InternationalJournal of Cardiology
40
Long-term prognosis and cost-effectiveness of left ventricular assist device as bridge to transplantation: A systematic review Michael Seco, Dong Fang Zhao, Michael J. Byrom, Michael K. Wilson, Michael P. Vallely, JohnF. Fraser, Paul G. Bannon PII: S0167-5273(17)31289-5 DOI: doi:10.1016/j.ijcard.2017.02.137 Reference: IJCA 24663 To appear in: International Journal of Cardiology Received date: 17 August 2016 Revised date: 26 February 2017 Accepted date: 27 February 2017 Please cite this article as: Seco Michael, Zhao Dong Fang, Byrom Michael J., Wilson Michael K., Vallely Michael P., Fraser John F., Bannon Paul G., Long-term prognosis and cost-effectiveness of left ventricular assist device as bridge to transplantation: A system- atic review, International Journal of Cardiology (2017), doi: 10.1016/j.ijcard.2017.02.137 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Transcript of InternationalJournal of Cardiology

�������� ����� ��
Long-term prognosis and cost-effectiveness of left ventricular assist device asbridge to transplantation: A systematic review
Michael Seco, Dong Fang Zhao, Michael J. Byrom, Michael K. Wilson,Michael P. Vallely, John F. Fraser, Paul G. Bannon
PII: S0167-5273(17)31289-5DOI: doi:10.1016/j.ijcard.2017.02.137Reference: IJCA 24663
To appear in: International Journal of Cardiology
Received date: 17 August 2016Revised date: 26 February 2017Accepted date: 27 February 2017
Please cite this article as: Seco Michael, Zhao Dong Fang, Byrom Michael J., WilsonMichael K., Vallely Michael P., Fraser John F., Bannon Paul G., Long-term prognosis andcost-effectiveness of left ventricular assist device as bridge to transplantation: A system-atic review, International Journal of Cardiology (2017), doi:10.1016/j.ijcard.2017.02.137
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Title
Long-term prognosis and cost-effectiveness of left ventricular assist device as bridge to transplantation: a
systematic review
Authors
Michael Seco BMedSc MBBS1,2,3,8
Dong Fang Zhao BA1,2,8
Michael J. Byrom MBBS PhD FRACS1,2,3,4,5,8
Michael K. Wilson MBBS FRACS2,3,5,6,8
Michael P. Vallely MBBS PhD FRACS1,2,3,4,5,6,8
John F. Fraser MBBS PhD MRCP FRCA FCICM7,8
Paul G. Bannon MBBS PhD FRACS1,2,3,4,5,8
Affiliations/Statement of Authorship
1. Sydney Medical School, The University of Sydney, Sydney, Australia
2. The Baird Institute of Applied Heart and Lung Surgical Research, Sydney, Australia
3. Cardiothoracic Surgical Unit, Royal Prince Alfred Hospital, Sydney, Australia
4. Institute of Academic Surgery, Royal Prince Alfred Hospital, Sydney, Australia
5. Sydney Heart and Lung Surgeons, Sydney, Australia
6. Australian School of Advanced Medicine, Macquarie University, Sydney, Australia
7. Critical Care Research Group, The Prince Charles Hospital, The University of Queensland
8. This author takes responsibility for all aspects of the reliability and freedom from bias of the data presented
and their discussed interpretation

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Corresponding Author
Paul G. Bannon
The Baird Institute of Applied Heart & Lung Surgical Research
305/100 Carillon Ave, Newtown NSW 2042, Australia
T: +61295503714
F: +61295197584
Acknowledgements, funding sources and disclosures
The authors thank the Centre of Research Excellence for Advanced Cardio-respiratory Therapies Improving
OrgaN Support (ACTIONS-CRE) and the National Health and Medical Research Council (NHMRC) for
supporting this research. We thank David McGiffin for critically reviewing the manuscript. We also thank Jeff
Geng for advice regarding the cost-effectiveness analysis.
There were no funding sources for this research.
The authors report no relationships that could be construed as a conflict of interest
Key words
Left ventricular assist device; Bridge-to-transplantation; Heart transplantation; Systematic review; Meta-analysis

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Abstract
Background: This systematic review aimed to evaluate the clinical outcomes and cost-effectiveness of left
ventricular assist devices (LVADs) used as bridge to transplantation (BTT), compared to orthotopic heart
transplantation (OHT) without a bridge.
Method: Systematic searches were performed in electronic databases with available data extracted from text and
digitized figures. Meta-analysis of short and long-term term post-transplantation outcomes was performed with
summation of cost-effectiveness analyses.
Results: Twenty studies reported clinical outcomes of 4,575 patients (1,083 LVAD BTT and 3,492 OHT). Five
studies reported cost-effectiveness data on 837 patients (339 VAD BTT and 498 OHT). There was no difference
in long-term post-transplantation survival (HR 1.24, 95% CI 1.00 – 1.54), acute rejection (HR 1.10, 95% CI 0.93
– 1.30), or chronic rejection and cardiac allograft vasculopathy (HR 0.99, 95% CI 0.73 – 1.36). No differences
were found in 30-day post-operative mortality (OR 0.91, 95% CI 0.42 – 2.00), stroke (OR 1.64, 95% CI 0.43 –
6.27), renal failure (OR 1.43, 95% CI 0.58 – 3.54), bleeding (OR 1.56, 95% CI 0.78 – 3.13), or infection (OR
2.44, 95% CI 0.81 – 7.38). Three of the five studies demonstrated incremental cost-effectiveness ratios below the
acceptable maximum threshold. The total cost of VAD BTT ranged from $316,078 to $1,025,500, and OHT
ranged from $179,051 to $802,200.
Conclusion: LVADs used as BTT did not significantly alter post-transplantation long-term survival, rejection, and
post-operative morbidity. LVAD BTT may be cost-effective, particularly in medium and high-risk patients with
expected prolonged waiting times, renal dysfunction, and young patients.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Introduction
End-stage heart failure (ESHF) is a major global health issue that continues to rise in prevalence, and is a
significant contributor to health-care expenditure (1). Orthotopic heart transplantation (OHT) is the gold-standard
treatment for ESHF and improves patient survival and quality of life (2). However, the availability of heart donors
has failed to keep pace with rising demand for transplantation (3). The United Network for Organ Sharing
(UNOS) data demonstrated that there remains a significant rate of death while patients await a donor organ (4).
The use of a left ventricular assist device (LVAD) may improve survival and quality of life among ESHF patients
refractory to optimal medical management (5). First generation LVADs, including the HeartMate I and Novacor
N100, were primarily volume displacement devices, which pumped blood via a pulse generator, thus creating
pulsatile flow. Second generation devices, including HeartMate II, Jarvik 2000, and Micromed DeBakey, were
continuous axial flow pumps that resulted in non-pulsatile flow, with advantages of reduced size, improved
durability and efficiency. Third and the latest generation of LVADs, including the HeartMate III, HeartWare
HVAD, and DuraHeart, are distinguished by the use of a magnetically elevated impeller to create a contactless
bearing. Increasingly, these devices are used in ESHF patients for bridge to transplantation (BTT) to improve
survival until suitable donors are located. Due to the shortage of donor organs, there is mostly no alternative to
LVAD as bridge to transplantation in most European countries and increasingly in the United States. The impact
of LVADs on long-term post-transplantation outcomes remains unclear, and these devices carry a significant
associated cost (6). The present systematic review and meta-analysis aimed to evaluate the short and long-term
clinical outcomes and cost effectiveness of LVADs as BTT compared to OHT.
Methods
Search strategy
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (7),
electronic searches were performed using Ovid Medline, Pubmed, Cochrane Central Register of Controlled Trials
(CCTR), Cochrane Database of Systematic Reviews (CDSR), ACP Journal Club, and Database of Abstracts of

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Review of Effectiveness (DARE), from their dates of inception to March 2016. To achieve maximum sensitivity
of the search strategy, the terms “left ventricular assist device”, “bridge to transplantation”, “mechanical
assistance”, “orthotopic heart transplant”, “inotrope”, “heart failure”, “cost-effectiveness”, “cost-utility”,
“cost-benefit analysis”, “life-time cost”, “incremental cost-effectiveness ratio”, “quality adjusted life years”,
and “life years” were combined as both text keywords and exploded MeSH headings where possible. Two
authors (D.F.Z and M.S) performed the search independently, and any discrepancies were resolved by discussion.
The reference lists of all retrieved articles were reviewed for further identification of potentially relevant studies,
assessed using the inclusion and exclusion criteria.
Selection criteria
Eligible studies for the present systematic review were those that compared long-term post-transplantation
survival outcomes or economic evaluations of cost-effectiveness between patients who received an LVAD as
BTT, and those who underwent OHT without and LVAD as BTT (including patients that required intra-aortic
balloon pump support or extracorporeal membrane oxygenation prior to transplantation). All LVAD generations
were included in order to provide a comprehensive analysis and to maximise long-term outcomes available. For
the meta-analysis of mortality and morbidity, only studies comparing LVADs against OHT and reporting actuarial
survival rates were included. For the review of cost-effectiveness, only studies reporting incremental cost-
effectiveness ratios (ICERs) for LVADs compared to OHT were included. Studies that did not contain a
comparative group or report relevant outcomes as endpoints were excluded. When institutions published duplicate
studies with accumulating numbers of patients or increased lengths of follow-up, only the most complete reports
were included for quantitative assessment. All publications were limited to those involving human subjects.
Abstracts, case reports, conference presentations, editorials, reviews, and expert opinions were excluded.
Data Extraction and Critical Appraisal
All data were extracted from article texts, tables, and figures. Two investigators (D.F.Z and M.S) independently
reviewed each included article. Because quality scoring is controversial in meta-analyses of observational studies,

