
Internal Reconstruction of the Pelvic Floor for Recurrent Groin Hernia
5
Internal Reconstruction of the Pelvic Floor for Recurrent Groin Hernia ERLE E. PEACOCK, JR., M.D. Repeated recurrence of groin hernia is more than an anatomical derangement that any trained surgeon can correct. Attempts to improve results include application of local patches of Marlex. There are two reasons (one theoretical and one practical) why a local synthetic patch may not be as useful as total reconstruction of endopelvic fascia with a biologically active, as well as struc- turally strong, living material. Such a restoration can be accom- plished with the entire fascia lata from one thigh utilized as a free graft extending from one pelvic wall to the other and from the symphysis to the pubic rami. The practical advantage of a single sheet of fascia extending across the pelvic floor (like an airplane wing) is that frequent medial recurrences are eliminated because there is no medial edge under which peritoneum can protrude. The theoretical advantage of a biologically active graft is based upon animal data revealing the inductive capacity of fascia in stimulating net collagen synthesis and deposition. Thir- teen patients with multiple recurrences following conventional repair of groin hernia have been reconstructed with large fascia lata grafts restoring the entire endopelvic floor. Over a 5-year period no recurrences have been detected. A technique for re- moving the entire fascia lata from one thigh through a single transverse incision will be shown. There have not been any donor site complications and there is no disability caused by removing the fascia. T HE MOST PROMINENT FINDING in acquired or direct groin hernia in elderly men usually is described as a weakness of the abdominal wall, particularly the pos- terior medial well of the inguinal canal.6 Weakness ac- tually means a deficiency of fibrous protein, however; it does not mean the opposite of muscular strength. The fibrous protein that is deficient is collagen and the layer that is affected most significantly is the deepest internal layer of dense connective tissue or transversalis fascia. Why transversalis fascia should become selectively defi- cient in the floor of the inguinal canal in elderly men has been largely speculative, although Read et al. made mea- surements of general collagen metabolism and interpreted their data as supporting the theory that groin hernia was Presented at the 104th Annual Meeting of the American Surgical Association, Toronto, Canada, April 25-27, 1984. Reprint requests: Erle E. Peacock, Jr., M.D., Suite 2204 Professional Village, 109 Conner Drive, Chapel Hill, NC 27514. Submitted for publication: April 30, 1984. From Professional Village, Chapel Hill, North Carolina only a localized manifestation of a generalized reduction in collagen synthesis and deposition.8"2 I do not agree with Read's conclusions. Regardless of the reason, how- ever, most surgeons agree that the major problem in re- pairing a direct groin hernia is replacing a deficient quan- tity of transversalis fascia in the posterior wall of the inguinal canal. Satisfactory repair, therefore, depends upon advancing or rotating local tissue as a sort of local pedicle flap after making relaxing incisions, etc. or by adding new material in the form of a free graft or synthetic implant. Autogenous grafts include fascial sutures, strips, and sheets; artificial grafts include Marlex, nylon, poly- prolene, mersilene, and metals in varying weaves and forms. The preponderance of enthusiasm at this time is for Marlex mesh even though rejection and mechanical problems have been reported following the use of all for- eign materials in a physically active area such as the groin. To try to elucidate further the true nature of the collagen metabolic disorder responsible for development of re- current direct inguinal hernia and to reverse the funda- mental biological problem involved, the following studies have been performed. Materials and Methods Thirteen patients at the Tucson Veterans' Hospital, the Arizona Medical Center, and Tulane University Medical Center were operated upon. All of the patients in the study had at least three recurrent groin hernias on one side and did not have any other hernia in the other groin or elsewhere. Five of the patients were studied under a research protocol in which the patient agreed to explo- ration of both inguinal areas through a single incision and preperitoneal exposure. The patients agreed to a bi- opsy of transversalis fascia at a comparable site on both sides. In order to prevent hernia formation in the control biopsy site on the nonherniated side, a single massive fascia lata graft was utilized to repair the recurrent hernia 321
Transcript of Internal Reconstruction of the Pelvic Floor for Recurrent Groin Hernia
Internal Reconstruction of the Pelvic Floorfor Recurrent Groin Hernia
ERLE E. PEACOCK, JR., M.D.
