
Interferon gamma release assay in diagnosis of pediatric tuberculosis: a meta-analysis
9
RESEARCH ARTICLE Interferon gamma release assay in diagnosis of pediatric tuberculosis: a meta-analysis Lin Sun, Jing Xiao, Qing Miao, Wei-xing Feng, Xi-rong Wu, Qing-qin Yin, Wei-wei Jiao, Chen Shen, Fang Liu, Dan Shen & A-dong Shen National Key Discipline of Pediatrics, (Capital Medical University), Ministry of Education, Key Laboratory of Major Diseases in Children, (Capital Medical University), Ministry of Education, Beijing Pediatric Research Institute, Beijing Children’s Hospital, Beijing, China Correspondence: A-dong Shen, Beijing Pediatric Institute, Beijing Children’s Hospital affiliated to Capital Medical University, 56 Nan Li Shi Road, Xi Cheng District, Beijing 100045, China. Tel.: +8610 59718655; fax: +8610 59718662; e-mail: [email protected] Received 24 March 2011; revised 15 June 2011; accepted 28 June 2011. Final version published online 23 August 2011. DOI: 10.1111/j.1574-695X.2011.00838.x Editor: Patrick Brennan Keywords meta-analysis; interferon gamma; diagnosis; tuberculosis; children. Abstract Although interferon gamma release assays (IGRAs) have been widely used for the diagnosis of latent and active tuberculosis in adults, a relative lack of vali- dation studies in children has led to caution in their clinical interpretation. This meta-analysis systematically evaluated two IGRAs (ELISA and ELISPOT) and the tuberculin skin test (TST). We searched databases (PubMed, MED- LINE, Ovid) between January 2000 and January 2011 using search terms of latent tuberculosis infection or tuberculosis and interferon gamma release assay, or T-SPOT.TB test, or QuantiFERON-TB Gold, or ESAT-6, or CFP-10, and child, or childhood, or pediatrics. We also collected data by performing a manual search of references from relevant articles and communicating with selected authors. The meta-analysis was conducted with random effects models to account for heterogeneity between selected studies. The sensitivities of all three tests in active tuberculosis were similar. The pooled sensitivity was 70% for ELISA studies, 62% for ELISPOT studies and 71% for TST. Calculated sen- sitivities for IGRAs and the TST differ in culture-confirmed tuberculosis [ELISA (85%) vs. ELISPOT (76%) vs. TST (85%)] and clinical diagnosed cases [ELISA (64%) vs. ELISPOT (58%) vs. TST (66%)]. The pooled specificity was 100% for ELISA and 90% for ELISPOT, but was much lower for TST [56% in all included studies and 49% in children with bacillus Calmette-Guerin (BCG) vaccination]. The agreement between the TST and IGRAs in non-BCG-vacci- nated children is higher than that in BCG-vaccinated children. In the diagnosis of active tuberculosis in children, the TST and IGRAs have similar sensitivity. By contrast, the specificity of IGRAs is far greater than the TST, particularly in children with previous BCG vaccination. Introduction Childhood tuberculosis is commonly extra-pulmonary, disseminated and severe, especially in children under 3 years of age, and is associated with high morbidity and mortality (Marais et al., 2006). In children, diagnosis of tuberculosis is complicated by its pauci-bacillary nature, resulting in atypical clinical signs and a lower probability of bacteriological confirmation (Rigouts, 2009). Currently, the diagnosis of latent tuberculosis infection (LTBI) is hindered by the lack of a ‘gold standard’. The tuberculin skin test (TST) was until recently the main method of detecting Mycobacterium tuberculosis infection and in diagnosing active tuberculosis. The TST uses a poorly defined mix of antigens from M. tuberculosis resulting in false-positive responses because of nontuberculous myco- bacteria (NTM) infection or previous bacillus Calmette- Guerin (BCG) vaccination. False-negative TST results can occur when children suffer from severe active tuberculosis or immune suppression. Therefore, alternative diagnostic tools for the detec- tion of tuberculosis have been explored. The interferon FEMS Immunol Med Microbiol 63 (2011) 165–173 ª2011 Federation of European Microbiological Societies Published by Blackwell Publishing Ltd. All rights reserved IMMUNOLOGY & MEDICAL MICROBIOLOGY
Transcript of Interferon gamma release assay in diagnosis of pediatric tuberculosis: a meta-analysis

R E S EA RCH AR T I C L E
Interferon gamma release assay in diagnosis of pediatrictuberculosis: a meta-analysis
Lin Sun, Jing Xiao, Qing Miao, Wei-xing Feng, Xi-rong Wu, Qing-qin Yin, Wei-wei Jiao, Chen Shen,Fang Liu, Dan Shen & A-dong Shen
National Key Discipline of Pediatrics, (Capital Medical University), Ministry of Education, Key Laboratory of Major Diseases in Children, (Capital
Medical University), Ministry of Education, Beijing Pediatric Research Institute, Beijing Children’s Hospital, Beijing, China
Correspondence: A-dong Shen, Beijing
Pediatric Institute, Beijing Children’s
Hospital affiliated to Capital Medical
University, 56 Nan Li Shi Road, Xi Cheng
District, Beijing 100045, China. Tel.: +8610
59718655; fax: +8610 59718662; e-mail:
Received 24 March 2011; revised 15 June
2011; accepted 28 June 2011.
