Interferon Gamma Release Assays in Denmark, population ......Interferon Gamma Release Assays in...
32
UNIVERSITY OF COPENHAGEN FACULTY OF HEALTH AND MEDICAL SCIENCES PhD thesis Thomas Stig Hermansen Interferon Gamma Release Assays in Denmark, population-based studies from a tuberculosis low-incidence country Academic supervisors: Pernille Ravn and Troels Lillebaek Submitted to the University of Copenhagen April 15 th 2016
Transcript of Interferon Gamma Release Assays in Denmark, population ......Interferon Gamma Release Assays in...

U N I V E R S I T Y O F C O P E N H A G E N
F A C U L T Y O F H E A L T H A N D M E D I C A L S C I E N C E S
PhD thesis
Thomas Stig Hermansen
Interferon Gamma Release Assays in
Denmark, population-based studies from a
tuberculosis low-incidence country
Academic supervisors: Pernille Ravn and Troels Lillebaek
Submitted to the University of Copenhagen April 15th 2016

PhD Thesis Thomas Stig Hermansen
1
ACADEMIC SUPERVISORS:
Pernille Ravn, MD, PhD
Department of Pulmonary and Infectious Diseases, Nordsjaellands Hospital, Hillerød, University
of Copenhagen, Hillerød, Denmark
Troels Lillebaek, MD, DMSc
International Reference Laboratory of Mycobacteriology, Statens Serum Institut, Copenhagen, Denmark
EVALUATION COMMITTEE
Chair
Ole Kirk, MD, DMSc
Department of Infectious Diseases, Copenhagen University Hospital Rigshospitalet, Denmark
Assessors
Christian Wejse, MD, PhD
Department of Infectious Diseases, Aarhus University Hospital, Skejby, Denmark
Frank van Leth, MD, MSc, PhD
Amsterdam Institute for Global Health and Development, Netherlands
This thesis was handed in April 15th 2016 for evaluation at the University of Copenhagen. The PhD
defence will take place at Copenhagen University Hospital, Hillerød, June 27th 2016, 14.00 at the
auditorium.
The PhD defense will take place Copenhagen University Hospital, Hillerød, at the 15 th
of September etcetc

PhD Thesis Thomas Stig Hermansen
2
PUBLICATIONS (referred to by their roman numerals in the text)
STUDY I (1)
Hermansen TS, Thomsen VO, Lillebaek T, Ravn P. Non-Tuberculous Mycobacteria and the
Performance of Interferon Gamma Release Assays in Denmark. PLoS One 2014 Apr
4;9(4):e93986.
STUDY II (2)
Hermansen TS, Lillebaek T, Hansen AB, Andersen PH, Ravn P. QuantiFERON-TB Gold In-Tube
test performance in Denmark. Tuberculosis 2014 Dec;94(6):616-621.
STUDY III (3)
Hermansen TS, Lillebaek T, Kristensen KL, Andersen PH, Ravn P. Prognostic value of
interferon-γ release assays, a population-based study from a TB low-incidence country.
Thorax 2016 Mar 30.

PhD Thesis Thomas Stig Hermansen
3
CONTENTS
PREFACE .......................................................................... 4
Acknowledgements ................................................................. 4
Abbreviations .......................................................................... 5
Funding .................................................................................... 5
INTRODUCTION .............................................................. 6
1. BACKGROUND ............................................................. 7
1.1. The TB spectrum ............................................................. 7
1.2. Diagnosis of active TB .................................................... 8
1.3. Diagnosis of latent TB .................................................... 8
1.4. Interferon gamma release assays ………….................. 9
1.5. QuantiFERON-TB Gold In-Tube Test ...................... 10
1.6. Non-tuberculous mycobacteria ................................... 10
2. OBJECTIVES .............................................................. 12
3. METHODOLOGICAL CONSIDERATIONS .......... … 13
3.1. Settings, design and populations ...................…..……… 13
3.2. Data sources .................................................................. 13
3.3. Statistics ......................................................................... 14
4. MAIN RESULTS ......................................................... 16
4.1. Study I .............................................................................. 16
4.2. Study II............................................................................. 16
4.3. Study III ........................................................................... 16
5. DISCUSSION ............................................................... 18
5.1. QFT Performance…….……..……................................. 18
5.2. Non-tuberculous mycobacteria .................................... 18
5.3. QFT performance in extreme age groups .................. 19
5.4. Predictive value of the QFT .......................................... 20
6. LIMITATIONS ................................................... ……. 21
6.1. Bias ................................................................................ . 21
6.2. QFT variability ............................................................ 21
6.3. QFT reproducibility and repeat indeterminate
tests…. .................................................................................. 22
6.4. Screening indication.................................................... 22
7. PERSPECTIVES ........................................................ 22
7.1. The local perspective, IGRA use in Denmark ....... .. 22
7.2. The global perspective, IGRA use worldwide ....... .. 23
7.3. The future .................................................................... .. 23
SUMMARY ...................................................................... 25
DANSK RESUME ........................................................... 26
REFERENCES ................................................................ 27
STUDY I .......................................................................... 32
STUDY II ......................................................................... 41
STUDY III ....................................................................... 48

PhD Thesis Thomas Stig Hermansen
4
PREFACE
ACKNOWLEDGEMENTS
This thesis would not have been possible without the help
and support from a number of people.
Pernille Ravn, the principal supervisor, has been
indispensable in planning the articles on which this thesis is
based. I am grateful for all your encouragement, guidance,
constructive criticism and introduction to the world of TB.
Troels Lillebaek, director for IRLM, my daily work place
throughout the majority of this thesis, has provided valuable
help always finding time for advice and fruitful discussion.
Thank you for providing an inspiring environment for young
researchers to learn and grow.
I am grateful to my colleagues at the PhD office, Mathias
Klok Pedersen, Dorte Bek Folkvardsen, Julie Prahl and
Karen Bjoern-Mortensen. We have created a fantastic
working environment that I will surely miss in the future.
I am indebted to Erik Svensson and Michael Rasmussen for
sparring, always keeping a door open to discuss R statistics,
data extracts or something else completely.
The Department of Pulmonary and Infectious Diseases,
Nordsjaellands Hospital, Hillerød, has provided me with the
opportunity to initiate this PhD and enrol as a PhD student.
Thanks to the entire department, in particular the research
group at LIA: Dorthe, Ellen, Andreas, Pelle, Stine, Gertrud,
Camilla and Kristina for sparring and exchange of ideas on
research meetings and conferences around the world.
Thanks to the staff at IRLM, for putting up with me through
the last years and for always being willing to assist.
The former director for IRLM, Vibeke Østergaard Thomsen,
gave me the opportunity to use data from the department
and perform the projects in this thesis; for that I am very
grateful. Peter H. Andersen has been very valuable in
providing data extracts regarding notified TB cases.
Last, but most important, I am grateful to my friends and
family, Louise, Sebastian, Karl August and Selma, for
putting everything into perspective and having made my life
enjoyable and versatile outside the world of TB for the last
three years.
Thomas Stig Hermansen, April 2016

PhD Thesis Thomas Stig Hermansen
5
ABBREVIATIONS
AFS – Acid Fast Staining
ATS – American Thoracic Society
BCG – Bacille Calmette-Guérin
CDC – Centers for Disease Control and Prevention
CI – Confidence Interval
CFP-10 – Culture Filtrate Protein-10
DIDE – Department of Infectious Disease Epidemiology
ELISA – Enzyme-linked Immunosorbent Assay
ESAT-6 – Early Secretory Antigenic Target-6
FDA – United States Food and Drug Administration
IDSA – Infectious Disease Society of America
IGRA – Interferon-gamma release assay
IRLM – International Reference Laboratory of
Mycobacteriology
KP – Kaplan Meyer
LIMS – Laboratory Information and Management System
LTBI – Latent M. tuberculosis Infection
MAC – Mycobacterium Avium Complex
Mtb – Mycobacterium tuberculosis
NICE - National Institute for Health and Care Excellence
NNT – Number Needed to Treat
NPV – Negative Predictive Value
NTM – Non-tuberculous mycobacteria
OPUS – The name of a patient administration and
reporting system
PCR – Polymerase Chain Reaction
PHA – Phytohaemagglutinin
PPV – Positive Predictive Value
PY – Person Years of follow-up
QFT – QuantiFERON-TB Gold in-Tube Test
TB – Tuberculosis
TB7.7 – TB protein 7.7kD
TBNET – Tuberculosis Network European Trials Group
TST – Tuberculin Skin Test
TU – Tuberculin Unit
TNF – Tumour Necrosis Factor
WHO – World Health Organization
FUNDING
The PhD fellowship was funded by the IRLM, Statens
Serum Institut, The Research Council at Nordsjaelland
Hospital, Hillerød and Olga Bryde Nielsens Fond.

PhD Thesis Thomas Stig Hermansen
6
INTRODUCTION
The aim of this thesis is to evaluate the performance of the
QuantiFERON-TB Gold In-Tube Test (QFT) in tuberculosis
(TB) and latent Mycobacterium tuberculosis infection (LTBI)
– often referred to as active TB and latent TB – as well as
the ability of the QFT to differentiate between TB and
disease caused by non-tuberculous mycobacteria (NTM).
The QFT is the most widely used immunological test to
diagnose LTBI and belongs to the group of Interferon
Gamma Release Assays (IGRA). By evaluating the current
use and limitations of these assays, we can potentially
advance in the seemingly never-ending task to control and
fight TB. IGRAs are considered an important asset in the
diagnosis of infection with Mycobacterium tuberculosis
(Mtb), and in many TB low-incidence, high-income
countries, they have replaced the tuberculin skin test (TST)
as the preferred screening tool.
The development of the IGRAs was made possible by studies
performed at Statens Serum Institut (SSI) by Professor
Peter L. Andersen and his group (4). Almost two decades
ago, they identified the mycobacterial antigens used in these
tests. The International Reference Laboratory of
Mycobacteriology (IRLM) at SSI was at the frontier when it
came to introducing the first commercial test using the new
antigens. The third generation of this test, the QFT, was
first used in Denmark late 2005, and in the following five
years, the QFT was almost exclusively performed at IRLM.
Consequently, the results of the nationwide coverage of TB
cases and performed QFT’s could be obtained from a single
laboratory. This provided a unique opportunity to combine
data on all notified TB cases and all cultured NTM cases
with QFT data, allowing us to create a cohort of persons
screened with a QFT that was useful for large-scale
evaluation of test performance.
This cohort serves as the basis for all studies in this thesis.

PhD Thesis Thomas Stig Hermansen
7
1. BACKGROUND
1.1. THE TB SPECTRUM
TB has unfortunately maintained a status as one of the
world’s most important infectious diseases. Alongside HIV,
it is a leading cause of mortality and morbidity worldwide
(5). Although a reported decrease in TB cases and TB related
deaths has taken place over the last decades, the disease
seems in no way to be controlled or controllable with
available measures. An estimated 1.9 billion people are
harbouring Mtb (6) and serve as a reservoir for future TB
disease. In 2014, the WHO estimated 9.6 million new TB
cases and 1.5 million deaths due to TB, with the vast
majority of both TB cases and fatalities occurring in the
developing world (5). In Denmark, over the last decade, the
occurrence of TB has remained at a constant level of 300-400
new cases per year, with approximately two thirds of these
cases found among the immigrant population (7).
Infection with Mtb begins with the inhalation of infectious
droplet nuclei containing the bacteria. The bacteria reaches
the lungs and are ingested by alveolar macrophages (8)
where they are able to replicate, and through an immune
reaction involving macrophages, T lymphocytes, B
lymphocytes, and fibroblasts create the primary site of
infection, referred to as the Ghon focus. Within this
granuloma, the host’s immune response is suppressed
allowing Mtb to survive and replicate (9). The majority of
infected persons will then remain infected without clinical
symptoms and are said to have LTBI, in general referred to
as “latent TB”. The bacteria are viable but contained by the
immune system without evidence of clinical disease, and the
majority of patients will never progress to overt disease. A
proportion will however develop clinical manifest TB with
ongoing bacterial replication, in general referred to as
“active TB”.
The general perception that infection with Mtb exists solely
as active TB or latent TB has been challenged over the last
decade (10,11), and the different ways in which the causative
agent, Mtb, can impact the host are being recognized as a
continuum, rather than a binary process (12). This
continuum spans from (i) early elimination of Mtb by the
innate immune system without any immunological priming
to (ii) the latent state that evokes an acquired immune
response, but does not surface as a clinical significant
disease to (iii) active TB, responsible for 1.5 million deaths
every year (5). These observations have led to speculations
on how Mtb infection perhaps should be considered more a
spectrum rather than separate entities (13) (Figure 1).
The lifetime risk of developing active TB, once latently
infected, is suggested to be 5-10% (14), with increased risk
the first two years after infection, where half of the cases
occur (15,16). This “reactivation” happens when the
bacterial load increases (Figure 1) and the infection can no
longer be contained by the host immune system. Essential
in controlling TB, especially in low-incidence countries
Figure 1. Depiction of a proposed
framework for considering tuberculosis
infection as a spectrum (Adapted from
(13)).

