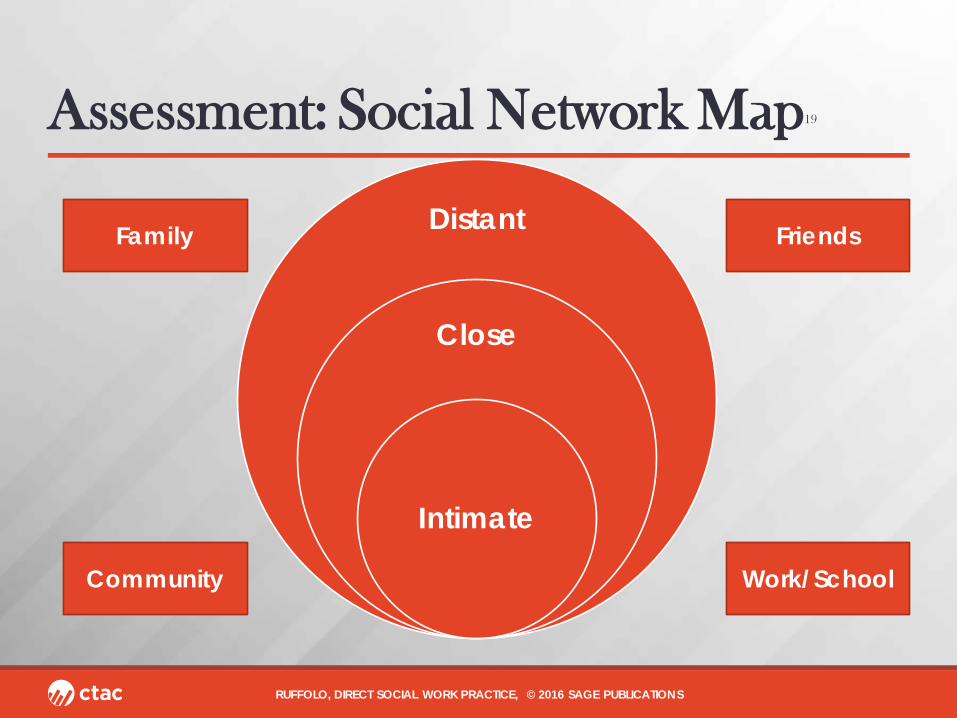
Assessment: Social Network Map19
Distant
Close
Intimate
RUFFOLO, DIRECT SOCIAL WORK PRACTICE, © 2016 SAGE PUBLICATIONS
Family Friends
Community Work/School
Screening and Assessment Tools • Vary based upon type of relationship (e.g., with parent, significant
other) and quality (e.g., trust, intimacy). Also may be part of a larger scale.
1. The Brief Impairment Scale-23 items, assesses functioning in three areas, including interpersonal relationships. For youth 4-17 years of age.24
2. Dyadic Trust Scale-8 items, assesses trust in a romantic relationship.25
Strategies 1. Identifying and Expressing Emotions in Current Relationships
• Helping the client understand what emotion they are feeling and why.
• Assisting the client in expressing emotion in a positive, healthy way.
2. Examining the connection between prior relationships and their influence upon current relationships, including one’s behaviors and emotions

Strategies 3. When working with couples and families, identify negative communication patterns, unrealistic expectations, and how family members interact;
Interventions may then include…
a. Communication skills
b. Education/setting realistic expectations
c. Changing patterns of interactions
4. Modeling and role play corrective/adaptive interactions with others.
Intervention: Interpersonal Psychotherapy (IPT)19,26
• Developed in the 1970’s.
• Psychodynamically informed.
• Concerned with the interpersonal context-relational factors that predispose, precipitate, and perpetuate the patient’s distress. Four problem areas.
• Brief treatment-ranges from 6-20 sessions.
• Effective for adolescents and adults.
• Individual, couples and group formats.
IPT19
‣ Stress-Diathesis Model
‣ Psychosocial stressors from any of the problem areas can lead to psychological distress, especially when combined with an attachment disruption in the context of a poor social support network.
‣ Goal-symptom reduction, improved functioning and enhanced social support.
IPT19
‣ The Interpersonal Triad
• Interpersonal distress leads to psychological sxs.
• Stressors start this process.
• Capacity of individual to manage crisis biologically and psychologically is influenced by: ◦ Biopsychosocialspiritual vulnerabilities (diatheses)
◦ Strengths (temperament, attachment style). May modulate or exacerbate the crisis.
• Significant relationships and social support provide the context in which the stress-diathesis interaction occurs, and further modifies the individual's ability to cope with his or her distress.
Problem Areas19
‣ Grief • Death or loss
‣ Interpersonal Disputes • e.g., disputes within families
‣ Role Transitions • e.g., divorce, new job, diagnosis of a health condition
‣ Interpersonal sensitivity (deficits) • Difficulty forming/maintaining relationships