Final version published online 23 August
2011.
DOI: 10.1111/j.1574-695X.2011.00838.x
Editor: Patrick Brennan
Keywords
meta-analysis; interferon gamma; diagnosis;
tuberculosis; children.
Abstract
Although interferon gamma release assays (IGRAs) have been widely used for
the diagnosis of latent and active tuberculosis in adults, a relative lack of vali-
dation studies in children has led to caution in their clinical interpretation.
This meta-analysis systematically evaluated two IGRAs (ELISA and ELISPOT)
and the tuberculin skin test (TST). We searched databases (PubMed, MED-
LINE, Ovid) between January 2000 and January 2011 using search terms of
latent tuberculosis infection or tuberculosis and interferon gamma release
assay, or T-SPOT.TB test, or QuantiFERON-TB Gold, or ESAT-6, or CFP-10,
and child, or childhood, or pediatrics. We also collected data by performing a
manual search of references from relevant articles and communicating with
selected authors. The meta-analysis was conducted with random effects models
to account for heterogeneity between selected studies. The sensitivities of all
three tests in active tuberculosis were similar. The pooled sensitivity was 70%
for ELISA studies, 62% for ELISPOT studies and 71% for TST. Calculated sen-
sitivities for IGRAs and the TST differ in culture-confirmed tuberculosis
[ELISA (85%) vs. ELISPOT (76%) vs. TST (85%)] and clinical diagnosed cases
[ELISA (64%) vs. ELISPOT (58%) vs. TST (66%)]. The pooled specificity was
100% for ELISA and 90% for ELISPOT, but was much lower for TST [56% in
all included studies and 49% in children with bacillus Calmette-Guerin (BCG)
vaccination]. The agreement between the TST and IGRAs in non-BCG-vacci-
nated children is higher than that in BCG-vaccinated children. In the diagnosis
of active tuberculosis in children, the TST and IGRAs have similar sensitivity.
By contrast, the specificity of IGRAs is far greater than the TST, particularly in
children with previous BCG vaccination.
Introduction
Childhood tuberculosis is commonly extra-pulmonary,
disseminated and severe, especially in children under
3 years of age, and is associated with high morbidity and
mortality (Marais et al., 2006). In children, diagnosis of
tuberculosis is complicated by its pauci-bacillary nature,
resulting in atypical clinical signs and a lower probability
of bacteriological confirmation (Rigouts, 2009). Currently,
the diagnosis of latent tuberculosis infection (LTBI) is
hindered by the lack of a ‘gold standard’. The tuberculin
skin test (TST) was until recently the main method of
detecting Mycobacterium tuberculosis infection and in
diagnosing active tuberculosis. The TST uses a poorly
defined mix of antigens from M. tuberculosis resulting in
false-positive responses because of nontuberculous myco-
bacteria (NTM) infection or previous bacillus Calmette-
Guerin (BCG) vaccination. False-negative TST results can
occur when children suffer from severe active tuberculosis
or immune suppression.
Therefore, alternative diagnostic tools for the detec-
tion of tuberculosis have been explored. The interferon
FEMS Immunol Med Microbiol 63 (2011) 165–173 ª2011 Federation of European Microbiological SocietiesPublished by Blackwell Publishing Ltd. All rights reserved
IMM
UN
OLO
GY
& M
EDIC
AL
MIC
ROBI
OLO
GY

gamma release assays (IGRAs) are based on two antigens:
the early-secreted antigenic target 6-kDa protein (ESAT-6)
and culture filtrate protein 10 (CFP-10). Several com-
mercially available IGRA tests have been developed to
assist in the diagnosis of latent and active M. tuberculosis
infection, including the T-SPOT.TB test (TSPOT)
(Oxford Immunotec, Oxford, UK) and QuantiFERON-TB
Gold (QFT-G) or QuantiFERON-TB Gold In-Tube
(QFT-IT) (Cellestis, Carnegie, Australia). TSPOT uses the
ELISPOT (enzyme-linked immunosorbent spot) tech-
nique to measure the number of individual mycobacte-
rium-specific T cells. QFT-G and QFT-IT measure the
concentration of interferon gamma produced in whole
blood with enzyme-linked immunosorbent assay (ELISA).
The assays have been widely used for identifying or
diagnosing tuberculosis infection and have become useful
additional tests in the diagnosis of active tuberculosis in
adults. In contrast, only a few studies have reported their
utility in children. Therefore, in this meta-analysis, we
aimed to compare the sensitivity and specificity of com-
mercial IGRAs with the TST in pediatric tuberculosis.
