Interleukin-32IncreasesHumanGastricCancerCellInvasion Associated with Tumor ... · IL-32,...
14
Human Cancer Biology Interleukin-32 Increases Human Gastric Cancer Cell Invasion Associated with Tumor Progression and Metastasis Chung-Ying Tsai 1 , Chia-Siu Wang 4 , Ming-Ming Tsai 2 , Hsiang-Cheng Chi 1 , Wan-Li Cheng 3 , Yi-Hsin Tseng 1 , Cheng-Yi Chen 1 , Crystal D. Lin 6 , Jun-I. Wu 5 , Lu-Hai Wang 5 , and Kwang-Huei Lin 1 Abstract Purpose: The proinflammatory cytokine interleukin-32 (IL-32) is a novel tumor marker highly expressed in various human carcinomas, including gastric cancer. However, its effects on prognosis of patients with gastric cancer and cancer metastasis are virtually unknown at present. The main aim of this study was to explore the clinical significance of IL-32 in gastric cancer and further elucidate the molecular mechanisms underlying IL-32–mediated migration and invasion. Experimental Design: Gastric cancer cells with ectopic expression or silencing of IL-32 were examined to identify downstream molecules and establish their effects on cell motility, invasion, and lung metastasis in vivo. Results: IL-32 was significantly upregulated in gastric cancer and positively correlated with aggressiveness of cancer and poor prognosis. Ectopic expression of IL-32 induced elongated morphology and increased cell migration and invasion via induction of IL-8, VEGF, matrix metalloproteinase 2 (MMP2), and MMP9 expression via phosphor-AKT/phospho-glycogen synthase kinase 3b/active b-catenin as well as hypoxia- inducible factor 1a (HIF-1a) signaling pathways. Conversely, depletion of IL-32 in gastric cancer cells reversed these effects and decreased lung colonization in vivo. Examination of gene expression datasets in oncomine and staining of gastric cancer specimens demonstrated the clinical significance of IL-32 and its downstream molecules by providing information on their coexpression patterns. Conclusions: IL-32 contributes to gastric cancer progression by increasing the metastatic potential resulting from AKT, b-catenin, and HIF-1a activation. Our results clearly suggest that IL-32 is an important mediator for gastric cancer metastasis and independent prognostic predictor of gastric cancer. Clin Cancer Res; 20(9); 2276–88. Ó2014 AACR. Introduction Gastric cancer is the fourth most common cancer type worldwide and ranks second in terms of global cancer- related mortality (1). In Taiwan, gastric cancer was recorded as the sixth leading cause of cancer-related deaths in 2010 (2). The prognosis of gastric cancer is poor, and the key players in molecular pathogenesis are predomi- nantly unknown at present. The tumor–node–metastasis (TNM) staging system is the only tool routinely used for predicting prognosis in the clinical setting. Currently, surgery is the major known cure for the disease. Therefore, elucidation of the molecular mechanisms involved in gastric cancer and identification of valuable prognostic markers as well as novel therapeutic strategies is of essen- tial clinical value (3). Increasing evidence has confirmed the hypothesis that several pro- and anti-inflammatory cytokines promote tumor progression and affect the host antitumor response (4). Inflammatory tumor microenvironments play a pivotal role, not only in tumor development but also metastasis. Cytokines released in response to infection affect tumor development in different ways. IL-8 produced by gastric cancer cells contributes to sustained angiogenesis and tumor invasion and metastasis via either autocrine or para- crine mechanisms (5). VEGF promotes breast cancer cell invasion through an autocrine pathway (6). Recent studies have revealed higher expression of IL-32, a novel pro- inflammatory cytokine, in human stomach (7, 8), lung (9), pancreas (10), liver (11), and esophagus (12) cancer tissues, compared with normal tissue or serum. Authors' Affiliations: 1 Department of Biochemistry, College of Medicine; 2 Department of Nursing, Chang-Gung University of Science and Technol- ogy; 3 Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Taoyuan; 4 Department of General Surgery, Chang Gung Memorial Hospital at Chiayi; 5 National Health Research Institute, Zhunan, Miaoli, Taiwan, Republic of China; and 6 Pre-med Program, Pacific Union College, Angwin, California Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/). C.-Y. Tsai and C.-S. Wang contributed equally to this article. Corresponding Author: Kwang-Huei Lin, Department of Biochemistry, Chang-Gung University, 259 Wen-hwa 1 Road, Taoyuan, Taiwan. Phone: 886-3-211-8263; Fax: 886-3-211-8263; E-mail: [email protected] doi: 10.1158/1078-0432.CCR-13-1221 Ó2014 American Association for Cancer Research. Clinical Cancer Research Clin Cancer Res; 20(9) May 1, 2014 2276 on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221
Transcript of Interleukin-32IncreasesHumanGastricCancerCellInvasion Associated with Tumor ... · IL-32,...

Human Cancer Biology
Interleukin-32 IncreasesHumanGastric Cancer Cell InvasionAssociated with Tumor Progression and Metastasis
Chung-Ying Tsai1, Chia-Siu Wang4, Ming-Ming Tsai2, Hsiang-Cheng Chi1, Wan-Li Cheng3, Yi-Hsin Tseng1,Cheng-Yi Chen1, Crystal D. Lin6, Jun-I. Wu5, Lu-Hai Wang5, and Kwang-Huei Lin1
AbstractPurpose: The proinflammatory cytokine interleukin-32 (IL-32) is a novel tumormarker highly expressed
in various human carcinomas, including gastric cancer. However, its effects on prognosis of patients with
gastric cancer and cancer metastasis are virtually unknown at present. The main aim of this study was to
explore the clinical significance of IL-32 in gastric cancer and further elucidate the molecular mechanisms
underlying IL-32–mediated migration and invasion.
ExperimentalDesign:Gastric cancer cells with ectopic expression or silencing of IL-32were examined to
identify downstream molecules and establish their effects on cell motility, invasion, and lung metastasis
in vivo.
Results: IL-32was significantly upregulated in gastric cancer andpositively correlatedwith aggressiveness
of cancer and poor prognosis. Ectopic expression of IL-32 induced elongatedmorphology and increased cell
migration and invasion via induction of IL-8, VEGF, matrix metalloproteinase 2 (MMP2), and MMP9
expression via phosphor-AKT/phospho-glycogen synthase kinase 3b/active b-catenin as well as hypoxia-
inducible factor 1a (HIF-1a) signaling pathways. Conversely, depletion of IL-32 in gastric cancer cells
reversed these effects and decreased lung colonization in vivo. Examination of gene expression datasets in
oncomine and staining of gastric cancer specimens demonstrated the clinical significance of IL-32 and its
downstream molecules by providing information on their coexpression patterns.
Conclusions: IL-32 contributes to gastric cancer progression by increasing the metastatic potential
resulting from AKT, b-catenin, and HIF-1a activation. Our results clearly suggest that IL-32 is an important
mediator for gastric cancer metastasis and independent prognostic predictor of gastric cancer. Clin Cancer
Res; 20(9); 2276–88. �2014 AACR.
IntroductionGastric cancer is the fourth most common cancer type
worldwide and ranks second in terms of global cancer-related mortality (1). In Taiwan, gastric cancer wasrecorded as the sixth leading cause of cancer-related deathsin 2010 (2). The prognosis of gastric cancer is poor, andthe key players in molecular pathogenesis are predomi-
nantly unknown at present. The tumor–node–metastasis(TNM) staging system is the only tool routinely used forpredicting prognosis in the clinical setting. Currently,surgery is the major known cure for the disease. Therefore,elucidation of the molecular mechanisms involved ingastric cancer and identification of valuable prognosticmarkers as well as novel therapeutic strategies is of essen-tial clinical value (3).
