
Internet-Based Patient Education: Facilitating Shared Decision-Making Between Plastic Surgeons and...
20
Education: Facilitating Shared Decision- Making Between Plastic Surgeons and Women Seeking Breast Reconstruction After Mastectomy Topics in Womens’ Health APHA Poster Session 4076.0, Board #5, 11/18/03 Elizabeth Steinberger RN, MA, MPH UNC School of Public Health Edwin Wilkins MD, MS University of Michigan Section of Plastic Surgery
-
Upload
joan-black -
Category
Documents
-
view
219 -
download
0
Transcript of Internet-Based Patient Education: Facilitating Shared Decision-Making Between Plastic Surgeons and...

Internet-Based Patient Education:Facilitating Shared Decision-Making
Between Plastic Surgeons and Women Seeking Breast Reconstruction
After Mastectomy
Topics in Womens’ HealthAPHA Poster Session 4076.0, Board #5, 11/18/03
Elizabeth Steinberger RN, MA, MPHUNC School of Public Health
Edwin Wilkins MD, MSUniversity of Michigan Section of Plastic Surgery
Abstract The Internet makes it possible to provide especially up-to-date, low-cost, and accessible health education interventions. Shared decision-making theory was used to construct a web site designed to give breast cancer patients complete, balanced, easy-to-understandinformation about breast reconstruction options after mastectomy.
In 2000, a pilot prospective cohort study (n=51) evaluated the acceptability and impact of the site. In one clinic, women viewed the web site before seeing the plastic surgeon. In a second clinic, women were given a brochure and a “pencil talk” while consulting the same surgeon. The groups did not vary by age, race, or computer literacy. Knowledge of breast reconstruction options; decision-making anxiety and desire for information; and satisfaction with the provider, length of provider visit, and quality of care likewise did not vary significantly between groups. However, the web group reported feeling more comfortable using computers (p<0.01) and web sites (p<0.009). Moreover, women using the web site reported significantly higher satisfaction with the quality of information (p<0.026) and spent an average of 14.7 minutes less with the surgeon (p<0.0005).
The Web is an acceptable educational venue for breast cancer patients. Internet-based interventions can facilitate shared decision-making between doctors and patients by saving physician time while providing higher quality health information to patients.
Breast Reconstruction Options After Mastectomy: A Consumer’s Guidehttp://www.surgery.med.umich.edu/breastrecon.htm
What is MBROS?The Michigan Breast Reconstruction Outcome Study (MBROS) is a six-year study (1994-2000) of multiple aspects of breast reconstruction outcomes. During the lifetime of the study, MBROS has assessed a total of 397 actively participating patients from 11 medical centers in the U.S. and Canada. Patients are followed for two years from the date of their breast reconstruction surgeries to determine long-term outcomes of breast reconstruction. MBROS is supported by a grant from the Department of Defense, United States Army Medical Research and Material Command, DAMD 17-94-J-4044.
Studies have been completed on:
• Psychosocial outcomes of breast reconstruction by procedure and timing of reconstruction. • Patient satisfaction with aesthetic results by procedure type (implants vs.
pedicle TRAMS vs. free TRAMS). • Objective, computerized assessments of symmetry of breast reconstruction results by procedure type. • Physical functioning one year after surgery by procedure type. • Mammography after TRAM flap reconstruction.
Web Site Development:Purposes and Sources
Purposes1) Provide thorough, accurate, easy-to-understand information about
available breast reconstruction options after mastectomy.
2) Facilitate shared decision-making between plastic surgeons and women seeking post-mastectomy breast reconstruction.
SourcesBreast Reconstruction Information:
• Unpublished University of Michigan Hospital patient manual onBreast reconstruction (Wilkins, 1996)• Published patient education brochures on breast reconstructionExisting web sites on breast cancer surgery
Input from Former Breast Reconstruction Patients:
• Focus group (n=5) to assess text drafts for relevance and readability.• Interviews (n=4) to gather personal vignettes of breast reconstruction.