Materials and methods
Study strategy
We conducted a literature search of databases (PubMed,
MEDLINE, Ovid) for articles published between January
2000 and January 2011. Search terms included latent
tuberculosis infection or tuberculosis and interferon
gamma release assay, or T-SPOT.TB test, or Quanti
FERON-TB Gold, or ESAT-6 or CFP-10, and child, or
childhood or pediatrics. We performed manual searches
of the references from relevant articles and corresponded
with the authors of some articles for complete informa-
tion.
Articles were included if they met the following selec-
tion criteria.
(1) Articles that reported original data were included;
reviews, case reports and editorials were excluded. Articles
with fewer than five enrolled subjects were excluded.
(2) Studies that presented data on the sensitivity and
specificity of the commercial versions of IGRAs, including
T-SPOT.TB, QuantiFERON-TB Gold or QuantiFERON-
TB Gold In-Tube, were included. For studies assessing
sensitivity, the participants were required to have active
tuberculosis confirmed by bacteriological evidence or
diagnosed by clinical evidence. For studies assessing speci-
ficity, the participants should be low-risk individuals
without identified exposure to active tuberculosis. Partici-
pants coinfected with HIV or other immune compro-
mises and those who had received antituberculosis
treatment were excluded.
(3) In studies that evaluated the concordance of the
tests, all tests should have been done simultaneously and
in the same people to ensure comparability.
Two independent reviewers (L.S. and J.X.) performed
searches and selected articles according to the inclusion
criteria designed in advance. One reviewer abstracted
both the test and participant characteristics of the arti-
cles collected. A second reviewer double-checked these
data.
Statistical analysis
For each study, we calculated sensitivity, specificity, posi-
tive rate and 95% confidence intervals (CIs) and summa-
rized the results in forest plots. Studies were weighted by
total sample size to pool estimates of sensitivity and spec-
ificity across the studies. Statistical analysis was conducted
using META-DISC, version 1.4 (Hospital Ramony Cajal,
Madrid, Spain). We evaluated heterogeneity by using the
chi-square test and I2 test. The random effects model
(DerSimonian and Laird) was performed when heteroge-
neity was present (P < 0.05 and I2 > 50%), and the fixed
effects model (Mantel–Haenszel) otherwise.
Results
Eligible studies
After independent review, 16 articles including 598
patients with tuberculosis and 432 controls were available
for analysis. Twelve of these studies were published in the
last 3 years (Fig. 1). Fourteen studies assessed sensitivity
of IGRAs and the TST among children diagnosed with
active tuberculosis. Of these, nine studies performed
ELISA, and 10 studies performed ELISPOT. Seven studies
assessed specificity of IGRAs and the TST among control
children without identified tuberculosis exposure. Of
these, three studies used ELISA and five studies used
ELISPOT (Table 1).
Sensitivity of IGRAs and the TST
For studies assessing sensitivity, the active tuberculosis
cases were confirmed by culture or by standard clinical
criteria. All cases were without HIV infection. Figure 2
shows the separate sensitivities of all three tests in active
tuberculosis. For ELISA, nine studies could be included,
resulting in a pooled sensitivity of 70% (229/328, 95% CI
65–75%). For ELISPOT, 10 studies were included, result-
ing in a pooled sensitivity of 62% (277/443, 95% CI 57–67%). For the TST, 12 studies were available, resulting in
a pooled sensitivity of 71% (365/512, 95% CI 67–75%).
Levels of heterogeneity between the studies were high
ª2011 Federation of European Microbiological Societies FEMS Immunol Med Microbiol 63 (2011) 165–173Published by Blackwell Publishing Ltd. All rights reserved
166 L. Sun et al.

(I2 = 80.3% for ELISA, 92.3% for ELISPOT, 85.8% for
TST).
Tuberculosis patients were further divided into two sub-
groups: culture-confirmed tuberculosis and clinically diag-
nosed tuberculosis. We observed an increased pooled
sensitivity for ELISA (85%), ELISPOT (76%) and TST
(85%) in the former subgroup, while the pooled sensitivity
dropped distinctly in cases diagnosed clinically, with sensi-
tivity for ELISA (64%), ELISPOT (58%) and TST (66%).
We then divided tuberculosis patients by grouping
their countries according to tuberculosis incidence rates.
High-incidence-rate countries (� 50 per 100 000) included
India, China, South Africa and Lithuania. All acceptable
published studies for ELISA were done in low-incidence-
rate countries and showed a pooled sensitivity of 70%.
Studies on ELISPOT and the TST were conducted in
both high- and low-incidence countries and a similar
pooled sensitivity was found (ELISPOT: 64 vs. 61%; TST:
71 vs. 71%).