PhD Thesis Thomas Stig Hermansen
8
where the majority of TB cases are due to reactivation (17),
is the prevention of disease. Thus, it is important to identify
individuals latently infected, who could benefit from
preventive treatment. Administration of preventive
treatment in a population with LTBI prevents 60-90% from
reactivation (18,19). Determinants of progression to active
TB are numerous, and are often a mixture of host and
environmental factors (12), that increase the risk of
progression from latent TB. Such known host factors are
suppressed cellular immunity by HIV infection (20,21),
tumour necrosis factor alpha (TNF-α) inhibitors (22),
glucocorticoids (23), transplantation (24,25), advanced age
(26) and diabetes (27). Reported environmental
determinants are prison stay (28), homeless status (29),
recent immigration from a TB high-burden country (30), and
recent TST conversion (31).
Depending on symptoms, bacterial load and recognition by
the immune system, different treatment strategies may be
used. Active TB disease with a drug susceptible strain is
traditionally treated during 6 months using the standard
four-drug regime consisting of isoniazid and rifampicin in
combination with ethambutol and pyrazinamide for the first
2 months (intensive phase) and isoniazid and rifampicin
alone for the subsequent 4 months (continuation phase).
LTBI may be treated by a variety of different regimes
depending on availability of drugs, compliance and adverse
effects. The WHO 2015 guidelines on LTBI recommend five
options for the treatment of LTBI: isoniazid monotherapy
daily for 6 or 9 months, the combination of rifampicin and
isoniazid daily for 3-4 months, the combination of
rifapentine and isoniazid once a week for 12 weeks, and
rifampicin as monotherapy daily for 3-4 months (32). In
Denmark, official guidelines suggest a 6 month course of
isoniazid therapy for the treatment of LTBI (33).
1.2. DIAGNOSIS OF ACTIVE TB
TB is the symptomatic disease caused by bacteria from the
M. tuberculosis complex (M. tuberculosis, M. africanum, M.
bovis, M. canetti, M. microti (34-36)). Classic symptoms of
pulmonary TB, although not necessarily present, include
chronic cough (sometimes with blood-tinged sputum),
weight loss, fever, and night sweats (37). The reference
standard for microbiological diagnosis of TB is culture, but
this requires specialized laboratory facilities, and bacterial
growth can take weeks or longer. Therefore, direct
microscopy of bacteria using acid fast staining (AFS) from
sputum samples remains the most common diagnostic
method worldwide. Various staining methods exist, but the
Ziehl-Neelsen stain, by which bacteria is dyed and viewed
under oil immersion or the newer auramine-rhodamine
stain (38) using fluorescence microscopy, are commonly
used. AFS is inexpensive and simple to perform, but lacks
sensitivity and specificity, as it cannot distinguish
mycobacterial species. In recent years, molecular methods to
detect TB have improved, and they are used increasingly in
both low- and high-incidence countries. PCR-based methods
such as the Xpert MTB/RIF (Cepheid) and the Geno-Type
line probe assays (HAIN Lifescience) offer advantages due
to the fast detection of Mtb and possible resistance to first
line anti-TB drugs. However, these methods detect bacterial
DNA solely and cannot separate live from dead bacteria -
consequently they are not useful for treatment monitoring.
In Denmark, the microbiological detection of TB is based on
direct smear microscopy using auramin-rhodamine stain as
well as culture in fluid and solid media for up to 56 days
using MGIT 960 and Löwenstein-Jensen slants respectively.
In addition, molecular methods are used to obtain rapid
results regarding susceptibility, species identification and to
monitor overall transmission dynamics (genotyping
methods). All TB cases are notifiable by the treating
physician, including culture-negative cases diagnosed based
on clinical criteria, radiological findings, histology,
treatment response, and sometimes also on immunological
tests (TST and IGRA). In Denmark, the proportion of
culture-negative TB cases was 23.5% from 1992 through
2011 (39) (including notified cases where no specimens were
sent for culture).
1.3. DIAGNOSIS OF LATENT TB
Currently, no gold standard for diagnosing latent TB exists,
and it is not possible to find viable bacteria directly. Instead,
indirect methods are used either in vivo by the widely used
TST or in vitro using the newer, blood based IGRAs. Both
methods depend on cell-mediated immunity and recognition
of mycobacterial antigens, as shown by the illustration from
Andersen et al (4) (Figure 2).

PhD Thesis Thomas Stig Hermansen
9
The tuberculin skin test
The TST contains a purified protein derivative tuberculin
unit (TU) which is a protein fraction from a Mtb strain. The
standard is injecting five TU intradermal using the Mantoux
technique. If cell-mediated immunity is present, the person
will develop a delayed-type hypersensitivity reaction
causing local inflammation and skin induration. After 48-72
hours, if an induration appears, the result is given by the
transverse diameter of the induration. However, pre-test
probability of infection, induration size and risk of TB
disease should be taken into consideration when
interpreting TST reaction (40). Also, the TST has important
limitations. The need for a return visit in 48-72 hours to read
the skin reaction is a logistic drawback, and because of
manual reading, the reproducibility of the test may be a
problem. Furthermore, boosting caused by a previous TST
and resulting hypersensitivity can make serial or repeat
testing difficult to interpret (41). More important, false
positive results can occur due to infection with the group of
NTM and if the person has been vaccinated with the M. bovis
Bacille Calmette-Guérin (BCG) strain. These false positive
results are caused by a cross-reaction between the non-
specific Mtb protein mixture contained in the PPD with the
majority of the NTMs (42) and the BCG strain (43). False
negative results of the TST is known to occur in
immunocompromised persons (due to both medical
conditions and immunosuppressive therapy), where test
sensitivity is poor (44). However, the TST remains the most
widely used test worldwide, requiring less laboratory setup
than the newer IGRAs.
1.4. INTERFERON GAMMA RELEASE ASSAYS
IGRAs are in vitro, blood based assays, which have their
main use in diagnosing Mtb infection. They cannot
discriminate between active disease and latent infection,
and are not intended as a stand-alone diagnostic test for TB,
but in certain situations they can however aid in the TB
diagnosis.
IGRAs are based on a cell-mediated release of interferon
gamma (IFN-γ) from T-lymphocytes, after stimulation with
antigens specific for Mtb. When Mtb enters the human host
(and is not eliminated by the innate immune response, see
Figure 1), its antigens will evoke a cellular response with
sensitization of T-lymphocytes by antigen presenting cells
(Figure 2). The sensitized T-lymphocytes are stimulated by
Mtb specific peptides, and recognition of these peptides in
the presence of major histocompatibility complex class II will
result in the production of different biomarkers, one of these
being IFN-γ. Infected individuals will have an IFN-γ level
above the threshold and the test will be positive. The basis
of these assays is a quantification of the IFN-γ production.
The peptide antigens in the IGRAs are the ESAT-6 (Early
Secretory Antigenic Target-6) and CFP-10 (Culture Filtrate
Protein-10) and the genes encoding these proteins are
located in the region of difference 1 locus in the Mtb genome,
whereas TB7.7 (used in the QFT) is encoded in region of
difference 11 (45). IGRAs have superior specificity compared
to the TST because the antigenic regions are not encoded in
the majority of NTM (except M. gastrii, M. kansasii, M.
marinum, M.riyadhense and M. szulgai (42)) or the vaccine
strain M. bovis BCG (46).
Two commercially available IGRAs exist, the T-Spot.TB (T-
Spot, Oxford Immunotec, Abingdon, UK) and the
QuantiFERON-TB Gold In-Tube Test (QFT, Cellesties,
Quiagen, Chadstone, Australia). The T-Spot utilizes an
enzyme-linked immunosorbent pot assay and report the
number of IFN-γ producing T-lymphocytes that respond to
ESAT-6 and CFP-10. If the spot count in the Mtb antigen
well reaches a predefined threshold after subtraction of the
count in the negative control well, the test is positive. The
Figure 2. Recognition and measurement of response to
mycobacterial antigens by the TST and the in vitro blood
tests (4). Abbreviations: TNF-α :Tumor necrosis factor alpha
IFN-γ: Interferon gamma IL-8: Interleukin 8

PhD Thesis Thomas Stig Hermansen
10
QFT provide a measurement of the interferon-γ release from
T-lymphocytes stimulated by the Mtb specific antigens
ESAT-6, CFP-10 and TB7.7, using the ELISA technique.
1.5. QUANTIFERON-TB GOLD IN-TUBE TEST
Third generation of the Quantiferon assay uses three pre-
coated tubes to collect heparinized whole blood from the
individual tested. One tube is coated with the mycobacterial
antigens (TBAG tube), one is a positive control containing
phytohaemagluttinin (PHA, an unspecific mitogen) used for
validation and control of the assay, and one is a negative
control (Nil tube) containing saline solution. The positive
control serves both as control of correct handling and as
control of the person’s immune status and ability to respond
to the test antigens. Within 16 hours from blood drawing,
the tubes are incubated for 16-24 hours before centrifugation
and harvesting of plasma. At this point the samples can be
stored between 2-8 oC for up to 8 weeks. The samples are
then analysed by an ELISA method in which the amount of
IFN-γ in IU/mL is measured.
For the test to be valid the Nil value has to be below 8.0
IU/mL and the positive control above 0.5 IU/mL.
Indeterminate tests are reported to be associated with an
array of different host factors, as well as environmental
factors and multiple sources of variability can influence test
results (described in the limitations section). The test is
positive if the IFN-γ readout in IU/mL is above 0.35 after the
Nil value has been subtracted, whereas a test is negative if
the IFN-γ level in the TBAG tube is below 0.35 IU/mL.
Interpretation of the IFN-γ responses in the three tubes is
depicted in Table 1.
1.6. NON-TUBERCULOUS MYCOBACTERIA
Mycobacteria can be classified into three major groups:
Mycobacteria from the M. tuberculosis complex (causing
TB), Mycobacterium leprae (causing leprosy) whereas the
remaining mycobacteria are named NTM or atypical
mycobacteria (to separate them from the “typical” M.
tuberculosis complex). This diverse group currently consists
of more than 150 different species and subspecies, found in
soil, dust, animals, and tap water worldwide (47,48).
NTM disease cases are often difficult to diagnose. Unlike
Mtb, a positive NTM culture from a sputum sample does not
equate with disease and it is often difficult to distinguish
insignificant colonization or contamination from clinically
significant NTM disease. An approach to assess the clinical
impact of NTM infection is presented in the American
ATS/IDSA guidelines (49), defining NTM definite disease,
NTM possible disease and NTM colonization based on a
combination of radiological, microbiological and clinical
criteria. A modified approach using only microbiological
criteria has been used and validated over the last years (50-
54), enabling laboratory based surveillance of NTM disease
occurrence.
The clinical presentation of NTM disease is often very
diverse, e.g. in the form of pulmonary lesions, cervical lymph
node enlargement, skin or soft tissue lesions or disseminated
disease (49). In children, the most common clinical
Table 1. Interpretation
Criteria for QuantiFERON-TB
Gold in-Tube Test based on
package insert.

PhD Thesis Thomas Stig Hermansen
11
presentation of NTM disease is cervical adenitis, most often
due to mycobacteria from the M. avium complex (MAC) (55).
This localized lymph node enlargement and chronic infection
is regarded an independent disease entity different from the
pulmonary disease observed among adults, and it is
occurring in immunocompetent children aged 1-5 years
without systemic symptoms (55). As NTM infection can
mimic both pulmonary and glandular TB, a diagnostic tool
that could facilitate differentiation would be valuable.