Repeated recurrence of groin hernia is more than an anatomicalderangement that any trained surgeon can correct. Attempts toimprove results include application of local patches of Marlex.There are two reasons (one theoretical and one practical) whya local synthetic patch may not be as useful as total reconstructionof endopelvic fascia with a biologically active, as well as struc-turally strong, living material. Such a restoration can be accom-plished with the entire fascia lata from one thigh utilized as afree graft extending from one pelvic wall to the other and fromthe symphysis to the pubic rami. The practical advantage of asingle sheet of fascia extending across the pelvic floor (like anairplane wing) is that frequent medial recurrences are eliminatedbecause there is no medial edge under which peritoneum canprotrude. The theoretical advantage of a biologically active graftis based upon animal data revealing the inductive capacity offascia in stimulating net collagen synthesis and deposition. Thir-teen patients with multiple recurrences following conventionalrepair of groin hernia have been reconstructed with large fascialata grafts restoring the entire endopelvic floor. Over a 5-yearperiod no recurrences have been detected. A technique for re-moving the entire fascia lata from one thigh through a singletransverse incision will be shown. There have not been any donorsite complications and there is no disability caused by removingthe fascia.
T HE MOST PROMINENT FINDING in acquired or directgroin hernia in elderly men usually is described as
a weakness of the abdominal wall, particularly the pos-terior medial well of the inguinal canal.6 Weakness ac-tually means a deficiency of fibrous protein, however; itdoes not mean the opposite of muscular strength. Thefibrous protein that is deficient is collagen and the layerthat is affected most significantly is the deepest internallayer of dense connective tissue or transversalis fascia.Why transversalis fascia should become selectively defi-cient in the floor of the inguinal canal in elderly men hasbeen largely speculative, although Read et al. made mea-surements ofgeneral collagen metabolism and interpretedtheir data as supporting the theory that groin hernia was
Presented at the 104th Annual Meeting of the American SurgicalAssociation, Toronto, Canada, April 25-27, 1984.
Reprint requests: Erle E. Peacock, Jr., M.D., Suite 2204 ProfessionalVillage, 109 Conner Drive, Chapel Hill, NC 27514.
Submitted for publication: April 30, 1984.
From Professional Village,Chapel Hill, North Carolina
only a localized manifestation of a generalized reductionin collagen synthesis and deposition.8"2 I do not agreewith Read's conclusions. Regardless of the reason, how-ever, most surgeons agree that the major problem in re-pairing a direct groin hernia is replacing a deficient quan-tity of transversalis fascia in the posterior wall of theinguinal canal. Satisfactory repair, therefore, dependsupon advancing or rotating local tissue as a sort of localpedicle flap after making relaxing incisions, etc. or byadding new material in the form ofa free graft or syntheticimplant. Autogenous grafts include fascial sutures, strips,and sheets; artificial grafts include Marlex, nylon, poly-prolene, mersilene, and metals in varying weaves andforms. The preponderance of enthusiasm at this time isfor Marlex mesh even though rejection and mechanicalproblems have been reported following the use of all for-eign materials in a physically active area such as the groin.To try to elucidate further the true nature of the collagenmetabolic disorder responsible for development of re-current direct inguinal hernia and to reverse the funda-mental biological problem involved, the following studieshave been performed.