Specificity of IGRAs and the TST
For studies assessing specificity, the participants enrolled
were low-risk individuals without identified exposure to
active tuberculosis, regardless of BCG vaccination.
The rate of BCG vaccination of the participants varied
(0–100%). As shown in Fig. 3, the pooled specificity was
100% for ELISA studies (73/73, 95% CI 84–100%), 90%
for ELISPOT studies (342/381, 95% CI 86–93%) and
56% for TST studies (214/385, 95% CI 50–61%). Because
only three studies targeting the evaluation of ELISA dem-
onstrated a high specificity, we chose to focus on the
comparison of ELISPOT and the TST in further analysis.
The specificity of ELISPOT was affected only slightly by
BCG vaccination status (89% for vaccinated vs. 95% for
unvaccinated), or by national incidence status (95% for
high-incidence vs. 86% for low-incidence groups). On the
other hand, the specificity of the TST was significantly
affected by BCG vaccination status (49% for vaccinated
vs. 93% for unvaccinated).
Concordance between IGRAs and the TST
Seven studies assessed the concordance between IGRAs
and the TST with varying rates of BCG vaccination.
Among them, five studies concluded that agreement
between TST and IGRA tests in non-BCG-vaccinated
children is higher than that in BCG-vaccinated children.
For example, one study (Tsolia et al., 2010) assessed the
concordance between ELISA and the TST according to
BCG immunization status, and found that among non-
BCG-immunized patients agreement was excellent (j =0.34–1.00), while among BCG-immunized children it was
fair to poor (j = 0.02–0.28).
Discussion
It is estimated that pediatric cases account for 10–15% of
the global tuberculosis case load. Diagnosis of pediatric
tuberculosis is challenging because of the limitations of
conventional methods. Culture and microscopy findings
are often negative in children. Advances in molecular
biology and genomics have led to alternatives to the TST
(Pai et al., 2006; Starke, 2006). Commercially available
IGRAs have evolved rapidly, and they have been widely
used in many settings. Regrettably, researchers have lim-
ited access to evaluate the assays in the field of pediatric
tuberculosis. Meta-analyses can increase the effective sam-
ple size under investigation through the pooling of data
from individual association studies, thereby enhancing
statistical power for assessing sensitivity and specificity of
IGRAs and the TST.
In our review, the sensitivity of the two commercial
IGRAs and the TST shows an equivalent sensitivity in
active tuberculosis. Results from an earlier review indi-
cated that a lower sensitivity of ELISA and the TST have
been found in pediatric tuberculosis compared with
402 articles screened
16 articles finally included into review Sensitivity: 14 Specificity: 7
52 articles excluded: Using in-house IGRAs other than T-SPOT.TB and QuantiFERON-TB Gold (n = 10)Study on participants with HIV infection or other immune compromises (n = 29)Study on participants received anti-tuberculosis treatment (n = 13)