Increasing evidence has confirmed the hypothesis thatseveral pro- and anti-inflammatory cytokines promotetumor progression and affect the host antitumor response(4). Inflammatory tumormicroenvironments play a pivotalrole, not only in tumor development but also metastasis.Cytokines released in response to infection affect tumordevelopment in different ways. IL-8 produced by gastriccancer cells contributes to sustained angiogenesis andtumor invasion and metastasis via either autocrine or para-crine mechanisms (5). VEGF promotes breast cancer cellinvasion through an autocrine pathway (6). Recent studieshave revealed higher expression of IL-32, a novel pro-inflammatory cytokine, in human stomach (7, 8), lung(9), pancreas (10), liver (11), and esophagus (12) cancertissues, compared with normal tissue or serum.
Authors' Affiliations: 1Department of Biochemistry, College of Medicine;2Department of Nursing, Chang-Gung University of Science and Technol-ogy; 3Department of Gastroenterology and Hepatology, Chang GungMemorial Hospital, Taoyuan; 4Department of General Surgery, ChangGung Memorial Hospital at Chiayi; 5National Health Research Institute,Zhunan, Miaoli, Taiwan, Republic of China; and 6Pre-med Program, PacificUnion College, Angwin, California
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
C.-Y. Tsai and C.-S. Wang contributed equally to this article.
Corresponding Author: Kwang-Huei Lin, Department of Biochemistry,Chang-Gung University, 259 Wen-hwa 1 Road, Taoyuan, Taiwan. Phone:886-3-211-8263; Fax: 886-3-211-8263; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-13-1221
�2014 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 20(9) May 1, 20142276
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

IL-32, originally designated natural killer cell transcript 4(NK4) in humans, was found to be absent in rodents. Therecently described cytokine is mainly produced by T cells,NK cells, epithelial cells, and monocytes after stimulationwith IL-2, IL-18, or IFN-g (13). The IL-32 gene is located onhuman chromosome 16p13.3, and has a full length of 705bp. Moreover, the gene is organized into 8 exons and has 6splice variants, IL-32a, IL-32b, IL-32g , IL-32d, IL-32e, and IL-32z, amongwhich the g isoformexhibits thehighest cytokineproducing activity (14). IL-32b is themajor secreted isoform,whereas the a isoform is located intracellularly (15). How-ever, the functionaldifferencesbetween these isoformsare yetto be established. The cytokine induction activity of IL-32 isactivated viapartial cleavagebyproteinase-3 (16).Althoughareceptor for IL-32 has not been described, it is defined asa proinflammatory cytokine, in view of its stimulation ofTNF-a, IL-1b, IL-6, and IL-8production, and activationof theNF-kB and the p38 mitogen-activated protein kinase path-ways (17). Overexpression of IL-32 in stomach cancer tissuehas been reported (7). However, the specific role of thiscytokine in gastric cancer has received little attention, andits clinicopathologic significance and underlying molecularmechanisms have rarely been studied to date. Therefore, wefocused on the clinical and functional significance, as well asthe signaling pathway of IL-32 in gastric cancer.
Materials and MethodsSubjectsAfter obtaining informed consent, 120 patients (67males
and 53 females; median age, 66 years; range 28–86 years)diagnosed patholgically with gastric cancer at the ChangGungMemorial Hospital (CGMH) from2000 to 2005wereenrolled in the study. None of the patients had receivedchemotherapy or radiotherapy before operation and all of
them were subjected to gastric resection that included totalgastrectomy in 35 patients and subtotal gastrectomy in 85.The pathologic examination and further biological studieswere carried out under informed consents of patients. Thisstudy protocol was approved by the Medical Ethics andHuman Clinical Trial Committee of the CGMH (IRB NO.95-0472B).
Postoperatively, the patients with stage 2 to 3 diseasesreceived adjuvant chemotherapy with 5-fluorouracil–basedregimens, and those with stage 4 diseases were treated withpalliative chemotherapy of various regimens as indicated.All patients were followed up regularly in the outpatientservice of our hospital, of every 3months in the first 2 years,every 6monthsbetween the3rd and5th years and thenoncea year thereafter.
Clinicopathologic studiesResected specimens were examined pathologically using
the criteria of the 6th edition of the American Joint Com-mittee on Cancer (pTNM) classification system and theJapanese General Rules for gastric cancer Study (18). Clin-icopathologic parameters included patient age and gender,tumor location, and size, gross (Borrmann) tumor type,wall invasion, resection margin, histologic type, lymph-nodemetastasis, vascular invasion, lymphatic invasion, andperineural invasion. After discharge, all patients had peri-odic follow-up visits at the outpatient department ofCGMHuntil death or the beginning of preparation of this article.
Tumor samplesFresh samples of tumor tissue and adjacent noncancerous
mucosawere harvested immediately following gastric resec-tion. Samples were dissected from resected specimens by apathologist at CGMH, and immediately snap-frozen inindividual vials using liquid nitrogen. Frozen specimenswere stored at �70�C in a tumor bank until use.
Real-time quantitative reverse transcription PCRQuantitative reverse transcription PCR (qRT-PCR) was
performed using SYBR green as described previously (19).Fluorescence emitted by SYBR green was detected using theABI PRISM 7500 sequence detection system (Applied Bio-systems). The following primers were used: human IL-32qPCR (forward primer, 50-TGAGGATAAAAATG ACATCCC-TAAAGA-30, and reverse primer, 50-TGTGTCAGCTCAAG-TGT AGCTTTC-30); human IL-8 qPCR (forward primer,50-CTGGCCGTGGCTCTC TTG-30, and reverse primer, 50-CCTTGGCAAAACTGCACCTT-30); human 18s rRNA qPCR(forward primer, 50-CGAGCCGCCTGGATACC-30, andreverse primer, 50-CCTCAGTT CCGAAAACCAACAA-30).
Immunoblot analysisTotal cell lysates from tumors and adjacent noncancerous
mucosa or cell lines were extracted by lysis buffer (150 mMNaCl/50 mM Tris, pH 7.8/1% Triton X-100/1 mM EDTA, 1mMphenylmethylsulfonylfluoride) and quantified by Brad-ford method. Equal amounts of protein were electrophor-esed through a 10% Tris-SDS gel and transferred onto a
Translational RelevanceMetastasis is the major cause of death in patients with
gastric cancer and involves a multistep process, includ-ing invasion of surrounding tissue. Although interleu-kin-32 (IL-32) has been reported as a gastric cancertumor marker, the role of IL-32 in gastric cancer pro-gression and metastasis is unknown. This study showsthat IL-32 contributes to gastric cancer progression byincreasing the metastatic potential, resulting in worsepatient survival. Silencing of IL-32 revealed decreasedcell invasion ability and lung colonization in vivo bydownregulation of IL-8 and VEGF expression via phos-pho-AKT/active b-catenin signaling pathways. Theseresults demonstrate a novel function and regulation ofIL-32 in gastric cancer and imply that it might be advan-tageous to target IL-32 for cancer therapy. New thera-peutic strategies directed at blocking IL-32 signaling orfunction may effectively be applied to prevention ofgastric cancer metastasis.
Regulation of IL-32 in Gastric Cancer
www.aacrjournals.org Clin Cancer Res; 20(9) May 1, 2014 2277
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

polyvinylidene difluoride membrane. The membranes wereblocked overnight with PBS containing 0.1% Tween 20 in5%skimmedmilk at 4�C,andsubsequently immunoblottedwith primary antibody listed in Supplementary Table S1.After further washing, the membrane was incubated for 1hour with a horseradish peroxidase-conjugated, affinity-purified anti-rabbit antibody (1:5,000dilution in TBS; SantaCruz Biotechnology Inc.). Immune complexes were visual-ized via chemiluminescence using an ECL Detection Kit(Amersham Inc.).
ImmunohistochemistryFormalin-fixed and paraffin-embedded tissues were
examined with immunohistochemistry (IHC) using prima-ry antibody listed in Supplementary Table S2 and theavidin–biotin complex method according to previouslydescribed procedures (20). The staining intensity was grad-ed as absent (0), weak (1þ), medium (2þ), or strong (3þ).The histoscore (Q) was calculated by multiplying the per-centage (P) of positive cells by the intensity (I), according tothe formula: Q ¼ P1 � I1 þ P2 � I2 þ . . . þ Pn � In.