PhD Thesis Thomas Stig Hermansen
12
2. OBJECTIVES
1. To assess the performance of the QFT among patients
with NTM disease and to review available literature on
the subject
2. To assess the performance of the QFT among
individuals with and without active TB.
3. To determine the predictive value of the QFT for
development of active TB in a Danish cohort and
identify factors potentially associated with increased
risk of progression.

PhD Thesis Thomas Stig Hermansen
13
3. METHODOLOGICAL
CONSIDERATIONS
3.1. SETTINGS, DESIGN AND POPULATIONS
All three studies were retrospective and based on a cohort of
individuals screened with a QFT from January 2005 until
the end of December 2010. During this period, more than
95% of all QFT done in Denmark were analysed at IRLM,
SSI. From 2011 onwards, the test has been increasingly
performed at several local biochemistry departments
instead of SSI, making similar nationwide studies difficult
to perform in the future. The present study is thus based on
a unique data material covering the majority of the Danish
population screened for LTBI with a QFT in a six-year
period.
Study I combined the QFT cohort with nationwide data on
persons with a positive NTM culture retrieved from the
IRLM. Study II and III both combined the QFT cohort with
an extraction from the Department of Infectious Disease
Epidemiology (DIDE) on notified cases of TB. In study III
additional data were retrieved from hospital case records.
Figure 3 depicts the participant flow from available data
sources. All databases were combined using the Personal
Identification Number (CPR) included in the Danish Civil
Registration System (56). Further description of study
design, study settings and populations can be found in
article I-III (1-3).
3.2. DATA SOURCES
LIMS
Data on QFT performed at IRLM from 2005 through 2010
were extracted from the Laboratory Information and
Management System (LIMS). LIMS is used to register and
report all diagnostic examinations performed at the Division
of Diagnostics & Infection Control at SSI. All entries in
LIMS are based on the CPR, and this number is used to
connect LIMS with other registries enabling reporting of
diagnostic examinations to the requestor. Data stored in
LIMS is incorruptible and cannot be altered once entered in
the system. This way data is stored in its original format
over time, ensuring perfect reproducibility and making the
LIMS a comprehensive data collection well suited for
research purposes. The drawback of having a database
where data cannot be modified or updated is that extracts
from the LIMS are very diverse if the reporting of a
Figure 3. Participant flow
from available data sources
study I-III
Abbreviations:
LIMS - Laboratory Information
and Management System;
IRLM - International Reference
Laboratory of Mycobacteriology;
DIDE - Department of
Infectious Disease
Epidemiology

PhD Thesis Thomas Stig Hermansen
14
diagnostic test changes. In the present thesis, this adversely
affected the extract because the description of a QFT result
in LIMS had been changed numerous times during the
initial years of testing. Hence, a lot of time-consuming data
cleansing was necessary before the analysis could be
performed. To eliminate some of the diversity in the QFT
reporting, we excluded the second generation of the test, the
QuantiFERON-TB Gold and included only the third
generation of the test, QuantiFERON-TB Gold In-Tube Test
(QFT).
IRLM Database
In Denmark, the culturing of Mycobacteria is centralized at
IRLM. The database contains information on all samples
received at the laboratory that turn out positive by either
microscopy, molecular methods or culture. Positive
specimens are manually entered into the registry by patient
ID. Sample type, citizenship, country of birth and address
are included in the registry, whereas negative samples are
not. The original and current purpose of the database at
IRLM is fast access to information on all patients with a
positive mycobacterial specimen and the opportunity to
perform population based research. As opposed to the LIMS,
the data in the IRLM database is updated and modified in
continuity, making data extracts readily usable without
cleansing and the need for interpretation of data output. In
this thesis, an extract of positive NTM cultures was used in
study I.
DIDE Database
Since 1990, the Department of Infectious Disease
Epidemiology (DIDE) at SSI has received nationwide data
on notified TB cases (57). In Denmark, the physician
responsible for treating the TB patient are required to notify
DIDE using a standardized form (58). This form contains
demographical, clinical and epidemiological data regarding
the TB patient, such as country of exposure, way of
transmission, type of infection (pulmonary or extra-
pulmonary), outbreak conditions and diagnostic method.
The database at DIDE is maintained and updated regularly,
and data concerning TB surveillance and disease control in
Denmark is published through the SSI website as short
reports and graphical displays available to the public (57).
3.3. STATISTICS
Descriptive statistics
The quantitative (continuous) variables were described as
mean and standard deviation of normally distributed
variables and as median and interquartile range of non-
normally distributed variables. The qualitative (categorical)
variables were summarized using frequency distributions
and described as numbers and percentages out of the total.
Statistical analysis
Wilcoxon rank sum/Mann-Whitney U was the non-
parametric test used to evaluate continuous variables and
Pearson’s chi-squared or Fisher’s exact test (frequency
counts <5) was used to compare categorical variables.
Cochran-Armitage test for trend is a modification of the
Pearson chi-squared test where a suspected ordering in the
proportions of the categorical variables is incorporated. The
null hypothesis is that the linear trend parameter is zero, so
a significant p-value is consistent with the presence of a
trend. It was used to evaluate an association between
binomial variables and variables with more than two
categories. Kaplan Meyer (KM) survival estimates were
used. To investigate significant differences between the KM
curves and the two derived survival distributions, the
nonparametric log-rank test was applied.
Table 2. Data sources
in Study I-III.

PhD Thesis Thomas Stig Hermansen
15
Statistics regarding diagnostic tests
Sensitivity was calculated as #true positive tests/(#true
positive tests + #false negative tests). Positive predictive
value of a test was defined as the proportion of patients with
an initial positive test that developed disease, and negative
predictive value defined as the proportion that scored
negative in the test and did not develop disease. Overall, a
two-sided p-value <0.05 was considered significant. For the
statistical analysis, SAS® 9.3 (SAS Institute Inc., Cary, NC,
USA) and R version 3.1.1 (59) were used.

PhD Thesis Thomas Stig Hermansen
16
4. MAIN RESULTS
4.1. STUDY I
Background
The incidence of NTM infections have been reported to be on
the rise and clinical manifestation of NTM disease can
mimic TB. If a blood test can differentiate between TB and
NTM disease, this could provide a minimally invasive tool
for the clinician compared to traditional microscopy, culture
and PCR. The reason why the QFT could potentially be
useful is that the majority of the NTM do not share the M.
tuberculosis specific antigenic regions used in the QFT.
Aim
The study objective was to investigate test performance
among patients infected with NTM and to review available
literature on IGRAs among patients with NTM disease.
Results
The majority (50/53) of patients had NTM disease due to
mycobacteria not sharing the antigenic region with Mtb, and
we found 2 positive, 43 negative and 5 indeterminate QFT
results, resulting in a specificity of 96% (43/45). Three
patients had disease due to Mycobacteria known to share the
antigenic region with Mtb, and in this group, 67% (2/3) were
positive.
We found 9 published studies with a total of 478 patients
with NTM disease and an IGRA. In patients infected with
an NTM without the antigenic region, the QFT was positive
in 12% (ranging from 0-50% in the different studies)
compared to our rate of 4.4% (2/45). Patients infected with
NTM sharing the region with Mtb had an overall positivity
rate of 57%, which is in line with our finding of 67%. Among
children, in the majority of cases, NTM disease was due to
infection with MAC and the localisation was extra-
pulmonary lymphadenitis. All children with MAC had a
negative QFT.
Conclusion
The QFT might hold potential in discriminating between
NTM and Mtb infections, in particular in children, where
lymphadenitis due to mycobacteria from the MAC was
predominant and because this clinical presentation may
mimic TB lymphadenitis.
4.2. STUDY II
Background
Even though IGRAs are used increasingly for the diagnosis
of LTBI worldwide, few studies have investigated the test
performance in extreme age groups. Current guidelines
warrants caution when using IGRAs in children less than
five years of age due to lack of studies performed. Similarly,
only a limited number of studies evaluate test performance
among elderly, and no guidelines specifically addresses the
ageing population.
Aim
To evaluate QFT performance among patients of different
age groups with and without TB.
Results
Among 383 patients with active TB, we found a low
indeterminate rate of 3.9% and a high sensitivity of 86.1%.
The latter was unaffected by localization of TB
(pulmonary/extra-pulmonary), sex and diagnostic group
(culture and PCR confirmed TB versus clinical TB diagnosis
only). Sensitivity declined with increasing age and was thus
found to be 71% among elderly persons aged more than 65
years, but was not impaired in young children with active
TB (100%). Among 15,709 persons without TB, the
indeterminate rate was overall 5.1%, and higher in infants
aged <1 year (15.6%) and elderly aged >65 years (8.1%).
From age one and above the indeterminate rate was not
significantly increased compared to adults aged 15-64 years.
Conclusion
QFT sensitivity among TB patients was overall 86% but
declined with increasing age (>65 years). In contrast to what
current guidelines on IGRA use in small children state, our
data suggest that the QFT performs well in children from
age 1, but that caution should be taken when using the test
among the elderly and infants.
4.3. STUDY III
Background
Latent TB is prevalent in high numbers throughout the
world, but only a small proportion of persons infected with

PhD Thesis Thomas Stig Hermansen
17
Mtb will eventually develop TB disease. A valuable
diagnostic test detecting the presence of latent infection
should be evaluated by its ability to predict how many will
develop disease and ultimately be able to identify those in
highest risk of progression.
Aim
To investigate the predictive value of the QFT.
Results
We included patients with a QFT performed and combined
these with notified TB cases. We defined “co-prevalent TB”
as cases 0-90 days after testing and “incident TB” as cases
developing after more than 90 days. In total, 231 patients
had co-prevalent TB and 40 patients developed incident TB
within the follow-up period. The cohort was subject to a
follow-up for 52,807 person-years, and median follow-up
time was 3.36 years. For incident TB, we confirmed a very
high negative predictive value of 99.85% and found a
positive predictive value of 1.32%. Expressed as risk of
developing incident TB, this corresponds to an incidence rate
(IR) of 383 per 105 PY for QFT positive patients and an IR of
45 per 105 PY for QFT negative patients. The risk of incident
TB was highest the first two years after a positive test, and
only two patients out of 20 with a positive test completed
preventive therapy.
Conclusion
We found a high NPV and a PPV of 1.32% for development
of incident TB. Development of incident TB was associated
with time interval after the QFT, but not with age.

PhD Thesis Thomas Stig Hermansen
18
5. DISCUSSION
5.1. QFT PERFORMANCE
Sensitivity among patients with active TB
Sensitivity of the QFT among patients with TB in Denmark
was comparable to what has been found in available
literature (86%). In line with previous studies, risk factors
such as gender (60), localization of disease (pulmonary vs.
extra-pulmonary TB) (61) and culture result (presence or
absence of a positive Mtb culture) (62) did not affect test
sensitivity (2). Sensitivity has been evaluated extensively
during the last decade. In general, the TST, QFT and T-Spot
have comparable sensitivities of 80-90% in most studies of
immunocompetent individuals (61,63,64), but because the
tests are based on the cellular immune response, reduced
sensitivity are linked to immunological function and
immunocompromised patients. HIV infection and very
young age are shown to reduce sensitivity for all diagnostic
tests (65,66), highlighting a paradoxical problem for all
immune based tests for TB; they suffer reduced performance
among those patient groups that are most susceptible to
both active and latent TB.
The QFT cannot separate latent from active TB and should
not be used alone in patients suspected of active TB. It can
however, be used as a tool in the diagnosis of active TB in
situations including; patients with extra-pulmonary TB,
patients who are persistently negative by microscopy or
culture, TB diagnosis in children, or as a supplement in
differential diagnosis between infections with NTM and TB
(67). Only few studies have assessed whether adding an
IGRA test to the existing diagnostic work-up for active TB
can successfully identify a greater proportion of TB cases in
TB high-incidence settings (68,69), TB low-incidence
settings (70) and in child populations (71). Discouragingly,
in most clinical situations an IGRA or TST was not of
additional value when combined with standard methods to
diagnose active TB (67).
Distinguishing active from latent TB using IFN-γ level
IGRAs (as well as the TST) cannot distinguish between
latent and active TB. If an algorithm based on the
commercially available IGRAs could make this distinction,
it would be immensely valuable. Numerous studies have
indeed investigated whether the level of IFN-γ readout is
higher in patients with active TB compared to those with
latent TB (70,72-76). In study III, we describe significantly
higher IFN-γ levels in the group that develops incident TB
compared to the group with a positive QFT that remain
healthy. However, the confidence limits are very wide and
the test cannot discriminate between the two groups, so this
observation has no practical use. A new generation of the
QuantiFERON test has recently been introduced (77). It
contains two tubes with mycobacterial antigens directed at
different subpopulations of T-lymphocytes and might have
potential in discriminating active TB from LTBI. The first
independent evaluation of this test (78) shows similar
specificity and sensitivity but suggest that accuracy might
have improved in patients with low CD4+ T-cell counts (78),
whereas discriminatory ability is not evaluated. So far, in
one decade of reporting and studying the IGRAs, no human
studies have conclusively shown that they can distinguish
between active and latent TB, and currently available IFN-
γ based assays will most likely not be able to (79). Numerous
studies are focusing on discriminating TB stages (80,81) and
the search for alternative biomarkers and dormancy
antigens that could be used in the development of next
generation assays is ongoing (82).
5.2. NON-TUBERCULOUS MYCOBACTERIA
The role of IGRAs in the diagnosis of NTM disease is as yet
insufficiently explored. European Centre for Disease Control
and Prevention guidelines state that an IGRA can contribute
with supplementary information in the differential
diagnosis between NTM and TB disease (67), but this
recommendation is based on very limited evidence. Study I
(1) as well as other studies find a low proportion of positive
tests among patients infected with NTM without the RD1
antigenic region and a significantly higher proportion
among patients infected with NTM sharing the RD1 (83-93).
Based on the high specificity of the QFT in patients with
NTM disease in study I and on available literature, we find
that the QFT holds potential to discriminate between NTM
and TB (1).