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
two reviewers (D.F.Z and M.S) independently appraised each article included in our analysis according to a
critical review checklist of the Dutch Cochrane Centre proposed by MOOSE (Supplementary Table 1) (8).
Discrepancies between the two investigators were resolved by discussion and consensus with the senior authors
(M.J.B and P.G.B).
Outcomes
The primary outcome was long-term post-transplantation survival in patients receiving LVAD BTT compared to
OHT. Secondary outcomes included long-term acute rejection, chronic rejection or cardiac allograft vasculopathy,
as well as 30-day post-operative mortality, stroke, renal failure, bleeding, and infection following transplantation.
Acute rejection was defined as high-grade cellular allograft rejection of minimum grade 3A or 3B detected by
endomyocardial biopsy according to the International Society for Heart & Lung Transplantation criteria (9-12).
Chronic rejection or cardiac allograft vasculopathy was defined as greater than 50% occlusion of graft coronary
arteries detected by post-transplantation coronary angiography (10-12). Post-operative stroke included all
cerebrovascular accidents diagnosed by imaging (13). Renal failure was defined as new onset renal impairment
following transplantation requiring haemodialysis (13). Bleeding was defined as post-transplantation
haemorrhagic complications requiring reoperation (13). Infection was defined as the development of deep sternal
infection or sepsis (14). All analysed outcomes included patients in United Network for Organ Sharing (UNOS)
status 1 and 2. Additional outcomes for analysis of cost-effectiveness included ICERs, total cost, and quality-
adjusted life years (QALYs) or life years (LYs) gained for VADs compared to OHT. The cost-effectiveness
threshold for VADs was set to $100,000 per QALY or LY, below which VADs are considered cost-effective and
thus worth paying for (15-17).
Statistical Analysis
Long-term clinical outcomes were assessed using meta-analysis techniques described previously, with the hazard
ratio (HR) used as a summary statistic to compare actuarial survival between groups (18, 19). Because not all
studies report hazard ratios and confidence intervals, long-term survival and rejection rates were extracted by

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
digitizing the Kaplan-Meier curves presented in the included studies, using DigitizeIt Version 2.1.3 (Köln,
Germany) and a spreadsheet developed by Tierney et al. (20). Aggregated Kaplan-Meier survival curves were
created using the mean weighted digitized coordinates in Microsoft Excel (Microsoft, Redmond, WA). Pooled
estimates and corresponding 95% confidence intervals (CI) were determined using inverse variance DerSimonian
and Laird random-effects models.
The reported incidence of post-operative outcomes were separately combined. Relative risk was chosen as a
summary statistic with both fixed and random effects models tested, and the later presented due to its more
conservative nature. The Mantel–Haenszel test was used to combine discrete data. Inverse variance-weighted
averages were used for continuous data and logarithmic odds ratios (OR). All P values were two-sided. Additional
tests include: χ2 to test heterogeneity between trials; I2 to estimate the percentage of total variation across studies
due to heterogeneity rather than chance. Heterogeneity is substantial when I2 > 50%. Analysis for potential
confounding factors was not performed due to the lack of raw data. Statistical analysis was conducted using
Review Manager Version 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen).
The reported outcomes for cost-effectiveness were separately extracted using techniques previously described
(21). All included cost-effectiveness studies employed Markov multi-state, decision-analytic, or novel decision-
analytic statistical modelling techniques for cost projections. These models accounted for medically
treated/waiting states, VAD-BTT/OHT states, post-VAD and post-OHT complications, and death. Modelling of
survival was based on previously published or national statistics, accounted for hemodynamic changes between
states (HF waiting state to BTT-VAD vs BTT-VAD patients to OHT state), adjusted risk of death after post-
VAD/OHT complications, and captured life-time costs and risks. In addition, the statistical models also took into
account device explantation, hypothetical worse case scenarios, and quality-of-life decrements. The total expense
of VAD BTT and OHT calculated by each model included the costs of initial hospitalization, device, procedures,
perioperative and long-term complications, repeat hospitalisations, physician fees, and drugs. All costs were
reported in US Dollars and converted according to base-year currency exchange rates if necessary. Costs were

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
derived from government or hospital data (15, 22). Time horizons of all studies varied from 20 years (15) to
lifetime (6, 22-24). Quality of life was measured using the EuroQOL 5 dimensions (EQ-5D) questionnaire (25).
Mean ICER values less than $100,000 (± $130) were deemed cost-effective (15). Pearson’s product moment
correlation coefficient (r) was used to assess the strength of association between total cost and QALYs gained for
both VAD BTT and OHT.
Results
Literature Search
A total of 1,874 studies were identified through six electronic database searches and from other sources including
reference lists (Figure 1). After exclusion of duplicate or irrelevant references, 86 potentially relevant articles
were retrieved. After application of inclusion and exclusion criteria, 25 relevant articles were included in the
present review (6, 10-15, 22-24, 26-40). Twenty of these studies, including 4,575 patients (1,083 receiving LVAD
BTT and 3,492 receiving OHT), were included in quantitative analysis of the post-operative and long-term
outcomes. Characteristics of these studies are summarized in Table 1. Inspection of the funnel plot did not show
significant asymmetry to suggest publication bias with the primary outcome selected (Supplementary Figure 1).
Five studies, including 837 base-case patients (339 receiving VAD BTT and 498 receiving OHT), were included
in quantitative analysis of cost-effectiveness data. Characteristics of these studies are summarised in Table 2. Full
model descriptions, assumptions, and cost data in each included study are reported in Supplementary Table 2.
Patient Characteristics
In the 1980s-2000s study period, patients receiving LVAD BTT were significantly younger (LVAD BTT
45.0±12.4, OHT 50.6±12.6, P <0.0001) and more likely to be male (89.7% vs 77.6%, P = 0.006). In the 1990s-
2000s study period, there was no significant difference between recipient age and gender. In the study period
starting from year 2000, recipient age was similar in both comparison arms but there were significantly more male
LVAD BTT recipients than those receiving OHT (80.5% vs 72.9%, P = 0.008). Overall, fewer LVAD BTT
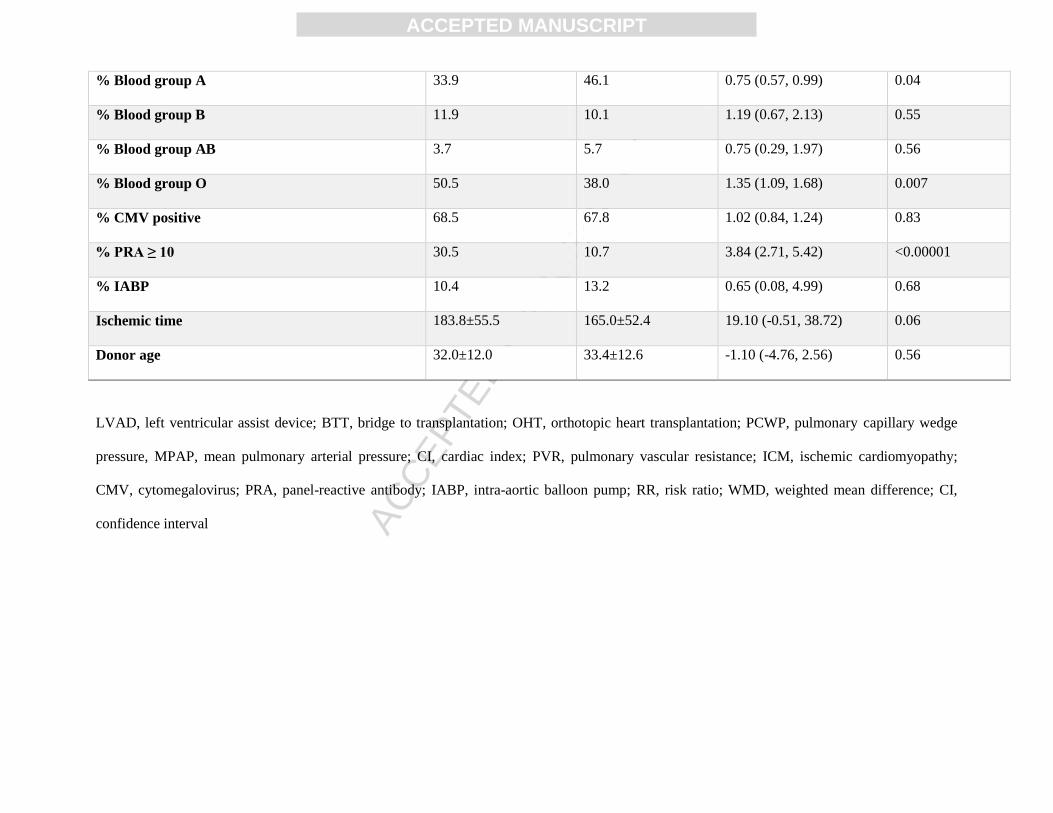
recipients had blood group A compared to OHT (33.9% vs 46.1%, P = 0.04), more had blood group type O