Materials and Methods
Thirteen patients at the Tucson Veterans' Hospital,the Arizona Medical Center, and Tulane UniversityMedical Center were operated upon. All of the patientsin the study had at least three recurrent groin hernias onone side and did not have any other hernia in the othergroin or elsewhere. Five ofthe patients were studied undera research protocol in which the patient agreed to explo-ration of both inguinal areas through a single incisionand preperitoneal exposure. The patients agreed to a bi-opsy of transversalis fascia at a comparable site on bothsides. In order to prevent hernia formation in the controlbiopsy site on the nonherniated side, a single massivefascia lata graft was utilized to repair the recurrent hernia
321
Ann. Surg. * September 1984
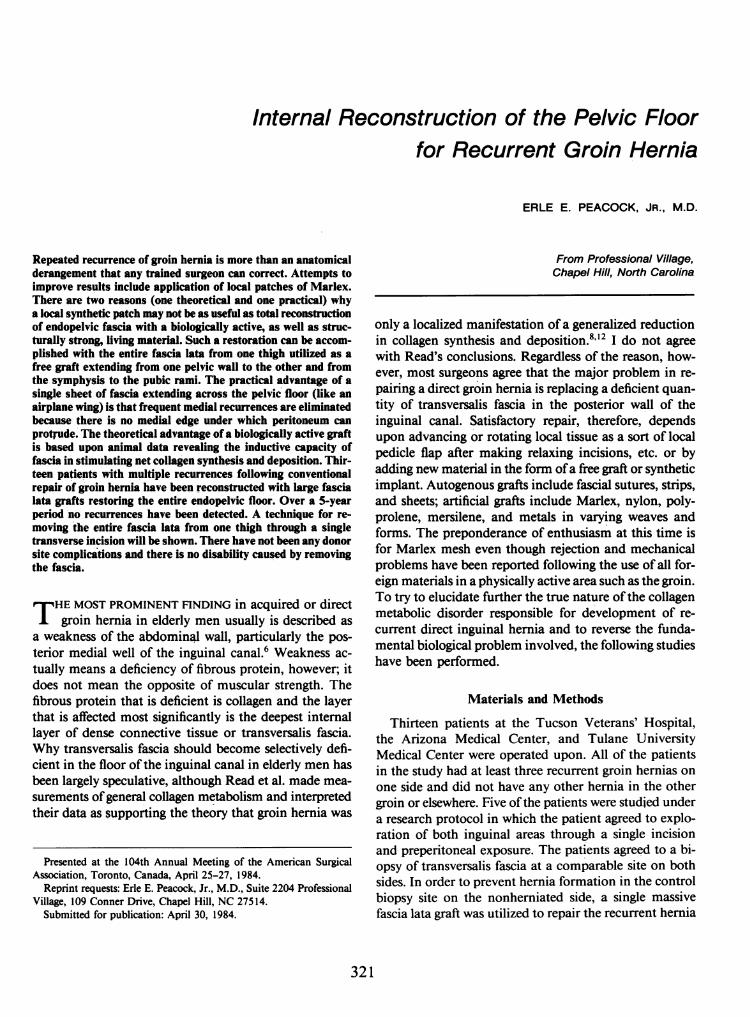
FIG. 1. Preperitoneal view of sutures closing direct hernia defect. Sutureshave been placed in superior transversalis fascia and inferior ileopubictract. Note difficulty in ascertaining "normil fascia" in supenor edgeof defect.
on one side and the biopsy site on the control side. Biopsyspecimens contained approximately 200 mg wet weightof fascia. A similar specimen also was taken from thefascia lata graft that was utilized in the repair. In all threespecimens, rate of net collagen synthesis and depositionwas measured by the Juva-Prockop method. Total col-lagen was measured by the Woessner method and tissuecollagenolysis was measured by a mammalian adaptationof the original amphibian tissue culture method.'3'3'9
Operative Technique
All ofthe patients were operated upon through a singletransverse lower abdominal incision approximately 3 cmsuperior to the symphysis. Muscle and fascia were splitlateral to the rectus abdominus muscle on both sides.The rectus fascia and muscles were not incised. Thus, a
single skin wound and two lateral abdominal wall woundswere utilized to explore the preperitoneal area ofthe entirepelvic floor. The hernia sac was readily identified andusually could be reduced without incising normal trans-versalis fascia. Closure of the hernia defect and biopsysite was carried out by suturing superior transversalis fasciato the inferior ileo-pubic tract with 0 Ethibond suturematerial as described by Nyhus et al.5 Closure of thebiopsy site on, the control side was carried out with in-terrupted sutures of the same material. Although tensionon the suture line was not a problem because of anteriorabdominal wall shift, sutures in some patients showed a
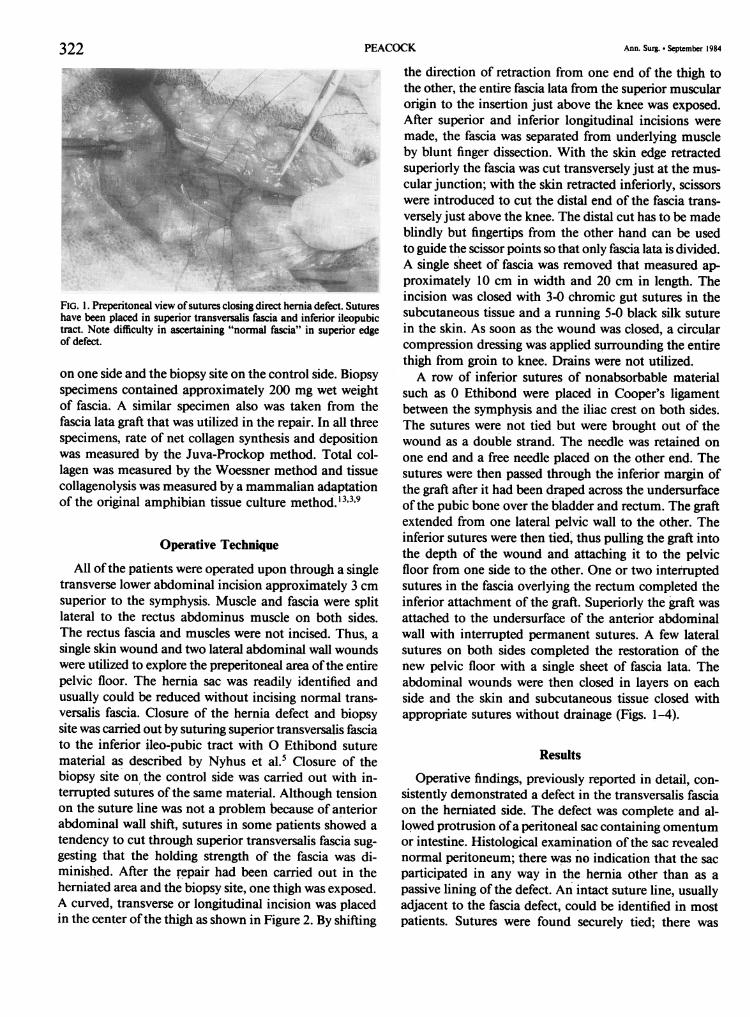
tendency to cut through superior transversalis fascia sug-gesting that the holding strength of the fascia was di-minished. After the repair had been carried out in theherniated area and the biopsy site, one thigh was exposed.A curved, transverse or longitudinal incision was placedin the center ofthe thigh as shown in Figure 2. By shifting