PhD Thesis Thomas Stig Hermansen
19
NTM disease is a rare event in Denmark (approximately 100
new patients per year), and the need to separate NTM from
TB using a QFT is not widely applicable in a Danish setting.
However, in children presenting with cervical
lymphadenitis, our study found all 15 children aged 0-9
years with MAC lymphadenitis to be QFT negative,
resulting in a specificity of 100%. Lymphadenitis due to
NTM is common in young children and the clinical
presentation can mimic extra-pulmonary TB. The
differentiation relies on a suitable biopsy specimen from
which the mycobacteria is identified by culture or molecular
methods. If a less invasive test such as an IGRA could aid in
this separation it could be useful, but the IGRAs suboptimal
sensitivity as reported in study II (86%) calls for caution
when using such tests to distinguish between TB and NTM.
5.3. QFT PERFORMANCE IN EXTREME AGE
GROUPS
Children
Young children are facing an increased risk of developing
active TB if they become infected, and they often have
disease with few bacilli (paucibacillary TB). Also the TB
disease manifestations are different from adults in the form
of more milliary TB and TB meningitis (94). This makes
children a particularly vulnerable group, difficult to
diagnose and suffering more severe disease than adults do.
As a result, a positive IGRA can be useful to support a
suspicion of TB along traditional diagnostic measures (67).
Study II suggests that already from age one, the
performance in children with active TB is good, although few
were included. Studies of IGRA performance in children are
very heterogeneous, and few investigate performance in
children aged less than 5. Some studies demonstrated a
lowered sensitivity in children aged <5 years (94,95),
whereas others report IGRA sensitivity comparable to
adults from 2 years of age (85,96,97). In TB high-incidence
countries both IGRAs and TST perform poorly among
children, most likely due to a combination of severe
comorbidity causing immunosuppression, misclassification
and high rates of reinfection (98). In the study by Rose et al
in a Tanzanian population of 211 children, of whom 77 were
aged <2 years, the QFT performed badly with sensitivity of
19% and indeterminate rate of 27% (98).
We evaluated the indeterminate rate in children without
active TB, and found no effect on indeterminate rates in
children from age 1, but among infants aged <1 the
indeterminate rate was high (15.6%) (2). This suggest that
an immature immune system in children seem to affect test
performance only the first year of life (2), and is most likely
caused by a T-cell population dominated by naïve cells (99).
Studies on indeterminate rate and children are numerous,
and some report that young age is associated with more
indeterminate results (100-103) whereas others do not reach
such a conclusion (95,97,104). Overall, IGRA and TST could
both be used for latent TB diagnosis from age 1 in otherwise
healthy children. None of the tests should be used for a
definitive diagnosis of active TB.
Elderly
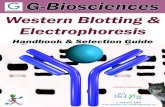
In the elderly, the T-lymphocyte response is decreased (105).
This can affect the QFT indeterminate rate and sensitivity,
Figure 4.
Mitogen response among
15,506 patients without TB.
PHA: Phytohaemagglutinin
0%
20%
40%
60%
80%
100%
Age
PHA>10
PHA<10
PHA<5
PHA<0.5

PhD Thesis Thomas Stig Hermansen
20
and is probably caused by an exhausted population of
memory T-cells. In study II, we found that among those aged
65 years and above, the QFT had more indeterminate results
as well as decreased sensitivity. Consequently, the
likelihood of both false negative and indeterminate tests is
higher amongst the elderly. Whether the decreased
sensitivity is a direct effect of old age or caused by age
related immunosuppression is not possible to determine (2).
Our findings are supported by a recent TBNET study (106)
where extreme age was the only significant factor associated
with higher rate of falsely negative IGRAs.
We have assessed the influence of age on the quantitative
PHA response and confirmed that the PHA response is
affected in the very young and the very old (Figure 4,
adapted from Table 4 in Study II). Figure 4 illustrates the
PHA response from persons screened for LTBI in different
age groups. In children 0-9 years and elderly >65 years the
response to PHA is lowered, but the indeterminate rate
(PHA<0.5) is only higher in infants <1 and elderly >65,
suggesting that IFN-γ release is lowered throughout early
childhood but does not affect QFT result in children aged >1
(2).
5.4. PREDICTIVE VALUE OF THE QFT
Negative predictive value
In a cohort of 13.463 individuals we found a very high NPV
of 99.85% (study III). We have hereby established that the
NPV of the QFT in Denmark is extremely high,
corresponding to the findings in other studies from TB-low-
incidence settings (72,76,107). The individuals in study III
constituted a heterogeneous group tested with QFT due to
recent exposure, in the diagnostic work-up of active TB, or
before the initiation of anti TNF-α treatment. Although we
cannot separate the groups by test indication, the NPV in
general was very high, and the QFT seemed a useful tool for
identifying those that would not progress to TB disease.
However, of the 40 patients who developed incident TB, 20
actually had a baseline negative test. This could be
explained by different factors such as an impaired immune
system or re-infection with a new strain. In environments
with active transmission, the NPV is reduced because of new
infections, and this could be an explanation among the
socially marginalized persons in Denmark, where the
prevalence of active TB are reported to be more than 2000
per 105 (108). Of the 20 patients with incident TB and a
baseline negative test, 25% (5/20) were immunosuppressed
at the time of testing, and these test results could potentially
be false negative.
Positive predictive value
In a mixed population of patients tested with the QFT, 1.32%
developed TB during follow-up (study III). This is equivalent
to an 8 times increased risk of developing TB when a person
has a baseline positive test compared to a baseline negative
test. The PPV vary substantially in available studies
(63,76,107,109) depending on the TB prevalence in general
and the population in particular: In a vulnerable population
of recently exposed children, Diel et al found a PPV of 28.6%
(107), whereas the PPV was well below 1% (110) amongst
health care workers. A PPV of 1.3% is intuitively low for a
diagnostic test but the PPV varied and was higher among
children and adolescents aged less than 35 years (2.22%).
The risk of progression to incident TB was significantly
higher within the first two years after the QFT, where 90%
of incident cases developed. IR of progression was almost
800 per 105 PY the first year, 400 per 105 PY the second year
and 90 per 105 PY after more than two years (3), in line with
historical data describing an increased risk during the first
years after testing (111). A general issue to consider
regarding the low PPV is that only 5-10% of persons with
LTBI develop disease (14), so even a flawless test with
perfect accuracy will have a low predictive value.
Number needed to treat (NNT)
Generally, the QFT should be performed with a clear
indication, and the reasons for testing as well as the
consequences of a positive or negative result have to be
considered before deciding to test. In 2011 the catchphrase
“Intention to test is intention to treat” was introduced (112).
The point of that concept is that unnecessary tests for LTBI
should be avoided. The purpose of screening to detect LTBI
is to prevent future TB cases by administration of preventive
therapy. The PPV reflects the proportion of the persons
screened with a positive test result, who ultimately develop
TB, but the clinical usefulness of the test can also be
evaluated using another measure: The Number Needed to
Treat (NNT) expresses the number of persons with LTBI
that have to be treated with preventive therapy to avoid one

PhD Thesis Thomas Stig Hermansen
21
case of active TB. NNT is central in cost-benefit analysis of
the use of IGRAs in TB low-incidence countries. Sester et al
(113) have reviewed the NNT to prevent a TB case among
close contacts (30-37 (76,114,115)), immunocompromised
(50-80 (116)), HIV infected (14-26 (116)) and health care
workers (no TB cases developed among >15,000 persons
(117-119)). Thus, NNT differs according to the risk group,
and in all studies, confidence limits were wide because of few
incident TB cases. In Denmark and comparable TB low-
incidence countries mass screening is not cost effective (63)
because both the number needed to screen to identify a
person with LTBI and the NNT is very high. All studies
point toward targeted screening in high risk groups (32).
Another relevant measure when addressing TB prevention
is the Number Needed to Harm (NNH). It indicates the
number of patients that can be treated with preventive
therapy for one patient to suffer adverse effects. With the
increasing likelihood of isoniazid-induced hepatotoxicity
with increasing age (120,121) the NNH is age related and
screening elderly have to take this into account.
6. LIMITATIONS
6.1. BIAS
In general, patients screened with IGRA have a high a priori
likelihood for TB and LTBI. Thus, the studied population is
not representative for the Danish population and our studies
will overestimate the prevalence. Selection bias is also
present when we investigate age and risk of latent and
active TB, because the indication to screen a child or a young
person is often different from screening elderly. Among
children, recent exposure or suspicion of active TB is a
common indication, and the risk of active TB is high if
infected (122). Reversely, among elderly aged 35 and above,
screening before starting immunosuppressive treatment is
increasingly common, and in this group the prevalence of
LTBI is low and consequently very few will develop TB.
Therefore, the risk of TB could differ because the age groups
have different a priori risks of TB and not because age is an
independent risk factor.
Misclassification can occur when cases and controls are not
correctly recognized as such. False negative test results
among patients with TB disease occurred in 14% of the
active TB population in study II, and this misclassification
could result in unrecognized TB cases. In study II, we
evaluate how age, sex, localization of disease and
culture/PCR versus clinical confirmation of active TB
influences the rate of false negative tests. Confounding is
present when two evaluated factors do not act independently
in their contribution to the outcome under investigation.
Confounders that should always be considered are sex and
age. In our studies these variables were controlled for in the
data analysis in study II and III.
6.2. QFT VARIABILITY
Challenges with the QFT assay in terms of variability can
be assigned to a number of overall sources (63);
Manufacturing issues, preanalytical sources of variability,
analytical sources of variability and immunological sources
of variability as depicted in Figure 5.
Figure 5. Sources of variability in the QuantiFERON-
TB Gold In-Tube assay. Reprint from (63)