196 articles included for further screening
206 articles excluded: Reviews and meta analysis (n = 59) Editorials (n = 14) Guidelines (n = 6) Case reports (n = 6) Non-diagnostic tests on TB (n = 88) Animal studies (n = 14) Non-English articles (n = 19)
144 articles included for further review
128 articles excluded: Study enrolled participants aged ≥18 year orincluding both children and adults (n = 95)Insufficient data for the meta analysis (n = 33)
Fig. 1. Flow chart of article selection.
FEMS Immunol Med Microbiol 63 (2011) 165–173 ª2011 Federation of European Microbiological SocietiesPublished by Blackwell Publishing Ltd. All rights reserved
IFN gamma and pediatric tuberculosis 167
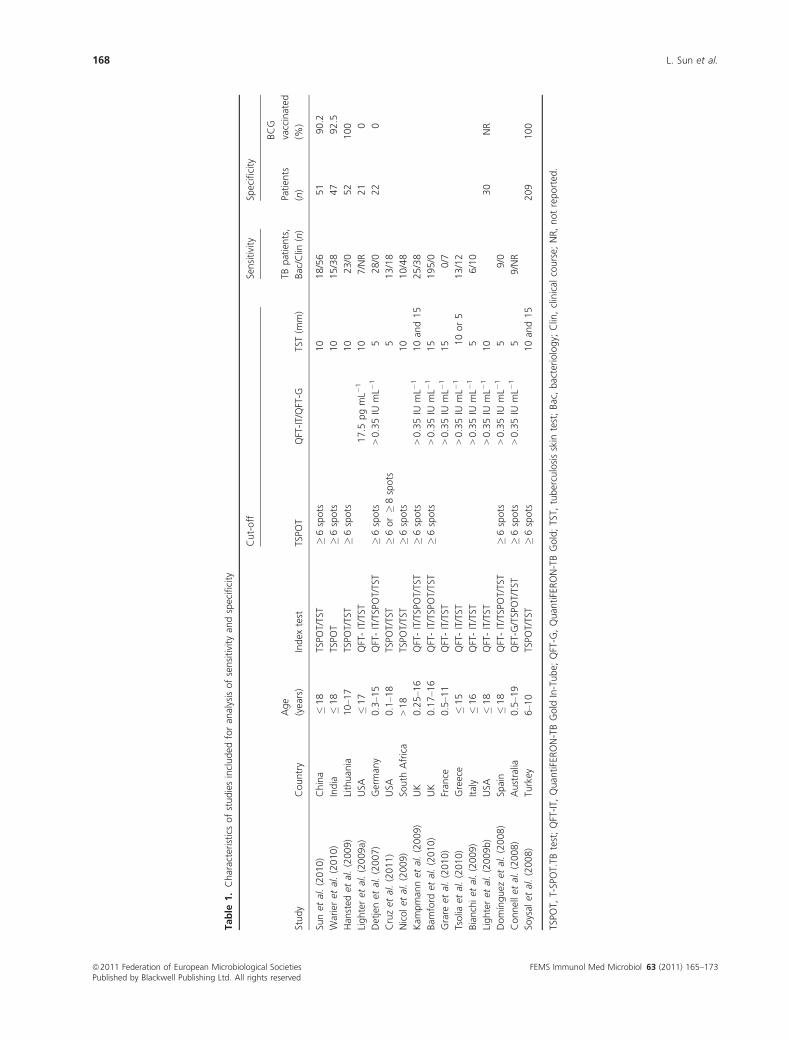
Table
1.Characteristicsofstudiesincluded
foran
alysisofsensitivity
andspecificity
Study
Country
Age
(years)
Index
test
Cut-off
Sensitivity
Specificity
TSPO
TQFT-IT/QFT-G
TST(m
m)
TBpatients,
Bac/Clin
(n)
Patien
ts
(n)
BCG
vaccinated
(%)
Sunet
al.(2010)
China
�18
TSPO
T/TST
�6spots
10
18/56
51
90.2
Warieret
al.(2010)
India
�18
TSPO
T�6spots
10
15/38
47
92.5
Han
sted
etal.(2009)
Lithuan
ia10–1
7TSPO
T/TST
�6spots
10
23/0
52
100
Lighteret
al.(2009a)
USA
�17
QFT-IT/TST
17.5
pgmL�
110
7/NR
21
0
Detjenet
al.(2007)
German
y0.3–1
5QFT-IT/TSPOT/TST
�6spots
>0.35IU
mL�
15
28/0
22
0
Cruzet
al.(2011)
USA
0.1–1
8TSPO
T/TST
�6or�8spots
513/18
Nicolet
al.(2009)
South
Africa
>18
TSPO
T/TST
�6spots
10
10/48
Kam
pman
net
al.(2009)
UK
0.25–1
6QFT-IT/TSPOT/TST
�6spots
>0.35IU
mL�
110an
d15
25/38
Bam
ford
etal.(2010)
UK
0.17–1
6QFT-IT/TSPOT/TST
�6spots
>0.35IU
mL�
115
195/0
Grare
etal.(2010)
Fran
ce0.5–1
1QFT-IT/TST
>0.35IU
mL�
115
0/7
Tsolia
etal.(2010)
Greece
�15
QFT-IT/TST
>0.35IU
mL�
110or5
13/12
Bianchiet
al.(2009)
Italy
�16
QFT-IT/TST
>0.35IU
mL�
15
6/10
Lighteret
al.(2009b)
USA
�18
QFT-IT/TST
>0.35IU
mL�
110
30
NR
Domınguez
etal.(2008)
Spain
�18
QFT-IT/TSPOT/TST
�6spots
>0.35IU
mL�
15
9/0
Connellet
al.(2008)
Australia
0.5–1
9QFT-G
/TSPOT/TST
�6spots
>0.35IU
mL�
15
9/NR
Soysal
etal.(2008)
Turkey
6–1
0TSPO
T/TST
�6spots
10an
d15
209
100
TSPO
T,T-SPOT.TB
test;QFT-IT,
Quan
tiFERON-TBGold
In-Tube;
QFT-G
,Quan
tiFERON-TBGold;TST,
tuberculosisskin
test;Bac,bacteriology;
Clin,clinical
course;
NR,notreported
.
ª2011 Federation of European Microbiological Societies FEMS Immunol Med Microbiol 63 (2011) 165–173Published by Blackwell Publishing Ltd. All rights reserved
168 L. Sun et al.

(a) (b)
(c)
Fig. 2. Forest plot of studies estimating sensitivity of the three tests in patients with active tuberculosis: (a) ELISA, (b) ELISPOT, (c) TST. The red
circles and horizontal lines correspond to the recorded percentage of true positive results among tuberculosis cases and their respective 95% CI.
The area of the red circles reflects the weight each study contributes to the analysis. The diamond represents the pooled value with its 95% CI.