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
(50.5% vs 38.0%, P = 0.007), and more had percentage of panel-reactive antibody greater than 10 (30.5% vs
10.7%, P <0.00001). All other baseline characteristics were similar in both comparison arms, including
pulmonary capillary wedge pressure, mean pulmonary arterial pressure, cardiac index, pulmonary vascular
resistance, ischemic cardiomyopathy, African-American or Caucasian ethnicity, blood group B or AB, positive
test for cytomegalovirus, proportion of intra-aortic balloon pump support, donor organ ischemic time, and donor
age (Table 3). One study reported extra-corporal membrane oxygenation support for LVAD BTT (30%) and OHT
(5%) patients prior to transplantation(28). All patients in cost-effectiveness studies (not including reference or
hypothetical patients for statistical modelling) had equal characteristics at baseline, including recipient age,
proportion male, ischemic cardiomyopathy, implantable cardiac defibrillator or cardiac resynchronisation therapy,
and Caucasian ethnicity (Supplementary Table 3).
Long-Term Survival
Five studies compared long-term post-transplantation survival for study period 1980s-2000s (11, 12, 30, 35, 36).
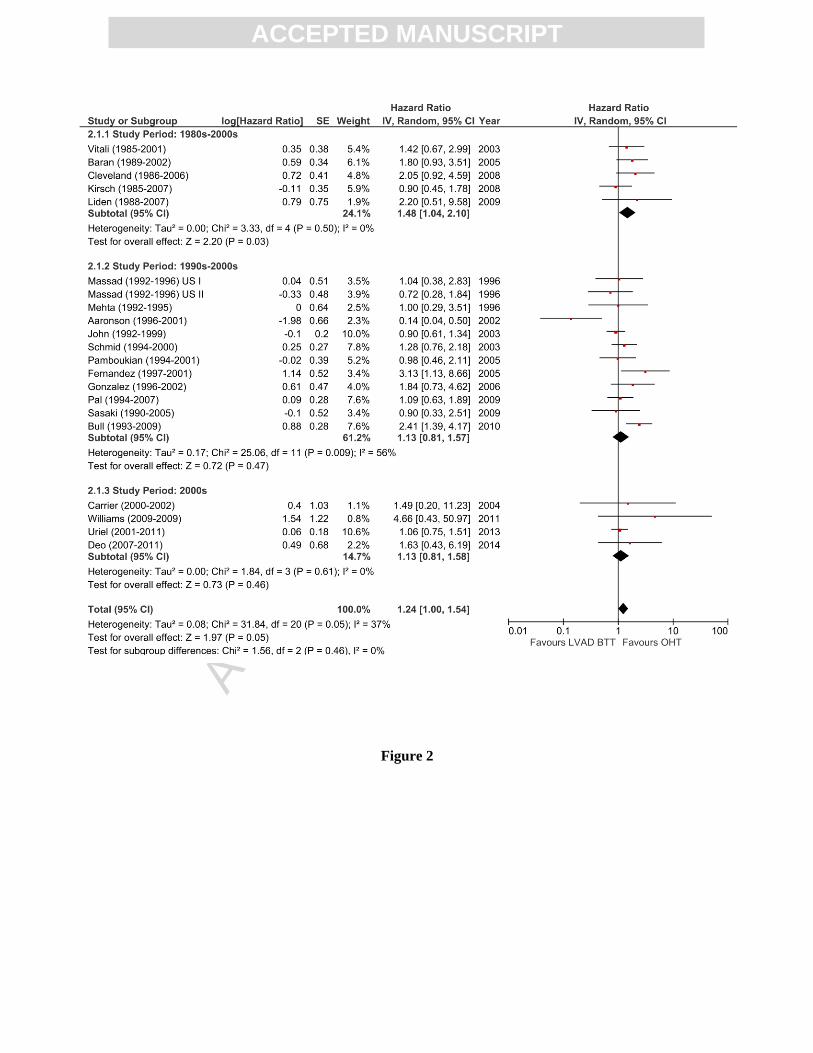
There was significantly reduced post-transplantation survival following LVAD BTT compared to OHT (HR 1.48,
95% CI 1.04 – 2.10, P = 0.03, I2 = 0%; Figure 2.1.1).
Eleven studies compared long-term post-transplantation survival for study period 1990s-2000s (10, 13, 26-29, 32-
34, 37, 38). There was no significant difference between LVAD BTT and OHT (HR 1.13, 95% CI 0.81 – 1.57;
Figure 2.1.2). There was substantial heterogeneity between the studies (I2 = 56%; heterogeneity P = 0.009).
Four studies compared long-term post-transplantation survival for study period 2000s (14, 31, 39, 40). There was
no significant difference between LVAD BTT and OHT (HR 1.13, 95% CI 0.81 – 1.58, I2 = 0%; Figure 2.1.3).
Overall, 20 studies compared long-term post-transplantation survival, including all study periods (10-14, 26-40).
The pooled HR demonstrated no significant difference (HR 1.24, 95% CI 1.00 – 1.54; Figure 2). There was
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
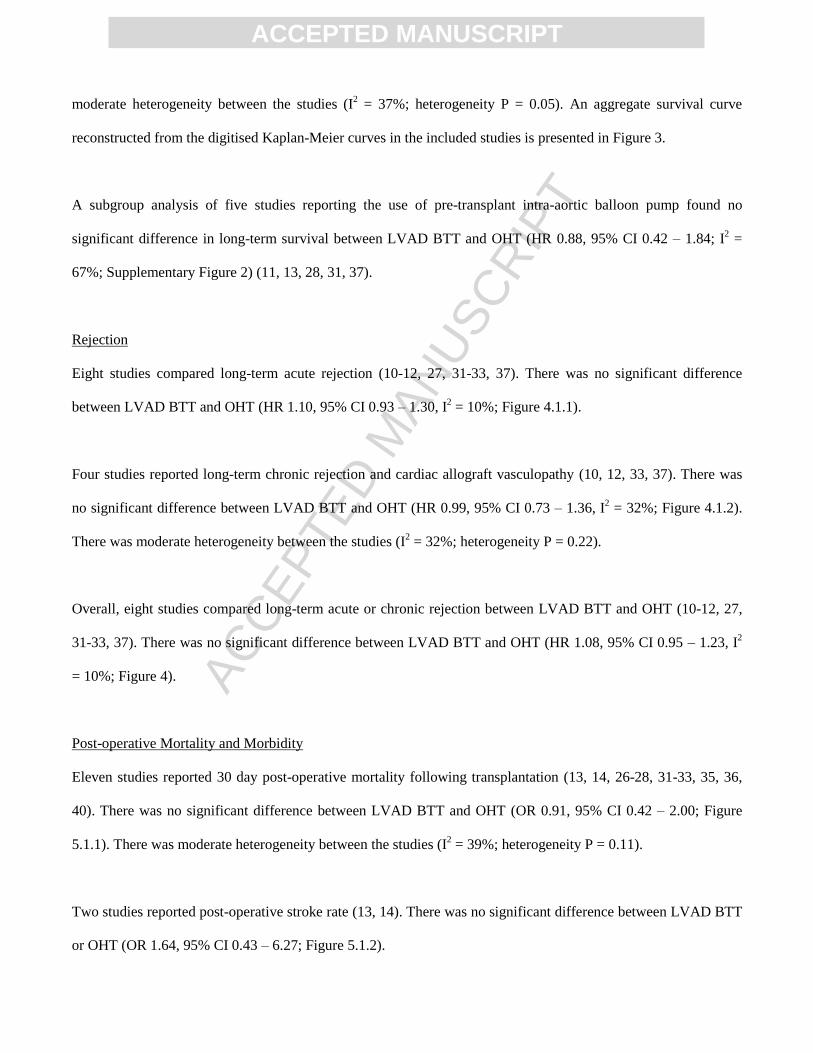
moderate heterogeneity between the studies (I2 = 37%; heterogeneity P = 0.05). An aggregate survival curve
reconstructed from the digitised Kaplan-Meier curves in the included studies is presented in Figure 3.
A subgroup analysis of five studies reporting the use of pre-transplant intra-aortic balloon pump found no
significant difference in long-term survival between LVAD BTT and OHT (HR 0.88, 95% CI 0.42 – 1.84; I2 =
67%; Supplementary Figure 2) (11, 13, 28, 31, 37).
Rejection
Eight studies compared long-term acute rejection (10-12, 27, 31-33, 37). There was no significant difference
between LVAD BTT and OHT (HR 1.10, 95% CI 0.93 – 1.30, I2 = 10%; Figure 4.1.1).
Four studies reported long-term chronic rejection and cardiac allograft vasculopathy (10, 12, 33, 37). There was
no significant difference between LVAD BTT and OHT (HR 0.99, 95% CI 0.73 – 1.36, I2 = 32%; Figure 4.1.2).
There was moderate heterogeneity between the studies (I2 = 32%; heterogeneity P = 0.22).
Overall, eight studies compared long-term acute or chronic rejection between LVAD BTT and OHT (10-12, 27,
31-33, 37). There was no significant difference between LVAD BTT and OHT (HR 1.08, 95% CI 0.95 – 1.23, I2
= 10%; Figure 4).
Post-operative Mortality and Morbidity
Eleven studies reported 30 day post-operative mortality following transplantation (13, 14, 26-28, 31-33, 35, 36,
40). There was no significant difference between LVAD BTT and OHT (OR 0.91, 95% CI 0.42 – 2.00; Figure
5.1.1). There was moderate heterogeneity between the studies (I2 = 39%; heterogeneity P = 0.11).
Two studies reported post-operative stroke rate (13, 14). There was no significant difference between LVAD BTT
or OHT (OR 1.64, 95% CI 0.43 – 6.27; Figure 5.1.2).