Structure19
‣ Five phases
1. Assessment-Clinical interview and determines the appropriateness of IPT for the individual.
2. Initial Sessions-Creating an interpersonal inventory, developing an interpersonal formulation, contracting for a number of sessions.
3. Middle Sessions-Address the relevant problem area
4. Termination Sessions for Acute Treatment
5. Maintenance Sessions
Techniques19
‣ Nondirective and directive exploration ‣ Clarification ‣ Encouragement of affect • Express, understand, and manage affect, so to recognize one’s affect,
communicate it to others ‣ Communication analysis • Identifying communication patterns and response elicited from others,
motivate client to communicate more effectively, learn new ways to communicate.
‣ Role play ‣ Problem solving ‣ Therapeutic relationship
IPT for Adolescents27
‣ Typically for adolescents between 12-18 years of age.
‣ 1x week, for 12-16 weeks. ‣ Goals: Remittance of depression via strengthening
communication and problem solving skills.
‣ Family involvement critical. Caregivers receive psychoeducation about depression, learn different patterns of interaction/communication, problem-solving skills, and practice with their child.
IPT for Adolescents27
‣ Phases
Initial Phase
1. Psychoeducation
2. Assigning the sick role
3. Interpersonal inventory
4. Formulating the problem area (same as adults)
IPT for Adolescents27
‣ Phases
Middle Phase
1. Actively work on problem area
‣ Strategies: clarification of and emotional expression
‣ Analysis of communication and problem solving
‣ Skill instruction in both areas
‣ Role play and homework assignments
IPT for Adolescents27
‣ Phases
Termination Phase
1. Review of work together/feelings about ending
2. Relapse prevention and assessment of need for future treatment