Failed or indeterminate test results were not included in the analysis.
FEMS Immunol Med Microbiol 63 (2011) 165–173 ª2011 Federation of European Microbiological SocietiesPublished by Blackwell Publishing Ltd. All rights reserved
IFN gamma and pediatric tuberculosis 169

(a)
(b)
(c)
Fig. 3. Forest plot of studies estimating specificity of the three tests in healthy children without identified exposure to active tuberculosis:
(a) ELISA, (b) ELISPOT, (c) TST. The red circles and horizontal lines correspond to the recorded percentage of true positive results among
tuberculosis cases and their respective 95% CI. The area of the red circles reflects the weight each study contributes to the analysis. The
diamond represents the pooled value with its 95% CI. Failed or indeterminate test results were not included in the analysis.
ª2011 Federation of European Microbiological Societies FEMS Immunol Med Microbiol 63 (2011) 165–173Published by Blackwell Publishing Ltd. All rights reserved
170 L. Sun et al.

adults (Menzies et al., 2007). Our data agree with find-
ings in other studies that the sensitivities of the three tests
(62–71%) are lower than those in adults (70–89%) (Jiang
et al., 2007; Pai et al., 2008; Diel et al., 2010). The results
of the three tests are based on the reaction of the immu-
nological effecter cells. It has been reported that CD4+
T cells were the major cell type producing interferon-
gamma (IFN-c), a type 1 cytokine which plays an impor-
tant role in the host immune response (Leung et al.,
2009). Some authors underline that there were statistically
significant differences in CD4+ T-cell subpopulations
between children at different ages (P < 0.05) (Lee et al.,
1996; Kam et al., 2001). As a consequence, we concluded
that a special diagnostic threshold for a positive result
may be adjusted for children based on their suboptimal
and developmental cellular immune responses.
The relatively poor performance of IGRAs in clinically
diagnosed cases remains a concern. Because of the pauci-
bacillary nature of the disease, the diagnosis of active
tuberculosis is often based on a combination of clinical
signs and symptoms, suggestive radiology, history of
household exposure, as well as the TST reaction. Accord-
ing to the decreased pooled sensitivity in clinical diag-
nosed tuberculosis in this analysis, some of the cases could
be over diagnosed as active tuberculosis due to the overlap
of symptoms with other childhood illnesses. Pediatric
tuberculosis clinicians had high hopes that applying the
results of IGRAs to guide clinical diagnosis would be more
helpful. The disappointing lack of sensitivity of IGRAs in
the context of clinical cases may be a result of failure to
detect IFN-c produced by antigen-specific T cells. To date,
in the absence of bacterial evidence, we cannot determine
if children with active tuberculosis were missing. Large
cohort studies are required to elucidate this issue.
The most important finding in this analysis is the sig-
nificantly low specificity of the TST and a high specificity
of IGRAs regardless of BCG vaccination of the subjects
enrolled. Although all the children enrolled for assessing
specificity have no identified tuberculosis risk, there was a
high rate of TST-positive cases – almost all false positive.
A significant reason is the effect of BCG vaccination.
First, among six studies assessing specificity of the TST,
three were available with BCG-vaccinated children, result-
ing in distinctly low specificities. When these studies were
removed from consideration, the pooled specificity of the
TST was remarkably improved. The specificity of the
IGRAs remained high in mostly BCG-vaccinated children.
Our findings were in line with the study of Menzies et al.
(2007), emphasizing that the average specificity of IGRAs
with RD1 antigens was 97.7 and 92.2% for ELISA and
ELISPOT, respectively, and were both more specific than
the TST in cases of BCG vaccination. Secondly, when
assessing the concordance between IGRAs and the TST
with varying rates of BCG vaccination, five studies con-
cluded that agreement between TST and IGRA tests in
BCG-vaccinated children is lower than that in non-BCG-
vaccinated children. According to our review, BCG
immunization can cause false positive reactions in the
TST but not in IGRAs which use antigens (ESAT-6 and
CFP-10) not present in BCG or in common environmen-
tal mycobacteria. The cut-off value for a TST-positive
result varies greatly, from 5, 10 and up to 15 mm of
induration, and there is no good conclusion supporting a
particular reasonable cut-off for injection of PPD (puri-
fied protein derivative) intradermally as positive in BCG-
immunized children. As a result, despite the cost and
complexity of IGRAs, they will be increasingly used in
screening LTBI in children with or without identified
tuberculosis risk.
Infection with NTM is also associated with high false-
positive results. The effect of NTM infection on IGRAs
and the TST is poorly studied. Only one study (Detjen
et al., 2007) enrolled 23 children with bacteriologically
confirmed nontuberculous mycobacterial lymphadenitis.