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Four studies reported post-operative renal failure (13, 14, 31, 40). There was no significant difference between
LVAD BTT or OHT (OR 1.43, 95% CI 0.58 – 3.54, I2 = 0%; Figure 5.1.3).
Four studies compared post-operative bleeding (13, 14, 26, 40). There was no significant difference between
LVAD BTT or OHT (OR 1.56, 95% CI 0.78 – 3.13, I2 = 0%; Figure 5.1.4).
Two studies reported post-operative infection rates (14, 40). There was no significant difference between LVAD
BTT or OHT (OR 2.44, 95% CI 0.81 – 7.38; Figure 5.1.5).
Cost-effectiveness
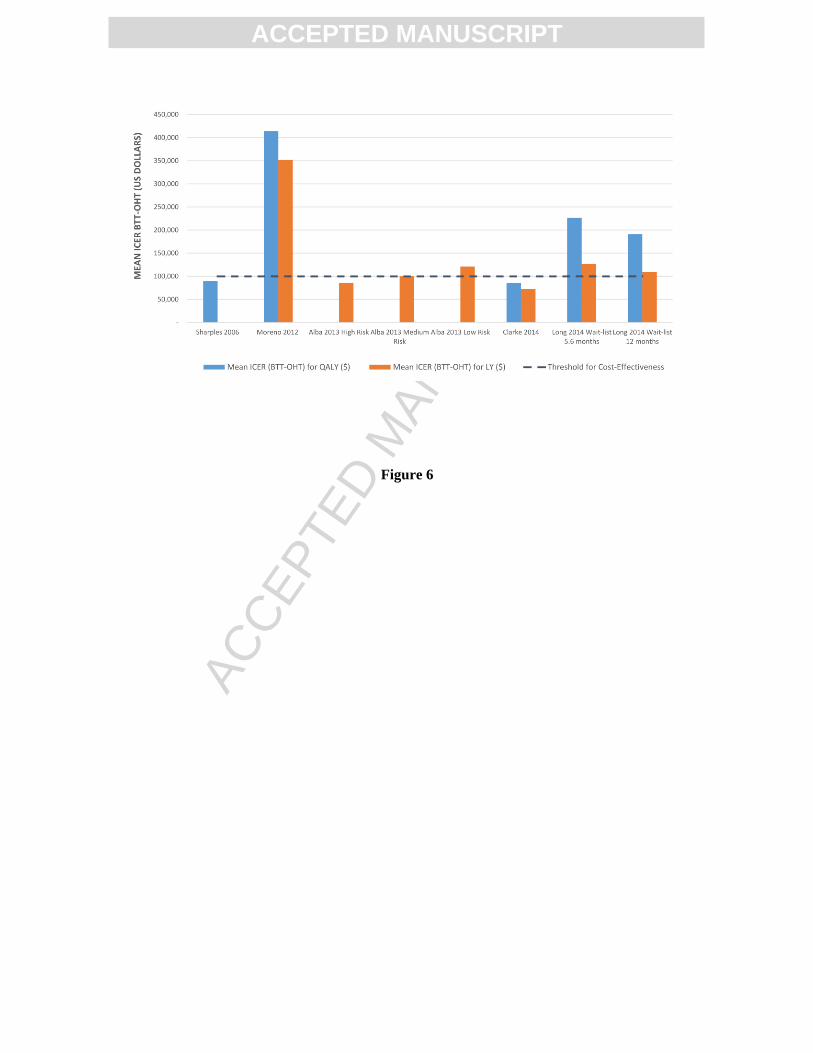
Overall, five studies reported ICERs (costs required to gain one additional QALY or LY) for VAD BTT
compared with OHT (6, 15, 22-24). In total, three of the five studies demonstrated ICERs consistent with cost-
effectiveness measured by QALY or LY (6, 15, 22) (Figure 6).
Four studies reported ICERs specifically to gain one additional QALY (6, 22-24). These ranged from $89,790 to
$414,275 per QALY gained. The results from two studies were below the threshold for cost-effectiveness
($100,000) with ICERs of $89,790 (22) and $84,963 (6) (Figure 6).
Four studies reported ICERs specifically to gain one additional LY (6, 15, 23, 24). These ranged from $72,475 to
$351,528 per LY gained. The results from two studies were below ICER threshold for cost-effectiveness: high
($85,899) and medium-risk ($100,128) VAD BTT patients analysed by Alba et al. (15), and patients reported by
Clarke et al. ($72,475) (6) (Figure 6).
Five studies reported the total cost of VAD BTT (range $316,078 to $1,025,500) and OHT (range $179,051 to
$802,200) (6, 15, 22-24). Mean QALYs gained was reported by four studies for VAD BTT (range 3.27 to 7.32
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
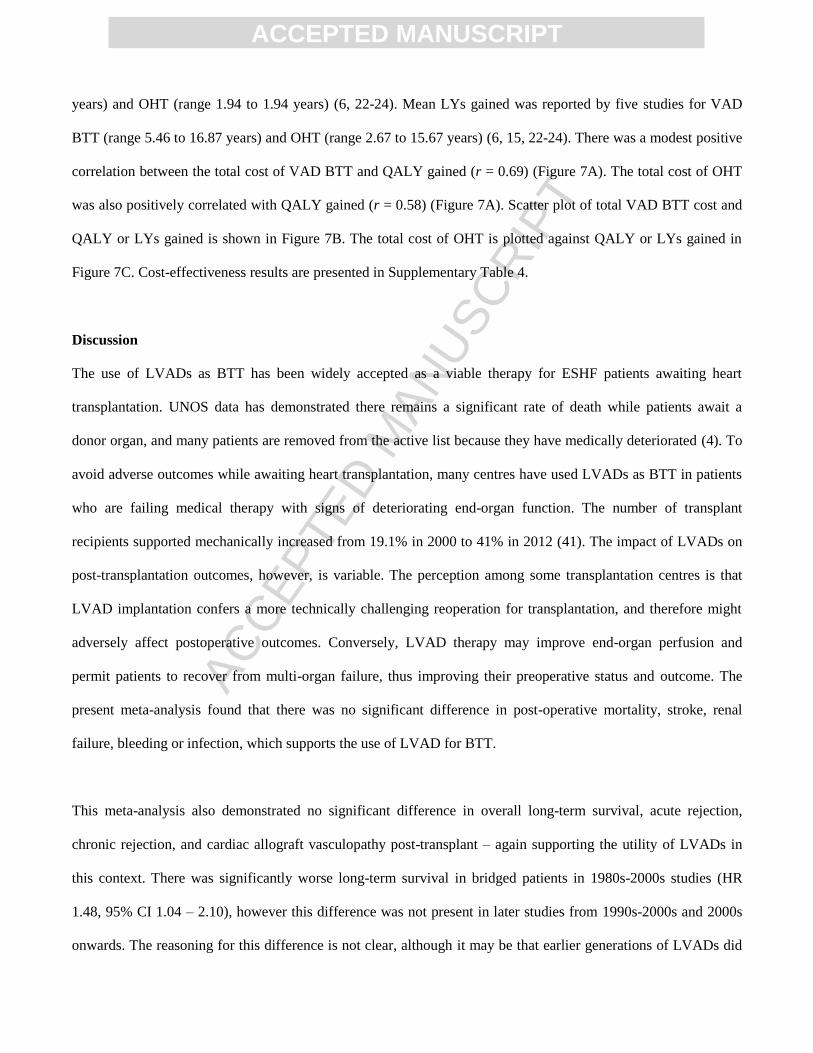
years) and OHT (range 1.94 to 1.94 years) (6, 22-24). Mean LYs gained was reported by five studies for VAD
BTT (range 5.46 to 16.87 years) and OHT (range 2.67 to 15.67 years) (6, 15, 22-24). There was a modest positive
correlation between the total cost of VAD BTT and QALY gained (r = 0.69) (Figure 7A). The total cost of OHT
was also positively correlated with QALY gained (r = 0.58) (Figure 7A). Scatter plot of total VAD BTT cost and
QALY or LYs gained is shown in Figure 7B. The total cost of OHT is plotted against QALY or LYs gained in
Figure 7C. Cost-effectiveness results are presented in Supplementary Table 4.
Discussion
The use of LVADs as BTT has been widely accepted as a viable therapy for ESHF patients awaiting heart
transplantation. UNOS data has demonstrated there remains a significant rate of death while patients await a
donor organ, and many patients are removed from the active list because they have medically deteriorated (4). To
avoid adverse outcomes while awaiting heart transplantation, many centres have used LVADs as BTT in patients
who are failing medical therapy with signs of deteriorating end-organ function. The number of transplant
recipients supported mechanically increased from 19.1% in 2000 to 41% in 2012 (41). The impact of LVADs on
post-transplantation outcomes, however, is variable. The perception among some transplantation centres is that
LVAD implantation confers a more technically challenging reoperation for transplantation, and therefore might
adversely affect postoperative outcomes. Conversely, LVAD therapy may improve end-organ perfusion and
permit patients to recover from multi-organ failure, thus improving their preoperative status and outcome. The
present meta-analysis found that there was no significant difference in post-operative mortality, stroke, renal
failure, bleeding or infection, which supports the use of LVAD for BTT.
This meta-analysis also demonstrated no significant difference in overall long-term survival, acute rejection,
chronic rejection, and cardiac allograft vasculopathy post-transplant – again supporting the utility of LVADs in
this context. There was significantly worse long-term survival in bridged patients in 1980s-2000s studies (HR
1.48, 95% CI 1.04 – 2.10), however this difference was not present in later studies from 1990s-2000s and 2000s
onwards. The reasoning for this difference is not clear, although it may be that earlier generations of LVADs did