PhD Thesis Thomas Stig Hermansen
22
In our cohort of persons screened with a QFT, all of the
factors shown above may influence test results in both a
positive and negative way. Because of the retrospective
nature of our studies, the influence of the preanalytical and
immunological sources of variability on our cohort is difficult
to address. No information regarding the preanalytical
filling of blood tubes or handling and transport of the
samples before they arrive in the laboratory are available.
Further, we lack information on host factors for the
individual patients because no indication for screening or
information on comorbidity is available. Regarding
analytical variability, quality control is performed in each
run of the ELISA test in accordance with manufacturer’s
instructions. Manufacturing defects could be defects such as
errors in the production of the kits or reagents used. It can
be difficult to detect for individual laboratories, but
monitoring of sudden increases in indeterminate or positive
test results is an important control measure.
6.3. QFT REPRODUCIBILITY AND
REPEAT INDETERMINATE TESTS
The systematic sources of variability of the QFT have been
accounted for (Figure 5), but random variation due to
immunological factors can also affect test results. Problems
with QFT reproducibility in the same person undergoing
serial testing is well known, and reports of conversions (a
negative test becomes subsequently positive) and reversions
(a positive test becomes negative) are numerous (118). The
introduction of a borderline zone to better understand test
dynamics has been proposed in order to counter this (123).
The grey zone is the level of IFN-γ release in IU/mL, where
most reversions and conversions appear, and it can be used
to alert the clinician to interpret results with caution. In
study III, we describe a larger proportion of patients who
develops incident TB are in the grey-zone from 0.2-1.0
(3,117,123) compared to the group without TB. This finding
is interesting albeit not surprising, because it suggests
impaired immunity plays a role in the susceptibility towards
developing TB disease.
In study II, the indeterminate rate of all persons tested was
5.1%. Of these, 40% were repeated and 67% changed to
either positive or negative in the subsequent test. The
recommendation when encountering an indeterminate QFT
is to repeat the test (33) and a majority of these repeats
turned out valid. More than 99% of all the indeterminate
results were caused by a low positive control, and most
likely, they are attributed to an impaired T-lymphocyte
response because of suppressed host immunity.
6.4. SCREENING INDICATION
A limitation in both study II and III is the lack of screening
indication when performing the QFT. In study II the group
consisting of persons with a QFT without TB disease was
heterogeneous and comprised individuals tested for
different reasons. Because we did not have access to clinical
information, we could not determine if the
immunosuppression seen with advanced age in study II was
a genuine effect of old age or an effect of age related co-
morbidity (2). Similarly in study III, we did not have clinical
data on the actual reason for testing, so calculation of the
PPV and NPV stratified by risk group was not possible.
However, in a very large cohort we did provide general
confidence limits for both the PPV and the NPV of a QFT per
see.
7. PERSPECTIVES
7.1. THE LOCAL PERSPECTIVE, IGRA USE IN
DENMARK
In Denmark and other high-income TB low-incidence
settings, the intended use of IGRAs is the use as tools to
screen high-risk groups and identify patients that will
benefit from preventive treatment. However, as our data
and other data (124,125) suggest, IGRAs are widely being
used to aid in the diagnosis of active TB and not always in a
correct way.
Use of the QFT test to diagnose active TB
In a subgroup analysis of the patients in study II, 100
patients with active TB had a QFT performed in 2010 among
361 notified TB cases (7). It follows that 28% (100/361) of the
notified TB cases in Denmark that year had a QFT
performed to aid in the TB diagnosis. To further support a

PhD Thesis Thomas Stig Hermansen
23
widespread use of the test in active TB diagnosis, in a recent
Danish study from Aarhus, Danielsen et al evaluated the
use of the T-Spot test from 2010-2011 (124). Suspicion of
active TB was the indication for screening in 32.7%
(533/1,631) of persons tested. Another study evaluated test
indication in 2005-2006 at Hvidovre Hospital, and
Browatzki et al (125) found active TB to be the indication in
81% (74/91) of all IGRAs performed.
These findings indicate that the test is used to screen for
active TB. This is not necessarily misuse of the test, but
according to guidelines IGRAs rarely have an added value in
combination with standard methods for diagnosing active
TB (67) indicating at least some misuse of the test. Based on
the studies in the current thesis and available Danish
literature, there seem to be a need for better adherence to
guidelines and improved information regarding IGRA
limitations. Although this is not a big problem in Denmark
with the majority of TB cases being confirmed by culture, it
is increasingly a concern globally (126).
Preventive treatment
According to Danish guidelines (33), the standard treatment
for latent TB infection is a 6-month course of isoniazid
monotherapy. Diagnosis of latent TB and prescription of
preventive treatment is not a notifiable event, and therefore
no summarized data is available. The total coverage of
isoniazid preventive therapy among individuals with a
positive QFT was estimated to be 35% (data not shown) and
among patients with a positive QFT who developed incident
TB, 90% did not receive preventive treatment (3). It follows
that adherence to guidelines concerning screening
indication and preventive treatment in Denmark is
suboptimal.
7.2. THE GLOBAL PERSPECTIVE, IGRA USE
WORLDWIDE
IGRA use in TB high-incidence countries
In TB high-incidence settings, IGRAs have limitations
because of their extensive laboratory requirements and a
high prevalence of LTBI in the population. Consequently,
WHO has issued different guidelines on the management of
latent tuberculosis infection in countries with a TB incidence
rate below 100 per 105 population (32) compared to TB-high-
incidence countries (127,128). In TB high-incidence
countries, WHO recommends to reserve the use of IGRAs for
HIV infected individuals (127) and children below the age of
five (128), both groups being vulnerable groups with
increased risk of progression to disease.
A novel RD-1 specific skin test has a potential use in
resource-limited settings because it does not require a
laboratory. The C-Tb (129) contains the same mycobacterial
antigens as the QFT and has similar specificity and
sensitivity, but still share the IGRAs restraints in settings
with high prevalence of LTBI.
Use and misuse of the test among patients suspected of
active TB
The off-label use of IGRAs in the diagnosis of active TB could
potentially result in overtreatment. In a recent article from
India (130), Little et al constructed an analytical decision
model and found an estimated 315,700 additional false-
positive persons would be diagnosed with TB each year at an
incremental cost of US$49.3 million. This finding supports
recent policies by WHO that now discourage the use of
IGRAs for the diagnosis of active TB in settings like India
(126) and the misuse of the IGRAs in TB high-incidence low
income countries is currently receiving global attention.
Another problematic tool when diagnosing TB is the
commercial, serological tests for recognition of Mtb antigens
by the humoral immune response (as opposed to the cellular
response used by the IGRAs). They are marketed in many
third world countries, although none of them are
recommended by official guidelines or FDA approved. They
are not superior to the IGRAs based on the performance
reported in study II and recent meta analysis (63). Overall
data quality in the studies of serological tests for active TB
are regarded as very low, and official recommendations
strongly advice against serological tests (131). In summary,
even though this is an unjustifiable malpractice, many
immunological tests are marketed for diagnosing active TB,
especially in high-burden countries with weak regulatory
systems.
7.3. THE FUTURE
Many questions regarding IGRAs and their role in TB
control and ultimately TB elimination in low-incidence
settings remain unanswered. Data from this thesis suggest
that a negative IGRA is valuable in ruling out TB with little

PhD Thesis Thomas Stig Hermansen
24
risk of progression to disease, and that the QFT has a high
sensitivity for TB and a high specificity when used among
the majority of patients with NTM disease. Critics often
pinpoint the low sensitivity and poor predictive value of the
IGRAs, and it is indeed not a perfect test. However,
currently IGRAs are the best available option in low-
incidence countries like Denmark, and they are important in
diagnostic algorithms as tools to identify persons with active
TB and LTBI.
When the IFN-γ based assays were introduced, it was
anticipated that they could provide the means to distinguish
active from latent TB and identify those at the highest risk
of progression. After more than a decade of studying and
reporting on IGRA performance, it has become clear that
none of the commercial IGRAs have met these expectations.
One could speculate whether IGRAs have reached their full
potential, and if the search for a better biomarker should be
prioritized rather than trying to improve existing assays
based on release of IFN-γ (77).
The discovery of a novel biomarker that is both highly
specific, sensitive and with good predictive value would be a
game changer in TB control in low-incidence countries. In
recent years many new biomarkers have emerged (79-81).
One example is the IP-10 marker and the recent
development of a dried blood spot that enables easy storage
and prolonged transport (132). IP-10 has similar properties
in separating NTM and TB, and might hold potential in
making immunological diagnosis of TB and differentiation
between TB and NTM accessible in low-income, TB high-
incidence settings (133). However, the IP-10 marker is not
commercially available and has not proven superior
compared to existing tests. Thus, until better biomarkers are
introduced, it is important to use the current available tests,
while being aware of the limitations. This is the focus of an
ongoing debate on how screening strategies using IGRAs in
high-income TB low-incidence countries should be organized
to achieve the most optimal results towards TB control and
elimination (113,134,135).
The burden of TB remains in third world countries, and
immunological assays, although important in a Danish
setting, is not useful for combating the disease measured in
terms of global morbidity and mortality. Rather, the same
basic but essential countermeasures are as important today
as they were 100 years ago.
"The disease is dying a natural death with improved
conditions of the working classes, and it is by further
developments on such lines, and not otherwise, that its
extermination will be attained."
Dr. T. D. Lister (Mount Vernon Hospital for
Consumption, Hampstead, early 20th century).

PhD Thesis Thomas Stig Hermansen
25
SUMMARY
In the past decade, the Interferon Gamma Release Assays
(IGRAs) have been increasingly used in tuberculosis (TB)
low-incidence countries for the diagnosis of both active and
latent TB. We evaluated test performance of the most widely
used IGRA, the QuantiFERON-TB Gold In-Tube test (QFT),
in a large cohort through 6 consecutive years from 2005
through 2010, and included all Danish patients with notified
TB and cultured non-tuberculous mycobacteria (NTM).
It would be of great clinical value if the QFT could serve as
a minimally invasive tool and aid in discriminating TB
disease from NTM disease. Disease caused by the majority
of NTM will not evoke a positive IGRA because they do not
cross-react with the mycobacterial antigens in the QFT. We
conducted an evaluation of IGRA performance in patients
with NTM disease, and in light of these result and available
literature, we suggest that the IGRAs could be useful in
discriminating between TB and NTM disease. Among NTM
patients, we found a high specificity of 96%, a finding which
is especially relevant in children, where lymphadenitis due
to mycobacteria from the M. avium complex are seen to
predominate and can mimic TB lymphadenitis.
The ability of the QFT to identify infection with Mtb among
patients with active TB was in line with other studies and
the overall sensitivity was 86%. Performance was poorer in
the extremes of age with lowered sensitivity among elderly
(aged >65 years) and increased indeterminate rates in
infants <1 year and elderly >65 years. We conclude that test
performance is impaired only in children aged less than 1
and elderly, and suggest revision of current guidelines
advising caution when using IGRAs in children below the
age of 5.
A pivotal measure for any diagnostic test is the prediction of
disease. We conducted the largest study to date in a TB low-
incidence setting and determined the negative predictive
value (NPV) and positive predictive value (PPV) of the test,
identifying incident TB cases during more than 50,000
person-years of follow-up. PPV was 1.3% and NPV 99,85%.
We conclude that a negative QFT in our cohort of persons
that were screened due to various indications predicts an
extremely low probability of developing TB disease. The PPV
was expectedly low, but a positive test still inferred a more
than 8 times increased risk of developing TB, with an
additional increase following the first 2 years after QFT
testing.
With the current studies, we have established and used a
comprehensive, nationwide cohort to provide novel insights
into the performance of the QFT. In summary, the test is
used extensively in Denmark both for active and latent TB.
Overall test performance is acceptable, but caution is
warranted in infants and elderly and our results suggest
that administration of preventive therapy for latent TB
could be improved. Screening indication, host susceptibility,
as well as a priori risk of TB remain vital factors to consider
both when deciding to test and when interpreting test result.