RNA interferenceThe lentiviral pLKO, control shLuc, and shRNA were
obtained from the National RNAi Core Facility at theInstitute of Molecular Biology/Genomic Research Center,Academia Sinica. Target information is listed in Supplemen-tary Table S3. Recombinant lentivirus carrying shRNA wasproduced by cotransfecting 293FT cells with a mixture ofplasmid DNA consisting of pMD-G (VSV-G envelope),pCMV-cR8.91 (Gag/Pol/Rev), and pLKO/1-shRNA vectorsusing TurboFect reagent (Fermentas) according to the man-ufacturer’s recommendations. Virus-containing culture sup-ernatants were collected 2 days after transfection and usedto infect AGS and TSGH9201 cells in combination with 10mg/mL polybrene (Sigma-Aldrich). Stable cell lines wereselected by culturing cells in 2 mg/mL puromycin (Calbio-chem) for 1 week. Western blot analysis or qPCR was usedto determine the effects of gene expression knockdown.
Cell lines and cultureTSGH9201 human gastric cancer cell line (BCRC 60146)
was obtained from the Bioresource Collection and ResearchCenter of Taiwan. Human gastric carcinoma cell line AGSwas obtained fromAmericanTypeCultureCollection (CRL-1739). The cell line was authenticated by assessments ofshort tandem repeat loci following database comparison.All cell lines were cultured in RPMI 1640 medium (Invitro-gen), supplementedwith 10%FBS (Invitrogen), 100 IU/mLpenicillin G, and 100 mg/mL streptomycin sulfate (Sigma-Aldrich) at 37�C in ahumidified atmosphere containing 5%CO2. All kinase inhibitors used in cell culture are listed inSupplementary Table S4.
In vivo tumor metastasis modelTSGH9201 cells with or without silencing IL-32 were
harvested and washed twice with PBS. Cells (1 �106/150 mL per mouse) were injected intravenously via a
30-gauge needle into the tail vein of 4 to 6 weeks old malesevere combined immunodeficiency (SCID; C.B17/Icr-scid) mice. Five weeks later, mice were sacrificed by CO2
and the lung was removed, fixed with 3.7% formaldehydeand sectioned. Paraffin sections were stained with hema-toxylin and eosin (H&E; Sigma). Lungmetastasis was quan-tified by counting the total tissue area per lung section (A1)andmetastasis present in the same area (A2). Themetastaticindex was calculated by the ratio A2/A1.
Statistical analysisTheMann–WhitneyU test or Fisher exact test was used for
between-group comparisons, where appropriate, and thecorrelation between the results obtainedwith the 2 differentanalyses analyzed with Spearman test. Follow-up studies ofpatients were performed until the time of writing or patientdeath. The cancer-specific survival outcome was evaluatedby applying the Kaplan–Meier method for all patients,except those who died from surgical complications. Thelog-rank test was used to compare the prognostic signifi-cance of individual variables on survival. Cox’s proportion-al hazards model was applied in a multivariate analysis toidentify independent predictors of survival. A P-value of<0.05 was considered statistically significant.
ResultsHigh expression of IL-32 in gastric cancer is correlatedwith tumor progression and poor prognosis
In our previous study (21), differential gene expressionpatterns from genome-wide microarray analyses revealedupregulation of several inflammation-associated genes ingastric cancer tissues, compared with adjacent nontumor-ousmucosa tissues.CXCL1 (22),SLIP (23), and SPARC (21)have been verified and studied for clinical significances inour setting. Furthermore, we focused on anovel pro-inflam-matory gene, IL-32, as a potential tumor marker for gastriccancer development. To verify the enhanced expression ofIL-32 in gastric cancer, IHC (n ¼ 120) and real-time qPCR(n¼ 66) were performed on clinical specimens. Among the120 patients analyzed using IHC, the mean score in tumortissues was 107.2� 4.8, whichwas significantly greater thanthat (32.33� 3.98) in thematching adjacentmucosa. IL-32was consistently detected in the majority of tumor regions,whereas levels were reduced in nontumor areas (Supple-mentary Fig. S1A). Four pairs of representative cases fromIHC analysis are shown in Supplementary Fig. S1B. Strongstaining of IL-32wasmostly detected in the cytosol of gastrictumor cells. In contrast, absent or weak staining for IL-32was observed in nontumor gastric epithelial cells. Stainingwas more intense in the advanced stages (SupplementaryFig. S1B, right), relative to early stages of the disease (Sup-plementary Fig. S1B, left). Data from qPCR experimentsrevealed high IL-32 expression (�1.5-fold) in 48 of 66(74%) gastric cancer tissues, compared with paired non-cancerous tissues (P < 0.001; Supplementary Fig. S1C).
Because the IL-32 isoforms cannot be distinguishedusing qPCR and IHC, we further analyzed expression ofIL-32 protein in paired specimens via Western blotting
Tsai et al.
Clin Cancer Res; 20(9) May 1, 2014 Clinical Cancer Research2278
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

(Supplementary Fig. S1D). As expected, IL-32 expressionin tumor areas was higher than that in matched noncan-cerous adjacent mucosa in 3 representative patients.Notably, all IL-32 isoforms, including a, b, and g , wereexpressed in the tumor, with the b isoform as the dom-inant variant, as reported previously (15). Similar resultswere obtained from a RT-PCR assay (data not shown).To determine the association between IL-32 expression
and tumor characteristics, the IHC score for IL-32 wasanalyzed using clinicopathologic parameters. Table 1 liststhe characteristics of study patients (n ¼ 120). Tumor size(maximum diameter) was on average 5.6 cm (median, 5.2cm; range, 0.3–20 cm). Tumors were located in the prox-imal third of the stomach in 24 cases (20%),middle third in29 (24.1%), distal third in 61 (50.8%), and the wholestomach in 6 (5%). Histologic tumor types were intestinal(n¼ 42, 35%) and diffuse (n¼ 78, 65%). As defined by thedepth of wall invasion, early gastric cancer (T1) was diag-nosed in 24 (20%) cases (mucosal in 10 and submucosal in14), whereas advanced cancers (T2; muscle proper andsubserosa) was diagnosed in 18 (15%) cases, and serosa(T3) in 59 (49.1%), and invasion to adjacent organs (T4) in19 (15.8%) cases. Lymph nodemetastasis was diagnosed in87 cases (72.5%). During surgery, peritoneal seeding wasdemonstrated in 22 (18.3%) cases, and liver metastasis wasidentified in 2 (1.6%) patients. Pathologic staging wasdistributed as follows: I, 30 cases, 25%; II, 10 cases,8.3%; III, 47 cases, 39.1%; and IV, 33 cases, 27.5%.Interestingly, higher levels of IL-32were detected in T3 and
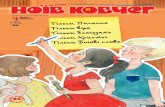
T4 groups where the serosal surface of the gastric wall wasinvaded by cancer, compared with T1 and T2 groups whereno invasion was evident (P¼ 0.016; Table 1 and Fig. 1A). Inaddition, IL-32 was significantly increased in patients withmetastasis to the lymph nodes (P ¼ 0.005; Table 1 and Fig.1B)and those at themoreadvancedpathologic stages (III andIV) of gastric cancer, compared with those in the earlierpathologic stages (I and II; P ¼ 0.011; Table 1 and Fig. 1C).Among the 120 patients, 65 died: 56 died because of
gastric cancer progression; 2 died from surgical complica-tions; and 7 died because of noncancerous causes. Medianfollow-up duration for survivors (n¼ 55) was 83.1 months(range, 64–137 months). Overall cumulative 5-year surviv-al rate for the 120 patients was 53.4%. After dichotomiza-tion based on the median IL-32 expression level, the IL-32-high group (n ¼ 73) presented significantly shorter cumu-lative survival, comparedwith the IL-32-low group (n¼ 47)using univariate analysis (Table 1 and Fig. 1D; 66.4% vs.40.4%, log-rank P ¼ 0.0045). Other factors that predictedoutcome significantly for cumulative survival in univariateanalysis included tumor location, gross type, tumor size,histologic type, depth of invasion, lymph node metastasis,distant metastasis, pathologic stage, liver metastasis, peri-toneal seeding, vascular invasion, lymphatic invasion, andperineural invasion (Table 1). Cox regression analysis (mul-tivariate)was performed todetermine theprognostic poten-tial of IL-32 independently for gastric cancer in relation tothe significant clinicopathologic parameters in univariateanalysis, including histologic type, serosal invasion, distant
metastasis, lymph node metastasis, peritoneal seeding, vas-cular invasion, lymphatic invasion, perineural invasion,gross type, and tumor size. Distant metastasis [P < 0.001;HR ¼ 3.325; 95% confidence interval (CI), 1.838–6.014],higher IL-32 expression (P ¼ 0.006; HR ¼ 2.340; 95% CI,1.277–4.290), serosal invasion (P ¼ 0.014; HR ¼ 2.893;95% CI, 1.239–6.752), and histologic type (P ¼ 0.005; HR¼ 2.918; 95% CI, 1.387–6.141) significantly emerged asindependent prognostic markers for gastric cancer in astepwise forward-conditional multivariate regression mod-el (Table 1). These data indicate IL-32 aswell as 3 pathologicparameters (distant metastasis, serosal invasion, and histo-logic type) displayed an independent prognostic value for 5-year cumulative survival. Our results support a strong asso-ciation between IL-32 expression and gastric cancer pro-gression, and support the utility of IL-32 as a useful prog-nosis marker for gastric cancer.