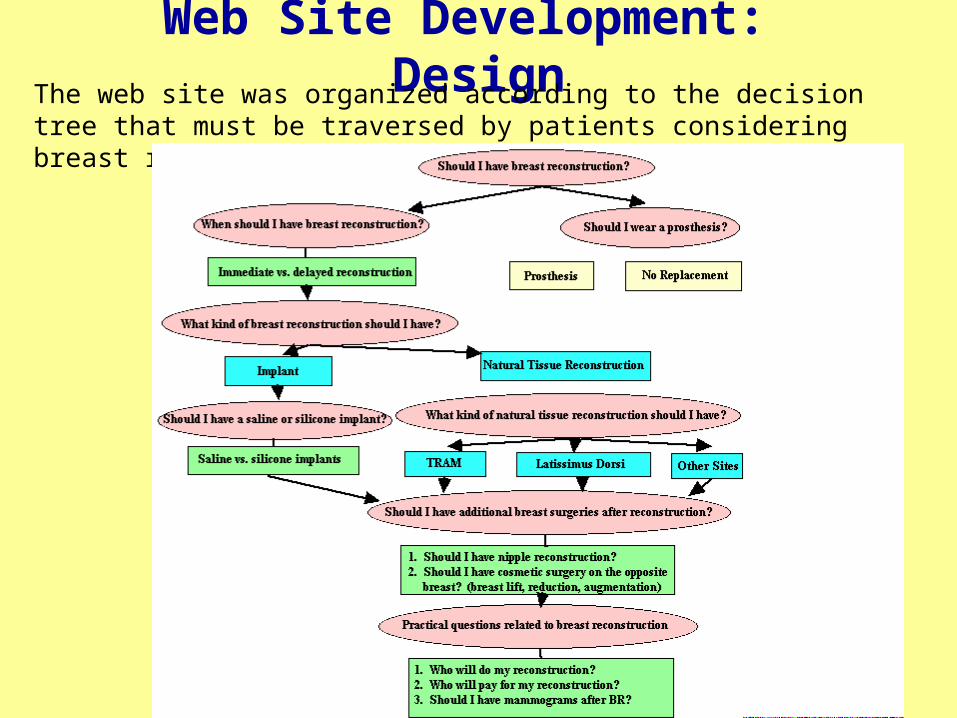
Web Site Development: DesignThe web site was organized according to the decision tree that must be traversed by patients considering breast reconstruction:
ConstructionAll options portrayed include discussions of equipment and procedures, advantages and disadvantages, risks, and an options summary. Some also include vignettes of the personal experiences of former breast reconstruction patients.
HOMEPAGE
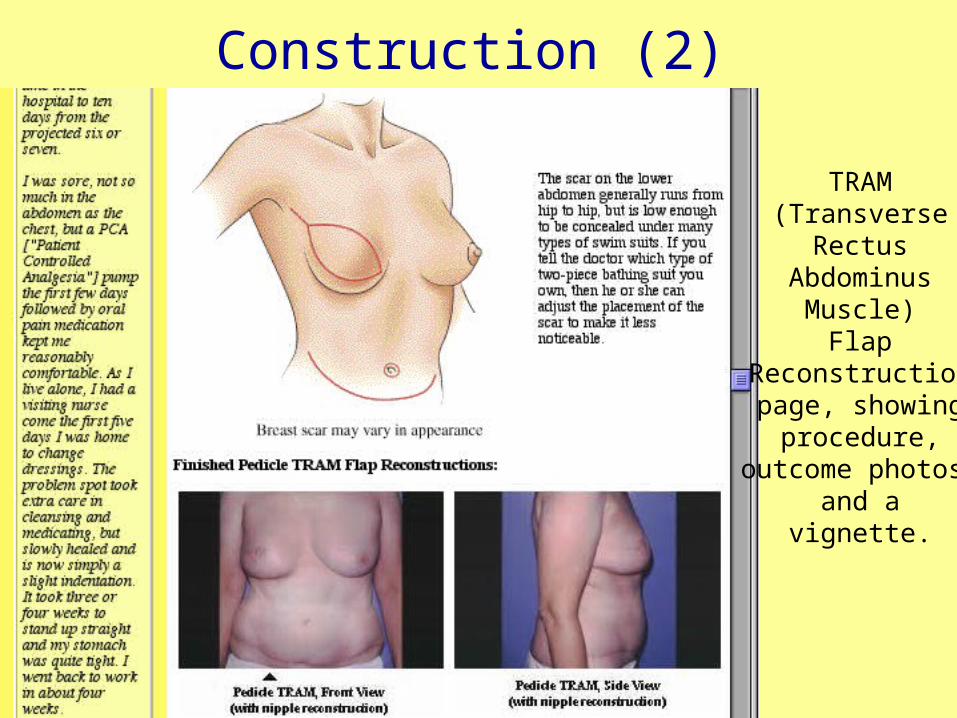
Construction (2)
TRAM(Transverse
RectusAbdominus
Muscle)Flap
Reconstructionpage, showing
procedure,outcome photos,
and avignette.