PhD Thesis Thomas Stig Hermansen
26
DANSK RESUME
I lande med en lav forekomst af tuberkulose (TB) påvises
infektion med tuberkulosebakterien i stigende grad ved
hjælp af interferon-γ release assays (IGRAs). I denne ph.d.
evaluerede vi den mest udbredte af disse tests,
QuantiFERON-TB Gold In-Tube testen (QFT) i en kohorte
bestående af alle personer med en udført test i perioden 2005
til og med 2010 i Danmark. Vi kombinerede QFT data med
alle anmeldte tilfælde af TB samt alle tilfælde af
dyrkningsverificeret sygdom forårsaget af gruppen af non
tuberkuløse mykobakterier (NTM) og undersøgte værdien af
QFT til at påvise disse sygdomme.
Det ville være en fordel hvis man kunne bruge QFT til at
skelne aktiv tuberkulose fra sygdom grundet NTM, da en
QFT er mindre invasiv end traditionel diagnostik ved
biopsitagning. Størstedelen af NTM vil give et negativt QFT
resultat, da de ikke indeholder de specifikke antigener som
testen er baseret på. Vi har evalueret QFT blandt patienter
med NTM sygdom og fandt en meget høj specificitet. Vi har
ydermere gennemgået tilgængelige studier vedrørende
IGRA og anvendelse hos patienter med NTM sygdom og
samlet set fandt vi, at testen har potentiale til at skelne
mellem TB og NTM. NTM sygdom er sjældent
forekommende, men hos især børn kan testen være relevant,
da en typisk præsentation af NTM sygdom er en hævet
lymfeknude på halsen, som klinisk kan have lighed med
glandel TB.
QFT evne til at påvise infektion med tuberkulosebakterien
blandt patienter med aktiv TB i vores kohorte var
sammenlignelig med andre studier, og samlet set var
sensitiviteten 86%. QFT var påvirket i begge ender af
aldersspektret, idet testen havde flere inkonklusive
resultater blandt både spædbørn yngre end 1 år og ældre
over 65 år. Endvidere havde testen nedsat følsomhed blandt
ældre >65 år. Vi konkluderer, at testen synes at virke godt
fra 1 år og opefter, men at man bør udvise forsigtighed når
testen anvendes hos spædbørn og ældre over 65 år, da
præstationen er nedsat blandt disse grupper. Dette er
interessant i et internationalt perspektiv, idet flere
retningslinjer fraråder testen hos børn under 5 år, hvorfor
en revision af disse bør overvejes.
En central egenskab ved en diagnostisk test er dens evne til
at forudsige udvikling af sygdom. I denne ph.d. har vi lavet
den hidtil største undersøgelse af QFT’s evne til at forudsige
udvikling af TB, og vi har bestemt den prædiktive værdi af
en positiv og negativ test i løbet af mere end 50,000
personårs opfølgning. Vi konkluderer, at den positive
prædiktive værdi er 1.3% og den negative prædiktive værdi
er 99.85%, hvilket betyder at en person der screenes, og har
en negativ test, iht. vores data har en meget lille risiko for
at udvikle TB. Hvis man har en positiv test, har man mere
end 8 gange større risiko for udvikling af TB.
Studierne i denne ph.d. har bekræftet og udbygget den viden
vi har om QFT’s anvendelse og karakteristika. QFT er meget
udbredt i Danmark og anvendes både til diagnostik af aktiv
og latent TB. Sensitiviteten af testen er acceptabel, men den
bør ikke bruges alene til påvisning af aktiv TB, og man bør
udvise forsigtighed ved tolkningen af resultater hos
spædbørn og gamle. Vores resultater tyder på, at brugen af
forebyggende behandling for at forhindre udvikling af TB
kunne optimeres. Samlet set er det vigtigt, at overveje
indikationen for at anvende testen og den individuelle
risikoprofil, når man tolker resultatet.

PhD Thesis Thomas Stig Hermansen
27
REFERENCES
(1) Hermansen TS, Thomsen VO, Lillebaek T, Ravn P. Non-
tuberculous mycobacteria and the performance of interferon gamma
release assays in denmark. PLoS One 2014 Apr 4;9(4):e93986.
(2) Hermansen T, Lillebaek T, Hansen AB, Andersen PH, Ravn P.
QuantiFERON-TB Gold In-Tube test performance in Denmark.
Tuberculosis (Edinb) 2014 Dec;94(6):616-621.
(3) Hermansen TS, Lillebaek T, Langholz Kristensen K, Andersen
PH, Ravn P. Prognostic value of interferon-gamma release assays, a
population-based study from a TB low-incidence country. Thorax
2016 Mar 30.
(4) Andersen P, Munk ME, Pollock JM, Doherty TM. Specific
immune-based diagnosis of tuberculosis. Lancet 2000 Sep
23;356(9235):1099-1104.
(5) World Health Organization W. Global Tuberculosis Report
2015. 2015;20.
(6) Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC.
Consensus statement. Global burden of tuberculosis: estimated
incidence, prevalence, and mortality by country. WHO Global
Surveillance and Monitoring Project. JAMA 1999 Aug
18;282(7):677-686.
(7) Statens Serum Institut. Overvaagning i tal, grafer og kort. 2014;
Available at:
http://www.ssi.dk/Smitteberedskab/Sygdomsovervaagning.aspx.
Accessed 03/10, 2014.
(8) Houben EN, Nguyen L, Pieters J. Interaction of pathogenic
mycobacteria with the host immune system. Curr Opin Microbiol
2006 Feb;9(1):76-85.
(9) Bozzano F, Marras F, De Maria A. Immunology of tuberculosis.
Mediterr J Hematol Infect Dis 2014 Apr 7;6(1):e2014027.
(10) Barry CE,3rd, Boshoff HI, Dartois V, Dick T, Ehrt S, Flynn J,
et al. The spectrum of latent tuberculosis: rethinking the biology and
intervention strategies. Nat Rev Microbiol 2009 Dec;7(12):845-855.
(11) Modlin RL, Bloom BR. TB or not TB: that is no longer the
question. Sci Transl Med 2013 Nov 27;5(213):213sr6.
(12) Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent
Mycobacterium tuberculosis infection. N Engl J Med 2015 May
28;372(22):2127-2135.
(13) Pai M, Denkinger CM, Kik SV, Rangaka MX, Zwerling A,
Oxlade O, et al. Gamma interferon release assays for detection of
Mycobacterium tuberculosis infection. Clin Microbiol Rev 2014
Jan;27(1):3-20.
(14) Comstock GW. Epidemiology of tuberculosis. Am Rev Respir
Dis 1982 Mar;125(3 Pt 2):8-15.
(15) Targeted tuberculin testing and treatment of latent tuberculosis
infection. This official statement of the American Thoracic Society
was adopted by the ATS Board of Directors, July 1999. This is a
Joint Statement of the American Thoracic Society (ATS) and the
Centers for Disease Control and Prevention (CDC). This statement
was endorsed by the Council of the Infectious Diseases Society of
America. (IDSA), September 1999, and the sections of this
statement. Am J Respir Crit Care Med 2000 Apr;161(4 Pt 2):S221-
47.
(16) Ferebee SH. Controlled chemoprophylaxis trials in tuberculosis.
A general review. Bibl Tuberc 1970;26:28-106.
(17) Horsburgh CR,Jr, Rubin EJ. Clinical practice. Latent
tuberculosis infection in the United States. N Engl J Med 2011 Apr
14;364(15):1441-1448.
(18) Horsburgh CR,Jr, Rubin EJ. Clinical practice. Latent
tuberculosis infection in the United States. N Engl J Med 2011 Apr
14;364(15):1441-1448.
(19) Akolo C, Adetifa I, Shepperd S, Volmink J. Treatment of latent
tuberculosis infection in HIV infected persons. Cochrane Database
Syst Rev 2010 Jan 20;(1):CD000171. doi(1):CD000171.
(20) Selwyn PA, Hartel D, Lewis VA, Schoenbaum EE, Vermund
SH, Klein RS, et al. A prospective study of the risk of tuberculosis
among intravenous drug users with human immunodeficiency virus
infection. N Engl J Med 1989 Mar 2;320(9):545-550.
(21) Soborg C, Ruhwald M, Andersen PH, Ravn P. 6-year follow-up
of 522 HIV-positive individuals screened for Mycobacterium
tuberculosis infection in Denmark. Eur Respir J 2014 May 2.
(22) Solovic I, Sester M, Gomez-Reino JJ, Rieder HL, Ehlers S,
Milburn HJ, et al. The risk of tuberculosis related to tumour necrosis
factor antagonist therapies: a TBNET consensus statement. Eur
Respir J 2010 Nov;36(5):1185-1206.
(23) Belard E, Semb S, Ruhwald M, Werlinrud AM, Soborg B,
Jensen FK, et al. Prednisolone treatment affects the performance of
the QuantiFERON gold in-tube test and the tuberculin skin test in
patients with autoimmune disorders screened for latent tuberculosis
infection. Inflamm Bowel Dis 2011 Nov;17(11):2340-2349.
(24) Al-Anazi KA, Al-Jasser AM, Alsaleh K. Infections Caused by
Mycobacterium tuberculosis in Recipients of Hematopoietic Stem
Cell Transplantation. Front Oncol 2014 Aug 26;4:231.
(25) Sidhu A, Verma G, Humar A, Kumar D. Outcome of latent
tuberculosis infection in solid organ transplant recipients over a 10-
year period. Transplantation 2014 Sep 27;98(6):671-675.
(26) Katsenos S, Nikolopoulou M, Gartzonika C, Manda-Stachouli
C, Gogali A, Grypaiou C, et al. Use of interferon-gamma release
assay for latent tuberculosis infection screening in older adults
exposed to tuberculosis in a nursing home. J Am Geriatr Soc 2011
May;59(5):858-862.
(27) Jeon CY, Murray MB. Diabetes mellitus increases the risk of
active tuberculosis: a systematic review of 13 observational studies.
PLoS Med 2008 Jul 15;5(7):e152.
(28) Baussano I, Williams BG, Nunn P, Beggiato M, Fedeli U,
Scano F. Tuberculosis incidence in prisons: a systematic review.
PLoS Med 2010 Dec 21;7(12):e1000381.
(29) Moss AR, Hahn JA, Tulsky JP, Daley CL, Small PM, Hopewell
PC. Tuberculosis in the homeless. A prospective study. Am J Respir
Crit Care Med 2000 Aug;162(2 Pt 1):460-464.
(30) Banfield S, Pascoe E, Thambiran A, Siafarikas A, Burgner D.
Factors associated with the performance of a blood-based interferon-
gamma release assay in diagnosing tuberculosis. PLoS One
2012;7(6):e38556.
(31) Dorman SE, Belknap R, Graviss EA, Reves R, Schluger N,
Weinfurter P, et al. Interferon-gamma release assays and tuberculin
skin testing for diagnosis of latent tuberculosis infection in
healthcare workers in the United States. Am J Respir Crit Care Med
2014 Jan 1;189(1):77-87.