Ectopic expression of IL-32 in TSGH9201 cellspromotes migration and invasion
Clinicopathologic data indicate that IL-32 is involved incell invasiveness. To confirm whether IL-32 is associatedwith invasiveness of gastric cancer cell lines, we establishedstable IL-32–expressing sublines. Because all IL-32 isoformsare expressed in clinical specimens, the largest g variant thatcan be spliced into IL-32b and IL-32a (24) was introducedin TSGH9201 cells (Supplementary Fig. S2A). All cellsoverexpressing IL-32 displayed protrusions at the leadingedge and elongated spindle-like morphology, comparedwith control cells (Supplementary Fig. S2B). Based on thesemorphologic characteristics, we propose that IL-32enhances cell motility (25). Indeed, IL-32–overexpressingcells exhibited significantly higher migration (Supplemen-tary Fig. S2C) and invasive (Fig. 2A) abilities toward a serumgradient, as well as wound healing ability (SupplementaryFig. S2D), relative to control cells. Similar findings wereconsistently obtained in doxycycline-inducible IL-32–over-expressing cells (Supplementary Fig. S3A), whereby cellmigration ability was increased following induction of IL-32 with doxycycline (Supplementary Fig. S3B). Our resultsclearly indicate that IL-32 is involved in gastric cancer cellmigration and invasion.
IL-32 accelerates cell invasion through IL-8, VEGF,MMP9, and MMP2 in an AKT-dependent manner
In general, cancer cells utilize an autocrine mechanismby releasing several important factors to enhance prolifer-ation and metastasis (26). Accordingly, we investigatedwhether IL-32 induces secretory factors to facilitate gastriccancer cell invasion. Following the addition of concentrat-ed conditionedmedium to the lower Boyden chamber as achemoattractant, IL-32 and the induced secretory proteinssignificantly enhanced the invasion ability of parentalTSGH9201 cells (Supplementary Fig. S2E). To furtherdefine the chemoattractant in the IL-32–induced secre-tome, several well-known invasion-associated factors, suchas IL-8, VEGF, MMP2, and MMP9, were determined inconditioned medium. As expected, ectopic expression of
Regulation of IL-32 in Gastric Cancer
www.aacrjournals.org Clin Cancer Res; 20(9) May 1, 2014 2279
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

Table 1. Clinicopathologic correlations of IL-32 expression and 5-year survival rate in patients with gastriccancer
Univariate analysis Multivariate analysis
Parameters n Mean � SEa Pb 5-y S.R.c Log-rank Pd HR 95% CI P
Age (y)<65 58 108.7 � 6.9 0.876 45.1 0.2329�65 62 107.0 � 6.6 56.1
GenderMale 67 109.0 � 6.7 0.880 52.0 0.7656Female 53 106.4 � 6.7 48.8
LocationUpper third 24 110.0 � 8.9 0.985 52.2 0.0005Middle third 29 106.6 � 10.5 54.5Lower third 61 106.7 � 8.8 53.3Whole 6 112.7 � 24.6 0.0
Gross typeLocalized 46 99.7 � 8.4 0.095 77.4 <0.0001Infiltrative 74 112.9 � 5.6 33.4
Size<5 cm 65 102.4 � 6.8 0.187 72.3 <0.0001�5 cm 55 114.3 � 6.5 24.6
Histologic type 2.918 1.387–6.141 0.005Intestinal 42 101.3 � 8.8 0.657 77.5 <0.0001Diffuse 78 108.7 � 5.6 35.4
Depth of invasion (pT)T1 24 83.8 � 12.5 0.033 91.5 <0.0001T2 18 108.6 � 12.5 68.9T3 59 115.3 � 6.3 39.8T4 19 114.2 � 9.6 11.1
Serosal invasion 2.893 1.239–6.752 0.014No (T1, T2) 42 93.5 � 9.0 0.016 82.4 <0.0001Yes (T3, T4) 78 115.6 � 5.3 32.7
Lymph node status (pN)N0 33 88.5 � 10.5 0.024 87.4 <0.0001N1 43 115.4 � 7.4 48.2N2 23 106.5 � 10.9 43.0N3 21 124.3 � 7.3 5.0
Lymph node metastasisNo (N0) 33 88.5 � 10.5 0.005 87.4 <0.0001Yes (N1, N2, N3) 87 115.2 � 5.0 36.1
Distant metastasis (pM) 3.325 1.838–6.014 <0.001No 91 106.9 � 5.8 0.631 64.1 <0.0001Yes 29 110.7 � 7.4 5.6
Pathologic stage (pStage)I 30 84.3 � 11.2 0.007 92.7 <0.0001II 10 116.5 � 11.0 80.0III 47 121.6 � 7.5 47.6IV 33 107.0 � 6.9 4.8Stages I, II 40 92.4 � 9.1 0.011 89.4 <0.0001Stages III, IV 80 115.6 � 5.3 30.4
Liver metastasisNo 118 108.0 � 4.8 0.853 51.5 0.0135Yes 2 100.0 � 50.0 0.0
(Continued on the following page)
Tsai et al.
Clin Cancer Res; 20(9) May 1, 2014 Clinical Cancer Research2280
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

IL-32 was accompanied by induction of IL-8, VEGF, MMP2,and MMP9 expression, both at the RNA (data not shown)andprotein levels (Fig. 2B), aswell as zymographic activity ofMMP2 andMMP9 (Supplementary Fig. S2F).Next, we inves-tigated the mechanism by which IL-32 regulates invasion-associated factors. To elucidate the specific signalingpathwayunderlying IL-32–mediated expression of IL-8, IL-32–over-expressing cells were treatedwith inhibitors for the followingpathways: phosphoinositide 3-kinase (PI3K; LY294002),extracellular signal–regulated kinase (ERK; U0126), NF-kB(Bay 11-7082), and TGF-b (SB431542). LY294002, whichmarkedly inhibits PI3KdownstreamphosphorylatedAKT (p-AKT) expression (Fig. 2C), suppressed IL-32–induced IL-8mRNA(Supplementary Fig. S4) andprotein (Fig. 2C) expres-sion to a significant extent. In addition, suppressionof p-AKTactivity led todecreasedVEGF,MMP2, andMMP9expression(Fig. 2C) and inhibition of the invasive ability of IL-32–overexpressing cells (Fig. 2D). Similar results were observedby using MK-2206, a highly selective non-ATP competitiveallosteric Akt inhibitor, toblockAKT activity (SupplementaryFig. S5). Our results collectively indicate that AKT activationby IL-32 is required to induce IL-8, VEGF,MMP2, andMMP9expression for cell invasion.