Construction (3)
Implantrisk page,listing anddescribing
complicationsof implants.
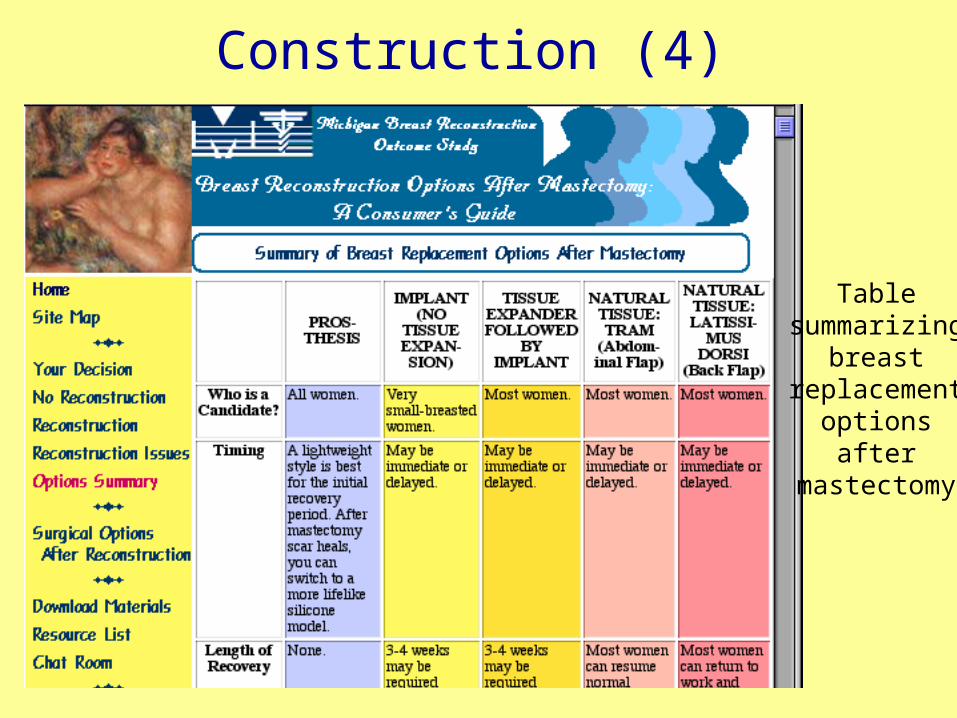
Construction (4)
Tablesummarizing
breastreplacement
optionsafter
mastectomy
Evaluation: Background• Shared medical decision-making theory (Mulley, Lindbergh--prostate cancer surgery). Provide patients with all of the information needed to understand the options, then allow them to choose their treatment in partnership with the doctor.
Patients are more likely to be satisfied with the outcome of treatment because:
1) they are invested in the decision-making process;2) they re better informed about the options; and3) the option chosen is more likely to suit their values and lifestyle.
• At the time of creation (1999):
1) No site existed that was solely dedicated to educating patients about breast reconstruction.
2) The feasibility of using Web-based materials to facilitate decision-making about surgery in clinical settings had not yet been tested.
(Now sites on breast augmentation also exist and have been evaluated.)
MethodsFrom January through June 2000, a pilot prospective cohort study (n=51) evaluatedthe acceptability and impact of the site. An experimental group of 34 pre-mastectomybreast cancer patients attending the breast cancer clinic at the University of MichiganHospital were instructed to view the web site online in the patient education center orclinic thirty minutes before their scheduled appointment with the plastic surgeon. Afesearch assistant taught those who were unfamiliar with computers or the Internethow to use the site. A control group of 17 pre-mastectomy patients attending a private breast reconstruction clinic were given a popular brochure on breastreconstruction options in the waiting room and a “pencil talk” explaining the optionsfrom the same surgeon.