The specificity of the TST was only 10.5% in these chil-
dren, with as a consequence false-positive results of NTM
infection. In contrast, the specificity for excluding tuber-
culosis was significantly better using the IGRAs (QFT-G
specificity 100%, 95% CI 91–100%, P < 0.001; T-SPOT
specificity 98%, 95% CI 87–100%, P < 0.001). It was
shown in this analysis that the IGRAs had a higher speci-
ficity and, in contrast with the TST, may be used to con-
firm positive TST results in children in areas with a high
incidence of BCG vaccination or NTM infection.
Our meta-analysis also suffers from a number of limi-
tations. Although sensitivity and specificity are useful in
assessing the diagnostic value of a test, we are compro-
mised by the lack of a gold standard of latent tuberculo-
sis. It is possible that some individuals enrolled in
specificity assessment in this meta-analysis had latent
tuberculosis infection, despite the fact that they had no
identified risk factors. Longitudinal studies are needed to
determine the incidence of active tuberculosis in partici-
pants with positive and negative results. According to our
strict inclusion criteria, only the commercial tests, QFT-G,
QFT-IT and T-SPOT, were within the scope of this analy-
sis, so the number of studies is insufficient and most of
them are small. The heterogeneous nature of the method-
ology also limited the comparability of the studies, so
additional studies are needed to better define their perfor-
mance in diagnosis of pediatric tuberculosis.
Conclusion
Although the results of our analysis should be interpreted
with caution, the results could provide useful information
FEMS Immunol Med Microbiol 63 (2011) 165–173 ª2011 Federation of European Microbiological SocietiesPublished by Blackwell Publishing Ltd. All rights reserved
IFN gamma and pediatric tuberculosis 171

to practising clinicians. In addition, most of the studies
were published in the past 3 years, making this analysis
up to date and timely.
We hope that research will focus on identifying vari-
ables that were associated with positive results for each
assay in pediatric tuberculosis, for example age, BCG vac-
cination, contact history and tuberculosis incidence rate
of the enrolled countries.
Acknowledgements
A.S. and L.S. conceived and designed the study. L.S. and
J.X. performed searches and selected articles according to
the inclusion criteria designed in advance. Q.M., W.F.,
X.W., Q.Y., W.J., C.S., F.L. and D.S. contributed to
materials/analysis tools. All authors read and approved the
final manuscript. We thank Hugh Nelson and Jifan Hu for
revision of the English text. This study was supported in part
by grants from the National Natural Science Foundation of
China (Nos. 30872788 and 81071315), Beijing Municipal
Science Technology Commission (No. Z09050700940903)
and Young Scientists fund of Beijing Health Bureau (No.
QN2010-025).
Authors’ contribution
L.S. and J.X. contributed equally to this study.
References
Bamford AR, Crook AM, Clark JE et al. (2010) Comparison of
interferon-c release assays and tuberculin skin test in
predicting active tuberculosis (TB) in children in the UK: a
paediatric TB network study. Arch Dis Child 95: 180–186.Bianchi L, Galli L, Moriondo M, Veneruso G, Becciolini L,
Azzari C, Chiappini E & de Martino M (2009) Interferon-
gamma release assay improves the diagnosis of tuberculosis
in children. Pediatr Infect Dis J 28: 510–514.Connell TG, Ritz N, Paxton GA, Buttery JP, Curtis N &
Ranganathan SC (2008) A three-way comparison of
tuberculin skin testing, QuantiFERON-TB gold and
T-SPOT.TB in children. PLoS ONE 3: e2624.
Cruz AT, Geltemeyer AM, Starke JR, Flores JA, Graviss EA &
Smith KC (2011) Comparing the tuberculin skin test and
T-SPOT.TB blood test in children. Pediatrics 127: e31–e38.Detjen AK, Keil T, Roll S, Hauer B, Mauch H, Wahn U &
Magdorf K (2007) Interferon-gamma release assays improve
the diagnosis of tuberculosis and nontuberculous
mycobacterial disease in children in a country with a low
incidence of tuberculosis. Clin Infect Dis 45: 322–328.Diel R, Loddenkemper R & Nienhaus A (2010) Evidence-
based comparison of commercial interferon-c release assays
for detecting active TB: a metaanalysis. Chest 137: 952–968.
Domınguez J, Ruiz-Manzano J, De Souza-Galvao M et al.
(2008) Comparison of two commercially available gamma
interferon blood tests for immunodiagnosis of tuberculosis.
Clin Vaccine Immunol 15: 168–171.Grare M, Derelle J, Dailloux M & Laurain C (2010)
QuantiFERON-TB Gold In-Tube as help for the diagnosis
of tuberculosis in a French pediatric hospital. Diagn
Microbiol Infect Dis 66: 366–372.Hansted E, Andriuskeviciene A, Sakalauskas R, Kevalas R &
Sitkauskiene B (2009) T-cell-based diagnosis of tuberculosis
infection in children in Lithuania: a country of high
incidence despite a high coverage with bacille Calmette-
Guerin vaccination. BMC Pulm Med 9: 41–48.Jiang J, Shi HZ, Liang QL, Qin SM & Qin XJ (2007) Diagnosis
value of interferon-c in tuberculosis pleurisy: a metaanalysis.