Active b-catenin is a downstream effector of phospho-AKT in IL-32–induced cell invasionNext, we investigated the mechanism underlying AKT-
dependent invasiveness in IL-32–overexpressing cells. Acti-vated AKT is capable of phosphorylating and inactivating
GSK3b, resulting in nuclear translocation and activation ofb-catenin (27). Several studies have reported that b-cateninregulates IL-8, VEGF, MMP2, and MMP9 expression (28,29), and acts as a major pathway frequently altered inhuman gastric cancer (30). Accordingly, we hypothesizedthat b-catenin operates in IL-32-phospho-AKT signaling.Interestingly, expression of active b-catenin was dramati-cally increased in the nuclei of IL-32–overexpressing cells inwhich p-AKT was activated as well as the intermediateregulator, phospho-GSK-3b (Fig. 3A). This finding wasfurther confirmed using doxycycline-inducible IL-32–over-expressing cells in which active nuclear b-catenin wasincreased via inducing IL-32 production over a short periodof time, compared with empty vector control cells (Supple-mentary Fig. S4A). To provide evidence of the mechanisticrole of b-catenin on the regulation of IL-32/p-AKT–inducedIL-8, VEGF,MMP2, andMMP9, we transduced vector- or IL-32–overexpressing TSGH cells with short hairpin RNAs(shRNA) targeting b-catenin (shb-catenin), IL-8 (shIL8), orluciferase control (shLuc), using the lentiviral delivery sys-tem. Silencing of b-catenin or IL-8 led to a dramatic decreasein IL-32–induced VEGF,MMP2, andMMP9 expression, buthad little effect on the endogenous level (Fig. 3B). Notably,IL-32–induced IL-8 was additionally decreased by silencingb-catenin, whereas knockdown of IL-8 did not affect activeb-catenin expression, implying that b-catenin regulates IL-8production in IL-32- overexpressing cells. LY294002 treat-ment suppressed active b-catenin expression (Fig. 2C),whereas, in contrast, p-AKT expression was not affected by
Table 1. Clinicopathologic correlations of IL-32 expression and 5-year survival rate in patients with gastriccancer (Cont'd )
Univariate analysis Multivariate analysis
Parameters n Mean � SEa Pb 5-y S.R.c Log-rank Pd HR 95% CI P
Peritoneal seedingNo 98 107.1 � 5.5 0.688 60.4Yes 22 110.9 � 8.3 0.0 <0.0001
Vascular invasionNo 95 107.1 � 5.6 0.654 59.6 <0.0001Yes 25 110.8 � 7.6 12.2
Lymphatic invasionNo 48 101.4 � 9.0 0.123 76.2 <0.0001Yes 72 112.2 � 5.1 32.6
Perineural invasionNo 76 106.8 � 6.3 0.682 63.7 0.0002Yes 44 109.6 � 6.9 28.4
IL-32 (IHC score) 2.34 1.277–4.29 0.006<100 (median) 47 56.4 � 3.5 <0.001 66.4 0.0045�100 73 141.0 � 4.1 40.4
NOTE:HRs, 95%CI, andP valueswere generated using aCoxproportional hazard analysis. Boldface indicates statistical significance.aIHC scores.bMann–Whitney test.cFive-year survival rate.dLog-rank test.
Regulation of IL-32 in Gastric Cancer
www.aacrjournals.org Clin Cancer Res; 20(9) May 1, 2014 2281
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

introducing either b-catenin or IL-8 shRNA (Fig. 3B). Thedata indicate that b-catenin and IL-8 act as downstreamtargets of p-AKT in the IL-32 signaling pathway and induceVEGF,MMP2, andMMP9production. To determinewheth-er active b-catenin and IL-8 are required for IL-32–inducedcell invasiveness, we performed an invasion assay withb-catenin or IL-8 knockdown cells. Consistent with theirwell-established role in cancer cell invasion, depletion ofb-catenin and IL-8 significantly suppressed IL-32–inducedmatrix invasion ability, but had little effect on invasivenessof control cells (Fig. 3C). Interestingly, elongated IL-32–overexpressing cells was partly restored to a round shapeupon b-catenin knockdown, but not IL-8 depletion (Fig.3D). Taken together, these results indicate that IL-32enhances the activity of AKT, and subsequent b-cateninactivation results in the production of IL-8, VEGF, MMP2,and MMP9 to promote cell invasion.
Silencing of IL-32 reduces the invasive ability of humangastric cancer cells mediated via inactivation of thep-AKT/b-catenin pathway
To investigate the significance of IL-32 in gastric cancermetastasis, we transduced AGS or TSGH cells with 2 inde-pendent shRNAs targeting human IL-32. Introduction ofIL-32 siRNA resulted in reduced IL-32 expression (Supple-mentary Fig. S6A and S6B), and more importantly, was
accompanied by decreased cell invasion, compared withshLuc control, in both gastric cancer cell lines (Fig. 4A andB). Consistent with the molecular changes in IL-32–over-expressing cells, IL-32 silencing resulted in decreasedexpression of p-AKT, active b-catenin, IL-8, and VEGF (Fig.4C). We additionally re-expressed a siRNA-resistant formof IL-32 by introducing a silent mutation in the siRNAtarget region into IL-32 knockdown cells. Immunoblotanalyses confirmed that expression of IL-32 is restored tothe control cell level (Supplementary Fig. S6A). Asexpected, re-expression of IL-32 was sufficient to restorethe invasive properties of TSGH IL-32 knockdown cells(Fig. 4A). Next, we compared in vivo metastasis formationof TSGH shLuc control and IL-32 knockdown cells tofurther establish the relationship between IL-32 expressionlevels and metastasis formation. Following injection ofcells into the tail vein of immunodeficientmice for 5weeks,the number of experimental lung metastatic nodules wasexamined macroscopically and microscopically for theoccurrence of metastasis. The number decreased signifi-cantly in animals injected with IL-32 knockdown cells,comparedwith those injected with shLuc control cells (Fig.4D). Our results clearly show that silencing of IL-32decreases invasive activity in vitro and pulmonary meta-static potential to a substantial extent in vivo in humangastric cancer cells.
300
200
100
0T1 T2Depth of wall invasion (pT)
A B
C D
T3 T4
I IIPathological stage (pStage)
Postoperative monthsIII IV0 12 24 36 48 60 72
N0 N1Lymph node metastasis (pN)
N2 N3
IL-3
2 e
xp
ressio
n (
IHC
sco
re)
300
200
100
0
IL-3
2 e
xp
res
sio
n (
IHC
sco
re) 1.0
0.8
0.6
0.4
0.2
0.0
Cu
mu
lati
ve
su
rviv
al
300
200
100
0
IL-3
2 e
xp
ressio
n (
IHC
sco
re)
Lower expression (n = 47)
Higher expression (n = 73)
Cutoff point = 100 (IL-32 IHC score)
Log-rank P = 0.0045
Figure 1. IL-32 overexpression inhuman gastric cancer is correlatedwith prognosis of patients. A,scatter plot of IL-32 IHC scoresaccording to depth of wall invasion(�, P ¼ 0.016, T1–T2 vs. T3–T4). B,scatter plot of IL-32 IHC scoresaccording to lymph nodemetastasis (���, P ¼ 0.005, N0 vs.N1–3). C, scatter plot of IL-32 IHCscores according to pathologicstage (��, P ¼ 0.011, stage I–II vs.stage III–IV). D, Kaplan–Meiersurvival curves of 2 groups ofpatients with gastric cancerdefined by an IL-32 expressionlevel cutoff value of 100 (themedian), established on the basisof IHC scores. The 5-year survivalrateof the lower expressiongroups(n ¼ 47) was significantly betterthan that of the higher expressiongroups (n ¼ 73; 66.4% vs. 40.4%;log-rank P ¼ 0.0045).