Each patient’s consultation with the plastic surgeon was timed to the nearest minute.All patients were then given an exit survey to assess their basic knowledge of breastreconstruction options; their satisfaction with materials, provider, and length of visit;their anxiety regarding breast reconstruction; and their use of computers and the Internet. Responses were recorded on five-point Likert scales. After completingthe survey, patients were given a copy of the Consumer’s Guide to Breast Reconstruction Options after Mastectomy in booklet form to refer to at home.
Research Design

ResultsDemographics:
Experimental Group(Web)
Control Group(Brochure)
Significance
Age
EducationalLevel
Race
47.3 51.5 p<0.156
85.3% White,8.8% Black
75.6% White,17.6% Black
p<0.597
4.0(college graduate)
3.1(some college) p<0.0015
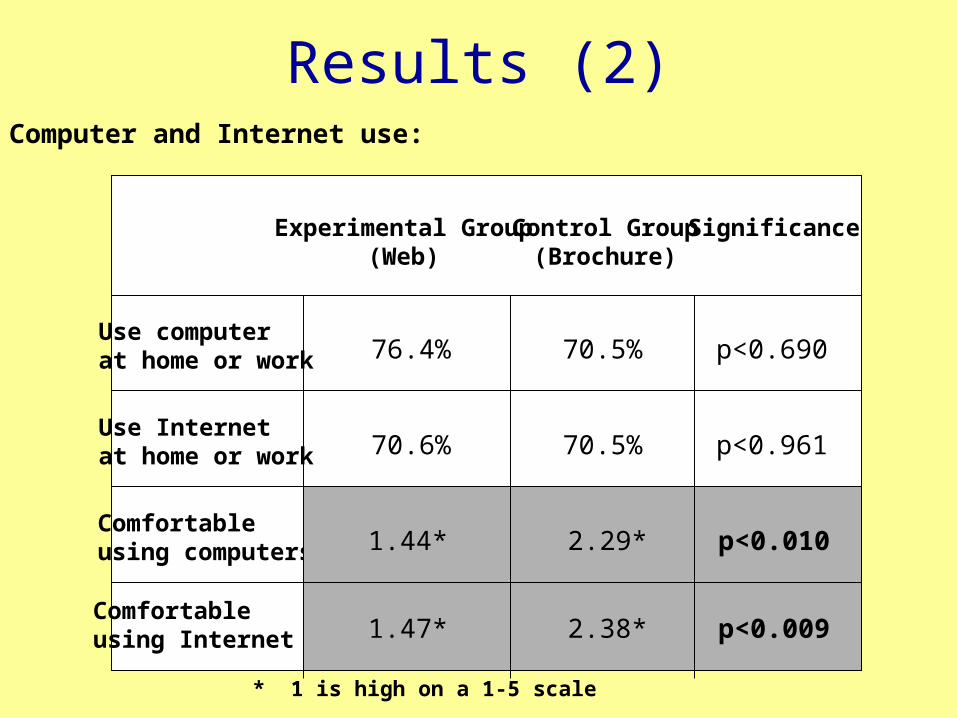
Results (2)Computer and Internet use:
Experimental Group(Web)
Control Group(Brochure)
Significance
Use computerat home or work
Use Internetat home or work
Comfortable using computers
Comfortable using Internet
76.4% 70.5%
70.5%70.6%
p<0.690
p<0.961
1.44* 2.29*
1.47* 2.38*
p<0.010
p<0.009
* 1 is high on a 1-5 scale