the direction of retraction from one end of the thigh tothe other, the entire fascia lata from the superior muscularorigin to the insertion just above the knee was exposed.After superior and inferior longitudinal incisions weremade, the fascia was separated from underlying muscleby blunt finger dissection. With the skin edge retractedsuperiorly the fascia was cut transversely just at the mus-cular junction; with the skin retracted inferiorly, scissorswere introduced to cut the distal end of the fascia trans-versely just above the knee. The distal cut has to be madeblindly but fingertips from the other hand can be usedto guide the scissor points so that only fascia lata is divided.A single sheet of fascia was removed that measured ap-proximately 10 cm in width and 20 cm in length. Theincision was closed with 3-0 chromic gut sutures in thesubcutaneous tissue and a running 5-0 black silk suturein the skin. As soon as the wound was closed, a circularcompression dressing was applied surrounding the entirethigh from groin to knee. Drains were not utilized.A row of inferior sutures of nonabsorbable material
such as 0 Ethibond were placed in Cooper's ligamentbetween the symphysis and the iliac crest on both sides.The sutures were not tied but were brought out of thewound as a double strand. The needle was retained onone end and a free needle placed on the other end. Thesutures were then passed through the inferior margin ofthe graft after it had been draped across the undersurfaceof the pubic bone over the bladder and rectum. The graftextended from one lateral pelvic wall to the other. Theinferior sutures were then tied, thus pulling the graft intothe depth of the wound and attaching it to the pelvicfloor from one side to the other. One or two interruptedsutures in the fascia overlying the rectum completed theinferior attachment of the graft. Superiorly the graft wasattached to the undersurface of the anterior abdominalwall with interrupted permanent sutures. A few lateralsutures on both sides completed the restoration of thenew pelvic floor with a single sheet of fascia lata. Theabdominal wounds were then closed in layers on eachside and the skin and subcutaneous tissue closed withappropriate sutures without drainage (Figs. 1-4).
Results
Operative findings, previously reported in detail, con-sistently demonstrated a defect in the transversalis fasciaon the herniated side. The defect was complete and al-lowed protrusion ofa peritoneal sac containing omentumor intestine. Histological examination of the sac revealednormal peritoneum; there was no indication that the sacparticipated in any way in the hernia other than as apassive lining of the defect. An intact suture line, usuallyadjacent to the fascia defect, could be identified in mostpatients. Sutures were found securely tied; there was
322 PEACOCK
PELVIC FLOOR RECONSTRUCTION*s}s i_.- ..................~~~....--... ..