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
not perform as well as later generations and clinical experience with these devices was lacking, which negatively
impacted outcomes. In addition, there was a selection bias toward younger patients receiving bridging in the
earlier studies (LVAD BTT 45.0±12.4 vs. OHT 50.6±12.6, P <0.0001), however this difference again disappeared
in later studies. Younger age may indicate more severe pathology, different aetiology, or a difference in one of the
pre-operative variables that was not measured. There were also a number of other differences in pre-operative
patient characteristics, including lower proportion of blood group A, higher proportion of blood group O, and high
proportion with RPA ≥ 10% (global allosensitisation), indicating the use of LVAD as BTT in a population where
finding a suitable donor is more difficult and waiting time prolonged (42). Nonetheless overall survival was not
significantly different, and survival in more recent studies using clinically relevant devices was not different, and
thus results are encouraging. This is especially important considering the poor condition of many patients at the
time of LVAD implantation and lack of treatment options.
Unfortunately, it was not possible with the current data to meta-analyse the effect of duration of LVAD support
on post-transplantation outcomes in detail. A sensitivity analysis that excluded studies with mean duration of
support >200 days did not change the outcomes significantly (HR 1.23, 95% CI 0.93 – 1.63). However, a number
of recent studies have found a negative impact on post-transplantation outcome with longer LVAD support times
(43, 44). Fukahara et al. found that continuous-flow LVAD support for two years or more resulted in reduced
survival at 30 days and two years post-transplantation, compared to patients who were supported for less than one
year and one to two years (44). Multi-variable analysis also identified duration as a significant predictor of
mortality at 2 years post-transplantation (HR 1.16; 95% CI 1.01-1.34) (44). Increased duration of pre-transplant
support also exposes patients to increased rates of adverse events related to the device, which may contribute to
reduced post-transplantation survival. This includes the adverse events related to continuous perfusion, including
vascular remodeling, disruption of neuroendocrine feedback, impaired platelet function, and higher rates of
bleeding (45, 46). However, the latest generation of devices have a number of design improvements aimed
specifically at reducing these complications, including artificial pulsatility, reduced haemolysis and thrombosis,