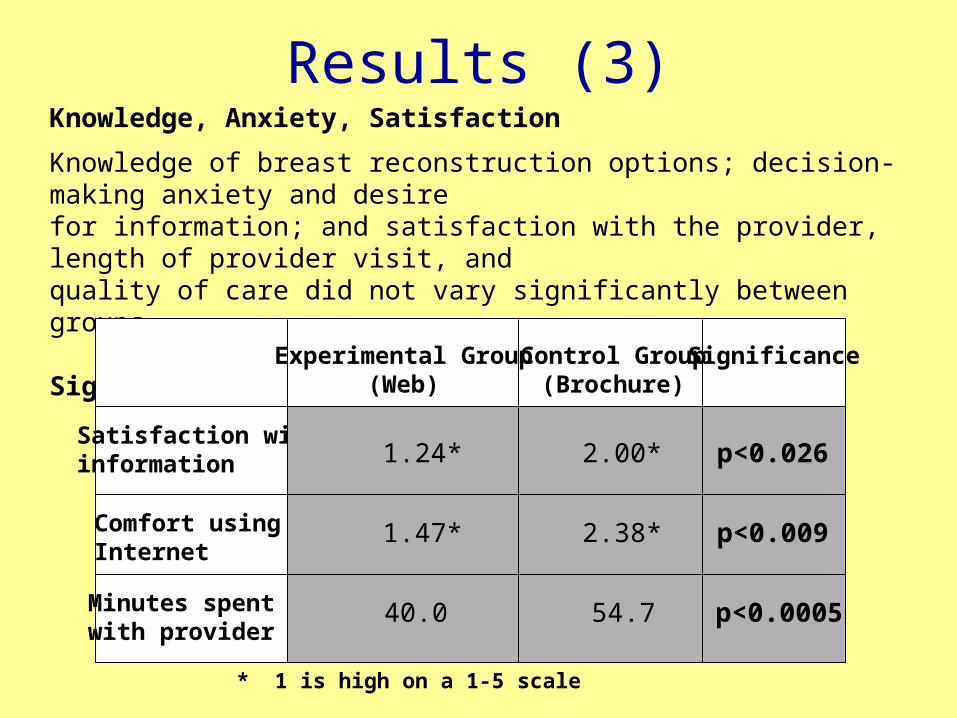
Knowledge, Anxiety, Satisfaction
Knowledge of breast reconstruction options; decision-making anxiety and desirefor information; and satisfaction with the provider, length of provider visit, andquality of care did not vary significantly between groups.
Significant Results:
Results (3)
Experimental Group(Web)
Control Group(Brochure)
Significance
Satisfaction withinformation
Comfort usingInternet
Minutes spent with provider
2.38* p<0.0091.47*
40.0 54.7 p<0.0005
p<0.0261.24* 2.00*
* 1 is high on a 1-5 scale

Significant Results: 1. Satisfaction with Information
00.20.40.60.8
11.21.41.61.8
2
Rating on 1 to 5 Scale (1 is
high)
Study Group
Satisfaction With Information
Experimental (Web)
Control (Brochure)
“I received very good explanations of my options for replacing or replacing my breast(s) after mastectomy.”
Experimental (Web) group more satisfied with information (p<0.026)
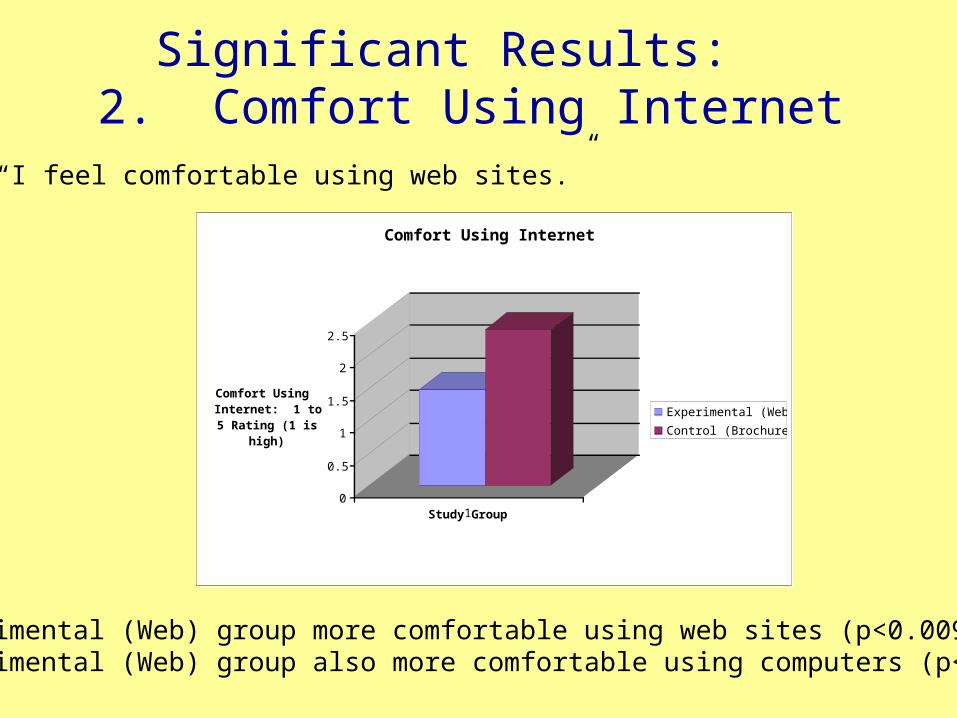
Significant Results: 2. Comfort Using Internet
0
0.5
1
1.5
2
2.5
Comfort Using Internet: 1 to 5 Rating (1 is
high)
1Study Group
Comfort Using Internet
Experimental (Web)
Control (Brochure)
“I feel comfortable using web sites.”