FIG. 2. Exposure of entire fascia lata in midthigh.
nothing to suggest that the hernia was the result of de-hiscence of a previous surgical wound. On the nonher-niated side transversalis fascia in some patients appearedattenuated, while in others there was no evidence of anychange in the amount of fascia present. The medial wallof the internal ring appeared selectively involved whendeficient fascia was encountered (Figs. 5-7).
Biochemical data are presented in Table 1. Collagen-olytic activity was present in all specimens. Net collagensynthesis and deposition were significantly elevated in themargin of the defect, which produced a hernia on one
side as compared to intact fascia on the nonherniated or
control side. Total collagen content of the transversalisfascia was not consistently or significantly different on
either side or in the fascia lata graft.Before the study reported in this paper was performed,
four patients were operated upon and repaired with a
unilateral fascia lata graft. Two patients developed a re-
current groin hernia within the first year and were re-
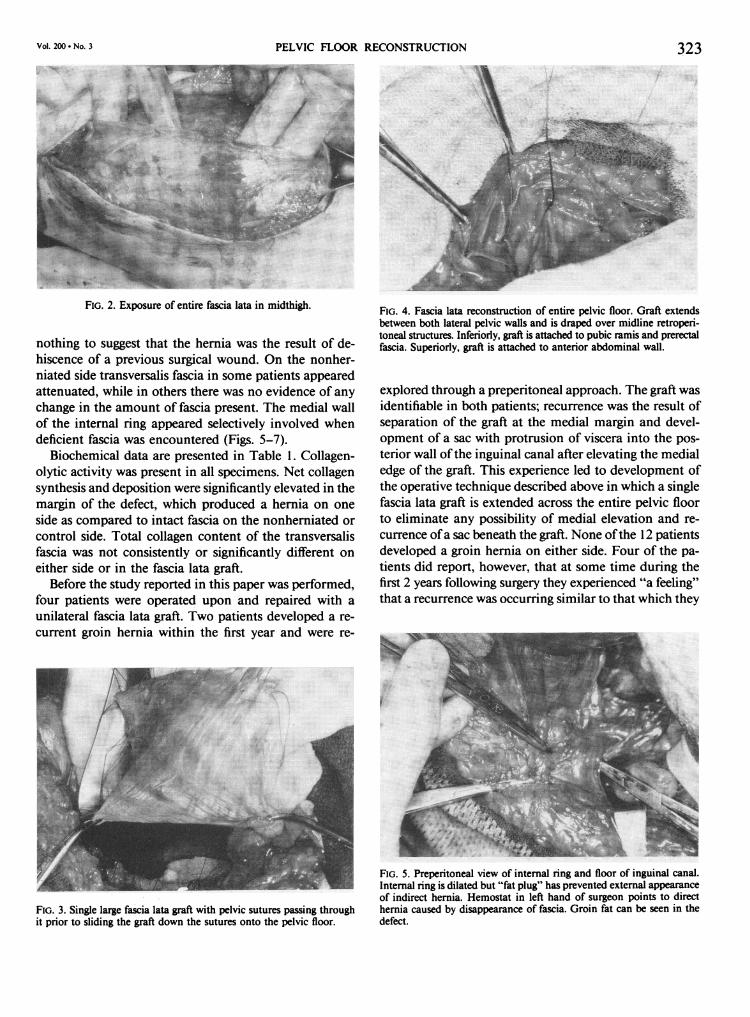
FIG. 3. Single large fascia lata graft with pelvic sutures passing throughit prior to sliding the graft down the sutures onto the pelvic floor.