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
and improved biocompatibility (47), which may facilitate longer support times without negative effects on post-
transplantation outcomes.
A strategy of earlier LVAD implantation in patients on the donor waiting list may also prevent some of the
attrition currently observed and improve functional status before transplantation. In fact, there has been a decrease
in the number of patients transplanted in the first year of bridging, from 48% during a multicentre clinical trial to
39% during the post-trial period (48). The results from a study using INTERMACS showed that following the
approval of the Thoratec HeartMate II as BTT in the US, one-year pre-transplantation survival increased from
73% in 2009 to 85% in 2011 (49). Other studies have shown that early LVAD implantation also reduces
complications including bleeding and post-implantation right ventricular failure (50, 51), improves survival
particularly in elderly patients (52), and improves functional status and quality of life (53). As such, further
studies are required to determine the optimal device and timing of transplantation in BTT patients if they are to be
performed in an increasingly elective setting.
The development of minimally invasive LVAD operative techniques will also influence patient selection and
post-transplantation outcomes. Some newer devices allow for intra-pericardial placement and no longer require
creating a ‘pump pocket’, allowing for less invasive techniques and even off-pump insertion (54). One strategy is
to combine a left anterolateral thoracotomy for pump insertion, with an upper hemi-sternotomy or second
intercostal thoracotomy for outflow graft anastomosis. These approaches have particular benefits in BTT patients:
they preserve the sternum for later transplantation, reduce the development of adhesions and makes explanation
easier, and in patients with previous coronary artery bypass grafting reduces risk of damage to the grafts. The
disadvantage of this technique however is the difficulty associated with smaller access to the left ventricular apex
and ascending aorta, and difficulty with tunnelling the outflow graft. Nonetheless, these minimally invasive
approaches continue to improve outcomes and enable procedures in higher risk patients.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
With recent improvements in LVAD technology and ongoing debates about early implantation, there is increasing
focus on its cost-effectiveness. An evaluation of the United States National Inpatient Sample from 2005 to 2009
revealed marginal increase in OHT while the rate of LVAD implantation nearly tripled (55). During this period,
the mean cost per patient increased 17% for LVAD and 40% for OHT. The cumulative LVAD cost also increased
232% (from USD $143 million to $479 million) (55). With an ICER threshold of $100,000, three of the five
studies in our review demonstrated that LVAD BTT may be cost-effective in patients who do successfully receive
a transplant. However, there were significant variations in reported ICER values. Although base year costs and
currency exchange rates were controlled for, geographical, device, and hospitalization cost differences may have
contributed to the observed variations in ICER. The Markov model economic analysis performed by Alba et al.
(15) demonstrated that while VAD BTT improved survival at increased costs compared to non-bridged patients,
bridging therapy may be cost-effective in certain populations: medium and high-risk patients with expected
prolonged waiting times for transplantation, patients with existing renal dysfunction, those with a high risk of
post-transplantation complications, and young patients. This finding was not replicated by a semi-Markov
analysis of the British National Health Service (NHS) Blood and Transplant Database, in which continuous
LVAD BTT delivered greater quality-adjusted life years at higher costs than medical management and was not
found to be cost-effective (6). In a separate NHS database analysis, the newer HeartWare LVAD was found to be
more cost-effective than HeartMate II for BTT (56). The impact of newer devices on survival outcomes and cost-
effectiveness remains an important question and deserves further investigation.
Limitations
The rapidly evolving technology of LVADs and the use of multiple device generations in later studies may have
affected the results. Based on the available studies, the primary end-point was able to be separated into different
time periods, which did demonstrate a difference. A proportion of LVAD BTT and OHT patients were supported
by intra-aortic balloon pump (10.4% vs 13.2%) or ECMO (30% vs 5%) and the results should be interpreted with
caution due to potentially worse OHT outcomes following mechanical support (57). In addition, all studies that
met the inclusion criteria were observational, and consequently confounding bias may have affected the results.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Accuracy of the digital extraction and Kaplan-Meier curve reconstruction using the DigitizeIt software depends
on the quality of the initial input image and the level of information provided by the publication. Unadjusted
summary estimates were used for meta-analysis and confounders could not be ruled out. There was a moderate
amount of heterogeneity in some outcomes, and these results should be interpreted with caution.
Cost-effectiveness estimates were performed using different statistical modelling techniques and thus need to be
interpreted with caution. These modelling techniques are not applicable in some countries with different LVAD
funding models, and thus limits their relevance. Time horizon for cost estimates were long-term or life-time.
Therefore, incremental cost estimates may vary depending on device technology, patient survival, and quality
adjusted life years gained. The ICER threshold was selected based on current evidence from developed countries
but may vary depending on a country’s health care system and allocation of available resources.
Conclusions
LVADs used as BTT in current practice do not significantly alter post-transplantation long-term survival,
rejection, and post-operative morbidity, and are thus a viable therapy in this context. More data is required to
determine the effect of duration of LVAD support on post-transplantation outcomes, and the optimal timing of
LVAD implantation in patients with ESHF. In patients who do receive a transplant, some studies have
demonstrated that LVADs used as BTT may be cost-effective, depending on the accepted ICER threshold. This is
particularly relevant for medium and high-risk patients with expected prolonged waiting times for transplantation,
patients with existing renal dysfunction, those with a high risk of post-transplantation complications, and young
patients.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
References
1. Bui AL, Horwich TB, Fonarow GC. Epidemiology and risk profile of heart failure. Nature reviews
Cardiology. 2011;8(1):30-41.
2. Deng MC. Cardiac transplantation. Heart. 2002;87(2):177-84.
3. McManus RP, O'Hair DP, Beitzinger JM, Schweiger J, Siegel R, Breen TJ, et al. Patients who die awaiting
heart transplantation. The Journal of heart and lung transplantation : the official publication of the International
Society for Heart Transplantation. 1993;12(2):159-71; discussion 72.
4. Karamlou T, Hirsch J, Welke K, Ohye RG, Bove EL, Devaney EJ, et al. A United Network for Organ Sharing
analysis of heart transplantation in adults with congenital heart disease: outcomes and factors associated with
mortality and retransplantation. The Journal of thoracic and cardiovascular surgery. 2010;140(1):161-8.
5. Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW, Dembitsky W, et al. Long-Term Use of
a Left Ventricular Assist Device for End-Stage Heart Failure. New England Journal of Medicine.
2001;345(20):1435-43.
6. Clarke A, Pulikottil-Jacob R, Connock M, Suri G, Kandala NB, Maheswaran H, et al. Cost-effectiveness of
left ventricular assist devices (LVADs) for patients with advanced heart failure: analysis of the British NHS bridge
to transplant (BTT) program. International journal of cardiology. 2014;171(3):338-45.
7. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-
analyses: the PRISMA statement. BMJ. 2009;339.
8. Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational
studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology
(MOOSE) group. JAMA. 2000;283(15):2008-12.
9. Billingham ME, Cary NR, Hammond ME, Kemnitz J, Marboe C, McCallister HA, et al. A working
formulation for the standardization of nomenclature in the diagnosis of heart and lung rejection: Heart Rejection
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Study Group. The International Society for Heart Transplantation. The Journal of heart transplantation.
1990;9(6):587-93.
10. John R, Lietz K, Schuster M, Naka Y, Rao V, Mancini DM, et al. Immunologic sensitization in recipients of
left ventricular assist devices. The Journal of thoracic and cardiovascular surgery. 2003;125(3):578-91.
11. Baran DA, Gass AL, Galin ID, Zucker MJ, Arroyo LH, Goldstein DJ, et al. Lack of sensitization and
equivalent post-transplant outcomes with the Novacor left ventricular assist device. The Journal of heart and
lung transplantation : the official publication of the International Society for Heart Transplantation.
2005;24(11):1886-90.
12. Kirsch L, Timmermans T, Van Caenegem O, Gurne O, Noirhomme P, Jacquet LM, et al. Allosensitization in
bridge to transplant Novacor left ventricular assist device patients: analysis of long-term outcomes with regard
to acute rejection and chronic allograft vasculopathy. European journal of cardio-thoracic surgery : official
journal of the European Association for Cardio-thoracic Surgery. 2008;34(2):268-74; discussion 74.
13. Pal JD, Piacentino V, Cuevas AD, Depp T, Daneshmand MA, Hernandez AF, et al. Impact of left ventricular
assist device bridging on posttransplant outcomes. The Annals of thoracic surgery. 2009;88(5):1457-61;
discussion 61.
14. Williams ML, Trivedi JR, McCants KC, Prabhu SD, Birks EJ, Oliver L, et al. Heart transplant vs left
ventricular assist device in heart transplant-eligible patients. The Annals of thoracic surgery. 2011;91(5):1330-3;
discussion 3-4.
15. Alba AC, Alba LF, Delgado DH, Rao V, Ross HJ, Goeree R. Cost-effectiveness of ventricular assist device
therapy as a bridge to transplantation compared with nonbridged cardiac recipients. Circulation.
2013;127(24):2424-35.
16. Farley TA. When Is It Ethical to Withhold Prevention? New England Journal of Medicine.
2016;374(14):1303-6.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
17. Eichler HG, Kong SX, Gerth WC, Mavros P, Jonsson B. Use of cost-effectiveness analysis in health-care
resource allocation decision-making: how are cost-effectiveness thresholds expected to emerge? Value in health
: the journal of the International Society for Pharmacoeconomics and Outcomes Research. 2004;7(5):518-28.
18. Zhao DF, Seco M, Wu JJ, Edelman JB, Wilson MK, Vallely MP, et al. Mechanical Versus Bioprosthetic
Aortic Valve Replacement in Middle-Aged Adults: A Systematic Review and Meta-Analysis. The Annals of
thoracic surgery. 2016.
19. Liu Z, Rich B, Hanley JA. Recovering the raw data behind a non-parametric survival curve. Systematic
Reviews. 2014;3(1):1-10.
20. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary
time-to-event data into meta-analysis. Trials. 2007;8:16-.
21. Indraratna P, Ang SC, Gada H, Yan TD, Manganas C, Bannon P, et al. Systematic review of the cost-
effectiveness of transcatheter aortic valve implantation. The Journal of thoracic and cardiovascular surgery.
2014;148(2):509-14.
22. Sharples LD, Dyer M, Cafferty F, Demiris N, Freeman C, Banner NR, et al. Cost-effectiveness of
ventricular assist device use in the United Kingdom: results from the evaluation of ventricular assist device
programme in the UK (EVAD-UK). The Journal of heart and lung transplantation : the official publication of the
International Society for Heart Transplantation. 2006;25(11):1336-43.
23. Moreno SG, Novielli N, Cooper NJ. Cost-effectiveness of the implantable HeartMate II left ventricular
assist device for patients awaiting heart transplantation. Journal of Heart and Lung Transplantation.
2012;31(5):450-8.
24. Long EF, Swain GW, Mangi AA. Comparative survival and cost-effectiveness of advanced therapies for
end-stage heart failure. Circulation Heart failure. 2014;7(3):470-8.
25. Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol Group. Annals of medicine.
2001;33(5):337-43.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
26. Massad MG, McCarthy PM, Smedira NG, Cook DJ, Ratliff NB, Goormastic M, et al. Does successful
bridging with the implantable left ventricular assist device affect cardiac transplantation outcome? The Journal
of thoracic and cardiovascular surgery. 1996;112(5):1275-81; discussion 82-3.
27. Mehta SM, Boehmer JP, Pae WE, Jr., Aufiero TX, Davis D, Pierce WS. Bridging to transplant. Equal
extended survival for patients undergoing LVAD support when compared with long-term medical management.
ASAIO journal (American Society for Artificial Internal Organs : 1992). 1996;42(5):M406-10.
28. Aaronson KD, Eppinger MJ, Dyke DB, Wright S, Pagani FD. Left ventricular assist device therapy improves
utilization of donor hearts. Journal of the American College of Cardiology. 2002;39(8):1247-54.
29. Schmid C, Welp H, Klotz S, Baba HA, Wilhelm MJ, Scheld HH. Outcome of patients surviving to heart
transplantation after being mechanically bridged for more than 100 days. The Journal of heart and lung
transplantation : the official publication of the International Society for Heart Transplantation. 2003;22(9):1054-
8.
30. Vitali E, Lanfranconi M, Bruschi G, Russo C, Colombo T, Ribera E. Left ventricular assist devices as bridge
to heart transplantation: The Niguarda Experience. Journal of cardiac surgery. 2003;18(2):107-13.
31. Carrier M, Perrault LP, Bouchard D, Pellerin M, Racine N, White M, et al. Effect of left ventricular assist
device bridging to transplantation on donor waiting time and outcomes in Canada. The Canadian journal of
cardiology. 2004;20(5):501-4.
32. Fernandez FG, Jaramillo A, Ewald G, Rogers J, Pasque MK, Mohanakumar T, et al. Blood transfusions
decrease the incidence of acute rejection in cardiac allograft recipients. The Journal of heart and lung
transplantation : the official publication of the International Society for Heart Transplantation. 2005;24(7
Suppl):S255-61.
33. Pamboukian SV, Costanzo MR, Dunlap S, Rayburn B, Westfall AO, You ZY, et al. Relationship between
bridging with ventricular assist device on rejection after heart transplantation. The Journal of heart and lung
transplantation : the official publication of the International Society for Heart Transplantation. 2005;24(3):310-5.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
34. Gonzalez-Stawinski GV, Cook DJ, Chang AS, Banbury MK, Navia JL, Hoercher K, et al. Ventricular assist
devices and aggressive immunosuppression: looking beyond overall survival. The Journal of heart and lung
transplantation : the official publication of the International Society for Heart Transplantation. 2006;25(6):613-8.
35. Cleveland JC, Jr., Grover FL, Fullerton DA, Campbell DN, Mitchell MB, Lindenfeld J, et al. Left ventricular
assist device as bridge to transplantation does not adversely affect one-year heart transplantation survival. The
Journal of thoracic and cardiovascular surgery. 2008;136(3):774-7.
36. Liden H, Haraldsson A, Ricksten SE, Kjellman U, Wiklund L. Does pretransplant left ventricular assist
device therapy improve results after heart transplantation in patients with elevated pulmonary vascular
resistance? European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-
thoracic Surgery. 2009;35(6):1029-34; discussion 34-5.
37. Sasaki H, Mitchell JD, Jessen ME, Lavingia B, Kaiser PA, Comeaux A, et al. Bridge to heart transplantation
with left ventricular assist device versus inotropic agents in status 1 patients. Journal of cardiac surgery.
2009;24(6):756-62.
38. Bull DA, Reid BB, Selzman CH, Mesley R, Drakos S, Clayson S, et al. The impact of bridge-to-transplant
ventricular assist device support on survival after cardiac transplantation. The Journal of thoracic and
cardiovascular surgery. 2010;140(1):169-73.
39. Uriel N, Jorde UP, Woo Pak S, Jiang J, Clerkin K, Takayama H, et al. Impact of long term left ventricular
assist device therapy on donor allocation in cardiac transplantation. The Journal of heart and lung
transplantation : the official publication of the International Society for Heart Transplantation. 2013;32(2):188-
95.
40. Deo SV, Sung K, Daly RC, Shah IK, Altarabsheh SE, Stulak JM, et al. Cardiac transplantation after bridged
therapy with continuous flow left ventricular assist devices. Heart, lung & circulation. 2014;23(3):224-8.
41. Lund LH, Edwards LB, Kucheryavaya AY, Benden C, Christie JD, Dipchand AI, et al. The registry of the
International Society for Heart and Lung Transplantation: thirty-first official adult heart transplant report--2014;