Tsai et al.
Clin Cancer Res; 20(9) May 1, 2014 Clinical Cancer Research2282
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

IL-32, CTTNB1 (b-catenin), IL-8, VEGF-A, MMP2, andMMP9 are coexpressed in human gastric malignanciesTo determine the clinical significance of the IL-32/b-cate-
nin/IL-8/VEGF/MMP2/MMP9 axis, we examined whetherthe observed correlation between IL-32 and these down-stream effectors could be extended to human gastric cancer.Usingoncomine, expression values for IL-32,CTTNB1, IL-8,VEGF-A, MMP2, and MMP9 were regained from the pub-lished Cho gastric microarray dataset (GEO accession:GSE13861; ref. 31). Spearman analysis performed on theplotted mRNA expression values revealed a significantlymoderate correlation between expression of IL-32 and itsdownstream effectors in 65 gastric adenocarcinoma speci-
mens (Fig. 5A and Supplementary Fig. S7). However, thisfinding remains to be experimentally confirmed. Furtherimmunohistochemical analysis for IL-32 and IL-8 in 85cases of gastric cancer disclosed a significantly moderatecorrelation between IL-32 and IL-8 (Fig. 5B and C; Spear-man r ¼ 0.562, P < 0.001). These results strongly suggestthat the regulation of CTTNB1 (b-catenin), IL-8, VEGF-A,MMP2, andMMP9 by IL-32occurs not only in gastric cancercell lines in vitro, but also human gastric tumors in vivo.
DiscussionGastric cancer is the second most common cause of
cancer-induced death worldwide. The prognosis in the late
Figure 2. Ectopic overexpression ofIL-32 increases IL-8, VEGF, MMP2,MMP9 expression as well asTSGH9201 cell invasion in aphospho-AKT–dependent manner.Three IL-32–overexpressingsublines (IL-32-pool, IL-32-1, andIL-32-2) and 2 control lines (v1 andv2) were established using parentalTSGH9201 cells. A, quantificationof serum-induced transwellinvasion (4 � 105 cells) by IL-32–overexpressing and control cells.The toppanel shows representativemicroscopic images of transwells.Magnification, �40. The scale barrepresents 500 mm (mean� SEM; 3independent experiments) �, P <0.05; ��, P < 0.01. B, IL-8, VEGF,MMP2, and MMP9 proteinexpression in the supernatant ofIL-32–overexpressing and controlcells. Fascin1wasusedasa loadingcontrol. C, V1 and IL-32-2 cellswere treated with vehicle (dimethylsulfoxide) or LY294002 (LY) for 48hours. Expression of the indicatedmolecules was detected viaWestern blotting. b-Actin andfascin1 were used as loadingcontrols of cytosolic and secretedproteins, respectively. D, aftertreatment, cells were analyzed withthe invasion assay, presented as ahistogram. The top panel showsrepresentative microscopic imagesof transwells. Magnification, �40.The scale bar represents 500 mm.��, P < 0.01. One-way ANOVA withTukey multiple comparison tests(mean � SEM; 3 independentexperiments).
Regulation of IL-32 in Gastric Cancer
www.aacrjournals.org Clin Cancer Res; 20(9) May 1, 2014 2283
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

Tsai et al.
Clin Cancer Res; 20(9) May 1, 2014 Clinical Cancer Research2284
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

stage of gastric cancer remains extremely poor, and mediansurvival rarely approaches 1 year, mainly because of metas-tasis (32). No effective therapeutic targets have been iden-tified to date. Themost important objective of gastric cancerresearch is to elucidate the molecular mechanism(s) under-lying metastasis.IL-32 was overexpressed in gastric cancer, whereas expres-
sion was significantly low in nontumor mucosa, as describedpreviously (7). IL-32 expression in tumors from the Chogastric microarray dataset was higher than that in nontumorspecimens, in keeping with our data. The mechanism under-lying IL-32 overexpression in gastric cancer is unclear atpresent. It has been reported that chromosome 16p13.3region, which contains the IL-32 gene is frequently amplifiedin breast and small intestine cancer (33, 34). The abovefindings provide implications of IL-32 dysregulation in themechanism of gastric cancer development, but more exper-imental evidence is needed to confirm this hypothesis. In ouranalyses, Kaplan–Meier survival analysis showed that higherIL-32 expression is significantly associated with poor prog-nosis of patients with gastric cancer. IL-32 was additionallyidentified as an independent prognostic marker in multivar-iate analysis in parallel with the known clinical and patho-logic factors for gastric cancer. Further analysis of the predic-tive potential of IL-32 expression supported its utility as apredictor to identify aggressive gastric cancer, consistent withboth Kaplan–Meier and Cox regression analyses. This studyprovides evidence that IL-32 is auseful independentbiomark-er for prognosis. Shortly before the publication of this article,a study also found higher IL-32 expression is correlated withpoor postoperative outcomes of patients with gastric cancer(8). Although that study only focused on clinical significance,the findings lend support to our claim of the importance ofthe regulation and function of IL-32 in gastric cancer.Ectopic expression of the largest g variant of IL-32, which
can be spliced into IL-32b and IL-32a in gastric cancer cells,leads to spindle-like morphology and increased cell migra-tion ability. Analogous results were obtained upon ectopicexpression of the b variant of IL-32, which generated both band a isoforms without the g isoform (data not shown).These results imply that all IL-32 isoforms may have similarfunctions in cellmigration. Amore recent study showed thatIL-32 contains an RGD motif that potentially binds to andactivates integrins and focal adhesion kinase (FAK) essentialfor cell anchorage and migration, consistent with our find-ings (35). Previous studies have identified Rac1 as an impor-tant downstreamcomponent of integrin/FAKsignaling (30).Accordingly, we hypothesize that IL-32 induces integrin andRac1 activation to enhance cellmigration ability.Our experi-ments showed that the Rac1-specific guanine nucleotide
exchange factor, Tiam1, is upregulated in IL-32–overexpres-sing cells. Furthermore, IL-32–induced cell migration wasabolished by a selective Rac1/Tiam1 inhibitor, NSC23766(Supplementary Fig. S8). However, activation of the Wnt/b-catenin pathway has also been shown to trigger changes inepithelial cell morphology (e.g., epithelial-mesenchymaltransition) and activate migration and invasion (36).Accordingly, downregulation of b-catenin in IL-32–overex-pressing cells partly reversed IL-32–induced cell elongation.Together, these results give possible molecular mechanismsby which IL-32 induce cell migration.
Data from this study indicate that IL-32 triggers cell inva-sion partially by inducing IL-8, VEGF, MMP2, and MMP9expression, resulting in degradation of the extracellularmatrix. These results are in line with previous findings show-ing that IL-32 is associatedwith acquisitionof an invasive andmetastasis phenotype in lung cancer mediated via coexpres-sion of IL-8 and VEGF (9). Furthermore, IL-8 and VEGF arewell defined pro-angiogenic and pro-metastatic factors innumerous human cancers. Ectopic expression of IL-32 isaccompanied by hypoxia-inducible factors 1a (HIF-1a) acti-vation, one of the most powerful regulators of angiogenesis(Supplementary Fig. S9). Furthermore, depletion of HIF-1adecreased IL-32–induced cell invasion and IL-8, VEGF,MMP9, MMP2 expression (Supplementary Fig. S9B andS9C). However, the expression of IL-32–induced phospho-AKT and activeb-catenin did not changebyHIF-1a depletion(Supplementary Fig. S9B). In addition, the expression of IL-32–induced HIF-1a also did not change by b-catenin or IL-8depletion (Supplementary Fig. S9D). Notably, both activeb-catenin and HIF-1a were inhibited whereas AKT was inac-tivated by MK-2206 (Supplementary Fig. S5A). Therefore,both b-catenin and HIF-1a involve in IL-32–induced cellinvasion under phospho-AKT activation. Other investigatorshave demonstrated an involvement of IL-32 in the regulationof IL-8 in endothelial cells, indicative of a role inmodulationof endothelial function (37). The results collectively supportan important role of IL-32 in angiogenesis in gastric cancer.