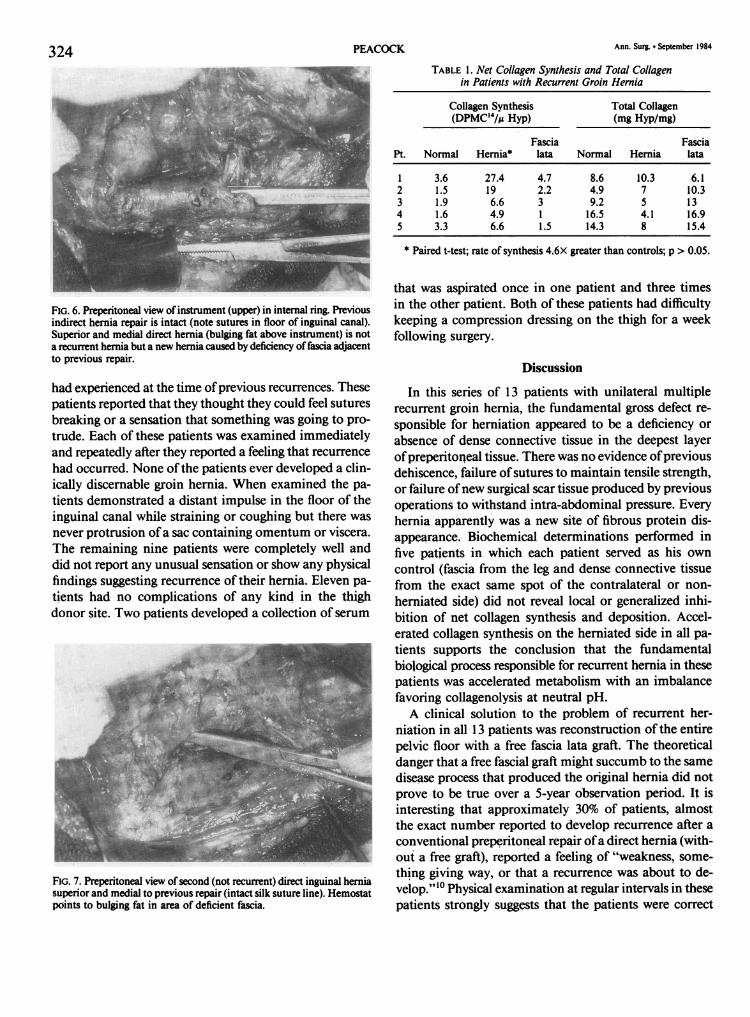
FIG. 4. Fascia lata reconstruction of entire pelvic floor. Graft extendsbetween both lateral pelvic walls and is draped over midline retroperi-toneal structures. Inferiorly, graft is attached to pubic ramis and prerectalfascia. Superiorly, graft is attached to anterior abdominal wall.
explored through a preperitoneal approach. The graft wasidentifiable in both patients; recurrence was the result ofseparation of the graft at the medial margin and devel-opment of a sac with protrusion of viscera into the pos-
terior wall ofthe inguinal canal after elevating the medialedge of the graft. This experience led to development ofthe operative technique described above in which a singlefascia lata graft is extended across the entire pelvic floorto eliminate any possibility of medial elevation and re-
currence ofa sac beneath the graft. None ofthe 12 patientsdeveloped a groin hernia on either side. Four of the pa-
tients did report, however, that at some time during thefirst 2 years following surgery they experienced "a feeling"that a recurrence was occurring similar to that which they
FIG. 5. Preperitoneal view of internal ring and floor of inguinal canal.Internal ring is dilated but "fat plug" has prevented external appearanceof indirect hernia. Hemostat in left hand of surgeon points to directhernia caused by disappearance of fascia. Groin fat can be seen in thedefect.
Vol. 200 * No. 3 323.. . . .... . ....... ...... . . ... . -} iS
Si ffi ; [ :!tg* .... o::B: . ' . .. . DE* . :-: :r:: w . . .. o... i.' }:: :*.. :! at.
;. .:. :. .... : .. . S. .}*: . : .. : :'. .. ..*: . : :: . !: e<t ,. . :..... X g X s . ' :... ' a : J., ;:
,.s,. . :. ,, t. i X k -,(l ... . : - She. tRE ___ .-i . t. < ::x: :: - -. :'.'-<a W N_ 5 ... ^.2 . !. sSe .. ':-:s'b.: ': .. ::oou la ::.*s o }.'':gl ^ . _ ... , ; .|L::SiF : res.