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
focus theme: retransplantation. The Journal of heart and lung transplantation : the official publication of the
International Society for Heart Transplantation. 2014;33(10):996-1008.
42. Drakos SG, Stringham JC, Long JW, Gilbert EM, Fuller TC, Campbell BK, et al. Prevalence and risks of
allosensitization in HeartMate left ventricular assist device recipients: the impact of leukofiltered cellular blood
product transfusions. The Journal of thoracic and cardiovascular surgery. 2007;133(6):1612-9.
43. Takeda K, Takayama H, Kalesan B, Uriel N, Colombo PC, Jorde UP, et al. Outcome of cardiac
transplantation in patients requiring prolonged continuous-flow left ventricular assist device support. The
Journal of heart and lung transplantation : the official publication of the International Society for Heart
Transplantation. 2015;34(1):89-99.
44. Fukuhara S, Takeda K, Polanco AR, Takayama H, Naka Y. Prolonged continuous-flow left ventricular assist
device support and posttransplantation outcomes: A new challenge. The Journal of thoracic and cardiovascular
surgery. 2016;151(3):872-80.e5.
45. Crow S, John R, Boyle A, Shumway S, Liao K, Colvin-Adams M, et al. Gastrointestinal bleeding rates in
recipients of nonpulsatile and pulsatile left ventricular assist devices. The Journal of thoracic and cardiovascular
surgery. 2009;137(1):208-15.
46. Hong KN, Iribarne A, Yang J, Ramlawi B, Takayama H, Naka Y, et al. Do posttransplant outcomes differ in
heart transplant recipients bridged with continuous and pulsatile flow left ventricular assist devices? The Annals
of thoracic surgery. 2011;91(6):1899-906.
47. Netuka I, Sood P, Pya Y, Zimpfer D, Krabatsch T, Garbade J, et al. Fully Magnetically Levitated Left
Ventricular Assist System for Treating Advanced HF: A Multicenter Study. Journal of the American College of
Cardiology. 2015;66(23):2579-89.
48. John R, Naka Y, Smedira NG, Starling R, Jorde U, Eckman P, et al. Continuous flow left ventricular assist
device outcomes in commercial use compared with the prior clinical trial. The Annals of thoracic surgery.
2011;92(4):1406-13; discussion 13.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
49. Starling RC, Naka Y, Boyle AJ, Gonzalez-Stawinski G, John R, Jorde U, et al. Results of the post-U.S. Food
and Drug Administration-approval study with a continuous flow left ventricular assist device as a bridge to heart
transplantation: a prospective study using the INTERMACS (Interagency Registry for Mechanically Assisted
Circulatory Support). Journal of the American College of Cardiology. 2011;57(19):1890-8.
50. Schmid C, Deng M, Hammel D, Weyand M, Loick HM, Scheld HH. Emergency versus elective/urgent left
ventricular assist device implantation. The Journal of heart and lung transplantation : the official publication of
the International Society for Heart Transplantation. 1998;17(10):1024-8.
51. Tsiouris A, Morgan JA, Nemeh HW, Hodari A, Shah R, Brewer RJ, et al. Does elective or emergent
operative status influence outcomes in patients undergoing implantation of left ventricular assist devices? The
heart surgery forum. 2014;17(2):E64-72.
52. Stepanenko A, Potapov EV, Jurmann B, Lehmkuhl HB, Dandel M, Siniawski H, et al. Outcomes of elective
versus emergent permanent mechanical circulatory support in the elderly: a single-center experience. The
Journal of heart and lung transplantation : the official publication of the International Society for Heart
Transplantation. 2010;29(1):61-5.
53. Estep JD, Starling RC, Horstmanshof DA, Milano CA, Selzman CH, Shah KB, et al. Risk Assessment and
Comparative Effectiveness of Left Ventricular Assist Device and Medical Management in Ambulatory Heart
Failure Patients: Results From the ROADMAP Study. Journal of the American College of Cardiology.
2015;66(16):1747-61.
54. Maltais S, Davis ME, Haglund N. Minimally invasive and alternative approaches for long-term LVAD
placement: the Vanderbilt strategy. Annals of Cardiothoracic Surgery. 2014;3(6):563-9.
55. Mulloy DP, Bhamidipati CM, Stone ML, Ailawadi G, Kron IL, Kern JA. Orthotopic heart transplant versus
left ventricular assist device: a national comparison of cost and survival. The Journal of thoracic and
cardiovascular surgery. 2013;145(2):566-73; discussion 73-4.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
56. Pulikottil-Jacob R, Suri G, Connock M, Kandala NB, Sutcliffe P, Maheswaran H, et al. Comparative cost-
effectiveness of the HeartWare versus HeartMate II left ventricular assist devices used in the United Kingdom
National Health Service bridge-to-transplant program for patients with heart failure. The Journal of heart and
lung transplantation : the official publication of the International Society for Heart Transplantation.
2014;33(4):350-8.
57. Gonzalez-Vilchez F, Segovia Cubero J, Almenar L, Crespo-Leiro MG, Arizon JM, Villa A, et al. Spanish
Heart Transplantation Registry. 26th Official Report of the Spanish Society of Cardiology Working Group on
Heart Failure and Heart Transplantation (1984-2014). Revista espanola de cardiologia (English ed).
2015;68(11):1008-21.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure Legends
Figure 1. PRISMA flow chart of search strategy
Figure 2. Forest plot of overall long-term post-transplantation survival associated with LVAD BTT compared to
OHT.
Figure 3. Overall Kaplan–Meier survival curves based on reconstructed individual study data. (A) Aggregated
survival curves for LVAD BTT compared with OHT. (B) Long-term post-transplantation survival of the LVAD
BTT cohort, reconstructed from 1083 patients. (C) Long-term post-transplantation survival of the OHT cohort,
reconstructed from 3492 patients.
Figure 4. Forest plot of overall long-term post-transplantation acute and chronic rejection with LVAD BTT
compared to OHT.
Figure 5. Forest plot of post-operative mortality and morbidity following transplantation with LVAD BTT
compared to OHT.
Figure 6. Mean ICER (BTT-OHT) for QALY and LY compared to threshold for cost-effectiveness.
Figure 7. Scatter plot of (A) total cost of VAD BTT or OHT per QALY gained, (B) total cost of VAD BTT per
QALY or LY gained, and (C) total cost of OHT per QALY or LY gained.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 1
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 2