To our knowledge, this study has shown for the first timethat IL-32 stimulates activation of AKT and b-catenin as wellas HIF-1a to induce IL-8, VEGF, MMP2, and MMP9 secre-tion for gastric cancer metastasis (Fig. 5D). Clearly, p-AKT,activated b-catenin as well as HIF-1a are upstream regula-tors of IL-8 expression. However, we cannot exclude thepossibility of cross-talk signaling between IL-8, VEGF,MMP2, andMMP9. Previous studies have reported suppres-sion of IL-1b, TNF-a, and INF-g–induced IL-32a expressionvia inhibition of the PI3K/AKT pathway in myofibroblasts(38). Gastric cancer cellsmay use the positive feedback loopto activate the PI3K/AKT pathway for cancer progression.
Figure 3. IL-32 induces IL-8, VEGF-A, MMP2, and MMP9 expression via b-catenin activation. A, expression of indicated molecules in IL-32–overexpressingand control cells was detected via Western blotting. B, expression of indicated proteins in v1 and IL-32-2 cells transfected with the gene silencers,shLuciferase (shLuc), b-catenin shRNA (shb-catenin), or IL-8 shRNA (shIL8), was detected using Western blotting. C, invasion assay of indicated cells wasperformed. Magnification, �100. Scale bar represents 200 mm. Quantified results are presented as a histogram in the right panel. One-way ANOVA withTukey multiple comparison tests (mean � SEM; 3 independent experiments). ��, P < 0.01. D, quantification of cells displaying elongated morphology.Elongation is presented as a percentage (mean� SEM; 3 independent experiments, n > 400) of cells with a length of more than 3 times the width. �, P < 0.05.Left: representative phase-contrast images. The arrows indicate the presence of a spindle shape. Magnification, �400. Scale bar represents 50 mm.
Regulation of IL-32 in Gastric Cancer
www.aacrjournals.org Clin Cancer Res; 20(9) May 1, 2014 2285
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

Figure 4. Depletion of IL-32 in gastric cancer cell lines reduces invasion ability in vitro and in vivo. A, invasion properties of the indicated cells (6 � 105)were analyzed. Magnification, �100. Scale bar represents 200 mm. Quantified results are presented as a histogram in the right panel. One-way ANOVA withTukey multiple comparison tests (mean � SEM; 3 independent experiments). �, P < 0.05; ���, P < 0.001. B, the invasive properties of indicated cellswere examined. Magnification,�100. Scale bar represents 200 mm. Quantified results are presented as a histogram in the right panel. One-way ANOVA withTukey multiple comparison tests (mean � SEM; 3 independent experiments). ���, P < 0.001. C, expression of indicated molecules in control or IL-32knockdownTSGHcellswasdetected viaWestern blotting.D, top:H&Estaining ofmetastatic lesions upon intravenous administrationof shLuc-1,KD-IL-32-1,and KD-IL-32-2 cells (1 � 106) into SCID mice. Microscopic images of the lung tumor nodules indicated with arrowheads. Magnification, �100. Scale barrepresents 200 mm. Bottom: lung sections of tumor-bearing mice were microscopically analyzed, and metastases per histologic section counted.N ¼ 4; �, P < 0.05; ��, P < 0.01; ���, P < 0.001.
Clin Cancer Res; 20(9) May 1, 2014 Clinical Cancer Research2286
Tsai et al.
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

In summary, significant overexpression of IL-32 wasobserved in gastric cancer, suggesting a critical role indevelopment and progression to malignancy. IL-32 maybe a useful independent prognostic tumor marker to pre-dict survival and metastasis of gastric cancer patients. Ourfindings collectively provide evidence that IL-32 functionsas a potential therapeutic target and support its utility as auseful independent prognostic marker of patient survival.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: C.-Y. Tsai, C.-S. Wang, Y.-H. Tseng, K.-H. LinDevelopment of methodology:M.-M. Tsai, H.-C. Chi, J.-I. Wu, L.-H. WangAcquisitionofdata (provided animals, acquired andmanagedpatients,provided facilities, etc.): C.-S. Wang, C.-Y. Chen, C.D. LinAnalysis and interpretation of data (e.g., statistical analysis, biosta-tistics, computational analysis): C.-S. Wang, M.-M. Tsai, W.-L. Cheng,C.-Y. Chen, K.-H. Lin
Writing, review, and/or revision of the manuscript: C.-Y. Tsai, C.-S.Wang, K.-H. LinAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases): H.-C. Chi, Y.-H. Tseng, K.-H. LinStudy supervision: C.-Y. Tsai, K.-H. Lin
AcknowledgmentsThe authors thankDr. Y. Liang for immunohistochemistry andpathologic
comments.
Grant SupportThis work was supported by grants from Chang-Gung University,
Taoyuan, Taiwan (CMRPG6B0011, NMRP 170441), and the National Sci-enceCouncil of theRepublic ofChina (NSC92-2314-B-182-077; 97-2314-B-182-009-MY2; 100-2314-B-182A-074).
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received May 9, 2013; revised December 19, 2013; accepted January 25,2014; published OnlineFirst March 6, 2014.
Figure 5. IL-32 is correlated withIL-8, VEGF-A, MMP2, MMP9,and CTNNB1 in human gastriccancer. A, heat map of expressionprofiles for IL-32, IL-8, VEGF-A,MMP2, MMP9, and CTNNB1(b-catenin) of 65 human gastricadenocarcinomas from anoncomine microarray dataset (asindicated in the figure). Spearmanrank correlation coefficient ofindividual genes with IL-32 shownin the left. B, representativepositive and negative staining ofIL-32 and IL-8 in human gastriccancer tissue sections.Magnification, �200. Scale barrepresents 100 mm. C, IL-32 andIL-8 IHC scores were plotted onthe basis of expression values.Spearman rank correlationcoefficients between IHC scores ofIL-8 (y-axis) and IL-32 (x-axis) in85 clinical specimens wereanalyzed. Spearman r ¼ 0.562,P < 0.001. D, proposed modelrepresenting the prometastaticeffect of IL-32 in the pathogenesisof gastric cancer.
www.aacrjournals.org Clin Cancer Res; 20(9) May 1, 2014 2287
Regulation of IL-32 in Gastric Cancer
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

References1. Jemal A, Siegel R, Ward E, Hao Y, Xu J, Murray T, et al. Cancer
statistics, 2008. CA Cancer J Clin 2008;58:71–96.2. Health Registry Annual Report 2010, Republic of China. Taipei City,
Taiwan, R.O.C: Bureau of Health Promotion, Department of Health,Executive Yuan; 2012.
3. Tsujimoto H, Ono S, Ichikura T, Matsumoto Y, Yamamoto J, Hase K.Roles of inflammatory cytokines in the progression of gastric cancer:friends or foes? Gastric Cancer 2010;13:212–21.
4. ZhaoZS,WangYY,ChuYQ,YeZY, TaoHQ.SPARC is associatedwithgastric cancer progression and poor survival of patients. Clin CancerRes 2010;16:260–8.
5. Tahara E. Molecular aspects of invasion and metastasis of stomachcancer. Verh Dtsch Ges Pathol 2000;84:43–9.
6. Bachelder RE, Wendt MA, Mercurio AM. Vascular endothelial growthfactor promotes breast carcinoma invasion in an autocrine manner byregulating the chemokine receptor CXCR4. Cancer Res 2002;62:7203–6.
7. Seo EH, Kang J, Kim KH, Cho MC, Lee S, Kim HJ, et al. Detection ofexpressed IL-32 in human stomach cancer using ELISA and immu-nostaining. J Microbiol Biotechnol 2008;18:1606–12.
8. Ishigami S, Arigami T, Uchikado Y, Setoyama T, Kita Y, Sasaki K, et al.IL-32 expression is an independent prognostic marker for gastriccancer. Med Oncol 2013;30:472.