Case Example? ‣ How would you apply these approaches to an adolescent or adult
with depression?
‣ What strategies would you use?
References 1. World Health Organization. (2003). The world health report 2003: shaping the future. World Health Organization.
2. Thapar, A., Collishaw, S., Pine, D. S., & Thapar, A. K. (2012). Depression in adolescence. The Lancet, 379(9820), 1056-1067.
3. Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of general psychiatry, 62(6), 593-602.
4. Gelaye, B., Rondon, M. B., Araya, R., & Williams, M. A. (2016). Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. The Lancet Psychiatry, 3(10), 973-982.
5. Ertel, K. A., Rich-Edwards, J. W., & Koenen, K. C. (2011). Maternal depression in the United States: Nationally representative rates and risks. Journal of Women's Health, 20(11), 1609-1617.
6. Lépine, J. P., & Briley, M. (2011). The increasing burden of depression. Neuropsychiatric disease and treatment, 7(Suppl 1), 3.
7. Romera, I., Perez, V., Menchón, J. M., Delgado-Cohen, H., Polavieja, P., & Gilaberte, I. (2010). Social and occupational functioning impairment in patients in partial versus complete remission of a major depressive disorder episode. A six-month prospective epidemiological study. European Psychiatry, 25(1), 58-65.
8. Kessler, R. C., Barber, C., Birnbaum, H. G., Frank, R. G., Greenberg, P. E., Rose, R. M., ... & Wang, P. (1999). Depression in the workplace: effects on short-term disability. Health affairs, 18(5), 163-171.
9. Greenberg, P. E., Kessler, R. C., Birnbaum, H. G., Leong, S. A., Lowe, S. W., Berglund, P. A., & Corey-Lisle, P. K. (2003). The economic burden of depression in the United States: how did it change between 1990 and 2000?. Journal of clinical psychiatry, 64(12), 1465-1475.
10. Wallace, J., Schnieder, T., & McGuffin, P. (2002). Genetics of depression.
References 11. Sullivan, P. F., Neale, M. C., & Kendler, K. S. (2000). Genetic epidemiology of major depression: review and meta-analysis. American Journal of Psychiatry, 157(10), 1552-1562. 12. Lewinsohn, P. M., Roberts, R. E., Seeley, J. R., Rohde, P., Gotlib, I. H., & Hops, H. (1994). Adolescent psychopathology: II. Psychosocial risk factors for depression. Journal of abnormal psychology, 103(2), 302. 13. Lewinsohn, P. M., Rohde, P., & Seeley, J. R. (1998). Major depressive disorder in older adolescents: prevalence, risk factors, and clinical implications. Clinical psychology review, 18(7), 765-794. 14. Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I. W., Harrington, H., ... & Poulton, R. (2003). Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science, 301(5631), 386-389. 15. Slavich, G. M., & Irwin, M. R. (2014). From stress to inflammation and major depressive disorder: a social signal transduction theory of depression. Psychological bulletin, 140(3), 774. 16. Boivin, M., Poulin, F., & Vitaro, F. (1994). Depressed mood and peer rejection in childhood. Development and Psychopathology, 6(3), 483-498. 17. Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: a meta-analytic review. PLoS medicine, 7(7), e1000316. 18. Slipp, S. (1976). An intrapsychic–interpersonal theory of depression. Journal of the American Academy of Psychoanalysis, 4(3), 389-409. 19. Ruffolo, M. C., Perron, B. E., & Voshel, E. H. (2014). Direct social work practice: Theories and skills for becoming an evidence-based practitioner. SAGE Publications. 20. Greenberg, J. (1983). Object relations in psychoanalytic theory. Harvard University Press
References 21. Coyne, J. C. (1976). Depression and the response of others. Journal of abnormal psychology, 85(2), 186. 22. Joiner Jr, T. E., & Metalsky, G. I. (2001). Excessive reassurance seeking: Delineating a risk factor involved in the development of depressive symptoms. Psychological Science, 12(5), 371-378. 23. Potthoff, J. G., Holahan, C. J., & Joiner, T. E. (1995). Reassurance seeking, stress generation, and depressive symptoms: An integrative model. Journal of personality and social psychology, 68(4), 664. 24. Bird, H. R., Canino, G. J., Davies, M., Ramírez, R., Chávez, L., Duarte, C., & Shen, S. (2005). The Brief Impairment Scale (BIS): A multidimensional scale of functional impairment for children and adolescents. Journal of the American Academy of Child & Adolescent Psychiatry, 44(7), 699-707. 25. Larzelere, R. E., & Huston, T. L. (1980). The dyadic trust scale: Toward understanding interpersonal trust in close relationships. Journal of Marriage and the Family, 595-604. 26. Klerman, G. L., & Weissman, M. M. (1994). Interpersonal psychotherapy of depression: A brief, focused, specific strategy. Jason Aronson, Incorporated. 27. Interpersonal Psychotherapy for Adolescents. Downloaded May 1, 2018 from http://www.cebc4cw.org/program/interpersonal-psychotherapy-for-depressed-adolescents/detailed

Q&A

Resources 1. IPT for adolescents http://www.cebc4cw.org/program/interpersonal-psychotherapy-for-depressed-adolescents/detailed 2. https://iptinstitute.com Contact Information: Mary C. Acri, PhD Senior Research Scientist [email protected]
Upcoming Events with CTAC ‣ Effectively Employing and Supervising Youth Peer Advocates,
with Bianca Logan, Brianna Valesey, and Azaria Wittekind ◦ When: Thursday, June 14 - 1:00 PM
‣ Motivational Interviewing: Clinical Updates Within Substance Abuse Treatment, with Tara Dewitt ◦ When: Tuesday, June 19 - 12:00 PM
‣ Addressing the Mental Health Needs of Children with Incarcerated Parents, with Anna Morgan-Mullane ◦ When: Wednesday, June 27 - 12:00 PM
‣ And, many other offerings! Visit www.ctacny.org for more information!