PhD Thesis Thomas Stig Hermansen
28
(32) WHO Report. Management of latent tuberculosis
infectionGuidelines on the management of latent tuberculosis
infection. 2015.
(33) Seersholm N, Andersen P, Andersen ÅB, Thomsen VØ,
Hilberg O, Ravn P, et al. Tuberkulosebekæmpelse i Danmark. 2010.
(34) van Ingen J, Rahim Z, Mulder A, Boeree MJ, Simeone R,
Brosch R, et al. Characterization of Mycobacterium orygis as M.
tuberculosis complex subspecies. Emerg Infect Dis 2012
Apr;18(4):653-655.
(35) van Soolingen D, Hoogenboezem T, de Haas PE, Hermans PW,
Koedam MA, Teppema KS, et al. A novel pathogenic taxon of the
Mycobacterium tuberculosis complex, Canetti: characterization of
an exceptional isolate from Africa. Int J Syst Bacteriol 1997
Oct;47(4):1236-1245.
(36) Panteix G, Gutierrez MC, Boschiroli ML, Rouviere M, Plaidy
A, Pressac D, et al. Pulmonary tuberculosis due to Mycobacterium
microti: a study of six recent cases in France. J Med Microbiol 2010
Aug;59(Pt 8):984-989.
(37) World Health Organization W. Tuberculosis, fact sheet no.
104 . 2015; Available at:
http://www.who.int/mediacentre/factsheets/fs104/en/.
(38) Kommareddi S, Abramowsky CR, Swinehart GL, Hrabak L.
Nontuberculous mycobacterial infections: comparison of the
fluorescent auramine-O and Ziehl-Neelsen techniques in tissue
diagnosis. Hum Pathol 1984 Nov;15(11):1085-1089.
(39) Lillebaek T, Andersen AB, Rasmussen EM, Kamper-Jorgensen
Z, Pedersen MK, Bjorn-Mortensen K, et al. Mycobacterium
tuberculosis outbreak strain of Danish origin spreading at worrying
rates among greenland-born persons in Denmark and Greenland. J
Clin Microbiol 2013 Dec;51(12):4040-4044.
(40) Menzies D, Gardiner G, Farhat M, Greenaway C, Pai M.
Thinking in three dimensions: a web-based algorithm to aid the
interpretation of tuberculin skin test results. Int J Tuberc Lung Dis
2008 May;12(5):498-505.
(41) Menzies D. Interpretation of repeated tuberculin tests. Boosting,
conversion, and reversion. Am J Respir Crit Care Med 1999
Jan;159(1):15-21.
(42) van Ingen J, de Zwaan R, Dekhuijzen R, Boeree M, van
Soolingen D. Region of difference 1 in nontuberculous
Mycobacterium species adds a phylogenetic and taxonomical
character. J Bacteriol 2009 Sep;191(18):5865-5867.
(43) Farhat M, Greenaway C, Pai M, Menzies D. False-positive
tuberculin skin tests: what is the absolute effect of BCG and non-
tuberculous mycobacteria? Int J Tuberc Lung Dis 2006
Nov;10(11):1192-1204.
(44) O'Garra A, Redford PS, McNab FW, Bloom CI, Wilkinson RJ,
Berry MP. The immune response in tuberculosis. Annu Rev
Immunol 2013;31:475-527.
(45) Wang S, Chen J, Zhang Y, Diao N, Zhang S, Wu J, et al.
Mycobacterium tuberculosis region of difference (RD) 2 antigen
Rv1985c and RD11 antigen Rv3425 have the promising potential to
distinguish patients with active tuberculosis from M. bovis BCG-
vaccinated individuals. Clin Vaccine Immunol 2013 Jan;20(1):69-
76.
(46) Harboe M, Oettinger T, Wiker HG, Rosenkrands I, Andersen P.
Evidence for occurrence of the ESAT-6 protein in Mycobacterium
tuberculosis and virulent Mycobacterium bovis and for its absence in
Mycobacterium bovis BCG. Infect Immun 1996 Jan;64(1):16-22.
(47) Falkinham JO,3rd. Nontuberculous mycobacteria in the
environment. Clin Chest Med 2002 Sep;23(3):529-551.
(48) von Reyn CF, Waddell RD, Eaton T, Arbeit RD, Maslow JN,
Barber TW, et al. Isolation of Mycobacterium avium complex from
water in the United States, Finland, Zaire, and Kenya. J Clin
Microbiol 1993 Dec;31(12):3227-3230.
(49) Griffith DE, Aksamit T, Brown-Elliott BA, Catanzaro A, Daley
C, Gordin F, et al. An official ATS/IDSA statement: diagnosis,
treatment, and prevention of nontuberculous mycobacterial diseases.
Am J Respir Crit Care Med 2007 Feb 15;175(4):367-416.
(50) Andrejak C, Thomsen VO, Johansen IS, Riis A, Benfield TL,
Duhaut P, et al. Nontuberculous pulmonary mycobacteriosis in
Denmark: incidence and prognostic factors. Am J Respir Crit Care
Med 2010 Mar 1;181(5):514-521.
(51) Marras TK, Mehta M, Chedore P, May K, Al Houqani M,
Jamieson F. Nontuberculous mycobacterial lung infections in
Ontario, Canada: clinical and microbiological characteristics. Lung
2010 Aug;188(4):289-299.
(52) Winthrop KL, McNelley E, Kendall B, Marshall-Olson A,
Morris C, Cassidy M, et al. Pulmonary nontuberculous
mycobacterial disease prevalence and clinical features: an emerging
public health disease. Am J Respir Crit Care Med 2010 Oct
1;182(7):977-982.
(53) Prevots DR, Shaw PA, Strickland D, Jackson LA, Raebel MA,
Blosky MA, et al. Nontuberculous mycobacterial lung disease
prevalence at four integrated health care delivery systems. Am J
Respir Crit Care Med 2010 Oct 1;182(7):970-976.
(54) Brode SK, Jamieson FB, Ng R, Campitelli MA, Kwong JC,
Paterson JM, et al. Increased risk of mycobacterial infections
associated with anti-rheumatic medications. Thorax 2015
Jul;70(7):677-682.
(55) Haverkamp MH, Arend SM, Lindeboom JA, Hartwig NG, van
Dissel JT. Nontuberculous mycobacterial infection in children: a 2-
year prospective surveillance study in the Netherlands. Clin Infect
Dis 2004 Aug 15;39(4):450-456.
(56) Pedersen CB, Gotzsche H, Moller JO, Mortensen PB. The
Danish Civil Registration System. A cohort of eight million persons.
Dan Med Bull 2006 Nov;53(4):441-449.
(57) Statens Serum Institut, Department of Infectious Disease
Epidemiology. TB surveillance in Denmark. 2016; Available at:
http://www.ssi.dk/Smitteberedskab/Sygdomsovervaagning/Sygdoms
data.aspx?sygdomskode=TUBE&xaxis=Aar&show=&datatype=Indi
vidual&extendedfilters=False#HeaderText.
(58) National board of health, Denmark. Form 1515. 2016;
Available at: http://www.ssi.dk/~/media/Indhold/DK%20-
%20dansk/Smitteberedskab/Overvaagning%20i%20Danmark/Lovpl
igtige%20meldesystemer/formular_1515.ashx.
(59) R core team 2014. R Core Team (2014). R: A language and
environment for statistical
computing. R Foundation for Statistical Computing, Vienna,
Austria.
URL http://www.R-project.org/. 2014; Available at: www.r-
project.com.
(60) Beffa P, Zellweger A, Janssens JP, Wrighton-Smith P,
Zellweger JP. Indeterminate test results of T-SPOT.TB performed
under routine field conditions. Eur Respir J 2008 Apr;31(4):842-
846.

PhD Thesis Thomas Stig Hermansen
29
(61) Ravn P, Munk ME, Andersen AB, Lundgren B, Lundgren JD,
Nielsen LN, et al. Prospective evaluation of a whole-blood test using
Mycobacterium tuberculosis-specific antigens ESAT-6 and CFP-10
for diagnosis of active tuberculosis. Clin Diagn Lab Immunol 2005
Apr;12(4):491-496.
(62) Sester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB,
et al. Interferon-gamma release assays for the diagnosis of active
tuberculosis: a systematic review and meta-analysis. Eur Respir J
2011 Jan;37(1):100-111.
(63) Pai M, Denkinger CM, Kik SV, Rangaka MX, Zwerling A,
Oxlade O, et al. Gamma Interferon Release Assays for Detection of
Mycobacterium tuberculosis Infection. Clin Microbiol Rev 2014
Jan;27(1):3-20.
(64) Sester M, Sotgiu G, Lange C, Giehl C, Girardi E, Migliori GB,
et al. Interferon-gamma release assays for the diagnosis of active
tuberculosis: a systematic review and meta-analysis. Eur Respir J
2011 Jan;37(1):100-111.
(65) Santin M, Munoz L, Rigau D. Interferon-gamma release assays
for the diagnosis of tuberculosis and tuberculosis infection in HIV-
infected adults: a systematic review and meta-analysis. PLoS One
2012;7(3):e32482.
(66) Mandalakas AM, Detjen AK, Hesseling AC, Benedetti A,
Menzies D. Interferon-gamma release assays and childhood
tuberculosis: systematic review and meta-analysis. Int J Tuberc
Lung Dis 2011 Aug;15(8):1018-1032.
(67) European Center for Disease Prevention and Control. Use of
interferon-gamma release assays in support of TB diagnosis. 2011.
(68) Ling DI, Pai M, Davids V, Brunet L, Lenders L, Meldau R, et
al. Are interferon-gamma release assays useful for diagnosing active
tuberculosis in a high-burden setting? Eur Respir J 2011
Sep;38(3):649-656.
(69) Rangaka MX, Gideon HP, Wilkinson KA, Pai M, Mwansa-
Kambafwile J, Maartens G, et al. Interferon release does not add
discriminatory value to smear-negative HIV-tuberculosis algorithms.
Eur Respir J 2012 Jan;39(1):163-171.
(70) Metcalfe JZ, Cattamanchi A, Vittinghoff E, Ho C, Grinsdale J,
Hopewell PC, et al. Evaluation of quantitative IFN-gamma response
for risk stratification of active tuberculosis suspects. Am J Respir
Crit Care Med 2010 Jan 1;181(1):87-93.
(71) Ling DI, Nicol MP, Pai M, Pienaar S, Dendukuri N, Zar HJ.
Incremental value of T-SPOT.TB for diagnosis of active pulmonary
tuberculosis in children in a high-burden setting: a multivariable
analysis. Thorax 2013 Sep;68(9):860-866.
(72) Diel R, Loddenkemper R, Niemann S, Meywald-Walter K,
Nienhaus A. Negative and positive predictive value of a whole-
blood interferon-gamma release assay for developing active
tuberculosis: an update. Am J Respir Crit Care Med 2011 Jan
1;183(1):88-95.
(73) Doherty TM, Demissie A, Olobo J, Wolday D, Britton S,
Eguale T, et al. Immune responses to the Mycobacterium
tuberculosis-specific antigen ESAT-6 signal subclinical infection
among contacts of tuberculosis patients. J Clin Microbiol 2002
Feb;40(2):704-706.
(74) Pai M, Joshi R, Dogra S, Mendiratta DK, Narang P, Kalantri S,
et al. Serial testing of health care workers for tuberculosis using
interferon-gamma assay. Am J Respir Crit Care Med 2006 Aug
1;174(3):349-355.
(75) Bakir M, Millington KA, Soysal A, Deeks JJ, Efee S, Aslan Y,
et al. Prognostic value of a T-cell-based, interferon-gamma
biomarker in children with tuberculosis contact. Ann Intern Med
2008 Dec 2;149(11):777-787.
(76) Zellweger JP, Sotgiu G, Block M, Dore S, Altet N, Blunschi R,
et al. Risk Assessment of Tuberculosis in Contacts by Interferon-
gamma Release Assays (IGRAs). A TBNET Study. Am J Respir
Crit Care Med 2015 Mar 12.
(77) QUIAGEN. QuantiFERON®-TB Gold Plus (QFT®-Plus)
ELISA Package Insert. 2016; Available at:
http://www.quantiferon.com/irm/content/PI/QFT/PLUS/2PK-
Elisa/UK.pdf.
(78) Barcellini L, Borroni E, Brown J, Brunetti E, Codecasa L,
Cugnata F, et al. First independent evaluation of QuantiFERON-TB
Plus performance. Eur Respir J 2016 Feb 11.
(79) Chegou NN, Heyckendorf J, Walzl G, Lange C, Ruhwald M.
Beyond the IFN-gamma horizon: biomarkers for immunodiagnosis
of infection with Mycobacterium tuberculosis. Eur Respir J 2014
May;43(5):1472-1486.
(80) Petruccioli E, Petrone L, Vanini V, Cuzzi G, Navarra A,
Gualano G, et al. Assessment of CD27 expression as a tool for
active and latent tuberculosis diagnosis. J Infect 2015
Nov;71(5):526-533.
(81) Guggino G, Orlando V, Cutrera S, La Manna MP, Di Liberto
D, Vanini V, et al. Granzyme A as a potential biomarker of
Mycobacterium tuberculosis infection and disease. Immunol Lett
2015 Aug;166(2):87-91.
(82) Latorre I, Domínguez J. Dormancy antigens as biomarkers of
latent tuberculosis infection. EBioMedicine 2015 Jun 19;2(8):790-
791.
(83) Kobashi Y, Mouri K, Yagi S, Obase Y, Miyashita N, Okimoto
N, et al. Clinical evaluation of the QuantiFERON-TB Gold test in
patients with non-tuberculous mycobacterial disease. Int J Tuberc
Lung Dis 2009 Nov;13(11):1422-1426.
(84) Lein AD, von Reyn CF, Ravn P, Horsburgh CR,Jr, Alexander
LN, Andersen P. Cellular immune responses to ESAT-6
discriminate between patients with pulmonary disease due to
Mycobacterium avium complex and those with pulmonary disease
due to Mycobacterium tuberculosis. Clin Diagn Lab Immunol 1999
Jul;6(4):606-609.
(85) Detjen AK, Keil T, Roll S, Hauer B, Mauch H, Wahn U, et al.
Interferon-gamma release assays improve the diagnosis of
tuberculosis and nontuberculous mycobacterial disease in children in
a country with a low incidence of tuberculosis. Clin Infect Dis 2007
Aug 1;45(3):322-328.
(86) Wang JY, Chou CH, Lee LN, Hsu HL, Jan IS, Hsueh PR, et al.
Diagnosis of tuberculosis by an enzyme-linked immunospot assay
for interferon-gamma. Emerg Infect Dis 2007 Apr;13(4):553-558.
(87) Siddiqi UR, Chagan-Yasutan H, Nakajima C, Saitoh H, Ashino
Y, Usami O, et al. Distinct clinical features in nontuberculous
mycobacterial disease with or without latent tuberculosis infection.
Tohoku J Exp Med 2012;226(4):313-319.
(88) Ra SW, Lyu J, Choi CM, Oh YM, Lee SD, Kim WS, et al.
Distinguishing tuberculosis from Mycobacterium avium complex
disease using an interferon-gamma release assay. Int J Tuberc Lung
Dis 2011 May;15(5):635-640.
(89) Park SY, Jeon K, Um SW, Kwon OJ, Kang ES, Koh WJ.
Clinical utility of the QuantiFERON-TB Gold In-Tube test for the