Experimental (Web) group more comfortable using web sites (p<0.009).Experimental (Web) group also more comfortable using computers (p<0.010).
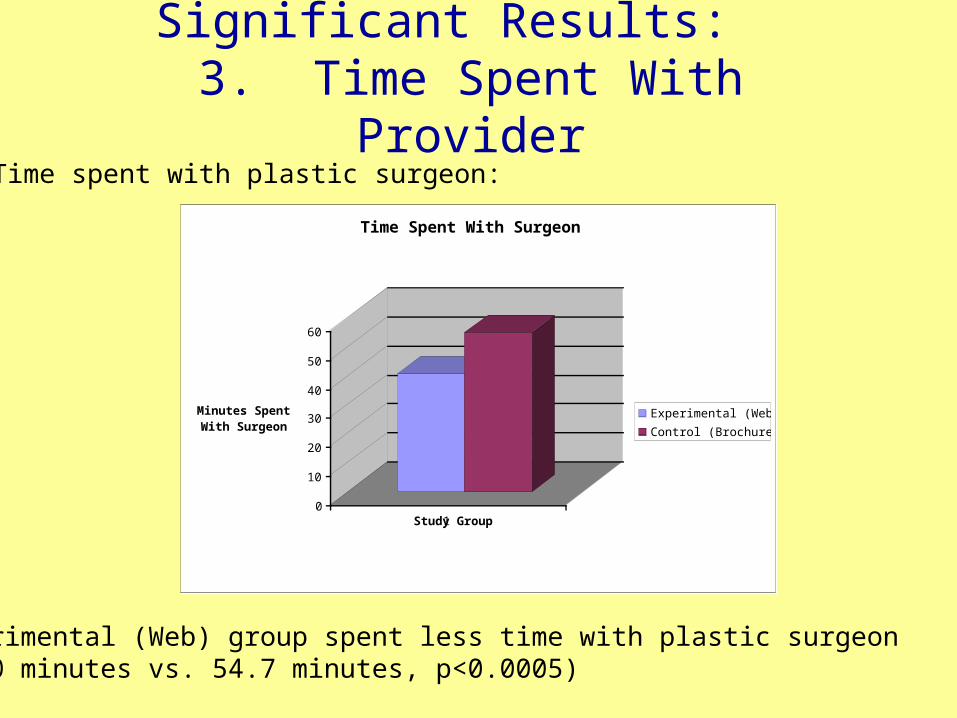
Significant Results: 3. Time Spent With Provider
0
10
20
30
40
50
60
Minutes Spent With Surgeon
1Study Group
Time Spent With Surgeon
Experimental (Web)
Control (Brochure)
Time spent with plastic surgeon:
Experimental (Web) group spent less time with plastic surgeon (40.0 minutes vs. 54.7 minutes, p<0.0005)
ConclusionsLimitations of the study:
1) Small sample size (n=51)2) Not randomized to conditions3) Possible confounders:
• Study setting (hospital vs. private clinic)• Educational level (higher for Web group)
Conclusions:
1) It is feasible to use web-based educational materials in a clinical setting.
2) Web-based materials provide higher quality information than brochures while saving physician time spent in explanation of options.
Contact InformationFor further information contact:
Elizabeth Steinberger RN, MA, MPHUNC School of Public HealthRosenau Hall 308, CB#7440Chapel Hill, NC [email protected]
Edwin Wilkins MD, MSSection of Plastic SurgeryUniversity of Michigan Hospital2130 Taubman Center1500 East Medical Center DriveAnn Arbor, MI [email protected]


