Ann. Surg. * September 1984PEACOCK
FIG. 6. Preperitoneal view of instrument (upper) in internal ring. Previousindirect hernia repair is intact (note sutures in floor of inguinal canal).Superior and medial direct hernia (bulging fat above instrument) is nota recurrent hernia but a new hernia caused by deficiency of fascia adjacentto previous repair.
had experienced at the time ofprevious recurrences. Thesepatients reported that they thought they could feel suturesbreaking or a sensation that something was going to pro-trude. Each of these patients was examined immediatelyand repeatedly after they reported a feeling that recurrence
had occurred. None ofthe patients ever developed a clin-ically discernable groin hernia. When examined the pa-
tients demonstrated a distant impulse in the floor of theinguinal canal while straining or coughing but there was
never protrusion ofa sac containing omentum or viscera.The remaining nine patients were completely well anddid not report any unusual sensation or show any physicalfindings suggesting recurrence of their hernia. Eleven pa-
tients had no complications of any kind in the thighdonor site. Two patients developed a collection of serum
MIG. 7. Preperitoneal view of second (not recurrent) direct inguinal herniasuperior and medial to previous repair (intact silk suture line). Hemostatpoints to bulging fat in area of deficient fascia.
TABLE 1. Net Collagen Synthesis and Total Collagenin Patients with Recurrent Groin Hernia
Collagen Synthesis Total Collagen(DPMC4/,u Hyp) (mg Hyp/mg)
Fascia FasciaPt. Normal Hernia* lata Normal Hernia lata
1 3.6 27.4 4.7 8.6 10.3 6.12 1.5 19 2.2 4.9 7 10.33 1.9 6.6 3 9.2 5 134 1.6 4.9 1 16.5 4.1 16.95 3.3 6.6 1.5 14.3 8 15.4
* Paired t-test; rate of synthesis 4.6X greater than controls; p > 0.05.
that was aspirated once in one patient and three timesin the other patient. Both of these patients had difficultykeeping a compression dressing on the thigh for a weekfollowing surgery.
Discussion
In this series of 13 patients with unilateral multiplerecurrent groin hernia, the fundamental gross defect re-sponsible for herniation appeared to be a deficiency orabsence of dense connective tissue in the deepest layerofpreperitoneal tissue. There was no evidence ofpreviousdehiscence, failure of sutures to maintain tensile strength,or failure ofnew surgical scar tissue produced by previousoperations to withstand intra-abdominal pressure. Everyhernia apparently was a new site of fibrous protein dis-appearance. Biochemical determinations performed infive patients in which each patient served as his owncontrol (fascia from the leg and dense connective tissuefrom the exact same spot of the contralateral or non-herniated side) did not reveal local or generalized inhi-bition of net collagen synthesis and deposition. Accel-erated collagen synthesis on the herniated side in all pa-tients supports the conclusion that the fundamentalbiological process responsible for recurrent hernia in thesepatients was accelerated metabolism with an imbalancefavoring collagenolysis at neutral pH.A clinical solution to the problem of recurrent her-
niation in all 13 patients was reconstruction of the entirepelvic floor with a free fascia lata graft. The theoreticaldanger that a free fascial graft might succumb to the samedisease process that produced the original hernia did notprove to be true over a 5-year observation period. It isinteresting that approximately 30% of patients, almostthe exact number reported to develop recurrence after aconventional preperitoneal repair ofa direct hernia (with-out a free graft), reported a feeling of "weakness, some-thing giving way, or that a recurrence was about to de-velop."'0 Physical examination at regular intervals in thesepatients strongly suggests that the patients were correct
324

Vol. 200 * No. 3 PELVIC FLOOR RECONSTRUCTION 325ih their assessment of "something giving way" and thatwhat the patients actually described was a breakdown ofthe transversalis fascia somewhere in the area of the il-eopubic tract repair. The fascial graft remained intact inall patients, however, and the barely palpable impulseseems likely to be the result of intraperitoneal contentsresting upon the new reconstructed pelvic floor.
Whether or not the fundamental biological phenom-enon responsible for recurrent direct hernia in elderlymen is decreased collagen synthesis or increased colla-genolysis and whether such an abnormality is generalizedor local is only ofacademic interest, except as it influencesthe type of repair the surgeon performs. The results ofusing tissue only to repair recurrent connective tissuedefects in the groin and the obvious conclusion that theend result ofthe process is a deficiency ofdense connectivetissue argue strongly for the addition of new dense con-nective tissue or a suitable synthetic substitute. There isno question that a commercial substance such as Marlexmesh is the prevalent choice of most surgeons today; butthere is a question that such a choice, although convenientfor the surgeon, is the best choice for the patient with abiological abnormality." There are both theoretical andpractical advantages to the use of living autogenous fascia.The advantages and disadvantages of autogenous andsynthetic substances can be summarized as follows.