Chest 131: 1133–1141.Kam KM, Leung WL, Wong KH, Lee SS, Hung MY & Kwok
MY (2001) Maturational changes in peripheral lymphocyte
subsets pertinent to monitoring human immunodeficiency
virus-infected Chinese pediatric patients. Clin Diagn Lab
Immunol 8: 926–931.Kampmann B, Whittaker E, Williams A, Walters S, Gordon A,
Martinez-Alier N, Williams B, Crook AM, Hutton AM &
Anderson ST (2009) Interferon-gamma release assays do not
identify more children with active tuberculosis than the
tuberculin skin test. Eur Respir J 33: 1374–1382.Lee BW, Yap HK, Chew FT, Quah TC, Prabhakaran K, Chan
GS, Wong SC & Seah CC (1996) Age- and sex-related
changes in lymphocyte subpopulations of healthy Asian
subjects: from birth to adulthood. Cytometry 26: 8–15.Leung WL, Law KL, Leung VS, Yip CW, Leung CC, Tam CM
& Kam KM (2009) Comparison of intracellular cytokine
flow cytometry and an enzyme immunoassay for evaluation
of cellular immune response to active tuberculosis. Clin
Vaccine Immunol 16: 344–351.Lighter J, Rigaud M, Huie M, Peng CH & Pollack H (2009a)
Chemokine IP-10: an adjunct marker for latent tuberculosis
infection in children. Int J Tuberc Lung Dis 13: 731–736.Lighter J, Rigaud M, Eduardo R, Peng CH & Pollack H (2009b)
Latent tuberculosis diagnosis in children by using the
QuantiFERON-TB Gold In-Tube test. Pediatrics 123: 30–37.Marais BJ, Gie RP, Schaaf HS, Beyers N, Donald PR & Starke
JR (2006) Children pulmonary tuberculosis: old wisdom and
new challenges. Am J Respir Crit Care Med 173: 1078–1090.Menzies D, Pai M & Comstock G (2007) Meta-analysis: new
tests for the diagnosis of latent tuberculosis infection: areas
of uncertainty and recommendations for research. Ann
Intern Med 146: 340–354.Nicol MP, Davies MA, Wood K et al. (2009) Comparison of
T-SPOT.TB assay and tuberculin skin test for the evaluation
of young children at high risk for tuberculosis in a
community setting. Pediatrics 123: 38–43.Pai M, Kalantri S & Dheda K (2006) New tools and emerging
technologies for the diagnosis of tuberculosis: part I. Latent
tuberculosis. Expert Rev Mol Diagn 6: 413–422.
ª2011 Federation of European Microbiological Societies FEMS Immunol Med Microbiol 63 (2011) 165–173Published by Blackwell Publishing Ltd. All rights reserved
172 L. Sun et al.

Pai M, Zwerling A & Menzies D (2008) Systematic review:
T-cell-based assays for the diagnosis of latent tuberculosis
infection: an update. Am Coll Phys 149: 177–184.Rigouts L (2009) Clinical practice. Diagnosis of children
tuberculosis. Eur J Pediatr 168: 1285–1290.Soysal A, Turel O, Toprak D & Bakir M (2008) Comparison of
positive tuberculin skin test with an interferon-gamma-based
assay in unexposed children. Jpn J Infect Dis 61: 192–195.Starke JR (2006) Interferon-gamma release assays for diagnosis
of tuberculosis infection in children. Pediatr Infect Dis J 25:
941–942.Sun L, Yan HM, Hu YH, Jiao WW, Gu Y, Xiao J, Li HM, Jiao
AX, Guo YJ & Shen AD (2010) IFN-c release assay: a
diagnostic assistance tool of tuberculin skin test in pediatric
tuberculosis in China. Chin Med J 123: 2786–2791.Tsolia MN, Mavrikou M, Critselis E, Papadopoulos NG,
Makrinioti H, Spyridis NP, Metsou F, Tsagaraki M,
Koulouri M & Kafetzis DA (2010) Whole blood interferon-crelease assay is a useful tool for the diagnosis of
tuberculsosis infection particularly among Bacille Calmette
Guerin-vaccinated children. Pediatr Infect Dis J 29: 1137–1140.
Warier A, Gunawathi S, Venkatesh, John KR & Bose A (2010)
T-cell assay as a diagnostic tool for tuberculosis. Indian
Pediatr 47:90–92.
FEMS Immunol Med Microbiol 63 (2011) 165–173 ª2011 Federation of European Microbiological SocietiesPublished by Blackwell Publishing Ltd. All rights reserved
IFN gamma and pediatric tuberculosis 173


