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 3

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 4

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 5
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 6

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Figure 7

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 1. Study characteristics for assessment of post-operative and long-term outcomes in patients receiving LVAD bridge-to-transplantation vs.
orthotopic heart transplantation.
First
Author
Year Study Period Country N
LVAD
BTT
N OHT Device Type Mean
Support
Duration
(Days)
Maximum
Follow-up
(Years)
Study
Design
Massad [26] 1996 1992-1996 USA 53 203 Heartmate 72 (median) 3 OS, R
Mehta [27] 1996 1992-1995 USA 19 73 Pierce-Donachy, Heartmate NR 2 OS, R
Aaronson
[28]
2002 1996-2001 USA 66 38 Heartmate pneumatic NR 5 OS, R
John [10] 2003 1992-1999 USA 105 416 NR 94±51 8 OS, R
Schmid [29] 2003 1994-2000 Germany 41 146 Novacor, Heartmate,
DeBakey, Thoratec
215±86 7 OS, R
Vitali [30] 2003 1985-2001 Italy 53 501 Novacor, DeBakey 84 ± 168 17 OS, R
Carrier [31] 2004 2000-2002 Canada 13 20 Thoratec 17±19 1 OS, R
Baran [11] 2005 1989-2002 USA 26 220 Novacor 78±71 10 OS, R
Fernandez
[32]
2005 1997-2001 USA 15 67 Novacor 174 (4-497) 4.1 OS, R
Pamboukian 2005 1994-2001 USA 48 50 Heartmate 87 (3-493) 6.8 OS, R

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
[33]
Gonzalez-
Stawinski
[34]
2006 1996-2002 USA 125 113 Heartmate, Novacor,
Thoratec, DeBakey, Jarvik
110 (1-1030) 8 OS, R
Cleveland
[35]
2008 1986-2006 USA 23 294 Heartmate VE, XVE 165±122 19 OS, R
Kirsch [12] 2008 1985-2007 Belgium 30 318 Novacor 172.3±111.1 10 OS, R
Liden [36] 2009 1988-2007 Sweden 11 22 Heartmate VE, DeBakey,
Jarvik, VentrAssist
239 (24-1002) 4 OS, R
Pal [13] 2009 1994-2007 USA 86 173 Pulsatile-flow device,
continuous-flow device
59±32 8.3 OS, R
Sasaki [37] 2009 1990-2005 USA 31 149 Heartmate pneumatic,
vented-electric
103±91 5 OS, R
Bull [38] 2010 1993-2009 USA 45 156 Heartmate I, II NR 15 OS, R
Williams
[14]
2011 2009-2009 USA 29 13 Continuous-flow LVAD 116±143 1 OS, R
Uriel [39] 2013 2001-2011 USA 227 451 HeartMate I and II,
DuraHeart, DeBakey,
Toyobo, VentrAssist
208±199 10 OS, R

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Deo [40] 2014 2007-2011 USA 37 69 Heartmate II, Jarvik,
VentrAssist, DuraHeart
227 (153-328) 5 OS, R
LVAD, left ventricular assist device; BTT, bridge to transplantation; OHT, orthotopic heart transplantation; OS, observational study; R,
retrospective; RS, randomized study; P, prospective; NR, not reported

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 2. Study characteristics for assessment of cost-effectiveness in patients receiving VAD bridge-to-transplantation vs. orthotopic heart
transplantation.
First
Author
Year Country Institution/
Database
Device Analysis Time-
Horizon
N Currency conversion
BTT OHT
Sharples
[22]
2006 UK EVAD-UK Heartmate VE,
Thoratec,
Multi-state Markov
modela, b
Life-time 70 71 1 £ = US$1.8182
Moreno
[23]
2012 UK EVAD-UK HeartMate II Multistate
probabilistic
Markov modela, c, d
Life-time 70 71 1 £ = US$1.6
Alba
[15]
2013 Canada Toronto
General
Hospital
HeartMate II,
HeartWare,
DuraHeart
Decision analytic
Markov modele
20 years 34 120 Estimated US$1 =
CDN$0.989f
Clarke
[6]
2014 UK NHS BTT
Program
HeartWare
HLVAD, Thoratec
HeartMate II,
Jarvik 2000
FlowMaker,
Micromed
HeartAssist
Semi-Markov
multi-state modela
Life-time 235 307 Estimated 1 £ = US$1.6g

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Longg
[24]
2014 USA NR NR Novel decision-
analytic, state-
transition modela, h
Life-time 20000
simulated
patients
NR
aConstant hazard rate assumed for analysis in statistical model;
bcomparative data taken from concurrent, hospitalized inotrope-dependent or
urgent listed transplant candidates and a hypothetical worst-case scenario (all VAD-eligible patients die within 30 days in the absence of VADs);
cestimates of survival for LVAD group obtained from Pagani et al.;
dcomparative survival data taken from US Scientific Registry of Transplant
Recipients 2000-2005, ecomparison data included UNOS database, International Society of Heart and Lung Transplantation registry (ISHLT),
INTERMACS, the United Kingdom database, and a systematic literature review; faverage 2011 US Dollar (noon) exchange rate from Bank of
Canada; gcurrency exchange value provided by Moreno et al.;
gonly heart transplant eligible patients were included for this systematic review;
hcontemporary survival rates for LVAD patients were obtained from INTERMACS, OHT survival from ISHLT
LVAD, left ventricular assist device; BTT, bridge to transplantation; OHT, orthotopic heart transplantation; NR, not reported

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Table 3. Baseline characteristics for assessment of post-operative and long-term outcomes in patients receiving LVAD bridge-to-transplantation
vs. orthotopic heart transplantation.
Baseline parameter LVAD BTT OHT
RR or WMD
(95% CI)
Overall
P-value
Recipient age (years) 50.0±13.2 50.7±12.7 -1.84 (-3.16, -0.52) 0.006
Study Period 1980s-2000s 45.0±12.4 50.6±12.6 -5.21 (-7.75, -2.68) <0.0001
Study Period 1990s-2000s 49.4±14.0 50.2±13.2 -1.12 (-2.58, 0.34) 0.13
Study Period 2000s 52.2±12.0 52.0±11.9 -0.73 (3.65, 2.18) 0.62
% Male 82.1 76.1 1.11 (1.04, 1.18) 0.002
Study Period 1980s-2000s 89.7 77.6 1.17 (1.00, 1.37) 0.006
Study Period 1990s-2000s 81.8 76.2 1.08 (0.99, 1.18) 0.07
Study Period 2000s 80.5 72.9 1.10 (1.03, 1.18) 0.008
PCWP (mmHg) 20.8±7.6 24.0±7.5 -0.07 (-3.98, 3.84) 0.97
MPAP (mmHg) 34.1±9.1 37.2±8.9 -0.43 (-2.41, 1.54) 0.67
CI (L/min/m2) 2.1±0.6 2.0±0.6 -0.15 (-0.44, 0.14) 0.30
PVR (Wood U) 2.8±1.5 3.4±1.4 -0.12 (-0.36, 0.12) 0.34
% ICM 60.8 41.8 1.14 (0.93, 1.41) 0.21
% African-American 25.0 19.1 1.08 (0.62, 1.86) 0.79
% Caucasian 82.2 82.6 1.00 (0.89, 1.13) 0.99
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
% Blood group A 33.9 46.1 0.75 (0.57, 0.99) 0.04
% Blood group B 11.9 10.1 1.19 (0.67, 2.13) 0.55
% Blood group AB 3.7 5.7 0.75 (0.29, 1.97) 0.56
% Blood group O 50.5 38.0 1.35 (1.09, 1.68) 0.007
% CMV positive 68.5 67.8 1.02 (0.84, 1.24) 0.83
% PRA ≥ 10 30.5 10.7 3.84 (2.71, 5.42) <0.00001
% IABP 10.4 13.2 0.65 (0.08, 4.99) 0.68
Ischemic time 183.8±55.5 165.0±52.4 19.10 (-0.51, 38.72) 0.06
Donor age 32.0±12.0 33.4±12.6 -1.10 (-4.76, 2.56) 0.56
LVAD, left ventricular assist device; BTT, bridge to transplantation; OHT, orthotopic heart transplantation; PCWP, pulmonary capillary wedge
pressure, MPAP, mean pulmonary arterial pressure; CI, cardiac index; PVR, pulmonary vascular resistance; ICM, ischemic cardiomyopathy;
CMV, cytomegalovirus; PRA, panel-reactive antibody; IABP, intra-aortic balloon pump; RR, risk ratio; WMD, weighted mean difference; CI,
confidence interval