PhD Thesis Thomas Stig Hermansen
30
diagnosis of active pulmonary tuberculosis. Scand J Infect Dis
2009;41(11-12):818-822.
(90) Adams LV, Waddell RD, Von Reyn CF. T-SPOT.TB Test(R)
results in adults with Mycobacterium avium complex pulmonary
disease. Scand J Infect Dis 2008;40(3):196-203.
(91) van Leeuwen RM, Bossink AW, Thijsen SF. Exclusion of
active Mycobacterium tuberculosis complex infection with the T-
SPOT.TB assay. Eur Respir J 2007 Mar;29(3):605-607.
(92) Kobashi Y, Obase Y, Fukuda M, Yoshida K, Miyashita N, Oka
M. Clinical reevaluation of the QuantiFERON TB-2G test as a
diagnostic method for differentiating active tuberculosis from
nontuberculous mycobacteriosis. Clin Infect Dis 2006 Dec
15;43(12):1540-1546.
(93) Kuznetcova TI, Sauty A, Herbort CP. Uveitis with occult
choroiditis due to Mycobacterium kansasii: limitations of interferon-
gamma release assay (IGRA) tests (case report and mini-review on
ocular non-tuberculous mycobacteria and IGRA cross-reactivity). Int
Ophthalmol 2012 Jun 2.
(94) Machingaidze S, Wiysonge CS, Gonzalez-Angulo Y, Hatherill
M, Moyo S, Hanekom W, et al. The utility of an interferon gamma
release assay for diagnosis of latent tuberculosis infection and
disease in children: a systematic review and meta-analysis. Pediatr
Infect Dis J 2011 Aug;30(8):694-700.
(95) Mandalakas AM, Detjen AK, Hesseling AC, Benedetti A,
Menzies D. Interferon-gamma release assays and childhood
tuberculosis: systematic review and meta-analysis. Int J Tuberc
Lung Dis 2011 Aug;15(8):1018-1032.
(96) Debord C, De Lauzanne A, Gourgouillon N, Guerin-El
Khourouj V, Pedron B, Gaudelus J, et al. Interferon-gamma release
assay performance for diagnosing tuberculosis disease in 0- to 5-
year-old children. Pediatr Infect Dis J 2011 Nov;30(11):995-997.
(97) Blandinieres A, de Lauzanne A, Guerin-El Khourouj V,
Gourgouillon N, See H, Pedron B, et al. QuantiFERON to diagnose
infection by Mycobacterium tuberculosis: performance in infants
and older children. J Infect 2013 Nov;67(5):391-398.
(98) Rose MV, Kimaro G, Nissen TN, Kroidl I, Hoelscher M,
Bygbjerg IC, et al. QuantiFERON(R)-TB gold in-tube performance
for diagnosing active tuberculosis in children and adults in a high
burden setting. PLoS One 2012;7(7):e37851.
(99) Gasparoni A, Ciardelli L, Avanzini A, Castellazzi AM, Carini
R, Rondini G, et al. Age-related changes in intracellular TH1/TH2
cytokine production, immunoproliferative T lymphocyte response
and natural killer cell activity in newborns, children and adults. Biol
Neonate 2003;84(4):297-303.
(100) Basu Roy R, Sotgiu G, Altet-Gomez N, Tsolia M, Ruga E,
Velizarova S, et al. Identifying predictors of interferon-gamma
release assay results in pediatric latent tuberculosis: a protective role
of bacillus Calmette-Guerin?: a pTB-NET collaborative study. Am J
Respir Crit Care Med 2012 Aug 15;186(4):378-384.
(101) Bergamini BM, Losi M, Vaienti F, D'Amico R, Meccugni B,
Meacci M, et al. Performance of commercial blood tests for the
diagnosis of latent tuberculosis infection in children and adolescents.
Pediatrics 2009 Mar;123(3):e419-24.
(102) Critselis E, Amanatidou V, Syridou G, Spyridis NP, Mavrikou
M, Papadopoulos NG, et al. The effect of age on whole blood
interferon-gamma release assay response among children
investigated for latent tuberculosis infection. J Pediatr 2012
Oct;161(4):632-638.
(103) Haustein T, Ridout DA, Hartley JC, Thaker U, Shingadia D,
Klein NJ, et al. The likelihood of an indeterminate test result from a
whole-blood interferon-gamma release assay for the diagnosis of
Mycobacterium tuberculosis infection in children correlates with age
and immune status. Pediatr Infect Dis J 2009 Aug;28(8):669-673.
(104) Pavic I, Topic RZ, Raos M, Aberle N, Dodig S. Interferon-
gamma release assay for the diagnosis of latent tuberculosis in
children younger than 5 years of age. Pediatr Infect Dis J 2011
Oct;30(10):866-870.
(105) Murasko DM, Nelson BJ, Silver R, Matour D, Kaye D.
Immunologic response in an elderly population with a mean age of
85. Am J Med 1986 Oct;81(4):612-618.
(106) de Visser V, Sotgiu G, Lange C, Aabye MG, Bakker M,
Bartalesi F, et al. False-negative interferon-gamma release assay
results in active tuberculosis: a TBNET study. Eur Respir J 2015
Jan;45(1):279-283.
(107) Diel R, Goletti D, Ferrara G, Bothamley G, Cirillo D,
Kampmann B, et al. Interferon-gamma release assays for the
diagnosis of latent Mycobacterium tuberculosis infection: a
systematic review and meta-analysis. Eur Respir J 2011
Jan;37(1):88-99.
(108) Jensen SG, Olsen NW, Seersholm N, Lillebaek T, Wilcke T,
Pedersen MK, et al. Screening for TB by sputum culture in high-risk
groups in Copenhagen, Denmark: a novel and promising approach.
Thorax 2015 Oct;70(10):979-983.
(109) Rangaka MX, Wilkinson KA, Glynn JR, Ling D, Menzies D,
Mwansa-Kambafwile J, et al. Predictive value of interferon-gamma
release assays for incident active tuberculosis: a systematic review
and meta-analysis. Lancet Infect Dis 2012 Jan;12(1):45-55.
(110) Torres Costa J, Silva R, Ringshausen FC, Nienhaus A.
Screening for tuberculosis and prediction of disease in Portuguese
healthcare workers. J Occup Med Toxicol 2011 Jun 9;6:19-6673-6-
19.
(111) Rieder HL, Cauthen GM, Comstock GW, Snider DE,Jr.
Epidemiology of tuberculosis in the United States. Epidemiol Rev
1989;11:79-98.
(112) Lange C, Rieder HL. Intention to test is intention to treat. Am
J Respir Crit Care Med 2011 Jan 1;183(1):3-4.
(113) Sester M, van Crevel R, Leth F, Lange C. Numbers needed to
treat to prevent tuberculosis. Eur Respir J 2015 Dec;46(6):1836-
1838.
(114) Geis S, Bettge-Weller G, Goetsch U, Bellinger O, Ballmann
G, Hauri AM. How can we achieve better prevention of progression
to tuberculosis among contacts? Eur Respir J 2013 Dec;42(6):1743-
1746.
(115) Sloot R, Schim van der Loeff MF, Kouw PM, Borgdorff MW.
Risk of tuberculosis after recent exposure. A 10-year follow-up
study of contacts in Amsterdam. Am J Respir Crit Care Med 2014
Nov 1;190(9):1044-1052.
(116) Sester M, van Leth F, Bruchfeld J, Bumbacea D, Cirillo DM,
Dilektasli AG, et al. Risk assessment of tuberculosis in
immunocompromised patients. A TBNET study. Am J Respir Crit
Care Med 2014 Nov 15;190(10):1168-1176.
(117) Schablon A, Nienhaus A, Ringshausen FC, Preisser AM,
Peters C. Occupational screening for tuberculosis and the use of a
borderline zone for interpretation of the IGRA in German healthcare
workers. PLoS One 2014 Dec 26;9(12):e115322.

PhD Thesis Thomas Stig Hermansen
31
(118) Dorman SE, Belknap R, Graviss EA, Reves R, Schluger N,
Weinfurter P, et al. Interferon-gamma release assays and tuberculin
skin testing for diagnosis of latent tuberculosis infection in
healthcare workers in the United States. Am J Respir Crit Care Med
2014 Jan 1;189(1):77-87.
(119) Slater ML, Welland G, Pai M, Parsonnet J, Banaei N.
Challenges with QuantiFERON-TB Gold Assay for Large-Scale,
Routine Screening of US Healthcare Workers. Am J Respir Crit
Care Med 2013 Aug 26.
(120) Kopanoff DE, Snider DE,Jr, Caras GJ. Isoniazid-related
hepatitis: a U.S. Public Health Service cooperative surveillance
study. Am Rev Respir Dis 1978 Jun;117(6):991-1001.
(121) Stead WW, Lofgren JP, Warren E, Thomas C. Tuberculosis as
an endemic and nosocomial infection among the elderly in nursing
homes. N Engl J Med 1985 Jun 6;312(23):1483-1487.
(122) Marais BJ, Gie RP, Schaaf HS, Beyers N, Donald PR, Starke
JR. Childhood pulmonary tuberculosis: old wisdom and new
challenges. Am J Respir Crit Care Med 2006 May 15;173(10):1078-
1090.
(123) Fong KS, Tomford JW, Teixeira L, Fraser TG, van Duin D,
Yen-Lieberman B, et al. Challenges of interferon-gamma release
assay conversions in serial testing of health-care workers in a TB
control program. Chest 2012 Jul;142(1):55-62.
(124) Danielsen AV, Floe A, Lillebaek T, Hoffmann HJ, Hilberg O.
An interferon-gamma release assay test performs well in routine
screening for tuberculosis. Dan Med J 2014 Jun;61(6):A4856.
(125) Browatzki A, Meyer CN. Interferon-gamma release assay on
suspicion of active tuberculosis? Ugeskr Laeger 2009 Sep
7;171(37):2631-2635.
(126) World Health Organization Country Office for India.
Standards for TB Care in India
. 2014.
(127) World Health Organization W. Guidelines for intensified
tuberculosis case-finding and isoniazid preventive therapy for people
living with HIV in resource-constrained settings. 2011.
(128) World Health Organization W. Recommendations for
investigating contacts of persons with infectious tuberculosis in low-
and middleincome countries. 2011.
(129) Hoff ST, Peter JG, Theron G, Pascoe M, Tingskov PN,
Aggerbeck H, et al. Sensitivity of C-Tb: a novel RD-1-specific skin
test for the diagnosis of tuberculosis infection. Eur Respir J 2016
Mar;47(3):919-928.
(130) Little KM, Pai M, Dowdy DW. Costs and Consequences of
Using Interferon-gamma Release Assays for the Diagnosis of Active
Tuberculosis in India. PLoS One 2015 Apr 28;10(4):e0124525.
(131) World Health Organization W. Commercial Serodiagnostic
Tests for Diagnosis of Tuberculosis, Policy Statement. 2011.
(132) Blauenfeldt T, Heyckendorf J, Graff Jensen S, Lange C, Drabe
C, Hermansen TS, et al. Development of a one-step probe based
molecular assay for rapid immunodiagnosis of infection with M.
tuberculosis using dried blood spots. PLoS One 2014 Sep
3;9(9):e105628.
(133) Alsleben N, Ruhwald M, Russmann H, Marx FM, Wahn U,
Magdorf K. Interferon-gamma inducible protein 10 as a biomarker
for active tuberculosis and latent tuberculosis infection in children: a
case-control study. Scand J Infect Dis 2012 Apr;44(4):256-262.
(134) Lonnroth K, Migliori GB, Abubakar I, D'Ambrosio L, de
Vries G, Diel R, et al. Towards tuberculosis elimination: an action
framework for low-incidence countries. Eur Respir J 2015
Apr;45(4):928-952.
(135) Matteelli A, Lonnroth K, Getahun H, Falzon D, Migliori GB,
Raviglione M. Numbers needed to treat to prevent tuberculosis. Eur
Respir J 2015 Dec;46(6):1838-1839.