Synthetic materials are quickly and easily made avail-able in the operating room at reasonable expense. Nodonor site scar is produced and approximately 15 minutesof operating room time can be saved. The disadvantagesof synthetic substances are that a large graft is needed torepair both sides simultaneously with a single restorationand this amount of foreign material is a potential sourceof chronic infection and mechanical irritation. Calne,using Mersilene mesh threaded behind the rectus musclesand sutured to both ileac spines, reported one infection,six unilateral recurrences, and one bilateral recurrence.2Marlex and other synthetic mesh does have to be removedin some patients and, even though the incidence appar-ently is low, the procedure is difficult and prolonged whennecessary. In a survey performed by Adler, 65% of over800 randomly selected general surgeons utilized Marlexmesh in 20% of hernia repairs. Thirty-five per cent of thesurgeons reported having to remove mesh because of re-current hernia, chronic infection, or fluid accumulation.'Marlex, apparently like "the little girl with the curl who,when she is good is very very good, but when she is badshe is horrible," can be gratifyingly successful or extremelycomplicated.
Autogenous fascia has the practical disadvantage ofrequiring a separate surgical incision and approximately15 minutes of additional operating room time. Therehave been no significant or lasting complications in thedonor area in many hundreds of grafts removed for var-ious purposes during the last 30 years. Practically, fasciaconforms most naturally to the convulutions and con-figurations of pelvic structures and replaces most naturallythe substance that is missing in that area. Autogenousfascia lata provides a powerful inductive stimulus for netcollagen synthesis and deposition which is known to lastin human beings for at least 2 years.4'7 Theoretically,therefore, induction of net collagen synthesis and de-position corrects most directly what appears to be thefundamental defect in groin hernia-excess collagenolysisover net collagen synthesis and deposition. Although fullreconstruction of the entire pelvic floor with a free au-togenous fascia lata graft has only been performed a rel-atively small number of times, the clinical results appearto be excellent. It would seem, therefore, that the practicaland theoretical advantages of autogenous fascia over asynthetic substitute and the excellent results that havebeen obtained in a limited number of patients justifymore extensive clinical trial and evaluation.
References
1. Adler RH. An evaluation of surgical mesh in the repair of herniasand tissue defects. Arch Surg 1962; 85:836.
2. Calne RY. Repair of bilateral hernia with Mersilene mesh behindrectus abdominus. Arch Surg 1974; 109:532.
3. Juva K, Prockop DJ. Modified procedure for the assay of H3 orC'4 labeled hydroxyproline. Anal Biochem 1966; 15:77.
4. Merritt W, Peacock EE Jr, Chvapil M. Comparative biology offascial autografts and allografts. Surg Forum 1974; 25:524.
5. Nyhus LM, Condon RE, Harkins HN. Clinical experiences withpreperitoneal hernial repair for all types of hernia of the groin.Am J Surg 1960; 100:234.
6. Peacock EE Jr. Studies on the biology and treatment of recurrentinguinal hernia. II. Morphological changes. Ann Surg 1974;179:567.
7. Peacock EE Jr, Chvapil M, unpublished data.8. Read RC. Attenuation of the rectus sheath in inguinal herniation.
Am J Surg 1970; 120:610.9. Riley WB, Peacock EE Jr. The identification, distribution, and sig-
nificance of a collagenolytic enzyme in human tissues. Proc SocExp Biol Med 1967; 124:207.
10. Thieme ET. Recurrent inguinal hernia. Arch Surg 1971; 103:238.11. Usher FC. Hernia repair with Marlex mesh. In Nyhus and Condon,
eds. Hernia, 2nd ed. Philadelphia: J. B. Lippincott & Co., 1978;563.
12. Wagh PV, Leverich AP, Sun CN. Direct inguinal herniation in men:a disease of collagen. J Surg Res 1974; 17:425.
13. Woessner JF Jr. The determination of hydroxyproline in tissue andprotein samples containing small proportions ofthis amino acid.Arch Biochem Biophys 1961; 93:440.




![10 Groin Hernia - University of Birmingham · d:/postscript/10-chap10_3.3d – 27/1/4 – 9:29 [This page: 671] 10 Groin Hernia Wendy Phillips and Mark Goldman 1 Summary Statement](https://static.fdocuments.net/doc/165x107/5ad660157f8b9a6b668b8b6e/10-groin-hernia-university-of-birmingham-postscript10-chap1033d-2714.jpg)