9. Sorrentino C, Di Carlo E. Expression of IL-32 in human lung cancer isrelated to the histotype and metastatic phenotype. Am J Respir CritCare Med 2009;180:769–79.
10. Nishida A, Andoh A, Inatomi O, Fujiyama Y. Interleukin-32 expressionin the pancreas. J Biol Chem 2009;284:17868–76.
11. Kang YH, Park MY, Yoon DY, Han SR, Lee CI, Ji NY, et al. Dysregula-tion of overexpressed IL-32a in hepatocellular carcinoma suppressescell growth and induces apoptosis through inactivation of NF-kB andBcl-2. Cancer Lett 2012;318:226–33.
12. Yousif NG,Al-Amran FG,HadiN, Lee J,Adrienne J. Expressionof IL-32modulates NF-kB and p38 MAP kinase pathways in human esoph-ageal cancer. Cytokine 2013;61:223–7.
13. Kim SH, Han SY, Azam T, Yoon DY, Dinarello CA. Interleukin-32: acytokine and inducer of TNF-a. Immunity 2005;22:131–42.
14. Choi JD, Bae SY, Hong JW, Azam T, Dinarello CA, Her E, et al.Identification of the most active interleukin-32 isoform. Immunology2009;126:535–42.
15. Shoda H, Fujio K, Yamamoto K. Rheumatoid arthritis and interleukin-32. Cell Mol Life Sci 2007;64:2671–9.
16. Novick D, Rubinstein M, Azam T, Rabinkov A, Dinarello CA, Kim SH.Proteinase 3 is an IL-32 binding protein. Proc Natl Acad Sci U S A2006;103:3316–21.
17. Netea MG, Azam T, Ferwerda G, Girardin SE, Walsh M, Park JS, et al.IL-32 synergizes with nucleotide oligomerization domain (NOD) 1 andNOD2 ligands for IL-1b and IL-6 production through a caspase 1-dependentmechanism. ProcNatl Acad Sci USA2005;102:16309–14.
18. Japanese Gastric Cancer A. Japanese classification of gastric carci-noma—2nd English edition. Gastric Cancer 1998;1:10–24.
19. ShihCH,Chen SL, YenCC, HuangYH,ChenCD, LeeYS, et al. Thyroidhormone receptor-dependent transcriptional regulation of fibrinogenand coagulation proteins. Endocrinology 2004;145:2804–14.
20. Wang CL, Wang CI, Liao PC, Chen CD, Liang Y, Chuang WY, et al.Discovery of retinoblastoma-associated binding protein 46 as a novelprognostic marker for distant metastasis in nonsmall cell lung cancerby combined analysis of cancer cell secretome and pleural effusionproteome. J Proteome Res 2009;8:4428–40.
21. Wang CS, Lin KH, Chen SL, Chan YF, Hsueh S. Overexpression ofSPARC gene in human gastric carcinoma and its clinic-pathologicsignificance. Br J Cancer 2004;91:1924–30.
22. Cheng WL, Wang CS, Huang YH, Tsai MM, Liang Y, Lin KH. Over-expression of CXCL1 and its receptor CXCR2 promote tumor invasionin gastric cancer. Ann Oncol 2011;22:2267–76.
23. Cheng WL, Wang CS, Huang YH, Liang Y, Lin PY, Hsueh C, et al.Overexpression of a secretory leukocyte protease inhibitor in humangastric cancer. Int J Cancer 2008;123:1787–96.
24. Heinhuis B, Koenders MI, van de Loo FA, Netea MG, van den BergWB, Joosten LA. Inflammation-dependent secretion and splicing ofIL-32g in rheumatoid arthritis. Proc Natl Acad Sci U S A 2011;108:4962–7.
25. Sanz-Moreno V, Gadea G, Ahn J, Paterson H, Marra P, Pinner S, et al.Rac activation and inactivation control plasticity of tumor cell move-ment. Cell 2008;135:510–23.
26. YoungsSJ, Ali SA, TaubDD, ReesRC.Chemokines inducemigrationalresponses in human breast carcinoma cell lines. Int J Cancer 1997;71:257–66.
27. Pap M, Cooper GM. Role of glycogen synthase kinase-3 in thephosphatidylinositol 3-kinase/Akt cell survival pathway. J Biol Chem1998;273:19929–32.
28. Levy L, Neuveut C, Renard CA, Charneau P, Branchereau S, GauthierF, et al. Transcriptional activation of interleukin-8 by b-catenin-Tcf4.J Biol Chem 2002;277:42386–93.
29. Doyle JL,Haas TL. Differential role ofb-catenin in VEGFand histamine-induced MMP-2 production in microvascular endothelial cells. J CellBiochem 2009;107:272–83.
30. Clements WM, Wang J, Sarnaik A, Kim OJ, MacDonald J, Fenoglio-Preiser C, et al. b-Cateninmutation is a frequent cause ofWnt pathwayactivation in gastric cancer. Cancer Res 2002;62:3503–6.
31. Cho JY, Lim JY, Cheong JH, Park YY, Yoon SL, Kim SM, et al. Geneexpression signature-based prognostic risk score in gastric cancer.Clin Cancer Res 2011;17:1850–7.
32. Catalano V, Labianca R, Beretta GD, Gatta G, de Braud F, Van CutsemE. Gastric cancer. Crit Rev Oncol Hematol 2009;71:127–64.
33. Naylor TL, Greshock J, Wang Y, Colligon T, Yu QC, Clemmer V, et al.High resolution genomic analysis of sporadic breast cancer usingarray-based comparative genomic hybridization. Breast Cancer Res2005;7:R1186–98.
34. Diosdado B, Buffart TE, Watkins R, Carvalho B, Ylstra B, Tijssen M,et al. High-resolution array comparative genomic hybridization insporadic and celiac disease-related small bowel adenocarcinomas.Clin Cancer Res 2010;16:1391–401.
35. Heinhuis B, Koenders MI, van den Berg WB, Netea MG, Dinarello CA,Joosten LA. Interleukin 32 (IL-32) contains a typical a-helix bundlestructure that resembles focal adhesion targeting region of focaladhesion kinase-1. J Biol Chem 2012;287:5733–43.
36. Sanchez-Tillo E, de Barrios O, Siles L, Cuatrecasas M, Castells A,Postigo A. b-Catenin/TCF4 complex induces the epithelial-to-mesen-chymal transition (EMT)-activator ZEB1 to regulate tumor invasive-ness. Proc Natl Acad Sci U S A 2011;108:19204–9.
37. Nold-Petry CA, Nold MF, Zepp JA, Kim SH, Voelkel NF, Dinarello CA.IL-32-dependent effects of IL-1b on endothelial cell functions. ProcNatl Acad Sci U S A 2009;106:3883–8.
38. Nishida A, Andoh A, Shioya M, Kim-Mitsuyama S, Takayanagi A,Fujiyama Y. Phosphatidylinositol 3-kinase/Akt signaling mediatesinterleukin-32a induction in human pancreatic periacinar myofibro-blasts. Am J Physiol Gastrointest Liver Physiol 2008;294:G831–8.
Clin Cancer Res; 20(9) May 1, 2014 Clinical Cancer Research2288
Tsai et al.
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221

2014;20:2276-2288. Published OnlineFirst March 6, 2014.Clin Cancer Res Chung-Ying Tsai, Chia-Siu Wang, Ming-Ming Tsai, et al. Associated with Tumor Progression and MetastasisInterleukin-32 Increases Human Gastric Cancer Cell Invasion
Updated version
10.1158/1078-0432.CCR-13-1221doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2014/03/07/1078-0432.CCR-13-1221.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/20/9/2276.full#ref-list-1
This article cites 37 articles, 14 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/20/9/2276.full#related-urls
This article has been cited by 3 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/20/9/2276To request permission to re-use all or part of this article, use this link
on April 17, 2020. © 2014 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst March 6, 2014; DOI: 10.1158/1078-0432.CCR-13-1221